
Abstract
Previous research has established a link between poverty and adverse health outcomes. In particular, poor health status in the middle-aged and elderly is often irreversible and can make it extremely difficult to escape poverty. Identifying poverty from multiple dimensions and assessing its relationship to health is crucial for active ageing. In this study, we sought to investigate the link between multidimensional poverty, income poverty, and health status using data from the China Health and Retirement Longitudinal Study (CHARLS). Employing panel fixed-effect logistic regression and instrumental variables estimation, we analyzed the impact of multidimensional poverty and income poverty on health status including subjective health, mental health, and physical health. The multidimensional poverty of middle-aged and older adults was classified into three groups: poverty group (n = 3272, 18.04%), precarity group (n = 8234, 36.07%), and prosperity group (n = 11,319, 49.59%). The results of regression analysis indicate that multidimensional poverty is significantly positively correlated with poor self-rated health, poor physical health and mental health, while income poverty is significantly negatively correlated with poor self-rated health, poor physical health and mental health. Moreover, we found that the impact of multidimensional poverty on health is attributed to the reduced healthcare utilization, and compromised health behaviors. This underscores the importance of considering not only income poverty but also multidimensional poverty when examining its association with health status. For promoting healthy aging, it is imperative to comprehensively assess, alert, and address the issue of middle-aged and elderly poverty from a multidimensional perspective.
Similar content being viewed by others

Introduction
Poverty serves as a significant social determinant of health, leading to disparities in health outcomes (Gitterman et al.,). Natural experiments have verified the causal links between poverty and health across both high-income countries, such as the United States, Belarus, Georgia, and low-income countries like Uzbekistan and Mongolia (Thomson et al., 2023; Zhang and Zhao, 2021; Habibov et al., 2019). Poverty causes ill-health as the poor suffer from a multitude of health-compromising negative shocks (Wagstaff, 2002), stemming from risker living conditions, undernutrition, psychological stress, and lack of access to preventive healthcare (Tekguc and Akbulut, 2022; Pinilla-Roncancio et al., 2020; Ridley et al., 2020). Specifically, the poor often reside in unsanitary and hazardous environment lacking clean drinking water, satisfactory sanitation, and unsafe or inadequate housing, all of which pose significant risks to their health (Díaz et al., 2022; Trani et al., 2023). Furthermore, the absence of a stable income source among those living in poverty frequently leads to heightened psychological stress and anxiety levels that can precipitate or exacerbate mental health problems, such as depression and anxiety disorders (Ridley et al., 2020; Zimmerman et al., 2022). In addition, people living in poverty often rely on low-quality healthcare or underutilize healthcare services, which can potentially expedite the health-risk output and worsen their overall well-being (Luo et al., 2020). Consequently, eradicating poverty in all its forms has emerged as a primary goal within the Sustainable Development Goals (SDGs) framework (Nations, 2015). However, studies on the relationship of poverty and health are not consistent across countries. For instance, higher levels of multidimensional poverty are associated with increased prevalence of depressive symptoms in Colombia and Mexico, whereas no significant association was observed in South Africa (Zimmerman et al., 2022).
Compared to other age groups, middle-aged and elderly demographics facing health and economic vulnerabilities constitute a substantial portion of the impoverished population in both high-income and low- to middle-income countries (LMICs) (Barrientos et al., 2003; Ebbinghaus, 2021). In 2021, old-age poverty rates in South Korea and the United States were 39.3% and 23.2%, respectively, exceeding the population-wide poverty rates of 15.1% and 18.0% (OECD, 2023). The relationship between socio-economic status and health among middle-aged and elderly exhibits distinct differences in material, psychosocial, and behavioral dimensions compared to other age groups (Domènech-Abella et al., 2018; Aue et al., 2016; Dalecka et al., 2024). First, given their relatively more fragile health status, the elderly may encounter greater challenges compared to other population groups who are unable to access medical care due to financial limitations (Kim et al., 2022). Second, given their substantial uncertainty and income volatility, sustained long-run exposure to psychosocial stress may threaten mental health either through biological or behavioral pathways (Yang et al., 2025; Steptoe et al., 2015; Staufenbiel et al., 2013). Third, risk-taking health behavior, such as unhealthy dietary behavior, smoking, or physical inactivity, can further exacerbate the health disparities observed among impoverished elderly populations (Contoyannis and Jones, 2004; Mullan et al., 2021). China is no exception, with a mid-aged and older adults poverty incidence of 13.2% in 2018 (Wang et al., 2023). Country-specific research on poverty and health, whether using China Health and Retirement Longitudinal Study (CHARLS) or household income and expenditure survey in Korea have shown that elderly individuals, as one of the most vulnerable and disadvantaged groups, are more likely to fall into poverty due to physiological degradation, reduced ability to adapt, and weakened family support function (Jin et al., 2020; Wang et al., 2023; Ku and Kim, 2020). However, poverty among the middle-aged and elderly has not received adequate attention.
The link between poverty—both multidimensional and income-based—and health has been extensively explored in existing research (Ridley et al., 2020; Oshio and Kan, 2014; Meisters et al., 2023; Reumers et al., 2022). However, the causal relationship linking poverty and health was controversial. The social determinants of health framework posit that poverty influences health outcomes through various pathways, including access to healthcare, nutrition, and living conditions (Fu et al., 2024). Contrarily, some studies suggest that poor health can, in turn, lead to poverty, creating a vicious cycle that complicates interventions (Zhou et al., 2023). This bidirectional relationship poses a challenge for establishing causal links between poverty and health. Accordingly, Fu et al. utilized China Family Panel Studies panel data with adults and applied conditional regression to validate the bidirectional cumulative cycle between health and poverty (Fu et al., 2024). Moreover, Habibov et al. analyzed cross-sectional data of individuals aged 18–65 years, employing instrumental variables to demonstrate the direct causal effects of poverty on health (Habibov et al., 2019). Accordingly, it is of interest to use nationally longitudinal data (five-wave balanced panel data) to examine whether multidimensional poverty has consistent causal effects on mid-aged and older adults’ health status.
