
Abstract
Most child-friendly court reforms are based on the assumption that the court setting is a stressful experience. Our objective was to analyze the acute stress levels of children who come to testify in a child-friendly investigative court using a person-by-environment approach. We employed a simple repeated measures design for this study, which included 42 minors of Spanish nationality who provided testimony as victims of violence in Spain’s inaugural Child-Friendly Court. Among the participants, 73.8% were girls with a mean age of 12.5 years (SD = 3.4), and 26.2% were boys with a mean age of 11.4 years (SD = 3.1). Stress levels were measured using heart rate variability, and anxiety was assessed using state-trait questionnaires. The study found that the mean percentile of anxiety remained at moderate levels, while stress remained at medium-low levels. No significant differences in anxiety or stress were found based on gender or type of crime. Repeated measures ANOVA revealed significant differences in stress levels among different court settings. Stress levels in the waiting room and Gesell room were significantly higher than those in the decompression room. In conclusion, the experience of testifying in a Gesell room about the aggressions suffered increases stress levels. However, in this sample and for this Pilot Court, the stress levels observed during testimony did not reach levels considered detrimental to children’s health. Our results lend support to the new European Judicial Policy, which includes the establishment and operation of Specialized Courts adapted to the needs of children and adolescents.
Similar content being viewed by others

Introduction
Acute stress can have deleterious effects on brain functioning (Zhang et al., 2020), even inducing depressive disorders in some cases (Hossein et al., 2023). Specifically, psychological stress associated with the criminal justice process has been linked to Secondary Victimization (SV). The court process especially in criminal trials does not typically take into account the developmental constraints of children nor do they fully understand trauma in children and the risks to testifying child witnesses (Crenshaw et al., 2019).
Some authors argue that young people who experience high levels of stress while testifying are more likely to report serious mental health problems later in life (Quas et al., 2005). In contrast to studies concluding that a high proportion of victims reported negative and traumatic effects associated with going through the justice system (Goodman et al., 1992), other studies have found no negative impact associated with testifying, and some authors have even suggested a potential restorative effect (Daignault et al., 2017). This discrepancy in studies regarding the harmful effects of having children testify in court can be explained through the lens of Carretta and García-Quiroga’s hypothesis (2021). They argue that participation in judicial processes is not inherently traumatic for minors; rather, it is strongly influenced by the specific conditions under which such participation occurs.
The new European Judicial Policy is placing special emphasis on justice that is specifically adapted to children, recognizing the unique needs and vulnerabilities of young individuals within the legal system. In November 2010, the Council of Europe published the Guidelines on child-friendly justice (2011) with the aim of safeguarding children and youth from secondary victimization. One of the main guidelines for child-friendly justice is the organization of the proceedings, a child-friendly environment, and the use of child-friendly language. Subsequently, the European Union Agency for Fundamental Rights (FRA) (2017), in its summary of children’s and professionals’ perspectives and experiences on Child-Friendly Justice, warns that children feel stressed when they have to testify in non-child-friendly environments, and not only when they have to speak more than once or in front of many people. To alleviate this stress for victims, they urge EU member states to use child-friendly facilities to listen to children, as well as video recording as a standard practice in criminal proceedings.
The Spanish Judicial System has implemented various measures to tailor the administration of justice to the specific needs of children and adolescents, while considering their unique vulnerabilities. One of the initial measures taken by the courts to gather testimony from minor victims while safeguarding their psychological well-being is the recording of their statements, which are subsequently incorporated as documentary evidence during the oral hearing, a procedure known in Spain as Preconstituted Evidence. Initially, this child victim witness videotaping (or Preconstituted Evidence) was incorporated into the Spanish judicial process as an advisable practice in cases of sexual violence; nowadays, it has been extended and is a compulsory protection mechanism in the taking of statements of all minors under 14 years of age who are victims of any type of violence (García, 2022). Preconstituted evidence serves two fundamental purposes: firstly, to prevent the repercussions of secondary victimization of the child; secondly, to safeguard the evidentiary element (the child’s testimony as witness evidence) to ensure the acquisition of the material truth (Sotoca, et al., 2013).
In Spain, since the beginning of the 21st century, the classic Gesell Room has been used to carry out child victim videotaping. These rooms have been widely used in different justice systems around the world and have proven useful in gathering accurate information and protecting the welfare of children involved in legal cases (Arantegui, 2022). Recently, these rooms have been replaced with modern, child-friendly designs in order to create a safe and comfortable environment, thereby reducing their potential as stressors. Goodman et al. (1998) reported that children who were to testify in court expressed greater anticipatory anxiety than those who expected to be questioned via closed-circuit television (CCT). In these modern examination rooms, mirrors have been replaced by video cameras connected to CCTV.
On 1 October 2021, Court of Instruction 3 in Las Palmas de Gran Canaria (Spain) became the first Spanish court specialized in cases involving violence against children and adolescents (Poder Judicial, 2021). Its main objective is to prevent SV by adapting its physical environment and procedures to children. Although we can find another similar pilot experience in a New Zealand court (Randell et al., 2022), in the first Spanish court specialized in cases involving violence against children and adolescents (the Pilot Court), we find a way of protecting children from acute stress that is unprecedented in the history of the courts. Based on scientific evidence, which suggests that Heart Rate Variability (HRV) biofeedback is useful for stress management (Goessl et al., 2017; Nolan et al., 2005; Prinsloo et al., 2013; Sherlin et al., 2009), the new court incorporated real-time stress measurement using a smart band as a preventive protective measure. The protocol of the Pilot Court included the possibility to momentarily stop the forensic interview, to introduce relaxation techniques or even to finish the interview if the reported stress levels were high, always in the best interests of the child.
This method of protecting minors from acute stress during the trial, involving real-time monitoring of stress, was an exclusive feature of this Pilot Court; otherwise, it adhered to the guidelines of the Council of Europe for child-friendly justice (2011). The examination of statements from child victims and witnesses took place in facilities specially designed for children, within an environment adapted and welcoming to them. Interview and waiting rooms were arranged for children in a child-friendly environment, along with a Decompression room to alleviate stress after providing their statement and before leaving the court.
Although court involvement is often perceived as stressful and distressing by young people (Eastwood, 2003; Randell et al., 2022), there are few quantitative scientific studies with objective measures to help us understand in depth the degree of stress experienced by children in a courtroom context. An exception is the empirical study conducted by Saywitz and Nathanson (1993), as well as the subsequent work by Nathanson and Saywitz (2003), in which they analyzed the heart rate variability (HRV) of children questioned in a simulated trial scenario. Based on these measurements, the researchers concluded that children questioned in the courtroom exhibited higher levels of stress compared to children interviewed in a small, private room. Since then, and in different parts of the world, several treatment approaches have been proposed to reduce the stress levels of children who come to testify (Cohen et al., 2006; Peterson et al., 2020).
