
Abstract
Background
Declining gait performance is seen in aging individuals, due to neural and systemic factors. Plasma biomarkers provide an accessible way to assess evolving brain changes; non-specific neurodegeneration (NfL, GFAP) or evolving Alzheimer’s disease (Aβ 42/40 ratio, P-Tau181).
Methods
In a population-based cohort of older adults, we evaluate the hypothesis that plasma biomarkers of neurodegeneration and Alzheimer’s Disease pathology are associated with worse gait performance. A sample of 2641 Mayo Clinic Study of Aging participants with measurements of plasma biomarkers and gait parameters was analyzed in this cross-sectional study. Linear regression models using plasma biomarkers as predictors of gait parameters and adjusted for age, sex, BMI, Charlson Comorbidity Index, and cognitive diagnosis were evaluated.
Results
In this study multiple statistically significant relationships are observed for GFAP, NfL, and P-Tau181 with gait parameters. Each standard deviation increase in GFAP, NfL, and P-Tau181 is associated with a reduction in velocity of 2.100 (95% CI: −3.004, −1.196; p = 5.4 × 10−6), 4.400 (−5.292, -3.507; p = 9.5 × 10−22), and 2.617 (−3.414, −1.819; p = 1.5 × 10−10) cm/sec, respectively. Overall, NfL has the strongest associations with poor gait performance. Models with age interactions show that the strength of associations between the plasma biomarkers and the gait parameters became stronger with increasing age. There are no specific gait parameters that associate with individual plasma biomarkers.
Conclusion
Plasma biomarkers of neurodegeneration and Alzheimer’s Disease pathology are not only markers of cognitive decline but also indicate motor decline in the aging population.
Plain language summary
Decline in gait and balance occurs as an individual gets older. These changes can increase risk for falls, death and disability. However, the brain changes that cause a declining gait and balance in aging are incompletely understood. Here, we evaluated gait performance in over 2000 individuals as well as blood biomarkers that indicate evolving Alzheimer’s disease or neurodegeneration. We found that gait changes in the aging individual are associated with neurodegeneration and accumulation of Alzheimer’s disease pathology independent of their memory performance. These findings offer evidence for the role of blood biomarkers in investigating gait decline. Future research will build upon these findings to expand our understanding of brain mechanisms that contribute to gait and balance abnormalities in aging individuals.
Similar content being viewed by others


Introduction
Gait and balance function incorporates several neural locomotor and cognitive brain systems that can be affected by neurodegeneration1,2. Gait decline in older individuals predicts impending morbidity from falls, nursing home placement, dementia and mortality3,4,5,6. Motoric decline is an important issue as rates of fatal falls in individuals over 65 years approximately doubled from 1999 to 2020 going from an age-adjusted mortality rate of 29.4 deaths due to falls per 100,000 people over age 65 per year in 1999 to 69.4 in 20207. The impact of disability from gait changes is predicted to increase with the growth of the aging population8. Motoric decline in an aging individual is multifactorial, but degeneration in distinct brain regions both in the cortical gray and connecting white matter is thought to play a role9,10.
Plasma biomarkers can measure by-products of non-specific neurodegeneration (NfL or GFAP) or specific neuropathologies like Alzheimer’s disease (Aβ 42/40 ratio, P-Tau181). Herein, we assess the relationship of plasma biomarkers with gait and balance function in older adults. Plasma biomarkers are less-invasive, more cost-effective, and more convenient to collect relative to biomarkers measured in cerebrospinal fluid (CSF) or through neuroimaging, such as magnetic resonance imaging (MRI) or positron emission tomography (PET) scans. Plasma biomarkers for amyloid and tau pathology, closely reflect Alzheimer’s disease-related neuropathological burden on PET imaging11,12,13,14 and in CSF15, and are associated with clinical cognitive decline16,17,18. Markers of axonal and astrocytic degeneration, such as neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP), respectively, albeit nonspecific, are markers of neuronal injury and reflect neurodegeneration19,20. Whether these plasma biomarkers are associated with motor decline in older adults is incompletely understood. When considering associations between these plasma biomarkers and gait parameters it is important to consider systemic factors that may be important confounders, affecting both gait performance and biomarkers levels. Renal dysfunction, for example, can affect the peripheral clearance of plasma biomarkers of Alzheimer’s Disease (AD) and neurodegeneration, hence affecting their levels, therefore medical comorbidities such as chronic kidney disease (CKD) should be taken into consideration when exploring these relationships21,22,23,24,25.
Few prior studies have explored the relationship between plasma biomarker levels and gait parameters. One study found no evidence of cross-sectional or longitudinal association between plasma amyloid-beta (Aβ) 42/40 ratio or NfL with gait speed in a sample of 507 individuals from the Multidomain Alzheimer’s Preventive Trial26. Another study, which utilized a large sample from the Framingham Heart Study Offspring Cohort, found that faster walking speed was associated with lower plasma total tau levels27. Gait decline in older adults is multi-factorial. The question remains whether plasma biomarkers of neurodegeneration and AD pathology reflect motor decline in older adults after controlling for age, sex, cognitive state, and medical comorbidities. While causation cannot be determined in a cross-sectional study, we sought to explore possible neural contributors to motor decline by assessing the relationship between plasma biomarkers of neurodegeneration and AD neuropathology in older adults. Gait is a complex multifaceted process, often quantified with different gait domains such as pace, rhythm, variability, and postural control28. Therefore, we hypothesized that analyzing diverse gait parameters, that can capture distinct properties of gait, in conjunction with a range of plasma biomarkers, may shed light on how early neurodegeneration (measured by NfL and GFAP) and AD neuropathology (measured by Aβ 42/40 ratio and P-Tau181) impacts motor performance. This premise is supported by previous work showing the differential impact of neurodegeneration on gait domains29,30,31. Our goal was to assess whether observed relationships provide insights into the neuropathological processes driving gait impairment in a cohort of older adults based on plasma biomarker profiles. In this study, we find that gait parameters associated with plasma biomarkers of AD pathology and neurodegeneration independently of cognitive status. These relationships get stronger with age and may differ between men and women.