Additionally, as poverty research deepens, multidimensional poverty may have a more pronounced impact on health than income poverty alone, suggesting that interventions addressing multiple facets of poverty could yield better health outcomes (Alkire and Santos, 2013). While some advocate for multidimensional indices that capture the complexity of deprivation (Alkire et al., 2021), others argue that income remains a more straightforward and quantifiable indicator of poverty, suggesting that variations in health can often be attributed to income disparities (Wang, 2022). To better capture the basic needs deprivation beyond the scope of income measurement, non-monetary approaches (Zimmerman et al., 2022; Angulo et al., 2016) such as the combined poverty index by Groh-Samberg, and the health-inclusive poverty measure used in the US have been proposed (Korenman et al., 2021; Aue et al., 2016). The dimensions of education and employment, which are typically included in these approaches, are not suitable for older individuals. According to the global experience of poverty alleviation, middle-aged and older adults constitute a primary demographic focus due to their heightened vulnerability to medical impoverishment compared to the general population (OECD, 2023). However, specific measures for middle-aged and elderly poverty are lacking.
Therefore, this study aims to construct a mixed evaluation system encompassing life domains, focusing on middle-aged and elderly individuals at risk of fundamental needs deprivation. The system integrates monetary and non-monetary poverty identification using a hybrid approach. Thus, this may provide valuable insights for addressing middle-aged and elderly poverty in nations experiencing rapid population ageing. This study utilizes panel fixed-effect logistic regression with data obtained from the CHARLS to investigate the effects of multidimensional poverty on the health status among middle-aged and elderly. In addition, the study further compares the differences in health impacts between multidimensional poverty and income poverty.
The remaining parts are organized as follows. Part “Background” presents the mechanisms and the definition. Part “Methods” describes the data sources and study design. Part “Results” shows the primary findings and potential influencing mechanisms. Part “Discussion” is the detail discussions. Conclusion including implications and limitations is in the final.
Background
Mechanisms for poverty-causing ill-health
The concept of health goes beyond just physical well-being; it encompasses a holistic state of well-being that needs to be measured with comprehensive indicators (Kühn and Rieger, 2017). A persisting debate within the field centers on disentangling the complex pathways through which poverty exerts differential impacts across these dimensions (Hirokazu et al., 2012; Zimmerman et al., 2022). While substantial research explores the health-poverty nexus, empirical findings remain inconsistent, particularly regarding the mediating mechanisms involved, and contain both significant and non-significant results (Hasan and Ghosal, 2024; Pfoertner and Demirer, 2022; Xiao et al., 2022). Figure 1 depicts the relationship between poverty and three dimensions of health status, drawing on the health inequality framework proposed by Mackenbach (Mackenbach, 2006).

Source: modified according to Mackenbach (2006). Figure 1 depicts the relationship between poverty and health status, drawing on the health inequality framework proposed by Mackenbach.
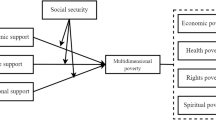
In this framework, health is determined by psychosocial factors, material factors, and health behaviors. Poverty, as a significant component of material factors, manifesting in inadequate nutrition and poor living environments—directly influence health status as well as via psychosocial factors and health behaviors (Garman et al., 2022). The psychosocial aspect, such as limited access to healthcare and stress, can directly impact health status both independently and through health behaviors (Wang and Ye, 2024). Stress exerts an influence on mental well-being through life satisfaction and social participation (Padmanabhanunni et al., 2023), whereas healthcare access directly impacts self-rated and physical health, and indirectly affects mental health through self-rated or physical health pathways. Individuals residing in lower-income households are less likely to use healthcare when they are sick compared to those from higher-income households. They often have limited access to more advanced, up-to-date, and specialized health procedures and services, which worsens their health (Habibov et al., 2019). The health behaviors serve as mediators linking poverty to diverse health outcomes, encompassing physical, mental, and self-rated health. Health-promoting behaviors, such as physical activity, adequate nutrition, timely medical treatment and stress management, directly impact older adults’ physical health (Shinyoung, 2009).
Income poverty vs. multidimensional poverty
Poverty in the traditional sense mainly refers to income poverty, which means that an individual or household’s consumption or expenditure falls below a specified benchmark (Alkire and Fang, 2019). The World Bank standardized the international poverty line at 1.90 dollars per day per person in 2015 (Bank, 2020). Additionally, in 2018, the World Bank introduced a supplementary poverty line of 3.20 dollars per day for LMICs, augmenting the initial 1.90 dollar threshold. Specifically, the European Union defines relative poverty as 60% of the median disposable income per capita (Van Vliet and Wang, 2015). In the United States, the poverty standard is determined by factors such as household size, composition of household members, and the age of the head of household (Zhang and Shen, 2020).
Evaluating poverty based solely on income is not comprehensive, as it fails to consider other dimensions that reflect the state of poverty, including health, education, and living conditions (Liu et al., 2023). Echoing the United Nations’ definition, multidimensional poverty encompasses more than just insufficient income for a sustainable life; its manifestations include hunger and malnutrition, limited access to education and other basic services, as well as social discrimination (United Nations, 2016). In addition to income poverty, the four deprivation dimensions considered are housing, consumption, financial reserves and unemployment in Groh-Samberg’s dimensions of deprivation. Similarly, the goal of poverty alleviation in China is set at “two non-worries and three guarantees”, i.e., no worries about food and clothing, and guarantees for compulsory education, basic medical care, and housing security (Liu et al., 2023). However, the aforementioned multidimensional identification criteria exhibit limited applicability to older adults, primarily due to their constrained employment opportunities and the structural barriers in altering educational attainment.
