
Abstract
Syndemic theory posits that multiple, interconnected health behaviors—such as substance use, anxiety, depression, sexual risk behaviors, and societal or social stressors—interact synergistically within specific populations, particularly in those who face social disadvantage. These health behaviors are not isolated, but are shaped and exacerbated by social, economic, and environmental factors. Using data from the 2021 Youth Risk Behavior Surveillance System (N = 17,232), this cross-sectional study examined how the co-occurrence of substance use, mental health challenges, sexual risk behaviors, and COVID-19 pandemic-related stress creates different risk profiles among adolescents. Latent class analysis (LCA) results identified five distinct profiles of behavioral health risks: Class 1 (Complex high-risk), Class 2 (Moderate risk experimenters), Class 3 (Recent polysubstance use/Covid distress), Class 4 (Low-risk/COVID distress), and Class 5 (Low-risk). COVID distress referred to pandemic-related anxiety or stress. Higher-risk classes were characterized by recent substance use, engagement in condomless sex and having multiple partners, and psychological distress. Females, sexual minority adolescents, older-aged adolescents, and racially/ethnically marginalized groups were disproportionately represented in high-risk classes. The co-occurrence of substance, mental health challenges, and sexual risk behaviors reflects underlying structural and social inequities. By applying a syndemic lens, this study highlights the need for integrated, culturally responsive and contextually appropriate interventions, alongside early prevention and systemic policy changes to promote positive adolescent health.
Similar content being viewed by others

Introduction
Syndemic theory suggests that the convergence of multiple health behaviors increases risks for and burden of negative health and social consequences than the experience of any single risk1. Syndemics suggests that interacting physical, mental, structural, and social problems contribute to health inequalities2. Rather than focusing on individual markers for a single disease, syndemics examines how diseases cluster within populations as a result of social inequality in a biosocial approach1,3. These factors were originally identified as a syndemic of HIV in men who have sex with men (MSM) and were characterized as co-occurring epidemics of substance abuse, violence and AIDs (SAVA)3,4. Syndemics is now widely applied in both infectious and chronic disease models and may be particularly appropriate for factors that cannot be explained solely by individuals’ risk behaviors (e.g., number of sex partners and condom use) nor prevented by universal behavioral interventions5,6. Interventions that singularly target independent risk factors such as substance use, anxiety and depression, or sexual risk behaviors have had limited success in improving health outcomes for adolescents7,8. Identifying multiple behavioral health profiles to target simultaneously could improve intervention efficacy. Using a syndemic theoretical framework to examine multiple co-occurring risk factors among high school adolescents could be critical in developing high-impact interventions targeted for adolescents at high risk for adverse health and wellbeing outcomes9,10. However, little is known about the co-occurring profiles of substance use, mental health outcomes, sexual risk behaviors, and societal stressors among US adolescents.
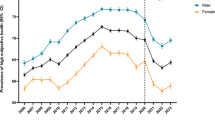
Understanding the landscape and context of adolescent health and wellbeing factors is crucial to improving outcomes and supporting positive transition to adulthood. Despite declining trends in sexual risk behaviors among US high school students, the Centers for Disease Control and Prevention (CDC) reports that between 2011 and 2021, condom use among sexually active students decreased from 67 to 58% among males and 54 to 47% in females11, and adolescent pregnancies and births remain higher than in comparable countries12. Some adolescents, such as those identifying as lesbian, gay, and bisexual (LGB), are at greater risk than heterosexuals to engage in risk behaviors (e.g., alcohol and substance use, inconsistent condom use) that may lead to negative health outcomes. For example, 19% of students with same sex partners have had sex with four or more lifetime partners compared to 13% of heterosexual students. Roughly 20% of gay or bisexual male students drank alcohol or used drugs before sex11. Population data show that 19% of all sexually active US adolescents drank alcohol or used drugs before their most recent sexual encounters11. Adolescents may engage in condomless sex under the influence of drugs or alcohol13,14,15,16, which are associated with increased risks for HIV and other sexually transmitted infections (STIs)17. The prevalence of drug and alcohol use before sex ranges from 12.6% to 34.6% among US adolescents11,18. Use of multiple illicit substances (i.e., polysubstance use) such as marijuana, tobacco, and alcohol among adolescents is a growing critical public health concern11. The prevalence of lifetime use of any illicit substance among adolescents ranges from 34 to 48%19. Lifetime prevalence of cigarette smoking ranges from 18% to 28%, the use of electronic vaporizer is 30 to 34%, marijuana use is 30 to 45%, and alcohol use is 43 to 61%19.
