
Abstract
Over 50% of persons with unresectable stage III non-small cell lung cancer (NSCLC) treated with standard-of-care concurrent chemoradiotherapy (CCRT) and durvalumab consolidation progress or die within 18 months. Here adults with untreated, unresectable stage III NSCLC were randomized to nivolumab plus CCRT followed by consolidation with nivolumab plus ipilimumab (arm A) or nivolumab alone (arm B) or CCRT followed by consolidation with durvalumab (arm C). The primary endpoint was progression-free survival (PFS) in arm A versus arm C and secondary endpoints included overall survival (OS), PFS in arm B versus arm C, response rates and safety. At a median follow-up of 30.5 months, there was no statistically significant difference in the primary endpoint of PFS in the nivolumab plus ipilimumab arm versus durvalumab arm (hazard ratio (HR): 0.95, 96% confidence interval (CI): 0.77–1.19; P = 0.65). Descriptive OS analysis showed no improvement (HR: 1.12, 95% CI: 0.87–1.43). Nivolumab alone did not improve PFS or OS versus durvalumab (PFS, HR: 0.84, 95% CI: 0.69–1.04; OS, HR: 0.97, 95% CI: 0.76–1.24). Nivolumab plus ipilimumab and nivolumab alone plus CCRT resulted in increased pneumonitis. These results emphasize the need for novel efficacious treatments for these individuals. (ClinicalTrials.gov: NCT04026412)
Similar content being viewed by others


Main
Locally advanced stage III non-small cell lung cancer (NSCLC) represents approximately 30% of NSCLC cases1. Concurrent chemoradiotherapy (CCRT) followed by durvalumab consolidation is the standard of care (SOC) for these persons on the basis of results from the phase 3 PACIFIC study, which showed significantly improved progression-free survival (PFS) with durvalumab versus placebo consolidation (hazard ratio (HR): 0.52, 95% confidence interval (CI): 0.42–0.65; P < 0.001)2. Despite this benefit, more than 50% of participants experienced disease progression or death within 18 months (18-month PFS rate of 44%)2 and the 5-year overall survival (OS) rate was 43% (ref. 3). Thus, there remains an unmet need for an efficacious and safe treatment regimen that improves long-term outcomes and cure rates for persons with locally advanced, unresectable, stage III NSCLC.
Combined radiotherapy and immunotherapy (IO) approaches have been investigated in the treatment of NSCLC to exploit their complementary and potentially synergistic mechanisms. Radiotherapy primes a broad T cell response4, while immune checkpoint inhibitors prevent exhaustion and suppression, converting a local immunogenic event into a systemic, durable antitumor response5,6,7. In preclinical NSCLC models, radiotherapy plus anti-programmed death ligand 1 (PDL1) therapy has achieved superior tumor control and off-target responses compared to either alone6,7,8. Consolidative therapy with anti-cytotoxic T lymphocyte antigen 4 (CTLA4) therapy may further enhance this synergy by promoting T cell activation, reducing regulatory T cells (Tregs) and supporting durable immune control9.
On the basis of this rationale, it has been hypothesized that the addition of IO earlier in combination with CCRT may improve outcomes. Several phase 2 studies in participants with stage III NSCLC assessing a concurrent approach demonstrated promising clinical benefits10,11,12. In the single-arm NICOLAS study, nivolumab (an anti-programmed death protein 1 (PD1) antibody), in combination with CCRT and used as consolidation, resulted in a 1-year PFS rate of 54% (ref. 10). Similarly, pembrolizumab (an anti-PD1 antibody) plus CCRT (KEYNOTE-799) also demonstrated promising antitumor activity (1-year PFS of 67%)11. Lastly, in the DETERRED study, chemoradiation with concurrent and/or consolidation atezolizumab (an anti-PDL1 antibody) resulted in a 1-year PFS of 50% and 57%, respectively13. All three studies demonstrated manageable safety profiles10,11,13; collectively, these results suggested an opportunity for the use of IO plus CCRT in stage III NSCLC.
The combination of nivolumab plus ipilimumab, with or without chemotherapy, has demonstrated long-term, durable survival benefits over chemotherapy alone as a first-line treatment in metastatic NSCLC, regardless of tumor PDL1 expression, in the CheckMate 9LA (ref. 14) and CheckMate 227 (ref. 15) studies. These data led to the hypothesis that this dual IO combination as consolidation after CCRT may further enhance antitumor activity in persons with untreated, unresectable stage III NSCLC.
We conducted the phase 3 CheckMate 73L (NCT04026412) study to compare concomitant nivolumab plus CCRT followed by nivolumab plus ipilimumab (nivolumab plus ipilimumab arm) or nivolumab alone (nivolumab arm) versus CCRT followed by durvalumab (durvalumab arm) in participants with untreated, locally advanced, unresectable stage III NSCLC. Here, we report the final efficacy and safety results.
Results
Participant and tumor characteristics
Between November 2019 and November 2022, a total of 1,787 previously untreated individuals with unresectable stage III NSCLC from 159 sites in 26 countries were screened, of whom 925 were randomized to the nivolumab plus ipilimumab arm (n = 287), nivolumab arm (n = 320) or durvalumab arm (n = 318) (Fig. 1). Baseline participant and clinical characteristics were similar across the three arms (Table 1). Across all arms, most participants (~78%) had stage IIIA or IIIB disease and up to 58% had tumors with squamous histology. More than 60% of the participants had tumor PDL1 ≥ 1% and one third had tumor PDL1 ≥ 50%.

The data cutoff date was March 22, 2024. The database lock date was April 26, 2024. The median follow-up duration (range) was 30.5 months (16.0–52.5 months). Arm A, nivolumab plus ipilimumab treatment; arm B, nivolumab treatment; arm C, durvalumab treatment. aNCT04026412. bUp to three cycles with 21 days per cycle. If radiotherapy planning is complete before the initiation of systemic anticancer therapy at cycle 1 of the CCRT period (arms A, B or C), cycle 1 may have been skipped and treatment initiated with concurrent radiotherapy and systemic anticancer therapy (started at cycle 2). cParticipants with squamous tumor histology received etoposide plus cisplatin or paclitaxel plus carboplatin. Participants with nonsquamous tumor histology received etoposide plus cisplatin, paclitaxel plus carboplatin or pemetrexed plus cisplatin. Chemo, chemotherapy; DURVA, durvalumab; IPI, ipilimumab; NIVO, nivolumab; Q#W, every # weeks; RT, radiotherapy.