Most reforms aimed at creating child-friendly courts are based on the assumption that the courtroom is experienced as stressful (Saywitz & Nathanson, 1993; Nathanson & Saywitz, 2003). However, we have not found studies with real victims, instead of simulated ones, that measure stress in real time and during the entire process of recording testimony in court, nor studies that tell us how much stress child victims or witnesses experience in the child-friendly court and during child victim videotaping. Do children endure high and potentially damaging levels of stress in child-friendly courts? This question guided our research. We conducted a field study that extends the work of Saywitz and Nathanson (1993). The objective is to analyze the acute stress levels of children who testify in a child-friendly investigative court using a person-by-environment approach. Repeated measures of stress (dependent variable) using Smart Bands were taken in the different courtrooms (contextual variable).
Method
The present study used a simple repeated-measures design (Arnau & Bono, 2008). We determined the sample size a priori to be sufficient through calculations performed with the GPower 3.1.9.4 computer program (Faul et al., 2007). Power analysis indicated that a total of 42 participants (number of measurements = 3) were needed for a medium partial η2 (0.06) when α = 0.05 for a power of 0.95 with 1 group. The statistical test selected was ANOVA: Repeated measurements within factors, from the F test family.
In 2022, the child-friendly Pilot Court conducted 80 sessions of Preconstituted Evidence, including victim witness videotaping; a sample of 42 constituted 52.5% of the total. We have encountered practical limitations in obtaining a sample larger than N = 42, mainly due to budgetary constraints and the availability of participants (real victims of violence who come forward to testify). However, repeated measures designs effectively diminish between-subject variability by employing each participant as their own control across multiple measurements. This inherent feature allows repeated measures designs to achieve heightened statistical power with a smaller sample size when contrasted with non-repeated designs (Zhang & Ahn, 2011). While non-repeated measures studies usually require hundreds of subjects, repeated-measures studies usually require only tens of subjects (Hopkins, 2020)
Participants
This study involved 42 minors, comprising both boys and girls, who were Spanish nationals and had provided statements as victims of violence to the Pilot Court in Las Palmas de Gran Canaria, Spain. Participants were selected through convenience sampling. Individuals over 18 years of age and those who did not provide statements in the modern Gesell Room were excluded from the study. No minors were excluded on the grounds of mental health or disability, as all had been previously assessed by the court psychologist and declared fit to testify in court.
Out of the sampled population, 73.8% comprised girls (n = 31), with ages ranging from 4 to 17 years (mean age = 12.5 years, SD = 3.4), while the remaining 26.2% constituted boys (n = 11), aged 7 to 17 years (mean age = 11.4 years, SD = 3.1). Most of the children were involved in cases of sexual assault (64.3%), while the remaining cases involved other forms of violence or abuse (35.7%). In the majority of instances, the violence occurred within the family (54.8%), with the reported perpetrators being primarily the father (23.8%), another relative (16.7%), or the mother (14.3%). Persons outside the family were the perpetrators in 45.2% of the cases. All participants came to court to testify as victims of violence and voluntarily participated in the real-time stress monitoring program. They also provided consent for the use of their anonymized data in the research.
Procedure
The stress measurements were taken on the fifth floor of Building III at the courthouse in Las Palmas de Gran Canaria.
Before the Child Victim Witness Videotaping session, a briefing meeting was held with family members or legal guardians to introduce them to the real-time stress monitoring program. The purpose of the meeting was to explain the dual objectives of the program: preventing elevated stress levels and collecting stress biomarker data for research purposes. On the day they went to court for Child Victim Witness Videotaping, they were presented with the Smart band and could choose to use it to prevent high levels of stress, to participate in the investigation, or both. The child also received an age-appropriate explanation in the presence of the accompanying parent or legal guardian. When the child and their legal representatives agreed to participate in the research, the adult signed the informed consent document, and the child became part of the study sample. A researcher, trained in preventing SV, greeted the child and their companion, presented the child to the smart band and its associated mobile device, and then positioned themselves in an adjacent room to manually measure the child’s stress levels. The researcher’s primary responsibility was child protection, involving real-time monitoring of children’s stress levels and immediate notification of the interviewer in case stress levels reached percentiles above 79. The researcher remained blinded to any subsequent data processing for the research.
The measures were taken in different courthouse rooms and in three different situations. The interior design of the rooms can be observed in the images available at Rodriguez-Pellejero et al. (2023). We took the same number of measurements at the same times so that the data would be balanced, cases with incomplete measurements were excluded. Following Arnau and Bono (2008), we refer to these temporal continuums that underlie the measurement of time as “occasions”:
-
Waiting Room (Occasion before): The researcher explained the objectives and also obtained verbal consent from the minor. She introduced the smart band device and calibrated the application following the manufacturer’s instructions, which included entering information such as age, weight, and activity level. In addition, the researcher completed the questionnaire provided by the application (Huawei Technologies Co., Ltd., 2022). In no case were identifying data of the child or the family member entered in order to preserve anonymity. Subsequently, the researcher retreats to an adjacent room, leaving the child in the care of a family member or companion. The first measurement (T1) is then taken after a 5-minute waiting period.
-
Gesell Room (Ocasion during): The new Gesell Room is a room with a child-friendly interior design, specifically designed to alleviate stress. The room is equipped with a closed-circuit video system, and there are no mirrors. This arrangement allows both the individuals under investigation and the other magistrates and lawyers to be on the same floor but in separate sections with independent entrances and exits. In all cases, the Achieving Best Evidence Interview followed the same protocol and was conducted by the same person. in the adjacent room, the researcher conducts a stress measurement 10 minutes after the interview has begun (T2). At the time of the measurement, all children were either freely recounting the offences or responding to the interviewer’s open-ended questions. Previously, the interviewer had made the introduction, established rapport and informed the child of his or her rights.
-
Decompression Room (Occasion after): After the Best Evidence Gathering Interview concludes, the child is escorted to a Decompression Room situated 10 meters away from the Gesell Room. In this space, they are warmly welcomed and provided with support for a ‘return to a state of calm. In this room, the researcher takes 4 resting measurements, with a 3-minute time interval, while the child completes anxiety questionnaires. This is done in order to later assess the consistency of the measurements (T3, T4, T5 y T6). When the child is ready to leave the court, they are informed that the session has concluded, and they can return home. At this point, a final stress measurement (T7) is recorded. After the records have been imported into the database, the researcher proceeds by clearing the application cache, preparing it for a new participant.
Instruments
To measure state-trait anxiety in children under 15 years of age, we used the Spanish version (2001) of Spielberger’s State-Trait Anxiety Inventory for Children. The T-Anxiety (Trait Anxiety) subscale measures an individual’s general predisposition or tendency to experience anxiety over time. It assesses the child’s likelihood to experience anxiety across various situations, offering insights into their overall anxiety levels as a stable trait. The S-Anxiety (State Anxiety) subscale assesses the child’s anxiety level in response to specific situations or events at a particular moment in time. It specifically examines the temporary and situational aspects of anxiety, providing a snapshot of the child’s anxiety state in the present context. Each scale has 20 items that are answered on a Likert-3 scale, with higher scores indicating greater anxiety. Values for the A-State items range from 1 (not at all) to 3 (a lot), while the T-Anxiety is scored from 1 (almost never) to 3 (often). The Spanish version of the STAIC demonstrates high reliability on both the T-Anxiety subscale (KR-20 = 0.87) and the S-Anxiety subscale (KR-20 = 0.91). According to the scales of the Spanish adaptation of the questionnaire, individuals with percentiles between 1 and 33 were categorized as having low levels of anxiety, those with percentiles between 34 and 66 were categorized as having moderate anxiety, and those with percentiles of 67 or higher were categorized as having high anxiety.
