
Abstract
Amyotrophic Lateral Sclerosis (ALS) is a progressive neurodegenerative disease that predominantly targets the motor system. Spread of pathology is thought to be driven by both local vulnerability and network architecture. Namely, molecular and cellular features may confer vulnerability to specific neuronal populations, while synaptic contacts may also increase exposure to pathology in connected neuronal populations. However, these principles are typically studied in isolation and it remains unknown how local vulnerability and network spreading interact to shape cortical atrophy. Here, we investigate how network structure and local biological features shape the spatial patterning of atrophy in ALS. We analyze the Canadian ALS Neuroimaging Consortium (CALSNIC) dataset and estimate cortical atrophy using deformation based morphometry (DBM). The course of atrophy closely aligns with structural connectivity. Atrophy is also more likely to occur in regions that share similar metabolic profiles. Disease epicenters are located in motor cortex. Epicenter probability maps show transcriptomic enrichment for biological processes involved in mitochondrial function as well as support cells, including endothelial cells and pericytes. Finally, individual differences in epicenter location correspond to individual differences in clinical and cognitive symptoms and differentiate patient subtypes.

Similar content being viewed by others


INTRODUCTION
Amyotrophic Lateral Sclerosis (ALS) is a terminal neurodegenerative disease associated with progressive impairment of motor functions1. Expected survival of most patients diagnosed with ALS is 2–5 years after onset2,3. The disease shows significant heterogeneity across individuals, and patients can be classified into subtypes based on multiple features, including the familial or sporadic occurrence of the disease, age of disease onset, symmetry of motor neuron involvement, and initial symptom location4. Most ALS patients experience a progression of symptom severity, which reflects ALS pathology spread in the central nervous system.
Most modern accounts of ALS revolve around two non-exclusive notions. The first is network spreading: that the spread of pathology, likely in the form of pathogenic misfolded proteins (e.g., TDP-43)5,6, occurs via synaptic contacts7,8,9,10,11,12,13,14,15. Here, initial infiltration via the corticospinal tract introduces pathogenic proteins in primary motor cortex, leading to progressive cell death and atrophy. This notion is supported by the existence of stereotypical patterns of pathology progression and the presence of pathology in regions that are topographically distant yet interconnected through the corticospinal tract14. The second notion is that of local vulnerability: that molecular and morphological features of specific cells predispose them to the disease16,17. Namely, the involvement of support cells has been noted in ALS, including astrocytes and pericytes, implicating energy homeostatic and vascular mechanisms. Here local atrophy leads to patterned deafferentation18,19,20,21,22. Importantly, the two perspectives may both be true; namely, pathology may spread via synaptic contacts, but the spread may be amplified in vulnerable neuronal populations, effectively guiding the network spread of atrophy.
What are the principles that shape the spatial patterning of atrophy in ALS? Here we address this question using the Canadian ALS Neuroimaging Consortium (CALSNIC) dataset (http://calsnic.org)23. We first establish that cortical atrophy reflects white matter architecture. We also assess the extent to which the spread of atrophy between brain regions depends on their molecular and cellular similarity, including transcriptomic similarity, neurotransmitter receptor similarity, metabolic similarity, and hemodynamic similarity. We then use methods from epidemiology to identify network epicenters of the disease process in the cortex. We show that cortical epicenters of atrophy co-localize with markers of metabolic and mitochondrial function. Finally, we show that individual differences in epicenter location can distinguish subtypes of patients (bulbar- versus spinal-onset) and correlate with clinical and cognitive function.
RESULTS
Data was derived from the CALSNIC repository23, and comprised N = 192 patients and N = 175 healthy control participants. Atrophy was estimated using deformation based morphometry (DBM), a morphometric technique that has previously been shown to be sensitive to tissue loss in both deep and superficial structures24, and across multiple neurodegenerative syndromes25,26,27,28,29. For details on demographic information, data acquisition and preprocessing, see “Methods”, Tables S1, and S2.
Spatial distribution of atrophy
We initially identify differences between the ALS patients and healthy controls. Figure 1a shows the group-average atrophy map. Throughout the manuscript, we use sign-inverted w-scores such that greater values correspond to greater atrophy: a w-score is a morphometric measure of atrophy that is corrected for differences in age, sex and imaging site. Consistent with previous reports, the map highlights pronounced atrophy throughout the brain, including both grey matter (cortex and subcortex) and white matter27,30,31,32,33,34. In Fig. 1a, negative inverted w-scores (originally positive w-scores) are not shown, these areas represent regions of enlargement and are mainly located in the ventricular and sulcal regions. For more detailed statistical comparisons between ALS patients and controls, refer to ref. 27.

a Sagittal, coronal, and axial views of mean atrophy across individuals with ALS. Atrophy is estimated as the group-average w-score across individuals with ALS. The map is thresholded to exclude voxels with atrophy values smaller than 0. Data is displayed on a T2-weighted MNI template (MNI152-NonLinear2009cSym, 1 × 1 × 1 mm; P = 118, C = 117, A = 87). b Sagittal, coronal, and axial views of white matter tract parcels colored by mean atrophy. White matter tracts are defined based on the JHU white matter tractography atlas (thresholded at 25% probability)35,36. Significant atrophy is observed in bilateral corticospinal tracts (FDR corrected; left: p = 8.83 × 10−16, t-statistic = 9.62; right: p = 4.13 × 10−16, t-statistic = 9.84), anterior thalamocortical tracts (FDR corrected; left: p = 6.53 × 10−8, t-statistic = 6.44; right: p = 2.04 × 10−5, t-statistic = 5.26) and superior longitudinal fasciculus-posterior limb tracts (FDR corrected; left: p = 7.39 × 10−4, t-statistic = 4.34; right: p = 1.68 × 10−4, t-statistic = 4.75). c Cortical atrophy map parcellated based on volume-based Schaefer-400 parcellation44; maps are displayed on fs-LR inflated cortical surfaces. d Mean atrophy is calculated within each of the cytoarchitectonic classes defined by Von Economo45,46,47. The Von Economo classes are depicted in Fig. S1. Statistical significance is estimated using a spatial autocorrelation-preserving spin test (1000 repetitions). Black borders shown on the fs-LR flat cortical surface correspond to the primary motor cortex borders defined by Von Economo cytoarchitectonic parcellation45,46,47.
Given that most cortical atrophy is concentrated in primary motor cortex, we implement an initial sanity check: whether atrophy can correspondingly be observed in the corticospinal tract. We segment the voxel-wise atrophy map using the Johns Hopkins University (JHU) white matter tractography atlas35,36 (Fig. 1b). Analysis of white-matter tracts reveals significant involvement of bilateral corticospinal tracts, bilateral anterior thalamic radiation, and bilateral superior longitudinal fasciculus bundles (p < 0.05, False Discovery Rate (FDR) corrected; Fig. 1b). These projections have previously been associated with ALS and suggest that cortical atrophy is related to white matter atrophy37,37,38,39,40,41, consistent with the notion that neurodegenerative disease pathology affects not only the cell bodies (grey matter) but also axonal projections (white matter)42,43. In the subsequent analyses, we directly assess the relationship between local grey matter atrophy and network connectivity.
To cross-reference the atrophy map with network connectivity data, we apply a high-resolution functional parcellation, subdividing the atrophy map into 400 parcels according to the Schaefer atlas44 (Fig. 1c). The 400-parcel resolution is chosen because it divides the somatomotor cortex into fine parcels that align with body representation. In the cortex, the most pronounced atrophy is observed near the pre-central gyrus, a hub for motor function. Atrophy also extends into the temporal and frontal cortices (Fig. 1c). To test whether the disease selectively targets primary motor cortical neurons, we compute mean atrophy in each of the canonical cytoarchitectural classes according to the histological Von Economo atlas45,46,47 (Fig. S1). We observe significant enrichment of atrophy in the primary motor cytoarchitectonic class (FDR corrected; pspin = 6.99 × 10−3; Fig. 1d). Collectively, these results suggest that the present morphometric approach is sensitive to the pathophysiology of ALS.
Structural connectivity shapes cortical atrophy
We next assess the extent to which the spatial patterning of atrophy is related to structural connectivity. We compute the correlation between a node’s atrophy value and the mean atrophy of its structurally connected neighbours, weighted by streamline density estimated using diffusion MRI. In this context, neighbours of a node are those that share a direct physical connection with the node of interest (Fig. 2a). To ensure that connectivity estimates reflect the healthy connectome prior to disease onset and deafferentation, we estimated structural connectivity in a sample of N = 327 unrelated healthy young adults from the Human Connectome Project (HCP-S90048). Figure 2a shows a positive correlation between the two (Pearson correlation coefficient; r = 0.52), suggesting that pathology in a brain region is correlated with greater exposure to pathology in anatomically connected regions, an effect that has been demonstrated in other neurodegenerative syndromes29,49,50,51,52.

a We test the hypothesis that local regional atrophy is related to atrophy in its anatomically connected neighbours. The scatter plot shows the atrophy of a node (y-axis) and the mean atrophy of that node’s structurally connected neighbours (x-axis) (Pearson correlation coefficient; r = 0.52). Grey circles indicate brain regions. Atrophy values are derived from the group-average atrophy map shown in Fig. 1c, d. The structural connectome is sourced from healthy young adults in the HCP-S900 dataset. b The observed correlation coefficients between node and neighbour atrophy (red circles) are shown with respect to three null models: (1) spatial autocorrelation preserving spin tests (pspin = 9.99 × 10−4, blue box plot), (2) degree-preserving rewired networks (p = 9.99 × 10−4, green box plot), and (3) degree- and edge length-preserving rewired networks (p = 0.026, red box plot). Asterisks indicate statistical significance with respect to each null model. c In the atrophy ranking method, epicenters are defined as nodes that are both highly atrophied and structurally connected to other highly atrophied nodes. To estimate the epicenter likelihood of a node, nodes are first ranked according to their atrophy and then ranked according to their neighbours' atrophy. The epicenter likelihood ranking of each node is defined as its mean ranking in the two lists. The epicenter maps are shown on both inflated and flat cortical fs-LR surfaces, with the top-ranked nodes highlighted by black borders. In the figure legend, LH stands for left hemisphere and RH stands for right hemisphere. For completeness, we additionally show the interindividual variability in node-neighbour correlation values and plot the mean, standard deviation, and mean divided by standard deviation of epicenter maps across individual ALS patients in Fig. S3.
To demonstrate that atrophy patterns are mainly driven by network topology and not by spatial proximity among regions or the spatial autocorrelation of the atrophy patterns, we apply three null models (Fig. 2b)53. The first null model is a spatial autocorrelation-preserving randomization that tests whether the correlation between node and neighbour atrophy is passively due to spatial autocorrelation in the atrophy map ("spin test”)54,55. This model generates a null distribution for node-neighbour correlation values by projecting the atrophy map to a sphere, applying random angular rotations, bringing the rotated map back to the cortical surface, and re-calculating the node-neighbour atrophy correlations using the values from the rotated atrophy maps. We observe significantly greater correlations for the empirical map compared to the rotated maps (pspin = 9.99 × 10−4), suggesting that the effect cannot be attributed to spatial autocorrelation. Moreover, the correlation between node and neighbour atrophy is significantly greater when using the empirical structural brain network compared to rewired null structural networks that randomize network topology, including both degree-preserving and degree- and edge length-preserving nulls (p = 9.99 × 10−4, 0.026; respectively)56. Collectively, these null models show that the correlation between node and neighbour atrophy is specifically due to network topology.
Lastly, to ensure that the results are not unduly influenced by the choice of parcellation, we repeated the analysis using the Schaefer-800 functional parcellation and replicated the observed dependence of atrophy on structural connectivity. Fig. S2 shows the correlation between node and neighbour atrophy in this case (Pearson correlation coefficient; r = 0.61). The observed correlation is again higher than values obtained using the spatially autocorrelated atrophy maps (pspin = 9.99 × 10−4) and surpasses the correlation values obtained using rewired null structural networks (p = 9.99 × 10−4).
Epicenters of cortical atrophy
Given that the structural connectome shapes the spread of ALS-related pathology, we next sought to identify the putative cortical epicenter of the atrophy. We apply two methods—one empirical and one computational—to back-reconstruct the spreading trajectory and infer the most likely cortical location of the epicenter: (1) a network-based node ranking method, and (2) a susceptible-infected-removed (SIR) dynamical model, detailed in the Fig. S4, Table S3, and Supplementary Information: The S.I.R model. Both methods have previously been applied to understand the course of multiple neurological diseases29,52,57,58,59,60,61.
The ranking method identifies an epicenter as a region that is severely impacted by disease-related atrophy and whose structurally connected regions also exhibit extensive atrophy. In this approach, brain regions are ranked based on both their own atrophy values and their neighbours’ atrophy values in two separate lists. Each cortical node is then assigned a value reflecting the node’s average rank across these two lists. Figure 2c showcases the final mean ranking values across brain regions; in this map, higher values indicate higher probability of a node being an epicenter. The two most probable epicenter locations are within the right and left pre-central gyrus (primary motor cortex).
In the second approach, we build an SIR model using the structural connectome as the only underlying foundation for the spread of pathogenic agents, and hence atrophy. The model works by simulating the misfolding of normal proteins in the cortex and their trans-neuronal spread through the structural connections between brain regions. The similarity between real atrophy map and simulated atrophy maps is computed at each time point (Fig. S4). Each trajectory in the plot corresponds to the similarity of real and simulated atrophy when a specific parcel is chosen as the epicenter for the spread of misfolded proteins. Brain parcels are ranked based on parcels’ maximal correlation value across all simulation time-points. The top two parcels which can best reproduce the atrophy pattern, are indicated in blue and yellow in Fig. S4, and again are located within the motor cortex. Altogether, both methods yield similar epicenter probability maps (Pearson correlation coefficient; r = 0.77, pspin = 9.99 × 10−4, nspin = 1000). Both maps suggest high probability of being an epicenter for parcels across the motor and premotor cortices, as well as dorsolateral prefrontal cortex, posterior parietal cortex, and superior temporal gyrus. The location of these epicenters is consistent with the ALS staging mechanisms developed by Brettschneider et al.14, where the motor cortex is identified as the initial site of pathology, with subsequent spread of the disease to more distal areas in the prefrontal and parietal brain regions.
