
Abstract
Low back pain (LBP) is a global issue involving biological, psychological, and social factors. Pain-related fear has been shown to influence movement behavior, however, its association with some measures of movement behavior, such as spinal movement variability, remains inconclusive. To further investigate this, spinal kinematics during various activities of daily living (i.e., walking, running, lifting, and stair climbing) of 49 patients with chronic LBP and a group of 51 sex-, age-, and BMI-matched healthy controls were used to calculate lumbar spine movement variability which was quantified using different indices (i.e., coefficient of variation, coupling angle variability in vector coding, deviation phase of the continuous relative phase and an angle-angular velocity variability). General and task-specific pain-related fear was assessed using the Tampa Scale of Kinesiophobia and the Photograph Series of Daily Activities—Short Electronic Version, respectively. Linear regression analyses showed no significant association between movement variability and pain-related fear, however, the sample consisted of younger individuals with moderate disability and with low levels of pain and pain-related fear. In addition, the different variability indices were weakly correlated and varied greatly depending on the method used and the task performed. Therefore, comparisons between studies with different movement variability calculation methods or different activities should be treated with caution.
Similar content being viewed by others


Introduction
Low back pain (LBP) is a common problem and has been the cause of most years lived with disability since 19901. It is defined as pain between the lower ribs and the gluteal sulcus2. In most cases, LBP is not caused by damage to a specific structure, and is therefore referred to as non-specific LBP, described as “a complex condition with multiple contributors to both the pain and associated disability, including psychological factors, social factors, biophysical factors, comorbidities, and central pain-processing mechanisms”3. A commonly known psychological factor that has been shown to be associated with LBP is pain-related fear, driven by fear-avoidance beliefs4. In recent systematic reviews, fear-avoidance beliefs have been associated with longer recovery time and risk of chronicity in subacute LBP5, and higher pain-related fear was associated with more rigid spine movement in patients with LBP6. However, examinations of the correlation between pain-related fear and spinal kinematics often revealed small effect sizes necessitating the incorporation of more nuanced indices of psychological determinants and spinal motor activity in subsequent investigations6,7. It is imperative that future research endeavors adopt a more granular approach by integrating e.g. assessments of task-specific rather than only general pain-related fear8. Additionally, the evaluation of spinal movement variability (SMV) should be considered as a potentially significant metric for spinal motor behavior9.
With respect to SMV, a certain degree of movement variability is crucial for maintaining optimal movement, whereas altered levels of movement variability might be associated with LBP9. However, studies examining SMV in individuals with LBP have produced conflicting findings, with some reporting heightened SMV and others reduced SMV compared with healthy controls9,10. This could be due to the presence of possible motor control subgroups (e.g., loose and tight control)11, differences in pain duration (e.g., acute or chronic), or psychological factors such as pain-related fear9. Given the absence of a standardized method for measuring SMV, various approaches are utilized, each of which could significantly influence the outcomes9,12,13,14. Regarding the association between pain-related fear and SMV in patients with LBP, a scant total of three experimental investigations have been documented15,16,17. While one study suggested that task-specific pain-related fear is inversely associated with movement coordination during lifting16, another study observed no association between pain-related fear and SMV during gait in patients with LBP15. The third study reported an interaction effect between the group (healthy controls, mixed acute and chronic LBP) and task-specific pain-related cognitions on variability during repetitive seated reaching, indicating that patients with LBP with high levels of pain-related fear had larger SMV17. There is some evidence, that pain-related fear is associated with reduced spinal movement even in healthy subjects18. Synthesizing these outcomes into a unified narrative proves challenging, given the disparate activities examined, the variation in SMV metrics employed, the differentiation between general versus task-specific measures of pain-related fear, and the absence of a control group for comparative analysis15.
This study aims to examine associations between pain-related fear and SMV in individuals with chronic LBP as well as in healthy participants for comparison, using various activities such as walking, running, object lifting, and stair climbing, alongside a spectrum of variability indices and both task-specific and general measures of pain-related fear for a comprehensive overview19. Based on previous studies6,15,16,17, we hypothesized that a significant negative relationship exists between task-specific (as opposed to general) pain-related fear and the variability of lumbar movement across the aforementioned activities, with this association anticipated to be more pronounced in patients with LBP compared to their healthy counterparts. Moreover, the strength of this relationship may vary depending on the specific demands of each activity.
Methods
Participants
This cross-sectional analysis was conducted as part of a larger study focusing on potential associations between cortical mechanisms and spine biomechanics in individuals with and without chronic LBP. Healthy individuals and patients with chronic LBP, aged between 18 and 50 years, without a history of vestibular disorders, obesity (body mass index [BMI] > 30 kg/m2), or known current pregnancy were recruited. Healthy individuals were included if they had no musculoskeletal pain within the past three months and had no history of chronic pain, no history of psychiatric or neurological disorders and no prior spine surgery. Patients with chronic LBP were included if they reported pain in the lower back region for more than three months but were excluded if they had a suspected or confirmed spinal pathology (e.g., tumor, infection, fracture, inflammatory disease, or nerve root compression), previous or scheduled spine surgery, neuromuscular diseases that affect gait and posture, or injuries to the movement system with permanent deformations.
A total of 112 healthy individuals and 58 patients with chronic LBP were recruited and completed all the assessments, as described below. To ensure comparability between the two groups, we excluded nine patients with LBP who were considerably older than any of the healthy individuals and performed proportional stratified random sampling according to sex, age, and BMI. This resulted in a final dataset of 51 healthy individuals and 49 LBP patients (Table 1).
The study protocol was approved by the ethics committee of the canton of Zurich, Switzerland (EK-01/2019/PB_2018_01001), and the study was performed in accordance with the Declaration of Helsinki and guidelines for Good Clinical Practice. After receiving written informed consent from each participant, all assessments for the current analysis were conducted during a single appointment at the Balgrist University Hospital in Zurich, Switzerland.
