
Abstract
Personalized treatment in head and neck cancer remains limited despite substantial biological heterogeneity. Using the SuPerTreat project as a case study, we outline a prototype clinical decision support system (CDSS) integrating transcriptomic data and artificial intelligence (AI), and summarize expert consensus on its potential, requirements for accuracy, validation, regulatory alignment, and clinical implementation. This Perspective provides a roadmap to guide future development and responsible integration of CDSS into precision oncology.
Similar content being viewed by others


Precision medicine is rapidly advancing across various medical fields, fueled by the continuous evolution of Artificial Intelligence (AI) technologies. In oncology, precision medicine is revolutionizing patient outcomes by tailoring treatments to individual genomic profiles. Precision oncology embraces the integration of genetic alterations in the decision-making process. Treatment targeting a defined molecular alteration largely demonstrated clinical efficacy across various tumor types1. Consequently, comprehensive multigene sequencing has become a standard tool for diagnosis and treatment allocation2.
This field of innovation usually applies for patients with advanced recurrent/metastatic cancer. Unfortunately, in the treatment of loco-regionally advanced non-metastatic head and neck squamous cell carcinoma (HNSCC), where curative treatments include various combinations of surgery, radiotherapy, and chemotherapy3,4, the implementation of personalized oncology has been challenging and remains underdeveloped.
To improve outcomes in the HNSCC definitive setting, several clinical trials have explored both therapeutic intensification and de-intensification strategies5,6. Notably, these studies did not reach the goal of modifying the standard of care (SoC) for HNSCC patients. Escalating curative treatments with concomitant or adjuvant immunotherapy did not significantly improve survival in unselected patients5,6,7. Survival benefit for HNSCC patients undergoing surgery has been recently observed with neoadjuvant immune checkpoint inhibitors8.
Moreover, it is central to consider that HNSCC should not be considered and managed with a “one-size-fits-all” approach. The clinical heterogeneity is made more complex by the biological intricacy. Unlike other solid cancers, HNSCC typically lacks druggable genetic mutations or actionable molecular alterations9, making genomics a relatively poorly informative field for HNSCCs. Nevertheless, transcriptomics was found to be informative in this setting. Indeed, six gene expression (GE) clusters were described in HNSCC10, and such heterogeneity makes these malignancies potentially suitable for personalized treatments11,12.
The need for a customized approach is now even more pressing due to the failure of the current patient stratification by prognostic factors as clinical and biological features, consisting mainly of stage, site of disease, performance status, comorbidities, smoking history, and HPV status. One could speculate that failures in achieving improved outcomes and effective patient stratification can be attributed to several factors as prognosis determined from a relatively small number of cases and/or based on inadequate or insufficient criteria. Other drawbacks include relying solely on a good prognosis for de-intensification, whereas additional selection factors are necessary. Failures may be also due to the presence of subgroups with varying prognoses even within diseases with an overall favorable clinical behavior (e.g., three GE clusters in HPV+ oropharyngeal carcinoma)13.
This manuscript does not aim to present original validation results, but rather to propose a translational framework and expert-informed roadmap for the development, validation, and future clinical implementation of CDSS in curative HNSCC.
AI and CDSS in oncology
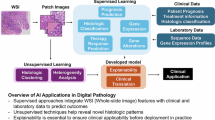
Recent years have seen exponential growth in AI applications in oncology14,15. These new tools have the potential to improve the precision in diagnosis, prediction of outcomes, and to reach a tailored treatment14,16. Today, AI systems are increasingly being incorporated into several clinical settings, such as image-based computer-aided discovery and diagnosis (subtyping, grading, staging); translation of genomic information; prediction and tracking of patient’s response; and identification of pathological features16,17. By combining omics and phenotype data, AI can assist physicians in patient stratification, in clinical decision-making, and in the discovery of new biomarkers to predict the recurrence of disease16,17.
A significant number of publications using AI to identify novel diagnostic and prognostic biomarker signatures on tissue images of different cancer types are currently accessible18. In particular, these studies demonstrated that the identification of biomarkers and genetic modifications by AI is effective, especially in breast, gastrointestinal, prostate, and lung cancers17. In this scenario, most of the biomarkers showed a significant role in cancer diagnosis, tumor subtyping, evaluation of pathologic features, and only in some cases for prognosis forecasting17. Therefore, the interest in exploiting AI for biomarker development is crucial, but so far, limited interest has been assigned in the field of HNSCC amenable to curative treatments, which is the main use case scenario and focus of the current work.