To assess state-trait anxiety in individuals aged 16 and older, we utilized the STAI (Spielberger, 1989), in its Spanish adaptation by Buela-Casal, Guillén-Riquelme, and Seisdedos (2015). This is a self-administered questionnaire that assesses, through 40 items, anxiety from its two facets: trait (10 items) and state (10 items). The response scale is presented in Likert-4 forma, S-Anxiety ranges from 0 (not at all) to 3 (very much), while T-Anxiety ranges from 0 (almost never) to 3 (almost always). The STAI has excellent reliability ratings (Buela-Casal et al., 2015). For S-Anxiety, the categorical alpha calculated from the polychoric correlation matrix was 0.964. In the case of T-Anxiety, the reliability coefficient was 0.927. According to the scales of the Spanish adaptation of the questionnaire, low levels of anxiety were defined as percentiles between 1 and 30, medium anxiety as percentiles between 31 and 70, and high anxiety as percentiles of 71 or higher.
To measure stress in real-time, we utilize the HUAWEI Band 6 in green, along with its corresponding health app. The smart band weighs 18 grams, and has a 1.47-inch display and an optical heart rate sensor. View the image of the smart band model used at Rodriguez-Pellejero et al. (2023).
Some research confirms that real-time stress monitoring can be done using wearable devices that measure HRV (Chalmers et al., 2022). Jarchi et al. (2018) conducted a study where they simultaneously measured HRV using two instruments: the Huawei Smart Band and a finger probe sensor. Their findings indicated a high level of concordance between the HRV estimates obtained from both instruments, leading them to conclude that HRV could be reliably estimated using the Huawei smart band. Furthermore, several studies have incorporated this device into their research (Ding et al., 2021; Doan, 2023; Guo et al., 2020; Fan et al., 2019; Harrison et al., 2023). Although other similar devices also demonstrated validity and reliability (Hernando et al., 2018), the Huawei device was selected for two reasons: because it allows manual, real-time measurements to be taken and because of its low cost. The device was also chosen due to its efficiency and ease of use in transmitting health data quickly and conveniently via smartphones. We connect the smart band to the HUAWEI Health App through a mobile phone (Huawei Technologies Co., Ltd., 2022).
Vital signs were collected using photoplethysmography (PPG) with sensors incorporated into the smart band. The HRV was obtained from the associated app, the algorithm of this application calculates stress levels from HRV measurements (Ding et al., 2021). Employing sex and age data, the algorithms generate a stress score, which is subsequently standardized and presented in percentile comparisons.
HRV is defined as the variation over time in the period between consecutive heartbeats (Acharya et al., 2006) and has been used in different research as an objective measure of psychological stress and anxiety (Li et al., 2018; Park & Thayer, 2014; Szu et al., 2014; Taelman et al., 2009). According to Shaffer et al. (2014), there is a brain-heart connection pathway, with the brain innervating the heart through stimuli via the autonomic nervous system. Sympathetic activity leads to an increase in heart rate when faced with a stressor stimulus (Deschodt-Arsac et al., 2018), while parasympathetic activity induces a lower heart rate in states of relaxation (Lehrer & Gevirtz, 2014). The two circuits constantly interact and it is this interaction that is reflected in the HRV (Kim et al., 2018; Ernst, 2017).
Several researchers have identified HRV as the most useful physiological metric for the detection of stress and anxiety (Hernando et al., 2018; Hong et al., 2010; Rodrigues et al., 2018). In a recent systematic review, the authors concluded that individuals with high trait anxiety tend to exhibit decreased HRV (Immanuel et al., 2023). HRV, as an index of psychological stress, has been previously investigated using prediction models by Ohsuga, Shimono, and Genno (2001) and Plarre et al. (2011). These studies concluded that HRV is a useful tool for discriminating between stressed and unstressed individuals.
Velmovitsky et al., 2023 explored the potential of smartwatches to quantify individual stress levels within real-world contexts, and their findings underscore the significance of smartwatches as a minimally intrusive instrument for monitoring stress. According to Martínez et al. (2022), HRV measures improve their predictive power for stress when used in controlled environments with specific stressors, so a courtroom could be an ideal opportunity to test its validity.
HRV measures exhibit explicit directional tendencies, making them useful for distinguishing between stressful and non-stressful conditions (Castaldo et al., 2015), and they have been used to determine whether a subject was more or less stressed than before. (Li et al.,2018). Some studies have tested the validity of wearable devices employing the PPG (photoplethysmography) sensor, like the Huawei Smart band we utilized. These studies have concluded that these devices can offer an alternative solution for measuring HRV, especially during periods of rest or light exercise, as their accuracy tends to decrease with higher levels of physical exertion (Georgiou et al., 2018). In a recent study conducted using the same smart band model as ours, researchers observed an average relative error in heart rate measurement of 1.4% (Peña, 2021). Another study validated the HRV measurement of a Huawei Watch equipped with a PPG sensor similar to that of the smart band 6. Employing an experimental design and comparing the measurements obtained from three different devices, the authors observed a strong agreement between the Huawei Watch and the other two devices in HRV measurement (Jarchi, et al., 2018). According to the Huawei application’s scales, low stress was considered when scores ranged from 1 to 29, medium-low stress when scores ranged from 30 to 59, medium-high stress when scores ranged from 60 to 79, and high stress when scores were 80 or higher (Ding et al., 2021).
Data analysis
Test-retest reliability was assessed by calculating the Pearson correlation coefficient for four measures taken under similar conditions. These measures were obtained in the Decompression Room, while the children were completing the anxiety questionnaires. To assess discriminant validity, we incorporated scores from various conditions with varying stressor potential into the correlation analysis. To evaluate convergent validity, we will examine the correlations between stress levels and state and trait anxiety scores. In a real situation, where a statement is taken from a child regarding sexual abuse or other forms of child maltreatment, data collection for the investigation should be conducted using non-invasive methods. The Spielberger anxiety questionnaire (2001) cannot be administered before, during, and after statement taking. For this reason, it has been used only to test the convergent validity of stress measures taken with the Smart band, a less invasive instrument that does not require the child to pay attention to the instrument and allows them to focus on the interviewer’s questions. The benefits of smartwatches over other devices include portability, compactness, low cost, and ease of use (Ding et al., 2021).
