
Abstract
This cross-sectional study investigated the relationship between dietary antioxidant indices and kidney function indicators in 240 outpatient adults with type 2 diabetes. Dietary intake was assessed using three 24-h dietary recalls. Dietary total antioxidant capacity (DTAC), dietary antioxidant index (DAI), and dietary antioxidant quality score (DAQS) were obtained. Indicators of kidney function, including serum creatinine, urea, blood urea nitrogen (BUN), and glomerular filtration rate (GFR), were extracted from medical records. After adjustment, the highest DAI tertile had lower serum creatinine (0.98 ± 0.27 vs 1.03 ± 0.32 mg/dL, P < 0.001), reduced urea (30.97 ± 8.75 vs 34.07 ± 14.45 mg/dL, P = 0.005), and higher GFR (85.16 ± 29.43 vs 74.16 ± 22.18 ml/min per 1·73 m2, P < 0.001) compared to the lowest tertile. The results of logistic regression analysis indicated a borderline significant inverse association of serum urea > 20 mg/dl with DTAC (odds ratio (OR):0.28; 95% CI: 0.07–1.09; Ptrend = 0.06). Multivariable linear regression analysis revealed a significant aligned correlation between DAQs and GFR (β: 0.20; P-value: 0.005) and a marginally significant direct relationship between DAI and GFR (β: 0.14; P-value: 0.06). However, no significant association was observed for DTAC with GFR (β:-0.02; P-value: 0.80). Diets with higher antioxidant capacity may be linked to improved kidney function in type 2 diabetes but our results did not support this strongly.
Similar content being viewed by others


Introduction
Diabetes-related kidney disease is one of the most frequent complications of type 2 diabetes, and is also the leading cause of chronic kidney disease (CKD) and end-stage renal disease (ESRD) worldwide1,2. Patients with diabetes face a higher risk of premature death, and having CKD further exacerbates this risk3,4. Therefore, early prevention and management of kidney failure in people with diabetes could significantly impact long-term morbidity and mortality5. Kamlesh Khunti's (2021) three-year prospective study highlighted the alarming prevalence of CKD among patients with type 2 diabetes, with findings indicating that nearly half (48.5%) of the 7,843 participants from 35 countries had stage 2 or higher CKD at baseline6. This underscores the broader global trend, as the World Health Organization (WHO) reported that diabetes was responsible for 460,000 kidney disease-related deaths in 2019. Complementing these findings, a 14-year cohort study by Seyyed Saeed Moazzeni et al. (2021) showed an annual CKD incidence rate exceeding 4% among the Iranian diabetic population7.
Oxidative stress plays a significant role in the pathogenesis and complications of type 2 diabetes8,9. Non-enzymatic protein glycation, oxidative protein breakdown, and glucose oxidation all contribute to the disproportionate formation of free radicals in diabetes, which can lead to increased renal complications10,11,12,13,14. Furthermore, oxidative stress exacerbates declining kidney function and becomes noticeably more severe in end-stage renal disease15. Dietary antioxidant consumption has been shown to gradually decrease kidney damage by reducing oxidative stress, inflammation, and cell apoptosis16,17.
Vegetables, fruits, nuts, cereals, beans spices, and herbs are natural sources of antioxidants in the diet. All these foods provide a range of antioxidants such as (vitamins: C , E, and carotenoids ; as well as some minerals: zinc, manganese, copper, and selenium ; and polyphenols) that have additional or synergistic effects18. Dietary antioxidant indices, such as dietary total antioxidant capacity (DTAC)19, dietary antioxidant quality score (DAQS)20, and dietary antioxidant index (DAI)21, have been validated as reliable tools for evaluating the total antioxidant capacity of the diet. Previous studies have revealed that higher DTAC is associated with improved kidney function in diabetic patients22,23. However, other studies have failed to find significant associations between DTAC and common biochemical indicators of renal function, such as albumin-to-creatinine ratio (ACR) and estimated glomerular filtration rate (eGFR)24,25. Moreover, the association between two other dietary antioxidant indices, DAQS and DAI, and kidney function in diabetes has been less extensively studied in previous research. Therefore, this cross-sectional study aims to investigate the associations between the dietary antioxidant indices DTAC, DAI, and DAQS and kidney function indicators, including serum urea, creatinine, BUN, and GFR, in adult patients with type 2 diabetes. By evaluating these associations, this study seeks to clarify the potential role of dietary antioxidants in the management and prevention of kidney dysfunction in individuals with type 2 diabetes. The findings may contribute to a better understanding of dietary interventions as a non-pharmacological approach to mitigating the progression of chronic kidney disease (CKD) in patients with type 2 diabetes. Ultimately, this research could provide valuable insights for developing dietary guidelines and public health strategies aimed at reducing the burden of CKD and improving the overall quality of life for individuals with type 2 diabetes.