Adolescents experiencing anxiety, depression, and suicidal ideation are more likely to use marijuana, drink alcohol, and engage in condomless sex20,21. Since 2007, the prevalence of psychological distress and suicidal ideation have increased from 14.5% in 2007 to 17.2% in 2017 among adolescents in the United States11. Studies have demonstrated that adolescents with anxiety and depression are more likely to use tobacco products, marijuana, and illicit drugs (e.g., meth, cocaine, and heroin)22,23. Additionally, adolescents who use substances are less likely to use condoms during sex than non-substance-using adolescents; they also have sex with multiple partners and perform varied types of sex (e.g., oral and anal)24. It is imperative to understand the influence of these co-occurring factors that may uniquely compound to result in substance use in adolescents and understand the drivers of the development of substance use disorders.
It is well established that sexual risk, substance use, and mental health are highly correlated25,26. Since adolescence is a crucial developmental period for self-exploration and susceptibility to negative psychosocial influences, understanding the interconnectedness of substance use, mental health, and sexual behavior among adolescents is particularly important. Polysubstance use and sexual risk behaviors at a young age are associated with increased risk for addiction, mental health problems, and STIs throughout the life course26,27. Additionally, the adoption of negative health behaviors in adolescence can lead to increased health and social disparities later in life11,19,28. Strategies to reduce sexual risk-taking, substance use, and improve mental health among adolescents are urgently needed29,30.
During the COVID-19 pandemic, drastic changes and significant disruptions (i.e., changes in learning modality, isolation)31, coupled with the loss of normalcy32, led to widespread psychological health issues among adolescents33,34. These mental health challenges have been associated with challenges in optimal sexual and psychological heath35, including increases in condomless sex and numbers of sexual partners in the past year, and an increase in varied substance use36. The prevalence of HIV testing decreased 3.7% among adolescents from 2019 to 2021, and condomless sex increased by 2.7%, further highlighting the pandemic’s disruptive nature on adolescent health services37.
The present study explores profiles of mental health, substance use, and sexual risk behaviors among US adolescents and the factors associated with these profiles. Guided by syndemic theory, latent class analysis (LCA) is a useful approach to explore how behavioral health risks co-occur without losing specificity regarding the individual domains of risk38. Specifically, LCA identifies subgroups within a sample and highlights the profiles and conditional probabilities of behaviors within an identified profile38. Although informative, the binary, independent measures of risk behaviors inform only part of the narrative surrounding risk factors among US adolescents. Examining how substance use, mental health indicators, and sexual risk behaviors might co-occur to enhance the progression of negative health outcomes is important in further devising optimal prevention strategies and timely interventions.
Additionally, the pandemic changed access to resources and introduced stressors that were not previously influencing health and psychological factors. Understanding the constructs that facilitate risk among adolescents, particularly in the context of the pandemic, may provide a unique opportunity to develop effective and culturally appropriate intervention strategies targeting high-risk, hard-to-reach subgroups. By examining subgroups of adolescents who use substances, have adverse mental health, and engage in sexual risk behaviors, the findings are hypothesized to provide a foundation for tailored and targeted interventions that could be developed for subpopulations of adolescents in the United States.
Methods
Data for this study were obtained from the CDC’s 2021 youth risk behavior survey (YRBS), representing an early opportunity to evaluate adolescents’ health behaviors within the context of ongoing public health surveillance efforts39,40,41. The YRBS includes a range of domains related to substance use, mental health, sexual risk behaviors, and other health-related behaviors. The survey is administered to high school students and uses a three-stage cluster sampling design to estimate the national rates of health-related behaviors among high school students (N = 17,232). A more detailed description of the sampling methods and study procedures is published elsewhere39,40. Briefly, 152 high schools (72.7% school response rate) completed the YRBS from all 50 states and the District of Columbia in 2021. The student response rate at the participating schools was 79.1%26. This study was conducted in compliance with the Declaration of Helsinki. Ethical approval and informed consent were not required as the analysis used secondary data collected by the CDC. The YRBS dataset was fully anonymized prior to being made available to the research team, and no personally identifiable information was provided.
Demographic measures
Single-item measures of sex at birth (male, female), sexual orientation (LGB, questioning, other sexual minority, and heterosexual), race/ethnicity (Asian, Black, Hispanic, multiracial Hispanic, multiracial non-Hispanic, and White) and high school grade levels (nine to twelve) were included as demographic covariates.