We conducted a descriptive analysis of the sample, calculating means and standard deviations for stress percentiles on three different occasions: in the Waiting Room, in the Gesell Room, and in the Decompression Room. Additionally, we assessed state and trait anxiety in the decompression room on a single occasion. Considering that both the smart band and the Spielberger anxiety tests yield percentile scores, placing each subject about their normative reference group and that the versions used to measure child anxiety employed Likert-3 scales, while those used for adolescents featured Likert-4 scales, we chose to use percentiles. For stress, we obtained them using the app’s algorithm, and for anxiety, we extracted them from tables of scales adapted to the Spanish population—the SATIC scale for boys and girls (Spielberger, 2001, p. 19), and the STAI scale for adolescents and adults (Buela-Casal et al., 2015, p. 38). Some authors argue that percentiles can replace raw scores in the statistical analysis of test data and that the use of percentiles, instead of raw scores, in statistical analysis protects the type I error rate and increases the power of t-tests for skewed distributions (Zimmerman & Zumbo, 2005). The variability in anxiety and stress scores was assessed by calculating the Interquartile Range (IQR), which offers a robust measure of dispersion around the median.
Independent samples t-tests were performed to assess baseline differences in anxiety and stress levels between genders, as well as between two types of offense categories: sexual assault and other forms of violence.
To find out whether there were significant differences in children’s stress levels before, during, and after videotaping, we conducted a repeated measures ANOVA and a post hoc Bonferroni test. As an intra-individual factor, we are considering different contexts within the Child-Friendly Court, comprising three levels or occasions: the Waiting Room, the Gesell Room, and the Decompression Room. The normality of the stress variable was previously assessed using the Shapiro-Wilk test, with a significance level of alpha = 0.05. Mauchly’s test was used to confirm the sphericity of the variance-covariance matrix. In repeated measures ANOVA designs, when no between factors are included, and there are no interactions, homogeneity of variance is not a requirement, and Mauchly’s sphericity criterion is sufficient (Arnau & Bono, 2008). The software package SPSS v.28 for Windows (IBM Corp) was used for all statistical analyses.
Results
Preliminary Analyses
Stress scores obtained during four consecutive assessments in the decompression room, conducted under similar conditions, exhibited bivariate correlations that ranged from statistically significant (p < 0.05) to highly significant (p < 0.01), providing evidence of test-retest stability. To assess discriminant validity, we computed correlations between stress measures across various conditions and potential stressors. Our analysis revealed no significant correlation between the stress levels reported in the Waiting Room and those in the other two rooms. However, we did observe a highly significant positive correlation between stress experienced in the Gesell Room and stress reported in the Decompression Room.
When we analyzed the correlations between anxiety (questionnaires) and stress (smart band) for convergent validity, we found a significant correlation (p < 0.05) and a positive association between S-Anxiety and stress in the Waiting Room. However, there was no significant correlation with stress reported in the Gesell Room or with stress reported at the time of completing the questionnaire in the Decompression Room, as would be expected. T-Anxiety also exhibited a positive and significant correlation (p < 0.01) with stress in the Waiting Room, but not with stress in either the Gesell Room or the Decompression Room (Table 1).
Intergroup stress and anxiety
Out of the total sample, only three children experienced high levels of stress, and this stress was exclusively observed in the Gesell Room during the Achieving Best Evidence Interview. In the Waiting Room, 2.4% of the participants experienced a low-stress level, 81.0% had a medium-low stress level, 16.7% had a medium-high stress level, and no participants had a high-stress level. In the Gesell Room, 9.5% of the participants experienced a low stress level, 66.7% had a medium-low stress level, 16.7% had a medium-high stress level, and 7.1% had a high stress level. In Decompression room, 19.0% of participants experienced a low stress level, 71.4% had a medium-low stress level, 9.5% had a medium-high stress level, and no participants had a high stress level.
The mean percentile score for S-Anxiety in the total sample was 53.62, with a considerable dispersion of scores (IQR = 56). For T-Anxiety, the mean percentile score was 55.12, also showing considerable dispersion (IQR = 61). The average stress reported by the Smartband in the Waiting Room was 47.32, with a small spread in the scores (IQR = 12); in the Gesell Room, it was 50.14, indicating a moderate dispersion of the data (IQR = 20.32), and in the Decompression Room, it was 39.93, with a small spread in the scores (IQR = 16).
Before evaluating the variations in stress levels across different situations, we deemed it essential to investigate whether there were disparities in scores based on gender, age, or the nature of the crime. If this were the case, the repeated measures analysis should include sex and type of crime as covariates. Table 2 shows the anxiety and stress scores assessed for each sex and on each occasion. No differences were found in anxiety or stress as a function of gender or type of crime. There were no significant age differences between boys and girls; however, significant differences in age were observed when considering the type of crime, the victims reporting sexual assault crimes were significantly older in age than victims of other violence. Did not find a significant correlation between age and stress in all three rooms. We did not observe a significant correlation between age and S-Anxiety. However, we did find a significant correlation between age and T-Anxiety (r = 0.37, p < 0.05); as age increases, T-anxiety tends to be higher.
Intrasubject stress and the judicial context
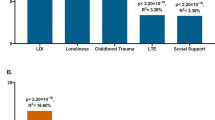
After checking for normality and assuming sphericity of the data, the ANOVA performed showed a significant effect of the different occasions on stress (F(2) = 9.91, p < 0.001, η²=0.195, β−1 = 0.981). Statistically significant differences were observed among at least two of the three measurement occasions, as illustrated in Fig. 1. 19.5% of the variability in stress levels is due to variation between occasions. The observed power is very high, indicating that we are unlikely to be making a type II error. Further post-hoc analyses were conducted to explore the specific nature of these differences and their implications for our study.

Real-time stress measurements of minors in the Waiting Room, Gesell Room, and Decompression Room.
Post hoc analysis with Bonferroni adjustment showed that participants experienced significantly higher levels of stress in the Gesell Room compared to leaving the courthouse (Decompression Room). There was no significant difference between stress in the Waiting Room and stress within the Gesell Room (Table 3).
Discussion
This research aimed to analyze the acute stress levels of children who testified in a child-friendly investigative court. It was found that most participants did not experience high levels of stress during their visit to the court to testify. In the context of the limitations of an investigation like the one proposed, when we separated minors into groups based on gender or the type of violence experienced, sexual assault, or other forms of violence, no significant differences were found in the acute stress of these minors during the statement-taking process. However, notable differences in intra-subject stress levels were identified depending on the context. This finding supports new judicial policies, which point out the importance of adapting procedures, offering a child-friendly environment, and the use of child-friendly language in court (Council of Europe. Committee of Ministers, 2011).
No previous studies have conducted measurements in real-time with real victims during court hearings; ours is the first. However, Hayes, Bunting (2013) examined the stress of children testifying in nonchild-friendly courts after the court process had concluded. The child victims responded to a questionnaire about experienced stress and anxiety, these authors concluded that young witnesses experience high levels of anxiety and stress before, during, and after trials. Like our study, Nathanson and Saywitz (2003) also measured stress in real-time using the HRV, but not in a real trial situation. Instead, they designed an experimental situation in which young individuals simulated trials in two different contexts: in a non-child-friendly courtroom and an educational setting. In their study, children questioned in the courtroom identified the experiences as more stressful than those in the control group. HRV measurements taken while testifying indicated significantly higher levels of stress in children testifying in the non-child-friendly courtroom compared to those in the group testifying in a school setting. Unlike studies that report high or harmful stress levels for children testifying in a regular court, our study found that stress levels measured in real-time did not reach levels considered harmful to health in a child-friendly court. In our research, the stress levels measured by the real-time smart-band did not reach levels that would be considered detrimental to health. The stress levels observed in our sample and compared to their normative sample remained at a medium level. The Gesell room emerged as the environment where the highest levels of stress were recorded, while the lowest levels were recorded in the Decompression room at the exit. These results also support Carretta and García-Quiroga’s hypothesis (2021) that participation in judicial processes is not inherently traumatic for minors.
