
Abstract
Background
Vaccine-preventable diseases and common viral infections pose substantial public health challenges worldwide. Applying multiplex serological assays to samples collected from cross-sectional studies allows assessment of population-level immunity to a broad range of pathogens.
Methods
We develop a high-throughput multiplex serological assay using bead-based Luminex technology to measure IgG antibody responses to a broad panel of pathogens. Vaccine preventable diseases include pertussis, diphtheria, tetanus, measles, mumps, and rubella. Common viral infections include adenovirus, cytomegalovirus, Epstein-Barr virus, chickenpox, respiratory syncytial virus, echovirus, Coxsackie B virus, rhinovirus, norovirus, rotavirus, influenza A, hepatitis A, hepatitis E, and the seasonal coronaviruses 229E, OC43, NL63, and HKU1. Measured antibody responses are analysed with statistical models to assess seroprevalence within the French population.
Results
The analysis of 2132 serum samples from French children and adults reveals notable variation in seroprevalence among different age groups. Consistently high seroprevalence for endemic viruses is observed across all age groups, suggesting widespread exposure from a young age and continuous exposure throughout life. Similarly, mandatory vaccine seroprevalence remains consistently high, reflecting a strong vaccination coverage in France.
Conclusions
These findings highlight the potential of high-throughput multiplex serology assays for routine surveillance of common viral infections and assessment of vaccine coverage.
Plain language summary
Vaccine-preventable diseases such as measles and common viral infections, including seasonal coronaviruses that cause common colds, pose significant public health challenges worldwide. We developed a test for measuring immunity against eight vaccine-preventable diseases and eighteen common viral infections in the French population. The analysis of over 2000 blood samples from French children and adults revealed notable variations in immunity among different age groups. Consistently high levels of immunity for common viral infections was observed across all age groups, suggesting widespread exposure from a young age and continuous exposure throughout life. We observed high levels of immunity to vaccine-preventable diseases, but with some notable immunity gaps in young children.
Similar content being viewed by others


Introduction
Serology is used for surveillance by detecting past or concurrent infections by measuring antibodies to specific pathogens. Traditionally, serological tests have been based on assaying the functional activity of antibodies, for example by observing how antibodies bind and neutralize a virus and prevent the formation of viral plaques. At present, the most widely used serological test is an enzyme-linked immunosorbent assay (ELISA) which measures antibodies bound to a target antigen. Neutralization assays and ELISA assays are single-plex, meaning that each experiment measures one biomarker.
Multiplex platforms allow antibody responses to multiple antigens to be measured using as little as 1 μL of serum. Multiplex serological assays are poised to revolutionise the field of sero-epidemiology by enormously increasing the quantity of available data. Notable technologies include bead-based assays (10 s–100 s of antigens), protein microarrays (100 s–1000 s of antigens)1 and phage arrays (100,000+ antigens)2. Two of the most widely used multiplex platforms for serological assays are the Luminex MAGPIX® (capable of measuring 50 analytes per sample) and the Luminex INTELLIFLEX® (500 analytes per sample). Advantages of these bead-based systems are low cost per sample, low sample volume, low measurement error, and ease of transfer to other labs3,4,5. Challenges to the development of multiplex serological assays include difficulties in identifying experimental conditions that are optimal for all considered pathogens, selection of appropriate controls, and analysis of the large amount of data generated.
Two of the most promising applications for multiplex assays are serological surveillance of vaccine preventable diseases (VPDs) and common viral infections (CVI). In France, childhood vaccination is mandatory6 for: diphtheria, tetanus, poliomyletis (DTP), pertussis, Haemophilus influenzae type B, hepatitis B, and pneumococcus with doses recommended at 2, 4 and 11 months of age; measles, mumps, and rubella with doses recommended at 12 and 18 months; and meningococcus C with doses recommended at 5 and 12 months7,8. Vaccines are funded through a co-payment model7. Coverage with these vaccines has varied over time, but typically exceeds 95%9, although there is substantial variation between population sub-groups, for example people with lower incomes are more likely to exhibit vaccine hesitancy10. There are optional vaccination programmes for tuberculosis, rotavirus, meningococcus B, human papillomavirus (HPV), influenza, COVID-19, and varicella-zoster virus (VZV). In addition, adult booster doses of DTP are recommended at ages 25, 45, 65, and then every 10 years; a pertussis booster dose is recommended for pregnant women; and a VZV booster dose is recommended for people aged 65 and over. These programs have been essential in reducing the incidence of VPDs and alleviating their publich health burden. The coverage of vaccination programs can be estimated from national public health data, but this data is typically incomplete. Vaccination coverage can instead be estimated from serological surveys based on samples from the general population. A notable example is the case of The Netherlands where multiplex serological assays are routinely used for surveillance of vaccine coverage11.
CVIs such as adenovirus, respiratory syncytial virus (RSV), norovirus, seasonal coronavirus and enteroviruses, pose a persistent burden to human health and can cause various respiratory and gastrointestinal symptoms. While these infections are generally mild, they can lead to more severe complications in children and immunocompromised individuals12,13,14. Additionally, the ongoing emergence of new infectious agents such as SARS-CoV-2 underscores the need for continuous surveillance to address emerging infectious threats15,16,17.
To gain insight into the epidemiology of circulating pathogens and assess population protection against infections, a focus on pathogen surveillance and immune monitoring is crucial. Valuable information on prevalent respiratory viruses and seasonal patterns is provided by routine PCR testing of hospitalized patients with clinical symptoms16,18. However, its effectiveness as a surveillance tool is constrained by the large number of asymptomatic or mildly symptomatic respiratory infections19. This limitation makes it impractical to estimate the prevalence of infections solely through PCR testing. Additionally, the abundance of co-circulating pathogens, sharing similar clinical profiles, notably fever and cough, poses a substantial challenge for symptomatic surveillance, particularly in environments where children gather, such as daycare and school settings20,21,22. This study specifically focuses on immune surveillance, employing antibody measurements as a cost-effective method to assess seroprevalence and immunity in the population.
