
Abstract
Background
Eribulin plus gemcitabine improves progression-free survival in chemotherapy-naive metastatic breast cancer patients, but its efficacy in second-line or later treatment remains unclear.
Methods
This single-arm, phase II study was conducted at 13 Chinese medical centers. Eligible patients had histologically confirmed human epidermal growth factor receptor 2 negative metastatic breast cancer and had received at least one prior taxane-containing chemotherapy regimen and anthracycline-containing regimens in the adjuvant setting. Patients received intravenous infusions of eribulin (1.4 mg/m2) and gemcitabine (1.0 g/m2) on days 1 and 8 of a 21-day cycle. Progression-free survival, objective response rate and disease control rate were assessed. Adverse events were also recorded.
Results
Here we show 70 patients took part in this study (71.4% hormone receptor positive/HER2 negative). Patients had received a median of three prior lines of systemic treatment. Overall, 48.6% have significant tumor shrinkage, 92.9% have tumor control, and median time without disease progression is 7.2 months (95% confidence interval, 5.5-10.9). Median time without disease progression is 8.4 months (hormone receptor positive) vs. 6.3 months (triple-negative, p = 0.1849). Grade 3–4 side effects mostly affect blood cells and are manageable.
Conclusions
Eribulin plus gemcitabine is effective and well-tolerated in patients with HER2-negative metastatic breast cancer needing second-line or later treatment, providing a valuable treatment option.
Plain language summary
People with advanced breast cancer that is HER2-negative often run out of treatment options after their first therapy. A drug combination called eribulin and gemcitabine works well as an initial treatment, but we didn’t know if it could help later on. To find out, we ran a study in 13 hospitals in China with 70 patients. They received both drugs every three weeks, and we tracked how their cancer responded and what side effects they had. Almost half of the patients saw their tumours shrink, and most had their cancer under control for an average of about seven months. Side effects, mainly related to blood counts, were manageable. These results suggest this drug combination could give people with advanced breast cancer another effective option.
Similar content being viewed by others

Introduction
Breast cancer (BC) has become the most common malignant tumor in the world1, and its morbidity and mortality in China rank fifth and seventh among the malignant tumors, respectively2. Some patients already have metastatic breast cancer (MBC) when diagnosed, while others with early-stage BC develop tumor metastasis even after comprehensive treatment3,4. MBC treatment is still a challenge in clinical practice5. Drug therapy is the main choice for MBC treatment. In particular, for BC with negative human epidermal growth factor receptor 2 (HER2), chemotherapy is the first-choice5,6,7 In the chemotherapy of MBC, anthracyclines and paclitaxel are the basic drugs, but patients who fail to respond to these two drugs are often seen in clinical practice8.
Eribulin is a microtubule dynamic inhibitor that causes irreversible mitotic blockage and cell death through high-affinity binding to the ends of microtubules9,10. It has a different mechanism of action from taxanes; thus, it may still be effective for patients resistant to taxanes11,12. Eribulin also has non-cytotoxic effects, including increasing the content of other drugs in the tumor microenvironment through vascular remodeling; it can also reverse the epithelial–mesenchymal transition of tumor cells and inhibit tumor invasion and metastasis13,14. Previous research results have indicated that eribulin can effectively treat HER2-MBC15,16,17. Kaufman et al. conducted a phase III randomized trial comparing eribulin mesylate with capecitabine in patients with MBC who had previously received anthracycline- and taxane-based therapy, finding that eribulin was not superior to capecitabine in terms of OS or PFS18. Cortes et al. reported a phase III open-label randomized study where eribulin monotherapy significantly improved OS (median 13.1 vs. 10.6 months) compared with treatment of physician’s choice (TPC) in heavily pretreated patients with MBC, with a manageable safety profile19.
Gemcitabine is a nucleoside antimetabolite drug that can be catalyzed into active dideoxycytidine triphosphate by nucleotide kinase in cells20. The dideoxycytidine triphosphate inhibits and destroys DNA synthesis inside tumor cells and promotes tumor cell apoptosis without producing cross-resistance when combined with paclitaxel. Gemcitabine also has some therapeutic effect in the treatment of MBC21. Studies have observed the combination of eribulin and gemcitabine (EG) as a first-line treatment regimen for MBC, revealing that EG gives a similar PFS and has less neurotoxicity compared with a regimen involving a combination of paclitaxel and gemcitabine (PG)22. Further analysis of patient quality of life suggested that the EG regimen inhibited neuropathy as compared with the PG regimen. Therefore, eribulin is considered to be a reasonable substitute for paclitaxel as first-line chemotherapy for MBC23. However, it is unclear whether EG can be used as a second-line or beyond treatment for MBC. This study aims to explore the efficacy and safety of EG as a second-line or beyond treatment for HER2-negative MBC.
Herein, this study demonstrates that EG is effective and safe as second-line or later treatment for heavily pretreated HER2-negative MBC patients. Among 70 participants, 71.4% had HR+/HER2− disease and a median of three prior systemic therapies. EG achieved an objective response rate of 48.6% and disease control in 92.9% of patients. Median progression-free survival was 7.2 months overall, with similar outcomes in HR+ and triple-negative subgroups. Notably, HR+ patients previously treated with CDK4/6 inhibitors maintained a median progression-free survival of 7.2 months. Adverse events were primarily hematologic and manageable, supporting EG as a viable later-line treatment strategy.
