
Abstract
PM2.5 pollution poses significant health risks in China, with over one million premature deaths annually. Although major air quality regulations were enacted in 2013 and substantial progress has been made, the equitable distribution of health benefits remains uncertain. This study uses epidemiological modeling and inequality decomposition to assess PM2.5-related health burden disparities in China from 2000 to 2019. Results show that premature deaths decreased by 85,500 (95% CI: 81,300–89,700) after 2013, with population growth, mortality rates, and aging contributing increases of 5.0%, 7.2%, and 8.3%, respectively, while PM2.5 reduction led to a 25.1% decrease. However, the Gini coefficient for health burden disparities rose by 19.7%, indicating an increasing concentration of health risks in certain regions and populations. Provincial and urban disparities contributed 78.9% and 88.3% of this inequality. Targeted policy interventions are urgently needed to ensure that future air quality improvements yield more equitable health outcomes across China.
Similar content being viewed by others

Introduction
In recent years, China has increasingly prioritized air quality, with PM2.5 (fine particulate matter) recognized as a major air pollutant posing serious risks to both human health and the ecological environment1,2,3. According to WHO estimates, PM2.5-related premature deaths exceed millions globally each year4, with China accounting for over one million annually. In China, PM2.5 pollution ranks as the fourth leading risk factor for mortality, following hypertension, smoking, and high-salt diets. Robust pathophysiological evidence links PM2.5 exposure to a wide range of diseases, particularly cardiopulmonary disorders, respiratory illnesses, and bronchogenic carcinomas5,6.
China’s vast territory, uneven population distribution, and significant disparities in economic development and industrialization have led to marked regional differences in PM2.5 emissions and exposure. Factors such as regional economic growth, industrial structure, transportation networks, and energy consumption patterns contribute to these variations7, resulting in pronounced disparities in PM2.5 exposure across regions8,9. For example, industrialized eastern coastal areas and less developed western regions show stark contrasts in PM2.5 concentrations and exposure10. The main sources of PM2.5 pollution in China include coal combustion, vehicular emissions, industrial processes, and biomass burning, with these sources being particularly concentrated in urban and rapidly developing regions. In response to severe air pollution, the Chinese government launched several landmark policies in 2013, most notably the Air Pollution Prevention and Control Action Plan (“Ten Measures for Air”) and subsequent regional initiatives, which have led to substantial improvements in air quality, especially in key regions such as Beijing–Tianjin–Hebei and the Yangtze River Delta. Building upon this context, our study goes beyond simple correlation analysis by integrating high-resolution epidemiological modeling, spatial inequality decomposition, and multi-scale assessment of PM2.5-related health burdens, thus providing a comprehensive evaluation of the spatial patterns, drivers, and equity of air pollution exposure and associated health impacts across China.
To address these challenges, China has implemented a series of ambitious air quality policies in the past decade11, including the Air Pollution Prevention and Control Action Plan (2013) and the Blue Sky Protection Campaign (2018). These measures have led to significant reductions in PM2.5 concentrations, especially in key regions such as Beijing–Tianjin–Hebei and the Yangtze River Delta, and have garnered widespread international attention12,13,14. However, despite overall improvements, it remains unclear whether the health benefits of PM2.5 reduction have been equitably distributed among different regions and population groups.
A unique aspect of this study is its integration of inequality analysis in PM2.5 exposure and health burden at both regional and city scales across China. By combining high-resolution epidemiological modeling and advanced inequality decomposition methods, this research provides a comprehensive assessment of current patterns in air pollution-related health disparities. This approach yields valuable insights into how demographic shifts, urbanization, and policy interventions influence the spatial and social distribution of environmental health risks15,16.
Understanding the equity of PM2.5 distribution and its relationship with mortality is crucial for informing effective policy decisions12,13. Differences in PM2.5 exposure can exacerbate socio-economic inequalities and widen social divides17,18. Therefore, evaluating the fairness of PM2.5 distribution offers important guidance for policymakers seeking to establish equitable and sustainable air quality management frameworks19,20. While previous studies have examined regional variations in PM2.5 concentrations and their health impacts, few have addressed the equity of PM2.5 distribution and its associated mortality21,22,23. This study aims to fill this gap by analyzing the fairness of PM2.5 distribution across different regions of China, identifying key influencing factors, and assessing the relationship between PM2.5 exposure and population mortality.
Results
Estimating PM2.5 exposure in China, 2000–2019
In 2019, China’s population-weighted average ambient PM2.5 exposure was 38.38 μg/m³, exceeding both the national air quality standard and the World Health Organization Interim Target 1 (WHO IT-1, 35 μg/m³). Approximately 780 million individuals were exposed to PM2.5 levels above 35 μg/m³. Despite an 18.14% decrease in the number of the population exposed to PM2.5 concentrations exceeding 35 μg/m³ since 2000, nearly the entire population remained exposed to concentrations far higher than the WHO Air Quality Guideline (WHO AQG), which recommends an annual mean of 5 μg/m³ (with an interim goal of 10 μg/m³). Population-weighted average PM2.5 exposure values refer to yearly mean concentrations. Specifically, for each year, the population-weighted average was calculated by aggregating PM2.5 exposure across all grid cells, weighted by the population of each cell. This approach ensures that the reported values accurately reflect the annual average exposure experienced by the population, rather than short-term or episodic concentrations.