Methods
Study design and participants
This cross-sectional study was conducted among 240 outpatients with Type 2 diabetes who were referred to the Diabetes Research Center, a part of the Endocrine and Metabolism Research Institute at Tehran University of Medical Sciences. The present study was conducted in accordance with the regulations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines26. The study took place from May 15, 2021, to October 5, 2021, and utilized convenience random sampling. Patients were classified as having Type 2 diabetes based on their medical history and self-reported information. In alignment with the American Diabetes Association (ADA) guidelines, the diagnosis of Type 2 diabetes was confirmed through one or more of the following criteria: a fasting plasma glucose level of ≥ 126 mg/dL (7.0 mmol/L), a 2-h plasma glucose level of ≥ 200 mg/dL (11.1 mmol/L) during an oral glucose tolerance test, or a glycated hemoglobin (HbA1c) level of ≥ 6.5%. CKD diagnosis was based on medical records, patient self-reports, and clinical criteria. Clinical criteria included persistent kidney function abnormalities, such as an eGFR below 60 mL/min/1.73 m2 for over three months or markers of kidney damage. This approach aligns with Kidney Disease Improving Global Outcomes (KDIGO) organization. The inclusion criteria encompassed individuals who met the following conditions: 1) a minimum of 2 years of Type 2 diabetes diagnosis, 2) an age range between 30 and 75 years, 3) possessing complete access to their medical records, and 4) having an HbA1c level below 9%. Conversely, the exclusion criteria comprised individuals who: 1) history of kidney disease 2) were pregnant or breastfeeding, 3) were undergoing estrogen hormone therapy, 4) had conditions such as mental disorders, autoimmune diseases, inflammatory diseases, thyroid disorders, gastrointestinal disorders, liver diseases, or cancer. Additionally, individuals with a daily energy intake below 800 or above 4200 kcal were deemed outliers, and their data was not subjected to analysis. All patients signed a consent form and this research received approval from the Research Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.EMRI.REC.1401.144), following the Helsinki Declaration.
Dietary intake assessment
The dietary intake of participants was recorded through the use of three 24-h dietary recalls, implemented on different days—consisting of one weekend day and two weekdays. These were collected via face-to-face interviews conducted by a proficient dietitian. Information on both micro and macronutrients was extracted using the Nutritionist IV software (N-Squared Computing, Version 4.0, Cincinnati, OH, USA).
Estimation of DTAC
Dietary total antioxidant capacity (DTAC) was assessed using the Ferric Reducing-Antioxidant Power (FRAP) values, which gauge the ability of dietary antioxidants to convert ferric ions to ferrous ions. These values were expressed in millimoles per 100 g of foods (mmol/100 g)27. The Antioxidant Food Table, compiled by Carlsen, provided the FRAP measurements, representing the ferric ion-reducing antioxidant potential, for over 3100 varieties of food and beverages28. To calculate DTAC for each participant, the daily consumption of individual food items was multiplied by the respective antioxidant potential, and these values were summed to obtain the overall dietary TAC27,29.
Estimation of DAQS
Dietary antioxidant quality score (DAQS) was derived from certain vitamins and minerals known for their antioxidant properties, including selenium, zinc, vitamin A, vitamin C, and vitamin E30. The intake of these antioxidant nutrients was obtained by assessing three 24-h dietary recalls. The assessment of dietary adequacy concerning these antioxidants involved a comparative analysis with Recommended Daily Intakes (RDI). The analysis included the calculation of the percentage of RDI intake as determined by the World Health Organization (WHO), as well as the proportion of individuals whose intake fell below the RDI, 2/3 of the RDI, and 1/3 of the RDI20. To estimate the risk of inadequate intake, the criterion employed was the proportion of individuals with intakes below 2/3 of the RDI31. Each of the five antioxidant nutrient intakes was individually evaluated, and a binary value (0 or 1) was assigned to each component. According to the methodology proposed by Tur et al.20, an intake lower than 2/3 of the RDI was denoted as 0, while an intake higher than 2/3 of the RDI was represented as 1. Consequently, the overall DAQS ranged from 0, indicating very poor dietary quality, to 5, signifying high dietary quality20.