Methods
In the present study, Aβ 42/40 ratio, GFAP, NfL, and phosphorylated tau 181 (P-Tau181) levels were measured in plasma specimens from a sample of 2641 Mayo Clinic Study of Aging (MCSA) participants. Gait parameters were measured using a pressure-sensitive walkway (GAITriteTM or ZenoTM ProtoKinetics) at or near (i.e., within a few days) the study visit corresponding to the plasma draw. We used linear regression models to evaluate relationships. Our models were controlled for important confounders such as age, sex, BMI, medical comorbidity burden (Charlson comorbidity index), and cognitive diagnosis (cognitively unimpaired-CU or cognitively impaired-CI). We also assessed how age, sex, CKD, and cognitive diagnosis each modifies observed relationships using interaction-based models. We hypothesized that higher levels of plasma biomarkers of neurodegeneration and AD (i.e., higher NfL or P-Tau181), would be associated with worse gait parameters (i.e., slower gait speed). Our exploratory hypothesis was to assess whether different gait parameters associated with distinct plasma biomarkers of neurodegeneration versus AD.
Mayo Clinic Study of Aging (MCSA)
The MCSA is a population-based study employing an age and sex-stratified random sampling scheme selected from those living in Olmsted County, Minnesota. Those consenting to study participation come into the clinic for a visit consisting of a complete neurological and neuropsychiatric exam administered by trained neurologists, neuropsychiatrists, and study coordinators. Additionally, a blood draw is performed as well as CSF collection through lumbar puncture, MRI, and PET imaging for those agreeing to participate in those aspects of the study. A clinical diagnosis of CU32,33,34,35, MCI36,37, or dementia38 is assigned to each participant at each visit based on published diagnostic criteria and further discussed at a consensus conference amongst experts in aging, dementia, and staff involved in examining the participant. The study protocol was approved by the Mayo Clinic and Olmsted Medical Center institutional review boards (IRB #14-004401). Complete study details can be found elsewhere39. Written informed consent was obtained from all participants or their legally assigned representative.
Plasma
Participants fasted overnight before plasms specimen collection. EDTA-plasma samples were collected and centrifuged. Aliquots of 500 μL each of plasma were stored at −80 °C in polypropylene tubes until testing. Simoa® Neurology 4-Plex E Advantage kit (N4PE, item #103670) was used to measure Aβ 1-40, Aβ 1-42, GFAP, and NfL. Simoa® pTau-181 Advantage V2 kit (item #103714P-Tau181) was used to measure pTau-181. Test was conducted per manufacturer’s instructions and the plasma sample was analyzed using a Quanterix HD-X analyzer (Quanterix, Lexington, MA, USA). The exact testing protocol included thawing and mixing of the plasma samples followed by centrifugation for 5 minutes at 4000 g. For each sample, 1:4 dilution was performed using the onboard dilution protocol and tested in singlet. A seven-point calibration curve and sample concentrations were determined on the Simoa® HD-X Analyzer software using a weighting factor of 1/y2 and a 4-parameter logistic curve fitting algorithm for P-Tau181. The N4PE test used eight-point calibration curves with 1/y2 weighting; a 4-parameter logistic fitting algorithm was used for NfL and GFAP, while a 5-parameter logistic fitting algorithm was used for Aβ 1-40 and Aβ 1-42. Quality control was performed with two levels after each calibration. The quality control material revealed variation between assays (expressed as % coefficient of variation) as follows: Aβ 1-40, 5% and 3% at approximate concentrations of 16 and 117 pg/mL; Aβ 1-42, 4% and 7% at approximate concentrations of 5.5 and 31 pg/mL; GFAP, 7% and 7% at approximate concentrations of 181 and 3702 pg/mL; NfL, 12% and 14% at approximate concentrations of 21 and 432 pg/mL; P-Tau181, 6% and 5% at approximate concentrations of 3.7 and 119 pg/mL. Selected plasma biomarkers were based on the assay available in this cohort at the time of this study.
Gait Assessment
Gait data was collected using a 10-meter long GAITriteTM or ZenoTM pressure sensitive walkway (ProtoKinetics). Participants were instructed to walk down the pressure sensitive walkway at a self-chosen pace. The pressure data obtained from the footfalls was processed using the Proto Kinetics Movement Analysis Software (PKMAS). Figure 1 shows a graphic representation of some of the spatial-temporal gait parameters used. Biologically meaningful variables capturing functionally relevant components of gait such as rhythm, pace, variability, and postural control were selected28. In brief, spatial features were captured using stride length. Temporal features were captured using absolute or percentage time of components of the gait cycle such as single support (time or percentage time spent on one foot per gait cycle). Spatial-temporal features were primarily summarized in velocity. Stability was also assessed using surrogate measures such as gait variability, captured using standard deviation (SD) of parameters (higher SD means greater variability)40 or center of pressure (COP) distance in stance or single support phases (shorter distance signifies abnormal foot placement). COP distance can be expressed as an absolute value or as a percentage (distance between the first and last contact of the foot expressed as a percentage of the foot length). Shorter single support time (time spent on one foot) also serves as a proxy for postural control. Those with poor balance tend to spend more time with both feet on the ground and less time with only one foot on the ground.

On a pressure sensitive mat, variables are derived through the pressure imprint of each foot and its x and y coordinates (location on the mat). In this figure a: maximum foot length, b: step length, c: stride length, d: step/stride width, e: stance center of pressure distance is the distance between the first and last contact of the foot as it lands on the ground.
