
Abstract
Virtual reality (VR) interventions have emerged as innovative approaches increasingly used to manage attention-deficit/hyperactivity disorder (ADHD) in children and adolescents. This systematic review included 22 randomized controlled trials, quasi-experimental, and open-label studies published between 2001 and 2025, comprehensively evaluating the feasibility of VR interventions, their effectiveness alone or combined with pharmacological treatment, the relative efficacy of different training modalities, and dosage-related factors. The results indicate that VR interventions, whether used independently or alongside medication, significantly improve core ADHD symptoms, executive functions, emotional regulation, and social skills, with long-term interventions (≥8 weeks) producing more pronounced and sustained benefits. Among the training modalities, interactive game training was the most frequently studied, followed by virtual scenario and exergaming, each demonstrating distinct effects on cognitive and behavioral outcomes. Overall, VR interventions generally demonstrated high adherence rates; however, adherence reporting was inconsistent across studies, and adverse effects were typically mild and transient. Future research should focus on large-scale randomized controlled trials employing standardized outcome measures and developing personalized VR protocols to further enhance treatment efficacy and clinical applicability for ADHD.
Similar content being viewed by others

Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a neuro developmental condition involving persistent and developmentally atypical behaviors such as inattention, hyperactivity, and impulsivity that impair functioning across multiple settings1. Globally, this disorder affects approximately 7–8% of children and adolescents, with estimates varying by methodology and clinical criteria for diagnosis2,3. While some individuals experience symptom remission with age, many continue to exhibit impairing symptoms into adolescence and adulthood, contributing to lifelong functional challenges4. ADHD imposes a significant burden on families, schools, healthcare systems, and broader society, leading to increased risks of academic failure, social dysfunction, mental health comorbidities, substance misuse, and even justice system involvement5,6. Given its widespread prevalence and high social cost, early diagnosis and sustained intervention are critical7.
Current clinical guidelines advocate for multimodal treatment approaches, combining pharmacological and non-pharmacological interventions tailored to individual needs8. Stimulant medications such as methylphenidate are often used as a first-line option, particularly in moderate-to-severe cases, but concerns regarding side effects, adherence, and long-term efficacy have led to increasing attention on non-pharmacological interventions9,10. Among non-pharmacological interventions, behavioral therapy is a well-established evidence-based treatment for ADHD, with robust support for improving attention and executive function11. In contrast, cognitive training and exercise interventions are considered experimental or of limited efficacy12. However, all non-pharmacological interventions generally face challenges, such as low engagement, lack of personalization, and difficulty maintaining long-term motivation, which can limit their overall effectiveness13,14,15. Specifically, neurofeedback may produce certain improvements in attention and executive function16, whereas the efficacy of biofeedback is more variable and highly dependent on the specific context17. Cognitive training, such as working memory and attention training, shows limited or inconsistent effects, typically influenced by training intensity, task design, and participant engagement18.
With rapid technological advances, VR technology has attracted increasing attention in ADHD interventions due to its high immersion, ecological validity, and ability to simulate real-life environments19,20. VR can provide multisensory dynamic interactions that enhance children’s engagement and motivation while enabling personalized training tailored to individual needs, thereby improving intervention outcomes21,22.
In recent years, various types of VR-based interventions have been introduced in the field of ADHD rehabilitation. Early VR programs were primarily built upon simple cognitive paradigms such as the Continuous Performance Test (CPT), often integrated with electroencephalogram (EEG)-based neurofeedback systems23,24. For instance, a study demonstrated that participants receiving VR neurofeedback training showed notable improvements in attention and behavioral control24. Since 2019, researchers have increasingly incorporated task-oriented interactive games into VR platforms to enhance motivation and engagement among children. Later, the study confirmed that VR-based cognitive training through interactive gaming improved attentional performance in children with ADHD25. Similarly, researchers combined visual attention training and breathing regulation within a VR system and found enhancements not only in attentional performance but also in physiological indicators such as maximal inspiratory pressure (MIP)26. These multisensory and biofeedback-integrated systems represent a shift toward more comprehensive and holistic VR-based intervention models.
Given the differences in active components and mechanisms among VR interventions, this review categorizes them into three types: VR Interactive Game Training, focusing on cognitive tasks to enhance attention, executive function, and problem-solving, with reward mechanisms improving attentional deficits in ADHD children27; VR exergaming/body-motion training, combining physical movement and cognitive training to target motor-cognitive integration, inhibitory control, and coordination28; and VR Virtual Scenario Training, simulating real-life scenarios to improve emotional regulation and social functioning, addressing limitations of other VR types29. This classification reflects both core intervention components and differing mechanisms, providing a theoretical basis for comparing efficacy across VR modalities.
Despite the growing application of VR in ADHD treatment, there remains a lack of systematic classification and evaluation of the different types of VR interventions. The previous review emphasized the potential of electronic, virtual, and augmented reality games in enhancing cognitive and metacognitive functions among children with ADHD30. However, it did not provide a detailed categorization of VR modalities and primarily focused on general digital interventions. In addition, several meta-analyses have evaluated the efficacy of immersive VR-based motor and cognitive training in children with ADHD, indicating improvements in executive function and motor skills31,32,33. Nonetheless, these reviews often lacked refined classification regarding types of VR interventions, dosage parameters (e.g., duration and frequency), and intervention outcomes. Moreover, the limited number of randomized controlled trials (RCTs) included in existing syntheses weakens the generalizability and robustness of conclusions.