Methods
Study participants
We used data from the CHARLS to examine the relationship between income poverty, multidimensional poverty and health status. The CHARLS is an ongoing panel survey of households and individuals conducted since 2011, and is representative of people aged 45 years and above in China. CHARLS national baseline survey was conducted in 2011, covering 150 county-level units, 450 village-level units, and 17,000 individuals in about 10,000 households (Zhao et al., 2014). We used CHARLS five-wave data, 2011, 2013, 2015, 2018 and 2020, and included a total of 96,221 observations. The panel data design is balanced to observe individuals’ health status and poverty dynamics. We employed logical interpolation for missing data in the panel and utilize information from two adjacent periods to fill in the gaps. Among these variables, 29,429 missing values were interpolated for income poverty, 21,310 missing values for health insurance, 6473 missing values for pension, and 208 missing values for housing structure. Subsequently, we removed 19,727 observations with missing self-rated health, 74 observations with missing physical health, and 3239 observations with missing mental health. Finally, we obtained 4565 samples of the balanced panel, encompassing a total of 22,825 observations. Figure 2 illustrates the sample screening process.

Figure 2 illustrates the sample screening process.
Measures
Health status
In this study, we utilized subjective health, physical health, and mental health as measures of individuals’ health status. Subjective health was measured through a self-rated health question: “How would you rate your health as very good, good, fair, poor or very poor?” Self-rated health was categorized into two categories: positive (very good or good or fair) and negative (poor or very poor) (Honjo et al., 2006). The physical health measure used was the activities of daily living (ADL) scale, which consists of six items, including dressing, bathing, or showering, self-feeding, getting into/out of bed, using the toilet, and controlling urination and defecation. Responses were categorized into four levels, with “no difficulty” representing the first level and “cannot do it” representing the fourth level. Participants who reported having no difficulty were classified as having no difficulty, while the rest were classified as having difficulty (Evandrou et al., 2014). The mental health measure used was the 10-item Center for Epidemiologic Studies Depression Scale (CESD-10), which assesses how participants felt and behaved over the past week. The CESD-10 comprises eight negative and two positive questions, and a score of 10 or higher indicates depressive symptoms (Andresen et al., 1994).
Income poverty and multidimensional poverty
In the post-poverty era, poverty reduction in China has shifted its focus from eliminating absolute poverty to alleviating relative poverty (Chong et al., 2022). Therefore, this study determined income poverty based on the extreme poverty threshold and the poverty threshold for middle-income countries proposed by the World Bank, using a measure of poverty at 1.90 dollars a day and 3.20 dollars a day, respectively, to calculate the poverty incidence (Bank, 2020). The income poverty converted based on purchasing power parity (PPP) is shown in the Appendix.
Since many researchers have proposed to supplement the measurement of income poverty with direct measurements of life domains (Benzeval and Judge, 2001; Nolan and Whelan, 2007), this study focuses on an existing multidimensional measurement that considers not only income but also additional aspects of deprivation (Aue et al., 2016). Given that middle-aged and older adults generally do not contend with educational insecurity and combined with the questionnaire used in CHARLS, this study narrows the dimensions of multidimensional poverty to include housing, health insurance, and pensions, referring to Groh-Samberg’s dimensions of deprivation and China’s goal of “two non-worries, three guarantees”. We replaced the Groh-Samberg consumption indicator with health insurance because older people have a higher likelihood of incurring catastrophic health expenditures owing to chronic or high-cost illnesses (Zhai et al., 2021). Subsequently, we substituted Groh-Samberg’s unemployment indicator with the pension, considering that employment opportunities are limited for older individuals. Pensions offer financial security for older adults, enabling them to feel assured and free from financial concerns (Shuo, 2023). The fundamental principle of this approach entails assessing poverty levels among these demographic populations by comprehensively comparing their income with the extent of deprivation across the three life domains.
Housing deprivation was defined as “Individuals whose housing structures are neither concrete and steel nor bricks and wood may lack housing security”. Pension deprivation was defined as individuals not receiving, not expected to receive, or not contributing to any of the following pension insurance schemes (such as urban and rural resident pension, new rural resident pension and urban resident pension). Health insurance deprivation was measured as following question: “Are you the policy holder/primary beneficiary of any of the types of health insurance listed below? (such as urban employee medical insurance, urban and rural resident medical insurance, government medical insurance). Assign a value of 1 if the answer is “no insurance”, 0 otherwise.
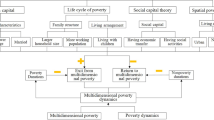
According to Groh-Samberg (Groh-Samberg, 2008), combining income poverty with multiple deprivations results in nine distinct combinations. Table 1 presents the six groups, namely extreme, moderate, and one-sided poverty, as well as vulnerability, fragile prosperity, and secure prosperity. To derive a combined poverty deprivation indicator, multiple deprivations can be observed if the sum of deprivations is greater than 2 each year, a single deprivation exists if the sum of deprivations is 1 each year, and no deprivation if the sum of four deprivations is equal to 0.
Referring to Aue et al.’s research, extreme poverty, moderate poverty, and one-sided poverty are defined as the poverty group, vulnerability, fragile prosperity is defined as the precarity group and secure prosperity is defined as the prosperity group (Aue et al., 2016). The prosperity group is characterized by individuals who have access to housing, receive pensions, possess health insurance, and expend more than 3.20 on consumption. The precarity group implies that there is either income poverty or multidimensional poverty, but that the extent of poverty is not as severe as that of the poverty group. It is a state of precarious income poverty or multidimensional poverty, and individuals in this group face the risk of falling into the poverty group if the dimensions of deprivation, such as multidimensional poverty or income poverty, increase. The poverty group comprises individuals who experience deprivation below the 1.9-dollar poverty threshold. However, even if the poverty threshold of 3.2 dollars is exceeded, individuals can still be classified within the poverty group if they face deprivation in three dimensions. Overall, the poverty group is in the most disadvantaged position, as it encompasses individuals who experience deprivation in multiple dimensions.
Multivariate analyses
Data spanning five periods were consolidated into a balanced panel, and a Hausman test was conducted to decide between employing a fixed-effects model or a random-effects model (Baltagi et al., 2003). Given that the Hausman test indicated a p-value of less than 0.01, a fixed-effect model was chosen for the panel analysis. Detailed results of the Hausman test can be found in Table 5. Subsequently, panel fixed-effect logistic regression models were utilized to examine self-rated health, physical health, and mental health in the final year for \({{individual}}_{i}\) as dependent binary variables (\({Y}_{i}\in \left\{\mathrm{0,1}\right\}\)), using income poverty and multidimensional poverty as the explanatory variables. For result interpretation, odds ratios (OR) along with 95% confidence intervals (CI) were employed. Additionally, the self-rated health model was adjusted for variables such as age, marital status, smoking, alcohol consumption, social participation, life satisfaction, physical activity, and chronic disease status. Within the ADL model, age, marital status, smoking, alcohol consumption, social participation, life satisfaction, physical activity, and chronic diseases status were incorporated as control variables; conversely, in the depression model, both pain status and sleep status were added as control variables.