Between 2000 and 2019, China’s population-weighted average ambient PM2.5 exposure exhibited a trend characterized by an initial increase followed by a significant decline. The average exposure rose from 46.89 μg/m³ in 2000 to a peak of 65.67 μg/m³ in 2013, representing a 40% increase. During this period (2000–2013), the population-weighted average was 57.45 μg/m³, with a statistically significant positive trend of 1.44 μg/m³ per year (p < 0.001). Following the implementation of major air quality policies in 2013, a marked decrease was observed, with the average exposure dropping to 47.77 μg/m³ and a significant negative trend of −4.55 μg/m³ per year (p < 0.001). By 2019, the population-weighted average exposure had declined to 38.38 μg/m³, reflecting a 42% reduction from the 2013 peak (Fig. 1g).

a–c PM2.5 exposure raster in 2000 (a), 2013 (b), and 2019 (c). d–f Raster plot of changes in exposure concentrations, 2000–2013 (d), 2013–2019 (e), 2000–2019 (f). g Population exposure concentration percentage curves. h China’s population-weighted average ambient PM2.5 exposure, 2000–2019.
In China, the percentage of the population exposed to PM2.5 concentrations of 35 μg/m³ or below has risen significantly, reaching 46% (Fig. 2c). This represents a significant rise from 24% in 2000 and a notable rebound from the nadir of 5% in 2013 (Fig. 2a, b). This rising trend highlights the efficacy of environmental regulations and initiatives in mitigating air pollution, indicating advancements in public health. Although this progress is notable, it underscores the necessity of ongoing commitment to further reduce air pollution, ensuring broader public access to cleaner air and associated health improvements.

a–c Population concentration shares in 2000 (a), 2013 (b), 2019 (c).
While China has achieved substantial progress in reducing average PM2.5 exposure and increasing the proportion of the population living below critical concentration thresholds, a considerable portion of the population is still exposed to levels exceeding both national and international guidelines. Continued and enhanced policy efforts are required to further improve air quality and protect public health across all regions.
Impact of key factors on the burden of premature mortality
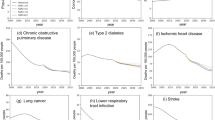
Our analysis estimated that between 2000 and 2019, approximately 28.99 million (95% CI: 26.67–31.85 million) premature deaths in China were attributable to PM2.5 exposure. Figure 3 presents the annual number of premature deaths, with further breakdown by disease category. At both the national and provincial levels, ischemic heart disease, and stroke were identified as the leading causes of PM2.5-related premature mortality. Among all PM2.5-related deaths, stroke (STR) was the predominant contributor, accounting for 51.58% (95% CI: 49.11–54.05), while ischemic heart disease (IHD) ranked second, contributing 29.34% (95% CI: 22.89–35.79) of cases. For clarity and consistency, all results are presented as the number of premature deaths attributable to PM2.5 exposure (Fig. 3).

By comparing raster data on premature deaths in different years, we found that China’s eastern coast faces greater health risks due to high PM2.5 exposure levels combined with dense population concentrations. Between 2000 and 2013, most areas experienced an increased health burden, largely attributed to rising pollution levels. The enforcement of air quality regulations has led to marked declines in PM2.5 concentrations, yielding enhanced public health outcomes and fewer health-related emergencies nationwide. Nonetheless, specific northwestern regions continue to face persistent challenges (Fig. 4d–f).

a–c PM2.5 premature death raster in 2000 (a), 2013 (b), 2019 (c). d–f PM2.5 premature deaths change.
Our study applied a decomposition method to assess how four major factors influenced PM2.5-related mortality changes in China during 2000–2013 and 2013–2019. Figure 5 presents the annual number of premature deaths attributable to PM2.5 exposure, depicted by gray bars, alongside the contribution of each factor to changes in mortality. Our results reveal that fluctuations in PM2.5 concentrations were the main driver of mortality changes, causing an 8.1% rise in 2013 and a 25.1% drop in 2019. Demographic factors and baseline mortality rates also significantly contributed to the increase in deaths, with population aging exerting the most pronounced negative impact.

The contribution of different factors to changes in premature PM2.5 deaths in China from 2000 to 2019.
From 2000 to 2019, China experienced a substantial population increase from 1.27 billion to 1.46 billion, reaching 1.39 billion inhabitants in 2013 (Fig. 5). This growth led to a 9.3% rise in attributable deaths from 2000 to 2013 and a 5.0% increase from 2013 to 2019. Changes in baseline mortality rates accounted for an additional 12.5% and 7.2% increase during the same periods. In contrast to declining PM2.5 concentrations, age structure changes have consistently driven an increase in deaths.