Statistical analysis
There were 2654 individuals identified with gait variables, relevant covariates, and at least one plasma biomarker. We examined the data for outliers. After close review, 13 people were removed from the analysis since the data appeared to have been affected by a technical error during the gait recording session. The final sample size was 2641. Given the omitted cases had invalid data, were a small minority, and we retain a very large sample, we do not believe this introduced any bias. A cross-sectional analysis was performed using linear regression models utilizing the plasma biomarkers as predictors and the gait parameters as outcomes. From these models, the beta coefficient estimates, confidence intervals (CI), adjusted r-squared values, and p-values are presented. All models included age, sex, BMI, Charlson Comorbidity Index, and cognitive diagnosis as covariates. The plasma biomarkers were standardized into z-scores (i.e., subtract the mean and divide by the SD) to be able to compare plasma marker coefficients for each gait outcome. Age was centered (i.e., subtract mean) and divided by 10 to be able to interpret coefficients as changes by decade. Log transformations (base e) were applied to stride velocity SD, stride length SD, stride width SD, and stance time to improve linear model fit. The linear models were also run, separately, including plasma biomarker interactions with age, sex, CKD, and cognitive diagnosis. These models employed a complete cases approach to missing data in that they used only observations where all variables included in the given model were non-missing. Medical comorbidities were extracted using an algorithm that searches the medical record for established diagnoses to assess presence of CKD. The usual alpha level of 0.05 was utilized to determine statistical significance. All data preparation and analysis were performed using SAS version 9.4 (SAS Institute, Cary, NC) and R version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Results
This study included 2641 participants in the MCSA with available gait and plasma biomarker data. Cohort characteristics are summarized by cognitive diagnosis category in Supplementary Data 1. The age range of those included was 50 to 98 with a mean of 73 and a standard deviation [SD] of (10.4) years. There were slightly more males (53.3%) than females and 10.2% had CKD. Cognitive diagnosis was 78.4% cognitively unimpaired (CU) and 21.6% cognitively impaired (CI - mild cognitive impairment [MCI]: 20.7%, Dementia: 0.9%). The mean body mass index (BMI) was 28.4 (5.2) kg/m2 and the mean Charlson Comorbidity Index was 3.4 (3.3). Over three-quarters of the cohort was CU, and as expected, individuals with cognitive impairment were older, and had worse gait parameters and more abnormal plasma biomarker levels. Rates of menopause were high (98.3% in CU and 100% in CI) and rates of hormone replacement therapy use were overall low (approximately 10% in CU and under 5% in the CI groups), see Supplementary Table 1 for details.
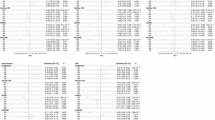
All linear regression models were controlled for age, sex, BMI, Charlson Comorbidity Index, and cognitive diagnosis to assess the relationship between plasma biomarkers and gait parameters independent of these factors (results are summarized in Supplementary Data 2). Only stride width SD was found to be statistically significantly related to Aβ 42/40 ratio. On the other hand, multiple statistically significant associations were found for GFAP, NfL, and P-Tau181 with gait parameters. The most notable relationships were with velocity and stride length. Each SD increase in GFAP, NfL, and P-Tau181 was associated with a reduction in velocity of 2.100 (95% CI: −3.004, −1.196; p = 5.4 × 10−6), 4.400 (−5.292, −3.507; p = 9.5 × 10−22), and 2.617 (−3.414, −1.819; p = 1.5 × 10−10) cm per second, respectively. Similarly, each SD increase in GFAP, NfL, and P-Tau181, was associated with a 1.766 (−2.514, -1.017; p = 4.0 × 10−6), 3.764 (−4.503, −3.025; p = 4.2 × 10−23), and 2.112 (−2.775, −1.450; p = 4.6 × 10−10) cm shorter stride length, respectively. Additionally, stance center of pressure (COP) distance, single support (SS) COP distance and single support (%) decreased, and stance time increased, all of which is consistent with worse gait performance, with higher plasma biomarker (NfL, GFAP, P-Tau 181) levels in a statistically significant manner. NfL tended to have the strongest associations. Velocity and stride length denote pace, while single support time and center of pressure measurements are a surrogate for balance or postural control. Results are presented graphically as a forest plot in Fig. 2. Meeker and Guo et al have demonstrated possible utility of normalizing CSF P-Tau 181 by Aβ 40 in predicting AD neuropathology41,42. This approach has not been applied to plasma biomarker measurements, however we explored this ratio with results included in supplementary data 1. The predictive power of this ratio was overall weaker than using P-Tau 181 in adjusted models, hence this was not included in further analyses.

Dots correspond with beta coefficients from linear regression models adjusting for age, sex, body mass index, Charlson Comorbidity Index, and cognitive diagnosis, and the ends of the lines represent the 95% lower and upper confidence limits, respectively, from these models. Although the overall sample size was 2641, sample sizes used in the models ranged from 2628 to 2632 depending on the availability of the plasma marker variable included in each model. Coefficients where the 95% confidence interval does not cross the vertical dotted line are statistically significant. See supplementary data 2 for complete model results including p-values. SD Standard deviation, GFAP Glial fibrillary acidic protein, NfL Neurofilament light chain, COP Center of pressure, SS Single support.