Estimation of DAI
The dietary antioxidant index (DAI) score was calculated using the Wright method to evaluate the antioxidant capacity of the diet21. Initially, the average global consumption levels of specific components, including vitamin A, vitamin C, vitamin E, magnesium, selenium, and zinc, were subtracted from an individual's specific intake of these components. Subsequently, the result was standardized by dividing it by the global standard deviation (SD), as determined by the United States Department of Agriculture (USDA)32. Ultimately, the standardized values for these six components were combined to determine the comprehensive DAI score21,33.
Biochemical measurements
During the initial evaluation, we collected data on HbA1c, fasting blood glucose (FBG), creatinine, urea, and BUN serum levels, which were extracted from the medical records. These measurements were based on a complete blood count (CBC). These measurements were part of the routine laboratory tests conducted as standard care for patients with Type 2 diabetes at the diabetes center, and no additional tests were specifically performed for this study.
Calculating GFR
We employed the following formula to calculate the Glomerular Filtration Rate (GFR)27:
Assessment of other variables
Demographic information such as gender, age, family members, marital status, education level, occupation, smoking habits, dietary supplements, and medications was obtained through in-person interviews, and participants were also asked about their history of illnesses or medical history. Health professionals measured participants' weight using a digital scale with a precision of 100 g, ensuring that participants were barefoot and wearing light clothing. Subsequently, height was measured using a wall stadiometer with a precision of 0.1 cm. The Body Mass Index (BMI) was then calculated based on the ratio of weight in kilograms (kg) to the square of the height in meters (m2). The study assessed physical activity using the International Physical Activity Questionnaire—Short Form (IPAQ-SF), a globally recognized tool. Previous research in various countries has confirmed the validity and reliability of this tool for assessing physical activity34. Metabolic equivalent of task (MET) values were assigned to various activity categories, and participants' weekly MET minutes were calculated by multiplying activity duration by days per week, providing a total weekly physical activity measure.
Statistical analysis
Participants were stratified into groups according to tertiles of DTAC, DAI, and DAQS, with higher tertiles indicating greater antioxidant consumption in comparison to lower tertiles. Continuous variables were presented as mean values along with the standard deviation (SD), while categorical variables were expressed as numbers and percentages. To assess variations in both qualitative and quantitative variables among the tertiles of DTAC, DAI, and DAQS, the Chi-square test and analysis of variance (ANOVA) were employed, respectively. The nutrient intake of participants, adjusted for age, gender, and energy, was assessed across the tertiles of DIA. The data is expressed as mean values with their corresponding standard errors (SE), and the analysis was conducted using analysis of covariance (ANCOVA). Multivariable logistic regression analysis was employed to explore the relationship between serum creatinine, urea, BUN, and GFR and the dietary antioxidant indices (DTAC, DAI, and DAQS) in both crude and adjusted models. The initial model was adjusted for age, gender, and energy intake. The second model included additional control for the effects of medication and supplementation, physical activity, blood glucose, body mass index, smoking, and comorbidities, and the third model included the variables from Model II and additionally considered fat, protein, and fiber intakes. Odds ratios and 95% confidence interval were calculated using the first tertile of DTAC, DIA, and DAQS as the reference. In the multivariable logistic regression models, the tertiles of DTAC, DAI, and DAQS were treated as ordinal variables to assess the P-trend across these tertiles, and multiple linear regression analyses were used to estimate the association between dietary antioxidants indices and GFR. The analyses were conducted using SPSS version 26 (IBM Corp, Armonk, NY, USA). Statistical significance was determined for P-values below 0.05.
Results
Baseline characteristics
Table 1 presents the baseline characteristics of 240 individuals across tertiles of DTAC, DAI, and DAQS. The mean age was 59.55 ± 10.86 and the majority of the participants were males (59.8%), married (88.4%), and non-smokers (83.4%). Chronic kidney disease was detected only for 9.1% of subjects. No statistically significant differences were observed in terms of gender, marital status, education level, occupation, chronic kidney disease, smoking status, BMI, and physical activity across tertiles of DTAC, DAI, and DAQS.