Sexual risk
Single-item measures of sexual risk behaviors were assessed through age of sexual debut, number of lifetime partners, condom use at last intercourse, and drug or alcohol use prior to last intercourse.
Substance use
Single-item measures of lifetime and recent history of substance use questions were included to assess alcohol, marijuana, cigarettes, electronic cigarettes, and electronic vaping. Responses were recoded into two questions for each substance: lifetime and past 30-day use. Each of these substances were categorized as “Never,” “Ever” (ever used within their lifetime), and “Recent” (past 30-day use).
Suicidal ideation and depression
The following items were used as two separate single-item mental health indicators: Depression was assessed as “During the past 12 months, did you ever feel so sad or hopeless almost every day for 2 weeks or more in a row that you stopped doing some usual activities?” and suicidal ideation as “ During the past 12 months, did you ever seriously consider attempting suicide?” Response options were dichotomous: “yes” or “no.”
COVID-19 pandemic
Two questions were added to the 2021 YRBS about experiences during the COVID-19 pandemic. Respondents were asked, “During the COVID-19 pandemic, how often was your mental health not good? (Poor mental health includes stress, anxiety, and depression.)” with responses trichotomized as “never/rarely,” “sometimes,” or “most of the time/always.” Respondents were also asked, “During the COVID-19 pandemic, did a parent or other adult in your home lose their job even for a short amount of time” to which responses were dichotomized as “yes” or “no.”
All analyses were conducted using Mplus 8.1027. Sample weights were included in analyses to adjust for survey non-response and sample selection probabilities. Primary sampling units (PSU) and stratum variables were included to account for the complex sampling design. Missing data for latent class indicators were handled using the full information maximum likelihood (FIML) capabilities of Mplus. We used latent class analysis (LCA) to identify homogeneous subgroups of adolescents based upon response patterns to the sexual risk, substance use, and mental health indicators. To determine the number of classes, a series of models were conducted. An initial one-class model was assessed, followed by two-, three-, four- and five-class models representing different patterns of behavioral health risk. Optimal model selection for the five-class model was based upon recommended indices, including low adjusted Bayesian information criterion (BIC) relative to other models, significant Lo–Mendell–Rubin likelihood ratio test (LMR LRT), and acceptable quality of classification28. After determining the appropriate number of classes, we used the R3STEP method in Mplus to conduct multinomial logistic regression to assess the odds of class membership associated with sex, sexual orientation, race, and grade level.
Results
Demographics
The student sample described in Table 1 was evenly distributed across grades, each comprising approximately one-fifth of the population. Most students identified as heterosexual (70.6%), though a significant portion identified as gay, bisexual, lesbian (14.4%), or other/questioning (4.9%). The majority were White (50.1%), followed by Black (12.0%), multiracial Hispanic (15.6%), and Hispanic (9.5%). Male (50.9%) and female (47.6%) students were nearly equally represented. Mental health concerns were prominent—41.6% reported feeling depressed, and 21.6% had experienced suicidal thoughts. Most students (63.4%) had never had sex; however, among those who had, 8.5% reported three or more partners and inconsistent condom use was reported at 14.5%. The pandemic had a clear impact on adolescent mental health: 29.3% felt mentally affected most of the time or always, and nearly one in four students (19.3%) had a parent who lost their job due to COVID-19.
Latent class analysis
Table 2 depicts the response probability results of the five-class model. The five-class latent class model revealed distinct subgroups of adolescents based on patterns of substance use, sexual behavior, mental health, and COVID-19-related distress. Approximately 14.6% of the sample belonged to the “complex high-risk” class, characterized by the highest levels of recent substance use across alcohol, marijuana, cigarettes, and e-cigarettes. Members of this class were also the most likely to report early sexual debut, multiple sexual partners, substance use during sex, and low condom use. Additionally, they had an increased probability of depressive symptoms (73.7%), suicidal ideation (51.0%), and feeling emotionally distressed (60.0%) most or all of the time due to the COVID-19 pandemic.