When using a person-by-environment approach, we found statistically significant differences in stress levels among the three conditions: Waiting Room, Gesell Room, and Decompression Room. These findings support the research of Nathanson and Saywitz (2003), who also found a significant effect of the interview environment on the heart rate reactivity index and on responses given to the Court-Related Stress Scale, an instrument for measuring the level of trial stress. In Nathanson and Saywitz’s (2003) study, children interviewed in the courtroom demonstrated higher stress levels than children interviewed in a private courtroom. In our study, participants experienced significantly higher stress levels in the Gesell Room (during the deposition) compared to when leaving the courthouse, but there was no significant difference between stress levels in the Waiting Room (before the deposition) and the Gesell Room. Stress levels in the Waiting Room were also significantly higher compared to stress at the time of leaving the courthouse. These findings suggest that disclosing traumatic events within the Gesell room has an impact on participants’ stress levels, albeit without reaching levels that pose a threat to their health.
The moment when a child has to confront traumatic events from their past inside the Gesell room results in higher stress levels compared to the moment of leaving the courthouse. This could be interpreted as a stress release effect following the deposition. According to some authors, testifying can be considered empowering even after brief initial distress (Quas et al., 2005). The waiting room and the Gesell room elicit similar levels of stress in participants. Stress in the waiting room could be interpreted as anticipatory anxiety (Nathanson & Saywitz, 2015), especially considering its correlation with the results of the anxiety questionnaires.
Our results delineate three distinct phases during the court process of testifying: intially, a preliminary period of stress accumulation in the waiting room, associated with the anticipation of the statement shot that will be recorded on video; secondly, a peak of stress during the interview concerning violent events in the Gesell room; and lastly, a moment of stress relief upon exiting the courthouse. According to the SmartBand data, the children in the study perceived the Gesell room and the time when they had to mentally engage with the reported violent events as the most stressful. However, even in these cases, the SmartBands did not indicate “high stress”; there were no stress levels potentially harmful to health, according to this tool. In any case, we cannot interpret the average stress levels experienced by the participants in our study as a direct result of the anti-victimization measures implemented in this adapted court. On one hand, the methodological design of this study does not allow for the establishment of causal relationships. On the other hand, there is a theory suggesting that populations regularly exposed to stressful events tend to report lower initial levels of perceived stress and exhibit more attenuated biological stress responses to external stressors compared to the general population (Duan et al., 2013).
We also utilized anxiety self-report questionnaires to assess children’s anxiety immediately after testifying, measuring both trait anxiety and state anxiety. For our study sample, we did not observe high levels of anxiety in the questionnaires; instead, we found average levels, only slightly above the mean of their normative sample. We found no significant differences in anxiety when comparing by gender or when comparing the group that had experienced sexual assault with the group that had experienced other violence. However, we cannot rule out that, if we were to increase the sample size, differences in anxiety could appear according to gender or type of aggression.
When analyzing the relationship between the stress scores reported by the SmartBand and the anxiety scores reported in the questionnaires, we expected to find a high correlation between them, but this was not the case. The anxiety questionnaire scores only correlated significantly with the waiting room stress scores, not with the Gesell room stress nor with the Decompression room stress. This can be explained according to the Multidimensional Anxiety and Coping Theory (Endler & Kocovski, 2001). According to this model, anxiety state levels depend on both the stressful situation and the individual’s traits (T-anxiety), as well as on their coping resources. The authors argue that the situation must be congruent with the trait anxiety dimension to evoke increases in state anxiety.
The Multidimensional Anxiety and Coping Theory holds that anxiety and stress are different but related constructs. While anxiety is a dimensional construct, acute stress is a response to a situation that the subject assesses as threatening. Specifically, HRV is a biomarker that reflects the physiological defense response, that is, the ability to maintain the balance between sympathetic and parasympathetic activity in the presence of a stressor (Appelhans & Luecken, 2006; Chelidoni et al., 2020). Researchers such as Kim et al. (2011) also used HRV measures and also looked for correlations with measures from anxiety questionnaires (STAI), and from other questionnaires: anger (STAXI) and depression (BDI). These authors found correlations between HRV and anger-related defensive states but did not find correlations between HRV scores and anxiety scores. This suggests that HRV is capable of detecting defensive states in response to specific stressors, such as situations in which a child must testify in court regarding the aggressions suffered and identify the perpetrator. However, it may not be as effective at detecting more diffuse or low-level states of anxiety. Nathanson and Saywitz (2003) also found discrepancies between physiological and self-reported data and concluded that, like adults, children may not admit to the feelings they experience if they perceive them as socially undesirable. The difference between these two psychological phenomena, stress, and anxiety, along with the subjectivity in responses to the anxiety questionnaire, could explain the lack of correlation between anxiety and stress measures in certain contexts.
Beyond our main objective, an additional strength of this study is that it could provide further evidence of the reliability and validity of Smart bands in measuring stress through HRV. The way to verify the reliability of an instrument such as a smart band, unlike a questionnaire, is to observe the consistency or stability of different measurements under similar conditions. The smartband demonstrated test-retest consistency in resting situations and when no external stressors were identified. This finding is in agreement with that reported in the work of Georgiou et al. (2018). Furthermore, in agreement with other authors who also found no effect of gender and age on HRV-based stress (Pulopulos et al., 2018), the scores obtained in this research were not shown to be sensitive to these two individual variables. This may also be attributed to the inclusion of sex and age as data inputs during instrument calibration, which may have been taken into account by the application algorithm.
Regarding validity, we examine discriminant and convergent validity. The smartband also demonstrated discriminant validity, as it yielded significantly higher average readings in the Gesell Room compared to the Decompression Room, and these readings were found to be positively correlated. Our results confirm other studies that argue that HRV has directional tendencies and may be useful in distinguishing stressful and non-stressful conditions (Castaldo et al., 2015; Chalmers et al., 2022; Li et al., 2018; Nathanson & Saywitz, 2003). On the other hand, the convergent validity tests were inconclusive, this can be explained because we chose a questionnaire that does not mediate exactly the same phenomenon, and because the evaluation conditions could have influenced the responses to the questionnaires.
This research has certain limitations that need to be addressed. The Spielberger anxiety questionnaire has been used to test the convergent validity of stress measures taken with the smart band; however, the correlations have not turned out as expected. An important limitation is that we did not use a distress scale. It is also important to collect data from a larger sample, ensuring a more balanced representation of boys and girls to facilitate a more comprehensive gender analysis. Given that a control group was not used in the design, we cannot solely attribute the observed differences to the contextual factor. Additionally, the absence of an assessment of chronic stress is a limitation of this study, which focused solely on acute stress. Furthermore, a significant limitation is that children provided prior consent and received information about the objective of our research, which may have interfered with responses to the anxiety questionnaires, although not with the objective measures of the Smart bands. In any case, it would have been more comprehensive to collect state anxiety data both before and after statement taking, not only after.