Anticipated population aging is projected to further intensify the health burden associated with PM2.5 exposure. Mitigating these challenges will require more stringent air quality regulations to achieve significant reductions in pollutant concentrations, thereby offsetting the impacts of an aging population. In summary, while population aging and reductions in PM2.5 concentrations are the two most prominent drivers of changes in attributable deaths, improving air quality remains the most effective strategy for reducing the health burden in the context of inevitable demographic transitions.
Our findings highlight the complex interplay between environmental and demographic factors in shaping PM2.5-related health outcomes in China. While national air quality improvements have led to substantial reductions in premature mortality, ongoing demographic shifts (particularly population aging) continue to pose significant public health challenges.
Intensifying disparities of PM2.5 exposure
China’s PM2.5 exposure levels and premature deaths have significantly improved over the past two decades. However, whether these improvements have been equitably distributed across regions and populations remains unclear. Our analysis of PM2.5 exposure inequality reveals complex variation patterns across multiple geographic scales in China from 2000 to 2019. Through the application of the Dagum decomposition algorithm, we identified distinct trends in inequality between provinces and cities, highlighting the uneven progress in addressing PM2.5 exposure across the country.
Our analyses reveal a significant increase in PM2.5 exposure disparities across China from 2000 to 2019. The spatial distribution of PM2.5 concentrations highlights persistent hotspots, with levels exceeding 70 μg/m³ in Henan, Hebei, Tianjin, and Beijing, particularly in Hebei (>75 μg/m³). In contrast, regions such as Yunnan and Tibet consistently maintained low concentrations (<30 μg/m³) throughout the study period. This pronounced spatial heterogeneity is strongly linked to population-based exposure inequalities, underscoring the uneven distribution of PM2.5-related health risks.
Our findings suggest that inequalities in PM2.5 exposure in China have increased significantly since 2000. The Gini coefficient for population-based PM2.5 exposure increased from 0.168 in 2000 to 0.189 in 2019 (10⁻³ Gini/year, P < 10⁻³), reflecting a growing disparity in exposure across the country. Notably, inequalities between provinces accounted for a substantial portion of this disparity, with a Gini coefficient of 0.15 (95% CI: 0.137–0.162, P < 0.001) and 85.7% (95% CI: 83.5%–87.9%) of national inequality attributable to differences between provinces (Fig. 6c). Population-based exposure inequality varied widely across provinces, ranging from 0.007 to 0.244, with worsening inequality observed in 22 provinces (Fig. 6b).

a Average 20-year Gini coefficient for PM2.5 exposure at the provincial scale and city-level scales (d). b Rates of change in the Gini coefficient for PM2.5 exposure at the provincial scale and city-level scales (e). c Decomposition of inequality in PM2.5 exposure at province-level scales and city-level scales (f).
At the city level, the intra-city Gini coefficient for PM2.5 exposure ranged from 0.007 to 0.158, suggesting a relatively equitable distribution within cities. While the range of intra-city Gini coefficients is from 0.007 to 0.158, it is important to note that the majority of cities have Gini values well below 0.1 Supplementary Fig. 12), with only a small fraction exceeding 0.1. This distribution indicates that, within most cities, PM2.5 exposure or health burden is relatively evenly distributed among residents, and only a few cities experience notable internal inequality. In contrast, the inter-city Gini coefficient of 0.163 (95% CI: 0.157–0.169, P < 0.001) reflects the disparity in PM2.5-related health burdens between different cities across the country. Since most cities have low internal inequality, the higher inter-city Gini value demonstrates that the overall inequality is primarily driven by differences among cities rather than within them. Inter-city differences remained significant, with an inter-city Gini coefficient of 0.163 (95% CI: 0.157–0.169, P < 0.001) contributing 96.3% of the national inequality (Fig. 6f). In the past two decades, 220 Chinese cities have experienced a rise in PM2.5 exposure inequality, underscoring the enduring and expanding nature of these disparities across geographic and administrative divisions (Fig. 6e).
Intensifying disparities of PM2.5-health-burden
Analysis of the grid-based premature mortality rate shows high-risk areas are mostly in eastern China and Xinjiang, while low-risk areas are mainly in southwestern and northern China. A comparison of data from 2000 and 2019 shows an overall increase in premature mortality rates across most regions, while the southwestern and northern regions have experienced a decline. This trend has contributed to a growing polarization in health risks across the country.
An analysis of population exposure patterns highlights concerning trends in PM2.5 exposure in China. Between 2000 and 2019, the percentage of China’s population living in areas with PM2.5 concentrations below 25 μg/m³ rose from 2.07% to 13.9%, marking a substantial 5.7-fold increase. Meanwhile, the population exposed to high PM2.5 concentrations (>60 μg/m³) has diminished from 17.9% to 5.1%, but this decline is much smaller compared to the progress in reducing low-exposure levels. This widening disparity has exacerbated inequalities in PM2.5-related mortality among the Chinese population. The proportion of the high-risk population (180+ deaths per 10⁵ people) surged from 0.4% (95% CI: 0.02–0.06) in 2000 to 18.7% (95% CI: 15.4–22.0) in 2019. Conversely, the share of the low-risk population (≤100 deaths per 10⁵ people) showed little change. The Gini coefficient for premature mortality exhibited a statistically significant increase from 0.076 (95% CI: 0.072–0.08) in 2000 to 0.091 (95% CI: 0.086–0.096) in 2019 (P < 0.001) (Fig. 7). It is noteworthy that 2013 recorded a relatively low value of 0.065. With the implementation of policies and improvements in air quality, the Gini coefficient for health risks has significantly increased. This trend reflects a growing disparity in the distribution of health risks attributable to PM2.5 exposure, suggesting an increasing polarization in the burden of such risks over time.