Local biological features guide pathogenic spread
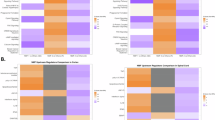
We next investigate the potential contribution of multiple biological features in guiding disease spread. We consider the hypothesis that spread may be more likely between regions that display or share specific biological features. Specifically, we reconstruct five inter-regional similarity networks that describe the biological similarity of pairs of brain regions. The networks include: (1) gene expression similarity, (2) neurotransmitter receptor similarity, (3) laminar differentiation similarity, (4) metabolic similarity, and (5) hemodynamic similarity (i.e., functional connectivity) (Fig. 3)51.

Inter-regional similarity networks reflect the similarity of brain regions according to multiple biological features. We analyze transcriptomic (gene expression) similarity, receptor similarity, laminar similarity, metabolic similarity, and hemodynamic similarity51. The heatmaps visualize these networks. Negative-valued elements are excluded from all analyses. The node-neighbour atrophy correlations are estimated for each inter-regional similarity network. The group-averaged ALS atrophy pattern in Fig. 1c, d is used to derive the correlations. The significance of node-neighbour correlations is assessed with respect to spatial autocorrelation preserving spin tests (nspin = 10,000; FDR corrected; transcriptomic similarity: pspin = 1.55 × 10−2, receptor similarity: pspin = 1.55 × 10−2, laminar similarity: pspin = 0.14, metabolic similarity: pspin = 9.99 × 10−4, hemodynamic similarity: pspin = 0.03). Red dots depict node-neighbour correlations, and boxplots depict the corresponding spin test-estimated null distributions. Additionally, we construct linear regression models to predict ALS cortical atrophy using two variables: (1) weighted mean neighbour atrophy, where the weights are derived from the structural connectome, and (2) weighted mean neighbour atrophy, where the weights come from the interregional similarity matrices. We assess whether adding the second regressor (weighted mean neighbour atrophy based on a specific interregional similarity matrix) improves model fit (adjusted R2), compared to adding a regressor with the same spatial organization. Adjusted R2 is improved only when incorporating data from metabolic similarity matrix. See Fig. S5 for further details.
To assess whether regions with similar biological features are also more likely to experience atrophy, we compute node-neighbour similarity as in Fig. 2a. Namely, we define the “exposure” that region i has to region j’s atrophy as the product between the edge weight (cij if cij > 0) and the extent of atrophy in the neighbouring nodes. Here, we use the connection weights derived from each of the five inter-regional similarity networks. If the weights from a network yield a high value for node-neighbour atrophy, this suggests that the biological feature encoded by that network contributes to the spread of pathology through the synaptic connections51. We assess significance with respect to spatial autocorrelation-preserving spin tests and apply FDR correction to the resulting p-values.
We find that all networks of inter-regional biological similarity except laminar similarity yield significant correlations between node and neighbour atrophy values (Fig. 3). Interestingly, metabolic similarity—estimated using dynamic FDG PET—yields the greatest node-neighbour similarity compared to other tested interregional similarity matrices (Pearson correlation coefficient; r = 0.45, pspin = 9.99 × 10−4). For other types of biological similarity matrices, following node-neighbour correlation values are obtained: gene expression similarity, r = 0.35 (pspin = 1.55 × 10−2); neurotransmitter receptor similarity, r = 0.34 (pspin = 1.55 × 10−2); laminar similarity, r = 0.22 (pspin = 0.14, not significant), and hemodynamic similarity, r = 0.24 (pspin = 0.03).
Finally, we test whether adding information from any biological similarity matrix improves disease propagation prediction beyond what structural connectivity alone provides. To address this question, we construct linear regression models to predict ALS cortical atrophy using two variables: (1) weighted mean neighbour atrophy, where the weights are derived from the structural connectome, and (2) weighted mean neighbour atrophy, where the weights come from the interregional similarity matrices (Fig. S5a). We find that only addition of metabolic similarity information as a second regressor results in improved model fits (adjusted R2), compared to adding a randomized regressor with the same spatial autocorrelation pattern (Fig. S5b; increase in adjusted R2 from 0.266 to 0.280, pspin = 1.40 × 10−2). This is consistent with numerous reports that ALS is associated with metabolic dysfunction, including abnormal mitochondrial physiology leading to a decreased level of adenosine triphosphate (ATP) and oxidative stress, as well as dysfunction of astrocyte mitochondrial and glutamate transporters leading to increased capture of free glutamate and excitotoxicity41,62,63. The results suggest that network structure and the metabolic connectivity jointly contribute to the spatial patterning of atrophy. In the next subsection, we investigate the molecular and cellular features associated with atrophy in greater detail.
Molecular and cellular signatures of epicenters
Up to now, we find that atrophy patterns reflect network organization and are centered on a compact set of epicenters. We next ask whether the network epicenters of ALS atrophy are enriched for specific biological processes, cellular components, and cell types. We cross-reference the ALS epicenter probability map (Fig. 2c) with microarray gene expression from the Allen Human Brain Atlas64. We submitted the gene list to Gene Category Enrichment Analysis (GCEA) to isolate Gene Ontology (GO) categories in which the constituent genes are significantly more correlated with epicenter likelihood map than a population of randomized maps with preserved spatial autocorrelation65 (see “Methods”).
Consistent with the intuition developed in the previous subsection—suggesting involvement of metabolic features in disease spread—the top GO categories are mainly associated with metabolic processes and energetic homeostasis (Fig. 4a). These terms include “ATP metabolic process”66, “Tricarboxylic acid cycle”, “gluconeogenesis”, “mitochondrial calcium ion transport”67,68, “glycolytic process”69, “glycosphingolipid metabolic process”70,71, “mitophagy”72,73,74, “positive regulation of mitochondrial fission”75,76, “mitochondrial matrix”77, “mitochondrial membrane”77,78, “integral component of mitochondrial inner membrane”78, “integral component of mitochondrial outer membrane”78, “protein import into mitochondrial matrix”79,80, “amino acid transport”, “branched-chain amino acid catabolic process”81, “peroxisome”82,83, and “peroxisomal matrix”82,83, all of which point toward altered energy metabolism and mitochondrial dysfunction. Additionally, categories related to cells’ cytoskeletal structure, such as “actin filament-based movement”, “apical dendrite”84, “microtubule associated complex”84,85, “vesicle transport along microtubule” and “anchored component of membrane” are implicated in the disease, which point to the structural dysregulations happening in the cells causing axonal transport disturbance86, impairment of information integration in cells84, and impairing cell adhesion. A brief explanation of biological processes and cellular components shown in Fig. 4a, b can be found in the Gene enrichment details section of the Supplementary Information. A comprehensive list of significant terms can be found in the Supplementary Data 1: Gene-enrichment.

a Top 30 biological process terms from the GO Consortium knowledge base associated with gene sets correlated with the ALS epicenter likelihood map, shown in Fig. 2c214. b All cellular components terms from the GO Consortium knowledge base that are significantly enriched in gene sets correlated with the ALS epicenter likelihood map214. Terms in both categories are ordered by their category scores (c-scores). c Cell type enrichment analysis of ALS epicenter map reveals significant hits for pericytes and endothelial cells87. Used gene markers for endothelial cells and pericytes are shown in Fig. S6. The graphical representation of pericytes and endothelial cells is created in BioRender (Farahani, A. (2025) https://BioRender.com/xswclks). For more details, including gene markers for each biological process, cellular component, and cell type, exact c-score values, and corresponding p-values, refer to the Supplementary Data 1: Gene-enrichment.
In addition, we estimated cell type enrichment associated with ALS epicenters using genetic markers of different cell types, as determined through single-nucleus droplet-based sequencing and single-cell transposome hypersensitive site sequencing of human brain cells87 (Fig. 4c). We find significant enrichment for pericytes88,89,90,91 and endothelial cells92,93 (see Fig. S6). This observation points to possible vascular dysfunction in ALS, potentially explaining the consistent enrichment of metabolic categories. The finding is consistent with previous reports that show a reduction in pericytes in the spinal cord in ALS93,94. These cellular changes occur even prior to the initial clinical manifestations of the disease95,96. Collectively, these findings show that the spatial patterning of atrophy in ALS is related to both network structure as well as local molecular and cellular features that confer greater vulnerability to the disease. In other words, axonal projections are the physical conduit for disease spread, but the trajectory of spreading is guided by local biological features.
The correlation coefficients between all stable genes (differential stability greater than 0.1) from the Allen human brain atlas, the group-average atrophy map (Fig. 1c, d) and the epicenter map (ranking approach, Fig. 2c), along with their corresponding p-values from spin tests and FDR-corrected p-values are detailed in the Supplementary Data 2: Gene-correlation.
Epicenter location is correlated with clinical presentation and symptom severity
If cortical epicenters reflect the spatial focus of ALS pathology, do they also correlate with the clinical manifestation? To address this question, we analyzed the covariance between individual patient epicenter maps and individual differences across a variety of clinical, cognitive, and demographic variables. We used a multivariate pattern learning algorithm—partial least squares (PLS)—to identify epicenter locations and clinical subtypes that maximally covary with each other97,98,99 (see “Methods”).
The analysis revealed two latent variables that accounted for 24.89% and 12.21% of covariance between epicenter maps and clinical scores (Fig. 5, Fig. S7). Both latent variables were statistically significant using permutation tests (p = 9.99 × 10−4 and 4.89 × 10−2, respectively), but only the first latent variable could be cross-validated (p = 0.039). The first latent variable captures a mainly primary motor cortical epicenter pattern (Fig. 5a). Individuals who display this epicenter pattern tend to have worse motor function, including abnormal index finger and foot tapping scores, daily physical functions (Revised Amyotrophic Lateral Sclerosis Functional Rating Scale; ALSFRS scores), and muscle tone. Interestingly, pathology in these epicenters is uncorrelated with most cognitive scores, except for worse cube counting and delayed recognition scores. In other words, atrophy load in this cortical location is linked with worse motor symptoms and a higher level of disability.

a The first latent variable from a PLS analysis relating individual epicenter maps and clinical-behavioral measurements. Brain loadings are shown on the fs-LR inflated and flat cortical surfaces. Regions demarcated by the black border are those with the greatest effect sizes (parcels in which over 50% of the vertices have a Cohen’s d effect size exceeding 1) in the group-average activation map from S1200 Human Connectome Project package for the movement task contrasts219. Regions demarcated by green borders showcase areas 44 and 45 from the Glasser parcellation222. These regions, specifically in the left hemisphere104, correspond to the Broca’s area223. b The scatter plot visualizes the individual ALS participants' brain scores versus behavioral PLS scores (Pearson correlation coefficient, r = 0.54; Spearman correlation coefficient, r = 0.54); each participant’s score is colored based on the revised-ALSFRS total score. The total ALSFRS score quantifies the degree of functional disability resulting from the disease (greater values correspond to lower disease severity)149. c The bar plot visualizes the behavioral/clinical measures' loadings. The contribution (effect size) of individual measures is assessed by bootstrap resampling (1000 repetitions). For further details on the included measures refer to Table S4. Fig. S8 shows the PLS results when atrophy maps are used instead of epicenter maps.
Despite statistical significance and a large effect size, the second latent variable could not be cross-validated. We therefore relegate the figure to the supplement (Fig. S7) and only describe this latent variable for completeness. The second latent variable captures mainly a dorsolateral prefrontal cortical epicenter pattern. Individuals who display this epicenter pattern tend to have worse ALSFRS speech scores, as well as respiratory insufficiency (i.e., worse ALSFRS-respiratory insufficiency score). The clinical pattern also captures covariance between atrophy in medial prefrontal cortex and lower scores in multiple cognitive measures. Collectively, these patterns suggest that individual differences in epicenter location are closely linked with clinical presentation. Importantly, the two latent variables are reminiscent of spinal-onset and bulbar-onset ALS clinical subtypes, which we examine in detail next.
Atrophy epicenters in spinal- and bulbar-onset ALS
So far, we focused the analysis on a common atrophy pattern across the patient sample. However, ALS is heterogeneous, and in clinical practice individuals are often stratified according to the initial body region of onset100. Most individuals experience spinal (limb) onset of the disease where the first symptoms appear in the legs and/or hands, while a third of patients report the first symptoms being in bulbar areas3, citing difficulties in salivation, swallowing, and speaking101,102. The present dataset (CALSNIC) provides stratification for both bulbar- (N = 38) and spinal-onset (N = 140) ALS subtypes (see “Methods” and Table S5). There are also rare cases of patients who report respiratory difficulties in the initial stages of the disease103, but these were not included in the analysis. Neither were patients with mixed spinal- and bulbar-onset, nor those with frontotemporal dementia-onset.
Here we investigate whether cortical network epicenters are related to spinal- and bulbar-onset of the disease. We estimate epicenter probability maps for spinal and bulbar ALS with the two methods presented in the Epicenters of cortical atrophy subsection (the ranking approach, Fig. 6a and the SIR modeling approach, Fig. S9). The two methods yield similar epicenter likelihood maps for both disease onset types (Pearson correlation coefficient; rspinal = 0.76, rbulbar = 0.78, pspin = 9.99 × 10−4) (Fig. S9). Importantly, epicenter probability maps in spinal and bulbar ALS are different: in spinal-onset ALS atrophy is mainly confined to primary motor cortex and paracentral lobule; conversely, in the bulbar-onset ALS atrophy infiltrates areas in lower paracentral gyrus and inferior frontal gyrus. To highlight epicenter differences between these two subtypes, we contrast cortical epicenter maps for individuals with spinal and bulbar ALS using t-tests. In this analysis, we used individualized epicenter maps derived from the node-neighbour approach. The obtained t-statistic map identifies regions that are more likely to be epicenters in one type compared to the other (Fig. 6b). For reference, we use the Human Connectome Project motor task group average effect size maps to delineate and overlay borders of cortical regions associated with movement of the tongue, hands, and feet. Additionally, we include the borders of areas 44 and 45 of Glasser parcellation (Broca’s area). These areas are functionally involved in speech production104, a phenomenon that is affected in ALS. Consistent with their clinical subtypes, bulbar-onset individuals show cortical disease epicenters in regions linked to tongue movement and in Broca’s area, accounting for increased speech deterioration in the bulbar group compared to the spinal group105. Conversely, the spinal-onset individuals predominantly have more likely epicenters in regions associated with movement of feet.