Methods
Study design and participants
This open-label, single-arm, phase II study (NCT05263882) was conducted at 13 institutions in China. All 13 institutions were tertiary-level hospitals in China with certified oncology departments and experience in conducting phase II/III oncology trials. All study drugs were administered by licensed oncologists or oncology nurses trained in the study protocol. The trial was registered on ClinicalTrials.gov under the name “Gemcitabine Combined With Eribulin Regimen in the Treatment of Second-line Above Recurrent HER2-negative Breast Cancer” (registration number: NCT05263882) on March 2, 2022. The study protocol can be accessed in the supplemental material. This study was approved by the Ethics Committee of The Fifth Affiliated Hospital of Sun Yat-Sen University (Approval Number: K93-1) and the ethics committees of all 12 participating institutions (the Ethics Committee of The First Affiliated Hospital of Guangxi Medical university (No. 2022-081); the Ethics Committee of Zhuhai Hospital of lntegrated Traditional Chinese and Western Medicine (No. 2022-002); the Ethics Committee of Zhuhai Maternity and Child Health Hospital (No. 2022-24-02); the Ethics Committee of The First People’s Hospital of Zhaoqing (No. 2022Y042-011); the Ethics Committee of Cancer Hospital Chinese Academy of Medical Sciences (No. 2022-33-2); the Ethics Committee of Jiangmen Central Hospital (No. JMZX2023089-G); the Ethics Committee of Panyu central Hospital (No. PYZX-2022-056-09); the Ethics Committee of Dongguan Tungwah Hospital (No. DG-DH-2022073); the Ethics Committee of Dongguan People’s Hospital (No. 2023YL035-8H); the Ethics Committee of Zhongshan Hospital of Traditional Chinese Medicine Affiliated to Guangzhou University of Traditional Chinese Medicine (No. 2022-327); the Ethics Committee of Sun Yat-sen University Cancer Center (No. A2022-023-X04); the Ethics Committee of Zhongshan City People’s Hospital (No. 2022-084). All procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all patients. Patients or public representatives were not involved in the design of this phase II trial or the drafting of the manuscript. No important changes to the trial protocol were made after trial commencement. All analyses were prespecified in the original protocol. Objective response assessments were independently verified by a central radiology committee to minimize assessment bias.
Our study exclusively examined females because the disease is mostly relevant in females. Eligible patients were between 18 and 75 years old with histologically confirmed HER2-MBC and had received at least one prior taxane-containing chemotherapy regimen for the advanced disease and anthracycline-containing regimens in the adjuvant setting. The patients included had adequate bone marrow, renal, and liver function. Patients who were pregnant or had severe heart failure or severe uncontrolled infection were excluded.
Procedures
Patients received intravenous infusions of eribulin (1.4 mg/m2) and gemcitabine (1.0 g/m2) on days 1 and 8 of a 21-day cycle until disease progression, unacceptable toxic effects, or death.
Treatment interruptions and dose reductions to manage adverse events (AEs) were allowed.
Dose reductions of eribulin stepwise from 1.4 mg/m2 to 1.1 mg/m2 to 0.7 mg/m2 were permitted if necessary, as well as stepwise dose reductions of gemcitabine by 20%.
AEs were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 5.0. Efficacy outcomes, including progression-free survival (PFS), objective response rate (ORR), and disease control rate (DCR), were assessed using Response Evaluation Criteria In Solid Tumors (RECIST) version 1.1. Follow-up was conducted every two cycles.
Outcomes
The safety was assessed according to the occurrence of dose-limiting toxic effects. All adverse events (AEs) were evaluated for the entire duration of study treatment, plus a 30-day follow-up period after the last dose (consistent with ICH-GCP guidelines). The primary endpoint of the study was ORR. Secondary endpoints included PFS, DCR, and AEs.
PFS was defined as the time from the first eribulin treatment to disease progression or death due to various causes (which occurs first), in accordance with RECIST version 1.1. ORR was defined as the percentage of evaluable patients who had either a complete response (CR) or partial response (PR) as the best objective tumor response. DCR was defined as the percentage of evaluable patients at baseline who had CR, PR, or stable disease (SD) as the best objective tumor response. AEs were graded using NCI-CTCAE version 5.0.
Statistics
The primary endpoint of the study was ORR. Based on historical data24,25 HR+/HER2− locally recurrent inoperable or metastatic breast cancer showed an ORR rate of approximately 20%. The hypothesis was that eribulin plus gemcitabine would achieve at least a 40% ORR rate in patients with HER2-negative MBC. Simon’s two-stage design was used with error probabilities α and β of 0.05 and 0.2, respectively. We fixed the final figure at 50 patients, which included a 20% increase because of potential dropouts. The first stage would consist of 13 patients. If three or fewer ORRs were observed, the trial had to be terminated; otherwise, recruitment could continue. Thirteen or more ORRs in 43 evaluable patients had to be observed to meet the primary end point of the study. Patients lost to follow-up had data censored via last observation carried forward (LOCF) at the last confirmed disease assessment. Patients with missing imaging had data classified as “non-responders” per RECIST v1.1 to avoid overestimation.