Understanding both individual and population-level immunity is essential for designing effective surveillance programs. Individual immunity, acquired through natural infection or vaccination, is influenced by various factors such as age, genetics, and environmental exposures23. In contrast, population immunity, also known as herd immunity, refers to the indirect protection against infectious diseases that occurs when a substantial portion of the population become immune, either through vaccination or prior infection. This concept plays a crucial role in limiting the spread of infectious agents within a community.
In response to an infection or vaccination, the immune system produces antibodies, also known as immunoglobulins (Ig), that possess the ability to recognize and neutralize a pathogen. Among these, IgG antibodies persist for years after infection or immunization and are actively synthesized by plasma B cells, which originate from the differentiation of memory B cells24. This ensures a continuous and sustained production of antibodies, contributing substantially to long-term immunity. This robust immune response prevents reinfections and mitigates the severity of the disease in the event of a second infection. In the case of children, monitoring antibody levels provides valuable insights into their first exposure to an infectious disease and vaccination status.
Here we describe the development of a high-throughput multiplex serology assay to assess IgG levels against a comprehensive panel of eight mandatory vaccine-preventable diseases (VPDs) comprising tetanus, diphtheria, measles, mumps, rubella, pertussis, papillomavirus, and 18 common viral infections (CVIs) typically occurring in early childhood stages, including adenovirus, cytomegalovirus (CMV), RSV and varicella-zoster virus (VZV). This assay is applied to samples from the French population to provide a quantitative description of multi-pathogen sero-epidemiology.
Methods
The SeroPed study
In this cross-sectional study 1132 serum samples were collected from children and adults who were attending hospitals in northeastern France between February 2020 and August 2020 to evaluate the seroprevalence of SARS-CoV-225. Samples from individuals providing blood samples for routine medical procedures in participating hospitals were eligible for inclusion in the study. Samples from individuals with confirmed or suspected COVID-19 were excluded. The samples used in this study consisted of leftover samples derived from routine medical testing within French hospital laboratories. They were processed in accordance with existing regulations and guidelines of the French Commission for Data Protection (Commission Nationale de l’Informatique et des Libertes). All identifiable information was destroyed for these samples, with the exception of age, sex and hospital location.
Table 1 summarizes the number and percentage of individuals in each age and sex group. The age of the sampled individuals ranges from 0 to 100 years old, with a special note for those labeled < 1 who were sampled at the hospital at the time of birth. This last inclusion allows us to gain insights into the presence of maternal antibodies
The Milieu Intérieur cohort
The Milieu Intérieur (MI) cohort consists of 1000 healthy adults recruited in Rennes, France between 2012 and 201326. Participants were chosen based on the absence of any indication of severe, chronic, or recurrent medical conditions. Samples from 1000 individuals were available for the current study, 500 female and 500 male, ranging from 20−70 years of age with 100 men and 100 women in each 10 year age group. This cohort is used to validate our assay by comparing it with serological data generated using clinically graded immunoassays on 900 samples.
The clinical study was approved by the Comité de Protection des Personnes - Ouest 6 on June 13, 2012, and by the French Agence Nationale de Sécurité du Médicament on June 22nd, 2012. The study is sponsored by Institut Pasteur (Pasteur ID-RCB Number: 2012-A00238-35) and was conducted as a single-center study without any investigational product. The original protocol was registered under ClinicalTrials.gov (study# NCT01699893). The samples and data used in this study were formally established as the Milieu Intérieur biocollection (NCT03905993), with approvals by the Comité de Protection des Personnes—Sud Méditerranée and the Commission Nationale de l’Informatique et des Libertés (CNIL) on April 11, 2018.
Antigens included in the assay
We assembled a list of antigens for pathogens on the basis of epidemiological interest and commercial availability. In some cases, it was possible to obtain multiple antigens for the same pathogen. In total, we included 15 distinct antigens targeting 8 vaccine-preventable diseases (tetanus, diphtheria, measles, mumps, rubella, human papillomavirus, pertussis) and 32 antigens targeting 15 viral infections commonly observed during early childhood stages (including adenovirus, cytomegalovirus, respiratory syncytial virus).
The proteins used were either purchased from Native Antigen (Oxford, UK), ProSpec-Tany Techno Gene (Israel), Ray Biotech (Georgia, US) or NIBSC (Herts, UK). Antigen names, suppliers, catalogue numbers, expression systems, and coupling conditions (optimal antigen concentration and coupling buffer) are provided in Supplementary Data 1.
Antigen-bead coupling
To establish this assay, 47 distinct Luminex magnetic bead regions were utilized, where each antigen was coupled to a specific bead type. The magnetic beads were vortexed before being transferred to a 1.5 mL microcentrifuge tube. For the preparation of a 500 µL antigen-coupled bead premix, 125 µL of each Luminex magnetic bead type was employed. Subsequently, a magnetic rack was used to remove the supernatant before washing the beads with Milli-Q water. The beads were activated using 0.1 M sodium phosphate (NaP) pH 6.2, 10 mg/mL of EDC (1-ethyl-3-[3-dimethylaminutesopropyl] carbodiimide hydrochloride) and 10 mg/mL sulfo-NHS (sulfo N- hydroxylsulfosuccinimide), followed by incubation on a rotor in the dark for 20 min at room temperature. This activation step allows the coupling of antigens to magnetic beads, through the formation of a covalent bond formed between a stable ester on the surface of the bead and the primary amine of the antigen. Thereafter, a magnetic rack was used to remove the supernatant before the beads underwent two washes with PBS 1X (phosphate-buffered saline). The mass of proteins coupled onto the beads was optimized previously, using a reference pool and validated by generating a log-linear standard curve, ensuring optimal antigen concentration coupling. The antigen-coupled beads were incubated either with PBS 1X or MES buffer (determined during the optimization stage) on a rotor in the dark overnight, at 4 °C. Subsequently, the antigen-coupled beads underwent three washes with PBS-TBN (phosphate buffer saline supplemented with 1% bovine serum albumin, 0.02% sodium acid and 0.05% Tween-20) and were resuspended in 500 µl of PBS-TBN buffer before being stored at 4 °C.