Future lines of research could expand the sample and ensure a more balanced representation of boys and girls to facilitate a comprehensive gender analysis. Another avenue for research could involve adding comparative groups from other courts, enabling comparative-causal or quasi-experimental research. A comparison between stress levels in juvenile-adapted courtrooms and non-adapted courtrooms would be particularly beneficial.
In conclusion, in this sample and for this Pilot Court, the stress levels observed during testimony did not reach levels considered detrimental to children’s health. However, the experience of testifying in a Gesell Room about the aggressions suffered increases stress levels. Since this stress can be maintained at non-harmful levels, our study supports the new European Judicial Policy, which advocates for the establishment and operation of Specialized Courts adapted to the needs of children and adolescents, these courts ensure a child-friendly environment and language that contribute to reducing the stress of minor victims of violence.
These findings may have implications for understanding the experiences of individuals involved in a judicial context, preventing SV, and designing best practices in child-centered judicial care. Given that satisfaction with the outcome is a powerful predictor of SV (Orth, 2002) and that good judicial sentences require thorough investigations, which, in turn, depend on the active participation of victims, judicial procedures should not base their protection mechanisms on systematically reducing the child’s participation in the procedure. Instead, the focus should be on providing procedural justice and adapting the environment and language to the needs of children, making the procedure more child-friendly. The present research supports the theory that participation in judicial processes is not inherently traumatic for minors.
Data availability
The datasets generated and analyzed during the current study are not publicly available because individual privacy could be compromised, but they are available from the corresponding author upon reasonable request. Images of the smart bands used to evaluate stress, along with the various contexts assessed, are available in the FIGSHARE repository at [https://doi.org/10.6084/m9.figshare.24310486.v2].
References
Acharya UR, Joseph KP, Kannathal N, Lim CM, Suri JS (2006) Heart rate variability: a review. Med. Biol. Eng. Comput. 44(12):1031–1051. https://doi.org/10.1007/s11517-006-0119-0
Appelhans BM, Luecken LJ (2006) Heart rate variability as an index of regulated emotional responding. Rev. Gen. Psychol. 10(3):229–240
Arantegui A (2022) El uso de cámaras Gesell con niños: derechos humanos y victimización secundaria [The use of Gesell cameras with children: human rights and secondary victimization]. Rev. de. Victimología 13:35–64. https://doi.org/10.12827/RVJV.13.02
Arnau J, Bono R (2008) Estudios longitudinales. Modelos de diseño y análisis [Longitudinal studies. Design and analysis models]. Escr. de. Psicol.ía - Psychol. Writ. 2(1):32–41. https://doi.org/10.24310/espsiescpsi.v2i1.13356
Buela-Casal, G, Guillén-Riquelme, A, & Seisdedos Cubero, N (2015) Cuestionario de ansiedad estado-rasgo: Adaptación española (9ª ed.). TEA Ediciones
Carretta F, García-Quiroga M 2021Justicia de familia y victimización secundaria: un estudio aplicado con niños, jueces y abogados. Derecho Pucp 87:471–497. https://doi.org/10.18800/derechopucp.202102.014
Castaldo R, Melillo P, Bracale U, Caserta M, Triassi M, Pecchia L (2015) Acute mental stress assessment via short term HRV analysis in healthy adults: A systematic review with meta-analysis. Biomed. Signal Process. Control 18:370–377. https://doi.org/10.1016/j.bspc.2015.02.012
Chalmers T, Hickey BA, Newton P, Lin C-T, Sibbritt D, McLachlan CS, Clifton-Bligh R, Morley J, Lal S (2022) Stress watch: The use of heart rate and heart rate variability to detect stress: a pilot study using smart watch wearables. Sensors 22:151. https://doi.org/10.3390/s22010151
Chelidoni O, Plans D, Ponzo S, Morelli D, Cropley M (2020) Exploring the effects of a brief biofeedback breathing session delivered through the BioBase app in facilitating employee stress recovery: Randomized experimental study. JMIR mHealth uHealth 8(10):e19412. https://doi.org/10.2196/19412
Cohen, JA, Mannarino, AP, and Deblinger, E (2006) Treating trauma and traumatic grief in children and adolescents. Guilford Press
Council of Europe. Committee of Ministers. (2011) Guidelines of the Committee of Ministers of the Council of Europe on child-friendly justice (Vol. 5). Council of Europe
Crenshaw DA, Stella L, O’Neill-Stephens E, Walsen C (2019) Developmentally and trauma-sensitive courtrooms. J. Humanist. Psychol. 59(6):779–795. https://doi.org/10.1177/0022167816641854
Daignault IV, Hébert M, Pelletier M (2017) L’influence du système de justice sur le rétablissement d’enfants victimes d’agression sexuelle et suivis dans un centre d’appui aux enfants [The influence of the justice system on the recovery of children victims of sexual assault and followed in a child support center]. Criminologie (Spec. Ed.) 50(1):51–73. https://www.jstor.org/stable/44656803
Deschodt-Arsac V, Lalanne R, Spiluttini B, Bertin C, Arsac LM (2018) Effects of heart rate variability biofeedback training in athletes exposed to stress of university examinations. PLoS ONE 13(7):1–13. https://doi.org/10.1371/journal.pone.0201388
Ding X, Wei S, Gui X, Gu N, Zhang P(2021) Data engagement reconsidered: a study of automatic stress tracking technology in use. In Proceedings of the 2021 CHI conference on human factors in computing systems. CHI '21: CHI Conference on Human Factors Comput Syst 535:1–13. https://doi.org/10.1145/3411764.3445763
Doan TN (2023) A novel low-cost system for remote health monitoring using smartwatches. Indian J. Comput. Sci. Eng. 14(3):429–443. https://doi.org/10.21817/indjcse/2023/v14i3/231403068
Duan H, Yuan Y, Zhang L, Qin S, Zhang K, Buchanan TW, Wu J (2013) Chronic stress exposure decreases the cortisol awakening response in healthy young men. Stress 16(6):630–637. https://doi.org/10.3109/10253890.2013.840579
Eastwood C (2003) The experiences of child complainants of sexual abuse in the criminal justice system. (cover story). Trends Issues Crime. Crim. Justice 250:1–6. https://search.ebscohost.com/login.aspx?direct=true&db=edo&AN=57276461&site=eds-live
Endler NS, Kocovski NL (2001) State and trait anxiety revisited. J. anxiety Disord. 15(3):231–245. https://doi.org/10.1016/s0887-6185(01)00060-3
