
Abstract
Reduced functional connectivity of physiological systems is associated with poor prognosis in critically ill patients. However, physiological network analysis is not commonly used in clinical practice and awaits quantitative evidence. Acute liver failure (ALF) is associated with multiorgan failure and mortality. Prognostication in ALF is highly important for clinical management but is currently dependent on models that do not consider the interaction between organ systems. This study aims to examine whether physiological network analysis can predict survival in patients with ALF. Data from 640 adult patients admitted to the ICU for paracetamol-induced ALF were extracted from the MIMIC-III database. Parenclitic network analysis was performed on the routine biomarkers using 28-day survivors as reference population and network clusters were identified for survivors and non-survivors using k-clique percolation method. Network analysis showed that liver function biomarkers were more clustered in survivors than in non-survivors. Arterial pH was also found to cluster with serum creatinine and bicarbonate in survivors compared with non-survivors, where it clustered with respiratory nodes indicating physiologically distinctive compensatory mechanism. Deviation along the pH-bicarbonate and pH-creatinine axes significantly predicts mortality independent of current prognostic indicators. These results demonstrate that network analysis can provide pathophysiologic insight and predict survival in critically ill patients with ALF.
Similar content being viewed by others

Introduction
The human body is a complex system composed of an intertwined network of physiological components that interact with each other to maintain homeostasis. The study of robustness in complex physiological networks is important because it can aid in understanding disease processes and the compensatory mechanisms that lead to survival after critical illnesses such as multiple-organ failure. Our knowledge about predictors of survival in critically ill patients is limited to clinical and epidemiological studies that have identified risk factors for mortality, such as a greater number of failing organs assessed by the SOFA score (Sequential Organ Failure Assessment)1,2. Recent studies using various machine learning approaches have also indicated that the aggregation of previous disease history and acute physiology measures can predict in-hospital mortality in critically ill patients3. While all these studies are useful for prognostication in intensive care units, they rarely provide hypotheses that may lead to the development of interventions to alter the progression of the disease.
Recently, the network of physiological organ interactions has been studied within the context of critical illness4,5,6. The emerging field of network physiology has established the groundwork for understanding and quantifying global physiological behaviours arising from networked interactions across systems in health and disease7,8. At least in theory, mapping the physiological network during an acute pathological insult in survivors may reveal compensatory mechanisms deployed to regain homeostasis with the potential for the development of new therapies. Indeed, physiological network mapping can also improve our understanding of the pathophysiology of the disease.
The liver plays a pivotal role in physiological processes within the body, positioning it as a central hub in the control of various physiological mechanisms. Clinicians readily acknowledge the functional connectivity of the liver with other organs, which is particularly evident in patients with liver failure who manifest involvement of multiple organs, such as neural, cardiovascular, renal, and metabolic dysfunction, as well as acid/base and electrolyte imbalance9. Chronic liver failure (cirrhosis) is associated with impaired cardiovascular control10,11,12 and thermoregulatory dynamics13,14,15. The application of a network approach in patients with cirrhosis has also revealed that organ system network disruption is associated with a poor prognosis in patients with chronic liver failure16,17. Specifically, there was a greater correlation between physiological biomarkers in liver cirrhosis in survivors than in non-survivors, indicating that more connected organ systems are present in survivors16,17. Furthermore, physiological network connectivity indices could predict 6-month survival in patients with cirrhosis independent of age and the severity of liver disease17,18. Such a network approach in liver cirrhosis is helpful, as it can provide prognostic information (e.g., for application in liver transplant allocation) as well as aid in predicting response to therapy (e.g., targeted albumin therapy)18.
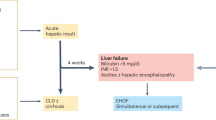
The process of cirrhosis is a slow process that takes more than a decade to significantly affect physiological networks. On the other hand, acute liver failure (ALF) is an acute process defined as the presence of severe worsening acute liver injury (< 26 weeks) in patients with no history of chronic liver disease19. ALF can be caused by acute exposure to high doses of hepatotoxins such as paracetamol (acetaminophen). Paracetamol-induced ALF is the most common cause of ALF in Western countries20. The rapid deterioration of liver function in ALF patients is strongly associated with a high risk of mortality, which may be prevented by timely liver transplantation. However, a subpopulation of ALF patients is known to recover fully without transplantation. Due to its accidental occurrence (e.g., drug overdose), paracetamol-induced ALF often occurs in otherwise healthy individuals. These patients need to adapt and employ suitable compensatory mechanisms to survive rapidly. While ALF is a multiorgan systemic disease involving other organ systems (e.g., hepatic encephalopathy), a network approach has not yet been applied to understand the differences in organ-system interactions between survivors and non-survivors. In this study, we aimed to apply a network mapping approach to investigate the interaction between multiple variables representing various organ systems in a cohort of critically ill patients with ALF. We also aimed to compare the prognostic value of the network mapping approach with the current clinical prognostic indicators used to assess critically ill patients with ALF (e.g., the King’s College Criteria score and SOFA score).
Methods
Database description and extraction
The data analysed in this study were sourced from the third version of the Medical Information Mart for Intensive Care (MIMIC-III) following training, application, and acquisition of the required permissions. MIMIC-III data has been deidentified in accordance with Health Insurance Portability and Accountability Act (HIPAA) standards and the project approved by the Institutional Review Boards of Beth Israel Deaconess Medical Centre and the MIT (IRB protocol nos. 2001P001699/14 and 0403000206, respectively). The authors involved in data extraction (TO and ARM) completed mandatory online ethics training at MIT and were credentialled (IDs 10304625 and 48067739).