Given these limitations, the present systematic review aims to comprehensively evaluate current evidence on VR-based interventions for children and adolescents with ADHD, focusing on four key aspects: (1) The feasibility and acceptability of VR interventions, assessed through adherence rates, satisfaction levels among participants and therapists, and intervention settings; (2) Whether VR is applied as a standalone intervention or in conjunction with pharmacological treatment, and the differential outcomes observed in each case; (3) The comparative effectiveness of three major types of VR training—VR Interactive Game Training, VR Exergaming (body-motion-based training), and VR Virtual Scenario Training—on cognitive and behavioral outcomes; (4) Dosage-related variables, including intervention duration, frequency, and total exposure time, with specific attention to the distinction between short-term and long-term interventions (with a minimum duration of 8 weeks).
Results
Search results
Figure 1 illustrates the process of study identification, including the initial search, title and abstract screening, and final study selection. The study selection process followed the PRISMA 2020 guidelines. A total of 1649 records were initially identified through database and register searches. After removing 881 duplicate records, 768 unique records remained for title and abstract screening. Based on the screening results, 33 full-text articles were retrieved and assessed for eligibility. Among these, 13 reports were excluded for not meeting the inclusion criteria. In addition, a manual search through citation tracking identified two additional records, both of which met all eligibility criteria and were also included in the review. Ultimately, 22 studies were included in the final systematic review.

Flowchart of literature screening.
Study selection, characteristics, and participants
As presented in Table 1, this review included 22 studies, comprising 11 RCTs23,29,34,35,36,37,38,39,40,41,42, 8 quasi-experimental studies (including one within-group pre-post design)24,25,26,27,43,44,45,46, and 3 open-label experiments47,48,49. Most studies were conducted in South Korea (n = 7)23,24,25,26,36,40,44, Italy (n = 3)38,42,43, Germany (n = 2)39,47, Switzerland (n = 2)34,49, and China (n = 3)27,29,45, with additional studies originating from Portugal37, Spain41, Iran46, Israel48 and France35.
The publication years ranged from 2001 to 2025. Across these studies, a total of 896 participants were included. In child and adolescent studies, participants’ ages ranged from 5 to 18 years, whereas in adult studies, participants’ ages were reported in the range of 18–65 years. The majority were children and adolescents, with only four studies involving adult participants37,39,47,49. Participants were categorized into three groups: individuals formally diagnosed with ADHD (n = 652, 72.8%) according to DSM-IV, DSM-V, or ICD-1025,26,29,34,35,38,40,41,42,43,44,45,46,47,48,49; individuals exhibiting ADHD-related symptoms without a formal diagnosis (n = 218, 24.3%) identified via symptom checklists or behavioral observation23,24,36,37,39; and healthy controls (n = 26, 2.9%)25,47. All participants were cognitively and physically capable of engaging in VR-based training. Most interventions were conducted in clinical, laboratory, or educational settings, with some incorporating home-based or hybrid models.
Feasibility and acceptability
Participant dropout rates in VR-based interventions ranged from 0% to 23%. Thirteen studies reported adherence rates between 77% and 100%. Of the 13 studies reporting compliance, all but two demonstrated high adherence, with one study reporting 79%41 and another 77% adherence40, while all remaining studies exceeded 85%34,39,47,48, with 7 achieving 100%26,29,35,37,38,44,45. Five studies reported strategies to enhance adherence29,37,38,39,47. One study promoted competition among participants by setting up a leaderboard37. Other measures to improve adherence included reminder systems (phone calls or WhatsApp/WeChat messages) and incentive mechanisms such as token economies, lottery rewards (€2 × 50), or monetary compensation (€100) for completing all training sessions. Five studies reported strategies to enhance adherence, with adherence rates exceeding 95% in all five studies, and two studies29,38 achieving 100% adherence.
Ten studies assessed participant satisfaction. One study reported moderate satisfaction47, while another reported that participants’ satisfaction with the VR platform, assessed via a 9-item questionnaire, was generally high37. In another, the average interest score was 4.55 out of 544. One study noted that 82% of participants enjoyed the experience and 79% would recommend it41. One study reported a satisfaction rate of 82.5%48.
No serious adverse effects were reported. Mild side effects included: a sensation of “heaviness in the head” due to headset weight44; mild dizziness (mean score: 0.10/1), with 58% reporting increased dream activity41; mild simulator sickness47; and one withdrawal due to discomfort with the VR environment39.
Intervention settings
Of the 22 studies, 18 were conducted in laboratory or clinical settings; 1 used hybrid environments (home and hospital); 1 was implemented entirely at home; and 1 was school-based; and 1 was conducted exclusively in a hospital setting. Among the laboratory/clinical studies, improvements in attention, symptom severity, working memory, and cognitive function were consistently observed23,24,25,26,27,29,35,36,37,39,40,42,43,45,46,47,48,49. The home-based study enhanced inhibition and cognitive flexibility but showed no significant changes in parent-rated Conners-3 scores, although a significant improvement was observed on the DSM-IV-TR global index34. The school-based intervention showed significant gains in academic performance, with the VR group outperforming the traditional training group38. In hybrid settings, participants demonstrated significant improvements in attention and inhibition41. In hospital-based settings, sense of presence improved in the experimental group, whereas no significant EEG changes25.
Compliance was 90% in the only home-based study34. In the hybrid studies, one study reported a 79% compliance rate with a high dropout rate41. The school-based study achieved 100% compliance38. In clinical/laboratory settings, 8 studies did not report compliance23,24,25,27,36,42,43,46, while one reported a 77% compliance rate40, 9 studies achieved rates above 85%26,29,35,37,39,44,45,47,48.
VR interventions for children vs. adults with ADHD
VR interventions for children with ADHD demonstrated clear efficacy in RCTs. For example, one study combined VR serious games with hospital- and home-based practice, resulting in significant improvements in parent-rated SNAP-IV symptoms (inattention and hyperactivity/impulsivity) and objective neurocognitive measures (e.g., working memory and executive function), outperforming medication-only or psychoeducation interventions41. Similarly, significant reductions in parent-rated ADHD-RS total scores and Conners-3 hyperactivity/impulsivity subscales were reported35,42. Quasi-experimental studies further supported the potential of VR to improve children’s objective cognitive performance (e.g., error rates in attention tasks) as well as parent-reported symptoms44,45.