Clinical decision support systems (CDSS) are tools that may integrate clinical data and features obtained through AI. The systems process data adequately, matching them to their database and reaching a recommendation that can be implemented in the decision-making process at the point of care and should be aligned with clinical practice guidelines19. An increasing number of applications of CDSSs in precision oncology have been described. Kumar and colleagues developed a machine learning CDSS capable of identifying predictive features in patients affected by breast cancer. The tool can select patients and predict cancer outcomes, outperforming the state-of-the-art strategy in precision, specificity, accuracy, and sensitivity20.
CDSSs validation criteria
Despite their potential, only a few CDSSs have been externally validated and implemented in clinical practice19. CDSSs should satisfy numerous validation criteria to be safely implemented in daily care. Data are keys and should be interoperable, accurate, and available. Validity of recommendations and interoperability are the most important facilitators for implementation19. Hendriks and colleagues have built an algorithm to check the validity of CDSS aimed at ensuring the concordance between multidisciplinary teams’ decisions and CDSS recommendations19. The CDSS should also be made available for everyday clinical practice, aligned with the preferences of the clinicians involved and of the patients. Finally, it should be easy to use and transparent19. The main barriers to the implementation of CDSS are missing data, inability to reuse data, insufficient standardized definition, and time-consuming data collection17. Other hurdles include the failure of the CDSS to deliver real-time support and be integrated into the clinical workflow19.
AI and CDSS in HNSCC
So far, the application of AI in the context of HNSCC has focused in the following areas: detection of precancerous and cancerous lesions in histopathologic slides; prediction of histopathologic nature of a lesion from imaging; prognostication; extraction of pathological findings from imaging; and applications in radiation oncology21.
Biological model applications in HNSCC have demonstrated excellent prognostic and potentially predictive powers. Indeed, an unsupervised analysis of the molecular heterogeneity of HNSCC revealed the existence of six GE subtypes. These molecular data provided useful information for the prognosis of HNSCC patients10.
Another prediction model has been developed in the field of HPV+ oropharyngeal squamous cell carcinoma22. The peculiarity of this model was the inclusion of genomic adjusted radiation dose (GARD), a previously described model of the treatment effect of radiotherapy, in outcomes prediction of patients treated with radiotherapy (+/− chemotherapy)22. In a virtual trial, GARD outclassed a clinical nomogram in predicting overall survival (OS). Moreover, GARD predicted the decrease of OS in association with RT dose de-escalation, and proposed a new method to stratify patients based on GE22.
Translating the biological complexity into clinical practice—expert discussion
An international team of HNSCC specialists met on January 26th, 2024, in Milan, Italy, to discuss the challenges and opportunities of integrating biological complexity, particularly gene expression (GE), into clinical practice. They focused on a CDSS aimed to support personalized treatment decisions in HNSCC candidate to definitive treatments. This CDSS, developed within the SuPerTreat project (“Supporting Personalized Treatment Decisions in Head and Neck Cancer through Big Data”, funded by ERA PerMed, and the EU’s Horizon 2020 under the Marie Skłodowska-Curie Actions Grant), was used as a case study. The discussion highlighted the unmet needs for integrating CDSS-based decision-making into clinical practice, the potential for CDSS to modify therapeutic approaches, its acceptance among clinicians, and the required accuracy for reliable predictions.
A novel CDSS in HNSCC management/case study—prototype description
In the present manuscript, SuPerTreat is not described in terms of model training, dataset composition, or clinical utility metrics, but rather as a prototype CDSS used to support a translational and expert-driven discussion. In this scenario, the SuPerTreat project led to the development of a CDSS to predict patient prognosis by integrating clinical and biological data. This collaborative European initiative aimed to validate methods that incorporate real-world data from transcriptomic analyses. The SuPerTreat CDSS leverages proprietary and public repositories of gene expression data to identify subpopulations that could benefit from specific treatments. The AI-based models developed under SuPerTreat allow the entry of different covariates for the survival analysis, such as dataset (proprietary vs public); genomic data, age, sex, TNM stage (I-II vs. III/IVa/IVb), smoking status (current/former vs. never), tumor subsite (oral cavity vs. HPV+ oropharynx vs. HPV- oropharynx vs. larynx vs. hypopharynx), treatment (surgery, radiotherapy, systemic treatment), setting (curative, rec/met). The endpoints considered are: overall survival (all patients); disease-free survival (curative setting only), and progression-free survival (rec/met setting only).