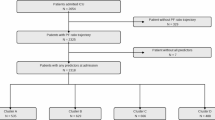
The MIMIC-III dataset includes more than 53,000 unique admissions to a single hospital (i.e., the Beth Israel Deaconess Medical Centre in Boston between 2001 and 2012). Thus, this is a retrospective study based on a single centre dataset. Initially, the complete MIMIC-III clinical dataset was downloaded to a secured cloud storage of the University College London (UCL), and structure query language (SQL) code was used to extract the required data based on the inclusion criteria. Thus, the inclusion criteria included being an adult (aged 18 years and above) and being diagnosed with ALF linked with paracetamol/acetaminophen overdose at the time of ICU admission. Patients with less than 50% of clinical data records or those with missing follow-up and hospital mortality records were excluded from this study.
Specifically, the SQL code extracted data of patients aged 16 years and older of any sex who were diagnosed with acute liver failure (ICD_DIAGNOSIS) based on the International Classification of Diseases 9th revision (ICD9) Code (570)21 and who had a combination of the strings ‘acetaminophen’ or ‘paracetamol’ or other known commercial names of acetaminophen-containing combination drugs as well as the string ‘overdose’ in their clinical notes (NOTEEVENTS). The combination of the clinical note details with the ICD9 code was performed to reduce the error inherently associated with the now obsolete ICD9 diagnostic code used in the MIMIC-III data, especially for acetaminophen/paracetamol-induced ALF22. The list of patients was then used to extract the laboratory variables (LABEVENTS) and vital variables (CHARTEVENTS). Other clinical variables of the identified patients, including age, sex, ICU length of stay, and in-hospital mortality, were also extracted for analysis. Specifically, the clinical and laboratory variables collected are those collected within the first 24 h of ICU stay. Where more than one measurement is taken within the first 24 h of ICU admission, the mean measurement is computed to give a central measure of patients’ physiological status. Patients who do not have variables taken within the first day were automatically excluded during data extraction.
Furthermore, the minimum Glasgow Coma Score (GCS) and King’s College Criteria (KCC), which index patients’ level of consciousness23 and severity of ALF24, respectively, were computed based on the available data recorded during the first day of ICU admission and included in the analysis. The GCS score was calculated based on the patient’s verbal and motor responses and eye opening25. For KCC, patients were scored based on acidosis (arterial pH < 7.30), coagulopathy (international normalized ratio > 6.5), kidney function (serum creatinine > 3.4 mg/dL), and the presence of hepatic encephalopathy of grade 3 or 4 according to the West Haven grading system24. However, because the MIMIC-III dataset does not contain the West Haven grades (or any grading system) of hepatic encephalopathy, patients whose GCS score was ≤ 8 were classified as West Haven grade III or IV according to clinical guidelines26,27.
The sequential organ failure assessment (SOFA) score, which is often used to assess the severity (morbidity) of critically ill patients, was also calculated since the study population is primarily those admitted to the ICU28. Patients were followed for 28 days, and data were collected on the occurrence of death or liver transplantation. Patients who underwent liver transplantation for ALF within 28 days were classified as ‘non-survivors’ on the day of transplantation, as they were in immediate need of a new liver and would not have survived without it.
Physiological network mapping
We applied Parenclitic network mapping for network mapping based on patients’ clinical or biochemical biomarkers. Parenclitic network mapping is a novel approach for network analysis17 that facilitates the mapping of individual data points within models constructed from a reference population (e.g., patients who survive ALF). Initially, the correlation between clinical/biochemical biomarkers was assessed in the reference population (i.e., patients with ALF in the MIMIC-III cohort that survived for 28 days in the ICU) to determine the expected relationship between the pair of biomarkers. To map the network of individual patients, a parenclitic approach was used. This analysis measures the deviations of an individual patient from the expected relationship between variables in the reference population. In this study, the data of patients who survived ALF 28 days post-ICU admission were used as the reference population. Regression analysis was performed on pairs of clinical variables based on a p value that was corrected for the number of comparisons (Bonferroni correction). A population network was then created based on statistically significant regressions. The parenclitic deviations from the significantly correlated models along each axis (pairs of variables) were computed and used to construct a network map of individual patients. The deviation along each axis is reported as δ-A/B (e.g., δ-chloride/bicarbonate), where A or B represents a biochemical variable (e.g., chloride and bicarbonate), and δ denotes deviation from the regression line between A and B in survivors with ALF (i.e., the reference population). Network mapping was carried out using an in-house code developed in MATLAB (MathWorks, CA, USA). For a detailed exploration of Parenclitic network analysis in the context of cirrhosis, refer to the research conducted by Zhang et al.17.
Detection of local clusters within the network
For a complex physiological network containing a high number of nodes, understanding the cluster of tightly interconnected nodes could provide insight into the core structures within the network. The k-clique percolation method is a cluster detection technique that is robust to the overlap of shared characteristics between clusters within a network29,30. The technique defines all the cliques (a subgraph of a network where all member nodes are adjacent to each other) within a network that shares k-1 (at least one) nodes30. A clique in this instance is defined as a complete subnetwork within the overall phylogenetic network composed of physiological variables with a greater likelihood of being correlated compared with variables from other communities31. Thus, the physiological communities are defined as organ systems that are more closely aligned in terms of functionality compared with other nodes within the overall network. In this study, the k-clique percolation method was employed using a MATLAB function originally written by Ahn-Dung Nguyen32. The nodes and edges of the detected community (cliques) are color-coded for clarity and show which variables belong to the same clique.
Principal component analyses
Since Parenclitic network mapping is based on the correlation between physiological variables in a reference population, it shares some statistical insight with the principal component analysis commonly used for dimension reduction. Thus, principal component analysis was also performed on patient biomarkers to assess which combination of variables (principal components, PCs) can predict survival in patients with paracetamol-induced ALF. This analytic method can identify clusters of variables that are highly correlated before dimension reduction. Therefore, it has been used for the identification of clusters during network analysis within the context of critical care6. Briefly, principal component analysis reduces the dimension of a dataset by computing the best combination of variables (PCs) that explains most of the variability in a dataset33. For this analysis, Bartlett’s test of sphericity (chi-squared) and KMO-MSA (Kaiser, Meyer, Olkin’s Measure of Sampling Adequacy) were used to assess whether the dataset was suitable for factor analysis, while Kaiser’s rule based on eigenvalues > 1.0 was used to determine relevant PCs that explained a significant portion of the variability in the data. To extract variables that could be easily interpreted, the normalized varimax rotation method was used34.