VR interventions for adults with ADHD typically target specific functional deficits, such as higher-order executive functions, working memory, and cognitive control in complex environments. Limited RCT evidence indicates that VR may effectively improve these core cognitive domains. VR interactive games significantly enhanced processing speed and spatial working memory in young adults37, while VR neurofeedback training reduced reaction time variability and increased prefrontal cortex activation39.
Active treatment components of VR interventions
Among the 22 included studies, 11 used cognitive training as the primary intervention, 4 employed neurofeedback, 3 combined cognitive training with behavioral interventions, 1 used biofeedback, and 3 focused solely on behavioral interventions. Standalone VR cognitive training was shown to improve attention, working memory, and hyperactivity/impulsivity symptoms, as measured by objective neuropsychological tests (e.g., CPT reaction time tasks) and parent-rated scales such as the SNAP-IV37,44. When VR cognitive training was combined with medication or behavioral therapy, it provided additional improvements in core ADHD symptoms, objective cognitive performance, and social skills29,41,42. VR neurofeedback demonstrated greater effects on attention and EEG β-wave activity compared to standard screen-based neurofeedback, likely due to increased immersion23,36. fNIRS-based VR neurofeedback was superior to EMG biofeedback alone in activating the prefrontal cortex and enhancing inhibitory control39. One study reported negative findings: a single session of VR neurofeedback did not improve performance and actually increased distractibility, highlighting the importance of intervention dosage and adaptability, as well as the value of objective physiological measures in detecting potential adverse effects47. VR exergaming or behavioral strategy-based interventions were also effective in improving parent-rated ADHD symptoms, inhibitory control, and motor abilities34.
VR as a standalone vs. combined intervention
Ten studies incorporated VR alongside traditional treatments, such as pharmacological, behavioral, or cognitive therapies. Among these, six studies directly compared VR + standard care with standard care alone. Across these studies, the combined approach consistently produced superior outcomes. Significant reductions in hyperactivity-impulsivity were reported using the parent-rated SNAP-IV42. Objective cognitive measures: Improvements were observed in CPT performance26, working memory41, and executive functions, including planning and problem-solving42,43. Greater improvements were reported in clinician-rated social skills and parent-rated executive functions29.
Ten studies implemented VR as a standalone intervention. Based on the different control group settings, these studies can be categorized into three main types for comparative analysis. Compared with the no-treatment control, three studies24,37,44 found significant improvements in processing speed, working memory37, and attention task performance, including reductions in omission and commission errors44. Compared to active control groups, two studies23,36 compared immersive VR training with identical cognitive training delivered on a traditional fixed screen, showing that immersive VR led to greater improvements in CPT performance. Only one of these studies observed accompanying increases in EEG β-wave activity23, suggesting enhanced neural modulation. One study46 reported superior improvements on the Wechsler Memory Scale for VR cognitive training compared to stimulant medication. Additionally, one study39 found that fNIRS-based VR neurofeedback outperformed EMG-based biofeedback in reducing Go/No-Go task errors and increasing prefrontal cortex oxygenation. Beyond comparisons with traditional interventions, two studies focused on optimizing the feedback mechanisms within VR systems. One study27 showed that reward-based VR cognitive–motor training improved ADHD symptoms and executive function more than non-reward training, and another47 found ADHD-specific VR neurofeedback revealed greater attentional instability and slower responses compared with healthy controls. A single-group study using VR-augmented treadmill training48 did not observe immediate improvements in attention indices but reported enhancements in executive function, memory, gait stability, and psychosocial behaviors, with some cognitive benefits maintained at the 6-week follow-up. Two studies did not report whether VR was implemented as a standalone intervention or combined with other treatments35,43.
Effectiveness across different types of VR-based training
(1) VR interactive game training (55%, 12 studies)
As shown in Fig. 2, VR Interactive Game Training integrates immersive gameplay with cognitive tasks and real-time feedback mechanisms to enhance attention, working memory, and executive functions. Most programs required participants to perform goal-directed tasks such as target tracking, response inhibition, or memory-based matching while navigating virtual environments. Some interventions included adaptive difficulty levels or reward-based reinforcement to maintain engagement. Training was typically administered in laboratory or clinical settings, with session durations ranging from 10 to 45 min, training sessions were conducted 1–4 times per week over a period of 1 week to 6 months, with one study implementing 2 sessions per day27. Several studies also implemented remote, home-based formats to improve accessibility and ecological validity41,44.

VR cogntive training for ADHD patients. a VR cognitive training center at Gil Hospital; (b) Samsung Medical Center; (c) Inha University Hospital25. Reprinted from Oh, S. H., Park, J. W., & Cho, S. J. (2022), Journal of Web Engineering, 21, 767–788. © 2022 The Authors. Licensed under CC BY 4.0.
Figure 2 further illustrates that VR-based cognitive training can be conducted in diverse settings, including (a) clinical institutions, (b) rehabilitation centers, and (c) research laboratories, indicating its flexibility and potential for broader application in ADHD treatment.
Interactive VR game training was the most frequently used modality (n = 12). These interventions consistently led to improvements in attention, inattention/hyperactivity symptoms, executive functioning, and problem-solving abilities. One study additionally reported neurophysiological changes, including enhanced beta wave activity23. Among these 12 studies, three employed a combination of interactive and exergaming elements. These hybrid interventions were more likely to report improvements in impulsivity and hyperactivity symptoms26,42,43.
(2) VR Exergaming (18%, 4 studies)
As shown in Fig. 3, VR Exergaming utilizes motion-sensing technology combined with movement-based games to promote both physical activity and cognitive enhancement. Participants are typically required to perform physical tasks such as jumping, arm swinging, or balancing, designed to simultaneously stimulate attention, executive function, and coordination. Training settings vary and include home, rehabilitation centers, and clinical institutions. Sessions last 30–60 min, conducted three times per week over a period of 4 weeks to 3 months.