Adjusted dietary intakes of participants across Tertiles of DAI
Age, gender, and energy-adjusted dietary intakes of participants across tertiles of DAI are demonstrated in Table 2. The results showed that individuals in the highest tertile of DAI had significantly higher intakes of energy, macronutrients (including carbohydrates, protein, fat, saturated fatty acids, and total dietary fiber), and micronutrients (including fat-soluble vitamins, vitamin C, B vitamins, iron, magnesium, zinc, and calcium) compared to those in the lowest tertile.
Biochemical characteristics of renal function across Tertiles of DAI
Following adjustment for confounder variables, individuals in the higher tertile of DAI demonstrated lower levels of serum creatinine (0.98 ± 0.27 vs 1.03 ± 0.32 mg/dL, p < 0.001), reduced urea concentrations (30.97 ± 8.75 vs 34.07 ± 14.45 mg/dL, p = 0.005) and a higher GFR (85.16 ± 29.43 vs 74.16 ± 22.18 ml/min per 1·73 m2, p < 0.001) (Table 3).
Logistic regression and Multivariable linear regression analysis regarding the association between dietary antioxidant indices and kidney function indicators
Logistic regression analysis was applied to estimate the relationship between DTAC, DAI, DAQS, and odds of kidney function decline (Table 4). No statistically significant association was detected between DTAC and the odds of high levels of renal markers in adults with type 2 diabetes. Nevertheless, following further adjustments in model III, the results indicated a marginally significant inverse association between DTAC and serum urea > 20 mg/dl (OR: 0.28; 95% CI: 0.07–1.04; P trend = 0.06).
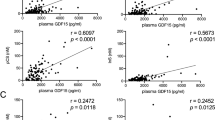
Moreover, upon accounting for confounding variables in model I, individuals in the highest DAI tertile exhibited higher glomerular filtration rates approaching statistical significance (OR: 2.34; 95% CI: 0.91–5.99; P trend = 0.06) compared to the lowest tertile. Nonetheless, DAQS was not associated with any kidney function markers in either the crude or adjusted models. Multivariable linear regression analyses examining the association between DTAC, DAI, DAQS, and GFR are depicted in Figs. 1–3. Notably, higher DAQS values were significantly correlated with improved GFR in patients with type 2 diabetes (β: 0.20; P = 0.005). Similarly, increased DAI values showed a marginally significant association with enhanced GFR (β: 0.14; P = 0.06). However, DTAC did not exhibit a significant association with GFR (β: -0.02; P = 0.80).

Please modify the title: Linear Regression of Observed Glomerular Filtration Rate (GFR) on Predicted GFR by Dietary Antioxidant Quality Score (DAQS).

Linear Regression of Observed Glomerular Filtration Rate (GFR) on Predicted GFR by Dietary Antioxidant Index (DAI).

Linear Regression of Observed Glomerular Filtration Rate (GFR) on Predicted GFR by Dietary Total Antioxidant Capacity (DTAC).
Discussion
In this study, we investigate the relationship between dietary antioxidant indices (namely DTAC, DAI, and DAQS) and kidney function indicators, including serum creatinine, urea, BUN, and GFR, in individuals with type 2 diabetes. The findings of multivariable logistic regression analysis revealed a marginally significant inverse association between DTAC and serum urea after adjusting for confounding variables. However, no significant relationships were observed between DAI and DAQS and the kidney function indicators after accounting for potential covariates.
Oxidative stress occurs when pro-oxidative mechanisms exceed the body's antioxidant defense, disrupting redox signaling and adaptation processes35. This condition is harmful as oxygen free radicals attack biological molecules, including lipids, proteins, and DNA. Oxidative stress is well-documented to contribute to the development of various lifestyle-related diseases, such as atherosclerosis, hypertension, diabetes mellitus, ischemic diseases, and malignancies36. Individuals with type 2 diabetes often have diets deficient in antioxidants, despite an increased demand for them37. There is strong experimental evidence supporting the role of oxidative stress in the development of kidney lesions in diabetes38. A diet rich in antioxidants, characterized by regular consumption of fish and vegetables, may be associated with improved kidney function indicators, such as decreased creatinine levels and increased eGFR, in individuals with type 2 diabetes39.
Historically, research has focused on the correlation between individual antioxidant nutrients or specific food categories, like fruits and vegetables, with health and disease. However, examining a single antioxidant or food group may not fully capture the synergistic effects and interactions of antioxidants in a whole diet25. The dietary antioxidant indices DTAC, DAI, and DAQS are methods used to assess the antioxidant potential of a diet25,40,41.