Statistical analysis
The characteristics of patients who survived and those who did not survive were compared with continuous and categorical variables and are presented as the mean ± standard deviation (SD) or median and interquartile range (IDR), respectively. For comparisons of continuous variables between patient groups, independent samples t tests or Mann‒Whitney U tests were used depending on whether the data were normally distributed. In general, parental deviations (δs), as well as principal components, were subjected to statistical analysis for survival predictions. The chi-squared test was used to compare categorical variables with significantly different variables (parenclitic and principal components) that were subjected to univariate and multivariate Cox regression analyses. To compare the hazard ratios of the network indices, the scales of the parenclitic deviations were normalized before Cox regression analysis using Z transformation. Receiver operating characteristic (ROC) curve analyses were performed for variables that were independently predictive of 28-day ICU mortality, and the area under the curve (AUC) was computed. Positive and negative predictive values of the ROC cut-offs were computed using the sensitivities and 1-point specificities. All the statistical analyses were performed with SPSS Statistics 26 (IBM Corp., Armonk, NY). For the assessment of prognostic improvement from the combination of parenclitic indices and principal components with the SOFA score, the Brier score, integrated discrimination improvement (IDI), and the net reclassification index (NRI) were computed with Stata statistical software (Stata/MP, Version 17.0). Essentially, lower Brier scores translate into a better predictive model, while IDI and NRI decrease misclassification due to the addition of a new variable to a predictive model35,36. For the interpretation of all the statistical analysis results, a two-tailed p-value less than 0.05 was used as the cut-off for significance. For the combination of the SOFA score with the independent predictive indices, composite scores were created using the formula β1 ×SOFA + β2 × δ, where β is the multivariate Cox regression coefficient of the variables.
Results
Patient characteristics
A total of 640 patients with ALF due to paracetamol overdose were included in this study, 249 (38.9%) of whom either did not survive a 28-day ICU stay or underwent liver transplantation during admission. Overall, there was no significant difference in age (years), sex, ICU length of stay (LOS), aspartate transaminase (AST), serum bicarbonate, serum sodium (Na), international normalized ratio (INR), white blood cell (WBC) count, heart rate (HR), respiratory rate (RespR), or arterial blood pH (pH). However, there was significantly greater alanine aminotransferase (ALT), serum albumin, chloride, platelet count, body temperature, mean blood pressure, oxygen saturation, haemoglobin, and Glasgow Coma Score (GCS) in surviving patients than in non-survivors (Table 1).
Differences in parenclitic network indices between ICU survivors and non-survivors
There was an overall greater correlation between variables in the survivors than in the non-survivors (Fig. 1). Detection of clusters within the networks using the k-clique percolation method showed observable differences in the pattern of network clusters between the groups with the optimum k number of 5. Specifically, a cluster of liver function-related biomarkers was found only in survivors. Additionally, arterial blood pH was strongly correlated with kidney function markers (serum creatinine) in survivors (Fig. 1), while in non-survivors, arterial pH was correlated with oxygen saturation and the respiratory rate (Fig. 2). In addition to the correlation map, we mapped the parenclitic network of individual patients based on the deviation of pairs of physiological variables from the reference model. In general, the significant differences in the parenclitic deviation along all physiological axes were significantly greater in non-survivors than in survivors, except along the chloride-bicarbonate and creatinine-alkaline phosphatase axes (Table 2).

Network map of clinical and laboratory variables showing correlations and k-clique percolation clusters of patients with acute liver failure who survived their ICU stay (optimized k—clique size = 3). The size of the nodes is automatically generated and does not represent any measure of influence or magnitude. Also, the colours of the nodes and edges were used to help differentiate the clusters from one another and have no analytical translation beyond this. Cl chloride, AST aspartate transaminase, ALT alanine aminotransferase, GCS Glasgow Coma Score, Bil total bilirubin, ALP alkaline phosphatase, Cr serum creatinine, Na serum sodium, Glu blood glucose, HR heart rate, RespR respiratory rate, Temp temperature.

Network map of clinical and laboratory variables showing correlations and k-clique percolation communities of patients with acute liver failure who did not survive their ICU stay (Optimized k—clique size = 3). Cl chloride, AST aspartate transaminase, ALT alanine aminotransferase, GCS Glasgow Coma Score, Bil total bilirubin, ALP alkaline phosphatase, Cr serum creatinine, Na serum sodium, Glu blood glucose, HR heart rate, RespR respiratory rate, Temp temperature.
Parenclitic deviations predict survival
Parenclitic deviations along the pH-bicarbonate, pH-creatinine, lactate-glucose, lactate-heart rate, and SpO2-respiratory rate axes were significantly linked with an increased risk of 28-day ICU mortality according to univariate Cox regression analysis. Specifically, each unit of deviation along the pH-bicarbonate and pH-creatinine axes was associated with greater than 37% and 36% increases, respectively, in the risk of ICU mortality. Additionally, unit deviations along the lactate-glucose, lactate-heart rate, and SpO2-respiratory rate axes were linked to approximately 40%, 36%, and 21% increases in the risk of 28-day mortality in the ICU, respectively (Table 3).