Reprinted from Khundam and Nöel50, International Journal of Computer Games Technology, 2021, Article ID 6668280.© 2021 The Authors. Licensed under CC BY 4.0.
Four studies focused exclusively on VR-based exergaming, emphasizing physical engagement. These interventions effectively improved inhibitory control, cognitive flexibility, and motor coordination. One study also reported increased N2 amplitude and reduced reaction time in a go/no-go task following the intervention40. Another study reported cognitive improvements but no significant changes in parent-rated Conners-3 ADHD symptoms, although a significant effect was observed on the total global index score using DSM-IV-TR Symptom Scale T-scores34.
(3) VR virtual scenario training (27%, 6 studies)
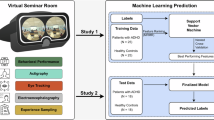
As shown in Fig. 4, VR Virtual Scenario Training simulates real-world environments such as classrooms and social settings to target improvements in social skills, emotion regulation, and attentional control. Participants engage in tasks like following classroom instructions, managing distractions, or practicing social interactions with virtual avatars. Some studies also incorporate neurofeedback tools to provide real-time monitoring of neural activity and enhance self-regulation. Training is typically conducted in settings including schools, rehabilitation centers, and laboratories. Including one study with a single training session and other studies with training conducted 2–4 times per week over a period of 2 weeks to 4 months.

A First-person view of the virtual seminar room showing the CPT on the front canvas; (B) Side view of a participant in the VR lab; (C) Distractor event; (D) Gaze-based feedback provision47. Reprinted from Selaskowski et al.47, BMC Psychiatry, 23(1), 74. © The Author(s) 2023. Licensed under CC BY 4.0.
Six studies utilized VR-based virtual scenario training. These interventions demonstrated beneficial effects on emotional regulation, social behavior, and sustained attention. Notably, two studies reported significant improvements in social skills and intrinsic motivation29,38.
The three main types of virtual reality (VR) training—interactive gaming, exergaming, and virtual scenario training—differ in content and duration, but all show good adherence and acceptance. Interactive gaming combines cognitive tasks with feedback, exergaming emphasizes physical movement, and virtual scenario training simulates real-life environments, often supplemented with neurofeedback. All three have minimal side effects and show great clinical potential. Figure 5 illustrates their characteristics and comparisons.

The figure categorizes three types of VR interventions, detailing their associated virtual modality, intervention characteristics, and feasibility for practice.
Dosage: duration, frequency, and total exposure
As presented in Table 2, the intervention duration ranged from 2 weeks to 6 months. Session length varied: five studies used 30-min sessions, seven used 10–25 min, and five used 30–60 min. Session frequency ranged from 1 to 4 times per week, with one study providing two sessions per day and another using a single-session intervention. Five studies did not report frequency.
Among the 22 included studies, six employed long-term interventions (defined as lasting at least 8 weeks)34,38,41,42,43,45. Of these, three studies reported improvements in core ADHD symptoms based on parent-rated scales such as SNAP-IV, ADHD-RS, and Conners-342,43,45. One study reported that the intervention group showed only a trend toward improvement on the inattention and hyperactivity-impulsivity subscales of the SNAP-IV41. One study found no significant changes on the parent-rated Conners-3, but reported improvements in inhibitory control, cognitive flexibility, and the DSM-IV-TR total global index score34. Another study observed a significant increase in accuracy on academic achievement tasks after the intervention38.
In contrast, among studies with interventions shorter than 8 weeks, three reported improvements in ADHD symptoms as assessed by parents or clinicians27,35,48. Although the remaining studies did not specifically report changes in core symptoms, significant improvements were observed in cognitive and attentional domains (e.g., CPT, working memory tasks) in the VR intervention groups.
Regarding session duration, five studies administered sessions longer than 30 min39,40,45,48,49. Improvements in parent-rated inattention and hyperactivity symptoms were reported in one study, and adherence rates exceeded 85% in three studies, while one study reported that five participants in the experimental group withdrew due to scheduling conflicts40; and another study did not report adherence49. Five studies employed 30-min sessions, of which two reported improvements in core ADHD symptoms based on parent or clinician ratings (ADHD-RS, SNAP-IV) and one observed no significant changes on the Conners-3 scale34,35,42. Additionally, seven studies used sessions of 10–25 min, with one reporting improvements in parent-rated SNAP-IV scores27.
Discussion
This systematic review evaluated the effectiveness and characteristics of VR-based interventions as non-pharmacological treatments for children and adolescents with ADHD. The included studies varied in design, setting, treatment goals, and VR formats. Despite generally small sample sizes and inconsistent methodological quality, the overall findings suggest that VR interventions are a feasible and promising adjunct or alternative treatment. Given the heterogeneity in study parameters and outcome measures, meta-analysis was not conducted, and the results should be interpreted with caution.
Overall, VR interventions demonstrated significant improvements in core ADHD symptoms, particularly attention deficits and hyperactivity/impulsivity, and outperformed no-intervention control groups. Notably, one study reported superior memory improvement in the VR group compared to the pharmacological treatment group46. Although few studies directly compared VR with pharmacological or psychological treatments, some evidence suggests that combining VR with traditional interventions may yield superior outcomes. For example, Kim et al. found that combined VR and standard treatment resulted in greater improvements in attention than traditional treatment alone26. Another study reported significant improvements were observed in working memory and executive functions with combined intervention41. These findings highlight that while VR interventions are independently effective, their integration with standard therapies may offer additional benefits. Future studies should explore the synergistic effects of VR when used alongside conventional treatments such as medication or cognitive behavioral therapy. Moreover, identifying subgroups—based on age, symptom presentation, or functional needs—that may benefit most from VR or combined interventions is essential for individualized treatment. As VR technology becomes more accessible, developing multimodal, scalable, and cost-effective VR protocols may play an increasingly vital role in comprehensive ADHD management strategies.