Activity and safety were analyzed in patients who received at least one study treatment. Continuous data were presented as median (range), whereas categorical data were presented as frequency (percentage). Clinicopathologic characteristics were analyzed using descriptive statistics. Kaplan–Meier plots were used to calculate median PFS, and the Brookmeyer–Crowley method was used to calculate the corresponding 95% confidence intervals (CIs). Median follow-up time was computed using inverse Kaplan-Meier methods. Intergroup comparisons were analyzed using the chi-square test, the continuous-corrected chi-square test, and the log-rank test. SAS statistical software version 9.4 (SAS Institute Inc., Cary, NC) was used for statistical analysis. P < 0.05 was considered statistically significant.
Missing data were stratified by outcome type and handled per regulatory guidelines (NCI-CTCAE v5.0, RECIST v1.1) and study protocol: three patients lost to follow-up had data censored via last observation carried forward (LOCF) at the last confirmed disease assessment. Two patients with missing imaging had data classified as “non-responders” per RECIST v1.1 to avoid overestimation. No missing data were observed for severe AEs.
Results
Patient characteristics
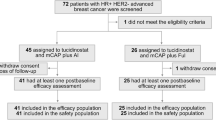
Seventy patients were enrolled from March 2022 to October 2023 and received the study treatment. All patients were female, and the median age was 50 years (range: 31–68). Fifty (71.4%) had HR+/HER2− (hormone receptor+/human epidermal growth factor receptor-2) MBC, and 20 (28.6%) had triple-negative MBC. Forty-nine patients were positive (≥15%) for the Ki-67 index. The metastatic sites of patients were the bone (68.6%), liver (52.9%), lymph nodes (48.6%), lung (44.3%), and brain (10.0%). Patients had received a median of three prior lines of systemic treatment, a median of two lines of chemotherapy, and a median of one line of endocrine treatment. Among the HR+/HER2− patients, 29 had received prior cyclin D-cyclin-dependent kinases 4 and 6 (CDK4/6) inhibitor treatment. The baseline characteristics of the participants are summarized in Table 1 and Table 2.
Efficacy
Among the patients, ORR was 48.6% (95% CI: 36.4–60.8) and DCR was 92.9% (95% CI: 84.1–97.6). Two patients (2.9%), who were both HR positive, had CR. Thirty-two (45.7%) patients had PR. Thirty-one (44.3%) patients had SD and 5 (7.1%) patients had PD (Table 3, Fig. 1).

(CR complete response, PR partial response, SD stable disease, PD progression disease.) Data were derived from 70 HER2-negative metastatic breast cancer (MBC) patients enrolled in this multicenter study across 13 hospitals in China. The EG regimen was administered as follows: eribulin 1.4 mg/m² on days 1 and 8, gemcitabine 1000 mg/m² on days 1 and 8, repeated every 3 weeks. The horizontal axis represents treatment duration (months), and each vertical line corresponds to an individual patient. Tumor response was evaluated every 2 cycles according to RECIST 1.1 criteria, with statuses categorized as CR (complete response), PR (partial response), SD (stable disease), PD (progressive disease), or DEATH (death during treatment). Patients were stratified by three factors: molecular subtype (HR+, hormone receptor-positive; HER2 Low, defined as immunohistochemistry [IHC] 1+ or IHC 2+/fluorescence in situ hybridization [FISH]-negative) and prior CDK4/6 inhibitor exposure (Y = exposed, N = naive).
The 6-month PFS rate was 65.1% (95% CI: 51.5–78.7), and the median PFS of all patients was 7.2 months (95% CI: 5.5–10.9; Fig. 2). For the HR-positive subgroup, the median PFS was 8.4 months (95% CI: 5.5 to not reached), whereas for the triple-negative subgroup, it was 6.3 months (95% CI: 3.6–8.6; p = 0.1849; Table 4, Fig. 3).

Kaplan–Meier curve illustrating PFS of all 70 HER2-negative MBC patients. PFS was defined as the time from the first EG regimen administration to disease progression, recurrence, or death from any cause. The total population had a median PFS of 7.2 months (95% confidence interval [CI]: 5.5–10.9 months). The vertical axis denotes the probability of progression-free survival, and the horizontal axis denotes time (months). Numbers below the horizontal axis indicate the number of patients at risk at each time point. Survival analysis was performed using the Kaplan–Meier method.

Kaplan–Meier curves comparing PFS between the HR+/HER2− subgroup (n = 50) and the TNBC-subgroup (n = 20) among HER2-negative MBC patients. PFS was defined as the time from the first EG regimen administration to disease progression, recurrence, or death from any cause. Nineteen progression events were recorded in the HR+/HER2− subgroup (median PFS: 8.4 months, 95% CI: 5.5–not available [NA]); 11 progression events were recorded in the TNBC-subgroup (median PFS: 6.3 months, 95% CI: 3.6–8.6 months). The Log-Rank test showed no statistically significant difference between the two subgroups (p = 0.1849). The vertical axis denotes the probability of progression-free survival, and the horizontal axis denotes time (months). Numbers below the horizontal axis indicate the number of patients at risk in each subgroup at each time point.