Ernst G (2017) Heart-rate variability-more than heart beats? Front. Public Health 5:240. https://doi.org/10.3389/fpubh.2017.00240
European Union Agency for Fundamental Rights. (2017) Child-friendly justice: Perspectives and experiences of children involved in judicial proceedings as victims, witnesses or parties in nine EU member states. Publication Office of the European Union
Fan YY, Li YG, Li J, Cheng WK, Shan ZL, Wang YT, Guo YT (2019) Diagnostic performance of a smart device with photoplethysmography technology for atrial fibrillation detection: pilot study (Pre-mAFA II registry). JMIR mHealth uHealth 7(3):e11437. https://doi.org/10.2196/11437
Faul F, Erdfelder E, Lang AG, Buchner A (2007) G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39(2):175–191
García MJ (2022) Ventajas de la nueva regulación de la prueba preconstituida para la declaración de las víctimas menores de edad y con discapacidad necesitadas de especial protección en el proceso penal. Bolet. del. Minist. de. Justicia 76(2258):3–75
Georgiou K, Larentzakis AV, Khamis NN, Alsuhaibani GI, Alaska YA, Giallafos EJ (2018) Can wearable devices accurately measure heart rate variability? A systematic review. Folia Med. 60(1):7–20. https://doi.org/10.2478/folmed-2018-0012
Goessl VC, Curtiss JE, Hofmann SG (2017) The effect of heart rate variability biofeedback training on stress and anxiety: a meta-analysis. Psychol. Med. 47(15):2578–2586. https://doi.org/10.1017/S0033291717001003
Goodman GS, Taub EP, Jones DP, England P, Port LK, Rudy L, Prado L (1992) Testifying in criminal court: emotional effects on child sexual assault victims. Monogr. Soc. Res. Child Dev. 57(5):1–161
Goodman G, Tobey A, Batterman-Faunce J, Orcutt H, Thomas S, Shapiro C, Sachsenmaier T (1998) Face-to-face confrontation: Effects of closed-circuit technology on children’s eyewitness testimony and jurors’ decisions. Law Hum. Behav. (Springe. Sci. Bus. Media B. V.) 22(2):165–203. https://doi.org/10.1023/A:1025742119977
Guo, Y, Wang, H, Zhang, H, Chen, Y, & Lip, GYH (2020) Population-based screening or targeted screening based on initial clinical risk assessment for atrial fibrillation: A report from the Huawei heart study. J. Clin. Med. 9(5). https://doi.org/10.3390/jcm9051493
Harrison SL, Buckley BJR, Zheng Y, Hill A, Hlaing T, Davies R, Guo Y, Lane DA, Lip GY, Choi SE, Elsheikh S, Sagris D, Joddrell M, Alobaida M, McCarthy E, McCarthy E, Eustace I, Eustace I, Hoad K, Jones IS (2023) Evaluation of Huawei smart wearables for detection of atrial fibrillation in patients following ischemic stroke: The Liverpool-Huawei stroke study. Am. Heart J. 257:103–110. https://doi.org/10.1016/j.ahj.2022.12.004
Hayes D, Bunting L (2013) Just be brave’ - The Experiences of young witnesses in criminal proceedings in Northern Ireland. Child Abus. Rev. 22(6):419–431. https://doi.org/10.1002/CAR.2242
Hernando D, Roca S, Sancho J, Alesanco Á, Bailón R (2018) Validation of the Apple watch for heart rate variability measurements during relax and mental stress in healthy subjects. Sens. (Basel, Switz.) 18(8):2619. https://doi.org/10.3390/s18082619
Hong S, Yang Y, Lee J, Yang H, Park K, Lee S, Lee I, Jang Y (2010) Ambulatory stress monitoring with a wearable bluetooth electrocardiographic device. Stud. health Technol. Inform. 161:66–76
Hopkins WG (2020) Sample-size estimation for various inferential methods. Sportscience 24:1–13
Hossein S, Cooper JA, DeVries BAM, Nuutinen MR, Hahn EC, Kragel PA, Treadway MT (2023) Effects of acute stress and depression on functional connectivity between prefrontal cortex and the amygdala. Mol. Psychiatry 28:4602–4612. https://doi.org/10.1038/s41380-023-02056-5
Huawei Technologies Co., Ltd. (2022) Huawei Health (Version 12.1.7.300). [Mobile app]. URL: https://consumer.huawei.com/es/mobileservices/health/
Immanuel, S, Teferra, MN, Baumert, M, & Bidargaddi, N (2023) Heart rate variability for evaluating psychological stress changes in healthy adults: A scoping review. Neuropsychobiology, 1–16. https://doi.org/10.1159/000530376
Jarchi, D, Salvi, D, Velardo, C, Mahdi, A, Tarassenko, L, & Clifton, DA (2018) Estimation of HRV and SpO2 from wrist-worn commercial sensors for clinical settings. 2018 IEEE. 15th International Conference on Wearable and Implantable Body Sensor Networks, BSN, 144–147. https://doi.org/10.1109/BSN.2018.8329679
Kim S-Y, Seo H-W, Kim J-W, Chung S-Y 2011[Relationship between Heart Rate Variability (HRV) and BDI, STAI and STAXI] J. Orient. Neuropsychiatry 22(4):87–100. https://doi.org/10.7231/JON.2011.22.4.087
Lehrer PM, Gevirtz RE (2014) Heart rate variability biofeedback: How and why does it work? Front. Psychol. 5:756. https://doi.org/10.3389/fpsyg.2014.00756
Li F, Xu P, Zheng S, Chen, W Yan, Y, Lu, S & Liu, Z (2018) Photoplethysmography based psychological stress detection with pulse rate variability feature differences and elastic net. Int. J. Distributed Sensor Networks. 14(9). https://doi.org/10.1177/1550147718803298
Martínez GJ, Grover T, Mattingly SM, Mark G, D MS, Aledavood T, Akbar F, Robles-Granda P, Striegel A (2022) Alignment between heart rate variability from fitness trackers and perceived stress: Perspectives from a large-scale in situ longitudinal study of information workers. JMIR Hum. Factors 9(3):411–431. https://doi.org/10.2196/33754
Nathanson R, Saywitz KJ (2003) The effects of the courtroom context on children’s memory and anxiety. J. Psychiatry Law 31(1):67–98. https://doi.org/10.1177/009318530303100105
Nathanson R, Saywitz KJ (2015) Preparing children for court: Effects of a model court education program on children’s anticipatory anxiety. Behav. Sci. Law 33(4):459–475. https://doi.org/10.1002/bsl.2191
Nolan RP, Kamath MV, Floras JS, Stanley J, Pang C, Picton P, Young QR (2005) Heart rate variability biofeedback as a behavioral neurocardiac intervention to enhance vagal heart rate control. Am. Heart J. 149(6):1137. https://doi.org/10.1016/j.ahj.2005.03.015
Ohsuga M, Shimono F, Genno H (2001) Assessment of phasic work stress using autonomic indices. Int. J. Psychophysiol. 40(3):211–220. https://doi.org/10.1016/S0167-8760(00)00189-6
Orth U (2002) Secondary victimization of crime victims by criminal proceedings. Soc. Justice Res. 15(4):313–325. https://doi.org/10.1023/A:1021210323461
Park, G, & Thayer, JF (2014) From the heart to the mind: Cardiac vagal tone modulates top-down and bottom-up visual perception and attention to emotional stimuli. Front. Psychol. 5. https://doi.org/10.3389/fpsyg.2014.00278