The models have produced validated prognostic and predictive GE signatures, which are incorporated into the CDSS as independent modules, without implying additive or synergistic performance at the current stage. To address skepticism about its usability,the prototype CDSS was qualitatively discussed by experts in terms of usability, interpretability, and potential clinical relevance; no formal quantitative consensus metrics were collected. The results showed that certain GE profiles could benefit more from specific therapies like radiation, surgery, or chemotherapy. The ultimate goal is to validate the SuPerTreat CDSS thoroughly to ensure its timely implementation in clinical practice in the future.
Results of expert discussion/qualitative consensus
The following section summarizes qualitative insights derived from expert discussion rather than quantitative outcome analyses. To shape the discussion, the experts discussed the following clinical use case scenarios for HNSCC patients candidates to curative treatments:
-
1.
HPV-negative HNSCC patient with a high-risk disease detected at tumor GE profiling. Would you accept to intensify the curative treatment? E.g., adding radiation for cases without indication as per current guidelines, or adding chemotherapy concomitantly with radiation for cases candidates to exclusive radiation as per current guidelines
-
2.
Assuming an equivalence between surgery and radiotherapy for a specific HNSCC, would you accept the following schema based on tumor GE profiling? If biologic profiling reveals that the tumor is radiosensitive, the patient receives radiotherapy. If biologic profiling reveals that the tumor is radioresistant, the patient undergoes surgery.
-
3.
HNSCC patient who is a candidate for radiation alone (either post-operative or definitive), meaning that no systemic therapies would be administered as per guidelines. GE profiling shows that the tumor has a profile characterized by suboptimal prognosis (compared to what may predicted by clinical characteristics) and a sensitivity to the drug cetuximab. Would you accept to intensify the curative treatment adding cetuximab to radiotherapy?
These three scenarios augmented the expert discussion, which elicited several thoughts and considerations that are reported herein. First of all, experts highlighted the urgent need for the application of AI in the integration of biological data in clinical decision-making in the context of definitive treatments for loco-regionally advanced HNSCC.
The discussion allowed to emphasize the potential of AI in oncology, not only in terms of outcome but also in training less experienced physicians in a better evaluation and decision process in HNSCC.
In clinical practice, a non-negligible fraction of HNSCC patients have poor outcomes, so it is crucial to implement transcriptomic data to guide clinical decisions in order to choose the best treatment. Some of the most important unmet needs are to know for which patient surgery or radiation, with or without chemotherapy, would be beneficial. All experts recognized the enormous potential value of SuPerTreat CDSS in HNSCC management.
Furthermore, several critical aspects emerged concerning the applicability of SuPerTreat CDSS in clinical practice that are discussed below.
Regulation
All experts agreed that the use of CDSS in clinical practice needs a good clinical practice (GCP) / good clinical laboratory practice (GCLP) validation. Data in the CDSS comes from research and can be re-analyzed in clinical labs, and it is crucial to perform further validation. A European initiative will regulate and facilitate the sharing and the pulling of data across borders and institutions. This kind of initiative will cover data standardization, analysis models, and patients’ consent for the use of data.
Accuracy
To discuss the accuracy, the experts considered the concordance index (Harrell’s C-index) in the prediction of 2-year overall survival of four GE models based on the clinical scenario of interest (Table 1). These C-index values are reported to illustrate the level of prognostic performance achieved by individual, previously validated GE models within their original clinical contexts, and are not intended to represent the performance of the integrated CDSS or to imply synergistic effects between models. Additional details regarding sample size, external validation, and clinical context of each model are summarized in Table 1.
Experts acknowledged that currently available gene expression models show prognostic performance around 70% in terms of concordance index (Table 1); however, there was broad agreement that substantially higher accuracy would be required to justify treatment intensification or de-intensification in routine clinical practice.
Validation
Even if data have been already externally validated (i.e., only already published GE models were included in the CDSS), further validation steps are needed for the workflow, possibly through prospective or retrospective trials. The model will need to be tested as a new paradigm in clinical practice, comparing the use of the model compared to SoC. Results must be consistent with current knowledge. Beyond prognostic performance, future validation steps will need to formally quantify clinical net benefit, including decision curve analysis, comparative effectiveness, and health-economic impact, before the CDSS can be considered for routine clinical use.