Among the HR+/HER2− patients who had received prior CDK4/6 inhibitor treatment, the median PFS was 7.2 months (95% CI: 5.0–15.8). For the subgroup of HR+/HER2− patients who had not received CDK4/6 inhibitor treatment, the median PFS was not reached (Table 5, Fig. 4). For the HER2-low subgroup, the median PFS was 6.5 months (95% CI: 5.4–15.8). For the HR+/HER2-low subgroup, the median PFS was 8.4 months (95% CI: 5.4–15.8; Table 5, Figs. 5 and 6).

Kaplan-Meier curves comparing PFS between patients with prior CDK4/6 inhibitor exposure (CDK4/6i group, n = 29) and those without (CDK4/6i naive group, n = 21) among HR+/HER2− MBC patients. PFS was defined as the time from the first EG regimen administration to disease progression, recurrence, or death from any cause. Fifteen progression events were recorded in the CDK4/6i group (median PFS: 7.2 months, 95% CI: 5.0–15.8 months); 4 progression events were recorded in the CDK4/6i naive group (median PFS: NA, 95% CI: 5.3–NA). The Log-Rank test showed no statistically significant difference between the two groups (p = 0.2179). The vertical axis denotes the probability of progression-free survival, and the horizontal axis denotes time (months). Numbers below the horizontal axis indicate the number of patients at risk in each group at each time point.

Kaplan–Meier curve illustrating PFS of the HER2 Low subgroup (n = 45; defined as IHC 1+ or IHC 2+/FISH-negative) among HER2-negative MBC patients. PFS was defined as the time from the first EG regimen administration to disease progression, recurrence, or death from any cause. Eighteen progression events were recorded, with a median PFS of 6.5 months (95% CI: 5.4–15.8 months). The vertical axis denotes the probability of progression-free survival, and the horizontal axis denotes time (months). Numbers below the horizontal axis indicate the number of patients at risk at each time point. Survival analysis was performed using the Kaplan–Meier method.

Kaplan–Meier curve illustrating PFS of the combined subgroup with HER2 Low expression (IHC 1+ or IHC 2+/FISH-negative) and HR positivity (HER2 Low & HR+, n = 36) among HER2-negative MBC patients. PFS was defined as the time from the first EG regimen administration to disease progression, recurrence, or death from any cause. Fifteen progression events were recorded, with a median PFS of 8.4 months (95% CI: 5.4–15.8 months). The vertical axis denotes the probability of progression-free survival, and the horizontal axis denotes time (months). Numbers below the horizontal axis indicate the number of patients at risk at each time point. Survival analysis was performed using the Kaplan–Meier method.
Safety
The most common AEs among all patients were hematological, including leukopenia (77.1%), neutropenia (71.4%), anemia (61.4%), and thrombocytopenia (54.3%). The most common perceptible AEs among all patients were decreased appetite (61.4%), nausea (60.0%), fatigue (52.9%), and peripheral neuropathy (40.0%). The most common grade 3 and 4 AEs were hematological, including neutropenia (38.6%), leukopenia (31.4%), anemia (24.3%), and thrombocytopenia (15.7%). Relatively few perceptible AEs were perceived to be grade≥3; these AEs were observed in three patients with severe fatigue and two patients with severe insomnia. No treatment-related deaths occurred. Treatment-related AEs (TRAEs) are summarized in Table 6. All patients received standard concomitant care per institutional guidelines: all patients received prophylactic antiemetics. Patients with grade 3–4 neutropenia received granulocyte colony-stimulating factor treatment. Patients with grade 3–4 thrombocytopenia received recombinant human thrombopoietin administration. No serious adverse events were attributed to concomitant medications.
Discussion
In this open-label, single-arm, phase II study, we demonstrated that EG was effective as a second-line or beyond treatment in heavily pretreated patients with HER2-MBC while maintaining a predictable and manageable safety profile. We found that for the MBC patients who had received a median of three prior lines of systemic treatment, EG still led to satisfactory ORR, DCR, and median PFS; more than half the patients achieved 6-month PFS; and no statistical difference was observed in this benefit between HR+/HER2− patients and triple-negative patients. In addition, CDK4/6 inhibitor treatment had no significant impact on the benefit of EG treatment.