Our study's measurement of DTAC was based on a database created using the FARP assay. DTAC can serve as an indicator of dietary quality, as evidenced by its correlation with serum antioxidant levels in hemodialysis patients42,43. We observed a marginally significant association between DTAC and urea levels, a kidney function indicator, after controlling for confounding factors. Individuals in the highest tertile of DTAC had a lower risk of elevated serum urea levels compared to those in the lowest tertile. However, we did not find significant associations between DTAC and other kidney functions. Our findings align with Abbasi et al., who reported no significant association between DTAC and CKD in patients with type 2 diabetes, where CKD was defined as a GFR less than 60 mL/min/1.73 m2. Similarly, we found no significant association between DTAC and GFR38. In contrast, Asghari et al. suggested a link between DTAC and a decreased risk of developing CKD, defined by an estimated GFR below 60 mL/min/1.73 m244. Notably, Asghari et al. used the ORAC (oxygen radical absorbance capacity) method for evaluating DTAC, while our study, along with Abbasi's, employed the FRAP method. Ghorbaninejad et al. found no association between DTAC adherence and renal function, although their study examined different kidney function indicators, including ACR and eGFR, and used the ORAC method25. In contrast, Moludi et al. demonstrated that higher DTAC scores, determined through the FRAP method, were positively correlated with improved renal function, showing a positive correlation between DTAC and estimated GFR and an inverse relationship with creatinine levels. However, they found no significant association between DTAC and urea. Their study focused on the general population, whereas ours targeted patients with diabetes45.
Despite participants in the highest DAI and DAQS groups consuming diets abundant in antioxidants like vitamin E, vitamin C, vitamin D, magnesium, and zinc, our study revealed no significant association between higher tertiles of DAI and DAQS and kidney function indicators in individuals with type 2 diabetes. We initially observed a positive association between DAI and GFR in the crude analysis. However, this association disappeared after adjustment for confounding factors. Regarding DAQS, no significant relationships with kidney function indicators were observed in both crude and adjusted models. Our findings are consistent with Moradi et al., who found no correlation between adherence to the antioxidant-rich Mediterranean diet and renal function in individuals with Diabetic Nephropathy46. However, Farhadnejad et al. reported that higher consumption of various micronutrients, such as vitamins C, E, D, and magnesium, was linked to a reduced likelihood of developing CKD47. The disparity may be due to their assessment of individual antioxidants, whereas we considered the collective effects of multiple antioxidants The DTAC index, being a quantitative continuous variable, may provide a more robust estimation of overall dietary antioxidant status compared to the DAQS and DAI indices.
Chronic hyperglycemia in diabetes initiates pathological processes in the kidneys, leading to structural and functional changes that eventually result in ESRD. The overproduction of reactive oxygen species (ROS), a consequence of disrupted metabolic pathways, plays a pivotal role in this process. Oxidative stress, caused by increased pro-oxidant enzyme activity and antioxidant depletion, contributes to renal inflammation, fibrosis, and endothelial dysfunction. This cascade results in tissue damage, including lipid peroxidation, DNA damage, and mitochondrial dysfunction48. Numerous studies suggest that antioxidant consumption may diminish oxidative stress levels and slow the deterioration of glomerular function49,50.
The present study has some strengths and limitations. This study is the first to investigate the association between dietary antioxidant intake using three indices—DTAC, DAI, and DAQS— and four kidney function indicators, including serum urea, creatinine, BUN, and GFR, in patients with diabetes. Furthermore, we accounted for various confounding variables. However, the study has limitations including: 1) As a cross-sectional study, we could not examine causal relationships. 2) Despite using three models to control for confounders, residual confounding factors may persist. 3) The study did not explore the potential protective effects of antioxidant supplements and other bioactive compounds. 4) Serum antioxidant data was not accessible, and the evaluation of DTAC relied on 24-h dietary recalls, which introduces the possibility of inaccuracies in estimating the antioxidant capacity of the diet. Nonetheless, dietary TAC is recognized as a reliable indicator of plasma antioxidant status51. 5) In this study, we used a 24-h dietary questionnaire to evaluate oxidation. This method may not accurately reflect actual dietary intake, potentially leading to discrepancies in estimating the antioxidant capacity of the diet. However, it has been suggested that using three 24HRs may be optimal for estimating energy intake, which could help improve the accuracy of dietary assessments52.