Treatment summary
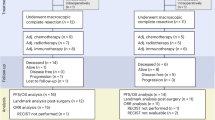
Data cutoff and database lock dates were March 22, 2024 and April 26, 2024, respectively (median follow-up duration: 30.5 months; range: 16.0–52.5 months). At the data cutoff, nearly all randomized participants received CCRT (nivolumab plus ipilimumab, 98.3%; nivolumab alone, 99.4%; durvalumab, 99.7%). Approximately 80% received at least one cycle of consolidation therapy (78%, 83% and 82%, respectively) and fewer than half of the participants completed both CCRT and consolidation treatment (36%, 43% and 45%, respectively) (Fig. 2). The most common reasons for discontinuation during the consolidation phase were disease progression (19%, 23% and 24%, respectively) and study drug toxicity (20%, 14% and 8%, respectively), with pneumonitis being the most common treatment-related adverse event (TRAE) leading to discontinuation in the nivolumab plus ipilimumab (6%) and nivolumab alone (5%) arms.

aOther includes participants requesting to discontinue study drug, no longer meeting criteria, withdrawing consent, dying or being lost to follow-up. bAll nine participants were off treatment. cParticipants completed treatment with both nivolumab and ipilimumab.
During the CCRT phase, exposure to chemotherapy (median, three cycles) and radiotherapy (median cumulative dose, 60 Gy) was similar across all arms. Nivolumab exposure was also comparable between the nivolumab plus ipilimumab arm and nivolumab arm (median, three doses) (Supplementary Table 1). In the consolidation phase, the median duration of therapy was approximately 10 months and was generally comparable across the treatment arms.
PFS and OS endpoints
There was no statistically significant difference observed in the primary endpoint of PFS by blinded independent central review (BICR) between the nivolumab plus ipilimumab and durvalumab arms. The median PFS was 16.7 months in the nivolumab plus ipilimumab arm and 15.6 months in the durvalumab arm, with an HR of 0.95 (96% CI, 0.77–1.19; P = 0.65) (Fig. 3a).

a,b, PFS by BICR in the intent-to-treat population (a) and participant subgroups (b). Symbols (tick marks) indicate censored data. A stratified two-sided log-rank test was used to compare PFS between the nivolumab plus ipilimumab arm and durvalumab arm. A Cox proportional hazards model with treatment as the single covariate was used to estimate the HR and corresponding CI.
Post hoc PFS analysis by key subgroups showed no improvement with nivolumab plus ipilimumab versus durvalumab across all subgroups assessed (Fig. 3b). However, there was a numerical improvement in PFS with nivolumab plus ipilimumab versus durvalumab in an exploratory analysis of participants with tumor PDL1 expression ≥50% (median PFS of 25.5 months versus 19.4 months) (Fig. 3b and Extended Data Fig. 1).
OS, a key secondary endpoint subject to hierarchical statistical testing, was not formally tested per protocol, as the primary endpoint of PFS did not reach statistical significance. According to the descriptive analysis, median OS was 34.6 months in the nivolumab plus ipilimumab arm and 40.2 months in the durvalumab arm (HR: 1.12, 95% CI: 0.87–1.43) (Fig. 4).

a,b, OS in the intent-to-treat population (a) and participant subgroups (b). Subsequent radiotherapy, surgery or systemic therapy received: nivolumab plus ipilimumab arm, 2%, 1% and 24%, respectively; durvalumab arm, 4%, <1% and 31%, respectively. Participants may have received ≥1 type of subsequent therapy (cancer-related therapy initiated after or on first dosing date or randomization date if the participant was never treated). Symbols (tick marks) indicate censored data. NR, not reached.
As with the findings between the nivolumab plus ipilimumab and durvalumab arms, no differences in PFS or OS (PFS, HR: 0.84, 95% CI: 0.69–1.04; OS, HR: 0.97, 95% CI: 0.76–1.24) were observed between the nivolumab alone arm compared to the durvalumab arm (Fig. 5).

a, PFS by BICR in the intent-to-treat population. b, PFS by BICR in the participant subgroups. c, OS in the intent-to-treat population. d, OS in the participant subgroups. Subsequent radiotherapy, surgery or systemic therapy received: nivolumab arm: 4%, <1% and 24%, respectively; durvalumab arm, 4%, <1% and 31%, respectively. Participants may have received ≥1 type of subsequent therapy (cancer-related therapy initiated on or after first dosing date (or randomization date if the participant was never treated). Symbols (tick marks) indicate censored data.
Overall, 25% of participants in the nivolumab plus ipilimumab arm, 25% in the nivolumab arm and 32% in the durvalumab arm (Supplementary Table 2) received any subsequent anticancer therapy. Subsequent systemic therapy was received by 24% of participants in each of the nivolumab-containing arms and 31% of participants in the durvalumab arm.
Response and disease progression
Objective response rates (ORRs) by BICR were 68% for nivolumab plus ipilimumab, 72% for nivolumab and 64% for durvalumab. The median duration of response (DOR) was 25.1 months, 31.1 months and 25.2 months for the nivolumab plus ipilimumab, nivolumab and durvalumab arms, respectively (Supplementary Table 3). The waterfall plots of the best reduction in target lesion from baseline to the end of the CCRT phase illustrated a similar trend across the three treatment arms, with most participants having at least a 30% reduction (Extended Data Fig. 2).
Disease progression (per investigator) occurred in 111 participants (39%) in the nivolumab plus ipilimumab arm, 127 (40%) in the nivolumab arm and 146 (46%) in the durvalumab arm. To better understand the patterns of progression, an exploratory analysis was conducted to assess the occurrence of distant versus only locoregional metastases by treatment arm. Of the participants who progressed, 59%, 56% and 51% in the nivolumab plus ipilimumab, nivolumab and durvalumab arms, respectively, had locoregional metastases, and 41%, 44% and 49%, respectively, had distant metastases. The most common sites of distant metastases across all treatment arms (n = 174) were the brain (45%), liver (17%), bone (17%) and adrenal gland (11%).
Participant-reported outcomes
Characterizing changes in cancer-related symptoms and quality of life between treatment arms was a prespecified exploratory endpoint. The mean (s.d.) NSCLC symptom assessment questionnaire (NSCLC-SAQ) total scores were similar across all three arms, with 5.93 (3.69) in the nivolumab plus ipilimumab arm, 5.79 (3.73) in the nivolumab only arm and 6.00 (3.68) in the durvalumab arm. Because the study’s primary endpoint was not statistically significant (P = 0.6460), no formal or further testing of symptom deterioration based on NSCLC-SAQ was performed per the statistical design.
