
Abstract
Background
New onsets of chronic urticaria (CU) have been reported after repeated immunizations, mainly with the Moderna mRNA-1273 vaccine (Spikevax). This study aims to evaluate patients with CU after COVID-19 mRNA vaccination. The contribution of SARS-Cov2 infection, atopy and IgE against the vaccine was analyzed.
Methods
We monitored the features of patients who developed CU after vaccination through two surveys conducted in 2022 and 2023. Fifty individuals with CU underwent blood tests, and their results were compared with individuals without a history of urticaria (N = 135). The presence of anti-vaccine IgE was tested in 185 individuals with basophil activation tests (BAT). We assessed anti-SARS-Cov2 humoral response, and the presence of IgEs against common respiratory allergens (Phadiatop) as a surrogate for atopy.
Results
Post-vaccination CU occurs after a median interval of 10 days and significantly more after the Spikevax booster, affecting middle-aged individuals (median 41, 66% females). In 2023, CU was still active in 53% of the cases. Inducible forms of CU, primarily dermographism, are reported in 54% (2022) and 61% (2023) of the cases. BAT positivity is not specific to CU, anti-nucleocapsid positivity, or atopy but is significantly associated with higher anti-spike neutralizing activities and younger age. Four CU patients tolerate an additional dose of mRNA vaccine with no disease exacerbation/recurrence.
Conclusions
The spikevax booster induces anti-vaccine IgE independently of CU, the latter being not directly associated with COVID-19 infection nor atopy. The tolerance to a new booster in 4/4 patients suggests that the Spikevax vaccine indirectly triggers CU in predisposed individuals.
Plain language summary
Urticaria is an itchy transient skin rash which can become in some cases recurrent and chronic. Repeated immunizations with COVID-19 mRNA vaccines can rarely lead to the development of chronic urticaria (CU), on average 10 days after vaccination. Here, we monitored people who developed CU after vaccination. One year following vaccination 53% of people still had CU. CU after vaccination was not directly associated with COVID infection, allergic predisposition or other effects of vaccination. Re-exposure to the vaccine was safe and well tolerated in four patients with vaccine-related CU suggesting an absence of a direct causality between the vaccine and CU. Therefore, managing CU post-vaccination should follow previously established guidelines as for other forms of CU.
Similar content being viewed by others


Introduction
A major contribution to reducing the burden of the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV2) pandemic was the rapid development of an efficient vaccination strategy1. The two mRNA vaccines, the mRNA-1273 (Spikevax®) from Moderna and BNT 162b2 (Comirnaty®) from Pfizer-BioNTech were authorized in January 20212 and December 20203 and were the most commonly given vaccines in Switzerland4,5,6. Yet, these COVID-19 vaccines were associated with several adverse effects with up to 17,000 reports of suspected adverse drug reactions collected in Switzerland by February 20237,8. In particular, new onsets of chronic urticaria (CU) have been reported after repeated immunizations, mainly with the Spikevax vaccine9,10,11.
CU is defined by the European Academy of Allergology and Clinical Immunology (EAACI) as the development of wheals (hives), angioedema, or both for more than six weeks12. It can be classified as spontaneous, inducible, or both. Chronic inducible urticaria is triggered by external factors such as pressure, contact, vibration, temperatures, sun, or cholinergic activity. In Switzerland, we observed an outbreak of CU starting in December 20219,11. In the first analysis, we collected pharmacovigilance data from the Swiss Agency for Therapeutic Products (Swissmedic), and we estimated the overall crude incidence rate of CU after a COVID-19 booster at 19/100,000 from 2021-01-21 to 2022-08-31. The relative risk of new-onset CU after Spikevax compared to Comirnaty was 16.1 (95%CI, 10.8-24.0)11. Immunological data in seven patients revealed a systematic sensitization against the mRNA lipid nanoparticles but not against the linear polyethylene glycol-2000 nor the tromethamine9. The contribution of this IgE dependent sensitization to the pathogenesis and persistence of CU remains undetermined13. Notably, the contribution of infections with the omicron variant could also have been a confounding factor.
In the present study, our primary objectives were (1) to analyze patient’s clinical features and evolution of patients who developed CU through two separate surveys sent in 2022 and 2023, (2) to better define the contribution of COVID-19 infection to the onset of CU, (3) to compare the high sensitization rate against the vaccine in CU patients with control populations without CU. In this perspective, we recruited 50 CU patients for blood tests. We compared the results to 135 individuals not suffering from CU but either infected with COVID-19 (cohort COSED) or vaccinated with the COVID-19 mRNA booster (cohort ImmunoVax). As our study was not designed to address the pathomechanistic pathways of CU, mainly sub-grouped as auto-allergic (type I) and autoimmune (IIb)14, we did not include a control population with CU unrelated to the vaccination status.
In this study, we show that post-vaccination CU most commonly occurs after the Spikevax booster, primarily affecting middle-aged women, with over half of the cases remaining active in 2023. We also observe that inducible CU forms, such as dermographism, are frequently present. Chronic urticaria after vaccination is not directly associated with COVID infection nor atopy and it initiates independently of vaccine sensitization. Re-exposure to the vaccine is safe in all four patients studied.
Methods
Ethical approval
This retrospective observational study was approved by the local ethical committee (“Commission cantonale d’éthique de la recherche sur l’être humain” CER-VD, BASEC 2021-00735 (COVURT), https://swissethics.ch/en/basec). All patients received a study information form. Written informed consent was not required for completing the two surveys, as local allergists were not allowed the enroll directly the patients. Written informed consent was obtained for all cases involving a blood test. This study followed the STROBE reporting guideline.