Among the three major types of VR interventions, interactive game-based training was the most commonly employed and yielded the most consistent results, improving attention, executive function, and problem-solving skills. Some studies also reported neurophysiological improvements (e.g., enhanced beta wave activity), suggesting potential brain-level changes23. In contrast, while exergaming benefited cognitive flexibility and motor control, its effects on attentional deficits were less stable34. Virtual scenario-based interventions showed promising outcomes in emotional regulation and social functioning, complementing the limitations of other VR training types29. Notably, hybrid training approaches demonstrated superior efficacy in reducing hyperactivity and impulsivity symptoms42,43. These findings suggest that interactive game-based VR is best suited for improving attention and executive functions, exergaming may enhance motor-cognitive integration and inhibitory control, while virtual scenario training is more appropriate for emotional and social skill enhancement. Tailoring the intervention type based on specific treatment goals may optimize outcomes.
Participants in the VR intervention groups generally reported high satisfaction. The overall feasibility and acceptability of VR interventions were favorable. Among the 13 studies reporting compliance, adherence was generally high, with most exceeding 85% and seven studies achieving 100%. Low dropout rates and high engagement indicate that VR interventions are well-received among children and adolescents with ADHD. This is likely attributable to the immersive, interactive, and gamified nature of VR, which enhances user motivation and engagement41. Qualitative data further support this, with participants describing the experience as enjoyable, challenging, and helpful in improving focus and emotional regulation37,43,44. Visual feedback and instant rewards embedded in VR may also play a key role in promoting behavior change and sustaining participation. These findings highlight VR’s dual strengths in therapeutic efficacy and user experience, making it a practical and engaging intervention modality.
The reporting of adherence plays a critical role in interpreting intervention outcomes. Studies that reported adherence demonstrated significant improvements across multiple domains, including cognitive, behavioral, and even neurophysiological measures, accompanied by high completion rates and participant satisfaction. Such comprehensive reporting enhances the credibility and feasibility of the interventions. In contrast, studies that did not report adherence mainly documented effects at the cognitive and behavioral level, such as CPT performance, memory, and auditory attention and impulsivity. Although positive outcomes were reported, the lack of information on participants’ actual engagement introduces uncertainty in interpreting the results. The lack of adherence data makes it unclear whether non-significant findings, such as the absence of EEG changes, reflect true intervention inefficacy or insufficient participant engagement25. Overall, consistent and detailed reporting of adherence is essential for accurately interpreting and comparing the effects of VR-based interventions for ADHD.
Regarding adverse effects, the included VR intervention studies generally reported no serious adverse reactions. A few studies mentioned mild side effects, mainly including a sensation of “heaviness in the head” caused by the weight of the head-mounted device44, mild dizziness (mean score 0.10/1) and increased dream activity reported by 58% of participants41, mild simulator sickness47, and one withdrawal due to discomfort with the VR environment39. These mild discomforts were generally transient and acceptable, not affecting overall adherence. Overall positive participant feedback suggests that VR interventions are safe and acceptable. Future studies should focus on technological improvements to reduce these mild adverse effects, further enhancing the comfort and user experience of VR interventions.
VR interventions show potential for both children and adults with ADHD, but their effects vary by age. In children, VR interventions combined with adult-supported behavioral strategies can improve parent-rated ADHD symptoms and objective cognitive measures35,41,42,45. In adults, VR primarily targets individual cognitive deficits, enhancing processing speed, working memory, and prefrontal cortex activation, with effects arising from direct interaction with VR tasks37,39. These findings highlight the importance of designing VR interventions tailored to different age groups and suggest that future research should explore combined intervention approaches and the transfer of VR training effects to real-world settings.
In terms of setting, most studies were conducted in clinical environments, which provide standardized implementation and higher adherence. However, the feasibility of delivering VR interventions in home settings has gained increasing attention, especially for individuals with limited access to clinical facilities. For instance, in a home-only intervention, participants completed approximately 80 min of training per week, corresponding to around 89% of the planned training time34. Future research should explore the scalability of home-based VR interventions, including the development of user-friendly platforms, remote monitoring tools, and technical support systems. Comparative studies assessing the effectiveness and adherence of VR interventions in clinical versus home environments are also warranted. With ongoing advances in VR technology, optimizing its application across diverse settings will be key to improving accessibility and sustained engagement in ADHD care.
Regarding dosage, long-term interventions (≥8 weeks) were associated with more significant and lasting improvements in attention and executive functions42,43. One 6-month program led to improvements in hyperactivity/impulsivity, learning difficulties, family relationships, and both visual and auditory attention42. In contrast, single-session interventions were generally ineffective47. These findings underscore the importance of sufficient intervention duration and frequency in achieving therapeutic benefits.
VR interventions have demonstrated reliable near-transfer effects in children and adolescents with ADHD, with most studies reporting significant improvements on laboratory-based cognitive tasks (e.g., CPT, ATA, working memory, and executive function tests) and neurophysiological measures (EEG, fNIRS)23,24,36,37,39,44. Evidence for far-transfer effects is limited, although some studies have shown improvements in core symptoms based on parent-rated scales27,35 and preliminary enhancements in social skills and motor functions29,48. In addition, one study reported that VR interventions could achieve classroom learning transfer, with the experimental group showing significantly higher accuracy on a history knowledge test and greater intrinsic motivation and engagement compared to the control group38. In addition, one study reported that VR interventions could enhance learning motivation and efficiency49.Overall, while VR interventions clearly improve cognitive performance in laboratory settings, evidence for far-transfer effects in daily life, school, and social functioning remains limited, highlighting the need for more objective assessments and long-term studies.