Data collection
Pain-related fear
General pain-related fear was assessed using a modified German version of the Tampa Scale for Kinesiophobia (TSK) for the general population, which consisted of 17 questions about the participants’ feelings, beliefs, and fear of pain and movement20,21. Each question was answered on a Likert scale ranging from 1 to 4 (strongly disagree, somewhat disagree, somewhat agree, strongly agree). A maximum total score of 68 points signifies severe pain-related fear, whereas a minimum of 17 points indicates no pain-related fear21. The internal consistency of the TSK total score was reported to be sufficient for both healthy individuals and patients with LBP (Cronbach’s alpha: 0.78 and 0.79, respectively)21.
Task-specific pain-related fear was assessed using the Photographic Series of Daily Activities—Short Electronic Version (PHODA-SeV), which has shown a high internal consistency (Cronbach’s alpha 0.98 for total score)22. The study participants rated their perceived harmfulness of the back for 40 photographs of activities of daily living on a visual scale from 0 (not harmful) to 100 (extremely harmful)22. For the current analysis, the TSK total score and the scores of the following single PHODA-SeV items were used: lifting a flowerpot with bent back (PHODA-lift), walking up the stairs (PHODA-upstairs), walking down the stairs (PHODA-downstairs), running (PHODA-run), and walking on level ground (PHODA-walk).
Spinal kinematics
All participants were equipped with 58 reflective markers according to a previously described configuration23. For a detailed representation of the spine, this configuration included markers placed on the most posterior tips of the spinous processes of the vertebrae C7, T3, T5, T7, T9, T11, L1-L5, and the sacrum at the height of S2.
The participants were then asked to stand and sit for approximately 10 s, to once maximally bend the spine forward and backward with minimal or no knee flexion, and to perform five repetitions of each of the following activities of daily living: walking and running, ascending and descending stairs, standing up and sitting down on a chair, and lifting and lowering a box. For the walking and running activities, participants were asked to walk or run along a 10-meter level-ground walkway without specific guidance on technique. The stair ascent and descent were performed on a custom-built four-step metal staircase with a riser height of 17.5 cm, a tread depth of 30 cm. Participants were instructed to navigate the stairs without using the handrails. Chair rising involved a round, backless chair with a fixed seat height of 46 cm. Participants were asked to stand up and sit down using their arms freely (i.e., no arm support, but arm swinging was allowed)24. For the lifting and lowering activities, participants lifted and lowered a 5 kg-box (40 × 30 × 17 cm) using a freestyle technique (i.e., intuitively, without any specific instructions), with the feet kept parallel about hip-wide apart and the box being initially placed 15 cm in front of their toes18. The activities were performed in a fixed order at a self-selected normal speed. One repetition of each activity was defined as: walking/running once along the walkway, walking up and immediately back down the stairs, standing up and sitting immediately back down on the chair, as well as grabbing the box from a standing position, lifting it up, putting it down, and standing back up without the box. Between each repetition, participants were allowed to pause quickly before performing the next repetition. Before data collection with a three-dimensional 27-camera optical motion capture system (Vicon UK; Oxford, United Kingdom), participants were allowed to practice each activity.
For the current analysis, only the data from activities corresponding to PHODA items (i.e., walking, running, walking upstairs and downstairs, and lifting) were considered.
Processing of kinematic data
In a first step, kinematic data were pre-processed using the software Nexus 2 (Vicon UK, Oxford, United Kingdom), which included marker reconstruction and labeling, gap filling, filtering of the trajectories, and the setting of temporal events to identify the data sections containing the relevant parts of the movements. For each repetition of the walking, running, and stair activities, a single left gait cycle was identified using the automated gait cycle event detection function in Nexus, with manual adjustments made if an event was incorrectly identified. For the lifting and lowering activities, the start of the lifting and the end of the lowering phase were manually identified in Nexus (i.e., the instants where the box was lifted off and placed on the ground, respectively). The end of the lifting and start of the lower phases were automatically determined using a custom MATLAB-based event detection algorithm. This algorithm identified the instant when the C7 marker moved cranially and posteriorly within 20 mm (lifting phase) or caudally or anteriorly by more than 20 mm from its position during upright standing (lowering phase). In a second step, the following angles were calculated for each of the included activities/phases over time (i.e., continuous): (1) sagittal and frontal plane curvature and transverse plane axial rotation angles of the lumbar spine (used for the calculation of the variability indices CV and AAVV, see below), and (2) sagittal, frontal, and transverse plane angles of a rigid pelvis and thorax segment with respect to the laboratory coordinate system (global angles; used for the calculation of the variability indices CAV and DP, see below). To calculate the curvature angles of the lumbar spine, we used a custom MATLAB routine (R2022a, MathWorks, Inc., Natick, MA) that applied a combination of a quadratic polynomial and a circle fit function to the sagittal and frontal plane trajectories of the markers placed on L1, L2, L3, L4, L5 and the sacrum (at the height of S2)25. Axial rotation angles were also calculated with the custom MATLAB routine as the relative angles between the intersecting lines of marker pairs placed laterally of the spine at the height of the costal arch (upper line) and on the posterior superior iliac spines (lower line)26. Global angles of the pelvis and thorax segments were calculated based on the “Plug-in Gait full body model” in Nexus27, where the pelvis segment was defined by the markers placed on the anterior and posterior superior iliac spines, and the thorax segment by markers on the lower and upper parts of the sternum as well as on C7, T10 (in this study placed on T11) and the right scapula. In a third step, velocities of all angles over time were determined by calculating their derivatives. Finally, all continuous angle (expressed in degrees [°]) and velocitie data (expressed in degrees/s [°/s]) were time-normalized to 101 data points.
