
Abstract
The present study aimed to investigate the effects of collaborative pain management by healthcare providers on sleep quality and self-efficacy in perioperative lumbar disc herniation patients. A total of 300 lumbar disc herniation patients admitted to our hospital from February 2022 to February 2023 were selected as the research subjects. They were divided into a study group (receiving collaborative pain management by healthcare providers) and a control group (receiving conventional pain management), with 150 patients in each group. Surgical parameters, pain levels at different time points, as well as pre- and post-intervention pain levels, sleep quality, self-efficacy, lumbar function, patients’ satisfaction, and psychological status were compared between the two groups. There were no significant differences between the two groups in terms of gender, age, smoking, alcohol consumption, body mass index, disease duration, type and location of lumbar disc herniation, and comorbidities (P > 0.05). Surgical duration, blood loss, and time to first meal did not significantly differ between the two groups (P > 0.05). However, the study group had significantly shorter times to first ambulation, first gas passage, first bowel movement, and length of hospital stay compared to the control group (P < 0.05). Pre-intervention comparisons of pain levels showed no significant differences between the two groups (P > 0.05). Postoperatively, at 12, 24, 48, and 72 h, the study group had lower pain levels than the control group, with statistically significant differences (P < 0.05). Pre-intervention comparisons of daytime dysfunction, hypnotic drug use, sleep disturbances, sleep efficiency, sleep duration, time to fall asleep, and sleep quality revealed no significant differences between the two groups (P > 0.05). However, post-intervention, the study group exhibited significantly lower PSQI scores in daytime dysfunction, hypnotic drug use, sleep disturbances, sleep efficiency, sleep duration, time to fall asleep, and sleep quality compared to the control group (P < 0.05). Pre-intervention comparisons of pain management, physical function, and symptom coping showed no significant differences between the two groups (P > 0.05). After intervention, the study group demonstrated significantly better pain management, physical function, and symptom coping compared to the control group (P < 0.05). Before the intervention, subjective symptoms, bladder function, daily activity limitation, and clinical signs showed no significant differences between the two groups (P > 0.05). After the intervention, however, the study group exhibited significantly better subjective symptoms, bladder function, reduced daily activity limitation, and clinical signs compared to the control group (P < 0.05). Before the intervention, there were no significant difference in patients’ satisfaction, anxiety score, and depression score between the two groups (P > 0.05). After the intervention, the study group showed lower anxiety score and depression score, and higher satisfaction with the nursing intervention compared to the control group (all P < 0.05). Collaborative pain management by healthcare providers can effectively improve sleep quality and enhance self-efficacy in perioperative lumbar surgery patients, and holds promise for clinical application.
Similar content being viewed by others
Introduction
Relevant statistics indicate that lumbar disc herniation is a common orthopedic disorder1, with approximately 5.7 million patients diagnosed with intervertebral disc degeneration in the United States annually, while the number in China is several times higher. Lumbar disc herniation is one of the prevalent diseases in spinal surgery, primarily resulting from degeneration of the lumbar intervertebral disc composed of the cartilaginous endplate, fibrous ring, and nucleus pulposus, leading to fibrous ring rupture and gradual protrusion of the nucleus pulposus. This condition manifests as a syndrome caused by irritation and compression of the cauda equina and nerve roots. Although most patients can achieve good treatment outcomes through conservative therapy, approximately 20% of patients have suboptimal responses to conservative treatment and require surgical intervention. The use of an analgesic pump postoperatively is an effective method for pain control. However, due to the specific nature of lumbar disc herniation surgery, where the surgical procedure is in close proximity to the dura mater and nerve roots, there is a risk of damaging the cauda equina and nerve roots, resulting in severe consequences. Therefore, the observation of lower limb motor function and sensation is a crucial aspect of postoperative care for lumbar disc herniation2,3. Because an analgesic pump can influence the early observation of lower limb motor function and sensation, selecting an appropriate analgesic method is of paramount importance in the management of such conditions4.
Collaborative pain management by healthcare providers is a novel service model for pain management, based on the cooperation of medical and nursing personnel under the guidance of an anesthesiologist, aimed at preventing, monitoring, and alleviating patient pain while enhancing the communication and coordination skills of medical and nursing staff5. Currently, nursing interventions involving collaborative pain management are primarily limited to fields such as cardiothoracic surgery nursing, with minimal research on their application in lumbar surgery patients. Given this context, this study sought to explore the effects of collaborative pain management by healthcare providers on sleep quality and self-efficacy in perioperative lumbar surgery patients.