Although most studies report positive effects of VR interventions in children and adolescents with ADHD, some null findings reveal limitations. One study found no improvement in core symptoms on the parent-rated Conners-3 scale34, and another reported only a trend toward improvement on the SNAP-IV inattention and hyperactivity-impulsivity subscales41. Cognitive improvements were inconsistent across studies, with some studies found no significant changes in attention or executive function measures41,43,48. Neurophysiological results also conflicted, with one study showing no EEG changes25 and another reporting increased β-wave activity23. One study highlighted potential negative effects, including more omission errors, slower reaction times, and increased distraction after VR training47. These findings suggest that VR effects may depend on participant characteristics, task type, intervention dosage, and individual sensitivity.
Despite the promising findings, several limitations should be acknowledged. First, although 22 studies were included, many had small sample sizes and varying study designs—including RCTs, quasi-experimental studies, and pilot experiments—limiting the generalizability and consistency of results. Second, the diversity in VR intervention formats, dosage, settings, and outcome assessments hindered quantitative synthesis, reducing the ability to draw definitive conclusions about intervention efficacy. Third, reporting of critical feasibility outcomes such as adherence, satisfaction, and adverse effects lacked standardization in many studies, impeding a comprehensive evaluation of intervention safety and usability. Fourth, only English-language publications were included, introducing potential language and publication bias and possibly omitting relevant studies from non-English databases. Additionally, some studies excluded participants with comorbid psychiatric conditions, limiting the applicability of findings to the broader, more heterogeneous clinical population. The cost of VR equipment and related technologies is relatively high, especially in developing countries, which may limit the accessibility of interventions and exacerbate treatment inequalities. Therefore, when implementing VR interventions, cost-effectiveness should be considered, and low-cost or shared solutions should be explored to improve accessibility. Future research should prioritize large-scale, high-quality RCTs with standardized protocols to clarify the comparative advantages of different VR modalities and identify optimal target populations.
Further investigations should aim to establish standardized VR intervention protocols and core outcome sets, incorporate both observer- and self-rated measures aligned with DSM criteria, and assess broader functional domains such as emotional well-being and quality of life. Large, rigorously designed trials are needed to compare VR directly with pharmacological treatments and elucidate underlying mechanisms of action, including neurocognitive, behavioral, and motivational pathways. The selection of VR intervention types should be tailored to treatment goals: interactive games for cognitive enhancement, exergaming for motor-executive integration, and scenario-based VR for emotional and social difficulties. Personalized VR intervention strategies based on ADHD subtypes or symptom profiles represent a promising direction for future development.
In summary, this systematic review indicates that VR interventions represent a promising non-pharmacological approach for treating children and adolescents with ADHD. These interventions are effective in improving core symptoms such as attention deficits, hyperactivity/impulsivity, executive function, emotional regulation, and social skills. The reviewed VR formats—interactive gaming, exergaming, and scenario-based training—are applicable across clinical and home settings, with high adherence and user acceptance and minimal adverse effects. Some evidence also points to neurophysiological benefits (e.g., improved EEG patterns), though further research is needed to clarify the underlying mechanisms. Future studies should employ larger sample sizes, standardized outcome measures, and rigorous RCT designs to validate both the independent and adjunctive effects of VR interventions. Moreover, expanding VR accessibility through optimized hardware (e.g., head-mounted displays) and tailoring interventions to age, symptom type, and functional needs may enhance their effectiveness and practical utility.
Methods
Search Strategy and Study Identification
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was conducted in October 2025 across six electronic databases: PubMed, Web of Science, Scopus, Embase, MEDLINE, and PsycINFO. The final search was performed on October 10, 2025. The search included peer-reviewed studies published in English from the earliest available date of each database. Keywords and their related terms for ADHD, VR, and intervention were combined using Boolean operators (see Supplementary Table 1). Titles and abstracts were independently screened by two reviewers to exclude studies that clearly did not meet inclusion criteria. Full texts of potentially eligible studies were further reviewed independently. Disagreements were resolved through discussion. To ensure comprehensive coverage, reference lists of included studies and relevant systematic reviews were also manually screened. The results of the initial screening and full-text review are shown in Fig. 1. A total of 1649 records were identified. After screening and eligibility assessment, 22 studies were finally included in the review, including two identified through manual searching.
Eligibility criteria
Eligible studies included participants diagnosed with ADHD or hyperkinetic disorder according to established diagnostic criteria (e.g., DSM-IV, DSM-5, or ICD-10), or individuals exhibiting clinically relevant ADHD symptoms. Participants of all ages were included, encompassing children, adolescents, and adults, with clear reporting of participant ages. Studies utilized VR-based non-pharmacological interventions aimed at improving behavioral, cognitive, executive, or motor outcomes.
All studies were required to employ RCTs, quasi-experimental designs, or open-label trials. Control conditions included waiting list, treatment as usual (TAU), pharmacological intervention, placebo, or alternative non-pharmacological interventions. To comprehensively evaluate the intervention effects, single-group studies or case studies without a control group were also included, provided that pre- and post-intervention assessment data were reported.
Studies were excluded if the primary intervention involved pharmacological treatment, dietary supplementation, or homeopathy. Studies combining VR with pharmacological or psychological treatments were included only if the VR component was clearly described and aligned with the objectives of this review. Studies not published in English or those reporting only neurophysiological or neurobiological outcomes without behavioral or functional assessments were also excluded.