Study population
We assembled the COVURT cohort with the help of local allergists, contacted trough their association (“Groupement Vaudois des allergologues et immunologues”). Sixteen allergists contributed in identifying eligible patients with CU after receiving a dose of COVID-19 mRNA vaccine. The University Hospital of Lausanne (CHUV) contacted patients who gave their consent and sent them a link to an online questionnaire and included cases which were previously reported11. Study data of the first survey were collected by participants between April 14th and January 5th 2023 and managed using REDCap electronic data capture tools hosted at Unisanté (Lausanne, Switzerland). All patients received a link to a second online questionnaire in 2023. Study data of the second survey were collected by participants between June 12th and September 4th 2023. Blood tests were performed from May 16th until January 23rd 2023. We arbitrary chose to perform blood tests in 50 patients.
As controls for the blood testing, we included patients from two observational cohorts without CU. The first study cohort regrouped patients with a formal diagnosis of COVID infection and who developed persistent symptoms in 56% (59/105) of the cases. Median age was 45 (IQR 35.5-54). 78/105 (74%) were females. Blood testing was performed between May 20, 2022 and January 13, 2023. The second group consisted of healthy collaborators from our hospital who systematically received a primary vaccination and a booster. Median age was 41 (IQR 35-48). 21/30 (70%) were females. Blood testing was performed between August 30th and October 4th 2022.
The third group consisted of heathy volunteers (n = 17) recruited at the Geneva University Hospitals between Dec 2021 and Feb 2022 willing to receive their dose of mRNA COVID-19 vaccine (Comirnaty or Spikevax). Blood samples were collected before the third vaccine dose. Nine out of 17 (53%) were females and median age was 44.
Whole blood RNA sequencing
Blood samples were collected in PAXgene Blood RNA Tube (BD Biosciences). RNA extraction was performed using the PAXgene Blood miRNA Kit (BD) on the QIAcube instrument (QIAGEN) following the manufacturer’s instructions. RNA concentration and quality were assessed by using the Qubit instrument (Invitrogen) and the Agilent 2100 Bioanalyzer, respectively. The Stranded Total RNA Ribo-Zero Plus kit from Illumina was used for the library preparation with 100 ng of total RNA as input. Library molarity and quality were assessed with the Qubit and Tapestation using a DNA High sensitivity chip (Agilent Technologies). Libraries were pooled at 2 nM for clustering and sequenced on an Illumina HiSeq4000 sequencer for aminimum of 30 million single-end 100 reads per sample. The RNA-sequencing libraries were aligned to the human genome (GRCh38.96) using STAR (15. Only uniquely mapped reads were kept for downstream steps. Gene expression quantification was performed with featureCounts16 for reads overlapping protein-coding genes. Low-count genes were filtered out with the filtered.data() function from the NOISeq R package 17using the following parameters: method = 1, norm = FALSE, cv.cutoff = 100, cpm = 1.
Basophil activation test
As previously reported vaccine-sensitization could be assessed by means of CD63 upregulation with Spikevax or Comirnaty in an interchangeable way, as a surrogate of intra-dermal skin test18. Briefly, blood samples were collected in 3 ml EDTA tubes and were used up to 24 h of blood collection using the Flow CAST® from Bühlmann Labs (Basel, Switzerland) according to manufacturer’s instructions (FK-CCR). Briefly, 50 μL whole blood from a 2.5ml K-EDTA venipuncture tube was added into a ready-to-use 1 ml vial pre-coated with an anti-CD63 FITC and anti-CCR3-PE antibodies (clones not disclosed by Bühlmann Labs). 50 μL of (a) stimulation buffer background, (b) 1-3 vaccine stimulations condition with Spikevax (1% 0.5% and/or 0.1%) and (c) a stimulation control (anti-FcεRI mAb and/or fMLP) was mixed with 100 μL of stimulation buffer containing calcium, heparin and IL-3 (concentration non disclosed by Bühlmann Labs) and mixed with 50 μL of whole blood (from a 2.5 ml K-EDTA venipuncture) in a ready-to-use 1 ml vial pre-coated with an anti-CD63 FITC and anti-CCR3-PE antibodies (clones/concentration not disclosed by Bühlmann Labs). After blood lysis, acquisition was performed by flow cytometry (BD LSRFortessa™ Cell Analyzer, BD Biosciences). A threshold of 10% in the αFcεRI-stimulated or FMLP condition was used to define non-responders (=areactivity). The same threshold was applied to the stimulated condition with mRNA vaccine to defined positivity (in any of the 3 different concentrations). For this study, 185 BAT were performed, 177 were interpretable, four subjects were classified as non-responder (all from the cohort CU), four subjects were excluded because of lack of basophils (two from the cohort CU). Results were analyzed using the FlowJo software (FLowJo LLC, Becton Dickinson, Ashland, OR).
Phadiatop assay
All analyses were performed retrospectively on frozen serum samples. ImmunoCAP Phadiatop (Réf. Article 14-4405-35, Thermo Fischer Scientific, Waltham, MA) is a ready to use qualitative and semi-quantitative in vitro test for the determination of aeroallergen-specific IgE antibodies in human plasma or serum. This test detected IgEs against a mixture of common respiratory allergens, including grass, birch, olive, mugwort, parietaria, dog, cat, horse, house dust mite, flour mite, and Cladosporium. The test was measured on a Phadia 250 instrument, Thermo Fischer Scientific). The lower detection limit was 0.35 kU/L for the Phadiatop assay. Patients with a positive Phadiatop (≥ 0.35 kU/L) were considered atopic as previously reported19.