Multiplex serological assay
The multiplex serological assay was performed using a panel of 47 antigen-coupled beads encompassing VPDs and CVIs. To measure the antibody levels against these antigens, we employed the Intelliflex® instrument from Luminex®.
In a 96-well plate, 50 µL of 1/100 diluted serum (for 1/200 final serum dilution) and 50 µL of antigen-coupled beads premix (500 beads/region/µL) were added. All serum dilutions and bead premixes were prepared in PBT buffer (phosphate buffered saline containing 1% bovine serum albumin and 0,05% (v/v) Tween-20). Then the plate was incubated on a shaker in the dark for 30 min, at room temperature. Three wash steps follow incubation, placing the 96-well plate on a magnetic plate separator (Luminex®, Austin, Texas, USA) with washes performed with PBT buffer. For the detection of specific IgG, a secondary antibody conjugated to R-phycoerythrin (from Jackson Immunoresearch, UK; cat#709-116-098) was utilized at a 1/120 dilution. 50 µL of the secondary antibody was added into each well and incubated on a shaker in the dark for 15 min at room temperature. Following incubation, three wash steps were performed using a magnetic plate separator and PBT buffer. Finally, 100 µL of PBT buffer was added as the final volume. Plates were read using the Intelliflex® system at low PMT setting and the median fluorescence intensity (MFI) was measured.
Each 96-well plate included a blank (beads without serum) as a control for background signal, along with a 7 point-2-fold serum dilution (1/50 to 1/102,400) of a reference pool of French donors. During the optimization phase, a sample set of French serum samples from a SARS-CoV-2 cohort study27 were screened from which 15 serum samples with the highest MFI for a large number of the pathogens included in the panel were selected for the reference pool. To conduct further analysis, a five-parameter logistic curve was employed to convert the MFI to relative antibody unit (RAU), relative to a standard curve of the reference pool on the same plate. Analysis of RAU data allows for assessment of quality control, adjustment of plate-to-plate variation, and ensures quantitative measures are titres.
Reference IgG immunoassays
To further validate the multiplex assay, a comparison was carried out using matched samples from healthy French MI participants. Complementary antigen-specific serological tests using ELISA were conducted to measure IgG levels within 900 samples of the MI cohort, following the manufacturer’s guidelines as previously described28. This validation was performed for a subset of ten antigens where it was possible to use commercially available ELISA kits23.
Anti-HBs and anti-HBc IgGs were measured on the Architect automate (CMIA assay, Abbott). Anti-CMV IgGs were measured by CMIA using the CMV IgG kit from Beckman Coulter on the Unicel Dxl 800 Access automate (Beckman Coulter). Anti-measles, anti-mumps, and anti-rubella IgGs were measured using the BioPlex 2200 MMRV IgG kit on the BioPlex 2200 analyzer (Bio-Rad). Anti-Toxoplasma gondii IgGs were measured using the BioPlex 2200 ToRC IgG kit on the BioPlex 2200 analyzer (Bio-Rad). Anti-influenza A IgGs were measured by ELISA using the NovaLisa IgG kit from NovaTec (Biomérieux) that explores responses to grade 2 H3N2 Texas 1/77 strain. In all cases, the manufacturers established the criteria for serostatus definition (positive, negative, or indeterminate).
Statistics and reproducibility
To determine sero-positivity status it is necessary to select a cut-off for each measured antibody response. Due to substantial variation in the epidemiology of the studied pathogens, it was not possible to use a single statistical method for selecting a sero-positivity cut-off. We instead developed a decision tree based on prior knowledge of pathogen exposure or vaccination, and whether the data followed a bimodal distribution (Fig. 1).

Decision tree used to choose between the different methods available to determine the cut-off discriminating between seropositive and seronegative patients.
The decision of low or high exposure was based on expert epidemiological knowledge of whether a pathogen had expected seroprevalence > 50% in France. For example, respiratory viruses and most vaccine preventable diseases are all expected to have seroprevalence > 50%. In cases of low exposure, if a visual examination of the data from all samples indicated that log antibody levels followed a bimodal distribution, we applied a Gaussian Mixture Model (GMM). This method was applied only to the Cytomegalovirus antigen.
In cases of low exposure when the data did not follow a bimodal distribution, we analysed data from children <5 years. We assume that when exposure is low, the majority of young children are unexposed and seronegative. A cut-off was selected based on the mean plus two standard deviations of samples from children < 5 years. For normally distributed data, this corresponds to specificity = 97.7%. This method was applied to analyse antibody levels to hepatitis A, hepatitis E, HPV16, and HPV18 antigens.
In cases of high exposure, we examined log antibody levels in children < 5 years. This group was selected to increase the likelihood of obtaining a substantial proportion of negative samples29. If the data followed a bimodal distribution, we applied a GMM. This method was applied to antibody data specific for adenovirus T3 and T5 lysates, HKU1 spike, OC43 spike, echovirus, NL63 spike, 229E spike, measles nucleoprotein, measles lysate, rubella, norovirus GII.4 VP1, Respiratory syncytial virus B, Epstein-Barr virus, tetatuns toxin (NIBSC), and varicella-zoster virus antigens.