Parenclitic deviations predict survival independent of SOFA score and the King’s College criteria
Multivariate Cox regression analyses were performed to assess whether the significantly predictive network indices were independent of the severity of ALF, as measured by the SOFA score and KCC. SOFA score and KCC were initially assessed for their predictive value and were both found to be individual predictors of 28-day mortality in this study population (hazard ratio, 95% CI = 1.04, 1.01–1.08, p = 0.014 and 1.18, 1.02–1.34, p = 0.034, respectively). Accordingly, multivariate analysis revealed that physiological deviations along the blood pH-bicarbonate (hazard ratio, 95% CI = 1.32, 1.11–1.56), arterial pH-serum creatinine (hazard ratio, 95% CI = 1.30, 1.11–1.52), lactate-glucose (hazard ratio, 95% CI = 1.34, 1.15–1.57), lactate-heart rate (hazard ratio, 95% CI = 1.32, 1.14–1.54) and SpO2-respiratory rate (hazard ratio, 95% CI = 1.19, 1.03–1.36) axes predict 28-day mortality independent of the SOFA score and King’s College Criteria (Table 4).
Principal component analysis
A total of 9 principal components had eigenvalues > 1 and were included in further analysis. Of these, only principal components 1, 3, and 7 were significantly linked with mortality according to univariate Cox regression analysis. Furthermore, multivariate Cox regression analysis revealed that each unit increase in PC-1 and decrease in PC-3 were associated with 28% and 26% increases, respectively, in the risk of mortality in ALF patients (Table 5). PC-1 identified ALT, AST, and INR, while PC-2 identified albumin, mean blood pressure, and haemoglobin as clusters for dimension reduction, as shown in Supplementary Table S1.
Parenclitic network indices improve the predictive value of SOFA score
Based on the area under the ROC curve, the addition of both parenclitic indices and principal components to the SOFA score significantly improved its predictive value, as shown by the percentage increase in the area under the curve (AUC) as well as the relatively lower Brier scores of the composite scores compared with those of the SOFA score alone (Table 6). The results from the IDI and NRI analyses showed that the addition of the parenclitic indices and principal components significantly improved the prognostic performance of the SOFA score. With regard to the IDI and NRI, the addition of principal component 1 showed the greatest reduction (IDI = 15.1% and NRI = 73.2%) in overall predictive error compared with the use of SOFA alone (Table 7).
Additionally, Kaplan–Meier survival curves (with the Mantel–Cox test) showed that compared with the SOFA score alone, the ROC cut-off of the composite score significantly differentiated between ICU-admitted ALF patients who survived and those who did not. Specifically, the cut-off values of the composite scores, including the SOFA score and independent predictive platelet deviations (δ-pH/bicarbonate, p < 0.001, δ-pH/creatinine, p = 0.005, δ-lactate/glucose, p = 0.041, δ-lactate/heart rate, p = 0.001), significantly classified survivors and non-survivors (Fig. 3).

Kaplan–Meier graphs of patients with acute liver failure admitted to the intensive care unit who survived and those who did not survive after 28 days, according to SOFA cut-off scores (A) and the cut-offs of the composite scores from the combination of SOFA with the parenclitic deviations along the pH-bicarbonate (pH-CO3) (B), pH-creatinine (pH-Cr) (C), lactate-heart rate (lactate-HR) (D), lactate-glucose (lactate-Glu) (E), and oxygen saturation-respiratory rate (SpO2-RespR) (F) axes.
Discussion
The liver serves as a major hub in the physiological network, and acute dysfunction is associated with mortality in many patients. Those who survive ALF may have adapted compensatory mechanisms that enhance survival. However, identifying these mechanisms necessitates a holistic or network approach. In this study, we employed parenclitic network mapping to demonstrate the prognostic value of this network approach in predicting survival among ICU-admitted patients with paracetamol-induced ALF. The results revealed that parenclitic deviations across different physiological axes can predict survival in this patient population independent of the current clinical prognostic factors (SOFA score and KCC). Additionally, compared with the SOFA score alone, the combination of the independent survival predictors with the SOFA score resulted in a greater than 30% reduction in classification error. This is the first study, to the best of our knowledge, to apply integrative network mapping in the prediction of survival in ICU-admitted ALF patients.
In terms of the correlation network, ALF patients who did not survive (or receive a liver transplant) in the ICU for at least 28 days were found to have overall lower organ system connectivity than survivors. Furthermore, network community detection also revealed a marked difference in network structure between the survivors and non-survivors characterized by a significant difference in organ system clustering (community formation). Generally, a community in a network defines a subpopulation of nodes (organ systems) that are more closely linked (clustered) than other nodes outside of the community37,38,39. As expected, the variables associated with liver function (e.g., ALT, AST, INR, and Alb) were relatively more clustered in survivors than in non-survivors (green nodes in Fig. 1vs. Fig. 2). This finding is in line with the results of the principal component analysis, as PC-1 in this analysis also revealed ALT, AST and INR in the same cluster. According to survival analysis, this cluster (PC-1), could predict mortality independently of the SOFA score and KCC.
In addition to the liver function community in the correlation network, arterial pH was also found to cluster with serum creatinine and bicarbonate in survivors compared with non-survivors, where it clustered with respiratory nodes (SpO2, respiratory rate) and bicarbonate (purple nodes in Figs. 1 and 2). Thus, physiologically different compensatory mechanisms for acid‒base balance between the groups were inferred. Essentially, it appears that the regulation of arterial pH was more closely linked with renal function in survivors, while in non-survivors, this function was mainly modulated by respiratory compensation. The role of the liver in acid‒base homeostasis via the regulation of systemic clearance of lactic acid and urea is generally dysregulated in liver disease40. This means that in liver disease, the role is generally shifted to classical regulatory pathways involving the respiratory and renal systems. In the context of ALF, acid-base disequilibrium has been previously shown to be driven mainly by a systemic increase in lactic acid, especially due to overproduction in peripheral organs41. Generally, the kidney plays a protective role in lactic acidosis through a pH-dependent increase in the rate of clearance of systemic lactic acid42,43. Indeed, lactic acidosis is significantly linked with poorer prognosis in patients with ALF44,45,46,47,48,49. Although ALF patients typically exhibit markedly increased lactate levels, frequently, there is no evident acid-base imbalance due to compensatory hypoalbuminemia alkalosis50. In our study, arterial pH was only slightly lower in non-survivors with ALF than in survivors (Table 1). It appears that sufficient renal function may be associated with improved survival in ALF patients admitted to the ICU, especially since the non-survivors in this study showed significantly greater deviation in the pH-creatinine axis (δ-pH/creatinine, Tables 2, 3 and 4). In line with this observation, δ-pH/creatinine was an independent prognostic factor for mortality, indicating the importance of this axis in the survival of critically ill patients with ALF.