As detailed above, statistically significant associations were discovered between plasma biomarkers and gait parameters while controlling for age. However, to assess how advancing age influences these relationships, we evaluated whether there were any significant interactions between plasma biomarkers and age using interaction terms in the linear models (Supplementary Data 3). Evidence for interactions with the plasma biomarkers in predicting gait variables was observed, for age with GFAP, NfL, and P-Tau181. This means that while there was a relationship between higher plasma biomarkers of neurodegeneration and AD with worsening gait parameters independent of age, this relationship was compounded with advancing age. As an example, those at the average age had slower velocity, on average, by 2.975 (−4.122, −1.828; p = 4.0 × 10−7) and 1.854 (−2.762, −0.946; p = 6.4 × 10−5) cm/sec for each one SD increase in NfL and P-Tau181, respectively. Each of these associations strengthened with increasing age: with each additional decade of age above the mean, each SD increase in NfL corresponded to an additional reduction in velocity of 1.726 (−2.602, -0.849; p = 1.2 × 10−4) cm/sec and each SD increase in P-Tau181 was associated with an additional decrease in velocity of 1.583 (−2.488, −0.677; p = 6.1 × 10−4) cm/sec. Similarly, those at the average age for this sample had no observed relationship between GFAP and velocity (−0.298; −1.447, 0.851; p = 0.611), but with each additional decade above the mean, each SD increase in GFAP was associated with slower velocity by an additional 2.207 (-3.082, -1.333; p = 8.0 × 10−7) cm/sec. This strengthening of the association with increasing age between plasma markers GFAP, NfL, and P-Tau181 and gait outcomes was also seen for stride length, SS COP distance, stance time, and single support (%). These interaction model results, along with models noted previously without interaction terms, demonstrate that the association between plasma biomarkers and gait parameters exists across the age spectrum and is strengthened by advancing age. No statistically significant interactions with age were seen for Aβ 42/40 ratio.
The effect of sex was evaluated using models including sex interaction terms with the plasma biomarkers to predict gait parameters (Supplementary Data 4). Some differences in the associations were seen for women when compared to men. We found higher GFAP, NfL, and P-Tau181 to be associated with lower single support (%) and longer stance time for women, with these associations either attenuated or no longer statistically significant for men. For example, amongst women, each one SD increase in GFAP, NfL, and P-Tau181 were, respectively, associated with lower single support by 0.383 (-0.512, -0.253; p = 7.8 × 10−9), 0.467 (−0.599, -0.334; p = 5.8 × 10−12), and 0.360 (-0.502, -0.219; p = 6.5 × 10−7) with positive sex interaction effects indicating less association for men (GFAP: 0.294 [0.131, 0.457; p = 4.1 × 10−4]; NfL: 0.197 [0.034, 0.359; p = 0.018]; P-Tau181: 0.208 [0.038, 0.377; p = 0.017]). On the other hand, increased levels in these three biomarkers were all associated with lower stance COP distance in men with these associations not being present for women.
We also evaluated whether there was an effect of CKD or cognitive diagnosis on the observed relationship between plasma biomarkers and gait parameters. Very few statistically significant interactions were noted for cognitive diagnosis and CKD. For example, a higher P-Tau181 level was associated with increased stride velocity SD, stride length SD, and stride width SD for those without CKD but not for those with CKD. This suggests that observed relationships between plasma biomarkers and gait parameters were not driven by CKD. Higher NfL was associated with longer stance time and lower single support (%) for those CU with these associations strengthening for those with cognitive impairment pointing to more imbalance experienced by those with cognitive impairment. There were only four other statistically significant interaction terms, suggesting that the observed relationships between plasma biomarkers and gait parameters were not driven by cognitive impairment status. These models were controlled for age, medical comorbidity burden, sex, and BMI. For complete interaction results, see Supplementary Data 5-6.
Discussion
In this cross-sectional study, we evaluated the relationships between plasma biomarkers of Alzheimer’s neuropathology and neurodegeneration with gait performance in a sample from a large population-based cohort of aging individuals. As hypothesized, higher levels of plasma biomarkers (GFAP, NfL, and P-Tau181) were associated with worse gait parameters in the pace, rhythm, and postural stability domains. These plasma biomarkers of neurodegeneration and AD neuropathology, which are commonly related to cognition, also appear to be markers of gait and balance decline in an aging cohort. These relationships were statistically significant even after controlling for age, sex, BMI, medical comorbidity burden, and cognitive diagnosis. NfL appeared to be most strongly related to gait parameters, however, associations were also observed for GFAP and P-Tau 181, suggesting that both axonal neurodegeneration and early AD neuropathology may contribute to motor decline in aging individuals. Prior studies have shown that worse gait performance is associated with multiple neuropathologies43,44,45,46. We also found a differential effect of plasma biomarkers on some gait parameters with increasing age and for women compared to men. We did not identify any specific gait parameter associated with a single specific plasma biomarker. Most of the gait parameters were associated with at least one, but often multiple, plasma biomarkers. Significant associations existed more so with pace and rhythm followed by postural stability and variability domains.
NfL had the strongest relationships with the gait variables. NfL is a non-specific marker of neuro-axonal injury20,47. NfL has been seen to increase with age48, which we accounted for by including age in our models. It is also elevated in aging individuals with poor physical function26 as well as in a variety of neuropathological processes, such as Alzheimer’s disease, Amyotrophic Lateral sclerosis (ALS), and Parkinson’s Disease49,50. With a low false positive rate, it is an effective tool to assess neurodegeneration, according to a recent multicenter validation study51. Elevated NfL may signal evolving pathological changes in neuronal gait circuits. We also found strong associations with GFAP, an astrocytic cytoskeletal protein that signals neurodegeneration and correlates with disability19, and P-Tau181, which is a marker of early Alzheimer’s disease-related neuropathological change52,53,54,55. No strong correlations between amyloid beta and gait metrics were seen in this cohort. This finding may be due to the sensitivity of the test assay used or the lack of biological significance of amyloid alone in gait change, however, the latter cannot be determined from the current study and will need further investigation. Plasma biomarkers provide an accessible and cost-effective global estimate of neurodegeneration in the brain, however, specific brain regions are known to play a role in motor function. While detailed neuroimaging is beyond the scope of this article, prior studies have implicated prefrontal, supplementary motor, sensory-motor cortices, hippocampus, basal ganglia, and their connecting white matter tracts in mediating gait decline in older adults56,57,58,59. Altered structural and functional connectivity of brain regions mediating attention and sensory-motor function has been associated with gait performance60,61,62. Whereas older adults who demonstrate resistance to motor and cognitive decline, termed “superagers” tend to have higher brain volumes63.