a, b Decomposition of inequality in premature mortality at province-level scales (a) and city-level scales (b).
The uneven distribution of PM2.5-attributable mortality across provinces and cities, as depicted in Fig. 8, highlights significant regional variations. The Gini coefficient for inter-provincial mortality disparities is 0.056 (95% CI: 0.05–0.062), accounting for 78.9% (95% CI: 75.6–82.2) of the national inequality, with a stable trend over the study period (P > 0.05). In contrast, inter-city disparities are more pronounced, with a Gini coefficient of 0.068 (95% CI: 0.059–0.077), contributing 88.3% (95% CI: 86.4–90.2) of the national disparity and showing a significant increasing trend over time (P < 0.001).

a Average 20-year Gini coefficient for premature mortality at the provincial scale. b Average Gini coefficient for 20-year premature mortality at city-level scales. c Average premature mortality raster from 2000 to 2019. d Rates of change in the Gini coefficient for premature mortality at the provincial scale and city-level scale (e). f Raster of change in premature mortality rates from 2000 to 2019.
These results highlight the enduring and increasing influence of regional disparities on the overall inequality resulting from PM2.5 exposure. Over the study period, 25 provinces (73.5% of the country) and 245 cities (65.8% of the country) experienced increasing inequality in premature deaths.
Discussion
Our study provides a comprehensive evaluation of PM2.5 exposure and associated health impacts across China from 2000 to 2019, revealing complex and evolving inequalities in PM2.5-related health burdens at multiple spatial scales. The three provinces/municipalities directly under the Central Government bearing the heaviest PM2.5-related health burdens (Henan Province, Hebei Province, and Tianjin Municipality) and Anyang City, Handan City, and Hebi City emerging as the three cities with the most severe impacts. Although national air quality policies have led to significant reductions in PM2.5 concentrations in many regions24,25, our findings reveal that improvements in exposure are not equitably distributed. Instead, there is an increasing polarization in health burdens, particularly among low- and high-risk populations, echoing trends observed in other rapidly developing countries1,26. This suggests that while current control practices have achieved substantial reductions in PM2.5 concentrations, they may inadvertently exacerbate health inequalities if not accompanied by targeted interventions.
Specifically, our results indicate that PM2.5 reduction contributed to a 25.1% decrease in premature deaths between 2013 and 2019. However, certain demographic factors, such as population aging and changes in baseline mortality rates, have offset some of these gains. The Gini coefficient, indicating disparities in PM2.5-related health burdens, rose by 19.7%, revealing that health risks have become increasingly concentrated in certain regions and populations. This increase in inequality means that while some areas benefit substantially from improved air quality, others, often with older populations or limited resources, are experiencing worsening health burdens. The provincial and urban disparities account for 78.9% and 88.3% of the overall inequality, respectively. These findings highlight that regional disparities remain the primary driver of PM2.5-related health inequalities, a pattern consistent across spatial scales and over time and in line with previous studies emphasizing persistent geographic health disparities in China27.
Moreover, demographic changes (especially the rapid aging of the population) have emerged as a critical factor increasing vulnerability, with older adults identified as the most at-risk group. Given the anticipated acceleration of population aging in the coming decade, the effectiveness of short-term demographic interventions may be limited. This underscores the importance of directly controlling PM2.5 exposures as a key strategy to mitigate associated public health risks28.
To address these challenges and make our findings actionable, we propose several specific policy recommendations. First, targeted healthcare support should be prioritized for regions with the highest PM2.5-related health burdens, including increased allocation of medical resources and the development of region-specific public health programs. Second, inter-provincial agreements to coordinate and limit emissions could help harmonize air quality improvements and reduce regional disparities. Third, special intervention programs in cities with persistently high pollution levels—such as stricter local emission standards, incentives for industrial upgrading, and enhanced public awareness campaigns—should be implemented. These approaches align with international best practices and the Sustainable Development Goals (SDG 3 and SDG 10), which emphasize reducing health inequalities and advancing environmental justice.
At the inter-regional level, a robust PM2.5 control framework is essential. This refers to an integrated system comprising national legislation, regional action plans, and standardized monitoring networks. Such a framework should enable real-time tracking of PM2.5 exposure disparities at both national and sub-national levels, facilitate coordinated policy responses, and support adaptive management based on ongoing monitoring and evaluation. This integrated approach has been shown to be effective in other contexts29, and its adoption in China could help ensure that air quality improvements translate into equitable health benefits. We recommend that organizations such as China’s Ministry of Ecology and Environment and local health authorities take the lead in implementing targeted regional interventions, prioritizing vulnerable populations, and enhancing interregional collaboration. Integrating broader social and economic policies with air pollution control measures is essential for achieving sustainable development goals.