Neutralization assay
Serum IgG anti-S and anti-nucleocapsid antibody levels and neutralizing antibody levels were determined using two Luminex bead-based binding assays recently developed in our laboratory20,21. Briefly, Spike protein-coupled beads (50 μg of homemade proteins derived from SARS-Cov2, wild type or the BA.1, BA.2, BA4, BQ.1, BQ.1.1 and XBB variants coupled to 1 ml of activated MagPlex-C Microsphere beads) were diluted in 1:100 PBS with 50 μl added to each well of a Bio-Plex Pro 96-well flat-bottom plates (Biorad, CA). 80 μl of individual serum samples at different dilutions (1:10, 1:30, 1:90, 1:300, 1:2700, and 1:8100) in PBS was added to the plate wells and incubated for 60 min on a plate shaker at 500 RPM. An ACE2 mouse Fc fusion protein (Creative Biomart or produced by École polytechnique fédérale de Lausanne (EPFL) Protein Production and Structure Core Facility) was then added to each well at a final concentration of 1 μg/ml. Following a 60 min incubation on a plate shaker, beads were washed and an anti-mouse IgG-PE secondary antibody (PE labeled (F(ab’)2-Goat anti-Human IgG (H + L) Antibody, Invitrogen) was added at a 1:100 dilution with 50 μl per well. Neutralizing activity was assessed by monitoring the ability of anti-S antibodies to prevent S-trimer protein binding to the angiotensin-converting enzyme 2 (ACE2) entry receptor, which is essential for the viral infection of a target cell. Half maximal inhibitory concentration (IC50) dilution values in the Spike-ACE2 surrogate neutralization assay and binding IgG anti-S antibody ratios were log10 transformed for visualization and statistical modeling as previously described22.
Statistics
The neutralization assay was analyzed with a two-way ANOVA test using the software package GraphPad PRISM v9. Two-tailed unpaired T tests were performed for comparing group with a positive versus negative BAT. Mean and standard deviation are shown. A value of P < 0.05 was considered statistically significant. Using a Fisher exact test, statistical analysis evaluated associations between vaccination parameters (type and doses), cohorts, gender, and BAT or PhadiatTop results. Unvaccinated donors served as the reference group for each specific vaccine dose. Analyses were conducted using R Statistical Software (v4.2.1). Patients with missing data were not excluded from the dataset.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Results
Initial survey
Among the 111 identified CU patients, we were able to contact 110, and 88 responded to our 2022 survey. One patient did not consent, one response was duplicated and excluded (Fig. 1a). Of these 88 patients, 66% were middle-aged female (median age 41, IQR 35-48, Fig. 1b). In 89% of cases, CU started after the booster shot and not after primary vaccination, predominantly with Spikevax (93%). The median interval time between vaccination and CU onset was 10 days. As of June 2022, CU remained active in 81% of these cases. Only 14% of the patients reported a previous history of urticaria, with the majority being cases of acute urticaria (92%). Inducible factors, mainly dermographism, were reported in 55% of the cases. The Urticaria Control Test (UCT) score, the number of lesions, and the severity of pruritus at disease onset indicated poor disease control. Although disease activity improved over time, control remained largely insufficient, possibly due to suboptimal antihistamine therapy (Table 1). Notably, only one-third of the patients reported pollinosis, and a mere 2% reported asthma, suggesting that the disease is unrelated to atopy.

a Flowchart of the patients included in the COVURT study. b Patients characteristics across the three groups. Foot note *cohort COVURT, §cohort COSED, ^cohort Immunovax.
Follow-up survey
A year later, we contacted the same patients for a follow-up survey, to which 61 patients responded (Table 2). Similar to the previous survey, 64% were middle-aged females (median age 41.5); 92% developed CU after the booster shot with Spikevax. CU was still active in 53% of these cases. In 41% (13/32) of cases (compared to 42% in 2022), patients reported inducible factors, primarily dermographism (68% compared to 77% in 2022). Of note, we could confirm the high prevalence of dermographism in patients who volunteered to come for a blood test. Of 40 patients analyzed, 19 had a negative FricTest, 12 had a strongly positive test (3 or 4), and in 10 patients, the test was only slightly positive (1/4, 2/4). When further analyzing the 2023 survey, the UCT score, number of lesions, and pruritus severity showed clear improvement compared to 2022. Yet the disease was still insufficiently controlled in 50% of the patients. Only four patients received omalizumab, which was discontinued in three cases. Worsening of CU by non-steroidal anti-inflammatory drugs was reported by 10% of cases (Tables 1 and 2). Importantly, mRNA vaccine was readministered in four CU patients—two in remission and two with persistent symptoms (Comirnaty in 3 and Spikevax in one) (Table 3). Subsequent immunization was not associated with CU re-occurrence or worsening.