Clinical impact and health-economic considerations
Demonstrating clinical utility is a prerequisite for the implementation of CDSS in oncology. For SuPerTreat, this will require formal assessment of net clinical benefit, comparison with standard-of-care decision strategies, and evaluation of cost-effectiveness in different healthcare systems. These aspects are integral components of the proposed development roadmap but are not addressed in the present work.
Simplicity and transparency
The experts found the tool simple to use. It is important that CDSS is understandable and will use performance indicators to monitor its performance, efficacy and accordance to current Guidelines.
Other aspects deemed worthy of attention are visualization, increasing patient numbers, trustworthiness, and data quality.
Visualization
A schematic overview of the end-to-end SuPerTreat CDSS workflow, from data input to decision-support output, is shown in Fig. 1. Three possible outputs of the CDSS were hypothesized: textual, bar graphs, and pictographs (Supplementary Fig. 1, panels A, B, and C, respectively). Experts agreed on the fact that the recommendation must be simple and immediately clear both for clinicians and patients. Therefore, a bar graph was deemed as an ideal example.

Patient-level clinical variables and transcriptomic data are integrated within the SuPerTreat CDSS, which incorporates previously published and externally validated gene expression models as independent modules. The system generates prognostic stratification and decision-support outputs intended to complement multidisciplinary discussion and guideline-based care. The CDSS is presented as a prototype framework and requires formal clinical validation before routine clinical implementation.
Acceptability
There was broad consensus that we will need a strategy to manage challenges in clinician acceptance, for example emphasizing the potential benefits in healthcare costs.
Increasing patient numbers
Experts consistently emphasized that accuracy depends mostly on the number of patients and statistics. Strategies will be initiated to involve pharmaceutical companies and international groups to expand patient data.
Data quality
All experts agreed that data should come from high-volume and high-reputation centers, where they perform both genomic expression tests and therapies.
Trustworthiness
The method should be transparent. Recommendations have to be perceived as replicable and consistent with current knowledge.
Summary of consensus statements
-
CDSS integrating transcriptomic data has strong potential to improve patient stratification in curative HNSCC.
-
Such systems should not be used to modify standard treatments outside clinical trials until formal validation is completed.
-
Accuracy thresholds substantially higher than current clinical models are required to justify treatment intensification or de-intensification.
-
Prospective validation and health-economic assessment are mandatory before clinical implementation.
Limitations
This work does not include independent retrospective or prospective validation of the SuPerTreat CDSS, nor formal comparative analyses against standard prognostic models. Therefore, the system should be considered a prototype and hypothesis-generating tool. Rigorous clinical validation, health-economic evaluation, and regulatory assessment are required before clinical adoption.
Proposed implementation roadmap for CDSS in curative HNSCC
Short-term (current stage)
-
Integration of previously validated transcriptomic models
-
Standardization of data pipelines and outputs
-
Retrospective benchmarking against standard-of-care decision pathways
Mid-term (1–3 years)
-
Prospective observational validation
-
Decision-analytic and health-economic evaluation
-
Regulatory alignment and good clinical practice and good clinical laboratory practice (GCP/GCLP) compliance
Long-term (3–5 years)
-
Interventional clinical trials guided by CDSS output
-
Reimbursement strategies and payer engagement
-
Full integration into multidisciplinary tumor boards
Conclusion
The integration of biological and clinical data enhances prognostic accuracy in HNSCC patients. GE is particularly promising, providing more precise prognostic information than clinical or pathological data, including HPV status. The SuPerTreat CDSS illustrates the potential role of transcriptomic-driven decision support systems in improving patient stratification strategies in the curative setting. Incorporating GE models into clinical research and practice will influence clinical trial ethics, cost-effectiveness, and serve educational purposes for patient information and empowerment.
Currently, modifying standard therapies based solely on biological prognostic models, even those that are highly accurate and externally validated, is not SoC. However, benchmark studies have shown benefits from treatment adjustments guided by these models. Furthermore, such models can help select clinical trial participants more effectively, potentially reducing the number of patients required for studies. Integrating GE and clinical data through tools like the SuPerTreat CDSS is a promising strategy for personalizing curative treatments in HNSCC. Stringent validation studies are needed to support its broader implementation in research and clinical settings. This work should be interpreted as a roadmap and consensus framework rather than as evidence of clinical utility. Demonstrating additive or synergistic prognostic value through formal comparative metrics will be a critical component of future validation studies. Engaging academic institutions in data sharing will be crucial for advancing clinical practice in HNSCC management.