Calculation of movement variability
There is no consensus on the most appropriate way to quantify spinal movement variability (SMV), with many different techniques being described in the literature9,12,13,14. Because the movements performed in the current study are not cyclical and are only repeated five times, most non-linear approaches are not applicable28. Instead, the following variability measures were chosen: (1) coefficient of variation, (2) angle-angular velocity variability, (3) vector coding coupling angle variability, and (4) continuous relative phase—deviation phase. These measures are suitable for the current data and quantify “within subject-between trial” variability as an index of how variable the individuals moved among the five repetitions, but cover different aspects of movement variability. The coefficient of variation provides a normalized measure of dispersion relative to the mean, highlighting overall movement consistency29. Angle-angular velocity variability assesses the relationship between joint angles and their corresponding velocities30. Vector coding coupling angle variability and continuous relative phase evaluate segmental coordination by analyzing the variability in coupling angles and the interaction between segments. All indices were calculated for sagittal, frontal, and transverse plane movements, except for object lifting, for which only sagittal movement was considered, because significant movements are not expected to occur in these planes during lifting tasks.
Coefficient of variation (CV)
The CV can be identified for time-series data and was calculated according to Eq. (1)29. For input, standard deviation (σi) and mean (\(\mu\)i) of the continuous lumbar curvature angles were used.
We calculated the CV for each subject and each activity as a discrete measure of variability and expressed it in percentage, where a higher value indicates a higher SMV29. An example of two subjects with different movement patterns is shown in Fig. 1. A CV of 40% is comparatively high and indicates that the curvature angle values during the lifting movement are more variable. With lower CV values (e.g., 5–10%), there is greater consistency of the values around the mean.

Lumbar curvature angles of five time-normalized lifting trials including plot of mean and standard deviation of the 5 trials. (a): Subject with a variable movement pattern across trials resulting in a coefficient of variation (CV) of 40%. (b): Subject with similar movement patterns across trials and a coefficient of variation of 8.6%.
Angle–angular velocity variability (AAVV)
To determine the AAVV, continuous angles of the lumbar curvature (\({\varphi}_{i}\)) were plotted against continuous angular velocities (\({\omega}_{i}\)) (Fig. 2a). For comparability, the curvature angles and angular velocities were normalized to a range from − 1 to 1 according to Eq. (2)12 and (3)30. To maintain the original variability of the data to a greater extent than normalizing individual trials, the minimum and maximum (\({\varphi}_{min/max}\) and \({\omega}_{min/max}\), respectively) of the values of all repetitions of a participant were considered.
We then calculated the vector length (\({r}_{i}\)) at each point of the time-normalized movement cycle according to Eq. (4)30 (Fig. 2b).
Standard deviation of the vector length \({r}_{i}\) over the five trials at each time point was a continuous measure of variability for each subject and activity30 (Fig. 2c). For statistical analyses, the mean of the continuous standard deviation per subject and activity was calculated.

Angle-angular velocity variability calculation of the lifting activity of one participant. (a): Lumbar curvature angles in degrees plotted against lumbar angular velocity in degrees/second for five trials. (b): Movement curve of the five trials with normalized range (− 1,1) and an example of vector ri at timepoint 80. (c): Continuous movement variability during lifting activity which is calculated as standard deviation (sd) of vector ri between the 5 trials at every point of the time-normalized movement cycle.
Vector coding coupling angle variability (CAV)
Vector coding is a method used to assess the variability of the coordination between two segments, whereas the coupling angle is the angle of the vector between two consecutive data points on an angle-angle-plot to the right horizontal axis (Fig. 3)12,31.

Coupling angle calculation in one subject during lifting. Angles of the thorax are plotted against angles of the pelvis. A coupling angle \(\gamma{i}\) is the angle between the right horizontal line and the vector between two consecutive points in the movement cycle (pi and pi + 1) of the 101 time-normalized points.
Coupling angles (\({\gamma}_{i}\)) between global thoracic (\({x}_{i}\)) and pelvic (\({y}_{i}\)) angles in one plane were calculated using the arctangent function described in Eq. (5)12,31,32.
To obtain an angular representation of all four-quadrants and values from − 180° to 180°, we applied the general conditions (6) for a four-quadrant inverse tangent to Eq. (5)32.
Condition (7) was applied to correct the angles to a value between 0° and 360°.
Coupling angle variability (\({CAV}_{i}\)) is defined as the angular deviation of the coupling angles at timepoint i32. Angular deviation in circular statistics is analogous to the standard deviation in linear statistics and must be applied because of the directional nature of coupling angles33. From the coupling angles (\({\gamma}_{i}\)) across n trials, the average horizontal (\(\overline{x}\)) and vertical (\(\overline{y}\)) components at each time point were determined using Eqs. (8) and (9) in order to calculate \(r\), a measure of angular dispersion, according to Eq. (10)12.
\(r\) was then inserted into the formula for angular deviation (11), which included a conversion to degrees to determine the continuous coupling angle variability (\({CAV}_{i}\)) across the five repetitions32,33.
For statistical analyses, the circular mean of \({CAV}_{i}\) (\(\overline{CAV}\)) was calculated according to Eq. (12)33 with the conditions (6) being applied to represent all four quadrants and values in degrees.
To correct \(\overline{CAV}\) values to a range from 0° to 360°, condition (13) was applied.
Continuous relative phase—deviation phase (DP)
The continuous relative phase (CRP) was originally developed to analyze inter-joint coordination of the limb34. It was later used to determine coordination variability based on CRP35 and has since been applied to assess spinal movement36,37,38. Lamb and Stöckl39 defined a new standard of the CRP and their proposed method was used in the current study: After centering the kinematic data \(\:{\alpha}_{i}\) around zero according to (14), Hilbert transformation was performed using the MATLAB function hilbert (Signal Processing Toolbox, MathWorks, Inc, Natick, MA) to get a complex, analytic signal of the centered data, consisting of the real part \({H}_{real\left(i\right)}={\alpha}_{centered\left(i\right)}\) and an imaginary part \({H}_{imag\left(i\right)}\). The use of the Hilbert transformation to calculate phase angles is recommended for human, non-sinusoidal movement data instead of the original technique with phase plane construction35,39.
Phase angles \({\phi}_{i}\) for thoracic and pelvic movement were calculated according to (15)39.
An example of segment and phase angles of one subject are presented in Fig. 4a/b.