Aside from connectivity and organ system community structure, overall parenclitic deviations of non-survivors were found to be significantly greater than those of survivors. For instance, non-survivors have greater deviation along the pH-bicarbonate, pH-creatinine, lactate-glucose, lactate-heart rate, and SpO2-respiratory rate axes, which are independently associated with survival. This translates to significantly reduced physiological coupling between these pairs of variables (i.e., higher parenclitic deviation means higher deviation from the regression line between two biomarkers in the reference population). Specifically, most of the physiological disconnections observed in non-survivors are associated with acid-base homeostasis (i.e., arterial pH, serum bicarbonate level, and serum lactate). These findings support the importance of acid‒base compensatory mechanisms in the prognosis of patients with ALF and critically ill patients51. Importantly, these network deviations predicted mortality even though there was only a slight difference in arterial pH between the patient groups (7.42 ± 0.07 versus 7.39 ± 0.11). Thus, considering the physiological network context rather than the individual isolated organ system is important for clinical management and prognosis. Additionally, deviation along the SpO2-respiratory rate axes predicted survival independent of SOFA score and KCC. SpO2 estimates the percentage of oxyhaemoglobin relative to the total blood haemoglobin and reflects cardiopulmonary efficiency in terms of systemic oxygen transportation. Although multiple cardiorespiratory factors contribute to oxygen saturation dynamics8, SpO2 and the respiratory rate have been shown to be physiologically inversely correlated52. Interestingly, there was a significantly greater mean baseline SpO2 and lower respiratory rate in ALF patients who survived than in non-survivors (Table 1). Thus, the loss of correlation and coordination between these two variables may be interpreted as a patient’s loss of adaptability and reduced ability to maintain systemic oxygen levels. Indeed, a previous study by Mower et al., showed a poor correlation between oxygen saturation and respiratory rate in approximately 15,000 patients admitted to the ICU for various reasons. However, the authors did not assess the relationship with patient survival53.
Indeed, the results of this study corroborate previous research in the field, where changes in organ system connectivity measured using network analysis and other methods were shown to improve traditional scoring systems for predicting patient outcomes in patients with cirrhosis or even detecting subgroups of patients who may respond to therapy (e.g., targeted albumin therapy)17,18,54,55. Specifically, a previous study using parenclitic network analysis showed reduced organ system connectivity (based on population-level correlation network mapping) in patients with cirrhosis who did not survive compared with survivors18. This corroborated the findings of a previous study in patients with cirrhosis referred for formal clinical assessment of hepatic encephalopathy, with similar findings showing that organ system connectivity was relatively lower in patients who did not survive after 12 months of follow-up17. However, the reduction observed in the patients with decompensated cirrhosis was greater in magnitude than that in the patients with ALF among the non-survivors. This may be due to the significantly different time course of development or clinical history of these diseases, whereby cirrhosis often develops over decades, while ALF progresses more rapidly over the course of a few weeks or days in otherwise healthy individuals56,57. Thus, while chronic cirrhosis probably affects the overall physiology of patients, culminating in a general loss of organ system coupling, ALF is likely linked to a shift in compensatory mechanisms to counter abrupt and rapidly deteriorating liver function. Regardless of the time course of liver failure, a physiological network approach appears to provide information not currently offered by existing clinical criteria (e.g., SOFA). This could open new avenues for improved prognostication and the discovery of novel personalized therapies based on individual networks in future investigations.
To further verify the results of the network analysis, especially network community detection, we performed principal component analysis to assess whether similar variables are combined within each component and whether these components can also predict survival in ALF patients. While principal component analysis is useful for dimension reduction in multivariate datasets, it is limited in scope compared with network mapping (e.g., correlation or parenclitic). Thus, while it could be used for validation, it does not suffice as a viable replacement for network analysis. This is due to several inherent limitations of principal component analysis. First, PCA is prone to the loss of crucial information and oversimplicity resulting from the reduction of dataset dimensions58. Importantly, because PCA is based on linear correlations between variables in the overall population, compared with Parenclitic network analysis, PCA does not consider the possibility that correlations may be different between subgroups (e.g., survivors and non-survivors, healthy individuals and diseased individuals) within the study population.
The study found that principal components related to liver function (AST, ALT, INR), hemodynamic function (serum albumin, mean blood pressure, haemoglobin), and metabolic function (lactate, glucose) were significantly linked to patient survival in ALF (Supplementary Table S2). However, only liver function and hemodynamic components were independent of the SOFA score and KCC (Table 5). Component 1 captures rapid liver deterioration and hepatocyte necrosis due to paracetamol toxicity and related factors59,60, aligning with a recent study that improved the prediction of drug-induced liver injury using INR and alkaline phosphatase61. Component 3, reflecting hemodynamic dysregulation, is associated with worse outcomes and has been shown to correlate with the severity of liver disease and liver transplantation outcomes62. Component 7, comprising glucose and lactate levels, also predicted mortality but not independently of patient severity scores. The Cori cycle describes the conversion of muscle-generated lactate, a byproduct of anaerobic glycolysis, to glucose in the liver. Physiologically, gluconeogenesis converts lactate to glucose in the liver, usually in response to hypoglycaemia. Thus, it could be assumed that hypoglycaemia and hyperlactatemia should not coexist. However, in conditions such as paracetamol-induced ALF, which is characterized by severe hepatocyte necrosis and loss of liver function and dysfunction in the Cori cycle, these conditions may coexist63,64. The presence of hyperlactatemia and hypoglycaemia in paracetamol-induced ALF reflects severe liver dysfunction, with both conditions linked to poorer prognosis45.