Endogeneity analysis
Considering the endogeneity arising from the potential bidirectional causal relationship between poverty and health, we employed an instrumental variables (IVs) approach to further investigate underlying causal effects. The existing literature has established the validity of community (village) level indicators as IVs (Zimin and Mingyan, 2020; Hou et al., 2022). Consequently, this study selected the community-level averages of multidimensional poverty and income poverty as IVs. Additionally, given the limitation that the panel IVs with fixed-effects method necessitate estimation through the two-stage least squares (2SLS) linear regression approach, we follow the methodology outlined by Pan et al. and convert income poverty and multidimensional poverty into multiple binary variables for 2SLS estimation (Pan et al., 2016). In addition, due to the small number of observations for each wave, such as extreme, moderate and single poverty, we further consolidate the six classifications of poverty into three classifications of poverty.
Mechanism analysis
Drawing on Mackenbach et al.’s health inequity framework (Mackenbach, 2006), we employed panel fixed-effects regression analyses to investigate the relationships between multidimensional poverty and depressed, life satisfaction, social participation, health check-ups, cooking fuels and risk-taking health behaviors like smoking, alcohol consumption and physical inactivity, respectively. The objective was to elucidate the potential mechanisms through which multidimensional poverty influences the health status of middle-aged and older adults.
Results
Descriptive statistics
Health status
Table 2 presents the distribution of health status for the total sample in 2011–2020, including sample size and percentage. The data reveals a decline followed by an increase in self-rated ill-health and mental ill-health, while physical ill-health has been on the rise. The percentage of individuals reporting poor self-rated health increased from 26.11% in 2011 to 28.21% in 2020, while poor physical health increased from 13.01% in 2011 to 25.17% in 2020. Poor mental health increased from 36.06% in 2011 to 42.65% in 2020.
Income poverty
Table 3 details the observation count and population percentages according to income poverty across all survey periods. Beneath the 1.90-dollar poverty line, poverty incidence saw a gradual reduction, from 19.87% in 2011 to 8.46% in 2020. An analogous decline is observed under the 3.20-dollar poverty threshold. In 2011, 61.53% of middle-aged and elderly people had an income exceeding 3.20 dollar. This percentage increased to 80.37% in 2020. Additionally, Table 3’s examination of income poverty measures shows that more than 8% of the sample falls below the 1.90-dollar poverty line, while around 23% lie beneath the 3.20-dollar threshold.
Multidimensional poverty
Table 4 presents the results for multidimensional poverty based on multiple deprivation indicators. The poverty group’s incidence is decreasing sequentially from 23.64% in 2011 to 10.95% in 2018, but increasing to 11.50% in 2020. The precarity group’s incidence exhibits a fluctuating trend, initially rising from 37.96% in 2011 to 38.84% in 2015, before decreasing to 29.84% by 2020. In contrast, the prosperity group’s trend is the inverse of both the poverty and precarity groups. The proportion of the prosperity group saw a substantial rise, escalating from 38.40% in 2011 to 58.66% in 2020. Extreme poverty was observed for less than 0.61% of the sample in 2020. Secure prosperity is achieved by approximately 58.66% in 2020.
Fixed-effect logistic regression results
The impact of income poverty on health status
Rows 3–5 in Table 5 display fixed-effect logistic regression outcomes for income poverty across panel data models concerning self-rated health, ADL, and depression. Our findings indicate that income poverty has a negative impact on poor self-rated health, but not significant. Middle-aged and elderly people between 1.90 dollars and 3.20 dollars, and those below the 1.90 dollar poverty threshold had a 6.3% and 10.0% lower risk of reporting poor self-rated health, respectively, compared to those exceeding the 3.20 dollar poverty threshold (P > 0.1). Similarly, a significant negative association was observed between income poverty and ADL at the 5% significance level. Compared with those above the 3.20-dollar poverty threshold, middle-aged and elderly people between 1.90 dollar and 3.20-dollar poverty threshold and those below the 1.90-dollar poverty threshold had a 14.1% (P < 0.05) and 25.9% (P < 0.01) lower risk of poor ADLs, respectively. Regarding mental health, individuals aged middle to senior with incomes below 1.90 dollars and between 1.90 dollar and 3.20 dollar exhibited a 7.5% (P > 0.1) and 14.2% (P < 0.05) lower propensity for depression compared to their counterparts earning above 3.20 dollars.
The impact of multidimensional poverty on health status
Rows 6–11 in Table 5 present panel fixed-effect logistic regression results, highlighting the influence of multidimensional poverty on health. The analysis shows that individuals in the categories of extreme, moderate, and one-sided poverty, as well as those deemed vulnerable or in fragile prosperity, face a heightened risk of self-reported ill-health in comparison to the secure prosperity group. Specifically, the risk increases by 2.4% (P > 0.1), 7.0% (P > 0.1), 23.6% (P < 0.01), 1.9% (P > 0.1), and 13.4% (P < 0.05), respectively. In terms of ADL, compared to the secure prosperity group, the risk of poor ADLs is higher by 91.9% (P < 0.01), 43.9% (P < 0.01), 31.5% (P < 0.01), 27.8% (P < 0.05), and 35.4% (P < 0.1) in the extreme poverty, moderate poverty, one-sided poverty, vulnerability, and fragile prosperity group, respectively. In terms of mental health, the risk of depression is higher by 64.6% (P < 0.05), 11.4% (P > 0.1), 13.3% (P < 0.1), and 14.4% (P < 0.01) in the extreme poverty, moderate poverty, one-side poverty, vulnerability and fragile prosperity group, respectively, compared to the secure prosperity group.