When there was no evidence for a bimodal distribution, we focused on data from individuals aged 18–60 years. We assume that when exposure is high, the majority of adults are exposed and seropositive. We exclude adults > 60 years because of the possibility of immunosenescence. In this framework, it was not possible to control specificity, so we instead selected a cut-off corresponding to sensitivity = 95%. As the data were not always normally distributed, we did not attempt to calculate means and standard deviation, but instead we calculated the cut-off based on the 5% percentile of the data. This method was applied to antibody data specific for Bordella p. toxin, OC43 nucleoprotein, HKU1 nucleoprotein, NL63 nucleoprotein, enterovirus CoxB3 VP1, adenovirus T5, mumps lysate, norovirus GII. 6 VLP, Respiratory syncytial virus A, Respiratory syncytial virus gG, rhinovirus T1A lysate, rotavirus VP7, tetanus toxin (NA), mumps, rubella E2, 229E nucleoprotein, mumps nucleoprotein, influenza A, Bordetella p.FHA, adenovirus T40, norovirus GII.4 VLP antigens.
A Gaussian Mixture Model (GMM) was used if the data were bimodally distributed. Formally, \({{Ab}}_{i}\) denotes the antibody level (MFI) of patient \(i\) and \({{Ab}}_{i}\, \sim \,\left(1-\theta \right)N\left({\mu }_{{neg}},{\sigma }_{{neg}}\right)+\theta N\left({\mu }_{{pos}},{\sigma }_{{pos}}\right)\), with \(\theta \) the prevalence of seropositive patients in this subpopulation, \({\mu }_{{neg}}\) and \({\mu }_{{pos}}\) the mean antibody levels of the seronegative and seropositive patients respectively and \({\sigma }_{{neg}}\) and \({\sigma }_{{pos}}\) their standard deviation. Thus, the model was defined by the following equation:
From which the estimated cut-off was derived as: \({\mu }_{{neg}}+2{\sigma }_{{neg}}\). This GMM is applicable to data on measured antibody responses from the total population, or to the restricted data from children under five. GMM parameters were estimated in a Bayesian statistical framework using Markov Chain Monte Carlo with Metropolis-Hastings sampling implemented in R. We assumed uniform priors such that θ ~ U(0,1). We assumed all other parameters ~ U(0, 10) based on knowledge of the dynamic range of the assay. MCMC chains were run for 10,000 iterations, discarding the first 1000 iterations for burn-in. The effective sample size for all chains was > 300. Cut-offs were estimated based on the median of the posterior distributions.
The cut-off determined in MFI was converted to RAU using the same method as for the samples.
To compare the seroprevalence between males and female, two-sided Pearson’s chi-squared statistical tests were performed using Rstudio. Microsoft Excel 2016 and R version 4.0.5. were used to conduct all analysis. The following R-Studio packages were required: dplyr, readxl, tidyr, ggplot2, openxlsx, forcats, scales, stringr, corrplot, patchwork, cowplot, ggrepel and gridExtra.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Results
Multiplex assay validation
Our multiplex assay is validated against clinical-grade ELISA assays by evaluation of the correlation in measured antibody levels between the two assays. ELISA assays were conducted on 900 samples from the Milieu Intérieur cohort on a subset of ten antigens. This subset includes four vaccine preventable diseases: rubella, mumps, measles, and hepatitis B as well as common persistent/recurrent viruses: CMV, EBV, VZV, influenza A, along with the parasite Toxoplasma gondii. In contrast to our assay, some commercially available ELISA tests lack information regarding the specific antigen target, however we have access to raw quantitative data along with the clinical interpretation of the serological status (either seropositive, seronegative or undefined/grey zone).
Strong correlations are observed for antigens such as Rubella, Measles, and VZV with 93.7%, 91.9% and 93.3% of individuals classified as seropositive (showed in green) with the reference assays (Fig. 2). This aligns closely with our in-house assay, which shows a seroprevalence of 97.8%, 90.3%, and 99.8% for each virus, respectively. Despite a high degree of correlation of measured antibody levels between assays for both Rubella and VZV, the estimated seroprevalence using the multiplex assay is substantially higher than when using ELISA. We attribute this to the selection of a more sensitive sero-positivity cut-off for the multiplex assay. For the remaining antigens the correlation is less pronounced. For EBV, a large number of samples reach the upper limit of the assay, whereas with our multiplex assay, they exhibit a broader dynamic range of RAU values, which result in the appearance of a weaker correlation. Lastly, the results for Toxoplasmosis are inconclusive, as no correlation is observed. Due to a lack of confidence in the quality of our serological assay for Toxoplasmosis, we refrain from reporting results for this pathogen.

Comparison of the serological data generated by the in-house Luminex INTELLIFLEX assay and those from clinical-grade ELISA assays using n = 1000 biologically independent samples. The x-axis displays relative antibody units (RAU), while the y-axis represents the unit from the various reference tests. Serological interpretation of the clinical-grade assays is shown, distinguishing between negatives (red), positives (green) and undetermined (grey). The data for this figure are available in Supplementary Data File 2.
Vaccine preventable diseases panel
Antibody levels against vaccine preventable diseases from different age groups are shown in Fig. 3. High antibody levels are detected in children <1 year old (newborns), consistent with the presence of maternal antibodies. When examining antibodies levels for antigens such as measles nucleoprotein or rubella VLP, we not only observe the initial presence of antibodies but also their subsequent decline before the administration of the MMR vaccine, typically around 12–18 months of age.

Data from n = 1132 biologically independent samples from the SeroPed study are presented. Relative Antibody Units (RAU) are calculated using the median fluorescence intensity (MFI) from a Luminex INTELLIFLEX. The horizontal dotted lines represent the antigen-specific cut-off for seropositivy. Vertical dotted lines denote specific recommended vaccination schedules. Antibody levels were colour-coded, according to the vaccine: red for Diphtheria, Tetanus, and Pertussis (DTaP) vaccine; blue for Measles, Mumps, Rubella (MMR) vaccine. The data for this figure are available in Supplementary Data File 3 and Supplementary Data File 4.