Limitations
One limitation of this study is the retrospective nature of this study, which is inherently linked with selection bias and a lack of some relevant variables (e.g., West Haven HE score), since the record was not specifically designed for the assessment of ALF65. Additionally, because the MIMIC-III dataset involves patients admitted to a single hospital serving a limited population, the results herein should be interpreted with this in mind. Specifically, most of the parameters included in the analysis show high level of within-group variability. Albeit the variables were all recorded within the first 24 h, there may be difference in the time between onset of paracetamol-induced-ALF symptoms and the time the variables were recorded which could affect the result of this analysis as paracetamol-induced-ALF is a highly dynamic condition with rapid onset and progression. For example, while transaminase levels are highly elevated at the onset of ALF, they typically decrease as the condition progresses, even as other indicators of hepatic failure worsen (e.g., a rise in serum bilirubin and a fall in albumin) [80]. This phenomenon may explain why ALT levels were higher in survivors compared to non-survivors in our cohort. However, further studies are needed to understand this unexpected finding. Furthermore, the physiological condition (and parameters) of ALF patient in the ICU is highly dynamic and generally influenced by various factors including pharmacological and non-pharmacological interventions which could confound the response and prognosis of patients. Thus, this work should be interpreted with this in mind. Another limitation of this study is related to the characteristics of the patient population, as patients were from a single centre in the USA and were from a specific region and demographic region. However, this study is based on one of the largest populations of paracetamol-induced-ALF patients subjected to rigorous mathematical and statistical analysis. In this study, we did not combine different parenclitic deviation indices to create a statistical prognostic composite due to the possibility of statistical or mechanistic dependencies between these variables. The relationships between parenclitic deviations could potentially be integrated using global network indices (e.g., network diameter, shortest path, etc.), which can be investigate separately in the future.
Conclusion
Reduced organ system connectivity and a shift from renal to respiratory compensatory mechanisms are associated with poorer prognosis in patients with ALF. This is further supported by physiological network disconnections along pH-associated axes, which predict mortality independent of SOFA score and KCC. Indeed, the strength of network analysis is the ability to assess the interactions of multiple organ systems in critically ill patients where the risk of multiple organ failure is high and similar findings continue to show significant promise66,67. Future studies could benefit from using a prospectively recruited, multicentre, and multinational cohort of ALF patients with uniformly recorded baseline parameters to validate the findings herein.
Data availability
Data are available upon request from the corresponding author.
References
Raith, E. P. et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA 317, 290–300. https://doi.org/10.1001/jama.2016.20328 (2017).
Maslove, D. M. et al. Redefining critical illness. Nat. Med. 28, 1141–1148. https://doi.org/10.1038/s41591-022-01843-x (2022).
Nielsen, A. B. et al. Survival prediction in intensive-care units based on aggregation of long-term disease history and acute physiology: a retrospective study of the Danish National Patient Registry and electronic patient records. Lancet Dig. Health 1, e78–e89. https://doi.org/10.1016/s2589-7500(19)30024-x (2019).
Asada, T. et al. Organ system network disruption in nonsurvivors of critically ill patients. Crit. Care Med. 44, 1 (2016).
Shashikumar, S. P., Li, Q., Clifford, G. D. & Nemati, S. Multiscale network representation of physiological time series for early prediction of sepsis. Physiol. Meas. 38, 2235–2248. https://doi.org/10.1088/1361-6579/aa9772 (2017).
Asada, T. et al. Organ system network analysis and biological stability in critically ill patients. Crit. Care 23, 83. https://doi.org/10.1186/s13054-019-2376-y (2019).
Ivanov, P. C. The new field of network physiology: building the human physiolome. Front. Netw. Physiol. 1, 711778. https://doi.org/10.3389/fnetp.2021.711778 (2021).
Jiang, Y. et al. A network physiology approach to oxygen saturation variability during normobaric hypoxia. Exp. Physiol. 106, 151–159. https://doi.org/10.1113/EP088755 (2021).
Golding, P. L., Smith, M. & Williams, R. Multisystem involvement in chronic liver disease. Studies on the incidence and pathogenesis. Am. J. Med. 55, 772–782. https://doi.org/10.1016/0002-9343(73)90258-1 (1973).
Oyelade, T. et al. Heart rate variability in patients with cirrhosis: a systematic review and meta-analysis. Physiol. Meas. 42, 888. https://doi.org/10.1088/1361-6579/abf888 (2021).
Mani, A. R. et al. Decreased heart rate variability in patients with cirrhosis relates to the presence and degree of hepatic encephalopathy. Am. J. Physiol. Gastrointest. Liver Physiol. 296, G330–338. https://doi.org/10.1152/ajpgi.90488.2008 (2009).
Abid, N. U. H. & Mani, A. R. The mechanistic and prognostic implications of heart rate variability analysis in patients with cirrhosis. Physiol. Rep. 10, e15261. https://doi.org/10.14814/phy2.15261 (2022).
Mani, A. R., Mazloom, R., Haddadian, Z. & Montagnese, S. Body temperature fluctuation analysis in cirrhosis. Liver Int. 38, 378–379. https://doi.org/10.1111/liv.13539 (2018).