a Epicenter likelihood maps for spinal-onset ALS and bulbar-onset ALS. Maps are obtained for each subtype using two methodologies: ranking approach and the agent-based SIR modeling approach (see Fig. S9). The maps derived by the ranking method are presented here. b The brain maps depict the t-statistics derived from contrasting the bulbar- versus spinal-onset ALS epicenter maps. Regions demarcated by the black border are those with the greatest effect sizes (parcels in which over 50% of the vertices have a Cohen’s d effect size exceeding 1) in the group-average activation map from S1200 Human Connectome Project package for the movement task contrasts219. Regions demarcated by green borders showcase areas 44 and 45 from the Glasser parcellation222. These regions, specifically in the left hemisphere104, correspond to the Broca’s area223. Cyan borders highlight three parcels that retain significance following FDR correction (FDR-corrected; p = 0.011, 0.011, and 0.021). Two of these parcels are located within the tongue movement area, while the other is adjacent to the tongue movement area toward the premotor region, this area might be involved in tongue movement control, given the homologous relationship between motor and premotor areas106,107. We further contrasted the behavioral/clinical measures for spinal- and bulbar-onset ALS patients. Bar plots show measures that are significantly different between the two subtypes (FDR corrected). Atrophy maps for each subtype are shown in Fig. S10.
The analysis indicates a statistically higher epicenter likelihood in bulbar ALS compared to spinal ALS in three parcels (all located in the right hemisphere). Two of the three significant parcels are located within the thresholded area of tongue movement and the third parcel is situated toward the premotor area, this area may be involved in tongue movement control, given the homologous relationship between motor and premotor regions106,107.
Additionally, assessing behavioral measures in CALSNIC dataset show that individuals with the bulbar-onset ALS have severe inability in their speech, salivation, and swallowing, and they have increased jaw and upper limb reflexes compared to the individuals with spinal-onset ALS; meanwhile, those with spinal-onset ALS displayed more significant weakness in dressing and hygiene, walking, and stair climbing abilities. These results show how network epicenters of cortical atrophy align with the clinical manifestation of the disease.
Discussion
The present report explores how network structure and local biological features shape the spatial patterning of atrophy in ALS. We find that structural connectivity, together with inter-regional similarity of metabolic features, closely aligns with the spatial patterning of atrophy and clinical expression of ALS. We identify consistent and prominent disease epicenters in motor cortex. Epicenter probability maps show transcriptomic enrichment for biological processes involved in mitochondrial function as well as support cells, such as endothelial cells and pericytes. Finally, individual differences in epicenter location correspond to individual differences in clinical and cognitive symptoms and differentiate patient subtypes.
We consistently find that atrophy in a brain region is correlated with the atrophy of anatomically connected regions, suggesting that atrophy spreads via white matter projections. This is consistent with the notion that ALS pathology is related to misfolding and network spreading of TAR-DNA binding protein (TDP)-43108,109,110,111. According to this account, pathological changes in conformation (misfolding) of endogenous TDP-43 induce aggregation and further misfolding. Trans-synaptic spread of pathogenic misfolded TDP-43 results in patterns of cell death and atrophy that ultimately resemble brain network architecture. Our results support this account in two ways. First, the corticospinal tract exhibits the most pronounced atrophy (consistent with findings in refs. 27,112,113,114), as does primary motor cortex, suggesting that cortical regions with strong physical connections to the corticospinal tract experience the greatest pathology. Second, a region’s atrophy and the atrophy of its neighbours are correlated, suggesting that network-based exposure to the pathology confers increased risk of pathology. This correlation is significantly greater than in rewired null models that preserve degree sequences and edge lengths, suggesting that the effect is not trivially due to spatial proximity or the total number of connections in a given region, but rather due to the arrangement of connections and the overall topology of the network. Network-based spreading of pathogenic proteins is implicated not only in ALS but across multiple neurodegenerative diseases, and can be observed across multiple spatial scales (e.g., cell-to-cell or region-to-region)115,116,117,118,119, measurement techniques (e.g., histopathological staining or MRI-based atrophy)120,121,122 and model organisms (e.g., mouse models and humans)123,124,125,126. Altogether, these results emphasize the role of structural network architecture as the mediator of the pathological protein spread in ALS7,8,9,10 and further challenge the notion that ALS is a non-prion-like spreading disease127.
In addition to structural connectivity, we find that the local metabolic features of brain regions contribute to disease spread. Numerous theories posit that the propagation of ALS is affected by atypical metabolic function63,128,129. Consistent with this notion, we find that metabolic inter-regional similarity also contributes to the patterning of atrophy. In other words, spreading of pathology is not only affected by structural connectome architecture but also more likely to take place between neuronal populations that share similar metabolic characteristics.
Given that disease spread appears to follow network structure, we next sought to identify the most likely cortical epicenters. We assessed the likelihood of various brain regions acting as cortical disease epicenters using two methods: (1) data-driven ranking, and (2) agent-based SIR modeling. Both methods identified regions located in the primary motor area to be the likeliest epicenters, as well as regions in frontal and temporal cortex, such as the temporoparietal junction. These results are in line with histopathological findings, showing TDP-43 pathology in motor cortex (Brodmann areas 4 and 6) in the initial stages of the disease14. The involvement of frontal and temporal areas in later stages of the disease is also well-documented14,27,130.
What biological features predispose regions to act as disease epicenters? The epicenter probability map is correlated with the spatial expression of genes involved in metabolic processes, pointing toward mitochondrial functions such as ATP production, as well as the structural organization of mitochondrial membrane and matrix, and disruption of mitochondrial calcium ion transport. This finding is in line with the idea of mitochondrial stress in ALS. Namely, dysregulation of mitochondrial calcium transport, potentially driven by increased excitatory cytosolic calcium uptake or changes in the function of mitochondrial calcium transporters, results in mitochondrial injury and triggers mitophagy. In addition, mitochondrial dysfunction is thought to cause further structural abnormalities in multiple cell types; for example, deletion of mitochondrial calcium uniporter changes dendritic spine morphometry131. The observation that cortical atrophy in ALS co-localizes with cortical regions enriched for mitochondrial function and structure further emphasize the need to consider the metabolic dimension of the disease in future neuroimaging studies (e.g., through use of FDG-PET imaging129).
In addition, the epicenter likelihood map overlaps with transcriptomic signatures of pericytes and endothelial cells. Endothelial cells are single-layer cells lining the blood vessels132. Pericytes surround the endothelial cells by extending their long cytoplasmic processes on the surface of endothelial tubes. The interaction between endothelial cells and pericytes is needed in formation and maintenance of blood-brain barrier (BBB), and blood-spinal cord barrier (BSCB); which contribute to maintaining the controlled chemical composition of the neuronal milieu133,134. Multiple studies point to a breakdown in both BBB and BSCB in ALS89,135. In mouse models of ALS, damage to BSCB, BBB, and endothelial cells is observed early in the disease136,137, and often precedes the onset of motor symptoms95. Similar vascular deficits have also been reported in human patients138. Indeed, cerebrospinal fluid abnormalities in ALS are thought to at least partly originate from the increase in BBB permeability139,140. Postmortem histology confirms the loss of integrity of BBB and SCSB due to endothelial cell damage and pericyte degeneration88,93. Our findings corroborate that the scope of inquiry for studying ALS should be broadened beyond motor neurons, and that support cells—such as vascular cells—should also be considered as therapeutic targets. Interestingly, recent findings suggest that treatment of ALS mice models with unmodified human bone marrow CD34+ (hBM34+) cells accelerates BSCB repair, leading to differentiation into endothelial cells, reduced astrogliosis and microgliosis, and improved perivascular integration, ultimately promoting survival of motor neurons141; likewise, treatment with pericytes improves overall survival in SOD1 mutant ALS mice142.
Finally, the locations of individual network epicenters map onto individual differences in clinical manifestation. Overall, individuals with greater epicenter probability in motor cortex had worse motor symptoms and signs, including poorer finger and foot tapping, increased muscle tone and reflexes, and lesser capability to perform daily functions involving the limbs (Fig. 5). The multivariate clinical subtype also included lower scores in naming, sentence completion, and verbal fluency tasks, presumably corresponding to greater epicenter probability in left inferior frontal cortex (Broca’s area; Fig. 5). Interestingly, disease epicenters in patients with bulbar- and spinal-onset of the disease evolve in different trajectories. Specifically, patients with bulbar-onset ALS displayed greater epicenter likelihood in three parcels involved in tongue movement. Collectively, these results demonstrate that studying ALS pathology from a network perspective can help trace the spatial origin of the disease, identify the molecular and cellular contributions to pathology, and, ultimately, map individual differences in brain-behavior relationships and clinical subtypes.
These findings build on multiple empirical reports8,40,111,130,143 and modeling studies on the relationship between connectivity and atrophy in ALS. Namely, several studies have modeled ALS-related degeneration and histopathological measurements, using various approaches, such as random walk models8,9 and network diffusion models10,144, showing that across a variability of models the whole-brain atrophy is related to the structural connectome. Importantly, Pandaya et al.10 showed that incorporating ALS gene risks coming from immunocytochemistry, exome sequencing and genome wide association studies, into the models can improve model accuracy, highlighting the importance of considering biological data to understand the underlying mechanisms of ALS neurodegeneration. The present report goes a step further and uses a data-driven approach to gene ontology analysis without relying on predefined gene sets, thereby identifying biological processes and cellular components that confer vulnerability to atrophy in ALS.
The present results should be considered with respect to several methodological limitations. First, we estimated atrophy using in vivo MRI deformation based morphometry, a technique that is well-validated but that does not directly measure pathology (e.g., neuronal loss, TDP-43 deposition). Despite this limitation, the results recapitulate numerous histopathological hallmarks of the disease. Meanwhile, when quantifying the atrophy maps of ALS participants, the potential influence of education145 and handedness146,147 was not excluded from the data. As some studies point to the potential for these variables to influence neuroanatomical metrics, future studies should consider their inclusion to fully account for confounding factors. Second, all network spreading effects were estimated using an independent high-resolution diffusion MRI dataset, rather than individual patient connectomes. Likewise, inter-regional transcriptomic similarity, receptor similarity, laminar similarity, metabolic similarity, and hemodynamic similarity matrices are estimated from non-ALS participants. This methodological decision highlights the need for more multimodal imaging and more extensive biological assays in patient samples. Third, all results are based on a single dataset. Although we used multiple methods whenever possible (e.g., when identifying epicenters), as well as cross-validation (e.g., for the PLS model), ideally, the results should be independently confirmed using a different ALS dataset. Fourth, the present analyses were performed without stratifying patients according to genetic mutation. Comprehensive comparison of sporadic and genetic cases is important to understand the heterogeneity of ALS, and highlights the need for larger sample sizes and targeted recruiting in future data collection efforts. Fifth, we did not use longitudinal MRI to assess the spreading mechanism in ALS due to several limitations; namely, not all ALS participants completed all three visits (71/192 had all three follow-up data available). Moreover, patients with more severe symptoms and faster disease progression are often unable to complete follow-up visits, either due to passing away before the next scan or becoming too dependent on intensive care. As a result, focusing solely on the subset of patients who completed follow-ups would likely bias the findings toward individuals with slower progression, limiting the generalizability of the results to the broader ALS population. We encourage future studies to reassess the findings presented in this paper using alternative methodological approaches—such as different structural connectome and inter-regional similarity matrix construction pipelines, or different parcellation schemes—to further validate the robustness of the results.
In conclusion, we reveal that network structure and local metabolic features leave an indelible mark on the expression of neurodegeneration in ALS. These two factors are closely related and should be studied simultaneously, rather than in isolation. Conceptualizing neurodegeneration as a multiscale spreading process may help to identify molecular, cellular and regional targets for therapies that slow or divert the course of pathology.
Methods
All codes used to perform the analyses are available on GitHub at https://github.com/netneurolab/Farahani_ALS and on Zenodo at https://zenodo.org/records/15865751 (https://doi.org/10.5281/zenodo.15865751).
CALSNIC dataset
Data was retrieved from the Canadian ALS Neuroimaging Consortium (CALSNIC) dataset (http://calsnic.org). The dataset comprises data from individuals diagnosed with possible, probable, or definite ALS, according to the revised El Escorial Criteria148, alongside data from healthy controls. All participants underwent 3T magnetic resonance imaging (MRI), yielding 1 mm isotropic T1-weighted (T1w) data for each individual. We use data acquired from eight different imaging sites, including: University of Calgary (CAL), University of Alberta (EDM), McGill University (MON), University of Toronto (TOR), University of British Columbia (VAN), University of Miami (MIA), Université Laval (QUE), and University of Utah (UTA). We exclude data from participants if they had other central nervous system abnormalities or reported psychiatric illness. The CALSNIC dataset provides longitudinal neuroimaging data with approximately four-month intervals between sessions for some but not all participants. We only keep individuals with a scan acquired at baseline for further analysis, resulting in 192 individuals with ALS (70 female; mean age: 59.62 ± 10.20 years) and 175 healthy control participants (96 female; mean age: 55.41 ± 10.00 years). Note that data used in this study comes from two phases of the CALSNIC dataset launched to date, which have slight changes in the structural MR imaging paradigm. Consequently, when building the ordinary least square model to estimate disease-related atrophy, if data from the same imaging site is acquired during different project phases, we treat the data from each phase as a separate entity. This assumption leads to considering twelve imaging sites in total when building the model (CAL: phase 1, 2; EDM: phase 1, 2; MON: phase 1, 2; TOR: phase 1, 2; VAN: phase 1; MIA: phase 2; QUE: phase 2; UTA: phase 2). All participants gave written informed consent, and the CALSNIC data collection was approved by the health research ethics boards at each of the participating sites. All ethical regulations relevant to human research participants were followed. Details regarding the demographic information of subjects per imaging site are provided in Table S1. Additionally, information on magnetic resonance vendors and imaging sequence details can be found in Table S2. For further data description refer to the original publication23.