Materials and methods
General information
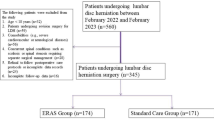
This is a prospective study. A total of 300 lumbar disc herniation patients admitted to our hospital from February 2022 to February 2023 were analyzed. They were randomly divided into a study group and a control group using a random number table method, with 150 patients in each group. In the study group, there were 84 males and 66 females, with an age range of 35–71 years and a mean age of (51.78 ± 15.38) years. In the control group, there were 79 males and 71 females, with an age range of 35–70 years and a mean age of (51.65 ± 15.31) years. This study protocol was approved by the Ethics Committee of The Third Hospital of Hebei Medical University. All participants received written and oral information prior to giving written consent, and the study was performed in accordance with the Helsinki II declaration.
Inclusion and exclusion criteria
Inclusion criteria
Patients were diagnosed according to the diagnostic criteria for lumbar disc herniation in the Diagnosis and Treatment Guidelines for Lumbar Disc Herniation6; Patients were eligible for percutaneous transforaminal endoscopic lumbar discectomy, with no surgical contraindications; Patients were well-informed and provided informed consent.
Exclusion criteria
Pregnant or lactating women; Patients with concomitant lumbar vertebral tuberculosis, tumors, or fractures; Patients with severe compression of the cauda equina due to nucleus pulposus protrusion; Patients with severe dysfunction of vital organs such as the heart, lungs, liver, and kidneys; Patients with severe mental disorders, cognitive impairments, or consciousness disorders; Patients with a history of previous lumbar surgery; Patients who could not tolerate or experience severe complications; Incomplete or unsuccessful surgery.
Methods
Patients were placed on different floors divided by the interventions used to avoid mutual contact and communication between the two groups. The patients were informed of the strategy concerning pain management they received without knowing about the measure of pain management in the other group. The same preoperative multimodal education was carried out in both groups. The preoperative and postoperative related contents of lumbar disc herniation, surgical methods, anesthesia methods, the application of analgesic pump, and the necessity of postoperative rehabilitation training were taught through special lectures, face-to-face communication, brochure or multimedia methods. The relevant matters and cooperation during the perioperative period were informed, and psychological nursing was given to reduce the anxiety and fear of patients.
Control group - conventional pain management
Nursing staff distributed health education brochures to patients, provided explanations about pain management and analgesic medications, and guided patients in maintaining a healthy diet. Pain relief was administered according to medical orders. Nursing staff also provided instructions on the operation of the patient-controlled analgesia pump (PCA pump). Patients were instructed to inform the nursing staff when experiencing significant pain, who then reported to the specialized physician for further pain management.
Study group - collaborative pain management by healthcare providers
The specific procedures were as follows: (1) Establishment of a collaborative pain management team, consisting of an orthopedic surgical director, a pharmacist, a pain medicine physician, a rehabilitation physician, an orthopedic head nurse, 12 nursing staff members, and a psychological counselor. Anesthesiologists provided training to the nursing staff on pain assessment, non-pharmacological and pharmacological pain management, and other relevant knowledge. The training involved practical scenarios to enhance the practical skills of medical and nursing personnel as well as their coordination abilities. A competency assessment was conducted to ensure that nursing staff were proficient and capable of independent pain management. Nursing staff managed mild pain, while specialized physicians managed moderate pain. The team members collectively discussed factors contributing to postoperative pain in patients and formulated tailored preventive interventions. A 24-hour pain hotline was established for patient convenience. (2) Preoperative intervention: Advanced pain management was administered 8 h before surgery according to the patient’s condition. Patients and their families received health education lectures on perioperative pain related to lumbar surgery to enhance the patient’s pain awareness. (3) Intraoperative intervention: Anesthesiologists personalized anesthesia induction and maintenance protocols based on the patient’s data, using different anesthesia drugs and dosages. (4) Postoperative intervention: Under the guidance of the team leader, physicians and nursing staff jointly conducted an assessment of the pain relief and sedation needs of patients during the perioperative period. The management goal was to ensure that patients were calm, comfortable, and cooperative. Postoperatively, nursing staff assessed the patient’s pain level using the Visual Analog Scale (VAS)7. For patients with mild postoperative pain, nursing staff provided non-pharmacological pain relief interventions such as abdominal breathing, music therapy, distraction techniques, and psychological suggestions based on the patient’s condition. For patients with moderate postoperative pain, nursing staff reported to the attending physician, who assessed and administered appropriate oral analgesics. For patients with severe postoperative pain, an anesthesiologist developed a pain management plan, guided nursing staff in pain management, and participated in patient rounds. They also instructed patients on the correct use of PCA and monitored the pain relief’s effectiveness and any adverse reactions. Any necessary adjustments to the treatment plan were made promptly, with a focus on close monitoring and observation. The nursing process continued until the patient’s discharge.