To obtain the CRP, the absolute difference between the phase angles of the pelvis and thorax was taken (16) and corrected to a 0–180° scale (17), since values of 0° and 360° both represent an in-phase movement39.
The deviation phase curve is a measure of variability, which is the continuous standard deviation of the CRP curves of several trials (Fig. 4c). Deviation phase (DP) is calculated by averaging the deviation phase curve. A higher DP value indicates a more variable relationship between the thoracic and pelvic segments during the analyzed movement36,40.

Continuous relative phase and deviation phase calculation. (a): Angles of pelvis and thorax in sagittal plane during lifting cycle of one subject. (b): Phase angles of thorax and pelvis during lifting cycle of the same trial. (c): Continuous relative phase (CRP) curves of all lifting trials of one subject and continuous deviation phase (standard deviation of all CRP curves of one subject).
Statistical analysis
Descriptive statistics were calculated for each variable using R-based open-source software jamovi (version 2.3.; jamovi project, Sydney, Australia). Independent samples t-tests were used to test for between-group differences of demographic and questionnaire data. The variability indices were assessed for normality using the Shapiro-Wilk test. The results indicated that more than half of the indices did not conform to a normal distribution. Therefore, for each activity, the Spearman’s rank correlation matrix of the variability indices was calculated. Furthermore, for every variability measure, hierarchical multiple linear regression analysis was performed using jamovi. Analyzing five different activities with four different variability indices in each plane resulted in 52 linear regressions. The variability measure was used as the dependent variable, and the process of hierarchical model building for the independent variables was as follows: In the first block, all nuisance and demographic variables that might influence movement variability were added (age, BMI, sex, group; model 1)9,16,41. In the second block, the TSK score was added as a measure of general pain-related fear (model 2). In the last block, the PHODA item and the interaction between the group and PHODA item were added to obtain the overall model (model 3). The TSK was added prior to the PHODA item in a separate step to test whether task-specific pain-related fear added additional explained variance and to exclude potential confounding effects of general pain-related fear. The change in R² (∆R2) was calculated between models to assess whether task-specific pain-related fear and the interaction terms explained unique variance in movement variability.
Statistical significance was assessed using F-tests, with the alpha level set to 0.05. To address the probability of false-positive results due to multiple testing, the p-values of the overall models (model 3) were adjusted using the Benjamini-Hochberg procedure in R (version 4.2.2, R Core Team, Vienna, Austria)42,43. This adjustment to control for the false discovery rate was applied across the entire set of 52 models collectively. The effect of adding blocks 2 and 3 was assessed using F-tests comparing models 1 to 3. Prerequisites for linear regression were checked in jamovi with the Shapiro-Wilk test and visual inspection of the Q-Q-plot for normality of the error and for homoscedasticity with visual examination of the residual plot. The presence of influential cases and outliers was checked using Cook distance and visual inspection of the results. Correlations between the different predictors were assessed by collinearity statistics (variance inflation factor and tolerance) using jamovi. If non-normality of the error or heteroscedasticity occurred, the robustness of the analysis was checked using a bootstrap residual sampling procedure44 performed with R and the R-package boot45. The advantage of this method is that no data transformation is required, but the validity of the model can be checked with modified residuals and changing samples (5000 repetitions were used)44. The confidence interval of the regression coefficients obtained by the bootstrapping procedure was compared with the original results, and normality was re-examined by visual Q-Q-plot inspection.
Results
Demographics and group comparisons
Following stratified random sampling, the participant demographics did not differ significantly between the two groups (Table 1). The patients with LBP reported moderate disability (Oswestry Disbility Index 29.39 ± 7.81) and a mean level of pain of 2.18 ± 1.48 on a visual analog scale. Comparisons of the questionnaire data revealed that some scores for task-specific pain related fear (PHODA-SEV total, PHODA-walk, PHODA-run, PHODA-downstairs, PHODA-upstairs) were significantly higher in patients with LBP, whereas no differences between the groups were found for PHODA-lift or TSK (Table 1).
Variability measures and correlations
A descriptive summary of the results of the variability calculations can be found in the Supplementary Table S1. Spearman rank correlation matrices are shown in Supplementary Tables S2–S6. For lifting, most of the variability measures were correlated, except for CV and DP. For all other activities, the variability measures showed mostly weak or no correlations with each other, whether within one plane or between different planes.
Linear regression analysis
In terms of prerequisites for linear regression analysis, no collinearity of the independent variables and influential cases were detected. In 26 of the 52 models, the assumption of normality of the error was violated, and heteroscedasticity of the residuals was observed in 14 models. Examination of the confidence interval after the bootstrap residual sampling procedure showed no difference from the original result, and the Q-Q-plot became normally distributed, which is why the original linear models were used. The results of the overall hierarchical multiple linear regression model fits are presented in Table 2. After p-value correction with the false discovery rate, only six of the 52 models were statistically significant (p < 0.05).
The linear regression models for all four variability measures for walking upstairs in the frontal plane remained statistically significant after p-value correction. 15% of the variation in CV, 26% of the variation in AAVV and CAV, and 35% of the variation in DP were explained by the set of independent variables. The regressor CAV for the transverse plane movements during walking upstairs showed an adjusted R2 of 0.133, whereas AAVV for the frontal plane movements during walking downstairs showed an adjusted R2 of 0.192. Table 3 provides an overview of the various impacts of the different independent variables in the six statistically significant regression models. In all six models, the independent variable sex had a statistically significant impact, with females demonstrating higher variability values than males (see Supplementary Fig. 1).
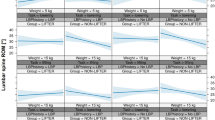
For the CV of the frontal plane movements during walking upstairs, a PHODA-upstairs x group interaction was detected (p = 0.031). The marginal effects of the interaction are shown in Fig. 5. In patients with LBP, a positive correlation between the PHODA-upstairs and CV in the frontal plane was observed, whereas for healthy controls, the observed pattern showed an inverse association.