Instrumental variables estimate
Appendix 4 presents the test results for IVs. First, we conducted a Hausman test for all models to assess endogeneity. The chi-square statistics from the regression analyses—specifically, those examining ADL and income poverty, as well as those exploring depression and precarity group, poverty group—indicate that we can reject the null hypothesis of exogeneity at the 1% significance level. This suggests that both income poverty and multidimensional poverty should be treated as endogenous variables, with the exception of the regressions focusing on self-rated health, depression, and income poverty, as well as those on self-rated health, ADL, precarity group, and poverty group. Second, the first-stage F-statistics across all models were substantially greater than the critical threshold of 10, alleviating concerns regarding weak instruments (Yogo, 2005). Third, the under-identification test rejected the null hypothesis (P-value = 0.000), confirming that the IVs are sufficiently correlated with the endogenous variables, indicating that all models are well-identified.
Rows 3–8 in Table 6 present the results of the IV estimates with individual fixed effects, which examine the relationship between income poverty and health status. Middle-aged and elderly people between 1.90 dollars and 3.20 dollars, and those below the 1.90 dollar poverty threshold, are at a lower risk of reporting poor ADLs compared to those exceeding the 3.20 dollar poverty threshold, but this difference is not significant. This suggests that endogeneity problems lead to estimation bias. In terms of self-rated health and depression, individuals aged middle to senior with incomes between 1.90 dollars and 3.20 dollars and incomes below 1.90 dollars failed the instrumental variable endogeneity test, suggesting that the panel fixed-effects logistic regression results are plausible.
Rows 9–14 in Table 6 provide the results of the IV estimates with individual fixed effects, emphasizing the impact of multidimensional poverty on health. The analysis reveals that individuals categorized as experiencing precarity and poverty are at an increased risk of self-reported ill-health as well as having an increased likelihood of functional limitations in ADLs and depression when compared to the secure prosperity group. Furthermore, we found no evidence of endogeneity bias between multidimensional poverty and self-rated health, poverty group and ADL, lending credibility to the main findings.
The results of the mechanism analysis
Appendix 5 shows that multidimensional poverty is negatively associated with depressed (P < 0.05), social participation (P > 0.1), health check-ups (P < 0.01), alcohol consumption (P > 0.1), and physical activity (P < 0.05) but is positively associated with smoking (P > 0.1) and non-use of clean fuels (P < 0.01). It indicates that multidimensional poverty has a profound impact on healthcare utilization and health behavior, thus influencing physical and mental health.
Discussion
In the context of China’s comprehensive elimination of absolute poverty, this study examines the relationship between poverty and health from the perspective of multidimensional poverty. We employ a panel fixed-effect model and instrumental variables estimation to examine the influence of poverty on health status. In general, we discover that poverty levels exert diverse effects on various health statuses. Our analysis provides new evidence that individuals experiencing poverty or precariousness are more likely to have poorer health compared to their prosperous counterparts. This study’s analysis offers crucial insights, demonstrating that multidimensional poverty exhibits a stronger correlation with health indicators than income poverty does. Not only those living in extreme poverty, but also those facing precarious situations are more likely to report poorer self-rated health, physical health and mental health compared to their prosperous counterparts (Aue et al., 2016; Zimmerman et al., 2022). This highlights the importance of a multidimensional approach, which is more effective than relying solely on income poverty identification to understand the effect of poverty on health status.
The overarching trend in multidimensional poverty shows a steady reduction in poverty incidence alongside a marginal decrease in the precarious group. This indicates an improvement in the housing security, healthcare, and old-age security for middle-aged and elderly people (Oshio and Kan, 2014). The findings indicate a marked rise in the prosperity group, with 58.66% of middle-aged and elderly individuals attaining relative prosperity by 2020, free from income poverty and concerns over housing, healthcare, and old-age security (Zeng et al., 2022). However, 41.34% of middle-aged and elderly people still belong to precarious and poverty groups in 2020, experiencing relative deprivation. Among them, 8.46% earn less than 1.90 dollars per day, while 21.80% earn more than 3.20 dollars but lack pension security or healthcare security or housing security. This highlights the necessity of not only addressing income poverty but also enhancing living security for older adults (Chen and Leu, 2022). It’s important to note that this study employed the concept of multidimensional poverty for measurement, considering multiple dimensions of deprivation rather than focusing solely on income poverty (Liu et al., 2023). Consequently, the incidence of multidimensional poverty in this study slightly exceeds that of studies solely measuring income poverty, as it incorporates multiple dimensions of deprivation to account for the multidimensional deprivation faced by middle-aged and elderly people (Wang et al., 2022).
Our study revealed that a multidimensional approach to poverty assessment proves more efficacious than income-based poverty identification alone in elucidating the impact of poverty on health. This study discerned varied impacts of poverty across self-rated health, mental health, and physical health. Regarding self-rated health, higher levels of poverty correspond to an increased probability of experiencing subpar self-rated health. Our results were consistent with Saito et al. (Saito et al., 2014). In terms of mental health, a clear positive correlation is observed with multidimensional poverty and depression, aligning with the findings of numerous studies (Fitzsimons et al., 2017; Ridley et al., 2020). Concerning physical health, our study uncovers a similar result: higher poverty levels are associated with an increased probability of poor physical health, consistent with the majority of earlier research (Duffee et al., 2016; Hajek and Koenig, 2022). Contrary to Zhou et al.‘s study on the association between health status (physical, mental, and self-rated health) and multidimensional poverty in older adults, but with a similar concluding statement (Zhou et al., 2023). Moreover, we found that the impact of multidimensional poverty on health is attributed to the reduced healthcare utilization, and compromised health behaviors (Wang et al., 2023; Zhou et al., 2023). The findings have far-reaching implications for policymakers aiming to implement prevention interventions against poverty recurrence and substantially enrich the existing body of literature on poverty and health.