COVID-19 and chronic urticaria
We further explored the potential association between COVID infection and CU. Based on our surveys, only 34% and 44% of patients reported a formal SARS-CoV-2 infection in 2022 and 2023, respectively. When analyzing the time to CU comparing COVID infection and vaccination, we observed that COVID infection was rarely detected before CU onset (Fig. 2a). Interestingly, CU exacerbation after infection occurred in one-third of the cases in 2022 and 15% in 2023. We also compared the CU onset dates with official COVID infection reports and vaccination dates in the population of the canton of Vaud. Interestingly, the peak of booster vaccinations preceded the peak of CU cases, which in turn preceded the peak of COVID cases (Fig. 2b). Antibodies against the nucleocapsid were negative in 21/50 (42%) of subjects tested. Importantly, seropositivity to the nucleocapsid as a surrogate for past COVID infection did not influence the UCT in 2022 nor disease duration (Supplementary Fig. 1A, B). These findings suggest that, in contrast to the vaccine, there is not association between COVID infection and CU.

a Distribution per participant of the days before (negative values) and after (positive values) the onset of chronic urticaria for the latest SARS-Cov-2 vaccination (black circles) and COVID-19 infection (gray squares) (n = 84, 4 missing values for onset date). b Peak incidence of the first booster (n = 312,723), new-onset chronic urticaria after booster (n = 74), and COVID-19 cases over time (n = 260,802). Only patients who developed CU after November 1st, 2021 without missing values were included in the analysis. VD, canton of Vaud.
Vaccine sensitization and chronic urticaria
We then explored the potential link between vaccine sensitization and CU. To do this, we conducted basophil activation tests (BAT) using a cryopreserved batch of the Spikevax vaccine, which we previously validated18. Out of 50 blood samples tested, two patients had no basophils, and four were excluded due to basophil areactivity. BAT was positive in 64% of the cases. To further understand the relevance of this sensitization, we included patients without a history of CU from two separate cohorts monitored by our division. The first cohort (n = 105) consisted of 59 patients with long COVID and 46 patients with an acute COVID infection yet without persistent symptoms. The second cohort comprised 30 healthy vaccinated volunteers. We were able to subgroup these patients according to the type of vaccine received (Spikevax versus BNT 162b2) and the number of doses (0-1-2-booster) (Fig. 3a). Notably, sensitized patients were predominantly those vaccinated with the Spikevax booster, regardless of their CU status. Females were sensitized in 60% compared to 44% of males. Younger age was associated with a higher rate of sensitization (Fig. 3b). Sensitization didn’t predict the duration of CU (Fig. 3c). No significant difference in CD63 levels on basophils, an activation marker, was observed in sensitized patients when comparing the two vaccines (Fig. 3d).

a Table summarizing the percentage of patients across the different cohort studies with positive versus negative basophil activation tests (BAT). Associations between the different variables were assessed using a Fisher exact test. b Age (mean and SD) of patients with a positive (+) (n = 45) or negative (−) BAT (n = 132). c CU duration in patients with a positive (+) (n = 19) or negative (−) BAT (n = 12). d CD63 expression (BAT condition shown 0.1%, missing data n = 8) in patients with a positive BAT who received the Spikevax (n = 32) and the BNT 16b2 (n = 4). e CD63 expression in CU patients with a positive (≥10 μg/ml) (n = 19) versus negative (n = 14) serology for the nucleocapsid (BAT condition shown 0.1%, missing data n = 11). Anti-nucleocapsid (f) and anti-spike (g) titers in patients with positive (+) (n = 45) or negative (−) BAT (n = 132). h Neutralizing activities against the different SARS-COV2 variants in patients with a positive (+) (n = 45) or negative (−) BAT (n = 132), or (i) with (n = 45) /without CU (n = 61) among patients who received the booster. j Table summarizing the percentages of patients across the different cohort studies with positive or negative Phadiatop results. For 13 patients, not sufficient material to perform the analysis. k Phadiatop titer in patients with a negative (−) (n = 55) or positive (+) (n = 16) BAT. l Phadiatop titer correlated to CD63 expression in patients with a positive BAT and phadiatop result (n = 12, BAT condition shown 0.1%, missing data n = 4). BAT, basophil activation tests; Nucl, nucleocapsid, CU chronic urticaria; ns non-significant. Statistics. Mean and SD are shown. Unpaired two-sided T tests or two-way ANOVAs were used for statistical analysis. For the tables, Fisher’s exact test was performed for each vaccine on a contingency table comparing the number of donors who received one, two, or three doses with the number of unvaccinated donors in the BAT-negative and BAT-positive groups (as a reference). In (a), Fisher’s exact test was performed on a contingency table comparing the number of donors who received the mRNA-1273 booster in the BAT-negative and BAT-positive groups, along with their cohort or gender.
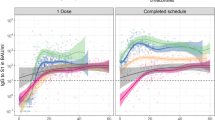
It was previously suggested that control patients who recovered from COVID infection are more likely sensitized against the vaccine23. Thus, we wanted to evaluate the frequency and level of anti-nucleocapsid antibodies in patients with positive and negative BAT against the vaccine. Anti-nucleocapsid antibodies did not correlate with higher CD63 expression. In fact, sensitized patients exhibited significantly lower level of nucleocapsid antibodies arguing against a direct link between COVID infection and vaccine sensitization (Fig. 3e, f). On the other hand, we found that sensitized patients had higher levels of anti-Spike antibodies, which correlated with a better neutralization against the wild-type but not the Omicron variant (Fig. 3h). Intriguingly, CU patients also had significantly higher anti-Spike neutralizing activity against the wild-type compared to patients from the two control cohorts (Immunovax, COSEDH) (Fig. 3i). Thus, our results suggest that younger females with good vaccine immuno-reactivity are at a higher risk of developing CU and getting sensitized against the vaccine. However, vaccine sensitization does not appear to be associated with the onset of CU.