Marginal effects for PHODA-upstairs x group interaction. Significant interaction effect between PHODA-upstairs and the group (p = 0.031) in the linear regression model for Coefficient of variation (CV) in walking upstairs in frontal plane. Predicted values are illustrated with consideration for random effects.
For AAVV of the frontal plane movements during walking downstairs, patients showed a significantly highervariability than healthy controls (p = 0.008). Neither general nor task-specific pain-related fear measures showed a statistically significant association with any of the variability parameters.
All statistically non-significant regression models (model 3) are shown in Supplementary Table S7. The single models (models 1 and 2) of the hierarchical regression models and the between-model comparisons (models 1 and 2, models 2 and 3) were not analyzed in more detail because only in three models there was a significant improvement between model 2 and 3. The overall model for the CV of the frontal plane movements during walking upstairs was the only overall significant model which improved statistically significantly (p = 0.007) by adding variables for task-specific pain-related fear (∆R2 = 0.089).
Discussion
This study aimed to comprehensively investigate the association between pain-related fear and SMV. Overall and irrespective of activity and SMV measure, the variance in SMV could not be explained by pain-related fear, neither general nor task-specific. An exception was the CV in the frontal plane during walking upstairs, where a significant PHODA-upstairs × group interaction was found. Among patients with LBP, variability increased with higher task-specific fear. Conversely, among healthy individuals, the opposite trend was observed: increased fear was linked to reduced variability. This is contradictory to our expectation of a negative association in both groups, which was hypothesized to be stronger in LBP patients compared to healthy controls, as higher fear could lead to more cautious movement. But the results are in line with the study of Wildenbeest et al.17, who found the same interaction during repetitive seated reaching. The observed interaction aligns with the hypothesis that psychological apprehensions concerning pain or injury—manifested through task-specific fear—may differentially influence motor control strategies between individuals with and without LBP. For patients with LBP, increased fear might trigger maladaptive movement patterns, potentially leading to greater variability in their movements due to sensorimotor impairment and lack of movement control. An alternative explanation for this increased variability could be a loose control strategy, where patients attempt to find non-painful movement patterns. Conversely, healthy individuals might respond to increased fear by adopting more conservative, less variable movement strategies, possibly reflecting an instinctive cautionary approach in the face of perceived risks. However, it is important to note that the PHODA-upstairs scores were 7.8/100 for individuals with LBP and 3.69/100 for healthy individuals, indicating that the fear levels were low. Consequently, it is unlikely that this would result in a clinical significantly altered movement pattern, especially given the low perceived risk of stair climbing. Regarding task-specific pain-related fear and SMV in patients with LBP, previous studies have shown an association16,17 that could not be confirmed in the current study. One possible explanation for the discrepancy between our hypothesis and the results could be the characteristics of the current sample. The patients with LBP are relatively young (29.63 ± 7.20 years) and reported low levels of pain at measurement. Furthermore, the levels of pain-related fear were lower compared to those reported in previous studies22,46,47. Additionally, the differences between groups in pain-related fear scores may be too small to be of clinical relevance. This may serve as a potential explanation for the absence of significant associations and group-interactions in this sample. The pain-related fear experienced by the participants, especially for the non-lifting tasks may have been too minimal to produce observable effects on their movement behaviour.
Another explanation for this discrepancy could be the different methodological approaches used. Instead of the PHODA-SeV, Wildenbeest et al.17 used an 11-point BORG scale to assess expected task-specific demands for the back. As an index for SMV, they calculated the mean standard deviation of 45 movement cycles of seated reaching; hence, significantly more repetitions and another activity, as in the current study. Fujii et al.16 used a non-validated retrospective measure of task-specific pain-related fear after the subject had performed the movements. They assessed the lifting of an object that was heavier (10%, 30%, and 50% of body weight) than 5 kg in the current study. The higher load could have led to a higher SMV, similar to another study that showed a higher SMV when running with load compared to no load48. Fujii et al.16 performed the variability calculation with CRP but the association was found in the mean absolute relative phase (MARP) rather than the DP we used as primary outcome parameter. MARP is an index for coordination between two body segments, whereas DP is an index of coordination variability between two segments16,40. Concerning the association between general pain-related fear and SMV, only one study showed such an association based on the Fear-Avoidance Beliefs Questionnaire (FABQ) and lumbar movement variability, which was defined as an averaged point-by-point standard deviation across 12 cycles of seated trunk flexion and extension49. Otherwise, the current results are in line with those of previous studies, where no association between general pain-related fear and SMV was found15,16,50. In those studies, general pain-related fear was assessed using the TSK whereas SMV was quantified using three different variability measures (CRP, principal component analysis, and mean residual standard deviation) based on activities such as walking on a treadmill and lifting an object.
In the current study, across all six significant regression models (i.e. walking upstairs), sex had a significant influence on SMV, reflected by a higher SMV in females compared to males, which may be attributed to several factors. Anatomically, females generally have a wider pelvis and different lumbopelvic alignment compared to males, which could influence spinal kinematics. Physiologically, hormonal differences, particularly the effects of oestrogen and relaxin, may affect ligament laxity and joint stability51, potentially leading to greater variability in movements. Biomechanically, differences in muscle strength, recruitment patterns, and movement strategies between sexes52,53 could also contribute to the observed disparities in SMV.
Numerous methods have been outlined in the literature to quantify movement variability, each with its own strengths and limitations9,12,14,54. Most of the existing tools were developed to assess the variability of lower extremity movements during walking and running, but some have later been applied to spinal movement and non-cyclical activities12,29,32,36. The selection of the variability calculation methods suitable for this study was limited because non-cyclical tasks with only five repetitions were recorded. Usually, studies use only one or two variability calculation techniques, and when studies apply different methods, a comparison might be difficult9,14,54. For a more comprehensive statement, four different calculations were performed. Spearman rank correlation matrices revealed mostly weak or no correlations between the four variability calculation methods. Each technique employs distinct input variables, thereby shedding light on unique facets of movement variability. Methods like VC and CRP, which evaluate coordinative variability between two segments, provide insights into the dynamic interactions and synchronization during movement. In contrast, the CV focuses more on the consistency and variability of movement amplitudes, while the AAVV additionally accounts for the angular velocities. Given their at best weak correlation, these methods are not interchangeable, and their divergent use across studies complicates the task of drawing comparisons. This diversity underscores the complexity of movement variability and highlights the need for a standardized approach to enhance the coherence and comparability of research findings in this field.