We acknowledge several limitations of our study. The use of modeled PM2.5 and population data introduces uncertainties related to data resolution, model assumptions, and environmental changes. Moreover, our analysis focused primarily on geographic disparities and did not explicitly account for other dimensions of inequality, such as socioeconomic status or ethnicity. Future research should aim to incorporate multi-dimensional equity assessments and more granular data to provide a comprehensive understanding of PM2.5-related health inequalities.
Furthermore, although this study focuses on China, similar patterns of inequality are observed in other rapidly developing countries facing urbanization and demographic transitions. To further support this point, we conducted equity analyses for several developing countries and consistently found comparable results regarding environmental health disparities. The data and results of these cross-country calculations are presented in Supplementary Table 2 and Table 3. Our findings may therefore provide valuable insights for policymakers and researchers working in comparable contexts, highlighting the global relevance of addressing environmental health disparities through integrated and equitable policy approaches.
Methods
Data
We analyzed PM2.5 air quality data, mortality rates, and population data for 372 key cities across 34 provinces in China, covering the period from 2000 to 2019. All datasets, including population, PM2.5 concentrations, and GDP per capita, were processed in raster format with a spatial resolution of 1 km. The China annual PM2.5 concentration dataset was obtained from the National Tibetan Plateau Science Data Center (TPDC)30, which was developed using artificial intelligence techniques to account for the spatiotemporal heterogeneity of air pollution. This dataset, with a spatial resolution of 0.01° (WGS84), has been validated against ground-based measurements to ensure reliability. Population data were sourced from the WorldPop Research Programmer31, which integrates census information and ancillary data such as nightlights, and has been rigorously validated for accuracy across latitudes. The WorldPop Global population dataset was used to quantify the number of residents in each 1 km × 1 km grid cell. Mortality data for Hong Kong, Macao, and Taiwan were obtained from the respective local Center for Health Protection or Census Bureau. The Detailed datasets are presented in Supplementary Table 1.
In this study, we utilized existing PM2.5 and population datasets to estimate PM2.5-attributable mortality using established epidemiological models. Subsequently, we applied decomposition analysis to assess the contribution of multiple factors to mortality disparities. The geographic distribution of PM2.5 and PM2.5-related mortality was then evaluated using the Gini index to quantify spatial inequality across regions and cities. This integrated approach provides a comprehensive framework for investigating the spatial patterns and drivers of air pollution-related health impacts in China.
Population-weighted PM2.5 concentrations
Following the World Health Organization (WHO) guidelines, this study utilized population-weighted PM2.5 concentrations to conduct a comprehensive analysis across multiple administrative levels, including national, provincial, municipal, and county32,33. By assigning greater weights to regions with higher population densities, this approach more accurately reflects the exposure levels of PM2.5 experienced by the populace. This measure combines population distribution in space with PM2.5 concentration differences across geographical regions, providing a more accurate depiction of real-world exposure. The calculation of the population-adjusted PM2.5 concentration is formulated as follows:
Where \({P}_{i}\) and \({C}_{i}\) are the population and PM2.5 concentration in grid pixels \(i\). n is the total number of grid pixels in the analytical area.
Disease burden assessment
In this study, an upgraded Global Exposure Mortality Model (GEMM) was employed to assess the health impact linked to long-term PM2.5 exposure. This refined GEMM incorporated mortality data for five diseases. The model’s computation is based on the following formula17,30,34:
\({\mathrm{RR}}_{i,j,k}\) denotes the relative risk; \({C}_{i}\) is the value of PM2.5 concentration (μg m−3) in the grid cell; \({C}_{0}\) denotes the theoretical minimum risk concentration (2.4 μg m−3); \(\theta\), \(\alpha\), \(\mu\), and \(v\) are the fitting parameters of the PM2.5 exposure–response function35,36,37. Considering the uncertainty of the relative risk \({\mathrm{RR}}_{i,j,k}\) in the model, 95% confidence intervals for \({\mathrm{RR}}_{i,j,k}\) were calculated using standard errors in the GEMM (global exposure mortality model), where SE (\({\theta }_{j,k}\)) in Eq. denotes the standard deviation of \({\theta }_{j,k}\).
In the equation, as the PM2.5 exposure level increases, the RR value shows an upward trend. The quantitative correlation between these factors is discernible through the exposure-response function. In this study, the exposure-response function was adapted from GBD’s published Bayesian, regularization, and trim (MR-BRT) model. This method provides a comprehensive evaluation of PM2.5-related health risks, consistent with the advanced statistical approaches used by GBD. The deaths attributable to PM2.5 pollution (DAPP) was calculated primarily using the MR-BRT model median as the main result.