The effect of age on the relationship between plasma biomarker levels and gait is an important consideration64,65. In an aging cohort, elevated levels of NfL in individuals over 60 years of age were shown to correlate with atrophy signifying neuro-axonal injury, which could manifest as gait changes64. Our findings agreed with this report, in that advancing age tended to strengthen the relationships between elevated plasma biomarkers and worse gait measures in older individuals, potentially signaling the accumulating burden of neuropathological changes in gait pathways. These relationships also existed when controlling for age as a covariate, meaning that there is also an age-independent association between plasma biomarkers and gait parameters. Plasma biomarker elevation (P-Tau181, NfL, amyloid beta) has been shown to be associated with faster cognitive decline in MCI and dementia16,54,66. Future longitudinal studies could further assess whether a similar association is present between plasma biomarkers and progressive gait and balance decline seen in neurodegenerative diseases with careful consideration of other systemic mediators of gait dysfunction in older adults such as medical comorbidities, sarcopenia etcetera.
Sex modified the relationship of plasma markers and some gait parameters. After adjusting for age, BMI, Charlson Comorbidity Index, and cognitive diagnosis, GFAP, NfL, and P-Tau181 were associated with lower single support (%) for women, with these associations being weaker for men. A lower single support percentage implies that the percentage of the gait cycle spent on one foot is lower, more time is spent with both feet on the ground, pointing to gait instability. Women tend to have slower gait speed and a higher dual-task cost of walking with age67,68,69. Amongst men, higher GFAP, NfL, and P-Tau181 were associated with lower stance COP distance. This association was not observed among women. While the exact reason for the observed differences is not clear, it may be because distinct gait parameters capture aspects of gait biomechanics that differ between men and women. Rowe et al have previously shown using detailed motion analysis that men and women use different walking strategies70. Prior studies have also shown the effect of sex on biological aging, for example, that women experience lower accelerated aging, but higher frailty indices compared to men in one cohort71. Survival varies between men versus women experiencing reduced gait speed72. Our results demonstrate the need to consider sex when interpreting gait parameters in an aging individual and when assessing the clinical utility of plasma biomarkers to assess the impact of neurodegeneration on gait function.
Some of the statistically significant interactions we saw with CKD showed stronger associations amongst those without CKD suggesting that our findings are not driven by CKD and are more likely to be indicative of underlying neurodegeneration. As we continue to learn about plasma markers, the influences of medical comorbidities on plasma biomarkers, especially renal function that may affect serum protein constituents, should be examined when interpreting any plasma biomarker. Prior reports have shown that plasma biomarker levels may be affected by renal function and should be considered covariates in analyses examining their association with clinical parameters73,74,75.
Another important consideration is cognitive impairment and its contribution to gait and balance function. A population-based study in Spain showed that gait variability under dual-task conditions among older adults was in part explained by declining cognition76. To assess whether cognitive impairment was driving the observed relationship between plasma biomarkers and gait parameters, we examined models controlled for cognitive state and included a cognitive diagnosis interaction term (cognitively unimpaired or cognitively impaired). Associations between plasma biomarkers and gait were statistically significant after controlling for cognitive diagnosis. Findings suggest that additional factors, other than cognitive state alone drive gait impairment in older individuals and require further investigation.
Strengths of this study include a large sample from a well-characterized population-based cohort with concurrent measurement of plasma biomarkers of Alzheimer’s pathology (amyloid and tau) and non-specific neurodegeneration (NfL and GFAP) as well as multiple gait parameters. We evaluated the relationship between these plasma biomarkers and gait performance, laying the groundwork for future research assessing the relative contributions of neurodegeneration and AD neuropathology to motor function in older adults. Our study has a few important limitations. We did not include phosphorylated tau 217 (P-Tau217) in our analysis as it was not available in the assay we used. P-Tau217 measured in plasma may be a better marker of Alzheimer’s disease (AD) neuropathology77. Another limitation is that the plasma markers utilized here were measured using an immunoassay. Mass spectrometry assays may outperform other assays in terms of detecting abnormal amyloid levels and progression to AD78. This could at least partially explain the limited number of associations between Aβ 42/40 ratio and gait measures seen in this study. Future investigations will incorporate plasma biomarkers measured via mass spectrometry and association with other markers of neurodegeneration as well as vascular pathology. The population of Olmsted County is predominantly non-Hispanic white, which may limit the overall generalizability of the findings to more diverse groups. Future work should evaluate these findings in a diverse cohort.
In this cross-sectional assessment of a sample from a population-based cohort, multiple gait variables were found to be statistically significantly associated with plasma biomarkers of Alzheimer’s pathology and neurodegeneration with worse plasma marker levels being related to worse gait performance after controlling for age, sex, BMI, medical comorbidities and cognitive diagnosis. These associations were present for GFAP, NfL, and P-Tau181. Furthermore, some of these observed relationships were modified by sex and made stronger with advancing age.
Data availability
The data used in this manuscript is from the Mayo Clinic Study of Aging (MCSA). Due to the sensitive nature of this data, it is not publicly available. Anonymized data will be available upon request in accordance with Mayo Clinic and MCSA data-sharing protocols. For data sharing, you may refer to the following website for information: https://www.mayo.edu/research/centers-programs/alzheimers-disease-research-center/research-activities/mayo-clinic-study-aging/for-researchers/data-sharing-resources. The source data for Fig. 2 is in “Supplementary Data 7”.
References
Allali, G., Ayers, E. I. & Verghese, J. Motoric cognitive risk syndrome subtypes and cognitive profiles. J. Gerontol. Ser. A 71, 378–384 (2016).