Behavioral/clinical measures
The CALSNIC dataset, in addition to the magnetic resonance imaging data, provides behavioral/clinical assessments for individuals. These encompass ALS-related motor and cognitive evaluations, including Revised Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS), Edinburgh Cognitive and Behavioral ALS Screen (ECAS), finger/foot tapping tests, and evaluations for abnormal muscle tone and reflexes. Data on individuals’ sex, age, symptom duration, years of education, and handedness are also provided. Below is a brief overview of each measure.
ALSFRS is a rating measure that quantifies the level of disability in ALS patients. Higher values of this scale (with a maximum of 48) indicate lower disease severity. Specifically, ALSFRS assesses the participants’ functional capability in speech, salivation, swallowing, handwriting, gastrostomy, cutting food and handling utensils, dressing and hygiene, turning in bed and adjusting bed clothes, walking, climbing stairs, dyspnea, orthopnea, and respiratory insufficiency149. ECAS is a cognitive screening test to assess executive function, letter and semantic fluency, attention, memory, language, and visuospatial function of individuals150. A higher total score for ECAS (up to 136) signifies better cognitive performance. The tapping score, which is a clinical motor symptom severity indicator, quantifies the number of taps a participant can perform in 10 s by their fingers or feet. A higher count in this test reflects better motor function. In CALSNIC dataset, the tapping scores for both index-finger, and foot are measured two times per participant. Muscle tone and reflex measures are also included, with lower scores signifying normal tone and reflex conditions. For further elaboration on what each measure quantifies, refer to Table S4.
In this study, we use behavioral/clinical measures to relate the cortical epicenter locations to the behavioral manifestations of individuals with ALS (see Epicenter location is correlated with clinical presentation and symptom severity and Atrophy epicenters in spinal- and bulbar-onset ALS sections). Of the 192 patients included in the study, 8 individuals have incorrect ECAS administration; these participants are therefore excluded from analyses relating brain and behavior data (PLS analysis).
Deformation based morphometry
T1w data is preprocessed and Deformation Based Morphometry (DBM) maps are derived per participant (ALS and control participants in CALSNIC) using the Montreal Neurological Institute Medical Imaging NetCD (MNI-MINC) tools, publicly available at https://github.com/BIC-MNI/minc-toolkit-v2. The preprocessing steps include image denoising151, intensity inhomogeneity correction152, and image intensity normalization into range (0–100) using histogram matching; next, each T1w image is first linearly and then nonlinearly registered into the MNI152-NonLinear2009cSym standard brain. DBM maps are derived by estimating the local deformation needed in each voxel in an individual’s T1w image to nonlinearly match it to the standard template (MNI152-NonLinear2009cSym standard brain—T1w contrast). The required deformation is estimated by the Jacobian determinant of the inverse nonlinear deformation field and can be used as an indirect estimate of brain atrophy153,154. DBM values lower than 1 indicate that the corresponding region is smaller in the participant than in the template (atrophy in the participant compared to the template). Conversely, DBM values greater than 1 indicate that the corresponding region in the participant space is larger than the same region in the template space (expansion in the participant compared to the template). Collectively, the DBM maps encode the morphological differences between the T1w data of a given participant and the standard brain defined by the MNI template.
Atrophy maps
The Jacobian determinant from the DBM analysis serves as a dependent variable, influenced not only by the diagnosis but also by factors such as age, sex, and imaging site. To isolate factors unrelated to diagnosis from the DBM maps of ALS patients and to obtain a more accurate measure of disease-specific atrophy, we compute w-score map per individual155. The w-score value at each voxel quantifies the normalized deviation of the observed DBM value from its expected DBM value, adjusted for age, sex, and imaging site. The expected value for DBM at each voxel is estimated using an ordinary least squares model (DBMexpected = β1 × age + β2 × sex + β3) that is constructed based on control participants’ data. Greater absolute disparity between the observed and expected value of DBM indicates more severe atrophy or expansion in a given voxel. The formula to calculate the w-score for a voxel of interest is provided in the following:
where std stands for standard deviation, DBMobserved is the raw DBM value without covariate adjustments, and DBMexpected is the predicted DBM value for a participant defined based on the already trained model (β1 × age + β2 × sex + β3). A negative w-score in this context signifies greater atrophy than the mean value expected for a healthy participant, with normal aging and sex effects accounted for. After calculating the w-score maps of all ALS participants under study, w-score maps are averaged across ALS patients to create a single collective atrophy map. To simplify interpretation, the w-score maps are multiplied by −1 so that the larger numerical values correspond to more atrophy. Throughout the manuscript, the w-score maps (post-inversion) are referred to as the “atrophy map”. The group-average ALS atrophy map is visualized in Fig. 1a.
Brain tissue parcellation
ALS atrophy maps are parcellated using two different atlases. For cortical regions, we apply the Schaefer-400 (and Schaefer-800) functional parcellation44, and to examine the sub-cortex, specifically the white matter tracts, we use the Johns Hopkins University (JHU) white matter tractography atlas (thresholded at 25% probability)35,36. We initially downloaded the MNI152-FSL versions of these atlases from https://github.com/ThomasYeoLab/CBIG/tree/master/stable_projects/brain_parcellation/Schaefer2018_LocalGlobal/Parcellations and https://web.mit.edu/fsl_v5.0.10/fsl/doc/wiki/Atlases.html, respectively. We then registered them into the MNI template of interest (MNI152-NonLinear2009cSym) using “antsRegistrationSyN” and “antsApplyTransforms” from Advanced Normalization Tools156,157.
Von Economo classes
To investigate the specificity of ALS cortical atrophy, we explored seven cytoarchitectonic classes coming from the Von Economo atlas45,46.
To assign von Economo classes to Schaefer-400 parcels44, we applied the classification provided by Scholtens et al.47 to the cortical brain surface, yielding vertex-level assignments. These vertex-level assignments were then used with the winner-take-all approach (majority voting) to generate parcel-level network assignments. With these network assignments established for each of the 400 parcels, we calculated the average atrophy values across the parcels belonging to each network class, resulting in a single atrophy value per class.
Network reconstruction
Brain networks (structural connectivity and inter-regional similarity networks) are retrieved from netneurolab51,158. Below we briefly describe how each network is reconstructed.
Structural connectome
Structural connectivity is a matrix that provides information regarding the white matter connections across pairs of brain regions. In this study, the dataset used to build the connectome comes from 327 unrelated healthy participants (182 female; age: 22–35 years) from the Human Connectome Project (HCP-S900 release), scanned using a 3T Connectome Skyra scanner. The diffusion MRI data is acquired with the spin-echo echo-planar imaging sequence (TR = 5520 ms; TE = 89.5 ms; FOV = 210 × 180 mm2; voxel size = 1.25 mm3; b-value = three different shells, i.e., 1000, 2000, and 3000 s/mm2; number of diffusion directions = 270; and number of b0 images = 18). Diffusion MRI data is preprocessed using the HCP minimal preprocessing pipeline. For detailed acquisition information and preprocessing steps refer to these refs. 48,159.
Structural connectome is reconstructed from the diffusion MRI using the MRtrix3 package (https://www.mrtrix.org)160. Different tissue types of cortical and subcortical grey matter, white matter, and cerebrospinal fluid are segmented using T1-weighted image for anatomical constrained tractography161. Fiber orientation distributions are generated using a multi-shell multi-tissue constrained spherical deconvolution algorithm (algorithm introduced by Jeurissen et al.162 is used to estimate the response function). Initially, a tractogram is generated with 40 million streamlines, with a maximum tract length of 250 and a fractional anisotropy cut-off of 0.06. Spherical-deconvolution informed filtering of tractograms (SIFT2) is used to reconstruct whole brain streamlines weighted by cross-section multipliers163. To build a structural connectome, the reconstructed cross-section streamlines are mapped onto the Schaefer-400 parcellation (as well as onto the Schaefer-800 parcellation)44. For further insights into individual network reconstructions, consult the reference provided164. A group consensus structural network is then created such that the mean density and edge length distribution observed across individual participants is preserved165. The weights of the edges in the consensus networks represent the averaged number of streamlines between parcels, computed across participants with nonzero connections158.
Hemodynamic similarity
Hemodynamic similarity, often referred to as functional connectivity, summarizes the similarity across brain regions in terms of the synchronization and similarity of their co-fluctuation in the BOLD signal. The dataset used to build the connectome comes from 326 unrelated healthy participants (181 female; age: 22–35 years) from the Human Connectome Project (HCP-S900 release), scanned using a 3T Connectome Skyra scanner48. In this dataset, each participant has undergone four 15-minute resting-state functional MRI scans, each with a TR of 720 ms. Data is preprocessed using the HCP minimal preprocessing pipeline. For detailed preprocessing steps, refer to the cited reference159. The voxel-wise functional MRI data is parcellated using the Schaefer-400 atlas44. The parcellated time-series are then used to construct functional connectivity matrices, computed as Pearson correlation coefficient between pairs of regional time-series for each of the four scans per participant. To obtain a group-level functional connectivity matrix, mean functional connectivity across all participants and scans is computed. This matrix is normalized using Fisher’s r-to-z transformation51.
Metabolic similarity
Metabolic similarity estimates the similarity between brain regions in terms of glucose metabolism or, in other words, in terms of energy consumption. This network is reconstructed using positron emission tomography (PET) images of the [F18]-fluordoxyglucose tracer. The dataset includes 26 healthy participants (77% female; age: 18–23 years) who participated in a 95-minute simultaneous MR-PET scan acquired using a 3T molecular MR scanner166. PET images are preprocessed according to ref. 167. Each volume of the PET time-series is registered to the MNI152 template space and is parcellated according to the Schaefer-400 atlas44. Parcellated time-series from pairs of brain regions are then correlated (Pearson’s correlation coefficient) to construct a metabolic connectivity matrix for each participant. Subsequently, by averaging connectivity matrices across all participants, a group-average metabolic connectome is obtained. This matrix is normalized using Fisher’s r-to-z transformation51.
Gene expression similarity
Correlated gene expression quantifies the transcriptomic similarity between pairs of brain regions. The underlying data to construct this connectome comes from the bulk tissue microarray expression data collected from six post-mortem brains (1 female; age: 24–57 years, mean age: 42.50 ± 13.38 years). This data is provided by the Allen Human Brain Atlas (AHBA) (https://human.brain-map.org)64 and is processed using the abagen toolbox, publicly available at https://github.com/rmarkello/abagen168, yielding a map for each gene in the parcellated MNI template (Schaefer-40044). Genes with high differential stability across donors (threshold of 0.1) are considered for the analysis, resulting in 8687 stable genes. A region × region gene expression similarity matrix is constructed by correlating normalized gene expression profiles between pairs of brain regions (Pearson correlation coefficient). This matrix is normalized using Fisher’s r-to-z transformation51.
Note that only two donors from the AHBA had tissue samples taken from the right hemisphere. This irregular sampling results in limited spatial coverage of expression in the right hemisphere; to resolve this, tissue samples were mirrored bilaterally across the left and right hemispheres. Consequently, the final gene expression profile for each region was estimated as the mean of both ipsilateral samples (from all six donors with left hemisphere samples) and contralateral samples (from the two donors with right hemisphere samples)169.
Receptor similarity
Receptor similarity measures how correlated the receptor density profiles are between brain regions. To construct this network, PET tracer images for 18 neurotransmitter receptors and transporters are used61,170. These receptors/transporters cover nine neurotransmitter systems, including dopamine (D1171, D2172,173,174,175,176, DAT177), norepinephrine (NET)178,179,180, serotonin (5-HT1A181, 5-HT1B181,182,183,184,185,186,187,188, 5-HT2189, 5-HT4189, 5-HT6190,191, 5-HTT189), acetylcholine (α4β2192,193, M1194, VAChT195,196), glutamate (mGluR5)197,198, GABA (GABAA)199, histamine (H3)200, cannabinoid (CB1)201,202,203,204, and mu-opioid (MOR)205. Each of these PET tracer images is parcellated based on the Schaefer-400 atlas44 and normalized using z-scores. A region × region receptor similarity matrix is constructed by correlating receptor profiles across all pairs of brain regions (Pearson correlation coefficient). This matrix is then normalized using Fisher’s r-to-z transform51. More information on the PET data acquisition is provided in Table S6.
Laminar similarity
Laminar similarity, estimated from histological data, assesses the similarity in cellular distributions across cortical layers within pairs of brain regions51,206. Data is recovered from the high-resolution (20 μm) BigBrain atlas, a postmortem Merker-stained histological atlas of a 65-year-old male207. Staining intensity profiles are sampled across 50 equi-volumetric surfaces within the cortical grey matter, enabling the assessment of neuronal density and soma size variations across cortical layers. These intensity profiles also help delineate boundaries among cortical layers, such as supragranular (layers I–III), granular (layer IV), and infragranular (layers V–VI). The BigBrainWarp toolbox208 is used to transform the data to the surface-based fs-LR template, which is then parcellated based on the Schaefer-400 atlas44. A laminar similarity matrix is estimated by computing the partial correlation between regional intensity profiles. The matrix is then normalized using Fisher’s r-to-z transform51.