Building on the established link between PM2.5 exposure and risk, we can derive additional metrics to assess its health impact. Particularly, we are able to compute additional metrics such as the mortality rate (deaths per 105 population) and the mortality fraction resulting from PM2.5 exposure:
where, \({\mathrm{MR}}_{i,j}\) represents the mortality rate of disease \(j\) in grid \(i\), and \({M}_{i,j}\) is the mortality attributable to PM2.5 exposure for disease \(j\) in grid \(i\); and \({P}_{i}\) denotes the exposed population in grid \(i\). \({\mathrm{MF}}_{k,j}\) represents the mortality fraction of disease \(j\) in province \(k\); \({\mathrm{AM}}_{k}\) represents the all-cause mortality in province \(k\).
Decomposition of health burden drivers
To systematically quantify the contribution of key drivers to changes in PM2.5-related death, we adopted a decomposition approach inspired by the Global Burden of Disease (GBD) study38. This methodology allows for the attribution of changes in PM2.5-attributable deaths to four major factors: population size, age structure, baseline mortality, and PM2.5 concentration. By sequentially adjusting each factor while holding others constant, we can isolate the specific impact of each driver on mortality trends.
Given that the order in which input variables are adjusted can influence the estimated contributions, we performed sensitivity analyses by calculating all possible permutations of the four factors. The final contribution values for each driver were derived by averaging across all 24 possible input sequences, thereby minimizing sequence-dependent bias and enhancing the robustness of our estimates.
The contribution of each driver to the change in PM2.5-related death was calculated using the following key equations:
Where \({C}_{\mathrm{Pop}}\), \({C}_{\mathrm{PS}}\), \({C}_{B}\), and \({C}_{\mathrm{AP}}\) represent the percentage contribution of changes in population size, age structure, baseline mortality, and PM2.5 concentration, respectively, to the total change in PM2.5-related death. \({M}_{t0}\) and \({M}_{\mathrm{AP}}\) denote the estimated number of PM2.5-related deaths at the baseline and after all factors have been updated.
This decomposition framework provides a transparent and quantitative basis for understanding the relative importance of demographic, epidemiological, and environmental factors in shaping PM2.5-related health outcomes.
Measuring and decomposing inequalities of PM2.5 and PM2.5-health-burdens
The Gini coefficient39,40 is a well-established metric for quantifying inequality and is widely used in fields such as economic growth41, environmental justice42, income distribution43, and resource allocation44. In this study, we employ the Gini coefficient to assess disparities in both PM2.5 exposure and PM2.5-attributable mortality.
To clarify, we calculate the Gini coefficient in two distinct ways to capture different aspects of inequality. The first approach is person-based: all individuals are ranked by their PM2.5 exposure (or mortality risk), and the Gini coefficient quantifies how unequally PM2.5 exposure (or mortality) is distributed across the population. The formula is as follows:
where \({E}_{i}\) and \({E}_{j}\) represent the PM2.5 exposure (or attributable mortality) for individuals \(i\) and \(j\), \(n\) is the total population size, and \(\bar{E}\) is the mean PM2.5 exposure (or mortality) across all individuals.
The second approach is grid cell-based: all 1-km grid cells are ranked by their average PM2.5 concentration (or mortality rate), and the Gini coefficient reflects the spatial inequality in PM2.5 or mortality across geographic units. The formula is:
Where \({C}_{i}\) and \({C}_{j}\) are the PM2.5 concentration(mortality) of grid cell \(i\) and \(j\). \(n\) is the total number of grid cells in the analytical unit, and \(\bar{C}\) is the mean PM2.5 concentration of all grid cells.
The person-based Gini index incorporates population weighting within each grid cell, thus reflecting disparities in exposure or health burden at the individual level. In contrast, the grid cell-based Gini index measures only the spatial heterogeneity of PM2.5 or mortality across geographic units, without considering population distribution within each cell. Using both metrics allows us to disentangle the effects of population distribution from pure spatial inequality.
To further dissect the sources of inequality, we apply the Dagum decomposition method45. This technique breaks down the overall Gini coefficient into three components: within-group inequality (\({G}_{\text{within}}\)), between-group inequality (\({G}_{\text{between}}\)), and an overlapping component (\({G}_{\text{overlap}}\)) that accounts for distributional overlap between groups. The decomposition is expressed as:
Where \({v}_{k}\) is the proportion of group \(k\)'s population relative to the total population, \({\lambda }_{k}\) is the ratio of group, and \({G}^{k}\) is the Gini coefficient of group \(k\). \({G}_{\mathrm{within}}\) is measured as the weighted average of Gini coefficients within each subgroup. \({G}_{\mathrm{between}}\) reflects the impact of between different subgroups on the overall Gini coefficient. \({G}_{\mathrm{overlap}}\) accounts for the residual effects due to the overlap or interaction of income distributions between subgroups. This decomposition provides a deeper understanding of disparities that exist both between different population groups and within individual groups46.