The “moderate risk experimenters” class accounted for 15.1% of the sample and included adolescents who had initiated sexual activity and engaged in moderate levels of experimentation with substances, particularly alcohol and marijuana. While recent substance use was lower than in the “Complex High-Risk” class, members displayed higher probabilities of depressive symptoms (42.3%) and suicidal ideation (20.1%). The “recent-polysubstance use-COVID-distress” class (12.2%) was defined by moderate to high levels of recent alcohol, marijuana, and e-cigarette use, but no sexual activity. Mental health concerns were also pronounced, with higher probabilities of reporting depressive symptoms (64.3%) and suicidal ideation (34.9%). This class appeared to be highly impacted by the pandemic, with a higher probability of experiencing COVID-related emotional distress most or all of the time (sometimes—29.5%; mostly/always—32.3%). The “low-risk/COVID distress” class made up 17.0% of the sample and included adolescents with very low conditional probabilities of substance use and no sexual activity, but strikingly high probabilities of depressive symptoms (86.2%) and suicidal ideation (41.7%). Despite their endorsement of low engagement in externalizing risk behaviors, this group appeared to be emotionally vulnerable and particularly affected by COVID-related distress.
Finally, the largest class, “low-risk” (41.2%), represented adolescents with conditional probabilities of minimal to no substance use, no sexual activity, and the lowest probabilities of depressive symptoms (6.7%) and suicidal ideation (0.9%). This group also reported the highest probabilities of having little to no COVID-related emotional distress (63.3%).
Multinomial regression analysis
Table 3 depicts the results of the multinomial logistic regression analysis, which was conducted because there are multiple levels in the classes and covariates. Comparing the complex high-risk class to the low-risk, males had significantly lower odds of being in “complex high-risk” class (OR = 0.45; 95% CI: 0.38– 0.53). All sexual minority adolescents and those questioning their sexual identity had higher odds of being in the “complex high-risk” class than the “low-risk” class: LGB adolescents (OR = 4.52; 95% CI: 3.58 —5.70), other sexual minority (OR: 2.95; 95% CI: 1.91—4.57), and questioning (OR = 1.60; 95% CI: 1.11—2.31). Compared to White adolescents, Asian adolescents were less likely to belong to the “complex high-risk” class than the “low-risk” class (OR = 0.19; 95% CI: 0.13—0.28) as opposed to multiracial Hispanic adolescents (OR = 1.36; 95% CI: 1.10—1.68). Ninth graders (OR = 0.18; 95% CI: 0.13—0.24) were less likely to belong to the “complex high-risk” class than the “low-risk” class compared to twelfth graders.
LGB adolescents were significantly more likely to be moderate risk experimenters (OR = 2.32; 95% CI: 1.93–2.80) compared to heterosexual adolescents. Asian adolescents had the lowest odds of belonging to the “moderate risk experimenters” class (OR = 0.27; 95% CI: 0.19–0.39); Black adolescents had the highest odds (OR = 1.62; 95% CI: 1.27– 2.07). Ninth graders were less likely (OR = 0.17; 95% CI: 0.13–0.21) to belong to the “moderate risk experimenters” class compared to 12th graders.
Males had significantly lower odds of being in the “recent-polysubstance-use-covid-sad” class (OR = 0.43; 95% CI: 0.34–0.54). Compared to heterosexual adolescents, all sexual minority adolescents and those questioning their sexual identity had higher odds of being placed in the “recent-polysubstance-use-covid-distress” class than the “low-risk” class: LGB adolescents (OR = 3.33; 95% CI: 2.48–4.45), other sexual minority (OR: 2.40; 95% CI: 1.53–3.77), and questioning (OR = 1.63; 95% CI: 1.02–2.61). Compared to White adolescents, Asian adolescents had the lowest odds of being in the “recent-polysubstance-use-covid-distress” class than “low-risk class” (OR = 0.50; 95% CI: 0.31–0.79), whereas multiracial Hispanic adolescents had the highest odds (OR = 1.31; 1.13–1.51). Only ninth graders had significantly lower odds been placed in this class than the “low-risk” class when compared to twelfth graders (OR = 0.60; 95% CI: 0.45–0.79).
For the “low-risk-covid-distress” class, males had significantly lower odds of being in this class than the “low-risk” class (OR = 0.29; 95% CI: 0.24–0.35). Compared to heterosexual adolescents, all sexual minority adolescents and those questioning their sexual identity had higher odds of being placed in the “recent-polysubstance-use-covid-distress” class than the low-risk class: LGB adolescents (OR = 4.40; 95% CI: 3.59–5.39), other sexual minority (OR: 6.23; 95% CI: 4.52–8.59), and questioning (OR = 2.89; 95% CI: 1.95–4.26).