Additionally, biomechanically demanding tasks (e.g., high-velocity, asymmetric, or repetitive movements) might lead to decreased variability in patients with LBP9. The five included activities were all activities of daily life without high loads; therefore, similar patterns across different activities were expected. It could be presumed that object lifting is more demanding because participants rated it as significantly more harmful according to the PHODA scores, whereas running is considered more demanding due to the higher speed involved. However, a comprehensive consensus remains elusive across the different measures and activities. This raises doubts about how well the different variability indices used in today’s literature really measure SMV: the indices vary greatly depending on the calculation method and the activity being studied. Therefore, comparisons among different studies should be performed with caution.
Studies regarding the existence of altered movement variability in patients with LBP compared with healthy controls are inconsistent. Increased, decreased, and unaltered SMV have been reported10,36,38,54,55. In our study, no significant group differences in movement variability were observed. This lack of difference may be due to the patients’ low pain levels, which may not have been sufficient to induce altered movement patterns. Moreover, while psychological factors—known to influence movement variability—did show significant differences between the groups, these differences may not be clinically meaningful. Differences in the direction of alterations could occur due to subgroups in patients with LBP9 such as decreased SMV for acute and subacute LBP with low-to-moderate pain-related fear, increased SMV for chronic or mechanical LBP with poor movement control, or no differences in SMV for patients with subacute or chronic LBP with a low pain index and low disability9. In the current study, the type of LBP was not further analyzed or classified. Dividing the sample into subgroups of different pain intensity or different movement characteristics (e.g., tight and loose motor control type11) could potentially reveal further insights.
This study has several limitations. The results of the current study can only be applied to a similar patient population according to their characteristics. Additionally, the lack of a power analysis specific to the current research question, as the data were originally collected for a different primary outcome, may affect the study’s ability to detect small effect sizes. The use of skin-marker-based three-dimensional motion capture was previously shown to be inaccurate for estimating absolute lumbar curvature angles56. However, since in the current study we did not focus on absolute values but rather on relationships between different movement trials within one subject, this should not have influenced the current findings in a significant way. All variability measures were averaged to obtain a discrete index for statistical analyses to allow for a simpler comparison. However, characterizing time series of kinematic data with an averaged measure can lead to loss of information. In future studies, the application of a statistical parametric mapping-based approach57 for analyzing continuous data could reveal new knowledge on the association between movement variability and pain-related fear.
A limitation of our study is the use of only five repetitions, which may not be sufficient to obtain a reliable estimate of within-subject between-trial variability58,59; we chose this number as a practical compromise between measurement accuracy, feasibility and participant burden, and similar methodologies have been employed in other studies16,32. The selected SMV measures only assessed between-trial variability, additionally within-trial variability would also be of interest. Most of the variability measurements for intra-trial variability are nonlinear tools, such as the entropy measure, recurrence quantification analysis, or Lyapunov exponent9,13,60. All of these require a certain number of continuous movement cycles; therefore, they are often applied to assess movement variability during walking and running on a treadmill, where the kinematics of multiple cycles can be relatively easily recorded59,61.
In the current study, a limited set of biopsychological interactions were analyzed, even though the clinical picture of LBP is much more complex, with many contributing factors according to the biopsychosocial model3. There is some evidence of a relationship between spinal motor behavior and pain-related fear in patients with LBP62, and although no association with SMV was found in the current study, it is important to further assess the factors contributing to LBP to improve prevention and treatment. A possible approach would be a prospective longitudinal study for several years with regular assessments of physical factors (e.g., kinematic, kinetic, and electromyography), as well as psychological and social factors. This would allow us to gain more insight into the temporal development of the different contributors leading to the onset of LBP, and thus, would enable the optimization of specific prevention and treatment approaches for this increasing health problem.
In conclusion, the findings of this study do not support the hypothesis that SMV during activities of daily living and pain-related fear are associated, except for the significant interaction effect of group and task-specific pain-related fear observed in the CV in the frontal plane during walking upstairs. However, results regarding SMV must be interpreted with caution since the four different movement variability indices were weakly correlated with each other and varied highly depending on the analyzed activity. Moreover, the absence of associations and interaction effects might be explained by the relatively low levels of pain and pain-related fear in the LBP patient group.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Wu, A. et al. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the global burden of Disease Study 2017. Ann. Transl. Med.8, 299 (2020).
Dionne, C. E. et al. A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine33, 95–103 (2008).
Hartvigsen, J. et al. What low back pain is and why we need to pay attention. Lancet391, 2356–2367 (2018).
Crombez, G., Vlaeyen, J. W., Heuts, P. H. & Lysens, R. Pain-related fear is more disabling than pain itself: Evidence on the role of pain-related fear in chronic back pain disability. Pain80, 329–339 (1999).
Wertli, M. M., Rasmussen-Barr, E., Weiser, S., Bachmann, L. M. & Brunner, F. The role of fear avoidance beliefs as a prognostic factor for outcome in patients with nonspecific low back pain: A systematic review. Spine J.14, 816–836e814 (2014).
Christe, G. et al. Relationship between psychological factors and spinal motor behaviour in low back pain: A systematic review and meta-analysis. Pain162, 672–686 (2021).
Christe, G., Benaim, C., Luthi, F., Jolles, B. M. & Favre, J. Reduction in pain-related fear is not associated with improvement in spinal biomechanics but with decrease in movement-evoked pain in patients with chronic low back pain. Pain Pract.23, 290–300 (2023).