Specifically, this approach allows for the decomposition of overall inequality into within-group, between-group, and overlapping components at multiple spatial scales. In our study, the decomposition can be applied at various administrative levels, such as provinces, cities, or counties, depending on the research focus. This flexibility enables us to systematically analyze and compare spatial inequality in PM2.5-related health burdens across different geographic units.
Mann–Kendall trend test
The Mann–Kendall (MK) trend test is a widely used nonparametric method for detecting monotonic trends in time series data. Unlike parametric approaches, the MK test does not require assumptions about the underlying data distribution, making it robust to small sample sizes and the presence of outliers. The test statistic S is calculated by evaluating all pairwise comparisons among data points in the series, where each comparison contributes positively, negatively, or neutrally depending on the direction of change.
To assess the significance of the observed trend, the standardized test statistic Z is computed, which under the null hypothesis of no trend follows a standard normal distribution. The p-value derived from Z is used to determine statistical significance, with P < 0.05 indicating a significant trend. In this study, a variance correction factor was applied to account for potential autocorrelation in the time series, thereby improving the reliability and robustness of the MK test results.
To evaluate the robustness of our mortality estimates, we conducted several sensitivity analyses (Supplementary Fig. 1). Specifically, we utilized alternative PM2.5 concentration datasets to recalculate PM2.5-attributable mortalities and compared the results across different data sources. For each dataset, we performed a spatial comparison of PM2.5 concentrations at identical locations to assess consistency and potential biases. Furthermore, principal component analysis (PCA) was applied to the PM2.5 data to investigate the similarity and usability of our primary dataset in relation to existing PM2.5 datasets. The results of these analyses demonstrate high concordance between different sources and confirm the reliability of our data.
Data availability
Data are provided within the Supplementary Information files. The Python code (standard regression analysis) used in this study is available from the corresponding author upon request.
References
Murray. et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study 2019. The Lancet 396, 1223–1249 (2020).
Cohen, A. J. et al. Estimates and 25-Year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the global burden of diseases study 2015. The Lancet 389, 1907–1918 (2017).
Brauer, M. et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: A systematic analysis for the global burden of disease study 2021. Lancet 403, 2162–2203 (2024).
World Health Organization. Ambient air pollution: A global assessment of exposure and burden of disease. https://www.who.int/publications/i/item/9789241511353 (2016).
Wu, X. et al. The epidemiological trends in the burden of lung cancer attributable to PM2.5 exposure in china. BMC Public Health 21, (2021).
Chen, J. & Hoek, G. Long-term exposure to PM and all-cause and cause-specific mortality: A systematic review and meta-analysis. Environment International 143, 105974 (2020).
Geng, G. et al. Drivers of PM2.5 air pollution deaths in china 2002–2017. Nature Geoscience 14, 645–650 (2021).
Liu, M. et al. How magnitude of PM2.5 exposure disparities have evolved across chinese urban-rural population during 2010–2019. Journal of Cleaner Production 382, 135333 (2023).
Yun, G. & Zhao, S. The imprint of urbanization on PM2.5 concentrations in china: The urban-rural gradient study. Sustainable Cities and Society 86, 104103 (2022).
Wang, X. et al. Responses of PM2.5 pollution to urbanization in china. Energy Policy 123, 602–610 (2018).
Geng, G. et al. Efficacy of china’s clean air actions to tackle PM2.5 pollution between 2013 and 2020. Nature Geoscience 17, 987–994 (2024).
Shi, S. et al. Evolution in disparity of PM2.5 pollution in china. Eco-environment & Health 2, 257–263 (2023).
Colmer, J., Hardman, I., Shimshack, J. & Voorheis, J. Disparities in PM2.5 air pollution in the united states. Science 369, 575–578 (2020).
Jbaily, A. et al. Air pollution exposure disparities across US population and income groups. Nature 601, 228–233 (2022).
Watts, N. et al. Health and climate change: Policy responses to protect public health. The Lancet 386, 1861–1914 (2015).
Yue H., He C., Huang Q., Yin D., Bryan B. A. Stronger policy required to substantially reduce deaths from PM2.5 pollution in china. Nature Communications 11, (2020).
Nansai, K. et al. Affluent countries inflict inequitable mortality and economic loss on asia via PM2.5 emissions. Environment International 134, 105238 (2020).
Gan, T., Yang, H. & Liang, W. How do urban haze pollution and economic development affect each other? Empirical evidence from 287 chinese cities during 2000–2016. Sustainable Cities and Society 65, 102642 (2021).
Li, Y., Zhao, X., Liao, Q., Yan, T. & Bai, Y. Specific differences and responses to reductions for premature mortality attributable to ambient PM2.5 in china. Science of The Total Environment 742, 140643 (2020).
Lelieveld, J., Evans, J. S., Fnais, M., Giannadaki, D. & Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525, 367–371 (2015).
Dong, Z. et al. Time-weighted average of fine particulate matter exposure and cause-specific mortality in china: A nationwide analysis. The Lancet Planetary Health 4, e343–e351 (2020).
Xue, T. et al. Rapid improvement of PM2.5 pollution and associated health benefits in china during 2013–2017. Science China Earth Sciences 62, 1847–1856 (2019).