Discussion
This cross-sectional study identified five distinct profiles of substance use, adverse mental health outcomes, and engagement in sexual risk behaviors that co-occurred among young people in the US adolescents in the study reported a high prevalence of adverse mental health outcomes, which were exacerbated during the COVID-19 pandemic. Polysubstance experimentation, anxiety, suicidal ideation, and sexual activity were common. One particularly complex high-risk group in the study was comprised of sexual minority females and multiracial Hispanic adolescents. Complex high-risk behaviors in this class also included higher probabilities of recent alcohol, marijuana, and e-cigarette use. Additionally, this class had a higher probability of feeling depressed, experiencing suicidal ideation, having three or more lifetime sexual partners, using drugs and alcohol at their last sexual encounter and not using a condom. Complex high-risk adolescents were regularly concerned about COVID-related stressors and had a parent who experienced job loss during the pandemic42.
A syndemic of mental health factors, societal stressors and risk behaviors—including substance use, higher numbers of lifetime sexual partners, and inconsistent condom use—is related to adverse health and social challenges in young adulthood and later life43,44. Our findings are similar to our previous study of complex psychosocial and behavioral factors among adolescents. In one sample of Black adolescents, polytobacco users had the highest probabilities of recent cigarette use, e-cigarette use, ever smoking cigars, or chewing tobacco42. Ever and current use of marijuana were associated with increased odds of e-cigarette use, and current marijuana use was associated with increased odds of polytobacco use (aOR = 24.61, CI = 6.95–87.11)42. In a separate analysis of representative US adolescents, we demonstrated that younger adolescents had a higher relative probability of co-occurring problem behaviors and polysubstance use, including illicit drug use, combustible tobacco, cannabis use, binge drinking, past 30-day use of alcohol, emotional distress, and three or more sexual partners45. The convergence of anxiety, societal stressors, and risk behaviors such as substance use and inconsistent condom use represents a syndemic that can lead to long-term health and social consequences.
Understanding the implications of polysubstance use for adolescents is imperative as use continues to rise. The co-occurrence of anxiety, depression and suicidal ideation is also concerning and suicidal ideation among high school-aged adolescents in the United States has increased from 16.0% in 2011 to 22.0% in 202111. Studies have demonstrated that adolescents with anxiety and depression are more likely to use tobacco products, marijuana, illicit drugs (e.g., meth, cocaine, and heroin) and alcohol22,23. The rising prevalence of polysubstance use alongside increasing rates of anxiety, depression, and suicidal ideation among adolescents underscores the need for integrated mental health and substance use interventions. Early screening and targeted prevention efforts should focus on adolescents experiencing psychological distress, as they are more likely to use substances to cope. Reducing stigma, expanding access to mental health care, and promoting emotional literacy in schools are essential steps46. Continued monitoring and research are also critical to understanding and responding to these converging trends in adolescent health.
Adolescents experiencing cultural stressors in addition to normal explorations of substance use and initiation of sexual behaviors would benefit from culturally responsive interventions for multiracial, Hispanic, female, and sexual minority adolescents who face compounded behavioral health risks. Prevention strategies should be intersectional, addressing co-occurring substance use, mental health issues, and sexual risk behaviors. These findings underscore the need for tailored and targeted interventions that incorporate social and societal stressors, such as pandemic-related stress, that could be developed for subpopulations of adolescents in the United States. A tailored intervention would be particularly impactful for high-risk groups like Black adolescents who engage in polytobacco and marijuana use. Culturally responsive, early intervention programs and updated substance use education are essential. For instance, interventions designed to reduce or delay substance use and sexual debut may focus on racial, gender-based programs that integrate important intersectional and empowerment theories to support protective factors such as racial identity and gender racial socialization47. Additionally, structural changes and supportive policies that reduce systemic stressors are critical, along with continued longitudinal research to inform effective public health responses.