Rosso, A. L. et al. Slowing gait and risk for cognitive impairment: The hippocampus as a shared neural substrate. Neurology 89, 336–342 (2017).
Verghese, J. et al. Abnormality of gait as a predictor of non-Alzheimer’s dementia. N. Engl. J. Med. 347, 1761–1768 (2002).
Buracchio, T., Dodge, H. H., Howieson, D., Wasserman, D. & Kaye, J. The trajectory of gait speed preceding mild cognitive impairment. Arch. Neurol. 67, 980–986 (2010).
Mielke, M. M. et al. Assessing the temporal relationship between cognition and gait: slow gait predicts cognitive decline in the Mayo Clinic study of aging. J. Gerontol. A Biol. Sci. Med Sci. 68, 929–937 (2013).
Best, J. R. et al. An evaluation of the longitudinal, bidirectional associations between gait speed and cognition in older women and men. J. Gerontol. A Biol. Sci. Med Sci. 71, 1616–1623 (2016).
Santos-Lozada, A. R. Trends in deaths from falls among adults aged 65 years or older in the US, 1999-2020. JAMA 329, 1605–1607 (2023).
Steinmetz, J. D. et al. Global, regional, and national burden of disorders affecting the nervous system, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 23, 344–381 (2024).
Rosano, C. et al. Special article: gait measures indicate underlying focal gray matter atrophy in the brain of older adults. J. Gerontol. A Biol. Sci. Med Sci. 63, 1380–1388 (2008).
De Laat, K. F. et al. Cortical thickness is associated with gait disturbances in cerebral small vessel disease. NeuroImage 59, 1478–1484 (2012).
Jack, C. R. et al. Predicting amyloid PET and tau PET stages with plasma biomarkers. Brain 146, 2029–2044 (2023).
Milà-Alomà, M. et al. Plasma p-tau231 and p-tau217 as state markers of amyloid-β pathology in preclinical Alzheimer’s disease. Nat. Med. 28, 1797–1801 (2022).
Hansson, O., Blennow, K., Zetterberg, H. & Dage, J. Blood biomarkers for Alzheimer’s disease in clinical practice and trials. Nat. Aging 3, 506–519 (2023).
Chatterjee, P. et al. Diagnostic and prognostic plasma biomarkers for preclinical Alzheimer’s disease. Alzheimers Dement J. Alzheimers Assoc. 18, 1141–1154 (2022).
Ashton, N. J. et al. Plasma and CSF biomarkers in a memory clinic: Head-to-head comparison of phosphorylated tau immunoassays. Alzheimers Dement J. Alzheimers Assoc. 19, 1913–1924 (2023).
Mattsson-Carlgren, N. et al. Prediction of longitudinal cognitive decline in preclinical Alzheimer disease using plasma biomarkers. JAMA Neurol. 80, 360–369 (2023).
Aschenbrenner, A. J. et al. Comparison of plasma and CSF biomarkers in predicting cognitive decline. Ann. Clin. Transl. Neurol. 9, 1739–1751 (2022).
Tropea, T. F. et al. Plasma phosphorylated tau181 predicts cognitive and functional decline. Ann. Clin. Transl. Neurol. 10, 18–31 (2022).
Abdelhak, A. et al. Blood GFAP as an emerging biomarker in brain and spinal cord disorders. Nat. Rev. Neurol. 18, 158–172 (2022).
Khalil, M. et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 14, 577–589 (2018).
Syrjanen, J. A. et al. Associations of amyloid and neurodegeneration plasma biomarkers with comorbidities. Alzheimers Dement 18, 1128–1140 (2022).
Ramanan, V. K. et al. Association of plasma biomarkers of Alzheimer disease with cognition and medical comorbidities in a biracial cohort. Neurology 101, e1402–e1411 (2023).
Pichet Binette, A. et al. Confounding factors of Alzheimer’s disease plasma biomarkers and their impact on clinical performance. Alzheimers Dement J. Alzheimers Assoc. 19, 1403–1414 (2023).
Jiang, X., O’Bryant, S. E., Johnson, L. A., Rissman, R. A. & Yaffe, K. Health and Aging Brain Study (HABS‐HD) Study Team. Association of cardiovascular risk factors and blood biomarkers with cognition: The HABS-HD study. Alzheimers Dement Amst. Neth. 15, e12394 (2023).
Mielke, M. M. et al. Performance of plasma phosphorylated tau 181 and 217 in the community. Nat. Med. 28, 1398–1405 (2022).
He, L. et al. Cross-sectional and longitudinal associations between plasma neurodegenerative biomarkers and physical performance among community-dwelling older adults. J. Gerontol. A Biol. Sci. Med Sci. 76, 1874–1881 (2021).
Jacob, M. E. et al. Grip strength, gait speed an plasma markers of neurodegeneration in asymptomatic middle-aged and older adults. J. Frailty Aging 11, 291–298 (2022).
Lord, S. et al. Independent domains of gait in older adults and associated motor and nonmotor attributes: validation of a factor analysis approach. J. Gerontol. A Biol. Sci. Med Sci. 68, 820–827 (2013).
Pieruccini-Faria, F. et al. Gait variability across neurodegenerative and cognitive disorders: Results from the Canadian Consortium of Neurodegeneration in Aging (CCNA) and the Gait and Brain Study. Alzheimers Dement J. Alzheimers Assoc. 17, 1317–1328 (2021).
Hagoort, I., Vuillerme, N., Hortobágyi, T. & Lamoth, C. J. C. Age and walking conditions differently affect domains of gait. Hum. Mov. Sci. 89, 103075 (2023).
Jayakody, O. et al. Age-related changes in gait domains: Results from the LonGenity study. Gait Posture 100, 8–13 (2023).
Ivnik, R. J. et al. Mayo’s older Americans normative studies: Updated AVLT norms for ages 56 to 97. Clin. Neuropsychol. 6, 83–104 (1992).