Disease exposure
In this section, our objective is to assess how a specific biological brain connectome affects the spread of pathology across the cortex in ALS. We initially apply a threshold to the connectome under study (e.g., metabolic similarity) to retain only positive values; the thresholded connectome is considered as a “network”, whose “nodes” correspond to the Schaefer-400 parcels44 and the “edges” are defined based on the values in the off-diagonal elements of the connectivity (similarity) matrix. We assume that these edges provide potential pathways for pathology propagation. At each node, we define the global disease “exposure” as a measure quantifying the extent of atrophy its neighbouring nodes are experiencing, weighted according to the strength of the edges that connect the node with its neighbours. Here, “neighbours” are defined as nodes directly connected to the node in focus. The following is a mathematical formulation of disease exposure at a given node, denoted as node i:
here Di represents the disease exposure at node i; which is calculated as the weighted average of atrophy across the neighbours of node i. The atrophy values of neighbours are denoted by dj, where j is the neighbour’s identifier. Each neighbour atrophy value, dj, is multiplied by the edge strength between region i and node j, represented by cij. Ci in the formula represents the weighted degree of connections made by node i within the network. To assess whether connectome architecture is related to the spatial patterning of atrophy, we correlate the degree of atrophy in individual nodes and their respective disease exposures. This analysis is repeated while considering various brain connectomes (including structural connectivity, gene-expression similarity, receptor similarity, laminar similarity, metabolic similarity, and hemodynamic similarity).
Epicenter mapping: data-driven method
With an atrophy map and an underlying connectome, it is possible to identify putative disease epicenters using either epidemiological data-driven methods, or computational modeling (see Epicenters of cortical atrophy)29,52. The data-driven approach is based on the notion that one of the main factors of disease spread is the existence of structural connectivity across brain regions (nodes). Here an epicenter is defined as a node that is both highly atrophied, and physically connected to nodes that are also highly atrophied (Fig. 2c). Epicenters are identified using two separate ranking procedures. In the first ranking procedure, nodes are ranked in ascending order according to their mean atrophy. The second ranking procedure is performed on the array containing the weighted neighbour atrophy values (nodes’ exposure values). The disease exposure value at each node is calculated as previously described in Disease exposure. This new set of values per node is also ranked in ascending order, quantifying the involvement of node’s neighbours in pathology. Finally, we calculate the average ranking of a node in the two lists, reflecting its likelihood to act as a disease epicenter29,52,58,209,210,211.
Epicenter mapping: agent-based spreading model
Disease epicenters can also be identified using a modeling approach known as the agent-based Susceptible-Infected-Removed (SIR) model59. In brief, this model simulates the brain spread of pathology considering the structural connectome as a network through which misfolded proteins (agents) can propagate15 (see Supplementary Information: The S.I.R model for model equations). In the case of ALS, these agents may represent TDP-43108,109,110.
We apply this methodology to find epicenters (model parameters outlined in Table S3). The epicenters are identified as the nodes that—if chosen as the disease’s initial point of pathology (seed region)—will lead to the highest Pearson correlation coefficient value between the simulated and observed cortical atrophy pattern during the spread of the agent. Here, the disease spread simulation is performed over a total of 10,000 time steps. Nodes are then ranked based on the maximum correlation value between the observed patterns of cortical atrophy and the simulated atrophy patterns when each node is used as the initial seed.
Gene category enrichment analysis
Biological processes and cellular components that are correlated with the ALS epicenter likelihood map are identified using a gene category enrichment analysis (GCEA). Cortical maps for biological processes and cellular components are defined according to the gene expression data coming from the AHBA64. The data is preprocessed and mapped to parcellated brain regions using the abagen toolbox, publicly available at https://github.com/rmarkello/abagen168. To perform the enrichment analysis, we use the ABAnnotate Matlab-based toolbox, publicly available at https://github.com/LeonDLotter/ABAnnotate212. The package is adapted from the toolbox initially developed by Fulcher et al. (https://github.com/benfulcher/GeneCategoryEnrichmentAnalysis)65. The GCEA procedure assesses whether genes in a particular category are more correlated with a given brain phenotype than a random phenotype with comparable spatial autocorrelation (ensemble-based null model)65.
To address spatial auto-correlation effects, 30,000 spatially auto-correlated null maps are generated from the epicenter likelihood map using the neuromaps toolbox (method = “vasa”170,213) and are inputted to ABAnnotate package for the testing procedure. After matching category and Allen Human Brain genes based on gene symbols, and removing the genes with differential stability lower than 0.1, the Pearson correlations between the epicenter map, the null maps, and all gene expression maps are calculated. For each null map and each category, null category scores are obtained as the mean z-transformed correlation coefficients. Positive-sided p-values, indicative of the relationship between the epicenter map and each category, are determined by comparing the actual category scores to the null distribution, with subsequent False Discovery Rate (FDR) correction applied. For gene-category annotations, we use the GO biological processes and cellular components214 as well as the cell-type categories introduced by Lake et al.87.
Statistics and reproducibility
The sample sizes, statistical methods used, and validation protocols are described for each result in the relevant subsections. Throughout the manuscript, statistical significance is assumed at p-value smaller than 0.05. In short, we use spin test (or network null models) when assessing the associations among brain maps, see Methods: Null models for more details. Significance of PLS latent variables is assessed by permutation tests. The generalization of PLS results is assessed using cross-validation approach; see Methods: Partial least squares for more details. Comparison of epicenter maps across patient subtypes is done using t-tests per parcel. Whenever multiple comparison correction is needed, the FDR correction is applied.
Null models
Reported associations among brain maps and/or networks are assessed with respect to three null models53. Here we briefly outline the logic and implementation of each. First, to assess the effect of spatial autocorrelation on spatial associations between brain maps, we use the so-called spatial auto-correlation preserving permutation tests, commonly referred to as “spin tests”54. Briefly brain phenotypes (e.g., cortical atrophy maps) are projected to spherical projection of the fsaverage surface. This involves selecting the coordinates of the vertex closest to the center of mass for each parcel. These parcel coordinates are then randomly rotated, and original parcels are reassigned to the value of the closest rotated parcel (n repetitions). For parcels where the medial wall is the closest, we assign the value of the next closest parcel instead. Following these steps, we obtain a series of randomized brain maps that have the same values and spatial autocorrelation as the original map but where the relationship between values and their spatial location has been permuted. These maps are then used to generate null distributions of desired statistics, such as null node-neighbour correlation values215.
When evaluating the role of the structural connectome in disease spread, we use two additional network randomization methods53. One approach constructs degree-preserving randomized networks53,216. In this case, the atrophy map is unchanged, but the structural connectome itself is randomized 1000 times. In each randomization realization, each edge is rewired 10 times to generate a randomized network with the same size, density, and degree sequence as the actual network216. Using these null networks, the Pearson correlation coefficient between node and its neighbours’ is recalculated, and a two-sided p-value is estimated in a non-parametric manner.
Finally, the most conservative approach to test the role of structural connectome in disease spread involves using degree- and edge length-preserving randomized networks. In this approach, the atrophy map is kept unchanged, but the structural connectome is randomized 1000 times to create randomized networks with preserved size, density, degree sequence, and edge length (sometimes referred to as “cost”)53,56. To achieve this, edges within the structural connectome are categorized based on Euclidean distance into 10 bins. Within each bin, pairs of edges are selected randomly and swapped, with the total number of swaps equaling the number of regions in the network multiplied by 20. This process is repeated 1000 times, yielding 1000 randomized structural networks. These randomized networks are then used to construct a null distribution for the node-neighbour Pearson correlation coefficient, and to calculate a two-sided p-value.
Partial least squares
The goal of partial least squares (PLS) analysis is to relate two data matrices to each other97,217. In the present case, the two matrices represent epicenter likelihood maps (participants × regions) and clinical-behavioral data (participants × measures). In the PLS analysis, we included data from 184 ALS participants and excluded data of 8 participants as they had incorrect administration of ECAS scores. We included 62 clinical-behavioral measures per participant; the details of these measures are provided in Table S4. In cases where participant’s data for a measure is missing, it is imputed using the median value from participants for whom the measure is available. For additional information on the number of ALS participants with missing values per measure, refer to Table S7. The analysis is initialized by computing the covariance between brain (X) and behavior features (Y). The resulting covariance matrix is subjected to singular value decomposition:
where U and V are orthonormal matrices of left and right singular vectors and S is a diagonal matrix of singular values. Each combination of a left singular vector, a right singular vector, and a singular value constitutes a latent variable. The elements of each singular vector weight the contribution of individual features to the overall multivariate pattern. In the present analysis, these weights correspond to a spatial pattern of cortical epicenters and clinical phenotypes that optimally covary with each other. To estimate the extent to which individual patients express these atrophy or behavioral patterns, patient-specific brain and behavioral scores are calculated. Scores are computed by projecting the original data onto the respective singular vector weights, such that each individual is assigned a brain and a behavioral score, indicating the degree to which a patient expresses each atrophy pattern and behavioral phenotype97.
The proportion of covariance accounted for by each latent variable is a measure of effect size and is quantified as the ratio of the squared singular value to the sum of all squared singular values. The statistical significance of each latent variable is estimated by permutation testing. This involves randomly permuting the order of observations (i.e., rows) of data matrix X for a total of 1000 repetitions, followed by constructing a set of “null” brain-behavior correlation matrices for the permuted brain and unchanged clinical data matrices. These “null” correlation matrices are then subjected to SVD to generate a distribution of singular values under the null hypothesis that there is no association between brain epicenters and behavioral measures. A non-parametric p-value can be estimated for a given latent variable as the probability that a permuted singular value exceeds the original, non-permuted singular value.
The contribution of individual features to the model is estimated using bootstrap resampling. Participants (rows of data matrices X and Y) are randomly sampled with replacement (1000 repetitions), resulting in resampled correlation matrices that are then subjected to SVD. This bootstrapping procedure generates a sampling distribution for each singular vector weight. A bootstrap ratio for each behavioral measure is then computed, defined as the ratio of its singular vector weight and its bootstrap-estimated standard error. High bootstrap ratios are indicative of features that make a large contribution to the latent variable and are consistent across samplings.
Finally, we use cross-validation to evaluate the out-of-sample correlation between cortical epicenter patterns and behavioral features. We use 100 random divisions of the dataset, allocating half of the data for training and the other half for testing. In each repetition, we apply PLS to the training data and estimate singular vector weights. Subsequently, each realization of the test data is projected onto the derived weights derived from the training set. We then estimate patient-specific scores and their correlation in the test sample. The procedure is repeated 100 times to establish a distribution of out-of-sample correlation values. To assess the statistical significance of these out-of-sample correlation values, we conduct permutation tests (100 repetitions). During each permutation, we shuffle the epicenter matrix rows and repeat the analysis to create a null distribution of correlation coefficients between epicenter and clinical scores in the test sample. This null distribution is then used to estimate a non-parametric p-value.
Somatotopic map from the HCP movement task
To localize the cortical activation boundaries associated with different body part movements, we utilize the Human Connectome Project’s group-average activation maps from the HCP-S1200 release. The group-average activation maps include the average strength of functional activation across 997 healthy young adults (532 female; age: 22–35 years) who completed 3T task fMRI runs (for detailed information on fMRI acquisition parameters and the preprocessing steps, refer to refs. 159,218,219). Here, we incorporate a set of group-average motor task activation maps, which reveal the somatotopic organization of the sensorimotor cortex. These motor tasks are originally developed by Bucker et al.220 and Yeo et al.221 and involve participants responding to visual prompts to execute specific movements. These movements include finger tapping (left and right), toe squeezing (left and right), and tongue moving. Each movement type is performed in a 12 s block, encompassing 10 movements, and is preceded by a 3 second cue. There are two runs per participant in total, each containing 13 blocks: two for tongue movements, four for hand movements (split evenly between right and left), four for foot movements (also evenly split), and three 15-second fixation blocks. To associate Schaefer-400 parcels with specific motor functions, we first threshold the group-average Cohen’s d maps at the vertex level to highlight regions with significant effect sizes (Cohen’s d greater than 1) in each contrast map of interest. Next, we identify parcels in which over 50% of vertices surpassed this threshold value. This method enabled us to link distinct cortical parcels to distinct motor functions.
Contrasting spinal- and bulbar-onset ALS
To compare cortical epicenter likelihood maps between spinal- and bulbar-onset ALS subtypes, we conduct a t-test for each cortical brain parcel. This analysis allows us to identify cortical areas that differ across the two disease subtypes in terms of their capacity to spread the disease. Here, individuals are assigned to the spinal subtype (N = 140) when the onset region is specified as either “upper motor neurons”, “lower motor neurons”, or a combination of both. Conversely, individuals reporting an onset region of “bulbar”, “bulbar-speech”, or “bulbar-speech and bulbar-swallowing” are categorized under the bulbar ALS subtype (N = 38) (see Table S5). We use individual epicenter likelihood maps as inputs for the t-test models, resulting in a map of t-statistics that illustrates the cortical epicenter differences between ALS subtypes. To ensure the reliability of the differences in epicenter locations between the two groups, we apply FDR correction to the p-values from the t-tests (n = 400). This correction signifies three cortical parcels in the right motor/premotor area, involved in the tongue movement, as the regions that have greater epicenter likelihood in the bulbar-onset group.
We also examine the behavioral/clinical differences across the disease subtypes. We compare groups (bulbar- and spinal-onset ALS) using Mann-Whitney U test for each metric, followed by adjustment for multiple comparisons using FDR. 62 different metrics are included for assessment in total, after removing the metrics which are not reported for more than 20 participants. Among the included subjects, 8 had incorrect ECAS administration. For these subjects, we retained them in this analysis by assigning “Not a Number” values for the corresponding ECAS measures, as they still provided useful information for other clinical and behavioral measures. If missing data is available for a measure, it is not incorporated in the t-statistic calculation (see Table S8 for the number of included subjects per measure for each subtype). We find significant differences in metrics including “ALSFRS-Speech” (FDR corrected; two-sided p = 2.58 × 10−14), “ALSFRS-Salivation” (p = 4.88 × 10−8), “ALSFRS-Swallowing” (p = 2.16 × 10−10), “ALSFRS-Dressing&hygiene” (p = 3.63 × 10−2), “ALSFRS-Walking” (p = 2.81 × 10−2), “ALSFRS-Climbingstairs” (p = 1.91 × 10−2); “Reflexes-Jaw” (p = 1.13 × 10−3) and “Reflexes-RightArm” (p = 4.37 × 10−3) (Fig. 6b).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Anonymized data will be shared at the reasonable request of qualified investigators. For more information on the CALSNIC dataset, refer to http://calsnic.org.