Although we do not have data on which individuals were vaccinated, a notable increase in antibody titers is observed following the recommended timing of vaccine doses. This is particularly evident for Bordetella pertussis toxin and FHA, where multiple booster doses are administrated over several years. Following the booster dose there is a decline in antibody levels; however, antibody levels remain above the initial pre-vaccination baseline. A similar pattern of boosting followed by waning is observed for tetanus and diphtheria toxin, which are administered simultaneously as part of the DTaP vaccine. Furthermore, high antibody levels in older individuals are consistent with vaccination guidelines, which advise for a DTaP booster dose every 10 years or after experiencing an injury as a precautionary measure. This phenomenon is also observed for antigens such as Measles lysate, Measles nucleoprotein, and rubella VLP, where a rise in antibody titers is observed during adulthood, despite no administration of booster doses.
The majority of individuals pass the established seropositivity cut-off for mandatory vaccines (e.g. MMR vaccine and DTaP vaccine) from a very young age. However, for the two HPV antigens included within the panel, we refrain from presenting further analyses of seroprevalence, as we did not have sufficient accompanying epidemiological data to support the calculation of a cut-off for sero-positivity. Age-stratified results have been reported in the Supplementary Fig. 5.
Common viral infections multiplex panel
As shown previously, newborns exhibit high levels of antibodies, indicating the transfer of antibodies acquired during the mother’s life. For diseases where vaccination is unavailable for infants and toddlers, the decline of maternal antibodies during the first year of life is apparent. This decrease is particularly evident for adenovirus and VZV. (Fig. 4)

Data from n = 1132 biologically independent samples from the SeroPed study are presented. Relative Antibody Units (RAU) have been generated using the median fluorescence intensity (MFI) measurements. The horizontal dotted lines represent the antigen-specific cut-offs for seropositivity. Antibody levels were colour-coded for clarity, with each distinct colour corresponding to a specific virus family or genus. The data for this figure are available in Supplementary Data File 3 and Supplementary Data File 4.
For gastro-intestinal viruses, there is a noticeable rise in antibody levels around 2 years of age, implying early exposure to these viruses. This pattern, characterized by the decline in temporary immunity conferred by the mother and the subsequent rise in antibodies following the first infection, is notably pronounced for antibodies targenting different adenovirus antigens. In contrast, a distinct pattern unfolds with the VZV, revealing a sharp increase in antibody levels around 4 years of age. This suggests that the first exposure to this virus occurs later in life, possibly in environments such as school or daycare.
For respiratory viruses, notably RSV, the majority of individuals exhibit antibody levels above the seropositivity threshold. This indicates a first infection typically occurring before 2–3 years of age and continuous exposure throughout life, maintaining consistently high levels of antibodies.
Antibody levels to influenza A increase with age due to the combined effect of both seasonal infections and vaccinations. Antibody levels are highest in older individuals, likely influenced by annual influenza vaccination campaigns specifically tailored to target older populations.
Seroprevalence across diverse age groups in a population
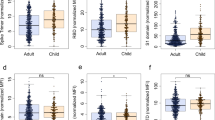
After establishing cut-offs for seropositivity using statistical models, the seroprevalence is calculated within the SeroPed study and Milieu Intérieur cohort, both representing the healthy French population. The cohorts differ in their composition; the first including newborn to elderly individuals, and the second exclusively adults. To facilitate analysis, we categorize the population into four distinct groups: young children (under 5 years old), older children and teenagers (5–18 years old), adults from the SeroPed study, and adults from Milieu Intérieur.
Seroprevalence for both mandatory and recommended vaccines in France is presented (Fig. 5). Seroprevalence for mandatory vaccines is consistently high across all age groups and antigens. Among adults, the seroprevalence varies from 88.4%−100% depending on antigens, indicating high vaccination coverage. Importantly, there is not definitive evidence of seroreversion for any pathogen, implying that the administered vaccines effectively induce an immune response and maintain stable antibody levels throughout an individual’s life.

Data are from n = 1132 biologically independent samples from the SeroPed study and n = 1000 biologically independent samples from the Milieu Intérieur cohort. The SeroPed study is divided into infants and toddlers (in red), children and adolescents (in blue), adults (in green), The Milieu Intérieur cohort contains only adults (in purple). 95% confidence intervals are calculated using Wilson’s method.
For pathogens in this study that target the respiratory or intestinal systems, seroprevalence remains high in all adults, with similar trends observed between vaccine-preventable diseases and high-prevalence viruses. Children under 5 years old exhibit varying seroprevalence, ranging from 30.9% for CMV to 98.7% for Rotavirus, indicating diverse virus exposure levels during early childhood. In contrast, adolescents and adults display seroprevalence ranging from 41.2% to 55.2% for CMV, reaching 100% for HKU1, reflecting ongoing exposure and long-term immunity.
The panel includes a dedicated section on hepatitis viruses; however, the seroprevalence for these antigens remain relatively low compared to other viral infections. The observed seroprevalence among adults in the MI cohort was 9.9% for Hepatitis A and 33.9% for Hepatitis E. In adults in the SeroPed study, the observed seroprevalence was 13.5% for Hepatitis A and 52.4% for Hepatitis E. We do not calculate the seroprevalence of Hepatitis B and Hepatitis C because we did not expect to observe enough positive antibody responses in our samples to allow accurate calculation of a cut-off. Supplementary Fig. 6 presents age-stratified results for all Hepatitis antigens comprised in our panel.
Discussion
In this study, we demonstrate how a laboratory-based multiplex serological assay can discern variations in antibody titers across age groups within healthy populations, allowing to establish sero-positivity cut-offs, and ascertain seroprevalence. Additionally, it enables us to better understand the effects of vaccines and booster doses, providing insights into the transfer of passive immunity to infants through maternal antibodies, and assessing the waning of antibodies over time.
The seroprevalence profiles of vaccine-preventable diseases (Fig. 5), align closely with the high vaccination coverage rates for mandatory vaccines in France, reaching ~95%. This is consistent with estimates from the World Health Organization and UNICEF regarding national immunization coverage, indicating a 96% coverage for the complete DTaP vaccine schedule and around 90% coverage for MMR vaccines in France. The agreement between seroprevalence and vaccination coverage underscores the effectiveness of the immunization programs30.