Data availability
No datasets were generated or analysed during the current study.
References
Bode, A. M. & Dong, Z. Recent advances in precision oncology research. Precision Oncol. 2, 11 https://doi.org/10.1038/s41698-018-0055-0 (2018).
Benary, M. et al. Leveraging large language models for decision support in personalized oncology. JAMA Netw. Open 6, e2343689 (2023).
Machiels, J. P. et al. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNSeESMOeESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 31, 1462–1475 (2020).
NCG GUIDELINES 2019 Head & Neck Cancer Management Guidelines
Machiels, J. P. et al. Pembrolizumab plus concurrent chemoradiotherapy versus placebo plus concurrent chemoradiotherapy in patients with locally advanced squamous cell carcinoma of the head and neck (KEYNOTE-412): a randomised, double-blind, phase 3 trial. Lancet Oncol. 25, 572–587 (2024).
Lee, N. Y. et al. Avelumab plus standard-of-care chemoradiotherapy versus chemoradiotherapy alone in patients with locally advanced squamous cell carcinoma of the head and neck: a randomised, double-blind, placebo-controlled, multicentre, phase 3 trial. Lancet Oncol. 22, 450–462 (2021).
Wong, D. J. et al. IMvoke010: A phase III, double-blind randomized trial of atezolizumab (atezo) after definitive local therapy vs placebo in patients (pts) with high-risk locally advanced (LA) squamous cell carcinoma of the head and neck (SCCHN) oral presentation at AACR 2024 reports efficacy and safety data from IMvoke010: a phase III randomized study of atezolizumab as therapy after multi-modal definitive treatment in patients with high-risk locally advanced squamous cell carcinoma of the head and neck.
Seymur, C. Perioperative Pembrolizumab Meets EFS End Point in Newly Diagnosed, Resected Stage III/IVA HNSCC Available at: https://www.onclive.com/view/perioperative-pembrolizumab-meets-efs-end-point-in-newly-diagnosed-resected-stage-iii-iva-hnscc.
The Cancer Genome Atlas Network Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature 517, 576–582 (2015).
De Cecco, L. et al. Head and neck cancer subtypes with biological and clinical relevance: Meta-analysis of gene-expression data. Oncotarget 6, 9627–9642 (2015).
Foy, J. P. et al. A 13-gene expression-based radioresistance score highlights the heterogeneity in the response to radiation therapy across HPV-negative HNSCC molecular subtypes. BMC Med. 15, 165 (2017).
Foy, J. P. et al. Immunologically active phenotype by gene expression profiling is associated with clinical benefit from PD-1/PD-L1 inhibitors in real-world head and neck and lung cancer patients. Eur. J. Cancer 174, 287–298 (2022).
Cavalieri, S. et al. Clinical validity of a prognostic gene expression cluster-based model in human papillomavirus–positive oropharyngeal carcinoma. JCO Precis. Oncol. PO.21.00094. https://doi.org/10.1200/PO.21.00094 (2021).
Zeng, J. et al. Molecular-based precision oncology clinical decision-making augmented by artificial intelligence. Emerg. Top. Life Sci. 5, 757–764 (2021).
Lotter, W. et al. Artificial intelligence in oncology: current landscape, challenges, and future directions. Cancer Discov. 14, 711–726 (2024).
Fawaz, A. et al. Systems biology in cancer diagnosis integrating omics technologies and artificial intelligence to support physician decision making. J. Pers. Med. 13, 1590 (2023).
Jiang, Y. et al. Emerging role of deep learning-based artificial intelligence in tumor pathology. Cancer Commun. 40, 154–166 (2020).
Huss, R. et al. Artificial intelligence and digital biomarker in precision pathology guiding immune therapy selection and precision oncology. Cancer Rep. 6, e1796 (2023).
Hendriks, M. P. et al. Clinical decision support systems for multidisciplinary team decision-making in patients with solid cancer: composition of an implementation model based on a scoping review. Crit. Rev. Oncol. Hematol. 195, 104267 (2024).
Kumar-Singh, L. et al. A novel enhanced hybrid clinical decisionsupport system for accurate breast cancerprediction. Measurement. 221, 113525 (2023).