Ivnik, R. J. et al. Mayo’s older Americans normative studies: WAIS-R norms for ages 56 to 97. Clin. Neuropsychol. 6, 1–30 (1992).
Ivnik, R. J. et al. Mayo’s older Americans normative studies: WMS-R norms for ages 56 to 94. Clin. Neuropsychol. 6, 49–82 (1992).
Malec, J. F. et al. Mayo’s older Americans normative studies: Utility of corrections for age and education for the WAIS-R. Clin. Neuropsychol. 6, 31–47 (1992).
Petersen, R. C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 256, 183–194 (2004).
Winblad, B. et al. Mild cognitive impairment–beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 256, 240–246 (2004).
Diagnostic and Statistical Manual of Metal Disorders. Fourth. American Psychiatric Association; 2000.
Roberts, R. O. et al. The Mayo Clinic Study of Aging: design and sampling, participation, baseline measures and sample characteristics. Neuroepidemiology 30, 58–69 (2008).
Lugade, V. & Kaufman, K. Center of pressure trajectory during gait: a comparison of four foot positions. Gait Posture 40, 252–254 (2014).
Meeker, K. L. et al. Comparison of cerebrospinal fluid, plasma and neuroimaging biomarker utility in Alzheimer’s disease. Brain Commun. 6, fcae081 (2024).
Guo, T. et al. Normalization of CSF pTau measurement by Aβ40 improves its performance as a biomarker of Alzheimer’s disease. Alzheimers Res. Ther. 12, 97 (2020).
Wennberg, A. M. V., Savica, R. & Mielke, M. M. Association between various brain pathologies and gait disturbance. Dement Geriatr. Cogn. Disord. 43, 128–143 (2017).
Wennberg, A. M. V. et al. Cerebral amyloid deposition is associated with gait parameters in the Mayo Clinic Study of Aging. J. Am. Geriatr. Soc. 65, 792–799 (2017).
Wennberg, A. M. V. et al. Longitudinal association between brain amyloid-beta and gait in the Mayo Clinic Study of Aging. J. Gerontol. A Biol. Sci. Med Sci. 73, 1244–1250 (2018).
Sullivan, K. J. et al. Imaging-based indices of Neuropathology and gait speed decline in older adults: the atherosclerosis risk in communities study. Brain Imaging Behav. 15, 2387–2396 (2021).
Leuzy, A. et al. Blood-based biomarkers for Alzheimer’s disease. EMBO Mol. Med. 14, e14408 (2022).
Bornhorst, J. A. et al. Plasma neurofilament light chain (NfL) reference interval determination in an Age-stratified cognitively unimpaired cohort. Clin. Chim. Acta Int J. Clin. Chem. 535, 153–156 (2022).
Lin, Y. S., Lee, W. J., Wang, S. J. & Fuh, J. L. Levels of plasma neurofilament light chain and cognitive function in patients with Alzheimer or Parkinson disease. Sci. Rep. 8, 17368 (2018).
Lu, C. H. et al. Neurofilament light chain. Neurology 84, 2247–2257 (2015).
Ashton, N. J. et al. A multicentre validation study of the diagnostic value of plasma neurofilament light. Nat. Commun. 12, 3400 (2021).
Tissot, C. et al. Plasma pTau181 predicts cortical brain atrophy in aging and Alzheimer’s disease. Alzheimers Res Ther. 13, 69 (2021).
McGrath, E. R. et al. Blood Phosphorylated Tau 181 as a biomarker for amyloid burden on brain PET in cognitively healthy adults. J. Alzheimers Dis. 87, 1517–1526 (2022).
Mielke, M. M. et al. Plasma phospho-tau181 increases with Alzheimer’s disease clinical severity and is associated with tau- and amyloid-positron emission tomography. Alzheimers Dement J. Alzheimers Assoc. 14, 989–997 (2018).
Karikari, T. K. et al. Blood phosphorylated tau 181 as a biomarker for Alzheimer’s disease: a diagnostic performance and prediction modelling study using data from four prospective cohorts. Lancet Neurol. 19, 422–433 (2020).
Fettrow, T., Hupfeld, K., Hass, C., Pasternak, O. & Seidler, R. Neural correlates of gait adaptation in younger and older adults. Sci. Rep. 13, 3842 (2023).
Wilson, J., Allcock, L., Mc Ardle, R., Taylor, J. P. & Rochester, L. The neural correlates of discrete gait characteristics in ageing: A structured review. Neurosci. Biobehav Rev. 100, 344–369 (2019).
Zapparoli, L., Mariano, M. & Paulesu, E. How the motor system copes with aging: a quantitative meta-analysis of the effect of aging on motor function control. Commun. Biol. 5, 1–15 (2022).
Tian, Q. et al. The brain map of gait variability in aging, cognitive impairment and dementia. A systematic review. Neurosci. Biobehav. Rev. 74, 149–162 (2017).
Zheng, J. J. J., Delbaere, K., Close, J. C. T., Sachdev, P. S. & Lord, S. R. Impact of white matter lesions on physical functioning and fall risk in older people: a systematic review. Stroke 42, 2086–2090 (2011).
Allali, G. et al. The neural basis of age-related changes in motor imagery of gait: An fMRI Study. J. Gerontol. Ser. A 69, 1389–1398 (2014).
Kim, C. W., Kim, Y., Kim, H. H. & Choi, J. Y. The aspect of structural connectivity in relation to age-related gait performance. Psychoradiology 3, kkad028 (2023).
Garo-Pascual, M. et al. Brain structure and phenotypic profile of superagers compared with age-matched older adults: a longitudinal analysis from the Vallecas Project. Lancet Healthy Longev. 4, e374–e385 (2023).
Khalil, M. et al. Serum neurofilament light levels in normal aging and their association with morphologic brain changes. Nat. Commun. 11, 812 (2020).