The observed high antibody levels in newborns indicate the presence of maternal antibodies transferred from the mother, which play a vital role in providing temporary immunity to the newborn31. The lifespan of maternal antibodies in the infant’s system varies, typically lasting ~6–9 months32,33. This passive immunity wanes over time, and infants gradually develop their own immune responses. Antibody titers then increase with age, after repeated infections, especially evident with RSV and Adenovirus, suggesting early initial exposure and re-infection occurring throughout life34. The timing disparity between certain infections may be associated with their distinct transmission dynamics or seasonal patterns35. RSV, transmitted via respiratory droplets, tends to infect infants during its seasonal peaks36, whereas varicella, transmitted mainly through direct contact (and respiratory droplets), usually manifests later in childhood as social interactions increase with age37. As observed with our assay, an increase in varicella antibody levels occurs around the age of 4 (Fig. 4), confirming reports of first exposure typically taking place in environments such as school or daycare37. On the other hand, high CMV seroprevalence during adulthood raises questions about the factors that could prevent some individuals from becoming seropositive upon later-life exposure, despite the virus’s high prevalence within the population. Nevertheless, our seroprevalence estimates align with previously reported estimates from the UK, indicating a CMV seroprevalence of ~50% among European adults5. CMV, and other herpesviruses, often persist in latent form, however our serological assay does not allow differentiation between the stage of infection38.
Across all age groups, there is consistently high seroprevalence for endemic viruses, suggesting widespread exposure from a young age and frequent reinfection throughout life, contributing to a balance between increased immunity from new infections (seroconversion) and declining antibody levels (seroreversion). Immunosenescence, the age-related decline in the functionality of both innate and adaptive immune responses, results in a reduction of antibodies levels in older individuals, as observed with certain diseases such as diphtheria (Fig. 3) where antibody production diminishes with age.
Our findings for Hepatitis A and E are consistent with those of other research teams, showing low seroprevalence for these viruses among adults, reaching, 9.9%, and 33.9%, respectively39,40,41,42,43,44. These results align with existing studies, such as the assessment of Hepatitis A seroprevalence in French children and adolescents, where the overall seroprevalence was 5%43. When analyzing our data for individuals under 18 years old in the Seroped cohort, we observe a slightly elevated seroprevalence of 6.6% for Hepatitis A. Futhermore, our assay revealed a seroprevalence of 13.5% among adults aged 18 years and over in the SeroPed study, mirroring the results of a separate French study that reported a seroprevalence of 16.5% for adults39. In a meta-analysis of Hepatitis E seroprevalence in Europe, France appears to have a higher seroprevelance compared to its neighbors, with a seroprevalence of 32% in the general population44. This difference could be attributed to the foodborne transmission of the virus, especially through undercooked or raw meat. However, estimates of Hepatitis E seroprevalence vary substantially in the literature.
We explored various approaches to validate our test. Ideally, well-characterized samples, including both negative and positive, would be used for validation; however this was not possible given the large number of pathogens studied. An alternative validation strategy is to study large cross-sectional cohorts enriched with epidemiological data. The SeroPed study, where the serological data was age- and sex-stratified, enabled us to observe the variation in antibody levels across different age groups within the population. Subsequently, we validated our assay by assessing the consistency between pre- and post-vaccination antibody titers according to the established French vaccine schedule. Furthermore, we performed comparative analyses against reference or gold-standard tests. In this context, we employed the Milieu Intérieur cohort’s serological data (IgG levels and serological status interpretation) allowing a correlation analysis for 10 of the 47 antigens present in our panel.
The developed assay has a number of limitations. Primarily, the absence of well-characterized samples or positive pool for each pathogen studied, has complicated certain steps, such as selecting the optimum antigen concentration to use during bead coupling. To overcome this obstacle, different concentrations of antigen-coupled beads were tested against a wide sample set, revealing the dynamic range of the assay. The use of a universal reference pool, prepared with serum from individuals exhibiting a high MFI response against a broad number of antigens, is a pragmatic and effective solution when a positive pool against all pathogens comprised in the panel is not available. This reference pool not only effectively addressed inter-plate variations for quality control but also allowed standardization of the results by converting MFI into RAU. Subsequently, the difficulty in obtaining verified negative control samples for globally endemic viruses that commonly infect young children was encountered. We addressed this challenge by fitting gaussian mixture models to measured antibody responses. A key limitation of these models is the risk of there being no identifiable seronegative and seropositive subpopulations45. For pathogens with a high force of infection, we minimize this risk by fitting models to data from samples from young children where a substantial proportion of the population is likely to be seronegative. These limitations, although present during the initial development process, highlight areas for improvement to consider for the future.
There was very good agreement in measured seroprevelance between the two studied populations, however there were some significant differences (Suppl. Table 2) which may be attributable to differences in overall health status. Participants in the Milieu Intérieur Cohort were all of good health according to a questionnaire administered at enrolment26. In contrast, samples in the SeroPed study were collected from participants presenting at hospitals for routine diagnostic procedures25, thus this population may be less healthy. SeroPed samples were collected from participants without suspected SARS-CoV-2 inpection in early 2020 during the start of the COVID-19 pandemic. The confinement protocols in France at that time may have altered the transmission and seroprevalence of other infectious diseases.
The quality of the antigens had an important influence on overall assay performance. Low protein quality or stability can induce the degradation of the antigen coupled onto the bead or lead to inadequate refolding of the antigen. Additionally, distinct complications were observed depending on the nature of the antigens utilized, whether they were recombinant proteins, virus-like particles (VLPs), or lysates. When employing lysates, aggregation of beads occasionally occurred, leading to a reduction in the bead count during plate reading. VLPs, characterized by their larger-sized particles mimicking the virus structure, appeared to be more immunogenic, as indicated by the high MFI response. However, this heightened MFI could potentially be attributed to increased cross-reactivity with other viruses. Evaluating potential cross-reactivity between different antigens posed a challenge, as we would need large volume of specific anti-serum, which was not feasible during this study. Further tests should be performed in order to understand and overcome possible cross-reactivity.