Makitie, A. A. et al. Artificial intelligence in head and neck cancer: a systematic review of systematic reviews. Adv. Ther. 40, 3360–3380 (2023).
Ho, E. et al. A clinicogenomic model including GARD predicts outcome for radiation treated patients with HPV+ oropharyngeal squamous cell carcinoma. medRxiv https://doi.org/10.1101/2023.09.14.23295538 (2023).
De Cecco, L., Bossi, P., Locati, L., Canevari, S. & Licitra, L. Comprehensive gene expression meta-analysis of head and neck squamous cell carcinoma microarray data defines a robust survival predictor. Ann. Oncol. 25, 1628–1635 (2014).
Eschrich, S. A. et al. A gene expression model of intrinsic tumor radiosensitivity: prediction of response and prognosis after chemoradiation. Int. J. Radiat. Oncol. 75, 489–496 (2009).
Torres-Roca, J. F., Grass, G. D., Scott, J. G. & Eschrich, S. A. Towards data driven RT prescription:integrating genomics into RT clinical practice. Semin. Radiat. Oncol. 33, 221–231 (2023).
Wells, J. D., Griffin, J. R. & Miller, T. W. Pan-cancer transcriptional models predicting chemosensitivity in human tumors. Cancer Inf. 20, 117693512110024 (2021).
Acknowledgements
Medical writing support was provided by Simona Caporali. The Authors are grateful to (in alphabetical order): Anna Brambilla, Silvana Canevari, Thanasis Dalianis, Estefania Estevez, Giuseppe Fico, Erlend Ignacio Fleck Fossen, Arnoldo Frigessi, Liss Hernandez, Eivind Hovig, Maritini Kalogerini, Maud Kamal, Marissa Erin LeBlanc, Laura Lopez Perez, Antonello Manocchio, Elena Martinelli, Francesca Mazzetti, Mauricio Moreira Soares, Vanessa Sachse, Kathrin Scheckenbach, Mara Serena Serafini, Ingeborg Tinhofer-Keilholz, Laura Vergani. This project was supported by FRRB (Fondazione Regionale per la Ricerca Biomedica) under the frame of ERA PerMed (2019 Joint Transnational Call for Proposals for “Personalised Medicine: Multidisciplinary Research Towards Implementation”), as part of the research project “Supporting Personalized Treatment Decisions in Head and Neck Cancer through Big Data - SUPERTREAT”. This research was partially funded by Italian Ministry of Health “Ricerca Corrente” funds.
Author information
Authors and Affiliations
Contributions
Stefano Cavalieri (S.C.) and Lisa Licitra (L.L.) wrote the manuscript text. All authors (Loris De Cecco [L.D.C.], Dario Monzani [D.M.], Hisham Mehanna [H.M.], Renata Ferrarotto [R.F.], Christian Simon [C.S.], Robert Haddad [R.H.], Pierre Saintigny [P.S.], Christophe Le Tourneau [C.L.T.]) contributed to the text, reviewed and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
Stefano Cavalieri (S.C.) declares occasional fees for participation as a speaker at conferences/congresses from AccMed; support for attending meetings and/or travel from AccMed, MultiMed Engineers srl, Care Insight sas, unrelated to the content of this work. Lisa Licitra (L.L.) declares the following conflicts of interest: research funds donated directly to the institute for clinical trials from AstraZeneca, BMS, Boehringer Ingelheim, Celgene International, Eisai, Exelixis, Debiopharm International SA, Hoffmann-La Roche Ltd, IRX Therapeutics, Medpace, Merck-Serono, MSD, Novartis, Pfizer, Roche, and Buran; occasional fees for participation as a speaker at conferences/congresses or as a scientific consultant for advisory boards from AstraZeneca, Bayer, MSD, Merck-Serono, AccMed, Neutron Therapeutics, Inc., and Alentis. Pierre Saintigny declares the following conflicts of interest: research funds donated directly to the institute from Illumina, HTG Molecular Diagnostics, Roche, and BMS. The remaining authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cavalieri, S., De Cecco, L., Monzani, D. et al. Integrating transcriptomic data and artificial intelligence to personalize curative treatments for head and neck cancer patients. npj Precis. Onc. 10, 170 (2026). https://doi.org/10.1038/s41698-026-01369-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41698-026-01369-2