In this study, all patients had received more than one line of systemic drug therapy, including taxane-containing chemotherapy regimens and anthracycline-containing regimens. For MBC patients with a long history of progression after standard treatment, it is difficult to obtain further effective treatment, although various attempts have been made to develop treatments in many previous studies. In an earlier study, capecitabine with bevacizumab failed to improve PFS, the primary end point, in a phase III trial involving heavily pretreated patients after failure of anthracyclines or taxanes26. In a phase II study, after the chemotherapy combination of gemcitabine and vinorelbine in taxane-pretreated MBC patients, the median PFS was 4.0 months, and the median OS was 11.7 months24. In a global, randomized, phase III study, sacituzumab govitecan (SG) was compared with the physician’s choice of chemotherapy (eribulin, vinorelbine, capecitabine, or gemcitabine) in endocrine-resistant, chemotherapy-treated HR+/HER2− locally recurrent inoperable or metastatic breast cancer. The results were a median PFS of 5.5 months (95% CI: 4.2–7.0) with SG and a median PFS of 4.0 months (95% CI: 3.1–4.4) with chemotherapy, the PFS rate at 6 and 12 months was 46% with SG (95% CI: 39–53) vs. 30% with chemotherapy (95% CI: 24–37) and 21% with SG (95% CI: 15–28) vs. 7% with chemotherapy (95% CI: 3–14), respectively25. In another phase II study, Zhu et al. investigated the efficacy and safety of the oral vinorelbine–apatinib combination in patients with pretreated MBC. They found that the median PFS was 5.2 months (95% CI: 3.4–7.0), the median OS was 17.4 months (95% CI: 8.0–27.0), ORR was 17.1% (6/35), and CBR was 45.7% (16/35)27. The relatively short PFS in these studies may be related to the severe condition of the patients included and the limited therapeutic effect of drugs on MBC. These results showed limited efficacy in different strategies for the survival of MBC.
Other studies have reported similar results to ours regarding PFS. A phase II study evaluated the efficacy and tolerability of combined treatment with irinotecan and capecitabine in anthracycline- and taxane-pretreated patients with MBC and found the median PFS was 7.6 months (95% CI: 5.0–10.2) and the median OS was 20.0 months (95% CI: 11.6–28.4)28. Herrscher et al. observed the efficacy of a fulvestrant–palbociclib combination in 77 heavily pretreated patients with HR + /HER2- MBC. They found that within a median follow-up of 14 months, the median PFS was 7.6 months. The median PFS significantly (P < 0.0001) decreased as the number of previous treatment lines in the metastatic setting increased29. In a multicenter, open-label, superiority, phase III, randomized controlled trial (RCT), Zhang et al. found that the median PFS in the utidelone plus capecitabine group was 8.44 months (95% CI: 7.95–9.92), compared with 4.27 months (95% CI: 3.22–5.68) in the capecitabine-alone group (hazard ratio: 0.46; 95% CI: 0.36–0.59; P < 0.0001)28. Modi et al. conducted a phase 3 trial involving patients with HER2-low metastatic breast cancer who had received one or two previous lines of chemotherapy. In the hormone receptor–positive cohort, the median PFS was 10.1 months in the trastuzumab deruxtecan group and 5.4 months in the physician’s choice group (hazard ratio: 0.51; P < 0.001)30. In a phase 1b/2 study, women with advanced/MBC and ≤3 prior chemotherapies received eribulin plus capecitabine. ORR was 43% and median PFS 7.2 months31. In our study, the overall PFS after EG treatment was 7.2 months in the intention-to-treat population, with a median PFS of 8.4 months for HR+/HER2− patients and a median PFS of 6.3 months for TNBC patients. The PFS in the present study was slightly lower than that in the above study28,29,32. Firstly, our study only included HER2-MBC patients, while the previous study included various MBC patients. Secondly, the median number of lines of treatment for patients in this study was 3, while it was 2 (range: 1–5) in the previous study.
Eribulin has been demonstrated to be effective in the treatment of advanced BC in multiple previous RCTs33. In a phase III, open-label, randomized study, Cortes et al. compared the overall survival of heavily pretreated MBC patients receiving eribulin with that of currently available treatments. They found that OS was significantly improved in patients assigned to eribulin (median: 13.1 months, 95% CI: 11.8–14.3) compared with treatment of physician’s choice (TPC; median: 10.6 months; 95% CI: 9.3–12.5; hazard ratio: 0.81; 95% CI: 0.66–0.99; P = 0.041), but the median PFS was only 3.7 months (95% CI: 3.3–3.9) with eribulin and 2.2 months (95% CI: 2.1–3.4) with TPC (hazard ratio: 0.87; 95% CI: 0.71–1.05; P = 0.137) in the intention-to-treat population in an independent review19. In a phase III RCT, eribulin was compared with capecitabine for patients with locally advanced or metastatic BC. The results revealed that the median PFS for eribulin and capecitabine was 4.1 and 4.2 months, respectively (hazard ratio: 1.08; 95% CI: 0.93–1.25; P = 0.30)18. Gemcitabine, a common anticancer drug, had also demonstrated its efficacy in treating patients with MBC, but the improvement of PFS was relatively limited, ranging from 3.5 to 5.1 months for second and third line cytotoxic treatment in pretreated MBC patients34,35.
Regarding EG combined treatment, a previous randomized, phase II, open-label, two-arm, multicenter study compared EG with paclitaxel plus gemcitabine (PG) chemotherapy as a first-line treatment for patients with HER2-MBC. In that study, the 6-month PFS rate was 72% for EG and 73% for PG (P = 0.457). No significant difference was observed in OS between the two groups. Clinical benefit rates were 44% for EG and 49% for PG. Major toxicities were neutropenia and neurotoxicity. Neurotoxicity of grade 2 or above was more common with PG than with EG (45.8% vs. 13.6%; P < 0.0001). These results demonstrate the efficacy and safety of EG as a first-line treatment for patients with MBC20. In another phase II study, Pellegrino et al. assessed the activity and safety of EG in patients with locally advanced or metastatic TNBC. Within a median follow-up of 28.8 months, the median PFS was 5.1 months, and the median OS was 14.5 months36. Our present study further demonstrated that EG also has promising efficacy as a second-line or beyond treatment for HER2− patients with MBC while maintaining a manageable safety profile and a low perceived toxicity response.