With the aging issues becoming severe, the studies increasingly emphasize the importance of health targeting middle-aged and older adults (Li et al., 2022). In this study, the incidence of poverty and precarity among mid-aged and older adults was 18.04% and 36.07%, respectively, which is higher than the incidence of multidimensional poverty among other groups (Liang et al., 2024; Zou et al., 2023; Zimmerman et al., 2022). For middle-aged and elderly poverty is not only associated with poor self-rated health status (Wang et al., 2024), but also has a positive impact on poor physical health and poor mental health (Zhou et al., 2023; Li et al., 2022). The relationship between poverty and health within middle-aged and older adults reveals significant differences across material, psychosocial, and behavioral dimensions when compared to younger populations (Domènech-Abella et al., 2018; Dalecka et al., 2024). Middle-aged and elderly individuals often experience unique vulnerabilities that stem from both socio-economic factors and health-related issues. These age groups are particularly susceptible to multidimensional poverty due to a combination of limited financial resources, decreased health status, and social isolation (Wang et al., 2023; Zhou et al., 2023; Jin et al., 2020). Moreover, older adults, once in poverty, have a harder time escaping it due to lack of ability to acquire income to overcome poverty (Tan et al., 2023; Wang et al., 2011). Therefore, it is imperative that we prioritize the overall mental well-being of this demographic group and ensure that essential items are not withheld due to financial restrictions in poverty alleviation efforts (Zhao et al., 2024).
Conclusions
The study highlights that multidimensional poverty has a greater impact on health status compared to income poverty. This emphasizes the critical need to account for various deprivations and their dynamics in analyzing the poverty-health nexus. Findings indicate that middle-aged and older adults, even those not classified as income poor, may endure worse health outcomes due to specific deprivations. Recognizing that poor health in middle-aged and elderly is often irreversible and significantly impedes escaping poverty is crucial. Hence, combating poverty in middle-aged and elderly populations demands attention to various factors, including pensions, housing, and health insurance, beyond just health concerns. Such an approach aids in maintaining optimal health and disrupting the poverty cycle. Insights from this study may benefit other nations that have eradicated absolute poverty and are keen on adopting a multidimensional approach to address middle-aged and elderly poverty.
This study is subject to limitations. Its design may introduce biases. Omitted variables and recall bias can lead to inaccuracies in interpreting the relationship between multidimensional poverty and health status. Furthermore, the relationship between multidimensional poverty and health status is multifaceted, extending beyond the scope of what can be captured by our study. While poverty can contribute to adverse health status, it is also influenced by a range of other factors, including social capital and healthcare services. Taking these limitations into consideration will contribute to a more nuanced and well-rounded understanding of the relationship between multidimensional poverty and health status.
Data availability
The data used in this study can be found here: https://charls.charlsdata.com/pages/data/111/zh-cn.html.
References
Alkire S, Santos ME (2013) A multidimensional approach: poverty measurement & beyond. Soc Indic Res 112:239–257
Alkire S, Fang Y (2019) Dynamics of multidimensional poverty and uni-dimensional income poverty: an evidence of stability analysis from China. Soc Indic Res 142:25–64
Andresen EM, Malmgren JA, Carter WB, Patrick DL (1994) Screening for depression in well older adults—evaluation of a short-form of thE CES-D. Am J Prev. Med 10:77–84
Angulo R, Diaz Y, Pardo R (2016) The Colombian Multidimensional Poverty Index: measuring poverty in a public policy context. Soc Indic Res 127:1–38
Aue K, Roosen J, Jensen HH (2016) Poverty dynamics in Germany: evidence on the relationship between persistent poverty and health behavior. Soc Sci Med 153:62–70
Baltagi BH, Bresson G, Pirotte A (2003) Fixed effects, random effects or Hausman–Taylor? A pretest estimator. Econ Lett 79:361–369
Bank W (2020) Monitoring poverty at the US$3.20 and US$5.50 lines: differences and similarities with extreme poverty trends. https://blogs.worldbank.org/en/opendata/monitoring-poverty-us320-and-us550-lines-differences-and-similarities-extreme-poverty
Barrientos A, Gorman M, Heslop A (2003) Old age poverty in developing countries: contributions and dependence in later life. World Dev 31:555–570
Benzeval M, Judge K (2001) Income and health: the time dimension. Soc Sci Med 52:1371–1390
Chen KM, Leu CH (2022) Multidimensional perspective of the poverty and dynamics of middle-aged and older adults in Taiwan. Int Soc. Work 65:139–156
Chong C, Cai M, Yue XM (2022) Focus shift needed: from development-oriented to social security-based poverty alleviation in rural China. Econ. Polit Stud 10:62–84
Contoyannis P, Jones AM (2004) Socio-economic status, health and lifestyle. J Health Econ 23:965–995
Council Community P (2016) Poverty and child health in the United States. Pediatrics 137(4):e20160339
Dalecka A, Bartoskova Polcrova A, Pikhart H, Bobak M, Ksinan AJ (2024) Living in poverty and accelerated biological aging: evidence from population-representative sample of U.S. adults. BMC Public Health 24:458
Díaz Y, Hessel P, Avendano M, Evans-Lacko S (2022) Multidimensional poverty and adolescent mental health: unpacking the relationship. Soc Sci Med 311:115324
Domènech-Abella J, Mundó J, Leonardi M, Chatterji S, Tobiasz-Adamczyk B, Koskinen S, Ayuso-Mateos JL, Haro JM (2018) The association between socioeconomic status and depression among older adults in Finland, Poland and Spain: a comparative cross-sectional study of distinct measures and pathways. J Affect Disord 241:311–318