Observation measures
Observation measures included comparison of surgical conditions, pain levels at different time points, pain levels before and after intervention, sleep quality, self-efficacy, and lumbar function between the two groups.
Pain levels
Pain levels were assessed before and after the intervention using the VAS7, which scores pain on a scale from 0 to 10 points, with higher scores indicating more pronounced pain.
Self-efficacy
Self-efficacy was evaluated before and after the intervention using the Chronic Pain Self-Efficacy Scale (CPSS)8, which includes three dimensions: pain management, physical function, and symptom coping over three months. The scoring ranges for each dimension were 5–25, 9–45, and 8–40, respectively, with higher scores indicating higher self-efficacy levels.
Sleep quality
Sleep quality was assessed before and after the intervention using the Pittsburgh Sleep Quality Index (PSQI)9, which comprises seven dimensions: daytime dysfunction, use of sleep medication, sleep disturbances, sleep efficiency, sleep duration, time to fall asleep, and sleep quality. Each dimension was scored on a scale from 0 to 3, with higher scores indicating poorer sleep quality.
Lumbar function
Lumbar function was evaluated before and after the intervention using the Japanese Orthopaedic Association Score (JOA)10,11, which covers four aspects: subjective symptoms, bladder function, limitations in daily activities, and clinical signs. Each aspect was scored within specific ranges, which is 0–9, 0–6, 0–14, and 0–2 respectively, with higher scores indicating better recovery of lumbar function.
Psychological status
Self-rating anxiety scale (SAS) contained 20 items, which were used to assess the anxiety of patients12. Less than 50 points was defined as no anxiety, 50–59 points was divided into mild anxiety, 60–69 points was classified as moderate anxiety, and a score above 70 was considered severe anxiety. Self-rating depression scale (SDS) contained 20 items, which were used to assess the depression of patients13. Less than 53 points was defined as no depression, 53–62 points was divided into mild anxiety, 63–72 points was classified as moderate anxiety, and a score above 73 was considered severe anxiety.
Satisfaction
The Nursing job satisfaction Scale for Inpatients was used14. The scale included 20 items in 4 dimensions of communication (5 items), system (5 items), service (5 items) and environment (5 items). Likert5 grading method was used to score 1–5 points from very dissatisfied to very satisfied. The average score of each dimension was calculated. The Cronbach’s α coefficient of the scale was 0.9534, which had good reliability. At discharge, the patient satisfaction questionnaire was distributed by the investigators of the service quality office of the hospital, and filled in by the patients anonymously. The investigators were only responsible for the interpretation of the questionnaire content, and it was not allowed to induce patients to choose the answer.
Statistical analysis
Data analysis was performed using SPSS 21.0 statistical software. For continuous variables that followed a normal distribution, means and standard deviations (x̄± s) were used for representation, and group comparisons were made using independent samples t-tests or one-way analysis of variance (ANOVA). For continuous variables that did not follow a normal distribution, medians (quartiles) [M (P25, P75)] were used, and group comparisons were carried out using Mann-Whitney analysis or Kruskal-Wallis tests. Categorical data were presented as counts and percentages [n (%)], and group comparisons were performed using chi-squared tests or Fisher’s exact probability test. Confounding factors were adjusted in the statistical analyses. A significance level of P < 0.05 was used to determine statistical significance.
Results
Comparison of general characteristics between the two groups
The comparison of general characteristics between the two groups, including gender, age, smoking, alcohol consumption, body mass index, duration of illness, type and site of lumbar disc herniation, and comorbidities, showed no significant differences (P > 0.05), as laid out in Table 1.
Comparison of surgical conditions between the two groups
Surgical duration, blood loss, and time to first meal did not significantly differ between the two groups (P > 0.05). However, the study group had significantly shorter times to first ambulation, first gas passage, first bowel movement, and length of hospital stay compared to the control group (P < 0.05). (Table 2)
Comparison of pain severity at different times in both groups
Before the intervention, there was no significant difference in pain severity between the two groups (P > 0.05). However, at 12 h, 24 h, 48 h, and 72 h after the surgery, the study group had lower pain severity compared to the control group, and the differences were statistically significant (P < 0.05). (Table 3).
Comparison of sleep quality in both groups
Before the intervention, no significant differences were found in daytime dysfunction, use of sleep-inducing medications, sleep disturbances, sleep efficiency, sleep duration, time to fall asleep, and sleep quality between the two groups (P > 0.05). However, after the intervention, the study group had significantly lower PSQI scores in daytime dysfunction, use of sleep-inducing medications, sleep disturbances, sleep efficiency, sleep duration, time to fall asleep, and sleep quality compared to the control group (P < 0.05). (Table 4).