Code availability
All codes used to perform the analyses are available on GitHub at https://github.com/netneurolab/Farahani_ALS and on Zenodo at https://zenodo.org/records/15865751 (https://doi.org/10.5281/zenodo.15865751).
References
Cleveland, D. W. & Rothstein, J. D. From Charcot to Lou Gehrig: deciphering selective motor neuron death in als. Nat. Rev. Neurosci. 2, 806–819 (2001).
Al-Chalabi, A. & Hardiman, O. The epidemiology of ALS: a conspiracy of genes, environment and time. Nat. Rev. Neurol. 9, 617–628 (2013).
Masrori, P. & Van Damme, P. Amyotrophic lateral sclerosis: a clinical review. Eur. J. Neurol. 27, 1918–1929 (2020).
Swinnen, B. & Robberecht, W. The phenotypic variability of amyotrophic lateral sclerosis. Nat. Rev. Neurol. 10, 661–670 (2014).
Blokhuis, A. M., Groen, E. J., Koppers, M., van den Berg, L. H. & Pasterkamp, R. J. Protein aggregation in amyotrophic lateral sclerosis. Acta Neuropathol. 125, 777–794 (2013).
Mejzini, R. et al. ALS genetics, mechanisms, and therapeutics: where are we now? Front. Neurosci. 13, 1310 (2019).
Verstraete, E., Veldink, J. H., Mandl, R. C., van den Berg, L. H. & van den Heuvel, M. P. Impaired structural motor connectome in amyotrophic lateral sclerosis. PloS one 6, e24239 (2011).
Schmidt, R., de Reus, M. A., Scholtens, L. H., van den Berg, L. H. & van den Heuvel, M. P. Simulating disease propagation across white matter connectome reveals anatomical substrate for neuropathology staging in amyotrophic lateral sclerosis. Neuroimage 124, 762–769 (2016).
Meier, J. M. et al. Connectome-based propagation model in amyotrophic lateral sclerosis. Ann. Neurol. 87, 725–738 (2020).
Pandya, S. et al. Modeling seeding and neuroanatomic spread of pathology in amyotrophic lateral sclerosis. NeuroImage 251, 118968 (2022).
Nonaka, T. et al. Prion-like properties of pathological TDP-43 aggregates from diseased brains. Cell Rep. 4, 124–134 (2013).
Westergard, T. et al. Cell-to-cell transmission of dipeptide repeat proteins linked to c9orf72-ALS/FTD. Cell Rep. 17, 645–652 (2016).
Münch, C., O’Brien, J. & Bertolotti, A. Prion-like propagation of mutant superoxide dismutase-1 misfolding in neuronal cells. Proc. Natl Acad. Sci. 108, 3548–3553 (2011).
Brettschneider, J. et al. Stages of ptdp-43 pathology in amyotrophic lateral sclerosis. Ann. Neurol. 74, 20–38 (2013).
Brettschneider, J., Tredici, K. D., Lee, V. M.-Y. & Trojanowski, J. Q. Spreading of pathology in neurodegenerative diseases: a focus on human studies. Nat. Rev. Neurosci. 16, 109–120 (2015).
Shaw, P. & Eggett, C. Molecular factors underlying selective vulnerability of motor neurons to neurodegeneration in amyotrophic lateral sclerosis. J. Neurol. 247, I17–I27 (2000).
Saez-Atienzar, S. et al. Genetic analysis of amyotrophic lateral sclerosis identifies contributing pathways and cell types. Sci. Adv. 7, eabd9036 (2021).
Barbeito, L. H. et al. A role for astrocytes in motor neuron loss in amyotrophic lateral sclerosis. Brain Res. Rev. 47, 263–274 (2004).
Rossi, D. et al. Focal degeneration of astrocytes in amyotrophic lateral sclerosis. Cell Death Differ. 15, 1691–1700 (2008).
Månberg, A. et al. Altered perivascular fibroblast activity precedes ALS disease onset. Nat. Med. 27, 640–646 (2021).
Sasaki, S. Alterations of the blood-spinal cord barrier in sporadic amyotrophic lateral sclerosis. Neuropathology 35, 518–528 (2015).
Tam, O. H. et al. Postmortem cortex samples identify distinct molecular subtypes of ALS: retrotransposon activation, oxidative stress, and activated glia. Cell Rep. 29, 1164–1177 (2019).
Kalra, S. et al. The Canadian ALS Neuroimaging Consortium (calsnic)-a multicentre platform for standardized imaging and clinical studies in ALS. MedRxiv 2020–07 (2020).
Ashburner, J. et al. Identifying global anatomical differences: deformation-based morphometry. Hum. Brain Mapp. 6, 348–357 (1998).
Teipel, S. J. et al. Multivariate deformation-based analysis of brain atrophy to predict alzheimer’s disease in mild cognitive impairment. Neuroimage 38, 13–24 (2007).
Borghammer, P. et al. A deformation-based morphometry study of patients with early-stage parkinson’s disease. Eur. J. Neurol. 17, 314–320 (2010).
Dadar, M. et al. Cerebral atrophy in amyotrophic lateral sclerosis parallels the pathological distribution of tdp43. Brain Commun. 2, fcaa061 (2020).
Tremblay, C. et al. Brain atrophy progression in parkinson’s disease is shaped by connectivity and local vulnerability. Brain Commun. 3, fcab269 (2021).
Shafiei, G. et al. Network structure and transcriptomic vulnerability shape atrophy in frontotemporal dementia. Brain 146, 321–336 (2023).
Grosskreutz, J. et al. Widespread sensorimotor and frontal cortical atrophy in amyotrophic lateral sclerosis. BMC Neurol. 6, 1–10 (2006).
Roccatagliata, L., Bonzano, L., Mancardi, G., Canepa, C. & Caponnetto, C. Detection of motor cortex thinning and corticospinal tract involvement by quantitative MRI in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. 10, 47–52 (2009).
Verstraete, E. et al. Structural MRI reveals cortical thinning in amyotrophic lateral sclerosis. J. Neurol. Neurosurg. Psychiatry 83, 383–388 (2012).
Mioshi, E. et al. Cortical atrophy in ALS is critically associated with neuropsychiatric and cognitive changes. Neurology 80, 1117–1123 (2013).
Chen, G. et al. White matter volume loss in amyotrophic lateral sclerosis: a meta-analysis of voxel-based morphometry studies. Prog. Neuro Psychopharmacol. Biol. Psychiatry 83, 110–117 (2018).
Wakana, S. et al. Reproducibility of quantitative tractography methods applied to cerebral white matter. Neuroimage 36, 630–644 (2007).
Hua, K. et al. Tract probability maps in stereotaxic spaces: analyses of white matter anatomy and tract-specific quantification. Neuroimage 39, 336–347 (2008).
Borsodi, F. et al. Multimodal assessment of white matter tracts in amyotrophic lateral sclerosis. PloS one 12, e0178371 (2017).
Prudlo, J. et al. White matter pathology in ALS and lower motor neuron ALS variants: a diffusion tensor imaging study using tract-based spatial statistics. J. Neurol. 259, 1848–1859 (2012).
Menke, R., Proudfoot, M., Talbot, K. & Turner, M. The two-year progression of structural and functional cerebral MRI in amyotrophic lateral sclerosis. NeuroImage Clin. 17, 953–961 (2018).
Agosta, F. et al. Assessment of white matter tract damage in patients with amyotrophic lateral sclerosis: a diffusion tensor MR imaging tractography study. Am. J. Neuroradiol. 31, 1457–1461 (2010).
Du, X.-Q. et al. Brain white matter abnormalities and correlation with severity in amyotrophic lateral sclerosis: An atlas-based diffusion tensor imaging study. J. Neurol. Sci. 405, 116438 (2019).
Geser, F. et al. Evidence of multisystem disorder in whole-brain map of pathological TDP-43 in amyotrophic lateral sclerosis. Arch. Neurol. 65, 636–641 (2008).
Kassubek, J. et al. Diffusion tensor imaging analysis of sequential spreading of disease in amyotrophic lateral sclerosis confirms patterns of TDP-43 pathology. Brain 137, 1733–1740 (2014).
Schaefer, A. et al. Local-global parcellation of the human cerebral cortex from intrinsic functional connectivity MRI. Cereb. Cortex 28, 3095–3114 (2018).
Economo, C. et al. Die cytoarchitektonik der hirnrinde des erwachsenen menschen. Arch NeurPsyche (1925).
von Economo, C. F., Koskinas, G. N. & Triarhou, L. C.Atlas of cytoarchitectonics of the adult human cerebral cortex, vol. 10 (Karger Basel, 2008).
Scholtens, L. H., de Reus, M. A., de Lange, S. C., Schmidt, R. & van den Heuvel, M. P. An mri von economo–koskinas atlas. NeuroImage 170, 249–256 (2018).
Van Essen, D. C. et al. The wu-minn human connectome project: an overview. Neuroimage 80, 62–79 (2013).
Seeley, W. W., Crawford, R. K., Zhou, J., Miller, B. L. & Greicius, M. D. Neurodegenerative diseases target large-scale human brain networks. Neuron 62, 42–52 (2009).
Yau, Y. et al. Network connectivity determines cortical thinning in early parkinson’s disease progression. Nat. Commun. 9, 12 (2018).
Hansen, J. Y. et al. Integrating multimodal and multiscale connectivity blueprints of the human cerebral cortex in health and disease. Plos Biol. 21, e3002314 (2023).
Shafiei, G. et al. Spatial patterning of tissue volume loss in schizophrenia reflects brain network architecture. Biol. Psychiatry 87, 727–735 (2020).
Váša, F. & Mišić, B. Null models in network neuroscience. Nat. Rev. Neurosci. 23, 493–504 (2022).
Alexander-Bloch, A. F. et al. On testing for spatial correspondence between maps of human brain structure and function. Neuroimage 178, 540–551 (2018).
Markello, R. D. & Misic, B. Comparing spatial null models for brain maps. NeuroImage 236, 118052 (2021).
Betzel, R. F. & Bassett, D. S. Specificity and robustness of long-distance connections in weighted, interareal connectomes. Proc. Natl Acad. Sci. 115, E4880–E4889 (2018).
Abdelgawad, A. et al. Predicting longitudinal brain atrophy in parkinson’s disease using a susceptible-infected-removed agent-based model. Netw. Neurosci. 7, 906–925 (2023).
Hansen, J. Y. et al. Local molecular and global connectomic contributions to cross-disorder cortical abnormalities. Nat. Commun. 13, 4682 (2022).
Zheng, Y.-Q. et al. Local vulnerability and global connectivity jointly shape neurodegenerative disease propagation. PLoS Biol. 17, e3000495 (2019).
Rahayel, S. et al. Brain atrophy in prodromal synucleinopathy is shaped by structural connectivity and gene expression. Brain 145, 3162–3178 (2022).
Hansen, J. Y. et al. Mapping neurotransmitter systems to the structural and functional organization of the human neocortex. Nat. Neurosci. 25, 1569–1581 (2022).
Tefera, T. W. & Borges, K. Metabolic dysfunctions in amyotrophic lateral sclerosis pathogenesis and potential metabolic treatments. Front. Neurosci. 10, 611 (2017).
Vandoorne, T., De Bock, K. & Van Den Bosch, L. Energy metabolism in ALS: an underappreciated opportunity? Acta Neuropathol. 135, 489–509 (2018).
Hawrylycz, M. J. et al. An anatomically comprehensive atlas of the adult human brain transcriptome. Nature 489, 391–399 (2012).
Fulcher, B. D., Arnatkeviciute, A. & Fornito, A. Overcoming false-positive gene-category enrichment in the analysis of spatially resolved transcriptomic brain atlas data. Nat. Commun. 12, 2669 (2021).
Schweingruber, C. et al. Single cell RNA sequencing in isogenic Fus and Tardbp mutant ALS lines reveals early mitochondrial dysfunction as a common pathway in motor neurons. bioRxiv 2023–03 (2023).
Nicholls, D. G. Mitochondria and calcium signaling. Cell Calcium 38, 311–317 (2005).
Kawamata, H. & Manfredi, G. Mitochondrial dysfunction and intracellular calcium dysregulation in ALS. Mech. Ageing Dev. 131, 517–526 (2010).
Tefera, T. W., Steyn, F. J., Ngo, S. T. & Borges, K. CNS glucose metabolism in amyotrophic lateral sclerosis: a therapeutic target? Cell Biosci. 11, 1–17 (2021).
Henriques, A. et al. Sphingolipid metabolism is dysregulated at transcriptomic and metabolic levels in the spinal cord of an animal model of amyotrophic lateral sclerosis. Front. Mol. Neurosci. 10, 433 (2018).
Bouscary, A. et al. Sphingolipids metabolism alteration in the central nervous system: amyotrophic lateral sclerosis (ALS) and other neurodegenerative diseases. In Seminars in Cell & Developmental Biology, vol. 112, 82–91 (Elsevier, 2021).
Evans, C. S. & Holzbaur, E. L. Autophagy and mitophagy in als. Neurobiol. Dis. 122, 35–40 (2019).
Madruga, E., Maestro, I. & Martínez, A. Mitophagy modulation, a new player in the race against ALS. Int. J. Mol. Sci. 22, 740 (2021).
Shefa, U. et al. Mitophagy links oxidative stress conditions and neurodegenerative diseases. Neural Regen. Res. 14, 749 (2019).
Altanbyek, V. et al. Imbalance of mitochondrial dynamics in Drosophila models of amyotrophic lateral sclerosis. Biochem. Biophys. Res. Commun. 481, 259–264 (2016).
Knott, A. B. & Bossy-Wetzel, E. Impairing the mitochondrial fission and fusion balance: a new mechanism of neurodegeneration. Ann. N. Y. Acad. Sci. 1147, 283–292 (2008).