Previous studies have confirmed that CDK4/6 inhibitors can increase PFS and OS of patients with metastatic HR+/HER2 BC and improve ORR and quality of life37,38. However, the selection of patient regimens remains difficult after the failure of CDK4/6 inhibitor treatment. Some studies have also shown that the benefit of PFS was less than 6 months39,40. In our study, we found that even among HR+ patients who had received prior CDK4/6 inhibitor treatment, the median PFS was 7.2 months. This result suggests that eribulin in combination with gemcitabine might be an effective rescue choice for patients with previously unsuccessful CDK4/6 inhibitor treatment. Notably, in HR + /HER2− patients naïve to CDK4/6i (n = 29), the median PFS was not reached (95% CI: 5.3–NR; Table 5, Fig. 4). This finding underscores the regimen’s potential for deeper efficacy in populations with limited prior targeted therapy—a scenario common in regions where CDK4/6i access remains constrained. By demonstrating activity across both CDK4/6i-naïve and -refractory HR+ disease, our data position eribulin–gemcitabine as a flexible therapeutic option, regardless of prior CDK4/6i exposure.
In the present study, we also found some treatment-related AEs (TRAEs). The most common TRAEs were leukopenia (77.1%), neutropenia (71.4%), and anemia (61.4%), most of which were grades 1 and 2. The most common grade 3 and 4 AEs were hematological, including neutropenia (38.6%), leukopenia (31.4%), anemia (24.3%), and thrombocytopenia (15.7%). Relatively few AEs were perceived to be grade ≥ 3. These results were consistent with some previous studies36,41. In a phase II, single-arm, open-label, multicenter study, Cortes et al. found that in patients with locally advanced and metastatic disease pretreated with anthracycline, taxane, and capecitabine, the most dominant eribulin-induced grade 3 and 4 TRAEs were neutropenia (54%), with grade 3 asthenia/fatigue recorded in 10% of patients and grade 3 (no grade 4) neuropathy occurring in 6.9% of patients41. In the study by Pellegrino et al., the most common grade 3 and 4 TRAE was also neutropenia (23.8%)36. In our study, we found no neuropathy in the examined population, although an elevation of liver enzymes occurred in 41.4% of patients, which was mostly grade 1. Only one case with grade 4 elevation of glutamic-pyruvic transaminase was recorded. In fact, we found no life-threatening or fatal TRAEs in the present study.
In MBC, sequential monotherapy is generally preferred in clinical practice—primarily due to lower cumulative toxicity and the ability to preserve treatment options for later lines. However, patients with rapidly progressive disease (e.g., symptomatic liver/lung metastases) require rapid tumor control to alleviate symptoms and prevent organ failure. Our combination of eribulin + gemcitabine achieved an objective response rate (ORR) of 48.6%. In contrast, sequential monotherapy often leads to a slower response. As noted in real-world practice, many patients (especially those with ≥2 prior lines) develop cumulative toxicities that make sequential monotherapies unfeasible. Our combination was well-tolerated while delivering faster symptom relief. Notably, we do not advocate for combination chemotherapy as a universal alternative to sequential therapy. Instead, we propose it as a patient-tailored option: sequential monotherapy remains first-choice for fit patients with low tumor burden or preserved organ function, while combination therapy is reserved for those with high burden, symptomatic disease, or limited tolerance to later-line monotherapies.
There are some limitations in the present study. First, the sample size was relatively small, and there were some heterogeneities between patients, including age, BMI, duration of BC, sites of metastasis, and number of therapy lines. Second, this study only included HER2− patients with MBC. The efficacy and safety of eribulin in combination with gemcitabine for HER2+ patients remain unknown. Third, the duration of follow-up was relatively short, which might narrow the time window used to calculate PFS. Fourth, our upper age limit of 75 years, while justified by limited safety data in older patients at study initiation, may restrict generalizability to frail or comorbid patients over 75 years. Further RCTs are warranted to evaluate the efficacy and safety of EG for metastatic MBC in a larger sample and with a longer follow-up.
Conclusion
Our study demonstrated that EG is efficacious for HER2-MBC while maintaining a manageable safety profile as a second-line or beyond treatment.
References
Sung, H.A.-O. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries, pp 1542–4863 (Electronic).
Xia et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants, pp 2542–5641 (Electronic).
Waks A. G. & Winer E. P. Breast Cancer Treatment: A Review. pp 1538–3598 (Electronic).
Itani, N., Grogan, N., Mott, S. & Phadke, S. Metastatic presentations of previously treated early-stage breast cancer patients and association with survival. Clin. Breast Cancer 20, 209–214 (2020).
Karihtala, P.A.-O., Jääskeläinen, A., Roininen, N. & Jukkola, A. Prognostic factors in metastatic breast cancer: a prospective single-centre cohort study in a Finnish University Hospital, pp 2044–6055 (Electronic).