Peterson L, Rolls Reutz JA, Hazen AL, Habib A, Williams R (2020) Kids and teens in court (KTIC): A model for preparing child witnesses for court. Am. J. Community Psychol. 65(1–2):35–43. https://doi.org/10.1002/ajcp.12390
Peña, JUL (2021, 13 mayo) Detección de la frecuencia cardiaca por técnicas de balistocardiografía y visión computacional. http://revistaaristas.tij.uabc.mx/index.php/revista_aristas/article/view/103
Plarre, K, Scott, M, Siewiorek, D, Smailagic, A, Wittmers, LE, Raij, A, Hossain, SM, Ali, AA, Nakajima, M, Al’absi, M, Ertin, E, Kamarck, T, & Kumar, S (2011) Continuous inference of psychological stress from sensory measurements collected in the natural environment. Proceedings of the 10th ACM/IEEE International Conference on Information Processing in Sensor Networks, Information Processing in Sensor Networks (IPSN), 2011 10th International Conference On, 97–108
Poder Judicial. (2021, 28 de septiembre) Abre en Canarias el primer juzgado de violencia contra la infancia de España [Press release]. Poder Judicial. https://www.poderjudicial.es/cgpj/es/Poder-Judicial/Tribunales-Superiores-de-Justicia/TSJ-Canarias/Oficina-de-Comunicacion/Archivo-de-notas-de-prensa/Abre-en-Canarias-el-primer-Juzgado-de-Violencia-contra-la-Infancia-de-Espana-
Prinsloo GE, Derman WE, Lambert MI, Laurie Rauch HG (2013) The effect of a single episode of short duration heart rate variability biofeedback on measures of anxiety and relaxation states. Int. J. Stress Manag. 20(4):391–411. https://doi.org/10.1037/a0034777
Pulopulos MM, Hidalgo V, Puig-Pérez S, Salvador A (2018) Psychophysiological response to social stressors: Relevance of sex and age. Psicothema 30(2):171–176. https://doi.org/10.7334/psicothema2017.200
Quas JA, Goodman GS, Ghetti S, Alexander KW, Edelstein R, Redlich AD, Cordon IM, Jones DP (2005) Childhood sexual assault victims: Long-term outcomes after testifying in criminal court. Monogr. Soc. Res. Child Dev. 70(2):vii–128. https://doi.org/10.1111/j.1540-5834.2005.00336.x
Randell I, Seymour F, McCann C, Blackwell S (2022) The experiences of young witnesses and caregivers in Aotearoa New Zealand’s Sexual Violence Pilot Courts. Psychiatry, Psychol. Law 29(1):134–153. https://doi.org/10.1080/13218719.2021.1904449
Rodrigues S, Paiva JS, Dias D, Aleixo M, Filipe RM, Cunha JPS (2018) Cognitive impact and psychophysiological effects of stress using a biomonitoring platform. Int. J. Environ. Res. Public Health 15(6):1080. https://doi.org/10.3390/ijerph15061080
Rodriguez-Pellejero, JM, Mulero, I, & Santana Amador, Z (2023) Interior design of the courthouse rooms [Photograph]. Figshare. https://doi.org/10.6084/m9.figshare.24310486
Saywitz KJ, Nathanson R (1993) Children’s testimony and their perceptions of stress in and out of the courtroom. Child Abus. Negl. 17(5):613–622. https://doi.org/10.1016/0145-2134(93)90083-H
Shaffer F, McCraty R, Zerr CL (2014) A healthy heart is not a metronome: an integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 5:1040. https://doi.org/10.3389/fpsyg.2014.01040
Sherlin L, Gevirtz R, Wyckoff S, Muench F (2009) Effects of respiratory sinus arrhythmia biofeedback versus passive biofeedback control. Int. J. Stress Manag. 16(3):233–248. https://doi.org/10.1037/a0016047
Sotoca A, Muñoz JM, González JL, Manzanero AL (2013) La prueba preconstituida en casos de abuso sexual infantil: aportaciones desde la psicología jurídica. La Ley Penal 102:112–122
Spielberger, CD (1989) State-Trait Anxiety Inventory: Bibliography (2nd ed.). Palo Alto, CA: Consulting Psychologists Press
Spielberger, CD (2001) STAIC: cuestionario de autoevaluación, ansiedad estado / rasgo en niños. TEA Ediciones
Szu HH, Dai L, Kaur B, Durek JJ, O’Kane BL, Tran N, Moses S, Luthra M, Ikonomidou VN (2014) Heart rate variability (HRV): an indicator of stress. Proc. SPIE 9118(1):91180V–91180V–8. https://doi.org/10.1117/12.2051148
Taelman, J, Vandeput, S, Spaepen, A, & Van Huffel, S (2009) Influence of mental stress on heart rate and heart rate variability (Vol. 22). Springer Berlin Heidelberg. https://doi.org/10.1007/978-3-540-89208-3_324
Velmovitsky PE, Lotto M, Alencar P, Leatherdale ST, Cowan D, Morita PP (2023) Can heart rate variability data from the Apple Watch electrocardiogram quantify stress? Front. Public Health 11:1178491. https://doi.org/10.3389/fpubh.2023.1178491
Zhang S, Ahn C (2011) How many measurements for time-averaged differences in repeated measurement studies? Contemp. Clin. trials 32(3):412–417. https://doi.org/10.1016/j.cct.2011.01.002
Zhang X, Li P, Chen J, Li H (2020) Acute stress impairs reward positivity effect in probabilistic learning. Psychophysiology 57(4):e13531. https://doi.org/10.1111/psyp.13531
Zimmerman D, Zumbo B (2005) Can percentiles replace raw scores in the statistical analysis of test data? Educ. Psychol. Meas. 65(4):616–638. https://doi.org/10.1177/0013164404272499
Acknowledgements
The researchers would like to express their gratitude to His Honour Tomás Martín Rodríguez, Magistrate of the 3rd Investigative Court of Las Palmas de Gran Canaria and director of the Project for the creation of the First Court of Violence Adapted to Children and Adolescents. We appreciate his valuable contribution to promoting a more equitable justice system for children, grounded in scientific evidence. The study is funded by the MAPFRE Canarias Foundation. Project identification number 2022/1006.
Author information
Authors and Affiliations
Contributions
These authors contributed equally to this work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study did not include medical research or human experimentation. The procedures used in this study adhere to the tents of the declaration of Helsinki. This study was approved by a Research Ethics Committee of the University of Las Palmas de Gran Canaria and by the examining magistrate of the Pilot Court for violence against children.
Informed consent
Written informed consent was obtained from the parents or legal guardians of the minors for their participation in the study and the publication of the results. Additionally, explicit and verbal assent was obtained from the minors in the presence of their legal guardians.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rodríguez-Pellejero, J.M., Mulero-Henríquez, I. & Santana Amador, Z. Real-time stress monitoring in a child-friendly court: a repeated measures field study. Humanit Soc Sci Commun 11, 913 (2024). https://doi.org/10.1057/s41599-024-03410-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-024-03410-w