Ebbinghaus B (2021) Inequalities and poverty risks in old age across Europe: the double-edged income effect of pension systems. Soc Policy Adm 55:440–455
Evandrou M, Fakingham J, Feng Z, Vlachantoni A (2014) Individual and province inequalities in health among older people in China: evidence and policy implications. Health Place 30:134–144
Fitzsimons E, Goodman A, Kelly E, Smith JP (2017) Poverty dynamics and parental mental health: determinants of childhood mental health in the UK. Soc Sci Med 175:43–51
Fu L, Pei T, Xu J, Han J, Yang J (2024) Inspecting the “health poverty trap” mechanism: self-reinforcing effect and endogenous force. BMC Public Health 24:917
Garman EC, Avendano M, Araya R, Evans-Lacko S, McDaid D, Zimmerman A, Lund C (2022) Understanding the complex relationship between multidimensional poverty and depressive symptoms among young South Africans: a cross-sectional study. J Affect Disord 319:352–360
Groh-Samberg (2008) Persistent poverty is increasing in Germany. http://www.diw.de/documents/publikationen/73/diw_01.c.91272.de/soep_wave_report_2008.pdf
Habibov N, Auchynnikava A, Luo R (2019) Poverty Does Make Us Sick Ann Glob Health 85(1):33
Hajek A, König HH (2022) What factors are associated with functional impairment among the oldest old? Front Med 9:1092775
Hasan MS, Ghosal S (2024) Unveiling the mechanism(s) Between poverty, deprivation, and depression in older indian adults: findings from a nationwide survey. J Aging Health 4:8982643241280529
Hirokazu Y, Lawrence AJ, Beardslee WR (2012) The effects of poverty on the mental, emotional, and behavioral health of children and youth: implications for prevention. Am Psychol 67:272–284
Honjo K, Kawakami N, Takeshima T, Tachimori H, Ono Y, Uda H, Hata Y, Nakane Y, Nakane H, Iwata N, Furukawa TA, Watanabe M, Nakamura Y, Kikkawa T (2006) Social class inequalities in self-rated health and their gender and age group differences in Japan. J Epidemiol 16:223–232
Hou J, Zhou W, Jiang Y (2022) Multidimensional energy poverty and depression among China's older adults. Front Public Health 10:977958
Jin Y, Zhu D, He P (2020) Social causation or social selection? The longitudinal interrelationship between poverty and depressive symptoms in China. Soc Sci Med 249:112848
Kim A-Y, Seo MS, Kang H-Y (2022) Health disparity and healthcare utilization inequity among older adults living in poverty in South Korea: a cross-sectional study. BMC Geriatrics 22:999
Korenman S, Remler DK, Hyson RT (2021) Health insurance and poverty of the older population in the United States: the importance of a health inclusive poverty measure. J Econ Ageing 18:100297. (prepublish)
Ku I, Kim C-O (2020) Decomposition analyses of the trend in poverty among older adults: the case of South Korea. J Gerontol Ser B 75:684–693
Kühn S, Rieger UM (2017) Health is a state of complete physical, mental and social well-being and not merely absence of disease or infirmity. Surg Obes Relat Dis 13:887
Li X, Yang H, Jia J (2022) Impact of energy poverty on cognitive and mental health among middle-aged and older adults in China. Humanit Soc. Sci Commun 9:253
Liang X, Xiao H, Hou F, Guo X, Li L, Huang L (2024) Breaking the chains of poverty: examining the influence of smartphone usage on multidimensional poverty in rural settings. Humanit Soc. Sci Commun 11:142
Liu M, Feng X, Zhao Y, Qiu H (2023) Impact of poverty alleviation through relocation: from the perspectives of income and multidimensional poverty. J. Rural Stud 99:35–44
Luo R-f LiuC-f, Gao J-j WangT-y, Zhi H-y ShiP-f, Huang J-k (2020) Impacts of the COVID-19 pandemic on rural poverty and policy responses in China. J. Integr Agric 19:2946–2964
Mackenbach JP (2006) Health inequalities: Europe in profile. http://ec.europa.eu/health/ph_determinants/socio_economics/documents/ev_060302_rd06_en.pdf
Meisters R, Putrik P, Westra D, Bosma H, Ruwaard D, Jansen M (2023) Two sides of the same coin? Absolute income and perceived income inadequacy as social determinants of health. Int J Equity Health 22:128
Mullan B, Olivier C, Thøgersen-Ntoumani C (2021) Mind the gap: Habit and self-determined motivation predict health behaviours in middle-aged and older adults. Br J Health Psychol 26:1095–1113
Nations U (2015) End poverty in all its forms everywhere. https://sdgs.un.org/goals/goal1
Nolan B, Whelan CT (2007) On the multidimensionality of poverty and social exclusion. In: Jenkins SP, Micklewright J (eds) Inequality and poverty re-examined. Oxford University Press
OECD (2023) Pensions at a glance 2023. OECD Pensions at a Glance, 2023
Oshio T, Kan M (2014) Multidimensional poverty and health: evidence from a nationwide survey in Japan. Int J Equity Health 13:128
Padmanabhanunni A, Pretorius TB, Isaacs SA (2023) Satisfied with Life? The Protective Function of Life Satisfaction in the Relationship between Perceived Stress and Negative Mental Health Outcomes Int J Environ Res Public Health 20:6777
Pan J, Lei X, Liu GG (2016) Health insurance and health status: exploring the causal effect from a policy intervention. Health Econ. 25:1389–1402
Pförtner T-K, Demirer I (2022) How working conditions, socioeconomic insecurity, and behavior-related factors mediate the association between working poverty and health in Germany Int J Public Health 67:1604555
Pinilla-Roncancio M, Mactaggart I, Kuper H, Dionicio C, Naber J, Murthy GVS, Polack S (2020) Multidimensional poverty and disability: a case control study in India, Cameroon, and Guatemala. SSM—Popul Health 11:100591
Reumers L, Bekker M, Hilderink H, Jansen M, Helderman J-K, Ruwaard D (2022) Qualitative modelling of social determinants of health using group model building: the case of debt, poverty, and health Int J Equity Health 21:72
Ridley M, Rao G, Schilbach F, Patel V (2020) Poverty, depression, and anxiety: Causal evidence and mechanisms. Science 370:1289–128
Saito M, Kondo K, Kondo N, Abe A, Ojima T, Suzuki K, Grp J (2014) Relative deprivation, poverty, and subjective health: JAGES cross-sectional study. PLoS ONE 9:e111169
Shinyoung S (2009) Factors related to the health related quality of life in elderly women. Korean J Women Health Nurs. 15:99–99
Shuo D (2023) Vulnerability to poverty in Chinese households with elderly members: 2013–2018. Sustainability 15:4947–4947