Barni S. & Mandalà M. Chemotherapy for metastatic breast cancer, pp 1569–8041 (Electronic).
Lin, P. H. & Laliotis, G. The present and future of clinical management in metastatic breast cancer. J. Clin. Med. 11, 5891 (2022).
Jerusalem, G., Rorive, A. & Collignon, J. Chemotherapy options for patients suffering from heavily pretreated metastatic breast cancer, pp 1744–8301 (Electronic).
Pereira, R. B. et al. Marine-derived anticancer agents: clinical benefits, innovative mechanisms, and new targets. Mar. Drugs 17, 329–349 (2019).
Oya, K. et al. Eribulin mesylate exerts antitumor effects via CD103. Oncoimmunology 12, 2218782 (2023).
Wan, M. C. et al. Biomaterials from the sea: future building blocks for biomedical applications, pp 2452–199X (Electronic).
Perez-Garcia, J. M. & Cortes, J. The safety of eribulin for the treatment of metastatic breast cancer. Expert Opin. Drug Saf. 18, 347–355 (2019).
Funahashi, Y. et al. Eribulin mesylate reduces tumor microenvironment abnormality by vascular remodeling in preclinical human breast cancer models, pp 1349–7006 (Electronic).
Sachdev, P., Ronen, R., Dutkowski, J. & Littlefield, B. A. Systematic analysis of genetic and pathway determinants of eribulin sensitivity across 100 human cancer cell lines from the cancer cell line encyclopedia (CCLE). Cancers 14, 4532–4552 (2022).
McIntyre, K. et al. Phase 2 study of eribulin mesylate as first-line therapy for locally recurrent or metastatic human epidermal growth factor receptor 2-negative breast cancer. Breast Cancer Res. Treat. 146, 321–328 (2014).
De Luca, R., Alù, M., Genova, G., Grassadonia, A. & Cicero, G. Use of Eribulin mesylate as second-line therapy in elderly patients with HER/2 negative metastatic breast cancer (MBC): efficacy, tolerability and Quality of Life. Eur. Rev. Med Pharm. Sci. 24, 12727–12734 (2020).
Smith, J. et al. Phase II study of eribulin mesylate administered biweekly in patients with human epidermal growth factor receptor-2-negative metastatic breast cancer. Clin. Breast Cancer 20, 160–167 (2020).
Kaufman, P. A. et al. Phase III open-label randomized study of eribulin mesylate versus capecitabine in patients with locally advanced or metastatic breast cancer previously treated with an anthracycline and a taxane. J. Clin. Oncol. 33, 594–601 (2015).
Cortes, J. et al. Eribulin monotherapy versus treatment of physician’s choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Lancet 377, 914–923 (2011).
Gesto, D. S., Cerqueira, N. M., Fernandes, P. A. & Ramos, M. J. Gemcitabine: a critical nucleoside for cancer therapy. Curr. Med Chem. 19, 1076–1087 (2012).
Jones, J. et al. Gemcitabine for the treatment of metastatic breast cancer. Health Technol. Assess. 13, 1–7 (2009).
Park, Y. H. et al. Phase II, multicentre, randomised trial of eribulin plus gemcitabine versus paclitaxel plus gemcitabine as first-line chemotherapy in patients with HER2-negative metastatic breast cancer. Eur. J. Cancer 86, 385–393 (2017).
Kim, J. Y. et al. Quality of life outcomes including neuropathy-associated scale from a phase II, multicenter, randomized trial of eribulin plus gemcitabine versus paclitaxel plus gemcitabine as first-line chemotherapy for HER2-negative metastatic breast cancer: Korean Cancer Study Group Trial (KCSG BR13-11). Cancer Commun. (Lond.) 39, 29 (2019).
Yamamura, J. et al. Gemcitabine and Vinorelbine Combination Chemotherapy in Taxane-Pretreated Patients with Metastatic Breast Cancer: A Phase II Study of the Kinki Multidisciplinary Breast Oncology Group (KMBOG) 1015. Chemotherapy 62, 307–313 (2017).
Rugo, H. S. et al. Sacituzumab Govitecan in Hormone Receptor-Positive/Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer. J. Clin. Oncol. 40, 3365–3376 (2022).
Miller, K. D. et al. Randomized phase III trial of capecitabine compared with bevacizumab plus capecitabine in patients with previously treated metastatic breast cancer. J. Clin. Oncol. 23, 792–799 (2005).
Zhu, A. et al. Phase II study of apatinib in combination with oral vinorelbine in heavily pretreated HER2-negative metastatic breast cancer and clinical implications of monitoring ctDNA. Cancer Biol. Med. 18, 875–887 (2021).
Lee, K. S., Park, I. H., Nam, B. H. & Ro, J. Phase II study of irinotecan plus capecitabine in anthracycline- and taxane-pretreated patients with metastatic breast cancer. Invest. N. Drugs 31, 152–159 (2013).
Herrscher, H. et al. Fulvestrant and palbociclib combination in heavily pretreated hormone receptor-positive, HER2-negative metastatic breast cancer patients. Breast Cancer Res. Treat. 179, 371–376 (2020).