Safety
Among all treated participants, any-grade AEs were reported in 99% of those in the nivolumab plus ipilimumab arm, 99% in the nivolumab arm and 98% in the durvalumab arm (Table 2). Any-grade TRAEs occurred in 95% of participants in the nivolumab plus ipilimumab arm, 96% in the nivolumab arm and 96% in the durvalumab arm; the most common were anemia, decreased white blood cell count, nausea, esophagitis, pneumonitis, decreased neutrophil count and fatigue. TRAEs of grades 3–4 occurred in 57% of the participants in the nivolumab plus ipilimumab arm, 54% in the nivolumab arm and 49% in the durvalumab arm (Extended Data Fig. 3), leading to discontinuation in 14%, 9% and 8% of participants, respectively (Table 2). Radiotherapy-related AEs of grades 3–4 were reported in 30% of participants in the nivolumab plus ipilimumab arm, 26% of those in the nivolumab arm and 25% of those in the durvalumab arm. The incidence of TRAEs of grades 3–4 by treatment phase were 50%, 47% and 44%, respectively, in the CCRT phase and 20%, 15% and 15%, respectively, in the consolidation phase (Supplementary Table 4).
Grade 1 and 2 treatment-related pneumonitis was reported in 4% and 14%, respectively, of participants in the nivolumab plus ipilimumab arm, 5% and 17% in the nivolumab arm and 5% and 9% in the durvalumab arm; rates for grade 3–4 treatment-related pneumonitis were 4%, 3% and <1%, respectively (Fig. 6 and Supplementary Table 5). There were no treatment-related grade 5 pneumonitis events in any arm, which includes events reported between the first dose and 30 days after the last dose of consolidation treatment or at the first dose of retreatment. Across all arms, most pneumonitis events occurred during the consolidation phase and approximately 90% of participants developed pneumonitis within 6 months of their last dose of radiotherapy, with 63% of these participants developing pneumonitis within the first 3 months of radiotherapy (Supplementary Table 6).

Data include events reported between the first dose and 30 days after the last dose of study therapy, excluding retreatment. No grade 5 pneumonitis was reported.
The most common immune-mediated AEs—AEs consistent with an immune-mediated mechanism or immune-mediated component for which noninflammatory etiologies (for example, infection or tumor progression) were ruled out—were pneumonitis, rash and diarrhea (Extended Data Fig. 4). Immune-mediated pneumonitis (including pneumonitis, immune-related lung disease and interstitial lung disease) was reported in 23% of the participants in the nivolumab plus ipilimumab arm, 23% of those in the nivolumab arm and 10% of those in the durvalumab arm.
Treatment-related deaths occurred in ten participants (4%) in the nivolumab plus ipilimumab arm, 11 participants (4%) in the nivolumab arm, and one participant (<1%) in the durvalumab arm (Supplementary Table 7). Of these, seven (2%), five (2%) and one (<1%) deaths occurred during the CCRT phase, while three (1%), six (2%) and zero deaths occurred during the consolidation phase. In total, 15 of the 22 treatment-related deaths (68%) were because of pneumonitis (two deaths were because of immune pneumonitis), all of which occurred between 31 and 100 days after the last dose of consolidation treatment. Other causes of death included sepsis (n = 2), cardiac arrest (n = 1), infection (n = 2), tumor invasion of blood vessels (n = 1) and cytokine release syndrome (n = 1).
Discussion
In CheckMate 73L, the addition of nivolumab concurrent to CRT followed by nivolumab plus ipilimumab consolidation did not improve PFS over SOC CCRT followed by durvalumab for participants with unresectable, stage III NSCLC. A descriptive analysis of OS also showed no improvement in the nivolumab plus ipilimumab arm. Additionally, there was no improvement in PFS or OS with nivolumab plus CCRT followed by nivolumab alone versus CCRT followed by durvalumab. While a formal comparison between the nivolumab plus ipilimumab and nivolumab alone arms could provide useful insights that may inform future use of these regimens, the study was not powered to compare outcomes between these two arms. No unexpected safety signal was observed in either the nivolumab plus ipilimumab or nivolumab arms. As observed previously, concomitant IO and CCRT were associated with increased pneumonitis rates10,12,16,17.
Similar to the overall participant population, no improvement in survival was observed in the nivolumab plus ipilimumab arm across key subgroups with the exception of a numerical trend toward improved PFS observed in the exploratory tumor PDL1 ≥ 50% subgroup analysis. These results are consistent with findings from studies of IO-based regimens in metastatic NSCLC, where persons with high PDL1 expression derived maximal benefit with nivolumab-based regimens14,15,18. A similar study evaluating IO plus CCRT regimens in untreated, unresectable NSCLC (KEYNOTE-867) did not assess differences in survival by PDL1 expression to our knowledge19; further research is needed to definitively assess this treatment effect.
The phase 3 PACIFIC study demonstrated survival benefit with CCRT followed by durvalumab consolidation over CCRT alone2, establishing CCRT followed by durvalumab as the SOC for persons with untreated, unresectable, stage III NSCLC. Notably, the median PFS results across all arms of CheckMate 73L were comparable to the durvalumab arm from PACIFIC (16.8 months)2; however, in CheckMate 73L, there appeared to be a trend toward improved PFS with durvalumab in the tumor PDL1 < 1% subgroup compared to the higher PDL1 subgroups. Nevertheless, cross-trial comparisons should be made with caution because of potential differences in study designs and participant populations. Of note, in the PACIFIC study, enrolled participants who had successfully completed CCRT and maintained adequate performance status were randomized to receive consolidation durvalumab, whereas participants in CheckMate 73L who were treatment-naive were randomized to receive CCRT on study.
Although phase 2 studies have demonstrated the promising efficacy of concurrent IO and CRT in stage III NSCLC10,12,16, similar to CheckMate 73L, the phase 3 PACIFIC-2 trial did not demonstrate clinical benefit. In that trial, durvalumab and CCRT followed by durvalumab consolidation provided no significant PFS improvement over CCRT alone17. In KEYNOTE-867, in participants with stage I or II NSCLC, pembrolizumab plus stereotactic body radiation therapy (SBRT) did not improve event-free survival over SBRT alone19. Furthermore, another phase 2, single-arm study in participants with stage III NSCLC evaluating concurrent radiotherapy plus durvalumab without chemotherapy followed by durvalumab consolidation was closed because of early disease progression and high-grade toxicity20.