Data extraction and synthesis
Data were extracted using Microsoft Excel as the platform to systematically organize and record relevant information from all included studies. Data were extracted using a standardized form covering key study details such as authorship, year, country, sample size, participant age, sex, diagnosis, study design, VR intervention type, duration, frequency, setting, control conditions, and primary outcomes (attention, core ADHD symptoms, working memory, and other neuropsychological measures). Two independent reviewers extracted all data. Discrepancies were resolved through discussion, and if necessary, a third reviewer adjudicated. All extracted data were cross-checked to ensure accuracy and minimize inter-rater bias. Due to variability in interventions and outcomes, a narrative synthesis was conducted. Risk of bias for all included studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal checklists appropriate for each study design. Key domains evaluated included study design, sampling methods, measurement of outcomes, statistical analysis, and reporting. Two independent reviewers (Yujie Cao and Leilei Ma) performed the assessment, and any discrepancies were resolved through discussion; if consensus could not be reached, a third reviewer adjudicated. The results of the assessment are presented in Supplementary Tables 2 and 3. This process ensured a systematic evaluation of methodological quality and enhanced the transparency and rigor of the review.
Data availability
All data analyzed in this study are included in this article and its supplementary information files.
References
American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Publishing, 2013).
Ayano, G., Demelash, S., Gizachew, Y., Tsegay, L. & Alati, R. The global prevalence of attention deficit hyperactivity disorder in children and adolescents: an umbrella review of meta-analyses. J. Affect Disorders 339, 860 (2023).
Thomas, R., Sanders, S., Doust, J., Beller, E. & Glasziou, P. Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. PLOS ONE 10, e0117297 (2015).
Barkley, R. A., Fischer, M., Smallish, L. & Fletcher, L. The persistence of attention-deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder. J. Abnorm. Psychol. 111, 279 (2002).
Doshi, J. A. et al. Economic impact of childhood and adult attention-deficit/hyperactivity disorder in the United States. J. Am. Acad. Child Adolesc. Psychiatry 51, 990 (2012).
Pelham, W. E., Foster, E. M. & Robb, J. A. The economic impact of attention-deficit/hyperactivity disorder in children and adolescents. J. Pediatr. Psychol. 32, 711 (2007).
Faraone, S. V., Biederman, J. & Mick, E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol. Med. 36, 159 (2006).
Subcommittee On Attention-Deficit Hyperactivity Disorder, S. C. O. Q., ADHD: clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 128, 1007 (2011).
Sibley, M. H. et al. Variable patterns of remission from ADHD in the multimodal treatment study of ADHD. Am. J. Psychiatry 179, 142 (2022).
Sonuga-Barke, E. J. et al. Nonpharmacological interventions for ADHD: systematic review and meta-analyses of randomized controlled trials of dietary and psychological treatments. Am. J. Psychiatry 170, 275 (2013).
Evans, S. W., Owens, J. S., Wymbs, B. T. & Ray, A. R. Evidence-based psychosocial treatments for children and adolescents with attention deficit/hyperactivity disorder. J. Clin. Child Adolesc. Psychiatry 47, 157 (2018).
Pelham, W., Wheeler, T. & Chronis-Tuscano, A. Empirically supported treatments for attention deficit hyperactivity disorder. J. Clin. Child Psychol. 27, 190 (1998).
Cortese, S. et al. Cognitive training for attention-deficit/hyperactivity disorder: meta-analysis of clinical and neuropsychological outcomes from randomized controlled trials. J. Am. Acad. Child Adolesc. Psychiatry 54, 164–174 (2015).
Attention deficit hyperactivity disorder: diagnosis and management. National Institute for Health and Care Excellence (NICE) (2019).
Nimmo-Smith, V. et al. Non-pharmacological interventions for adult ADHD: a systematic review. Psychol. Med. 50, 1 (2020).
Zhong, X., Yuan, X., Dai, Y., Zhang, X. & Jiang, C. Neurofeedback training for executive function in ADHD children: a systematic review and meta-analysis. Sci. Rep. 15, 28148 (2025).
Groeneveld, K. et al. Z-score neurofeedback and heart rate variability training for adults and children with symptoms of attention-deficit/hyperactivity disorder: a retrospective study. Appl. psychophysiol. Biofeedback 44, 291–308 (2019).
Veloso, A., Vicente, S. G. & Filipe, M. G. Effectiveness of cognitive training for school-aged children and adolescents with attention deficit/hyperactivity disorder: a systematic review. Front. Psychol. 10, 2019 (2020).
Babu, A. & Joseph, A. P. Integrating virtual reality into ADHD therapy: advancing clinical evidence and implementation strategies. Front. Psychiatry. 16, 1591504 (2025).
Corrigan, N., Păsărelu, C. R. & Voinescu, A. Immersive virtual reality for improving cognitive deficits in children with ADHD: a systematic review and meta-analysis. Virtual Real 27, 3545 (2023).
Barba, M. C. et al. Augmented reality, virtual reality, and computer graphics, pt I. In Proc. 6th International Conference on Augmented Reality, Virtual Reality and Computer Graphics (SALENTO AVR) (eds Tommaso De Paolis, L. & Bourdot, P.) Vol. 11613, 394 (Springer, 2019).
Rodrigo-Yanguas, M. et al. A virtual reality game (The Secret Trail of Moon) for treating attention-deficit/hyperactivity disorder: development and usability study. JMIR Serious games 9, e26824 (2021).
Cho, B. H. et al. Neurofeedback training with virtual reality for inattention and impulsiveness. Cyberpsychol. Behav. 7, 519 (2004).
Lee, J. M. et al. A study on the system for treatment of ADHD using virtual reality. In 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vol. 4, 3754–3757 (IEEE, 2001).
Oh, S. H., Park, J. W. & Cho, S. J. Effectiveness of the VR cognitive training for symptom relief in patients with ADHD. J. Web Eng. 21, 767 (2022).
Kim, J., Hong, S., Song, M. & Kim, K. Visual attention and pulmonary VR training system for children with attention deficit hyperactivity disorder. IEEE Access 12, 53739 (2024).