The COVID-19 pandemic significantly influenced mental health, social connectedness, and influenced drastic changes and significant disruptions to resources and available services for adolescents31,32,33,34. The interruption of engagement in social supports greatly impacted the health and well-being of young people, with effects still observed in substance use and sexual behaviors35,36,37. The present study observed pandemic-related stressors as part of a syndemic that included anxiety, substance use, and sexual risk behaviors for a proportion of adolescents in the sample. While the pandemic provided benefits to some, disengagement in social settings and isolation heightened for others, potentially accelerating adverse health behaviors48,49. In the current study, pandemic-related stressors were included as a broader societal influence that was outside of traditional health behaviors but had a significant and lasting influence on behaviors and outcomes for adolescents. The application of syndemics in the context of COVID-19 is helpful in examining the magnitude of influence of those factors within the model and the inclusion of those characteristics in profiles of adolescents at high risk for adverse health behaviors50. This has been explored in adult populations, but has not been widely applied in adolescents. While not exclusively a structural factor (e.g., housing, food security, and health care access), pandemic- related stress may have been a downstream effect of greater structural factors that could influence adolescents’ experiences, similar to social deprivation, and culturally marginalizing events51. Interventions for adolescents must address the social and contextual factors that currently contribute to their anxiety to most effectively improve health behaviors and outcomes.
Adolescent health interventions should adopt a biosocial framework to explore how issues like poverty, social stressors and health behaviors compound adolescent health risks. Developing multi-level interventions that target co-occurring challenges (i.e., mental health, substance use, sexual health) and integrate social context of societal stressors (i.e., the pandemic) can lead to more effective outcomes. Continued expansion of the use of syndemic models beyond HIV to broader adolescent health crises, such as mental health and substance use, and engaging marginalized communities through participatory research, will be essential for creating equitable, contextually relevant public health solutions.
This study must be interpreted with some limitations. The study was limited to the most recently available cycle for which data were collected from September to December 202152, and is further limited by the temporal context that behaviors and attitudes may have significantly shifted due to varying factors during the pandemic. Mental health factors included in this study were limited to suicidal ideation, anxiety and pandemic-related stress—included two questions about parent job loss and poor mental health due to the pandemic. While helpful indicators, the limited scope of the questions may not capture the full range of factors influencing anxiety among adolescents. Additionally, measurement validity may be lessened by the absence of a validated scale. The cross-sectional design of YRBS limits causal inferences, generalizability, and there is potential for misclassification within latent class results.
Results of this study reveal distinct profiles of co-occurring behavioral health risks among US adolescents, highlighting the compounded vulnerabilities faced by multiracial, Hispanic, female, and sexual minority adolescents. The intersection of substance use, mental health challenges, and risky sexual behaviors reflects broader structural and social inequities. A syndemic framework underscores the importance of integrated, trauma-informed, and culturally responsive interventions that address these overlapping risks. Early prevention, expanded mental health access, and structural policy changes are essential to reducing disparities and promoting long-term adolescent health.
Data availability
The data that support the findings of this study are openly available from the CDC’s YRBSS Data & Documentation at https://www.cdc.gov/yrbs/data/index.html.
References
Singer, M., Bulled, N., Ostrach, B. & Mendenhall, E. Syndemics and the biosocial conception of health. Lancet 389, 941–950 (2017).
Singer, M. AIDS and the health crisis of the U.S. urban poor; the perspective of critical medical anthropology. Soc. Sci. Med. 39, 931–948 (1994).
Singer, M., Bulled, N. & Ostrach, B. Whither syndemics?: trends in syndemics research, a review 2015-2019. Glob. Public Health 15, 943–955 (2020).
Stall, R. et al. Association of co-occurring psychosocial health problems and increased vulnerability to HIV/AIDS among urban men who have sex with men. Am. J. Public Health 93, 939–942 (2003).
Mendenhall, E., Kohrt, B. A., Logie, C. H. & Tsai, A. C. Syndemics and clinical science. Nat. Med. 28, 1359–1362 (2022).
Mendenhall, E., Newfield, T. & Tsai, A. C. Syndemic theory, methods, and data. Soc. Sci. Med. 295, 114656 (2022).
Coulter, R. W. S. et al. Mental health, drug, and violence interventions for sexual/gender minorities: a systematic review. Pediatrics 144, e20183367 (2019).
Jackson, C., Geddes, R., Haw, S. & Frank, J. Interventions to prevent substance use and risky sexual behaviour in young people: a systematic review. Addiction 107, 733–747 (2012).
Okumu, M., Ombayo, B. K., Small, E. & Ansong, D. Psychosocial syndemics and sexual risk practices among U.S. adolescents: findings from the 2017 U.S. youth behavioral survey. Int. J. Behav. Med. 26, 297–305 (2019).
Hill, A. V. et al. Identifying syndemics for sexually transmitted infections among young adults in the United States: a latent class analysis. J. Adolesc. Health 64, 319–326 (2019).