Smith, E. F., Shaw, P. J. & De Vos, K. J. The role of mitochondria in amyotrophic lateral sclerosis. Neurosci. Lett. 710, 132933 (2019).
Candelise, N. et al. Mechanistic insights of mitochondrial dysfunction in amyotrophic lateral sclerosis: An update on a lasting relationship. Metabolites 12, 233 (2022).
Lin, B. C. et al. ALS/FTD mutations in ubqln2 are linked to mitochondrial dysfunction through loss-of-function in mitochondrial protein import. Hum. Mol. Genet. 30, 1230–1246 (2021).
Li, Q. et al. Als-linked mutant superoxide dismutase 1 (sod1) alters mitochondrial protein composition and decreases protein import. Proc. Natl. Acad. Sci. USA 107, 21146–21151 (2010).
Yoo, H.-S., Shanmugalingam, U. & Smith, P. D. Potential roles of branched-chain amino acids in neurodegeneration. Nutrition 103, 111762 (2022).
Godoy-Corchuelo, J. M. et al. Lipid metabolic alterations in the ALS–FTD spectrum of disorders. Biomedicines 10, 1105 (2022).
Fransen, M., Nordgren, M., Wang, B., Apanasets, O. & Van Veldhoven, P. P. Aging, age-related diseases and peroxisomes. Peroxisomes and their key role in cellular signaling and metabolism 45–65 (2013).
Genç, B. et al. Apical dendrite degeneration, a novel cellular pathology for Betz cells in ALS. Sci. Rep. 7, 41765 (2017).
Wang, W., Zhou, Y. & Bi, R. Correlating genes and functions to human disease by systematic differential analysis of expression profiles. In International Conference on Intelligent Computing, 11–20 (Springer, 2005).
Liu, X. & Henty-Ridilla, J. L. Multiple roles for the cytoskeleton in ALS. Exp. Neurol. 355, 114143 (2022).
Lake, B. B. et al. Integrative single-cell analysis of transcriptional and epigenetic states in the human adult brain. Nat. Biotechnol. 36, 70–80 (2018).
Winkler, E. A. et al. Blood–spinal cord barrier breakdown and pericyte reductions in amyotrophic lateral sclerosis. Acta Neuropathol. 125, 111–120 (2013).
Coatti, G. C., Cavaçana, N. & Zatz, M. The role of pericytes in amyotrophic lateral sclerosis. Pericyte Biol. Disease 137–146 (2019).
Yamadera, M. et al. Microvascular disturbance with decreased pericyte coverage is prominent in the ventral horn of patients with amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Frontotemporal Degen. 16, 393–401 (2015).
Saul, J. et al. Global alterations to the choroid plexus blood-CSF barrier in amyotrophic lateral sclerosis. Acta Neuropathol. Commun. 8, 1–21 (2020).
Mirian, A. et al. Breached barriers: a scoping review of blood-central nervous system barrier pathology in amyotrophic lateral sclerosis. Front. Cell. Neurosci. 16, 851563 (2022).
Garbuzova-Davis, S. et al. Impaired blood–brain/spinal cord barrier in ALS patients. Brain Res. 1469, 114–128 (2012).
Kakaroubas, N., Brennan, S., Keon, M. & Saksena, N. K. Pathomechanisms of blood-brain barrier disruption in als. Neurosci. J. 2019, 2537698 (2019).
Zhong, Z. et al. ALS-causing sod1 mutants generate vascular changes prior to motor neuron degeneration. Nat. Neurosci. 11, 420–422 (2008).
Steinruecke, M. et al. Blood-CNS barrier dysfunction in amyotrophic lateral sclerosis: Proposed mechanisms and clinical implications. J. Cereb. Blood Flow. Metab. 43, 642–654 (2023).
McIntosh, A. R. & Mišić, B. Multivariate statistical analyses for neuroimaging data. Annu. Rev. Psychol. 64, 499–525 (2013).
Zeighami, Y. et al. A clinical-anatomical signature of parkinson’s disease identified with partial least squares and magnetic resonance imaging. Neuroimage 190, 69–78 (2019).
Kirschner, M. et al. Latent clinical-anatomical dimensions of schizophrenia. Schizophr. Bull. 46, 1426–1438 (2020).
Ravits, J. M. & La Spada, A. R. ALS motor phenotype heterogeneity, focality, and spread: deconstructing motor neuron degeneration. Neurology 73, 805–811 (2009).
Hillel, A. D. & Miller, R. Bulbar amyotrophic lateral sclerosis: patterns of progression and clinical management. Head. Neck 11, 51–59 (1989).
Kühnlein, P. et al. Diagnosis and treatment of bulbar symptoms in amyotrophic lateral sclerosis. Nat. Clin. Pract. Neurol. 4, 366–374 (2008).
Shoesmith, C. L., Findlater, K., Rowe, A. & Strong, M. J. Prognosis of amyotrophic lateral sclerosis with respiratory onset. J. Neurol., Neurosurg. Psychiatry 78, 629–631 (2007).
Rajimehr, R., Firoozi, A., Rafipoor, H., Abbasi, N. & Duncan, J. Complementary hemispheric lateralization of language and social processing in the human brain. Cell Rep. 41, 111617 (2022).
Makkonen, T., Ruottinen, H., Puhto, R., Helminen, M. & Palmio, J. Speech deterioration in amyotrophic lateral sclerosis (ALS) after manifestation of bulbar symptoms. Int. J. Lang. Commun. Disord. 53, 385–392 (2018).
Penfield, W. & Boldrey, E. Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain 60, 389–443 (1937).
Rizzolatti, G., Luppino, G. & Matelli, M. The organization of the cortical motor system: new concepts. Electroencephalogr. Clin. Neurophysiol. 106, 283–296 (1998).
Warren, J. D. et al. Molecular nexopathies: a new paradigm of neurodegenerative disease. Trends Neurosci. 36, 561–569 (2013).
Scotter, E. L., Chen, H.-J. & Shaw, C. E. Tdp-43 proteinopathy and ALS: insights into disease mechanisms and therapeutic targets. Neurotherapeutics 12, 352–363 (2015).
Carbonell, F., Iturria-Medina, Y. & Evans, A. C. Mathematical modeling of protein misfolding mechanisms in neurological diseases: a historical overview. Front. Neurol. 9, 37 (2018).
Li, W. et al. Disruption of the white matter structural network and its correlation with baseline progression rate in patients with sporadic amyotrophic lateral sclerosis. Transl. Neurodegen. 10, 1–12 (2021).
Ellis, C. et al. Diffusion tensor mri assesses corticospinal tract damage in als. Neurology 53, 1051–1051 (1999).
Filippini, N. et al. Corpus callosum involvement is a consistent feature of amyotrophic lateral sclerosis. Neurology 75, 1645–1652 (2010).
Senda, J. et al. Progressive and widespread brain damage in ALS: MRI voxel-based morphometry and diffusion tensor imaging study. Amyotroph. Lateral Scler. 12, 59–69 (2011).
Desplats, P. et al. Inclusion formation and neuronal cell death through neuron-to-neuron transmission of α-synuclein. Proc. Natl. Acad. Sci. USA 106, 13010–13015 (2009).
Brundin, P., Melki, R. & Kopito, R. Prion-like transmission of protein aggregates in neurodegenerative diseases. Nat. Rev. Mol. Cell Biol. 11, 301–307 (2010).
Kovacs, G. G. et al. Intracellular processing of disease-associated α-synuclein in the human brain suggests prion-like cell-to-cell spread. Neurobiol. Dis. 69, 76–92 (2014).
Guo, J. L. & Lee, V. M. Cell-to-cell transmission of pathogenic proteins in neurodegenerative diseases. Nat. Med. 20, 130–138 (2014).
Calafate, S. et al. Synaptic contacts enhance cell-to-cell tau pathology propagation. Cell Rep. 11, 1176–1183 (2015).
Masuda-Suzukake, M. et al. Prion-like spreading of pathological α-synuclein in brain. Brain 136, 1128–1138 (2013).
Ahmed, Z. et al. A novel in vivo model of tau propagation with rapid and progressive neurofibrillary tangle pathology: the pattern of spread is determined by connectivity, not proximity. Acta Neuropathol. 127, 667–683 (2014).
Vogel, J. W. et al. Spread of pathological tau proteins through communicating neurons in human alzheimer’s disease. Nat. Commun. 11, 2612 (2020).
Luk, K. C. et al. Pathological α-synuclein transmission initiates Parkinson-like neurodegeneration in nontransgenic mice. Science 338, 949–953 (2012).
De Calignon, A. et al. Propagation of tau pathology in a model of early alzheimer’s disease. Neuron 73, 685–697 (2012).
Raj, A., Kuceyeski, A. & Weiner, M. A network diffusion model of disease progression in dementia. Neuron 73, 1204–1215 (2012).
Henderson, M. X. et al. Spread of α-synuclein pathology through the brain connectome is modulated by selective vulnerability and predicted by network analysis. Nat. Neurosci. 22, 1248–1257 (2019).
Scekic-Zahirovic, J. et al. Evidence that corticofugal propagation of ALS pathology is not mediated by prion-like mechanism. Prog. Neurobiol. 200, 101972 (2021).
Dupuis, L., Pradat, P.-F., Ludolph, A. C. & Loeffler, J.-P. Energy metabolism in amyotrophic lateral sclerosis. Lancet Neurol. 10, 75–82 (2011).
Van Weehaeghe, D. et al. Is there a glucose metabolic signature of spreading TDP-43 pathology in amyotrophic lateral sclerosis? Q. J. Nucl. Med. Mol. Imaging 64, 96–104 (2017).
Verstraete, E., Veldink, J. H., van den Berg, L. H. & Van den Heuvel, M. P. Structural brain network imaging shows expanding disconnection of the motor system in amyotrophic lateral sclerosis. Hum. Brain Mapp. 35, 1351–1361 (2014).
Pannoni, K. E. et al. The mitochondrial calcium uniporter is necessary for synaptic plasticity and proper mitochondrial morphology and distribution in the distal dendrites of CA2 neurons. bioRxiv 2023–11 (2023).
Kadry, H., Noorani, B. & Cucullo, L. A blood–brain barrier overview on structure, function, impairment, and biomarkers of integrity. Fluids Barriers CNS 17, 1–24 (2020).
Zlokovic, B. V. The blood-brain barrier in health and chronic neurodegenerative disorders. Neuron 57, 178–201 (2008).
Zlokovic, B. V. Neurovascular pathways to neurodegeneration in alzheimer’s disease and other disorders. Nat. Rev. Neurosci. 12, 723–738 (2011).
Wu, Y., Yang, X., Li, X., Wang, H. & Wang, T. Elevated cerebrospinal fluid homocysteine is associated with blood-brain barrier disruption in amyotrophic lateral sclerosis patients. Neurol. Sci. 41, 1865–1872 (2020).
Garbuzova-Davis, S. et al. Evidence of compromised blood-spinal cord barrier in early and late symptomatic sod1 mice modeling ALS. PloS one 2, e1205 (2007).
Garbuzova-Davis, S. et al. Ultrastructure of blood–brain barrier and blood–spinal cord barrier in sod1 mice modeling als. Brain Res. 1157, 126–137 (2007).
Miyazaki, K. et al. Disruption of neurovascular unit prior to motor neuron degeneration in amyotrophic lateral sclerosis. J. Neurosci. Res. 89, 718–728 (2011).
Leonardi, A., Abbruzzese, G., Arata, L., Cocito, L. & Vische, M. Cerebrospinal fluid (CSF) findings in amyotrophic lateral sclerosis. J. Neurol. 231, 75–78 (1984).
Annunziata, P. & Volpi, N. High levels of c3c in the cerebrospinal fluid from amyotrophic lateral sclerosis patients. Acta Neurol. Scand. 72, 61–64 (1985).
Garbuzova-Davis, S. et al. Endothelial and astrocytic support by human bone marrow stem cell grafts into symptomatic ALS mice towards blood-spinal cord barrier repair. Sci. Rep. 7, 884 (2017).
Coatti, G. C. et al. Pericytes extend survival of ALS sod1 mice and induce the expression of antioxidant enzymes in the murine model and in iPSCs derived neuronal cells from an ALS patient. Stem Cell Rev. Rep. 13, 686–698 (2017).
Van Der Burgh, H. K. et al. Multimodal longitudinal study of structural brain involvement in amyotrophic lateral sclerosis. Neurology 94, e2592–e2604 (2020).
Bhattarai, A. et al. Network diffusion model predicts neurodegeneration in limb-onset amyotrophic lateral sclerosis. Plos One 17, e0272736 (2022).
Coffey, C. E., Saxton, J., Ratcliff, G., Bryan, R. & Lucke, J. Relation of education to brain size in normal aging: implications for the reserve hypothesis. Neurology 53, 189–189 (1999).
Good, C. D. et al. Cerebral asymmetry and the effects of sex and handedness on brain structure: a voxel-based morphometric analysis of 465 normal adult human brains. Neuroimage 14, 685–700 (2001).
Amunts, K. et al. Asymmetry in the human motor cortex and handedness. Neuroimage 4, 216–222 (1996).
Brooks, B. R. et al. El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. other Mot. Neuron Disord. 1, 293–299 (2000).
Cedarbaum, J. M. et al. The alsfrs-r: a revised als functional rating scale that incorporates assessments of respiratory function. J. Neurol. Sci. 169, 13–21 (1999).
Abrahams, S., Newton, J., Niven, E., Foley, J. & Bak, T. H. Screening for cognition and behaviour changes in ALS. Amyotroph. Lateral Scler. Front. Degener. 15, 9–14 (2014).
Coupé, P. et al. An optimized blockwise nonlocal means denoising filter for 3-d magnetic resonance images. IEEE Trans. Med. imaging 27, 425–441 (2008).
Sled, J. G., Zijdenbos, A. P. & Evans, A. C. A nonparametric method for automatic correction of intensity nonuniformity in MRI data. IEEE Trans. Med. imaging 17, 87–97 (1998).