Conclusion
In conclusion, adopting a high-antioxidant diet among individuals with diabetes appears to be associated with enhanced kidney function, but our results were inconclusive. A marginal inverse relationship was identified between DTAC and serum urea levels. Additionally, a positive association was initially observed between DAI and GFR, but this association lost significance after adjusting for confounding variables. Requiring the rigorous larger scale studies encompassing diverse ethnicities or distinctive populations, to fortify our findings' generalizability, is imperative. Furthermore, longitudinal investigations are warranted to validate and substantiate our observations longitudinally.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Change history
17 December 2024
A Correction to this paper has been published: https://doi.org/10.1038/s41598-024-81466-z
Abbreviations
- ACR:
-
Albumin to creatinine ratio
- ANCOVA:
-
Analysis of covariance
- ANOVA:
-
Analysis of variance
- BMI:
-
Body mass index
- BUN:
-
Blood urea nitrogen
- CBC:
-
Complete blood count
- CI:
-
Confidence interval
- CKD:
-
Chronic kidney disease
- DAI:
-
Dietary antioxidant index
- DAQS:
-
Dietary antioxidant quality score
- DTAC:
-
Dietary total antioxidant capacity
- eGFR:
-
Estimated glomerular filtration rate
- ESRD:
-
End-stage renal disease
- FBG:
-
Fasting blood glucose
- FRAP:
-
Ferric reducing-antioxidant power
- GFR:
-
Glomerular filtration rate
- IPAQ-SF:
-
International physical activity questionnaire-short form
- MET:
-
Metabolic equivalent of task
- OR:
-
Odds ratio
- ORAC:
-
Oxygen radical absorbance capacity
- RAE:
-
Retinol activity equivalents
- RDI:
-
Recommended daily intakes
- ROS:
-
Reactive oxygen species
- SD:
-
Standard deviation
- STROBE:
-
Strengthening the reporting of observational studies in epidemiology
- TAC:
-
Total antioxidant capacity
- USDA:
-
United States department of agriculture
- WHO:
-
World health organization
References
Doshi, S. M. & Friedman, A. N. Diagnosis and management of Type 2 diabetic kidney disease. Clin. J. Am. Soc. Nephrol 12(8), 1366–1373 (2017).
Koye, D. N. et al. The global epidemiology of diabetes and kidney disease. Adv. Chronic Kidney Dis. 25(2), 121–132 (2018).
Saran, R. et al. US renal data system 2016 annual data report: Epidemiology of kidney disease in the United States. Am. J. Kidney Dis. 69(3 Suppl 1), A7-a8 (2017).
Tonelli, M. et al. Chronic kidney disease and mortality risk: A systematic review. J. Am. Soc. Nephrol. 17(7), 2034–2047 (2006).
Hudson, K. B. & Sinert, R. Renal failure: Emergency evaluation and management. Emerg. Med. Clin. North Am. 29(3), 569–585 (2011).
Khunti, K. et al. Prevalence and progression of chronic kidney disease among patients with type 2 diabetes: Insights from the DISCOVER study. Diabetes Obes. Metab. 23(8), 1956–1960 (2021).
Moazzeni, S. S. et al. High incidence of chronic kidney disease among iranian diabetic adults: Using CKD-EPI and MDRD equations for estimated glomerular filtration rate. Diabetes Metab. J. 45(5), 684–697 (2021).
Newsholme, P. et al. Oxidative stress pathways in pancreatic β-cells and insulin-sensitive cells and tissues: Importance to cell metabolism, function, and dysfunction. Am. J. Physiol. Cell Physiol. 317(3), C420-c433 (2019).
Zhang, P. et al. Oxidative stress and diabetes: Antioxidative strategies. Front Med. 14(5), 583–600 (2020).
Aluksanasuwan, S. et al. High glucose induces phosphorylation and oxidation of mitochondrial proteins in renal tubular cells: A proteomics approach. Sci. Rep. 10(1), 5843 (2020).
Daenen, K. et al. Oxidative stress in chronic kidney disease. Pediatr. Nephrol. 34(6), 975–991 (2019).
Incalza, M. A. et al. Oxidative stress and reactive oxygen species in endothelial dysfunction associated with cardiovascular and metabolic diseases. Vascul. Pharmacol. 100, 1–19 (2018).
Kanwar, Y. S. et al. A glimpse of various Pathogenetic mechanisms of diabetic nephropathy. Annu. Rev. Pathol. 6, 395–423 (2011).