CDC. Youth Risk Behavior Survey-Data Summary & Trends Report:2011–2021 (Centers for Disease Control and Prevention, 2023).
World Health Organization. Adolescent birth rate (per 1000 women). https://www.who.int/data/gho/data/indicators/indicator-details/GHO/adolescent-birth-rate-(per-1000-women-aged-15-19-years) (2024).
Clayton, H. B., Andrzejewski, J., Johns, M., Lowry, R. & Ashley, C. Does the association between substance use and sexual risk behaviors among high school students vary by sexual identity? Addict. Behav. https://doi.org/10.1016/j.addbeh.2019.01.018 (2019).
Tucker, J. S. et al. Substance use and other risk factors for unprotected sex: results from an event-based study of homeless youth. AIDS Behav. 16, 1699–1707 (2012).
Ritchwood, T. D., Ford, H., DeCoster, J., Sutton, M. & Lochman, J. E. Risky sexual behavior and substance use among adolescents: a meta-analysis. Child Youth Serv. Rev. 52, 74–88 (2015).
Anderson, J. E. & Mueller, T. E. Trends in sexual risk behavior and unprotected sex among high school students, 1991–2005: the role of substance use. J. Sch. Health 78, 575–580 (2008).
Nagata, J. M. et al. Food insecurity, sexual risk, and substance use in young adults. J. Adolesc. Health 68, 169–177 (2021).
Kann, L. et al. Youth risk behavior surveillance—United States, 2017. MMWR Surveill. Summ. 67, 1–114 (2018).
Johnston, L. D. et al. Monitoring the future national survey results on drug use: overview, key findings on adolescent drug use. http://www.monitoringthefuture.org/pubs/monographs/mtf-overview2017.pdf (2018).
Feder, K. A. et al. Association of mental health symptoms and peer behaviors with risk for substance use and condomless sex among youths in juvenile drug court. J. Child Adolesc. Subst. Abus. 27, 133–145 (2018).
Ammerman, B. A., Steinberg, L. & McCloskey, M. S. Risk-taking behavior and suicidality: the unique role of adolescent drug use. J. Clin. Child Adolesc. Psychol. 47, 131–141 (2018).
Wolitzky-Taylor, K. et al. Transdiagnostic processes linking anxiety symptoms and substance use problems among adolescents. J. Addict. Dis. 35, 266–277 (2016).
Wu, P. et al. The relationship between anxiety disorders and substance use among adolescents in the community: specificity and gender differences. J. Youth Adolesc. 39, 177–188 (2010).
Shrier, L. A., Walls, C., Lops, C., Kendall, A. D. & Blood, E. A. Substance use, sexual intercourse, and condom nonuse among depressed adolescents and young adults. J. Adolesc. Health 50, 264–270 (2012).
Jackson, J. M., Seth, P., DiClemente, R. J. & Lin, A. Association of depressive symptoms and substance use with risky sexual behavior and sexually transmitted infections among African American female adolescents seeking sexual health care. Am. J. Public Health 105, 2137–2142 (2015).
Hill, A. V. et al. BDJJoAH. Identifying syndemics for sexually transmitted infections among young adults in the United States: a latent class analysis. J. Adolesc. Health 64, 319–326 (2019).
Hill, A. V. et al. Adolescent relationship abuse, gender equitable attitudes, condom and contraception use self-efficacy among adolescent girls. J. Interpers. Violence 37, NP22329–NP22351 (2022).
Vasilenko, S. A., Kugler, K. C., Butera, N. M. & Lanza, S. T. Patterns of adolescent sexual behavior predicting young adult sexually transmitted infections: a latent class analysis approach. Arch. Sex. Behav. 44, 705–715 (2015).
CDC. Mental health. https://www.cdc.gov/healthyyouth/mental-health/index.htm (2021).
CDC. Substance use and sexual risk behaviors among youth. https://www.cdc.gov/healthyyouth/factsheets/substance_use_fact_sheet-basic.htm (2023).
Hertz, M. F. et al. Adolescent mental health, connectedness, and mode of school instruction during COVID-19. J. Adolesc. Health 70, 57–63 (2022).
Walsh, F. Loss and resilience in the time of COVID-19: meaning making, hope, and transcendence. Fam. Process 59, 898–911 (2020).
Gotlib, I. H. et al. Effects of the COVID-19 pandemic on mental health and brain maturation in adolescents: implications for analyzing longitudinal data. Biol. Psychiatry Glob. Open Sci. 3, 912–918 (2023).