The reason for a lack of meaningful benefit when adding IO to CCRT remains unclear. One potential explanation is that IO may be more effective after CCRT in the presence of minimal residual disease compared to concurrent administration when notable disease burden may still be present6. Additionally, radiotherapy may negatively impact local and systemic adaptive immune responses and inhibit IO efficacy. Nevertheless, preclinical data have demonstrated improved antitumor activity with radiotherapy administered simultaneously with anti-PD1 or anti-PDL1 monoclonal antibodies, which was attributed to radiotherapy-mediated PDL1 upregulation in tumor cells21,22, and have also shown that radiotherapy draws immunosuppressive cells, including Tregs, to the tumor microenvironment22. Irradiating tumor-draining lymph nodes has been shown to impair trafficking of CD8+ T cells into the tumor microenvironment23. Taken together, the optimal timing of IO with CCRT and the optimal duration of radiotherapy have not yet been established. Of note, participants enrolled in studies using concurrent strategies are treatment-naive, with variability in the feasibility and efficacy of CRT. Consequently, demonstrations of improvement in clinical outcomes in this population may require a better understanding of the optimal radiation dose, fractionation and timing, which all remain key elements and the topics of ongoing research24.
Pneumonitis remains a key clinical concern with CCRT, even more so when combined with IO25. Higher rates of treatment-related pneumonitis of any grade and of grades 3–4 were observed in the nivolumab plus ipilimumab and nivolumab arms versus the durvalumab arm in CheckMate 73L; a total of 15 treatment-related deaths were because of pneumonitis across the treatment arms. Compared to the durvalumab arm, a greater number of pneumonitis-related deaths occurred in the nivolumab plus ipilimumab and the nivolumab alone arms (n = 6, n = 8 and n = 1, respectively). Similar findings were observed in other studies that have added IO to CCRT in NSCLC10,13,16,17.
In the CheckMate 73L study, beyond pneumonitis, TRAEs and immune-mediated AEs were generally comparable across all treatment arms and were less common during the consolidation period versus the CCRT period, including in the nivolumab plus ipilimumab arm. Furthermore, no unexpected safety signals were observed with nivolumab or ipilimumab; the overall safety profile in CheckMate 73L is aligned with those in studies of participants with nonmetastatic or metastatic NSCLC treated with nivolumab or nivolumab plus ipilimumab14,18,26,27.
The treatment paradigm for stage IIIA NSCLC continues to evolve, particularly for persons with N2 disease who were once considered unresectable. Increasingly, these individuals are being offered chemo-IO aimed at mediastinal downstaging to facilitate surgical resection28. In the phase 3 CheckMate 77T study (NCT04025879), which evaluated neoadjuvant nivolumab plus chemotherapy in participants with stage III NSCLC, an exploratory analysis by nodal status showed that, compared to placebo, participants who received nivolumab had improved event-free survival and pathologic complete response rates, as well as higher rates of definitive surgery and postoperative nodal downstaging29. In the interim analysis of the phase 2, single-arm, MDT-Bridge study (NCT05925530), 82% of baseline borderline-resectable NSCLC tumors were deemed resectable at reassessment following two cycles of neoadjuvant durvalumab plus chemotherapy30. For persons with stage IIIA NSCLC who remain unresectable, retrospective propensity score-matched analyses have suggested an OS advantage for surgery over CCRT; however, this benefit diminished after adjusting for baseline differences31. Moreover, as the use of IO has increased in both CCRT and induction regimens, higher rates of pneumonitis have been reported in the CheckMate 73L and other studies10,13,16,17. These findings underscore the importance of careful recipient selection, considering tumor burden, nodal status, pulmonary reserve, comorbidities and molecular and immunologic features, when determining the optimal use of CCRT.
The CheckMate 73L study uniquely evaluates both the timing (consolidative ± concomitant) and type (PD1/PDL1 ± CTLA4) of IO in combination with CCRT in a large population. This meticulous and robust study design allowed for a conclusive assessment of multiple hypotheses, the results of which may help guide clinical treatment strategies for both induction and maintenance for persons with unresectable stage III NSCLC and future analyses.
In this final analysis of CheckMate 73L, we found no significant improvement in survival outcomes with nivolumab plus CCRT followed by consolidation with nivolumab plus ipilimumab versus CCRT followed by consolidation durvalumab in participants with unresectable, stage III NSCLC. There were no unexpected safety signals with nivolumab or ipilimumab; however, there was increased rates of pneumonitis with IO plus CCRT versus CCRT alone. These results emphasize the need to investigate novel efficacious treatment options for this population.
Methods
Ethical oversight
CheckMate 73L was designed by the sponsor (Bristol Myers Squibb) and study steering committee. Data were collected by investigators (the list of investigators is provided in the Supplementary Information) and analyzed in collaboration with the sponsor, with an independent data monitoring committee providing oversight. The study was performed in accordance with the Declaration of Helsinki and the International Council for Harmonization Good Clinical Practice guidelines, with independent ethics committees or institutional review boards at each study site approving the protocol (additional information provided in the Supplementary Information). Participants provided written informed consent to participate. This manuscript was developed using medical writing support, with direction from the authors and funded by the sponsor. The authors confirmed the accuracy and completeness of data reported herein and approved the submission of this manuscript for publication. CONSORT guidelines were followed in the development of this manuscript32.
Participants
Adults with newly diagnosed, treatment-naive, locally advanced, unresectable, stage III histologically confirmed NSCLC (per the American Joint Committee on Cancer Staging Manual, eighth edition) amenable to definitive CCRT and an Eastern Cooperative Oncology Group performance status (ECOG PS) of 0–1 were eligible to enroll. Participants were not eligible if they received prior radiotherapy, had tumors that were positive for any EGFR mutation, ALK translocation and/or ROS1 rearrangement or had inadequate pulmonary function (defined as forced expiratory volume in 1 s ≤ 50% of predicted normal volume and/or carbon monoxide lung diffusing capacity ≤ 40% of predicted normal value). The full study protocol and statistical analysis plan are provided in the Supplementary Information.
Study design and treatments
CheckMate 73L (ClinicalTrials.gov number: NCT04026412) is a multicenter, randomized open-label, parallel, phase 3 study in which participants were screened between November 2019 and November 2022 and randomized (through an interactive response technology system) 1:1:1 to receive nivolumab 360 mg every 3 weeks (Q3W) plus CCRT followed by up to 1 year of consolidation with nivolumab 360 mg Q3W plus ipilimumab 1 mg kg−1 every 6 weeks (nivolumab plus ipilimumab arm), nivolumab 360 mg Q3W plus CCRT followed by up to 1 year of consolidation with nivolumab 480 mg every 4 weeks alone (nivolumab arm) or CCRT followed by up to 1 year of consolidation with durvalumab 10 mg kg−1 every 2 weeks (durvalumab arm) (Fig. 1). During the CCRT phase, all participants received histology-based, platinum-doublet chemotherapy (that is, participants with squamous tumor histology received etoposide plus cisplatin or paclitaxel plus carboplatin; participants with nonsquamous tumor histology received etoposide plus cisplatin, paclitaxel plus carboplatin or pemetrexed plus cisplatin) and thoracic radiotherapy in the form of intensity-modulated radiation therapy, volumetric-modulated arc therapy or three-dimensional radiotherapy. Irradiation commenced on day 1 of cycle 2 of systemic anticancer therapy (chemotherapy ± nivolumab; skipping cycle 1 was optional) and was delivered 5 days per week in a once daily fraction, 2 Gy per fraction, to a target dose of 60–66 Gy in 30–33 fractions (radiotherapy dose constraints are available in the radiotherapy guidelines in the Supplementary Information).