Gaser, C., Volz, H.-P., Kiebel, S., Riehemann, S. & Sauer, H. Detecting structural changes in whole brain based on nonlinear deformations-application to schizophrenia research. Neuroimage 10, 107–113 (1999).
Chung, M. K. et al. A unified statistical approach to deformation-based morphometry. NeuroImage 14, 595–606 (2001).
Jack, C. R. et al. Medial temporal atrophy on MRI in normal aging and very mild alzheimer’s disease. Neurology 49, 786–794 (1997).
Avants, B. B., Tustison, N. & Song, G. et al. Advanced normalization tools (ants). Insight J. 2, 1–35 (2009).
Avants, B. B. et al. A reproducible evaluation of ants similarity metric performance in brain image registration. Neuroimage 54, 2033–2044 (2011).
Bazinet, V. et al. Assortative mixing in micro-architecturally annotated brain connectomes. Nat. Commun. 14, 2850 (2023).
Glasser, M. F. et al. The minimal preprocessing pipelines for the human connectome project. Neuroimage 80, 105–124 (2013).
Tournier, J.-D. et al. Mrtrix3: A fast, flexible and open software framework for medical image processing and visualisation. Neuroimage 202, 116137 (2019).
Smith, R. E., Tournier, J.-D., Calamante, F. & Connelly, A. Anatomically-constrained tractography: improved diffusion MRI streamlines tractography through effective use of anatomical information. Neuroimage 62, 1924–1938 (2012).
Jeurissen, B., Tournier, J.-D., Dhollander, T., Connelly, A. & Sijbers, J. Multi-tissue constrained spherical deconvolution for improved analysis of multi-shell diffusion MRI data. NeuroImage 103, 411–426 (2014).
Smith, R. E., Tournier, J.-D., Calamante, F. & Connelly, A. Sift2: Enabling dense quantitative assessment of brain white matter connectivity using streamlines tractography. Neuroimage 119, 338–351 (2015).
Park, B.-y et al. Signal diffusion along connectome gradients and inter-hub routing differentially contribute to dynamic human brain function. Neuroimage 224, 117429 (2021).
Betzel, R. F., Griffa, A., Hagmann, P. & Mišić, B. Distance-dependent consensus thresholds for generating group-representative structural brain networks. Netw. Neurosci. 3, 475–496 (2019).
Jamadar, S. D. et al. Simultaneous bold-fMRI and constant infusion FDG-PET data of the resting human brain. Sci. Data 7, 363 (2020).
Voigt, K. et al. Metabolic and functional connectivity provide unique and complementary insights into cognition-connectome relationships. Cereb. Cortex 33, 1476–1488 (2023).
Markello, R. D. et al. Standardizing workflows in imaging transcriptomics with the ABagen toolbox. elife 10, e72129 (2021).
Romero-Garcia, R. et al. Structural covariance networks are coupled to expression of genes enriched in supragranular layers of the human cortex. Neuroimage 171, 256–267 (2018).
Markello, R. D. et al. Neuromaps: structural and functional interpretation of brain maps. Nat. Methods 19, 1472–1479 (2022).
Kaller, S. et al. Test–retest measurements of dopamine d 1-type receptors using simultaneous PET/MRI imaging. Eur. J. Nucl. Med. Mol. imaging 44, 1025–1032 (2017).
Smith, C. T. et al. Partial-volume correction increases estimated dopamine d2-like receptor binding potential and reduces adult age differences. J. Cereb. Blood Flow. Metab. 39, 822–833 (2019).
Sandiego, C. M. et al. Reference region modeling approaches for amphetamine challenge studies with [11c] flb 457 and PET. J. Cereb. Blood Flow. Metab. 35, 623–629 (2015).
Zakiniaeiz, Y. et al. Sex differences in amphetamine-induced dopamine release in the dorsolateral prefrontal cortex of tobacco smokers. Neuropsychopharmacology 44, 2205–2211 (2019).
Slifstein, M. et al. Deficits in prefrontal cortical and extrastriatal dopamine release in schizophrenia: a positron emission tomographic functional magnetic resonance imaging study. JAMA Psychiatry 72, 316–324 (2015).
Sandiego, C. M. et al. The effect of treatment with guanfacine, an alpha2 adrenergic agonist, on dopaminergic tone in tobacco smokers: an [11c] flb457 PET study. Neuropsychopharmacology 43, 1052–1058 (2018).
Dukart, J. et al. Cerebral blood flow predicts differential neurotransmitter activity. Sci. Rep. 8, 1–11 (2018).
Ding, Y.-S. et al. PET imaging of the effects of age and cocaine on the norepinephrine transporter in the human brain using (s, s)-[11c] o-methylreboxetine and hrrt. Synapse 64, 30–38 (2010).
Sanchez-Rangel, E. et al. Norepinephrine transporter availability in brown fat is reduced in obesity: a human PET study with [11c] MRB. Int. J. Obes. 44, 964–967 (2020).
Belfort-DeAguiar, R. et al. Noradrenergic activity in the human brain: a mechanism supporting the defense against hypoglycemia. J. Clin. Endocrinol. Metab. 103, 2244–2252 (2018).
Savli, M. et al. Normative database of the serotonergic system in healthy subjects using multi-tracer PET. Neuroimage 63, 447–459 (2012).
Gallezot, J.-D. et al. Kinetic modeling of the serotonin 5-HT1b receptor radioligand [11c] p943 in humans. J. Cereb. Blood Flow. Metab. 30, 196–210 (2010).
Murrough, J. W. et al. Reduced ventral striatal/ventral pallidal serotonin 1b receptor binding potential in major depressive disorder. Psychopharmacology 213, 547–553 (2011).
Murrough, J. W. et al. The effect of early trauma exposure on serotonin type 1b receptor expression revealed by reduced selective radioligand binding. Arch. Gen. Psychiatry 68, 892–900 (2011).
Matuskey, D. et al. Reductions in brain 5-HT1b receptor availability in primarily cocaine-dependent humans. Biol. Psychiatry 76, 816–822 (2014).
Pittenger, C. et al. Ocd is associated with an altered association between sensorimotor gating and cortical and subcortical 5-HT1b receptor binding. J. Affect. Disord. 196, 87–96 (2016).
Saricicek, A. et al. Test–retest reliability of the novel 5-HT1b receptor PET radioligand [11C] p943. Eur. J. Nucl. Med. Mol. imaging 42, 468–477 (2015).
Baldassarri, S. R. et al. Inverse changes in raphe and cortical 5-ht1b receptor availability after acute tryptophan depletion in healthy human subjects. Synapse 74, e22159 (2020).
Beliveau, V. et al. A high-resolution in vivo atlas of the human brain’s serotonin system. J. Neurosci. 37, 120–128 (2017).
Radhakrishnan, R. et al. Age-related change in 5-HT6 receptor availability in healthy male volunteers measured with 11C-gsk215083 PET. J. Nucl. Med. 59, 1445–1450 (2018).
Radhakrishnan, R. et al. In vivo 5-HT6 and 5-HT2a receptor availability in antipsychotic treated schizophrenia patients vs. unmedicated healthy humans measured with [11C] GSK215083 PET. Psychiatry Res. Neuroimaging 295, 111007 (2020).
Hillmer, A. T. et al. Imaging of cerebral α4β2* nicotinic acetylcholine receptors with (-)-[18f] flubatine PET: Implementation of bolus plus constant infusion and sensitivity to acetylcholine in human brain. Neuroimage 141, 71–80 (2016).
Baldassarri, S. R. et al. Use of electronic cigarettes leads to significant beta2-nicotinic acetylcholine receptor occupancy: evidence from a PET imaging study. Nicotine Tob. Res. 20, 425–433 (2018).
Naganawa, M. et al. First-in-human assessment of 11C-lsn3172176, an M1 muscarinic acetylcholine receptor PET radiotracer. J. Nucl. Med. 62, 553–560 (2021).
Aghourian, M. et al. Quantification of brain cholinergic denervation in alzheimer’s disease using PET imaging with [18F]-feobv. Mol. psychiatry 22, 1531–1538 (2017).
Bedard, M.-A. et al. Brain cholinergic alterations in idiopathic REM sleep behaviour disorder: a PET imaging study with 18F-FEObv. Sleep. Med. 58, 35–41 (2019).
DuBois, J. M. et al. Characterization of age/sex and the regional distribution of mGluR5 availability in the healthy human brain measured by high-resolution [11C] abp688 PET. Eur. J. Nucl. Med. Mol. imaging 43, 152–162 (2016).
Smart, K. et al. Sex differences in [11C] abp688 binding: a positron emission tomography study of mGlu5 receptors. Eur. J. Nucl. Med. Mol. Imaging 46, 1179–1183 (2019).
Nørgaard, M. et al. A high-resolution in vivo atlas of the human brain’s benzodiazepine binding site of GABAa receptors. NeuroImage 232, 117878 (2021).
Gallezot, J.-D. et al. Determination of receptor occupancy in the presence of mass dose:[11C] GSK189254 PET imaging of histamine h3 receptor occupancy by PF-03654746. J. Cereb. Blood Flow. Metab. 37, 1095–1107 (2017).
Normandin, M. D. et al. Imaging the cannabinoid cb1 receptor in humans with [11c] omar: assessment of kinetic analysis methods, test–retest reproducibility, and gender differences. J. Cereb. Blood Flow. Metab. 35, 1313–1322 (2015).
D’Souza, D. C. et al. Rapid changes in cannabinoid 1 receptor availability in cannabis-dependent male subjects after abstinence from cannabis. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 1, 60–67 (2016).
Ranganathan, M. et al. Reduced brain cannabinoid receptor availability in schizophrenia. Biol. Psychiatry 79, 997–1005 (2016).
Neumeister, A. et al. Positron emission tomography shows elevated cannabinoid CB1 receptor binding in men with alcohol dependence. Alcohol. Clin. Exp. Res. 36, 2104–2109 (2012).
Kantonen, T. et al. Interindividual variability and lateralization of μ-opioid receptors in the human brain. NeuroImage 217, 116922 (2020).
Paquola, C. et al. Microstructural and functional gradients are increasingly dissociated in transmodal cortices. PLoS Biol. 17, e3000284 (2019).
Amunts, K. et al. Bigbrain: an ultrahigh-resolution 3d human brain model. Science 340, 1472–1475 (2013).
Paquola, C. et al. The bigbrainwarp toolbox for integration of bigbrain 3d histology with multimodal neuroimaging. Elife 10, e70119 (2021).
Pandya, S., Mezias, C. & Raj, A. Predictive model of spread of progressive supranuclear palsy using directional network diffusion. Front. Neurol. 8, 692 (2017).
Brown, J. A. et al. Patient-tailored, connectivity-based forecasts of spreading brain atrophy. Neuron 104, 856–868 (2019).
Seeley, W. W. Mapping neurodegenerative disease onset and progression. Cold Spring Harb. Perspect. Biol. 9, a023622 (2017).
Lotter, L. D., Dukart, J. & Fulcher, B. D. ABAnnotate: A toolbox for ensemble-based multimodal gene-category enrichment analysis of human neuroimaging data https://doi.org/10.5281/zenodo.6463329 (2022).
Váša, F. et al. Adolescent tuning of association cortex in human structural brain networks. Cereb. Cortex 28, 281–294 (2018).
Ashburner, M. et al. Gene ontology: tool for the unification of biology. Nat. Genet. 25, 25–29 (2000).
Vázquez-Rodríguez, B. et al. Gradients of structure–function tethering across neocortex. Proc. Natl Acad. Sci. 116, 21219–21227 (2019).
Maslov, S. & Sneppen, K. Specificity and stability in topology of protein networks. Science 296, 910–913 (2002).
McIntosh, A. R. & Lobaugh, N. J. Partial least squares analysis of neuroimaging data: applications and advances. Neuroimage 23, S250–S263 (2004).
Uğurbil, K. et al. Pushing spatial and temporal resolution for functional and diffusion MRI in the human connectome project. Neuroimage 80, 80–104 (2013).
Barch, D. M. et al. Function in the human connectome: task-fMRI and individual differences in behavior. Neuroimage 80, 169–189 (2013).
Buckner, R. L., Krienen, F. M., Castellanos, A., Diaz, J. C. & Yeo, B. T. The organization of the human cerebellum estimated by intrinsic functional connectivity. J. Neurophysiol. 106, 2322–2345 (2011).
Yeo, B. T. et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol. 106, 1125–1165 (2011).
Glasser, M. F. et al. A multi-modal parcellation of human cerebral cortex. Nature 536, 171–178 (2016).
Blank, S. C., Scott, S. K., Murphy, K., Warburton, E. & Wise, R. J. Speech production: Wernicke, Broca and beyond. Brain 125, 1829–1838 (2002).
Acknowledgements
We thank Filip Milisav, Andrea Luppi, Zhen-Qi Liu, Eric G. Ceballos, Moohebat Pourmajidian, and Alicja Monaghan for their comments and suggestions on the manuscript. BM acknowledges support from the Natural Sciences and Engineering Research Council of Canada (NSERC), Canadian Institutes of Health Research (CIHR), Brain Canada Foundation Future Leaders Fund, the Canada Research Chairs Program, the Michael J. Fox Foundation, and the Healthy Brains for Healthy Lives initiative. The Canadian ALS Neuroimaging Consortium (CALSNIC) is supported by grants from CIHR, ALS Society of Canada, Brain Canada Foundation, and the Shelly Mrkonjic Research Fund.
Author information
Authors and Affiliations
Contributions
Conception of project: A.F., M.D., S.K., A.D., B.M. Analysis: A.F. Writing—original draft: A.F., B.M. Writing—editing: J.Y.H., V.B., G.S., D.L.C., M.D., S.K., A.D.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Biology thanks Jil Meier and the other anonymous reviewer(s) for their contribution to the peer review of this work. Primary Handling Editors: Jasmine Pan.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Farahani, A., Hansen, J.Y., Bazinet, V. et al. Network spreading and local biological vulnerability in amyotrophic lateral sclerosis. Commun Biol 8, 1153 (2025). https://doi.org/10.1038/s42003-025-08561-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s42003-025-08561-3