Imai, R. et al. Task-specific fear rather than general kinesiophobia assessment is associated with kinematic differences in chronic low back pain during lumbar flexion: A preliminary investigation. PAIN Rep.7, 1025 (2022).
Saito, H. et al. Spinal movement variability associated with low back pain: A scoping review. PLoS One16, e0252141 (2021).
Alsubaie, A. M., Sanderson, A., Cabral, H. V., Martinez-Valdes, E. & Falla, D. Spinal kinematic variability is increased in people with chronic low back pain during a repetitive lifting task. J. Electromyogr. Kinesiol.73, 102832 (2023).
Van Dieën, J. H., Reeves, P., Kawchuk, N., Van Dillen, G., Hodges, P. W. & L. R. & Motor control changes in low back pain: Divergence in presentations and mechanisms. J. Orthop. Sports Phys. Ther.49, 370–379 (2019).
Hamill, J., Haddad, J. M. & McDermott, W. J. Issues in quantifying variability from a dynamical systems perspective. J. Appl. Biomech.16, 407–418 (2000).
Alsubaie, A. M., Mazaheri, M., Martinez-Valdes, E. & Falla, D. Is movement variability altered in people with chronic non-specific low back pain: A protocol for a systematic review. BMJ Open11, e046064 (2021).
Miller, R. H., Chang, R., Baird, J. L., Van Emmerik, R. E. & Hamill, J. Variability in kinematic coupling assessed by vector coding and continuous relative phase. J. Biomech.43, 2554–2560 (2010).
Veeger, T. T. J., van Trigt, B., Hu, H., Bruijn, S. M. & van Dieën, J. H. Fear of movement is not associated with trunk movement variability during gait in patients with low back pain. Spine J.20, 1986–1994 (2020).
Fujii, R., Imai, R., Shigetoh, H., Tanaka, S. & Morioka, S. Task-specific fear influences abnormal trunk motor coordination in workers with chronic low back pain: a relative phase angle analysis of object-lifting. BMC Musculoskelet. Disord.23, 161 (2022).
Wildenbeest, M. H., Kiers, H., Tuijt, M. & van Dieen, J. H. Associations of low-back pain and pain-related cognitions with lumbar movement patterns during repetitive seated reaching. Gait Posture91, 216–222 (2022).
Knechtle, D. et al. Fear-avoidance beliefs are associated with reduced lumbar spine flexion during object lifting in pain-free adults. Pain162, 1621–1631 (2021).
Frymoyer, J. W. Back pain and sciatica. N Engl. J. Med.318, 291–300 (1988).
Rusu, A. C., Kreddig, N., Hallner, D., Hülsebusch, J. & Hasenbring, M. I. Fear of movement/(re)injury in low back pain: Confirmatory validation of a German version of the Tampa Scale for Kinesiophobia. BMC Musculoskelet. Disord.15, 280 (2014).
Houben, R. M., Leeuw, M., Vlaeyen, J. W., Goubert, L. & Picavet, H. S. Fear of movement/injury in the general population: Factor structure and psychometric properties of an adapted version of the Tampa Scale for Kinesiophobia. J. Behav. Med.28, 415–424 (2005).
Leeuw, M., Goossens, M. E., van Breukelen, G. J., Boersma, K. & Vlaeyen, J. W. Measuring perceived harmfulness of physical activities in patients with chronic low back pain: The photograph series of daily activities–short electronic version. J. Pain8, 840–849 (2007).
Schmid, S. et al. Spinal kinematics during gait in healthy individuals across different age groups. Hum. Mov. Sci.54, 73–81 (2017).
Cerrito, A., Bichsel, L., Radlinger, L. & Schmid, S. Reliability and validity of a smartphone-based application for the quantification of the sit-to-stand movement in healthy seniors. Gait Posture41, 409–413 (2015).
von Arx, M. et al. From Stoop to Squat: A comprehensive analysis of lumbar loading among different lifting styles. Front. Bioeng. Biotechnol.9, 769117 (2021).
Niggli, L. A., Eichelberger, P., Bangerter, C., Baur, H. & Schmid, S. Between-session reliability of skin marker-derived spinal kinematics during functional activities. Gait Posture85, 280–284 (2021).
Documentation Nexus 2.16: Full body modeling with Plug-in Gait, https://help.vicon.com/space/Nexus216/11607226/Full+body+modeling+with+Plug-in+Gait (accessed on august 17, 2024).
Harbourne, R. T. & Stergiou, N. Movement variability and the use of nonlinear tools: Principles to guide physical therapist practice. Phys. Ther.89, 267–282 (2009).
Winter, D. A. Biomechanics and motor control of human movement. Fourth Edition edn (John Wiley & Sons, 2009).
Wagner, H., Pfusterschmied, J., Klous, M., von Duvillard, S. P. & Müller, E. Movement variability and skill level of various throwing techniques. Hum. Mov. Sci.31, 78–90 (2012).
Sparrow, W. A., Donovan, E., van Emmerik, R. & Barry, E. B. Using relative motion plots to measure changes in intra-limb and inter-limb coordination. J. Mot Behav.19, 115–129 (1987).
Needham, R., Naemi, R. & Chockalingam, N. Quantifying lumbar-pelvis coordination during gait using a modified vector coding technique. J. Biomech.47, 1020–1026 (2014).
Batschelet, E. Circular Statistics in Biology (Academic, 1981).
Burgess-Limerick, R., Abernethy, B. & Neal, R. J. Relative phase quantifies interjoint coordination. J. Biomech.26, 91–94 (1993).
Hamill, J., van Emmerik, R. E., Heiderscheit, B. C. & Li, L. A dynamical systems approach to lower extremity running injuries. Clin. Biomech. (Bristol Avon)14, 297–308 (1999).
Ippersiel, P., Robbins, S. & Preuss, R. Movement variability in adults with low back pain during sit-to-stand-to-sit. Clin. Biomech. (Bristol Avon)58, 90–95 (2018).