Randomization was stratified according to age (<65 years versus ≥65 years), disease stage (IIIA versus IIIB versus IIIC) and tumor PDL1 expression (≥1% versus <1% versus not evaluable or indeterminate), as determined with the use of the PDL1 IHC 28-8 pharmDx assay (Dako). It should be noted that randomization to the nivolumab plus ipilimumab arm was temporarily suspended because of an Interactive Response Technology registration platform error. During that suspension period, 43 participants could be randomized to only the nivolumab alone or durvalumab arms.
Treatment was discontinued as follows: if participants experienced investigator-assessed disease progression, death, unacceptable toxicity or symptomatic deterioration, the investigator’s decision to discontinue treatment, withdrawal of consent on further treatment or lost to follow-up.
Endpoints and assessments
The primary endpoint was PFS by Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1) per BICR for the nivolumab plus ipilimumab arm versus the durvalumab arm. PFS was defined as the time between the date of randomization and the first date of documented progression (RECIST v1.1 per BICR) or death because of any cause, whichever occurred first, regardless of receipt of subsequent anticancer therapy before the documented progression per BICR.
Key secondary endpoints included OS for the nivolumab plus ipilimumab arm versus the durvalumab arm, PFS by RECIST v1.1 per BICR and per investigator assessment and OS for the nivolumab arm versus the durvalumab arm, tumor response assessment for both nivolumab arms versus the durvalumab arm (included ORR, DOR and time to response by RECIST v1.1 per BICR and per investigator assessment) and safety.
A key exploratory endpoint was the proportion of participants without meaningful symptom deterioration following 48 weeks after initiation of consolidation therapy using the NSCLC-SAQ, a seven-item participant-reported outcome measure.
Additional exploratory analyses included patterns of progression, onset of pneumonitis after last dose of radiotherapy (<3 months, 3–6 months or >6 months) and a comparison of PFS in participants with a PDL1 expression ≥50% in the nivolumab plus ipilimumab and durvalumab arms.
Data collection and analysis were not performed blind to the conditions of the experiments.
Statistical analysis
The sample size was determined on the basis of the primary endpoint of PFS between the nivolumab plus ipilimumab and durvalumab arms. A total of 346 PFS events (that is, progression events or deaths) in the nivolumab plus ipilimumab and durvalumab arms would provide approximately 82% power to detect an HR of 1 during the first 3 months and an HR of 0.69 thereafter, with a 0.05 two-sided α. On the basis of the enrollment projection and the accrual duration, a total of 888 participants were planned for randomization across the three treatment groups in a 1:1:1 ratio. The stopping boundary for the final PFS analyses reported here was based on the actual number of PFS events at the time of the analysis using the Lan–DeMets α spending function with O’Brien–Fleming boundaries. Formal testing of OS for the nivolumab plus ipilimumab and durvalumab arms and the nivolumab and durvalumab arms was planned but was not performed because PFS for the nivolumab plus ipilimumab and durvalumab arms was not significant. No formal testing was planned for PFS between the nivolumab arm versus durvalumab arm or for PFS or OS for the nivolumab plus ipilimumab arm versus the nivolumab arm.
Efficacy was evaluated in all randomized participants, with stratified analyses performed for main and supportive analyses of the efficacy outcomes and unstratified analyses performed for supplementary and subgroup analyses of the efficacy outcomes. A stratified two-sided log-rank test was used to compare PFS between the nivolumab plus ipilimumab arm and durvalumab arm. A Cox proportional hazards model with treatment as the single covariate was used to estimate the HR and corresponding CI (100 × (1 − α)% CI (adjusted for interim)). Because the other outcomes were not formally compared, standard 95% CIs are reported.
Safety was evaluated in participants who received at least one dose of a study treatment. Attribution of pneumonitis to radiation, IO or both was at the discretion of the investigator.
Classification of deaths were differentiated by time of occurrence related to treatment dosing. Grade 5 deaths were defined as those events reported between the first dose and 30 days after the last dose of consolidation treatment or at the first dose of retreatment. Treatment-related deaths were defined as those occurring between 31 and 100 days after the last dose of consolidation treatment.
The NSCLC-SAQ was administered at baseline, before dosing on day 1 of each cycle during the CCRT and consolidation phases and at each clinic visit during the recovery period. The minimal important difference was used to assess any meaningful deterioration in the NSCLC-SAQ total score by 48 weeks after the initiation of consolidation treatment.
All analyses were performed using Statistical Analysis System software (SAS Institute; version 9.04.01M7P08062020).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Researchers with a clearly defined scientific objective may submit requests for deidentified and anonymized datasets to Bristol Myers Squibb through the Vivli platform (https://vivli.org/resources/requestdata/). Criteria for data requests are available online (https://vivli.org/ourmember/bristol-myers-squibb/) and additional information on Bristol Myers Squibb’s policy on data sharing may be found on their website (https://www.bms.com/researchers-and-partners/clinical-trials-and-research/disclosure-commitment.html). Data considered for sharing may include nonidentifiable participant-level and study-level clinical trial data and full clinical study reports. The remaining data are available within the article or its Supplementary Information. The study protocol and statistical analysis plan are available in the Supplementary Information. Source data are provided with this paper.
References
Petrella, F. et al. Stage III non-small-cell lung cancer: an overview of treatment options. Curr. Oncol. 30, 3160–3175 (2023).
Antonia, S. J. et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N. Engl. J. Med. 377, 1919–1929 (2017).
Spigel, D. R. et al. Five-year survival outcomes from the PACIFIC trial: durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J. Clin. Oncol. 40, 1301–1311 (2022).
McCall, N. S., Dicker, A. P. & Lu, B. Beyond concurrent chemoradiation: the emerging role of PD-1/PD-L1 inhibitors in stage III lung cancer. Clin. Cancer Res. 24, 1271–1276 (2018).
Jiang, J. L. et al. Synergies between radiotherapy and immunotherapy: a systematic review from mechanism to clinical application. Front. Immunol. 16, 1554499 (2025).
Azghadi, S. & Daly, M. E. Radiation and immunotherapy combinations in non-small cell lung cancer. Cancer Treat. Res. Commun. 26, 100298 (2021).
Rajeev-Kumar, G. & Pitroda, S. P. Synergizing radiotherapy and immunotherapy: current challenges and strategies for optimization. Neoplasia 36, 100867 (2023).