Staufenbiel SM, Penninx BW, Spijker AT, Elzinga BM, van Rossum EF (2013) Hair cortisol, stress exposure, and mental health in humans: a systematic review. Psychoneuroendocrinology 38:1220–1235
Steptoe A, Deaton A, Stone AA (2015) Subjective wellbeing, health, and ageing. Lancet 385:640–648
Tan H, Dong Z, Zhang H (2023) The impact of intergenerational support on multidimensional poverty in old age: empirical analysis based on 2018 CLHLS data Humanit Soc Sci Commun. 10:439
Tekguc H, Akbulut B (2022) A multidimensional approach to the gender gap in poverty: an application for Turkey. Feminist Econ. 28:119–151
Thomson RM, Kopasker D, Leyland A, Pearce A, Katikireddi SV (2023) Effects of poverty on mental health in the UK working-age population: causal analyses of the UK Household Longitudinal Study. Int J. Epidemiol. 52:512–522
Trani J-F, Zhu Y, Park S, Khuram D, Azami R, Fazal MR, Babulal GM (2023) Multidimensional poverty is associated with dementia among adults in Afghanistan eClinicalMedicine 58:101906
UNDP (United Nations Development Programme) (2021) 2021 Global Multidimensional Poverty Index (MPI): Unmasking disparities by ethnicity, caste and gender. New York
United Nations (2016) Sustainable development goals explained: no poverty. https://www.un.org/en/academic-impact/page/no-poverty
Van Vliet O, Wang C (2015) Social investment and poverty reduction: a comparative analysis across fifteen European Countries. J. Soc. Policy 44:611–638
Wagstaff A (2002) Poverty and health sector inequalities: policy theme papers. Bull World Health Organ 80:97–105
Wang BB, Luo Q, Chen GP, Zhang Z, Jin PB (2022) Differences and dynamics of multidimensional poverty in rural China from multiple perspectives analysis. J Geogr Sci 32:1383–1404
Wang Q, Shu L, Lu X (2023) Dynamics of multidimensional poverty and its determinants among the middle-aged andolder adults in China Humanit Soc. Sci Commun 10:116
Wang X, Ye X (2024) Impact of the targeted poverty alleviation policy on older adults’ healthcare utilization: a quasi-experimental analysis from China. Soc Sci Med 356:117146
Wang X, Shang X, Xu L (2011) Subjective well-being poverty of the elderly population in China. Soc Policy Adm 45:714–731
Wang Y, Wu Y, Wang C, Li L, Lei Y, Wu S, Qu Z (2024) The impact of energy poverty on the health and welfare of the middle-aged and older adults. Front Public Health 12:1404014
Wang X (2022) On the relationship between income poverty and multidimensional poverty in China. In: Multidimensional poverty measurement: theory and methodology. Springer. pp. 85–106
Xiao H, Liang X, Chen C, Xie F (2022) The Impact of Multidimensional Poverty on Rural Households’ Health: From a Perspective of Social Capital and Family Care Int J Environ Res Public Health 19:14590
Yang H, Li X, Yan J (2025) The impact of energy poverty on subjective well-being: evidence from China. Humanit Soc Sci Commun. 12:379–379
Yogo SM (2005) Asymptotic properties of the Hahn-Hausman test for weak-instruments Econ Lett 89(3):333–342
Zeng W, Zhao P, Zhao Y, Saddique R (2022) The multidimensional relative poverty of rural older adults in China a nd the effect of the health poverty alleviation policy. Front Public Health 10:793673
Zhai S, Yuan S, Dong Q (2021) The impact of health insurance on poverty among rural older adults: an evidence from nine counties of western China. Int J Equity Health 20:47
Zhang L, Zhao Y (2021) Breaking the Vicious Cycle between Illness and Poverty: Empirical Actions on Land Use in an Oasis Agricultural Area Land 10:335
Zhang Q, Shen Y (2020) The comparison of international relative poverty standards and its inspiration to China. J Nanjing Agric Univ (Soc Sci Ed) 20:91–99
Zhao JP, Liu XX, Gao Y, Li DX, Liu FF, Zhou J, Zha FB, Wang YL (2024) Estimates of multidimensional poverty and its determinants among older people in rural China: evidence from a multicenter cross-sectional survey BMC Geriatr 24:835
Zhao Y, Hu Y, Smith JP, Strauss J, Yang G (2014) Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol 43:61–68
Zhou L, Zhu C, Walsh CA, Zhang X (2023) Assessing the effect of health status on multidimensional poverty among older adults: the Chinese longitudinal healthy longevity survey Front Public Health 11:1150344
Zimin L, Mingyan D (2020) Impact of energy poverty on the welfare of residents and its mechanism: an analysis based on CGSS data. China Soft Sci 08:143–163
Zimmerman A, Lund C, Araya R, Hessel P, Sanchez J, Garman E, Evans-Lacko S, Diaz Y, Avendano-Pabon M (2022) The relationship between multidimensional poverty, income poverty and youth depressive symptoms: cross-sectional evidence from Mexico, South Africa and Colombia. BMJ Glob Health 7:e006960
Zou W, Cheng XP, Fan ZZ, Yin WX (2023) Multidimensional relative poverty in China: identification and decomposition. Sustainability 15(6):4869
Acknowledgements
This paper is supported by the National Natural Science Foundation of China (Grant Number: 72274108) and the Natural Science Foundation of Shandong Province (Grant Number: ZR2022MG003).
Author information
Authors and Affiliations
Contributions
Shiju Dong: Data curation, methodology, writing—original draft; Zexuan Yu: Supervision, writing—editing; Siqian Zhang: Data curation, supervision; Jiajia Li: Conceptualization, funding acquisition, supervision, writing—review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study used open data. Our institute does not require ethical approval for this type of study. The CHARLS survey was approved by the Ethical Review Committee of Peking University (IRB00001052-11015).
Informed consent
In the data collection of the CHARLS (China Health and Retirement Longitudinal Study) survey, all participants signed the informed consent at the time of participation.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Dong, S., Yu, Z., Zhang, S. et al. Multidimensional poverty dynamics and health among middle-aged and elderly people: a longitudinal study in China. Humanit Soc Sci Commun 12, 927 (2025). https://doi.org/10.1057/s41599-025-05287-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-025-05287-9