Fang, H. et al. Reward feedback mechanism in virtual reality serious games in interventions for children with attention deficits: pre- and posttest experimental control group study. JMIR Serious Games 13, e67338 (2025).
Sarai, G., Jayaraman, P. P., Tirosh, O. & Wickramasinghe, N. Exploring virtual reality and exercise simulator interventions in patients with attention deficit hyperactivity disorder: comprehensive literature review. JMIR Serious Games 13, e57297 (2025).
Wong, K. P. et al. Empowering social growth through virtual reality–based intervention for children with attention-deficit/hyperactivity disorder: 3-arm randomized controlled trial. JMIR Serious Games 12, e58963 (2024).
Doulou, A. & Drigas, A. Electronic, VR & augmented reality games for intervention in ADHD. Tech. Soc. Sci. J. 28, 159 (2022).
Romero-Ayuso, D. et al. Effectiveness of virtual reality-based interventions for children and adolescents with ADHD: a systematic review and meta-analysis. Children 8, 70 (2021).
Yu, C., Wang, C., Xie, Q. & Wang, C. Effect of virtual reality technology on attention and motor ability in children with attention-deficit/hyperactivity disorder: systematic review and meta-analysis. JMIR Serious Games 12, e56918 (2024).
Zhang, W., Li, H. & Sheng, Y. A study of the effects of virtual reality-based sports games on improving executive and cognitive functions in minors with ADHD—A meta-analysis of randomized controlled trials. Behav. Sci. 14, 1141 (2024).
Benzing, V. & Schmidt, M. The effect of exergaming on executive functions in children with ADHD: a randomized clinical trial. Scand. J. Med. Sci. Sports 29, 1243 (2019).
Bioulac, S. et al. Virtual remediation versus methylphenidate to improve distractibility in children with ADHD: a controlled randomized clinical trial study. J Atten. Disord. 24, 326 (2018).
Cho, B. H. et al. The effect of virtual reality cognitive training for attention enhancement. Cyberpsychol. Behav. 5, 129 (2002).
Cunha, F. et al. The effect of a virtual reality based intervention on processing speed and working memory in individuals with ADHD—A pilot-study. Front. Virtual Real. 4, 2023 (2023).
Frolli, A., Ricci, M. C., Di Carmine, F. & Rega, A. Using virtual reality to improve learning in children with ADHD. Curr. Pediatr. Res. 26, 1244 (2022).
Hudak, J. et al. Near-infrared spectroscopy-based frontal lobe neurofeedback integrated in virtual reality modulates brain and behavior in highly impulsive adults. Front. Hum. Neurosci. 11, 425 (2017).
Ji, H. et al. The effects of exergaming on attention in children with attention deficit/hyperactivity disorder: randomized controlled trial. JMIR Serious Games 11, e40438 (2023).
Martin-Moratinos, M. et al. Effectiveness of a virtual reality serious video game (The Secret Trail of Moon) for emotional regulation in children with attention-deficit/hyperactivity disorder: randomized clinical trial. JMIR Serious Games 13, e59124 (2025).
Schena, A. et al. IAmHero: preliminary findings of an experimental study to evaluate the statistical significance of an intervention for ADHD conducted through the use of serious games in virtual reality. Int. J. Env. Res. Public Health 20, 3414 (2023).
De Luca, V. et al. Serious games for the treatment of children with ADHD: the BRAVO Project. Inform. Syst. Front. 27, 841–863 (2024).
Kim, S. et al. Eye-contact game using mixed reality for the treatment of children with attention deficit hyperactivity disorder. IEEE ACCESS 8, 45996–46006 (2020).
Ou, Y. et al. Development of virtual reality rehabilitation games for children with attention-deficit hyperactivity disorder. J. Ambient Intel. Humaniz. Comput. 11, 5713 (2020).
Tabrizi, M., Manshaee, G., Ghamarani, A. & Rasti, J. Comparison of the effectiveness of virtual reality with medication on the memory of attention deficit hyperactivity disorder students. Int. Arch. Health Sci. 7, 37 (2020).
Selaskowski, B. et al. Gaze-based attention refocusing training in virtual reality for adult attention-deficit/hyperactivity disorder. BMC Psychiatry 23, 74 (2023).
Shema, S. et al. Virtual reality training to enhance behavior and cognitive function among children with attention-deficit/hyperactivity disorder: brief report. Dev. Neurorehabil. 22, 1 (2018).
Cuber, I. et al. Examining the use of VR as a study aid for university students with ADHD. In Proc. 2024 CHI Conference on Human Factors in Computing Systems 65 (ACM, 2024).
Khundam, C. & Nöel, F. A study of physical fitness and enjoyment on virtual running for exergames. Int. J. Comput. Games Technol. 2021, 6668280 (2021).
Acknowledgements
This study was supported by the Brain Science and Brain-like Intelligence Technology-National Science and Technology Major Project (2021ZD0200500), the National Natural Science Foundation of China (32200873), the China Postdoctoral Science Foundation Fellowship (2022M720487), and the Fundamental Research Funds for the Central Universities (2022NTST13).
Author information
Authors and Affiliations
Contributions
Yanpei Wang conceived and designed the study; Yujie Cao carried out the literature analysis and the writing of manuscripts under the supervision of Yanpei Wang. Yujie Cao and Leilei Ma accessed and verified the study data, developed the analysis plan, and performed the statistical analyses under the supervision of Yanpei Wang. Yujie Cao, Leilei Ma, Ningyu Liu, Jiali Wang, Charlotte Walton, and Yanpei Wang amended and proofread the draft of the paper. All authors reviewed and commented on the study and manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cao, Y., Ma, L., Liu, N. et al. Virtual reality interventions for attention deficit/hyperactivity disorder: a systematic review. npj Digit. Med. 9, 303 (2026). https://doi.org/10.1038/s41746-026-02505-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41746-026-02505-9