Atopy and chronic urticaria
To understand whether new-onset CU following mRNA vaccination was associated with atopy, i.e., a genetic predisposition to produce IgE against common respiratory allergens, we performed a Phadiatop analysis. This test quantifies the presence of IgE against various allergens including grass, birch, olive, mugwort, parietaria, dog, cat, horse, house dust mite, flour mite, and Cladosporium. Patients with CU were not more frequently atopic compared to those in the two control cohorts (Fig. 3j). In addition, IgE sensitization to the vaccine was not associated with atopy, nor was it correlated with the level of IgE against common respiratory allergens (Fig. 3k, l). Finally, we did not find any specific signature for CU based on a pilot bulk RNA study comparing the transcriptional profile of 15 patients with CU and 17 vaccinated heathy volunteers recruited at the university hospital of Geneva (Supplemental Fig. 2).
Discussion
This study represents the first comprehensive analysis of a large cohort of patients who developed CU following mRNA vaccination, mostly the Moderna vaccines, an observation also made by others24. The majority of patients were middle-aged individuals with in overall 54-61% suffering from an inducible form of CU. We demonstrated that CU was unrelated to the Omicron Wave, atopic predisposition, and vaccine sensitization. Importantly, 4/4 CU patients re-exposed to the mRNA vaccine did not exacerbate CU and tolerated the vaccine well. These results expand a series cases of another four patients with CU who received a subsequent COVID-19 booster vaccine without disease exacerbation at a military academy25. They also corroborate the low frequency (9%) of vaccine-induced exacerbation of CU as recently reported by the UCARE COVAC-CU study26. Altogether, these results may help reinsuring patients and possible reduce vaccine hesitancy, a feeling highly prevalent in patients who develop acute urticaria after COVID-19 vaccine27. In all cases, it is recommended to have CU under control before considering a re-vaccination28,29.
The primary objective of this study was to understand the contribution of COVID-19 infection in the onset of CU after vaccination. Thus, in acute urticaria, there is undoubtedly a causal relationship with infection, notably viral upper airway infection (mainly in children)30. In chronic urticaria, viral hepatitis, HIV, and herpes viruses are also discussed as possible triggers of CU30. For COVID-19, the relationship to CU remains scarce in the literature. A case series from five Urticaria Centers of Reference and Excellence (UCARE) reported only 14 cases with a mean of 18 days after infection31. While, we cannot exclude a contribution of the Omicron wave in the onset and/or exacerbation of CU after vaccination, our survey revealed only rare cases of COVID-19 infection prior to CU and was reported by only 34% of the patients. Importantly, a positive titer against the nucleocapsid did not correlated with disease duration nor with disease severity. Finally, even if caution should be made when comparing the results of a case series cohort to the general statics of the Canton, we did not find a temporal relationship with peak of COVID cases.
Interestingly too, the incidence of CU reported to the Swiss national pharmacovigilance database was significantly higher than in other countries. This could be related to the notably higher proportion of Spikevax administered in Switzerland as compared to other European countries (Fig. 4). Whether this explains the higher number of CU cases remains still speculative. Finally, reinfection with SARS-CoV-2 only led to CU exacerbation in a minority of cases (15%). This is less than initially reported by a cross-sectional, international study that found that one third of the patients had CU exacerbation upon SARS-CoV2 infection32. Since this study was performed before the Omicron wave, it is tempting to speculate that the variants and disease severity may influence the mast-cell degranulation sensitivity in CU patients.

The map of Europe shows the proportion of individuals who received Spikevax (black) and the Comirnaty (blue circles) vaccines for each country. The larger the circle is, the larger the frequency is. The red arrow indicates Switzerland. Data were downloaded from the European Centre for Disease Prevention and Control (ECDC) and Federal Office of Public health (FOPH) of Switzerland on November 27th. Bivalent vaccines were not included in the analysis.
In our study, we observed a substantial number of patients who were sensitized to mRNA vaccines independently of known allergies nor active CU. These findings are consistent with the higher prevalence of positive skin tests in patients vaccinated with Spikevax13. This sensitization is mediated through specific IgE against the spherical polyethylene glycol (PEG) conformation of the lipid nanoparticle33. The clinical relevance of those IgE remains undefined. On the one hand, they could contribute to protective immunity as previously suggested in the context of flu vaccines34 corroborating the positive association we observed between the anti-spike titer and anti-vaccine IgE. On the other hand, they could predispose individuals to developing allergic reactions35. At this stage, this remains speculative as it has been repeatedly shown that the majority of sensitized patients can tolerate the vaccine33. Thus, there is growing evidence showing that immediate reactions are primarily non-IgE dependent, due to complement activation36, and that C5a could be a relevant biomarker of anaphylaxis37. In conclusion, IgE against PEG molecules on lipid nanoparticles (LNP) are frequently produced after multiple exposures to mRNA-based vaccines independently of CU. Their clinical relevance requires further investigation and careful monitoring.
We did not observe a direct link between CU and atopy. This is corroborated by the rate of allergic rhinitis (28%) in CU patients which is comparable to the general population and confirmed by the Phadiatop analysis, which was positive in one-third of CU patients, a rate not higher than that observed in controls. Thus, the relationship between atopy and CU, while frequently discussed, is currently recognized as a co-occurring condition without a clear pathogenetic link12,38. Even in cases of auto-allergic or type 1 CU, conditions associated with self-antigen IgEs like anti-TPO or anti-IL2439,40, atopic disease affects less than half of the patients39.