Wu, L. et al. Radiation combined with immune checkpoint inhibitors for unresectable locally advanced non-small cell lung cancer: synergistic mechanisms, current state, challenges, and orientations. Cell. Commun. Signal. 21, 119 (2023).
Kim, G. R. & Choi, J. M. Current understanding of cytotoxic T lymphocyte antigen-4 (CTLA-4) signaling in T-cell biology and disease therapy. Mol. Cells 45, 513–521 (2022).
Peters, S. et al. Progression-free and overall survival for concurrent nivolumab with standard concurrent chemoradiotherapy in locally advanced stage IIIA-B NSCLC: results from the European Thoracic Oncology Platform NICOLAS phase II trial (European Thoracic Oncology Platform 6-14). J. Thorac. Oncol. 16, 278–288 (2021).
Jabbour, S. K. et al. Pembrolizumab plus concurrent chemoradiation therapy in patients with unresectable, locally advanced, stage III non-small cell lung cancer: the phase 2 KEYNOTE-799 nonrandomized trial. JAMA Oncol. 7, 1351–1359 (2021).
Liu, Y. et al. Final efficacy outcomes of atezolizumab with chemoradiation for unresectable NSCLC: the phase II DETERRED trial. Lung Cancer 174, 112–117 (2022).
Lin, S. H. et al. Phase II trial combining atezolizumab concurrently with chemoradiation therapy in locally advanced non-small cell lung cancer. J. Clin. Oncol. 37, 8512 (2019).
Reck, M. et al. Five-year outcomes with first-line nivolumab plus ipilimumab with 2 cycles of chemotherapy versus 4 cycles of chemotherapy alone in patients with metastatic non-small cell lung cancer in the randomized CheckMate 9LA trial. Eur. J. Cancer 211, 114296 (2024).
Ramalingam, S. S. et al. Six-year survival and HRQoL outcomes with 1L nivolumab + ipilimumab in patients with metastatic NSCLC from CheckMate 227. J. Thorac. Oncol. 18, S76–S77 (2023).
Reck, M. et al. Two-year update from KEYNOTE-799: pembrolizumab plus concurrent chemoradiation therapy (cCRT) for unresectable, locally advanced, stage III NSCLC. J. Clin. Oncol. 40, 8508 (2022).
Bradley, J. D. et al. Platinum-based chemoradiotherapy in unresectable stage III non-small cell lung cancer: the phase III PACIFIC-2 study. J. Clin. Oncol. 43, 3610–3621 (2025).
Borghaei, H. et al. Nivolumab plus chemotherapy in first-line metastatic non-small-cell lung cancer: results of the phase III CheckMate 227 Part 2 trial. ESMO Open 8, 102065 (2023).
Pircher, A. et al. Stereotactic body radiotherapy (SBRT) with pembrolizumab (pembro) for unresected stage I/II non-small-cell lung cancer (NSCLC): the randomized, double-blind, phase 3 KEYNOTE-867 study. Immunooncol. Technol. 24, 101027 (2024).
Zhang, Y. et al. Concerning safety and efficacy of concurrent and consolidative durvalumab with thoracic radiation therapy in PDL1-unselected stage III non-small cell lung cancer: brief report. Int. J. Radiat. Oncol. Biol. Phys. 121, 68–74 (2025).
Dovedi, S. J. et al. Acquired resistance to fractionated radiotherapy can be overcome by concurrent PD-L1 blockade. Cancer Res. 74, 5458–5468 (2014).
Weichselbaum, R., Liang, H., Deng, L. & Fu, Y.-X. Radiotherapy and immunotherapy: a beneficial liaison? Nat. Rev. Clin. Oncol. 14, 365–379 (2017).
Marciscano, A. E. et al. Elective nodal irradiation attenuates the combinatorial efficacy of stereotactic radiation therapy and immunotherapy. Clin. Cancer Res. 24, 5058–5071 (2018).
Galluzzi, L., Aryankalayil, M. J., Coleman, C. N. & Formenti, S. C. Emerging evidence for adapting radiotherapy to immunotherapy. Nat. Rev. Clin. Oncol. 20, 543–557 (2023).
Acker, F. et al. Efficacy and safety of immune checkpoint inhibition combined with concurrent chemoradiotherapy in patients with stage III unresectable non-small cell lung cancer: a systematic review and meta-analysis. Eur. J. Cancer 218, 115266 (2025).
Cascone, T. et al. Perioperative nivolumab in resectable lung cancer. N. Engl. J. Med. 390, 1756–1769 (2024).
Forde, P. M. et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N. Engl. J. Med. 386, 1973–1985 (2022).
Wang, Y. et al. Efficacy and safety of neoadjuvant chemoimmunotherapy and chemotherapy in patients with potentially resectable stage IIIA/IIIB NSCLC: a retrospective study. Front. Immunol. 15, 1479263 (2025).
Provencio, M. et al. Clinical outcomes with perioperative nivolumab (NIVO) by nodal status among patients (pts) with stage III resectable NSCLC: results from the phase 3 CheckMate 77T study. J. Clin. Oncol. 42, LBA8007 (2024).
Reck, M. et al. Neoadjuvant durvalumab (D) + chemotherapy (CT) followed by either surgery (Sx) and adjuvant D or CRT and consolidation D in patients (pts) with resectable or borderline resectable stage IIB–IIIB NSCLC: interim analysis (IA) of the phase II MDT-BRIDGE study. Ann. Oncol. 36, S1606–S1607 (2025).
Shigenobu, T. et al. Surgery versus concurrent chemoradiotherapy for stage III non-small cell lung cancer: a retrospective study with propensity score matching. BMC Cancer 25, 121 (2025).
Schulz, K. F., Altman, D. G., Moher, D. & CONSORT Group CONSORT 2010 Statement: updated guidelines for reporting parallel group randomized trials. Open Med. 4, e60–e68 (2010).
Acknowledgements
We thank the participants and families who made this study possible, the investigators and clinical study teams who participated in the study, Dako (an Agilent Technologies company) for collaborative development of the PDL1 IHC 28-8 pharmDx assay and Ono Pharmaceutical Company. Medical writing and editorial support for the development of this manuscript, under the direction of the authors, was provided by S. Thier, S. L. Dwyer and M. Salernitano of Ashfield MedComms, an Inizio company, funded by Bristol Myers Squibb. Bristol Myers Squibb sponsored the study and participated in the study design, data collection and analysis and writing of the manuscript.