Rodiño-Janeiro, B. K. et al. Glycated albumin, a precursor of advanced glycation end-products, up-regulates NADPH oxidase and enhances oxidative stress in human endothelial cells: Molecular correlate of diabetic vasculopathy. Diabetes Metab. Res. Rev. 26(7), 550–558 (2010).
Ho, H. J. & Shirakawa, H. Oxidative Stress and Mitochondrial Dysfunction in Chronic Kidney Disease. Cells https://doi.org/10.3390/cells12010088 (2022).
Darenskaya, M. et al. Diabetic Nephropathy: Significance of Determining Oxidative Stress and Opportunities for Antioxidant Therapies. Int. J. Mol. Sci. https://doi.org/10.3390/ijms241512378 (2023).
Østergaard, J. A., Cooper, M. E. & Jandeleit-Dahm, K. A. M. Targeting oxidative stress and anti-oxidant defence in diabetic kidney disease. J Nephrol 33(5), 917–929 (2020).
Chen, X. et al. The synergistic and antagonistic antioxidant interactions of dietary phytochemical combinations. Crit. Rev. Food Sci. Nutr. 62(20), 5658–5677 (2022).
Puchau, B. et al. Dietary total antioxidant capacity: A novel indicator of diet quality in healthy young adults. J Am. Coll. Nutr. 28(6), 648–656 (2009).
Tur, J. A. et al. Does the diet of the Balearic population, a Mediterranean type diet, still provide adequate antioxidant nutrient intakes?. Eur. J. Nutr. 44(4), 204–213 (2005).
Wright, M. E. et al. Development of a comprehensive dietary antioxidant index and application to lung cancer risk in a cohort of male smokers. Am. J. Epidemiol. 160(1), 68–76 (2004).
Li, Y. et al. Association of dietary total antioxidant capacity with all-cause and cardiovascular mortality in patients with chronic kidney disease: Based on two retrospective cohort studies of NHANES. Ren. Fail. 45(1), 2205950 (2023).
Moludi, J. et al. Dietary total antioxidant capacity and its association with renal function and kidney stones: Results of a RaNCD cohort study. Food Sci. Nutr. 10(5), 1442–1450 (2022).
Abbasi, M. et al. Dietary total antioxidant capacity and the risk of chronic kidney disease in patients with type 2 diabetes: A nested case-control study in the tehran lipid glucose study. J. Ren. Nutr. 29(5), 394–398 (2019).
Ghorbaninejad, P. et al. Dietary total antioxidant capacity and its association with renal function and progression of chronic kidney disease in older adults: A report from a developing country. Clin. Nutr. Res. 9(4), 296–306 (2020).
Von Elm, E., et al., The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. (2007).
A Milajerdi et al. Dietary total antioxidant capacity in relation to depression and anxiety in Iranian adults. 65 85 90, (2019).
Carlsen, M., et al., Additional file 1: the antioxidant food table. (2010).
Nouri, M. et al. Dietary Antioxidant Capacity Indices are Negatively Correlated to LDL-Oxidation in Adults. Int. J. Clin. https://doi.org/10.1155/2023/5446163 (2023).
Nikrad, N. et al. Dietary Antioxidant Quality Score (DAQS), serum lipids, markers of glucose homeostasis, blood pressure and anthropometric features among apparently metabolically healthy obese adults in two metropolises of Iran (Tabriz and Tehran): a cross-sectional study. BMC Endocr. Disord. 23(1), 157 (2023).
Aranceta, J. et al. Vitamins in Spanish food patterns: the eVe Study. Public Health Nutr. 4(6a), 1317–1323 (2001).
U.S. Department of Agriculture, Agricultural Research Service. 2020. Nutrient Intakes from Food and Beverages: Mean Amounts Consumed per Individual, by Gender and Age, What We Eat in America, NHANES (2017–2018).
Aminnejad, B. et al. Association of dietary antioxidant index with body mass index in adolescents. Obes. Sci. Pract. 9(1), 15–22 (2023).
Booth, M.J.R.q.f.e. and sport, Assessment of physical activity: an international perspective. Res. Q. Excer Sport https://doi.org/10.1080/02701367.2000.11082794, (2000).
Ji, L. L. & Yeo, D. Oxidative stress: an evolving definition. Fac. Rev. https://doi.org/10.12703/r/10-13 (2021).