Zhou, M. et al. Mortality, morbidity, and risk factors in china and its provinces, 1990–2017: A systematic analysis for the global burden of disease study 2017. The Lancet 394, 1145–1158 (2019).
Zhang, Q., He, K. & Huo, H. Cleaning China’s air. Nature 484, 161–162 (2012).
Yang, Y., Luo, L., Song, C., Yin, H. & Yang, J. Spatiotemporal Assessment of PM2.5-Related Economic Losses from Health Impacts during 2014–2016 in China. International Journal of Environmental Research and Public Health 15, 1278 (2018).
Brauer, M. et al. Ambient Air Pollution Exposure Estimation for the Global Burden of Disease 2013. Environmental Science & Technology 50, 79–88 (2015).
Chen, R. et al. Fine Particulate Air Pollution and Daily Mortality. A Nationwide Analysis in 272 Chinese Cities. American Journal of Respiratory and Critical Care Medicine 196, 73–81 (2017).
Liu, C. et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. New England Journal of Medicine 381, 705–715 (2019).
Apte, J. S., Marshall, J. D., Cohen, A. J. & Brauer, M. Addressing Global Mortality from Ambient PM2.5. Environmental Science & Technology 49, 8057–8066 (2015).
Wei, J. & Li, Z. ChinaHighPM2.5: Big data seamless 1 km ground-level PM2.5 dataset for china. Zenodo (CERN European Organization for Nuclear Research) (2019).
WorldPop. Population Counts. https://hub.worldpop.org/geodata/listing?id=64 (2024).
Lin, C. et al. Estimation of long-term population exposure to PM2.5 for dense urban areas using 1-Km MODIS data. Remote Sensing of Environment 179, 13–22 (2016).
Li, J. et al. Estimation of PM2.5 mortality burden in china with new exposure estimation and local concentration-response function. Environmental Pollution 243, 1710–1718 (2018).
Chowdhury, S. & Dey, S. Cause-specific premature death from ambient PM2.5 exposure in india: Estimate adjusted for baseline mortality. Environment International 91, 283–290 (2016).
Burnett, R. T. et al. Erratum: ‘An Integrated Risk Function for Estimating the Global Burden of Disease Attributable to Ambient Fine Particulate Matter Exposure’. Environ. Health Perspect. 122, A235 (2014). 122:.
Pope, C. A. et al. Cardiovascular mortality and exposure to airborne fine particulate matter and cigarette smoke. Circulation 120, 941–948 (2009).
Pope, C. A. et al. Lung cancer and cardiovascular disease mortality associated with ambient air pollution and cigarette smoke: Shape of the Exposure–Response relationships. Environmental Health Perspectives 119, 1616–1621 (2011).
Bu, X. et al. Global PM2.5-Attributable health burden from 1990 to 2017: Estimates from the global burden of disease study 2017. Environmental Research 197, 111123 (2021).
Giorgi, G. M. & Gigliarano, C. The gini concentration index: A review of the inference literature. Journal of Economic Surveys 31, 1130–1148 (2016).
Davidson, R. Reliable inference for the gini index. Journal of Econometrics 150, 30–40 (2009).
Gagliani, G. Income inequality and economic development. Annual Review of Sociology 13, 313–334 (1987).
Harner, J., Warner, K., Pierce, J. & Huber, T. Urban environmental justice indices. The Professional Geographer 54, 318–331 (2002).
Molero-Simarro, R. Inequality in china revisited: The effect of functional distribution of income on urban top incomes, the urban-rural gap, and the gini index, 1978–2015. China Economic Review 42, 101–117 (2017).
Dai, G., Li, R. & Ma, S. Research on the equity of health resource allocation in TCM hospitals in china based on the gini coefficient and agglomeration degree: 2009–2018. International Journal for Equity in Health 21, (2022).
Mookherjee, D. & Shorrocks, A. A decomposition analysis of the trend in UK income inequality. The Economic Journal 92, 886 (1982).
Bai, Y. & Liu, M. Multi-scale spatiotemporal trends and corresponding disparities of PM2.5 exposure in china. Environmental Pollution 340, 122857 (2024).
Acknowledgments
J.X. acknowledge funding from National Natural Science Foundation of China (No. 42171400); Guangdong Marine Economy Development Special Project (GDNRC [2023]25); Shenzhen Science and Technology Program (JCYJ20220818100200001, SYSPG20241211173845013).
Author information
Authors and Affiliations
Contributions
K.X., J.X., and W.T. conceptualized the idea and developed the outline. K.X., Z.H., and J.X. prepared the initial paper text, and H.L., R.C., Q.D., and Y.W. prepared Figure. All authors (K.X., Z.H., Y.W., H.L., R.C, W.T., and J.X.) reviewed, revised, and contributed to the final paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xia, K., Huang, Z., Deng, Q. et al. Inequality in PM2.5 Exposure and Health burden attributable in China. npj Clim. Action 5, 14 (2026). https://doi.org/10.1038/s44168-026-00340-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44168-026-00340-y