As of June 1st 2022, in Switzerland, 44% and 26 % of the population were fully vaccinated with Spikevax and Comirnaty, respectively41. Yet, over 90% of CU occurred after the Spikevax booster. Several hypotheses might explain this observation. Firstly, the mRNA content in the Spikevax vaccine is higher (100 μg) compared to Comirnaty (30 μg). Secondly, the Spikevax vaccine seems more stable in solution than Comirnaty after reconstitution18. Thus, we recently demonstrated that cell lines become spike protein positive in culture when exposed to Spikevax but not to Comirnaty18. Apart from the dosage differences, the Pfizer and Moderna platforms have few distinctions, with some variations in the structures of LNP carriers. Both contain PEG-2000, albeit in different forms and quantities (ALC-0519 and ALC-0315 in Comirnaty, PEG2006-DMG in Spikevax (8,20,52,53)) potentially also contributing to the immunogenicity of the vaccine. Thus, it has been repeatedly shown that the mRNA-1273 vaccine elicits higher and more persistent antibody production22,42,43. Future research should explore the contribution of vaccine intervals and prior COVID-19 infection as risk factors for the development of new-onset CU.
This study has several limitations. First, this study only recruited patients who developed CU with a temporal relationship to the vaccination. Thus, we did not include CU patients unrelated to the vaccine as a control group. As the study started after the booster doses, there could also be a selection bias towards patients who received multiple doses. Yet, the data from the Swissmedic showed that CU occurred in 81% of the cases after the booster11. Secondly, we did not investigate the presence of type IIb autoimmune mechanisms by performing autologous serum skin tests, immunoassays for IgG autoantibodies, or indirect basophil activation tests14. Thirdly, several measures, such as total IgE, IgG anti-thyroid peroxidase, and complete blood count, were not available for all patients in this study. Indeed, CU is associated with an increased odds ratio for antithyroid antibodies and a higher incidence of autoimmune diseases including rheumatoid arthritis, Sjögren’s syndrome, celiac disease, type I diabetes mellitus, and systemic lupus erythematosus44. Given that only 4 out of 58 required omalizumab, of which 75% were able to discontinue the treatment, one might speculate that type IIb autoimmune CU, which is typically more refractory to anti-IgE therapies14, is less frequently present in our CU population. Thus, future metanalysis should compare the phenotype of our population to other CU cases which are unrelated to vaccination.
In conclusion, our one-year survey revealed that CU remained active in about 50% of the cases, with the inducible form of CU being quite common. There was no direct correlation between the onset of CU, PEG sensitization, atopy, and the concurrent Omicron virus infection. The fact that several individuals were able to tolerate an additional dose of the COVID mRNA vaccine without disease exacerbation, and considering that new onset CU remains a relatively rare event following vaccination, strongly suggests that the mRNA vaccine is not an inducer for CU but rather a facilitator in predisposed individuals. Yet, repeated exposure to the vaccine appears to be necessary in most cases to reveal this predisposition, indicating that a vaccine-specific pre-existing immunity may provide a favorable condition and environment for recruitment of a CU-specific B cell repertoire. Therefore, future research should focus on characterizing the nature of the auto-antibody response and comparing it to CU cases that are temporally unrelated to mRNA vaccines. Finally, the results of this study should not prevent nor restrain any vulnerable patients from getting vaccinated or boosted for COVID-19.
Data availability
The clinical data are not publicly available due to ethical restrictions. The raw sequencing data files for RNA sequencing generated in this study have been deposited in the GEO database: GSE272645. The source data for Figs. 2a-b, 3b-l and 4 are provided in Supplementary Data 1. All other data supporting the findings of this study are available from the corresponding author on reasonable request.
Code availability
The associated R scripts are available on https://github.com/MathildeFogPerez/manuscript-CU-schwab/ Foglierini Perez, M.45. R script used in the manuscript ‘Features of chronic urticaria after COVID-19 mRNA vaccine’. Zenodo. https://doi.org/10.5281/zenodo.1393966845, and on Duperrex, O.46. R script for Fig. 2A and B of manuscript ‘Features of chronic urticaria after COVID-19 mRNA vaccine’ by Schwab et al. Zenodo. https://doi.org/10.5281/zenodo.1397095546.
Abbreviations
- BAT:
-
basophil activation test
- CIU:
-
chronic inducible urticaria
- COVID-19:
-
coronavirus disease
- CSU:
-
chronic spontaneous urticaria
- CU:
-
chronic urticaria
- EAACI:
-
European Academy of Allergology and Clinical Immunology
- FcεRI:
-
high-affinity IgE receptor
- Spikevax:
-
The mRNA-1273 Moderna vaccine
- NSAID:
-
non-steroidal anti-inflammatory drugs
- PEG:
-
polyethylene glycol
- Comirnaty:
-
BNT 162b2 vaccine from BioNtech/Pfizer
- SARS-CoV2:
-
severe acute respiratory syndrome coronavirus 2
- UCT:
-
urticaria control test
References
Zhang, Z., Shen, Q. & Chang, H. Vaccines for COVID-19: a systematic review of immunogenicity, current development, and future prospects. Front. Immunol 13, 843928 (2022).
Public Summary SwissPAR—Spikevax® [Internet]. Available from https://www.swissmedic.ch/swissmedic/fr/home/ueber (2023).