Author information
Authors and Affiliations
Contributions
S.P., R.N., G.P., L.Y. and D.D.R. contributed to the conceptualization or design. S.P., D.S.W.T., D.E.G., J.U., S.R., J.Y., L.X., A.R., T.-E.C., J.d.M., H.R.K., C.R., K.S., H.H., A.H., D.C., D.B., M.K., A.C. and D.D.R. contributed to data acquisition. R.N., G.P. and L.Y. contributed to data analysis. All authors contributed to data interpretation.
Corresponding author
Ethics declarations
Competing interests
S.P. has received research funding to their institution from Amgen, Arcus, AstraZeneca, BeiGene, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, GSK, iTeos, Merck Sharp & Dohme, Mirati, Pfizer, PharmaMar, Promontory Therapeutics, Roche/Genentech and Seattle Genetics, consulting fees to their institution from AbbVie, Amgen, Arcus, AstraZeneca, Bayer, BeiGene, BioNTech, BerGenBio, Bicycle Therapeutics, Biocartis, BioInvent, Blueprint Medicines, Boehringer Ingelheim, Bristol Myers Squibb, Clovis, Daiichi Sankyo, Debiopharm, Eli Lilly, F-star, Foundation Medicine, Genmab, Genzyme, Gilead, GSK, Hutchmed, Illumina, Incyte, Ipsen, iTeos, Janssen, Qlucore, Merck Sharp & Dohme, Merck Serono, Merrimack, Mirati, Nuvation Bio, Nykode Therapeutics, Novartis, Novocure, PharmaMar, Promontory Therapeutics, Pfizer, Regeneron, Roche/Genentech, Sanofi, Seattle Genetics, Takeda and Zymeworks, honoraria to their institution from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Foundation Medicine, GSK, Illumina, Ipsen, Merck Sharp & Dohme, Mirati, Novartis, Pfizer, Roche/Genentech, Sanofi, Seattle Genetics and Takeda and support for meetings or travel to their institution from AstraZeneca, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly, Merck Sharp & Dohme, Novartis, Pfizer, Roche/Genentech and Takeda and has participated in the data safety and monitoring boards for AbbVie, Amgen, Arcus, AstraZeneca, Bayer, BeiGene, BioNTech, BerGenBio, Bicycle Therapeutics, Biocartis, BioInvent, Blueprint Medicines, Boehringer Ingelheim, Bristol Myers Squibb, Clovis, Daiichi Sankyo, Debiopharm, Eli Lilly, F-star, Foundation Medicine, Genmab, Genzyme, Gilead, GSK, Hutchmed, Illumina, Incyte, Ipsen, iTeos, Janssen, Qlucore, Merck Sharp & Dohme, Merck Serono, Merrimack, Mirati, Nuvation Bio, Nykode Therapeutics, Novartis, Novocure, PharmaMar, Promontory Therapeutics, Pfizer, Regeneron, Roche/Genentech, Sanofi, Seattle Genetics, Takeda and Zymeworks. D.S.W.T. has served a consulting or advisory role with Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, DKSH, GSK, Merck, Novartis, Pfizer, Roche and Takeda, has received research funding to their institution from ACM Biolabs, Amgen, AstraZeneca, and Pfizer and holds stock options with Oncoshot and C2i Genomics. D.E.G. has received grants or contracts to their institution from AstraZeneca, BerGenBio, Karyopharm, and Novocure, royalites from Oxford University Press and consulting fees from Catalyst Pharmaceuticals, has served on advisory boards for AbbVie, AstraZeneca, Daiichi Sankyo, Elevation Oncology, Janssen Scientific Affairs, Jazz, Regeneron and Sanofi, secured patent 11,747,345 for the ‘prediction and treatment of immunotherapeutic toxicity’ and has four additional patents pending, has served as the chief medical officer for OncoSeer Diagnostics, has participated in the data safety monitoring board for Daiichi Sankyo and Summit Therapeutics and has stock options with Gilead. J.U. serves as the Vice Chair on the Respiratory Committee for the Alliance for Clinical Trials in Oncology (National Cancer Institute-Sponsored Cooperative Group). S.R. has received grants to their institution from Amgen, AstraZeneca, Bristol Myers Squibb, Merck and Pfizer and meeting or travel support from AstraZeneca and AbbVie and has participated in the data safety monitoring board for Johnson & Johnson and Gilead. A.R. has participated in the data safety and monitoring boards for AbbVie, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly, GSK, Merck Sharp & Dohme, Novartis, Pfizer and Roche. T.-E.C. has received honoraria from Amgen, Astellas, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, EMD Serono, Ipsen, Janssen/Johnson & Johnson Innovative Medicine, Lilly, Medison, Merck Sharp & Dohme, Novartis, Pfizer, Roche, Sevier and Takeda and travel support from Amgen, Astellas, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, EMD Serono, Janssen/Johnson & Johnson Innovative Medicine, Ipsen, Lilly, Medison, Merck Sharp & Dohme, Novartis, Pfizer, Roche, Sevier and Takeda and has participated in the data safety and monitoring boards or advisory boards for Amgen, Astellas, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, EMD Serono, Ipsen, Janssen/Johnson & Johnson Innovative Medicine, Lilly, Medison, Merck Sharp & Dohme, Novartis, Pfizer, Roche, Sevier and Takeda. H.R.K. has received research funding to their institution from ABL Bio, AstraZeneca, Bristol Myers Squibb, Genentech/Roche, Merck & Co. and Merck Sharp & Dohme and honoraria from AstraZeneca and Takeda. C.R. has received honoraria from AstraZeneca, Bristol Myers Squibb, Pfizer, Merck Sharp & Dohme and Roche and has participated in the data safety and monitoring boards for Bristol Myers Squibb, Pfizer, Merck Sharp & Dohme, and Sanofi. K.S. has received consulting fees from Amgen, AstraZeneca, Bristol Myers Squibb and Merck Sharp & Dohme. H.H. has received grants from A2 Healthcare Corp, AbbVie, Amgen, Ascent Development Services, Astellas Pharma, AstraZeneca, Bayer Yakuhin, Bristol Myers Squibb, Chugai Pharmaceutical, CMIC, Clinical Research Support Center Kyushu, Comprehensive Support Project for Oncological Research of Breast Cancer, Daiichi Sankyo, Eisai Ltd., Eisai Inc, Eli Lilly Japan, EP-CRSU CO, EPS Corporation, GSK, ICON Japan, IQVIA Services JAPAN, Kobayashi Pharmaceutical, Kyowa Kirin, Janssen Pharmaceutical, Japan Clinical Cancer Research Organization, Japanese Gastric Cancer Association, Labcorp Development Japan, Medpace Japan, Merck Biopharma, Merck Sharp & Dohme, Mochida Pharmaceutical, Nippon Boehringer Ingelheim, Nippon Kayaku, Novartis Pharma, Otsuka Pharmaceutical, PPD-SNBL, Pfizer Japan, Pfizer R&D Japan, PRA Health Sciences, Public