Yoshikawa, T. and Y.J.J.m.a.j. Naito, What is oxidative stress? (2002).
Zujko, M. E. et al. Reduced intake of dietary antioxidants can impair antioxidant status in type 2 diabetes patients. Polish Arch. Int. Med. https://doi.org/10.20452/pamw.2497 (2014).
Abbasi, M. et al. Dietary total antioxidant capacity and the risk of chronic kidney disease in patients with type 2 diabetes: a nested case-control study in the Tehran Lipid Glucose Study. J. Renal Nutr. https://doi.org/10.1053/j.jrn.2018.11.008 (2019).
Hsu, C.-C. et al. Associations between dietary patterns and kidney function indicators in type 2 diabetes. Clin. Nutr. 33(1), 98–105 (2014).
Shahinfar, H. et al. The association between dietary antioxidant quality score and cardiorespiratory fitness in Iranian adults: a cross-sectional study. Clin. Nutr. Res. 9(3), 171 (2020).
Wang, M. et al. Association between the composite dietary antioxidant index and chronic kidney disease: evidence from NHANES 2011–2018. Foods Funct. https://doi.org/10.1039/D3FO01157G (2023).
Ozkalayci, R.E.; Coban, S.; Rakicioglu, N. The Relationship between Dietary Total Antioxidant Capacity with Serum Antioxidant and Oxidant Parameters in Hemodialysis Patients. Turk. J. Nephrol. 2021, 30, 300–307.
Salari-Moghaddam, A. et al. Association between dietary total antioxidant capacity and diet quality in adults. Front. Nutr. 9, 838752 (2022).
Asghari, G. et al. Dietary total antioxidant capacity and incidence of chronic kidney disease in subjects with dysglycemia: Tehran Lipid and Glucose Study. Eur. J. Nutr. 57, 2377–2385 (2018).
Moludi, J. et al. Dietary total antioxidant capacity and its association with renal function and kidney stones: Results of a RaNCD cohort study. Foof Sci Nutr. 10(5), 1442–1450 (2022).
Moradi, M. et al. Association between adherence to the Mediterranean diet and renal function biomarkers and cardiovascular risk factors among diabetic patients with nephropathy. Clin. Nutr. ESPEN 40, 156–163 (2020).
Farhadnejad, H. et al. Micronutrient intakes and incidence of chronic kidney disease in adults: Tehran lipid and glucose study. Nutrients 8(4), 217 (2016).
Jha JC, Banal C, Chow BS, Cooper ME, Jandeleit-Dahm K. Diabetes and Kidney Disease: Role of Oxidative Stress. Antioxid Redox Signal. 2016 Oct 20;25(12):657-684. doi: 10.1089/ars.2016.6664. Epub 2016 Apr 1. PMID: 26906673; PMCID: PMC5069735.
Neri, S. et al. Effects of antioxidants on postprandial oxidative stress and endothelial dysfunction in subjects with impaired glucose tolerance and type 2 diabetes. Eur. J. Nutr. 49, 409–416 (2010).
Farvid, M. S. et al. Comparison of the effects of vitamins and/or mineral supplementation on glomerular and tubular dysfunction in type 2 diabetes. Diabetes Care 28(10), 2458–2464 (2005).
Wang Y, Yang M, Lee SG, Davis CG, Koo SI, Chun OK. Dietary total antioxidant capacity is associated with diet and plasma antioxidant status in healthy young adults. J Acad Nutr Diet. 2012 Oct;112(10):1626-35. doi: 10.1016/j.jand.2012.06.007. PMID: 23017573.
Ma, Y. et al. Number of 24-hour diet recalls needed to estimate energy intake. Annal. Epidemiol. 19(8), 553–559 (2009).
Author information
Authors and Affiliations
Contributions
MM and LA and EN designed the study and contributed to data collection. NO and RT imported the data for analysis, conducted the statistical analysis, and drafted the main manuscript text. LA supervised the study. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical statement
All participant signed an informed consent form.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained errors in Tables 1-4, where the Dietary Adequacy Index (DAI) ranges in the headings were incorrect.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Omid, N., Esfahani, E.N., Tabaeifard, R. et al. Association of dietary antioxidant indices with kidney function indicators in patients with type 2 diabetes: a cross-sectional study. Sci Rep 14, 22991 (2024). https://doi.org/10.1038/s41598-024-71683-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-71683-x
