
Abstract
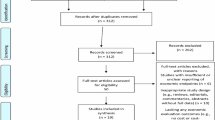
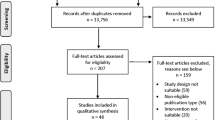
Artificial intelligence (AI) is progressively utilized in cardiology; nonetheless, the overarching advantages across various care domains remain ambiguous. We conducted a search of PubMed, Embase, CINAHL, and trial registries for randomized controlled trials up to January 16, 2026, assessing prospectively applied interventions based on machine/deep-learning algorithms while excluding rule-based systems. Endpoints were categorized according to NICE evidence tiers: workflow efficiency (Tier A), patient engagement/health promotion (Tier B), and clinical outcomes (Tier C). The risk of bias was evaluated using RoB 2.0. In 32 randomized controlled trials (27 of which were meta-analyzed), artificial intelligence improved all levels. Tier A: workflow time reduced (SMD − 0.71; 95% CI − 1.04 to −0.39), corresponding to a diagnostic time that is 30–120 s shorter and a decrease of 1.0–4.2 hospital days in trials reporting length of stay. Tier B: Behavioral nudging enhanced medication adherence (RR 1.59; 95% CI 1.01–2.50; NNT = 12). Tier C: decision-support implementations decreased all-cause mortality (RR 0.84; 95% CI 0.75–0.94; I² = 8%; NNT = 32). Limitations encompassed restricted blinding and insufficient sham-AI controls. Data-driven clinical AI yields quantifiable efficiency improvements, enhances engagement, and reduces adverse outcomes when integrated with actionable decision support, hence informing a structured framework for governance and implementation.
Similar content being viewed by others
Acknowledgements
We express our gratitude for the administrative support provided by Miss Ming-Hsuan Chang from the AI Impact Research Center at Taipei Veterans General Hospital. Funding sources include grants from Taipei Veterans General Hospital (VN115-11, V115E-004-1) and the Ministry of Health and Welfare, Taiwan (MOHW113-IM-I-212-000013-16, MOHW114-IM-1-212-000004-5, MOHW114-58070-03-1-2). The funding source had no role in the design, data collection, analysis, interpretation, or writing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
S.-J.W. reports grants/contracts from Eli Lilly Taiwan, Novartis, and Orient Europharma; consulting fees from AbbVie, Eli Lilly Taiwan, Percept Co., and Pfizer; and honoraria from AbbVie, Biogen, Eli Lilly, Hava Biopharma, and Pfizer. All other authors declare no competing financial or non-financial interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lin, YE., Yang, SM., Huang, CJ. et al. Impact of artificial intelligence on cardiovascular workflow, engagement, and outcomes: a systematic review. npj Digit. Med. (2026). https://doi.org/10.1038/s41746-026-02690-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41746-026-02690-7