Bottaro, M. et al. Skin temperature variability is an independent predictor of survival in patients with cirrhosis. Physiol. Rep. 8, e14452. https://doi.org/10.14814/phy2.14452 (2020).
Abid, N. U. H. et al. Application of short-term analysis of skin temperature variability in prediction of survival in patients with cirrhosis. Front. Netw. Physiol. 3, 1 (2024).
Tan, Y. Y., Montagnese, S. & Mani, A. R. Organ system network disruption is associated with poor prognosis in patients with chronic liver failure. Front. Physiol. 11, 1 (2020).
Zhang, H., Oyelade, T., Moore, K. P., Montagnese, S. & Mani, A. R. Prognosis and survival modelling in cirrhosis using parenclitic networks. Front. Netw. Physiol. 2, 833119 (2022).
Oyelade, T., Forrest, E., Moore, K. P., O’Brien, A. & Mani, A. R. Parenclitic network mapping identifies response to targeted albumin therapy in patients hospitalized with decompensated cirrhosis. Clin. Transl. Gastroenterol. 14, e00587. https://doi.org/10.14309/ctg.0000000000000587 (2023).
Williams, R., Schalm, S. W. & O’Grady, J. G. Acute liver failure: redefining the syndromes. Lancet 342, 273–275. https://doi.org/10.1016/0140-6736(93)91818-7 (1993).
Bernal, W., Auzinger, G., Dhawan, A. & Wendon, J. Acute liver failure. Lancet 376, 190–201. https://doi.org/10.1016/S0140-6736(10)60274-7 (2010).
Forns, J. et al. Validity of ICD-9 and ICD-10 codes used to identify acute liver injury: a study in three European data sources. Pharmacoepidemiol. Drug Saf. 28, 965–975. https://doi.org/10.1002/pds.4803 (2019).
Udo, R. et al. Validity of diagnostic codes and laboratory measurements to identify patients with idiopathic acute liver injury in a hospital database. Pharmacoepidemiol. Drug Saf. 25, 21–28. https://doi.org/10.1002/pds.3824 (2016).
Teasdale, G. & Jennett, B. Assessment of coma and impaired consciousness: a practical scale. Lancet 304, 81–84. https://doi.org/10.1016/S0140-6736(74)91639-0 (1974).
O’Grady, J. G., Alexander, G. J. M., Hayllar, K. M. & Williams, R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology 97, 439–445 (1989).
Jain, S. & Iverson, L. M. Glasgow Coma Scale (2018).
Montagnese, S. et al. Hepatic encephalopathy 2018: a clinical practice guideline by the Italian Association for the study of the liver (AISF). Digest Liver Dis. 51, 190–205. https://doi.org/10.1016/j.dld.2018.11.035 (2019).
Wendon, J. et al. Bernardi, M. EASL clinical practical guidelines on the management of acute (fulminant) liver failure. J. Hepatol. 66, 1047–1081 (2017).
Vincent, J. L. et al. The SOFA (Sepsis-Related Organ Failure Assessment) Score to Describe Organ Dysfunction/Failure: On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine (See Contributors to the Project in the Appendix) (1996).
Shirazi, A. H. et al. Evolution of communities in the medical sciences: evidence from the medical words network. PLoS ONE 11, e0167546. https://doi.org/10.1371/journal.pone.0167546 (2016).
Palla, G., Derényi, I., Farkas, I. & Vicsek, T. Uncovering the overlapping community structure of complex networks in nature and society. Nature 435, 814–818. https://doi.org/10.1038/nature03607 (2005).
Barabási, A. L. Network science. Philos. Trans. R. Soc. Math. Phys. Eng. Sci. 371, 20120375 (2013).
Nguyen, A. D. k-Clique Algorithm MATLAB Central File Exchange (MATLAB Central File Exchange, 2024).
Abdi, H. & Williams, L. J. Principal component analysis. Wiley Interdiscipl. Rev. Comput. Stat. 2, 433–459 (2010).
Kaiser, H. F. Computer program for varimax rotation in factor analysis. Educ. Psychol. Meas. 19, 413–420 (1959).
Brier, G. W. Verification of forecasts expressed in terms of probability. Mon. Weather Rev. 78, 1–3 (1950).
Pencina, M. J., D’Agostino Sr, R. B., D’Agostino, R. B. & Vasan, R. S. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat. Med. 27, 157–172 (2008).
Derényi, I., Palla, G. & Vicsek, T. Clique percolation in random networks. Phys. Rev. Lett. 94, 160202. https://doi.org/10.1103/PhysRevLett.94.160202 (2005).
Porter, M. A., Onnela, J. P. & Mucha, P. J. Communities in networks. Not. Am. Math. Soc. 56, 1082–1097 (2009).
Fortunato, S. Community detection in graphs. Phys. Rep. 486, 75–174. https://doi.org/10.1016/j.physrep.2009.11.002 (2010).
Katopodis, P., Pappas, E. M. & Katopodis, K. P. Acid-base abnormalities and liver dysfunction. Ann. Hepatol. 27, 100675. https://doi.org/10.1016/j.aohep.2022.100675 (2022).
Walsh, T. S., Mc Lellan, S., Mackenzie, S. J. & Lee, A. Hyperlactatemia and pulmonary lactate production in patients with fulminant hepatic failure. Chest 116, 471–476. https://doi.org/10.1378/chest.116.2.471 (1999).
Yudkin, J. & Cohen, R. D. The contribution of the kidney to the removal of a lactic acid load under normal and acidotic conditions in the conscious rat. Clin. Sci. Mol. Med. 48, 121–131 (1975).
Bellomo, R. Bench-to-bedside review: lactate and the kidney. Crit. Care 6, 322–326. https://doi.org/10.1186/cc1518 (2002).