Comirnaty®, Concentré pour reconstitution d’une dispersion injectable (Tozinameranum) [Internet]. Available from https://www.swissmedic.ch/swissmedic/fr/home/humanarzneimittel/authorisations/new-medicines/comiraty-tozinameranum.html (2023).
Swissmedic octroie une autorisation de durée limitée au vaccin Nuvaxovid de Novavax contre le Covid-19 [Internet]. [cited 2023 Aug 10]. Available from https://www.swissmedic.ch/swissmedic/fr/home/news/coronavirus-covid-19/zl-nuvaxovid-novovax.html.
Contrats d’acquisition des vaccins COVID-19 [Internet]. Available from https://www.bag.admin.ch/bag/fr/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/impfen/beschaffungsvertraege-covid-19-impfstoffe.html (2023).
OFSP Office fédéral de la santé publique. Coronavirus: Vaccination contre le COVID-19 [Internet]. Available from https://www.bag.admin.ch/bag/fr/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/information-fuer-die-aerzteschaft/covid-19-impfung.html (2023).
Reports of suspected adverse reactions to COVID-19 vaccines in Switzerland—update 29 [Internet]. Available from https://www.swissmedic.ch/swissmedic/en/home/news/coronavirus-covid-19/covid-19-vaccines-safety-update-19.html (2023).
Klein, N. P. et al. Surveillance for adverse events after COVID-19 mRNA vaccination. JAMA 326, 1390–1399 (2021).
Pescosolido, E. et al. Clinical and immunological data from chronic urticaria onset after mRNA SARS-CoV-2 vaccines. Clin. Exp. Allergy 52, 1343–1346 (2022).
Wolfson, A. R., Freeman, E. E. & Blumenthal, K. G. Urticaria 12 days after COVID-19 mRNA booster vaccination. JAMA 327, 1702–1703 (2022).
Duperrex, O., Tommasini, F. & Muller, Y. D. Incidence of chronic spontaneous urticaria following receipt of the COVID-19 vaccine booster in Switzerland. JAMA Netw Open 6, e2254298 (2023).
Zuberbier, T. et al. The international EAACI/GA²LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy 77, 734–766 (2022).
Stehlin, F. et al. Intradermal testing with COVID-19 mRNA vaccines predicts tolerance. Front. Allergy 3, 818049 (2022).
Kolkhir, P. et al. Autoimmune chronic spontaneous urticaria. J. Allergy Clin. Immunol. 149, 1819–1831 (2022).
Dobin, A. et al. STAR: ultrafast universal RNA-seq aligner. Bioinformatics 29, 15–21 (2013).
Liao, Y., Smyth, G. K. & Shi, W. featureCounts: an efficient general purpose program for assigning sequence reads to genomic features. Bioinformatics 30, 923–930 (2014).
Tarazona, S. et al. Data quality aware analysis of differential expression in RNA-seq with NOISeq R/Bioc package. Nucleic Acids Res. 43, e140 (2015).
Alcaraz-Serna, A. et al. Basophil activation tests with cryopreserved mRNA-based COVID-19 vaccines. Allergol. Int. 72, 600–603 (2023).
Porret, R. et al. Atopy as an independent predictor for long-term patient and graft survival after kidney transplantation. Front. Immunol 13, 997364 (2022).
Fenwick, C. et al. Changes in SARS-CoV-2 spike versus nucleoprotein antibody responses impact the estimates of infections in population-based seroprevalence studies. J Virol 95, e01828–20 (2021).
Fenwick, C. et al. A high-throughput cell- and virus-free assay shows reduced neutralization of SARS-CoV-2 variants by COVID-19 convalescent plasma. Sci. Transl. Med. 13, eabi8452 (2021).
Obeid, M. et al. Humoral responses against variants of concern by COVID-19 mRNA vaccines in immunocompromised patients. JAMA Oncol 8, e220446 (2022).
Labella, M. et al. The value of the basophil activation test in the evaluation of patients reporting allergic reactions to the BNT162b2 mRNA COVID-19 vaccine. Allergy 77, 2067–2079 (2022).
Nickels, A. et al. Case series of patients with acute and chronic urticaria after COVID-19 vaccination. Ann Allergy Asthma Immunol. 132, 395–397 (2024).
Miller, M. A., Raffetto, E. R. & Lee, R. U. Chronic spontaneous urticaria following mRNA COVID-19 booster vaccination at a military academy. Mil Med. 189, e911–e914 (2024).
Kocatürk, E. et al. Urticaria exacerbations and adverse reactions in patients with chronic urticaria receiving COVID-19 vaccination: Results of the UCARE COVAC-CU study. J Allergy Clin Immunol 152, 1095–1106 (2023).
Judd, A. et al. Urticaria after COVID-19 vaccination and vaccine hesitancy. J. Allergy Clin. Immunol. Pract. 11, 958–960 (2023).
Picard, M., Stone, C. A. & Greenhawt, M. Management of patients with immediate reactions to COVID-19 vaccines. J. Allergy Clin. Immunol. 151, 413–415 (2023).
Banerji, A., Norton, A. E., Blumenthal, K. G., Stone, C. A. & Phillips, E. Rapid progress in our understanding of COVID-19 vaccine allergy: a cause for optimism, not hesitancy. J. Allergy Clin. Immunol. 150, 12–16 (2022).