In the near future, we aim to overcome the previously reported limitations and expand the potential applications of our assay. It is possible to extend this assay to measure antibody to other pathogens, from arboviruses to neglected tropical diseases46,47. It is planned to adapt this protocol to measure additional isotypes, as well as to conduct our assay using nasopharyngeal or saliva samples, as it has been demonstrated that specific mucosal IgA antibodies have a crucial role in early virus neutralization and long-term protection48. Application of statistical algorithms for combining the signal from antibody responses to multiple antigens from the same pathogen may allow for more accurate estimation of seroprevalence4,49. Further development of these protocols would provide us with a larger dataset enabling us to gain insights into the kinetics of antibodies and the role of different immunoglobulin isotypes post-immunization.
Conclusion
This study addresses the challenges of serosurveillance of vaccine-preventable diseases and common viral infections through the development of a high-throughput multiplex serology assay, providing insights into natural and vaccine-acquired immunity. This tool allows us to estimate the time of the first infection and vaccine doses and evaluate the decline of antibodies over time. The key advance of this study is in the development of protocols to allow multiplexing of different serological tests in the same assay, and integrated analytic methods for determination of sero-positivity cut-offs to multiple pathogens. This contributes to the development of serosurveillance tools that are essential to monitor population immune status and design effective vaccination strategies to prevent outbreaks and improve global health.
Data availability
All data in the present study are provided as Supplementary Data files. Source data for Fig. 2 can be accessed from Supplementary Data 2, and Figs. 3 and 4 can be accessed from Supplementary Data 3. All data from the SeroPed study is available in this publication. Additional data from the Milieu Intérieur study can be obtained through a Data Access Form submitted at https://www.milieuinterieur.fr/en/data-and-samples/.
References
Crompton, P. et al. A prospective analysis of the Ab response to Plasmodium falciparum before and after a malaria season by protein microarray. Proc. Natl. Acad. Sci. USA. 107, 6958–6963 (2010).
Shrock, E. L., Shrock, C. L. & Elledge, S. J. VirScan: High-throughput profiling of antiviral antibody epitopes. Bio-Protoc. 12, e4464 (2022).
Van Gageldonk, P. G. M., Van Schaijk, F. G., Van Der Klis, F. R. & Berbers, G. A. M. Development and validation of a multiplex immunoassay for the simultaneous determination of serum antibodies to Bordetella pertussis, diphtheria and tetanus. J. Immunol. Methods 335, 79–89 (2008).
Rosado, J. et al. Multiplex assays for the identification of serological signatures of SARS-CoV-2 infection: an antibody-based diagnostic and machine learning study. Lancet Microbe 2, e60–e69 (2021).
Mentzer, A. J. et al. Identification of host-pathogen-disease relationships using a scalable multiplex serology platform in UK Biobank. Nat. Commun. 13, 1818 (2022).
Partouche, H., Gilberg, S., Renard, V. & Saint-Lary, O. Mandatory vaccination of infants in France: is that the way forward?. Eur. J. Gen. Pract. 25, 49–54 (2019).
Sheikh, S. et al. A report on the status of vaccination in Europe. Vaccine 36, 4979–4992 (2018).
Service Publique France. Schedule of Vaccinations. https://www.service-public.fr/particuliers/vosdroits/F724?lang=en (2025).
World Health Organization. Immunization Dashboard France. https://immunizationdata.who.int/dashboard/regions/european-region/FRA (2025).
Vaux, S., Gautier, A., Nassany, O. & Bonmarin, I. Vaccination acceptability in the French general population and related determinants, 2000-2021. Vaccine 41, 6281–6290 (2023).
den Hartog, G., van Binnendijk, R., Buisman, A.-M., Berbers, G. A. M. & van der Klis, F. R. M. Immune surveillance for vaccine-preventable diseases. Expert Rev. Vaccines 19, 327–339 (2020).
Alter, S. J., Bennett, J. S., Koranyi, K., Kreppel, A. & Simon, R. Common childhood viral infections. Curr. Probl. Pediatr. Adolesc. Health Care 45, 21–53 (2015).
Teoh, Z. et al. Burden of respiratory viruses in children less than 2 years old in a community-based longitudinal us birth cohort. Clin. Infect. Dis. 77, 901–909 (2023).
Jackson, D. J. The role of rhinovirus infections in the development of early childhood asthma. Curr. Opin. Allergy Clin. Immunol. 10, 133–138 (2010).
Guarino, C. et al. Development of a quantitative COVID-19 multiplex assay and its use for serological surveillance in a low SARS-CoV-2 incidence community. PLoS ONE 17, e0262868 (2022).
Al-Tawfiq, J. A. et al. Surveillance for emerging respiratory viruses. Lancet Infect. Dis. 14, 992–1000 (2014).
Hao, R. et al. Surveillance of emerging infectious diseases for biosecurity. Sci. China Life Sci. 65, 1504–1516 (2022).
Iwane, M. K. et al. Population-based surveillance for hospitalizations associated with respiratory syncytial virus, influenza virus, and parainfluenza viruses among young children. Pediatrics 113, 1758–1764 (2004).
Galanti, M. et al. Rates of asymptomatic respiratory virus infection across age groups. Epidemiol. Infect. 147, e176 (2019).
Gardner, G., Frank, A. L. & Taber, L. H. Effects of social and family factors on viral respiratory infection and illness in the first year of life. J. Epidemiol. Community Health 38, 42–48 (1984).
Ferson, M. J. Infections in day care. Curr. Opin. Pediatr. 5, 35–40 (1993).
Churchill, R. B. & Pickering, L. K. Infection control challenges in child-care centers. Infect. Dis. Clin. North Am. 11, 347–365 (1997).
Olin, A. et al. A systematic investigation into the non-genetic and genetic factors affecting the human anti-viral antibody repertoire. medRxiv. https://doi.org/10.1101/2023.11.07.23298153 (2023).