Panchal, U. et al. The impact of COVID-19 lockdown on child and adolescent mental health: systematic review. Eur. Child Adolesc. Psychiatry 32, 1151–1177 (2023).
Alamolhoda, S. H., Zare, E. & Nasiri, M. The status of adolescent health during the COVID-19 pandemic. J. Med. Life 15, 675–678 (2022).
Temple, J. R. et al. The impact of the COVID-19 pandemic on adolescent mental health and substance use. J. Adolesc. Health 71, 277–284 (2022).
Szucs, L. E. et al. Role of the COVID-19 pandemic on sexual behaviors and receipt of sexual and reproductive health services among U.S. high school students - youth risk behavior survey, United States, 2019-2021. MMWR Suppl. 72, 55–65 (2023).
Assanangkornchai, S., Li, J., McNeil, E. & Saingam, D. Clusters of alcohol and drug use and other health-risk behaviors among Thai secondary school students: a latent class analysis. BMC Public Health 18, 1–10 (2018).
Brener, N. D. et al. Methodology of the youth risk behavior surveillance system—2013. MMWR Recomm. Rep. 62, 1–20 (2013).
CDC. 2017 YRBS Data User’s Guide (2018).
Mpofu, J. J. et al. Overview and methods for the youth risk behavior surveillance system - United States, 2021. MMWR Suppl. 72, 1–12 (2023).
Gilreath, T. D., Dangerfield, D. T., Montiel Ishino, F. A., Hill, A. V. & Johnson, R. M. Polytobacco use among a nationally-representative sample of black high school students. BMC Public Health 21, 206 (2021).
Choi, H. J., Lu, Y., Schulte, M. & Temple, J. R. Adolescent substance use: latent class and transition analysis. Addict. Behav. 77, 160–165 (2018).
Merrin, G. J. et al. Continuity and change in substance use patterns during the transition from adolescence to young adulthood: examining changes in social roles. Int. J. Ment. Health Addict. 23, 4155–4177 (2024).
Cadet, K., Hill, A. V., Gilreath, T. D. & Johnson, R. M. Grade-level differences in the profiles of substance use and behavioral health problems: a multi-group latent class analysis. Int. J. Environ. Res. Public Health 21, 1196 (2024).
Khanal, S. P., Budhathoki, C. B. & Okan, O. Effectiveness of a school-based health literacy intervention in improving adolescent health literacy and the intention to take health-promoting actions. BMC Public Health 25, 3551 (2025).
Opara, I., Martin, R., Hill, A. V. & Calhoun, A. Addressing gendered racism against black girls using a strengths-based empowerment-intersectional framework for sexual health and substance use prevention programming. Health Promot. Pract. 24, 617–622 (2023).
Liu, J., Chai, L., Zhu, H. & Han, Z. COVID-19 impacts and adolescent suicide: the mediating roles of child abuse and mental health conditions. Child Abus. Negl. 138, 106076 (2023).
Donker, M. H., Mastrotheodoros, S., Yanagida, T. & Branje, S. Changes in adolescents’ COVID-19-health-related stress, parent-adolescent relationships, and mental health during the COVID-19 pandemic: the effect of personality traits. J. Youth Adolesc. 54, 209–224 (2025).
Shiau, S., Krause, K. D., Valera, P., Swaminathan, S. & Halkitis, P. N. The burden of COVID-19 in people living with HIV: a syndemic perspective. AIDS Behav. 24, 2244–2249 (2020).
Orben, A., Tomova, L. & Blakemore, S.-J. The effects of social deprivation on adolescent development and mental health. Lancet Child Adolesc. Health 4, 634–640 (2020).
Mpofu, J. J. Overview and methods for the youth risk behavior surveillance system—United States, 2021. MMWR Suppls. 72, 1–12 (2023).
Author information
Authors and Affiliations
Contributions
A.V.H.: Conceptualization; methodology; formal analysis; writing—original draft; writing—review and editing; and visualization. M.J.G.: Writing—original draft; writing—review and editing; and visualization. J.B.: Writing—review & editing. T.D.G.: Formal analysis; writing—original draft; writing—review & editing; and visualization. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hill, A.V., Grant, M.J., Blake, J. et al. Syndemics of complex risk factors in adolescents: findings from the youth risk behavior survey, 2021. npj Mental Health Res 5, 23 (2026). https://doi.org/10.1038/s44184-026-00203-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44184-026-00203-8