Kocatürk, E. et al. How infection and vaccination are linked to acute and chronic urticaria: a special focus on COVID-19. Viruses 15, 1585 (2023).
Öztaş Kara, R. et al. Features of chronic spontaneous urticaria induced by COVID-19. Int. Arch. Allergy Immunol. 184, 792–796 (2023).
Kocatürk, E. et al. The global impact of the COVID-19 pandemic on the management and course of chronic urticaria. Allergy 76, 816–830 (2021).
Ieven, T. et al. Endotyping of IgE-mediated polyethylene glycol and/or polysorbate 80 allergy. J. Allergy Clin. Immunol. Pract. 11, 3146–3160 (2023).
Smith-Norowitz, T. A. et al. Long term persistence of IgE anti-influenza virus antibodies in pediatric and adult serum post vaccination with influenza virus vaccine. Int. J. Med. Sci. 8, 239–244 (2011).
Nagao, M., Fujisawa, T., Ihara, T. & Kino, Y. Highly increased levels of IgE antibodies to vaccine components in children with influenza vaccine-associated anaphylaxis. J. Allergy Clin. Immunol. 137, 861–867 (2016).
Stehlin, F. et al. Graded-dosing immunization in adults at risk for immediate-type reactions to mRNA SARS-CoV-2 vaccines. Allergol. Int. 72, 332–334 (2023).
Lim, X. R. et al. Anaphylatoxin complement 5a in Pfizer BNT162b2-induced immediate-type vaccine hypersensitivity reactions. Vaccines (Basel) 11, 1020 (2023).
Chen Q., Y. X., Ni B., Song Z. Atopy in chronic urticaria: an important yet overlooked issue. Authorea 15 (2023).
Sánchez, J., Sánchez, A. & Cardona, R. Causal relationship between anti-TPO IgE and chronic urticaria by in vitro and in vivo tests. Allergy Asthma Immunol. Res. 11, 29–42 (2019).
Schmetzer, O. et al. IL-24 is a common and specific autoantigen of IgE in patients with chronic spontaneous urticaria. J. Allergy Clin. Immunol. 142, 876–882 (2018).
FOPH, F. O. O. P. H. https://www.covid19.admin.ch/en/vaccination/status?vaccZoomVaccine=2021-01-27_2022-08-26&vaccZoomDev=2021-04-19_2022-09-04.
Steensels, D., Pierlet, N., Penders, J., Mesotten, D. & Heylen, L. Comparison of SARS-CoV-2 antibody response following vaccination with BNT162b2 and mRNA-1273. JAMA 326, 1533–1535 (2021).
Collier, A. Y. et al. Differential kinetics of immune responses elicited by Covid-19 vaccines. N. Engl. J. Med. 385, 2010–2012 (2021).
Confino-Cohen, R. et al. Chronic urticaria and autoimmunity: associations found in a large population study. J. Allergy Clin. Immunol. 129, 1307–1313 (2012).
Foglierini Perez, M. R script used in the manuscript ‘Features of chronic urticaria after COVID-19 mRNA vaccine’. Zenodo https://doi.org/10.5281/zenodo.13939668 (2024).
Duperrex, O. R script for Figs. 2A and 2B of manuscript ‘Features of chronic urticaria after COVID-19 mRNA vaccine’ by Schwab et al. Zenodo https://doi.org/10.5281/zenodo.13970955 (2024).
Acknowledgements
This work was supported by the Giorgi-Cavaglieri Foundation (to Y.D.M.). The authors are indebted to the patients who participated in the study, to Silvia Sabatino and Claudia Lima de Paiva Campos from the Vaccine and Immunology Center as well as to the Immunology and Allergy Department staff the for their most valuable efforts. The authors thank all the local allergists from the GVAIC who contributed to identifying patients and Giuseppe Pantaleo (Lausanne University Hospital and University of Lausanne) for critical reading and helpful comments.
AI-assisted technologies were used only to improve the grammar and readability of the text. YDM reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Author information
Authors and Affiliations
Contributions
Conceptualization: Y.D.M. Supervision: Y.D.M. Designed experiments: A.D, C.F, O.D, Y.D.M. Contributed in data collection/analysis: J.S., M.F., E.V., I.P., G.A.R.B., N.M., C.P., V.M., Y.D.M. Provided reagents and advice: C.F., C.R., M.B., A.D., O.D. Wrote the original draft: J.S. Y.D.M. Reviewed and edited the manuscript: all. All authors approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare the following competing interests: Dr Fenwick report having a patent pending (application No. EP20205298.1) for a SARS-Cov2 neutralization assay. Prof. Muller has received grant support/consulting income from AstraZeneca, Viatris, Blueprint Medicine, Sanofi and GSK. Prof. Didierlaurent received research grants from Moderna, GSK and Sanofi outside the scope of this study. The research was conducted without any other commercial or financial relationships that could be construed as a potential conflict of interest to this study. Authors J. Schwab, M. Foglierini, E. Pescosolido, I. Pacheco, G. A. Ruiz Buendía, N. Madelon, C. Pellaton, V. Banderet, C. Ribi, M. M. Bergmann, and O. Duperrex declare no competing interests relevant to this study.
Peer review
Peer review information
Communications Medicine thanks Emek Kocatürk Göncü and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Schwab, J., Foglierini, M., Pescosolido, E. et al. Features of chronic urticaria after COVID-19 mRNA vaccine over time. Commun Med 4, 254 (2024). https://doi.org/10.1038/s43856-024-00656-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-024-00656-y