Modi, S. et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N. Engl. J. Med. 387, 9–20 (2022).
Twelves, C. et al. A phase 1b/2, open-label, dose-escalation, and dose-confirmation study of eribulin mesilate in combination with capecitabine. Br. J. Cancer 120, 579–586 (2019).
Zhang, P. et al. Utidelone plus capecitabine versus capecitabine alone for heavily pretreated metastatic breast cancer refractory to anthracyclines and taxanes: a multicentre, open-label, superiority, phase 3, randomised controlled trial. Lancet Oncol. 18, 371–383 (2017).
Garrone, O. et al. Eribulin in advanced breast cancer: safety, efficacy and new perspectives. Future Oncol. 13, 2759–2769 (2017).
Heinemann, V. Gemcitabine in metastatic breast cancer. Expert Rev. Anticancer Ther. 5, 429–443 (2005).
Ferrazzi, E. & Stievano, L. Gemcitabine: monochemotherapy of breast cancer. Ann. Oncol. 17, v169–v172 (2006).
Pellegrino, B. et al. Phase II study of eribulin in combination with gemcitabine for the treatment of patients with locally advanced or metastatic triple negative breast cancer (ERIGE trial). Clinical and pharmacogenetic results on behalf of the Gruppo Oncologico Italiano di Ricerca Clinica (GOIRC). ESMO Open 6, 100019 (2021).
Finn, R. S. et al. Overall survival results from the randomized phase 2 study of palbociclib in combination with letrozole versus letrozole alone for first-line treatment of ER+/HER2- advanced breast cancer (PALOMA-1, TRIO-18). Breast Cancer Res Treat. 183, 419–428 (2020).
Slamon, D. J. et al. Ribociclib plus fulvestrant for postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in the phase III randomized MONALEESA-3 trial: updated overall survival. Ann. Oncol. 32, 1015–1024 (2021).
Bardia, A. et al. Phase I/II trial of exemestane, ribociclib, and everolimus in women with HR(+)/HER2(-) advanced breast cancer after progression on CDK4/6 inhibitors (TRINITI-1). Clin. Cancer Res. 27, 4177–4185 (2021).
Kalinsky, K. et al. Randomized phase II trial of endocrine therapy with or without ribociclib after progression on cyclin-dependent kinase 4/6 inhibition in hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer: MAINTAIN trial. J. Clin. Oncol. 41, 4004–4013 (2023).
Cortes, J. et al. Phase II study of the halichondrin B analog eribulin mesylate in patients with locally advanced or metastatic breast cancer previously treated with an anthracycline, a taxane, and capecitabine. J. Clin. Oncol. 28, 3922–3928 (2010).
Acknowledgements
This study received no external funding.
Author information
Authors and Affiliations
Contributions
Xiaolu Xu, Jincai Zhong, Hong Lin, Hong Wang, and Jinhui Ye contributed equally to this work. Xiaolu Xu: Conceptualization, Patient recruitment (leading enrollment at the affiliated institution), Clinical follow-up, Data collection and verification, Writing—Original Draft. Jincai Zhong: Patient recruitment (key enrollment at the affiliated institution), Clinical follow-up, Adverse event documentation, Data curation. Hong Lin: Patient recruitment (major enrollment at the affiliated institution), Clinical follow-up, Data collection, Adverse event monitoring. Hong Wang: Patient recruitment (core enrollment at the affiliated institution), Clinical follow-up, Sample management, Data collection. Jinhui Ye: Patient recruitment (primary enrollment at the affiliated institution), Clinical follow-up, Treatment implementation supervision, Data organization. Caiwen Du: Data collection, Data sorting, Statistical analysis support. Zhihui Wang: Resources (study site coordination), Patient screening, Clinical follow-up assistance, Data supplementary collection. Guorong Zou: Resources (institutional collaboration), Patient recruitment support, Sample storage management, Clinical follow-up. Jie Ouyang: Patient eligibility assessment, Clinical follow-up, Data collection and supplementary. Gengsheng Yu: Data curation, Data sorting, and Table construction support. Yongxia Wang: Patient recruitment assistance, Clinical follow-up, and Adverse event documentation. Luzhen Li: Patient screening, Clinical follow-up, Data collection. Fei Xu: Literature retrieval support, Patient recruitment assistance, Data verification. Shien Cui: Methodology support, Treatment protocol standardization, Clinical follow-up guidance. Mei Xiao*: Supervision, Project administration, Funding acquisition, Writing—Review & Editing, Final paper approval. Peijian Peng*: Supervision, Conceptualization, Study design, Data analysis oversight, Writing— Review & Editing, Final paper approval. *Corresponding authors.
Corresponding authors
Ethics declarations
Competing interest
The authors declare no competing interests.
Peer review
Peer review information
Communications Medicine thanks Toshinari Yamashita, Wei Jin and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xu, X., Zhong, J., Lin, H. et al. Efficacy and safety of eribulin plus gemcitabine as second-line treatment for recurrent HER2-negative breast cancer: a phase II, single-arm, open-label trial. Commun Med 6, 202 (2026). https://doi.org/10.1038/s43856-026-01483-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-026-01483-z