Bihari, D., Gimson, A. E., Lindridge, J. & Williams, R. Lactic acidosis in fulminant hepatic failure. Some aspects of pathogenesis and prognosis. J. Hepatol. 1, 405–416. https://doi.org/10.1016/s0168-8278(85)80778-9 (1985).
Bernal, W., Donaldson, N., Wyncoll, D. & Wendon, J. Blood lactate as an early predictor of outcome in Paracetamol-induced acute liver failure: a cohort study. Lancet 359, 558–563. https://doi.org/10.1016/s0140-6736(02)07743-7 (2002).
Riordan, S. M. & Williams, R. Blood lactate and outcome of Paracetamol-induced acute liver failure. Lancet 360, 573. https://doi.org/10.1016/s0140-6736(02)09729-5 (2002).
Bernal, W. Lactate is important in determining prognosis in acute liver failure. J. Hepatol. 53, 209–210. https://doi.org/10.1016/j.jhep.2010.02.017 (2010).
Schmidt, L. E. & Larsen, F. S. Blood lactate as a prognostic marker in acetaminophen-induced acute liver failure. Hepatology 37, 1199–1201. https://doi.org/10.1002/hep.510370530 (2003).
Alcorn, J. Arterial blood lactate measurements quickly identified risk for death from Paracetamol-induced liver failure. ACP J. Club 137, 117 (2002).
Scheiner, B. et al. Acid-base disorders in liver disease. J. Hepatol. 67, 1062–1073. https://doi.org/10.1016/j.jhep.2017.06.023 (2017).
Bihari, D., Gimson, A. E. S., Lindridge, J. & Williams, R. Lactic acidosis in fulminant hepatic failure: some aspects of pathogenesis and prognosis. J. Hepatol. 1, 405–416. https://doi.org/10.1016/S0168-8278(85)80778-9 (1985).
Mikael, L. et al. Are there differences in the relationship between respiratory rate and oxygen saturation between patients with COVID-19 and those without COVID-19? Insights from a cohort-based correlational study. Emerg. Med. J. 40, 805. https://doi.org/10.1136/emermed-2022-212882 (2023).
Mower, W. R., Sachs, C., Nicklin, E. L., Safa, P. & Baraff, L. J. A comparison of pulse oximetry and respiratory rate in patient screening. Respir. Med. 90, 593–599. https://doi.org/10.1016/S0954-6111(96)90017-7 (1996).
Oyelade, T. et al. Heart rate turbulence predicts survival independently from severity of liver dysfunction in patients with cirrhosis. Front. Physiol. 11, 602456 (2020).
Tan, Y. Y., Montagnese, S. & Mani, A. R. Organ system network disruption is associated with poor prognosis in patients with chronic liver failure. Front. Physiol. 11, 983 (2020).
D’Amico, G., Garcia-Tsao, G. & Pagliaro, L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J. Hepatol. 44, 217–231 (2006).
Asrani, S. K. & Kamath, P. S. Natural history of cirrhosis. Curr. Gastroenterol. Rep. 15, 1–6 (2013).
Geiger, B. C. & Kubin, G. Relative information loss in the PCA. In Proceedings of the IEEE Information Theory Workshop 562–566 (2012).
National Institute of Diabetes and Digestive and Kidney Diseases. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury (National Institute of Diabetes and Digestive and Kidney Diseases, 2012).
Hinson, J. A., Roberts, D. W. & James, L. P. Mechanisms of acetaminophen-induced liver necrosis. Handb. Exp. Pharmacol. 1, 369–405. https://doi.org/10.1007/978-3-642-00663-0_12 (2010).
Yang, R. et al. Alanine aminotransferase and bilirubin dynamic evolution pattern as a novel model for the prediction of acute liver failure in drug-induced liver injury. Front. Pharmacol. 13, 1 (2022).
Larsen, F. S., Hansen, B. A. & Blei, A. T. Intensive care management of patients with acute liver failure with emphasis on systemic hemodynamic instability and cerebral edema: a critical appraisal of pathophysiology. Can. J. Gastroenterol. 14, 105–111. https://doi.org/10.1155/2000/493629 (2000).
Oldenbeuving, G. et al. A patient with acute liver failure and extreme hypoglycaemia with lactic acidosis who was not in a coma: causes and consequences of lactate-protected hypoglycaemia. Anaesth. Intens. Care 42, 507–511. https://doi.org/10.1177/0310057x1404200413 (2014).
Record, C. O., Iles, R. A., Cohen, R. D. & Williams, R. Acid-base and metabolic disturbances in fulminant hepatic failure. Gut 16, 144–149. https://doi.org/10.1136/gut.16.2.144 (1975).
Talari, K. & Goyal, M. Retrospective studies–utility and caveats. J. R. Coll. Phys. Edinb. 50, 398–402 (2020).
Moss, T. J. et al. Signatures of subacute potentially catastrophic illness in the ICU: model development and validation. Crit. Care Med. 44, 1639–1648. https://doi.org/10.1097/ccm.0000000000001738 (2016).
Gheorghita, M. et al. Reduced oxygen saturation entropy is associated with poor prognosis in critically ill patients with sepsis. Physiol. Rep. 10, e15546 (2022).
Acknowledgements
We would like to extend our gratitude to Prof Sara Montagnese for her advice regarding assessment of hepatic encephalopathy in patients with acute liver failure.
Author information
Authors and Affiliations
Contributions
T.O., K.P.M., and A.R.M. contributed to the conceptualization. TO. contributed to clinical data extraction. T.O. and A.R.M. contributed to the formal analysis and software development. A.R.M. contributed to the supervision. T.O., A.R.M., and K.P.M. contributed to the writing, review, and editing of the manuscript. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Oyelade, T., Moore, K.P. & Mani, A.R. Application of physiological network mapping in the prediction of survival in critically ill patients with acute liver failure. Sci Rep 14, 23571 (2024). https://doi.org/10.1038/s41598-024-74351-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-74351-2