Health Research Foundation, Sanofi, Shionogi & Co., SRL Medisearch, Sysemex, Syneos Health Clinical, Taiho Pharmaceutical, Takeda Pharmaceutical, Thoracic Oncology Research Group and West Japan Oncology Group and honoraria from 3H Clinical Trial, AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Care Net, Chugai Pharmaceutical, Daiichi Sankyo, Eisai Ltd., Eli Lilly Japan, Guardant Health Japan, Hisamitsu Pharmaceutical, Ishiyaku Publishers, Janssen Pharmaceutical, Kyowa Kirin, Medical Review, Merck Biopharma, Merck Sharp & Dohme, Nippon Boehringer Ingelheim, Nippon Kayaku, Novartis Pharma, Novocure, Ono Pharmaceutical, Pfizer Japan, Reno, Medical, Sysmex Corporation, Taiho Pharmaceutical and Takeda Pharmaceutical and has participated in the data safety and monitoring boards for AbbVie, AstraZeneca, Bristol Myers Squibb, Chugai Pharmaceutical, Daiichi Sankyo, Janssen Pharmaceutical and Novocure. A.H. has received honoraria from AstraZeneca and Bristol Myers Squibb. D.C. has received consulting fees from AstraZeneca, Amgen, BeOne, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Johnson & Johnson, Lilly, Merck Sharp & Dohme and Roche and honoraria from Pfizer and has participated in the data safety and monitoring boards for Catalym. D.B. has received grants or contracts from AstraZeneca, Bristol Myers Squibb, Daiichi Sankyo, Dragonfly Therapeutics, F. Hoffmann-La Roche, Gilead, Merck, Seagen, honoraria from AstraZeneca and meeting or travel support from AstraZeneca, Bristol Myers Squibb, Novocure and Regeneron and has participated in data safety and monitoring boards for AstraZeneca, Bristol Myers Squibb, Merck, Novocure and Regeneron. M.K. has received research funding from Bristol Myers Squibb, consulting fees from Bristol Myers Squibb and Johnson & Johnson, honoraria from AstraZeneca, Bristol Myers Squibb and Takeda and meeting or travel support from BeiGene, Johnson & Johnson and Pierre Fabre, has participated in the data safety and monitoring boards for Amgen, Bristol Myers Squibb and Johnson & Johnson and received the study drug from Bristol Myers Squibb. A.C. has received consulting fees from AstraZeneca, Boehringer Ingelheim, Pfizer, Roche/Genentech, Eli Lilly and Company, Novartis, Takeda, Merck Sharp & Dohme, and Bristol Myers Squibb, research funding from Merck Sharp & Dome; received honoraria from AstraZeneca, Boehringer Ingelheim, Bayer, Pfizer, Roche, Novartis, Merck Sharp & Dohme and Bristol Myers Squibb and meeting or travel support from Roche, Boehringer Ingelheim, Pfizer, Merck Sharp & Dohme and Bristol Myers Squibb. R.N. and G.P. are employees of Bristol Myers Squibb and own stock options. L.Y. is an employee of Bristol Myers Squibb. D.D.R. has received research grants, support or advisory board funding to their institution from AstraZeneca, Bristol Myers Squibb, BeiGene, Phillips and Olink and has served on an advisory board for Eli Lilly. The other authors declare no competing interests.
Peer review
Peer review information
Nature Cancer thanks Jeffrey Clarke, Ben Creelan and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 PFS in patients from the nivolumab plus ipilimumab versus durvalumab arms by tumor PD-L1 expression.
PFS in patients with tumor PD-L1 expression (a) <1%, (b) ≥1%, and (c) ≥50%. Symbols (tick marks) indicate censored data. NR, not reached; PD-L1, programmed death-ligand 1; PFS, progression-free survival.
Extended Data Fig. 2 Best reduction from baseline in target lesion (at end of CCRT phase) in patients from the nivolumab plus ipilimumab, nivolumab, and durvalumab arms.
Patients with a target lesion at baseline and ≥1 evaluable post-baseline tumor assessment prior to consolidation or who did not enter consolidation were included. Best reduction was maximum reduction in the sum of the diameters of target lesions (negative values mean true reduction; positive values mean increase only observed over time). Horizontal reference line indicates the 30% reduction consistent with RECIST v1.1 response. CCRT, concurrent chemoradiotherapy; RECIST v1.1, Response Evaluation Criteria in Solid Tumors Version1.1.
Extended Data Fig. 3 Most common TRAEsa (≥15% in any arm).
Nivolumab plus ipilimumab arm, n = 282; nivolumab arm, n = 318; durvalumab arm, n = 317. aAdverse events per CTCAE v4.0 and MedDRA v26.1. Includes events reported between the first dose and 30 days after the last dose of study therapy, excluding re-treatment. CTCAE, Common Terminology Criteria for Adverse Events; MedDRA, Medical Dictionary for Regulatory Activities; TRAE, treatment-related adverse event.
Extended Data Fig. 4 Immune-mediated adverse events.
Nivolumab plus ipilimumab arm, n = 282; nivolumab arm, n = 318; durvalumab arm, n = 317. Immune-mediated AEs were AEs consistent with an immune-mediated mechanism or an immune-mediated component for which noninflammatory etiologies (eg, infection or tumor progression) were ruled out. aAll-cause pneumonitis included pneumonitis, immune-mediated lung diseases, and interstitial lung disease. One grade 5 pneumonitis event was reported in the nivolumab alone arm.
Supplementary information
Supplementary Information (download PDF )
Supplementary Tables 1–7 and Notes 1–6.
Source data
Source Data Fig. 2 (download XLSX )
Statistical source data.
Source Data Fig. 3 (download XLSX )
Statistical source data.
Source Data Fig. 4 (download XLSX )
Statistical source data.
Source Data Fig. 5 (download XLSX )
Statistical source data.
Source Data Fig. 6 (download XLSX )
Statistical source data.
Source Data Extended Data Fig. 1 (download XLSX )
Statistical source data.
Source Data Extended Data Fig. 2 (download XLSX )
Statistical source data.
Source Data Extended Data Fig. 3 (download XLSX )
Statistical source data.
Source Data Extended Data Fig. 4 (download XLSX )
Statistical source data.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Peters, S., Tan, D.S.W., Gerber, D.E. et al. Nivolumab plus chemoradiotherapy followed by nivolumab with or without ipilimumab for untreated locally advanced stage III NSCLC: a randomized phase 3 trial. Nat Cancer (2026). https://doi.org/10.1038/s43018-026-01161-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43018-026-01161-y