Lin, H., Seerden, S., Zhang, X., Fu, W. & Vanwanseele, B. Inter-segmental coordination of the spine is altered during lifting in patients with ankylosing spondylitis: A cross-sectional study. Med. (Baltim)99, e18941 (2020).
Shojaei, I., Vazirian, M., Salt, E. G., Van Dillen, L. R. & Bazrgari, B. Timing and magnitude of lumbar spine contribution to trunk forward bending and backward return in patients with acute low back pain. J. Biomech.53, 71–77 (2017).
Lamb, P. F. & Stöckl, M. On the use of continuous relative phase: Review of current approaches and outline for a new standard. Clin. Biomech. (Bristol Avon)29, 484–493 (2014).
Stergiou, N., Jensen, J. L., Bates, B. T., Scholten, S. D. & Tzetzis, G. A dynamical systems investigation of lower extremity coordination during running over obstacles. Clin. Biomech. (Bristol Avon)16, 213–221 (2001).
Kowalski, K. L., Boolani, A. & Christie, A. D. Sex differences in the impact of state and trait fatigue on gait variability. Hum. Mov. Sci.80, 102884 (2021).
Glickman, M. E., Rao, S. R. & Schultz, M. R. False discovery rate control is a recommended alternative to Bonferroni-type adjustments in health studies. J. Clin. Epidemiol.67, 850–857 (2014).
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. Roy. Stat. Soc.: Ser. B (Methodol.)57, 289–300 (1995).
Davison, A. C. & Hinkley, D. V. Bootstrap Methods and Their Application (Cambridge University Press, 1997).
Canty, A. & Ripley, B. D. boot: Bootstrap R (S-Plus) Functions. (2022). https://cran.r-project.org/web/packages/boot/index.html
Oliveira, C. B. et al. Psychometric properties of the photograph series of daily activities-short electronic version (PHODA-SeV) in patients with chronic low back pain. J. Orthop. Sports Phys. Ther.48, 719–727 (2018).
Matheve, T., De Baets, L., Bogaerts, K. & Timmermans, A. Lumbar range of motion in chronic low back pain is predicted by task-specific, but not by general measures of pain‐related fear. Eur. J. Pain23, 1171–1184 (2019).
Liew, B. X. W., Morris, S. & Netto, K. Trunk-pelvis coordination during load carriage running. J. Biomech.109, 109949 (2020).
Alsubaie, A. M., Martinez-Valdes, E., De Nunzio, A. M. & Falla, D. Trunk control during repetitive sagittal movements following a real-time tracking task in people with chronic low back pain. J. Electromyogr. Kinesiol.57. (2021).
Lamoth, C. J. C., Meijer, O. G., Daffertshofer, A., Wuisman, P. I. J. M. & Beek, P. J. Effects of chronic low back pain on trunk coordination and back muscle activity during walking: Changes in motor control. Eur. Spine J.15, 23–40 (2005).
Raj, R. D. et al. The impact of the menstrual cycle on orthopaedic sports injuries in female athletes. Bone Joint J.105-b, 723–728 (2023).
Plamondon, A., Larivière, C., Denis, D., St-Vincent, M. & Delisle, A. Sex differences in lifting strategies during a repetitive palletizing task. Appl. Ergon.45, 1558–1569 (2014).
Arampatzis, A., Frank, J., Laube, G. & Mersmann, F. Trunk muscle strength and lumbo-pelvic kinematics in adolescent athletes: Effects of age and sex. Scand. J. Med. Sci. Sports. 29, 1691–1698 (2019).
Alsubaie, A. M., Mazaheri, M., Martinez-Valdes, E. & Falla, D. Is movement variability altered in people with chronic non-specific low back pain? A systematic review. PLoS One18, e0287029 (2023).
Asgari, N., Sanjari, M. A. & Esteki, A. Local dynamic stability of the spine and its coordinated lower joints during repetitive lifting: Effects of fatigue and chronic low back pain. Hum. Mov. Sci.54, 339–346 (2017).
Zemp, R. et al. Soft tissue artefacts of the human back: Comparison of the sagittal curvature of the spine measured using skin markers and an open upright MRI. PLoS One9, e95426 (2014).
Pataky, T. C. Generalized n-dimensional biomechanical field analysis using statistical parametric mapping. J. Biomech.43, 1976–1982 (2010).
Hafer, J. F. & Boyer, K. A. Variability of segment coordination using a vector coding technique: Reliability analysis for treadmill walking and running. Gait Posture51, 222–227 (2017).
Riva, F., Bisi, M. C. & Stagni, R. Gait variability and stability measures: Minimum number of strides and within-session reliability. Comput. Biol. Med.50, 9–13 (2014).
Komar, J., Seifert, L. & Thouvarecq, R. What variability tells us about motor expertise: Measurements and perspectives from a complex system approach. Mov. Sport Sci.89, 65–77 (2015).
Tsigkanos, C., Demestiha, T., Spiliopoulou, C. & Tsigkanos, G. Gait kinematics in low back pain: A non-linear approach. J. Back Musculoskelet. Rehabil.34, 707–714 (2021).
Ippersiel, P., Teoli, A., Wideman, T. H., Preuss, R. A. & Robbins, S. M. The relationship between pain-related threat and motor behavior in nonspecific low back pain: A systematic review and Meta-analysis. Phys. Ther.102 (2022).
Acknowledgements
This study was supported by the Swiss National Science Foundation (SNSF; Grant-No.: 185123).
Author information
Authors and Affiliations
Contributions
C.K. calculated SMV, conducted the data analysis and wrote the original draft. M.S. and E.J. were responsible for data collection and data processing. M.D. and C.B. provided valuable inputs on methodology and data interpretation. S.S. and M.M. contributed to conceptualization and methodology and supervised the study. All authors reviewed the manuscript and approved the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kehl, C., Suter, M., Johannesdottir, E. et al. Associations between pain-related fear and lumbar movement variability during activities of daily living in patients with chronic low back pain and healthy controls. Sci Rep 14, 22889 (2024). https://doi.org/10.1038/s41598-024-73430-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-73430-8