De Wolf, F. et al. Plasma tau, neurofilament light chain and amyloid-β levels and risk of dementia; a population-based cohort study. Brain J. Neurol. 143, 1220–1232 (2020).
Simrén, J. et al. The diagnostic and prognostic capabilities of plasma biomarkers in Alzheimer’s disease. Alzheimers Dement J. Alzheimers Assoc. 17, 1145–1156 (2021).
Piche, E. et al. Effects of age, sex, frailty and falls on cognitive and motor performance during dual-task walking in older adults. Exp. Gerontol. 171, 112022 (2023).
Sialino, L. D. et al. The sex difference in gait speed among older adults: how do sociodemographic, lifestyle, social and health determinants contribute? BMC Geriatr. 21, 340 (2021).
Callisaya, M. L., Blizzard, L., Schmidt, M. D., McGinley, J. L. & Srikanth, V. K. Sex modifies the relationship between age and gait: a population-based study of older adults. J. Gerontol. A Biol. Sci. Med Sci. 63, 165–170 (2008).
Rowe, E., Beauchamp, M. K. & Astephen Wilson, J. Age and sex differences in normative gait patterns. Gait Posture 88, 109–115 (2021).
Phyo, A. Z. Z. et al. Sex differences in biological aging and the association with clinical measures in older adults. GeroScience 46, 1775–1788 (2024).
Studenski, S. et al. Gait speed and survival in older adults. JAMA 305, 50–58 (2011).
Zhang, B. et al. Effect of renal function on the diagnostic performance of plasma biomarkers for Alzheimer’s disease. Front Aging Neurosci. 15, 1150510 (2023).
Dittrich, A. et al. Association of chronic kidney disease with plasma NfL and other biomarkers of neurodegeneration. Neurology 101, e277–e288 (2023).
Wu, J. et al. The impact of kidney function on plasma neurofilament light and phospho-tau 181 in a community-based cohort: the Shanghai Aging Study. Alzheimers Res Ther. 16, 32 (2024).
Zhou, J. et al. The age-related contribution of cognitive function to dual-task gait in middle-aged adults in Spain: observations from a population-based study. Lancet Healthy Longev. 4, e98–e106 (2023).
Palmqvist, S. et al. Discriminative accuracy of Plasma Phospho-tau217 for Alzheimer disease vs other neurodegenerative disorders. JAMA 324, 1–11 (2020).
Janelidze, S. et al. Head-to-head comparison of 10 plasma phospho-tau assays in prodromal Alzheimer’s disease. Brain 146, 1592–1601 (2022).
Acknowledgements
We would like to thank the participants and staff at the Mayo Clinic Study of Aging. Funding supporting this work came from RF1-AG069052, U01AG006786, NINDS K23-NS124688, and Tianqiao & Chrissy Chen Institute.
Author information
Authors and Affiliations
Contributions
F.A. led the study design and manuscript draft. J.A.S. led statistical analysis and assisted in manuscript drafting along with W.K.K. D.J.F., M.M.M., and A.A.S. contributed to plasma biofluid analysis and interpretation. A.A.S. and R.C.P. provided overall guidance and critical revisions. L.B. provided input on data analysis, and manuscript draft. R.C.P., P.V., J.G.R., G.W., C.R.J., and D.S.K. participated in study design and conceptualization, review and interpretation of results, manuscript draft, and editing.
Corresponding author
Ethics declarations
Competing interests
Authors declare the following competing interests: Farwa Ali receives funding from the NIH. Walter K. Kremers receives research funding from NIH, Astra Zeneca, Biogen, and Roche. Michelle M. Mielke receives research support from the NIH and DOD and has consulted for Biogen, Brain Protection Company, LabCorp, Lilly, Merck, Roche, Siemens Healthineers, and Sunbird Bio. Clifford R. Jack receives no personal compensation from any commercial entity. He receives research support from NIH, the GHR Foundation, and the Alexander Family Alzheimer’s Disease Research Professorship of the Mayo Clinic. David S. Knopman serves on a data safety monitoring board for the Dominantly Inherited Alzheimer Network TREATMENT UNIT (DIAN-TU) study and was an investigator in clinical trials sponsored by Biogen, Lilly Pharmaceuticals, and the University of Southern California. Prashanthi Vemuri receives research support from the NIH. Jonathan Graff-Radford receives funding from the NIH. He is an investigator in clinical trials sponsored by Biogen, Eisai, and the University of Southern California. He serves on the DSMB for NINDS StrokeNET. B. Gwen Windham receives funding from the NIH. Ronald C. Petersen has consulted for Roche, Inc.; Genentech, Inc.; Eli Lilly, Inc.; Nestle, Inc. and Eisai, Inc.; a DSMB for Genentech, Inc. and receives royalties from Oxford University Press for Mild Cognitive Impairment and from UpToDate. His research funding is from NIH/NIA. Alicia Algeciras-Schimnich has participated in advisory boards for Roche Diagnostics, Fujirebio Diagnostics, and Siemens Healthineers. Jeremy A. Syrjanen, Dan J. Figdore, and Leland R. Barnard report no disclosures.
Peer review
Peer review information
Communications Medicine thanks the anonymous reviewers for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ali, F., Syrjanen, J.A., Figdore, D.J. et al. Association of plasma biomarkers of Alzheimer’s pathology and neurodegeneration with gait performance in older adults. Commun Med 5, 19 (2025). https://doi.org/10.1038/s43856-024-00713-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-024-00713-6
This article is cited by
-
Critical perspectives on proenkephalin A 119–159 for shock-associated acute kidney injury
International Urology and Nephrology (2025)
-
Elevated plasma GFAP levels in MCI link APOE ε4 allele with impaired gait speed
GeroScience (2025)
-
Sensorimotor function as an early marker of cognitive decline and alzheimer’s biomarker burden
GeroScience (2025)