Slifka, M. K., Antia, R., Whitmire, J. K. & Ahmed, R. Humoral immunity due to long-lived plasma cells. Immunity 8, 363–372 (1998).
Woudenberg, T. et al. Humoral immunity to SARS-CoV-2 and seasonal coronaviruses in children and adults in north-eastern France. EBioMedicine. 70, 103495 (2021).
Thomas, S. et al. The Milieu Intérieur study — an integrative approach for study of human immunological variance. Clin. Immunol. 157, 277–293 (2015).
Woudenberg, T. et al. Estimated protection against COVID-19 based on predicted neutralisation titres from multiple antibody measurements in a longitudinal cohort, France, April 2020 to November 2021. Euro Surveill. 28, 2200681 (2023).
Scepanovic, P. et al. Human genetic variants and age are the strongest predictors of humoral immune responses to common pathogens and vaccines. Genome Med. 10, 59 (2018).
De Thoisy, A. et al. Seroepidemiology of the seasonal human coronaviruses NL63, 229E, OC43 and HKU1 in France. Open Forum Infect. Dis. 10, ofad340 (2023).
Bechini, A. et al. Childhood vaccination coverage in Europe: impact of different public health policies. Expert Rev. Vaccines 18, 693–701 (2019).
Dolatshahi, S. et al. Selective transfer of maternal antibodies in preterm and fullterm children. Sci. Rep. 12, 14937 (2022).
Madani, G. & Heiner, D. C. Antibody transmission from mother to fetus. Curr. Opin. Immunol. 1, 1157–1164 (1989).
Grindstaff, J. L., Brodie, E. D. & Ketterson, E. D. Immune function across generations: integrating mechanism and evolutionary process in maternal antibody transmission. Proc. R. Soc. B Biol. Sci. 270, 2309–2319 (2003).
Lu, G. et al. Large-scale seroprevalence analysis of human metapneumovirus and human respiratory syncytial virus infections in Beijing, China. Virol. J. 8, 62 (2011).
Moriyama, M., Hugentobler, W. J. & Iwasaki, A. Seasonality of respiratory viral infections. Annu. Rev. Virol. 7, 83–101 (2020).
Azzari, C. et al. Epidemiology and prevention of respiratory syncytial virus infections in children in Italy. Ital. J. Pediatr. 47, 198 (2021).
Viner, K. et al. Transmission of varicella zoster virus from individuals with herpes zoster or varicella in school and day care settings. J. Infect. Dis. 205, 1336–1341 (2012).
Sepúlveda, N. et al. Revisiting IgG Antibody reactivity to epstein-barr virus in myalgic encephalomyelitis/chronic fatigue syndrome and its potential application to disease diagnosis. Front Med. 9, 921101 (2022).
Lagarde, E., Joussemet, M., Lataillade, J. J. & Fabre, G. Risk factors for hepatitis A infection in France: drinking tap water may be of importance. Eur. J. Epidemiol. 11, 145–148 (1995).
Mansuy, J.-M. et al. Hepatitis E virus antibodies in blood donors, France. Emerg. Infect. Dis. 17, 2309–2312 (2011).
Kwon, S. Y. & Lee, C. H. Epidemiology and prevention of hepatitis B virus infection. Korean J. Hepatol. 17, 87–95 (2011).
Hudu, S. A. et al. Isolated hepatitis B core antibody positive among vaccinated cohort in Malaysia. Ann. Saudi Med. 33, 591–594 (2013).
Faillon, S. et al. Impact of travel on the seroprevalence of hepatitis A in children. J. Clin. Virol. 56, 46–51 (2013).
Hartl, J. et al. Hepatitis E seroprevalence in Europe: a meta-analysis. Viruses 8, 211 (2016).
Fonseca, A., Spytek, M., Biecek, P., Cordeiro, C., Sepúlveda, N. Antibody selection strategies and their impact in predicting clinical malaria based on multi-sera data. BioData Min. 17, 2 (2024)
Chan, Y. et al. Assessing seroprevalence and associated risk factors for multiple infectious diseases in Sabah, Malaysia using serological multiplex bead assays. Front Public Health. 10, 924316 (2022).
Chan, Y. et al. Multiplex serology for measurement of igg antibodies against eleven infectious diseases in a national serosurvey: haiti 2014-2015. Front Public Health. 10, 897013 (2022).
Sterlin, D. et al. IgA dominates the early neutralizing antibody response to SARS-CoV-2. Sci. Transl. Med. 13, eabd2223 (2021).
Longley, R. et al. Development and validation of serological markers for detecting recent plasmodium vivax infection. Nat. Med. 26, 741–749 (2020).
Acknowledgements
This work was supported by the the French government’s Integrative Biology of Emerging Infectious Diseases (Investissement d’Avenir grant ANR-10-LABX-62-IBEID) and INCEPTION programs (Investissement d’Avenir grant ANR-16-CONV-0005); the URGENCE COVID-19 fundraising campaign of Institut Pasteur, the European Research Council (MultiSeroSurv ERC Starting Grant 852373). Milieu Intérieur was funded by the French government’s Invest in the Future programme; reference ANR-10-LABX-69-01.
Author information
Authors and Affiliations
Consortia
Contributions
E.B. developed the assay, analysed samples, and wrote the first draft of the manuscript. G.B. analysed the data. L.G., F.D. and S.P. supported assay development. A.F., D.D. and L.Q.M. provided access to samples. M.W. designed the study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Medicine thanks Nuno Sepúlveda, Marianna Karachaliou and Joshua LaBaer for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional information can be found at: https://www.milieuinterieur.fr/en/.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Bloch, E., Baudemont, G., Donnadieu, F. et al. Investigation of the sero-epidemiology of vaccine preventable diseases and common viral infections in French populations. Commun Med 5, 465 (2025). https://doi.org/10.1038/s43856-025-01162-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-025-01162-5