Comparison of self-efficacy in both groups
Pre-intervention comparisons of pain management, physical function, and symptom coping showed no significant differences between the two groups (P > 0.05). After the intervention, the study group demonstrated significantly better pain management, physical function, and symptom coping compared to the control group (P < 0.05). (Table 5).
Comparison of lumbar function in both groups
Before the intervention, we observed no significant differences in subjective symptoms, bladder function, daily activity limitations, and clinical signs between the two groups (P > 0.05). However, after the intervention, the study group had significantly higher JOA scores in these parameters compared to the control group, and the differences were statistically significant (P < 0.05). (Table 6).
Comparison of psychological status in both groups
There were no differences in anxiety score and depression score between the two groups before the intervention (P > 0.05, Table 7), while significant differences were observed in anxiety score and depression score after the intervention (P < 0.05).
Comparison of satisfaction in both groups
There were no differences in scores of nursing communication, nursing system, nursing service and nursing environment between the two groups before the intervention(P > 0.05, Table 8), while scores of the items in the study group was higher than those in the control group after the intervention (P < 0.05).
Discussion
Lumbar disc herniation is a common and frequently occurring disease in spine surgery, characterized by a long course and a tendency for recurrence, severely impacting the quality of life of patients. Most patients with lumbar disc herniation who require surgical treatment experience severe radiating back and leg pain before surgery, and conservative treatment often yields unsatisfactory results. As such, there is an urgent need for surgery to provide thorough pain relief15. After surgical treatment of lumbar disc herniation, complete relief of pain is achieved in approximately 80% of cases. However, surgery may also introduce incisional pain and, in some cases, lead to significant emotional distress in patients16. Therefore, how to achieve effective postoperative pain management in patients with lumbar disc herniation has always been a critical issue for healthcare professionals in orthopedics. Despite the use of various analgesic drugs, the results of pain management are often unsatisfactory. This study applied a pain management model involving collaborative care by medical and nursing staff to perioperative care for patients with lumbar disc herniation in orthopedics. The purpose was to explore the nursing effectiveness of the pain management care model, provide a reference for postoperative care for patients with lumbar disc herniation, achieve the best possible patient recovery, improve their quality of life, enhance comfort, and increase overall satisfaction with surgical outcomes.
Percutaneous puncture endoscopic surgery can effectively treat lumbar disc herniation patients17. Effective nursing interventions significantly alleviate postoperative pain and improve lumbar function, resulting in favorable patient outcomes18. Effective nursing interventions may shorten the time to first ambulation after surgery, time to discharge, alleviate patient pain, and improve lumbar function in patients with osteoporotic vertebral compression fractures19. This study revealed that the study group had significantly shorter times for the first postoperative ambulation, first gas passage, first bowel movement, and shorter hospital stay compared to the control group (P < 0.05). This suggests that pain management with collaborative involvement of both medical and nursing staff can effectively shorten the time for the first postoperative ambulation, first gas passage, first bowel movement, and the length of hospital stay for patients undergoing lumbar disc herniation surgery, as well as improve patient prognosis.
In recent years, pain has been recognized as the fifth vital sign, following blood pressure, temperature, respiration, and pulse. Pain management has become a critical area of research. Effectively implementing nursing interventions for perioperative pain in orthopedics significantly improved sleep disturbances20. This not only alleviated the intensity of pain and enhanced the quality of patient sleep but also promoted postoperative recovery20. Effective perioperative nursing interventions could effectively alleviate the pain intensity in patients undergoing degenerative lumbar surgery21. Based on our study, at 12, 24, 48, and 72 h after surgery, the study group had lower pain severity compared to the control group (P < 0.05), suggesting that collaborative pain management involving both medical and nursing staff can effectively alleviate pain severity in patients during the perioperative period of lumbar disc herniation surgery. The reasons for this may be attributed to the fact that collaborative pain management by healthcare providers maximizes the roles of physicians and nurses in providing nursing interventions during patient treatment. This model enables the attending physician and nursing staff to intervene with the patient from their respective perspectives and emphasizes the synergy between the medical and nursing staff. Medical and nursing staff jointly develop targeted and appropriate clinical care services for patients, thereby enhancing coordination. Preoperative health education in pain control improves the patient’s and family’s correct understanding of postoperative pain control. It corrects misconceptions about the addictive potential of analgesic drugs and provides preventive and multimodal pain management postoperatively, achieving effective pain relief through multiple modalities.
Patients in the perioperative period of lumbar spine surgery often experience reduced sleep quality due to factors such as pain and restricted mobility, which can affect their behavior. Therefore, postoperative sleep management for patients in the perioperative period of lumbar spine surgery is an important aspect of the work of healthcare providers. Sleep quality can impact patient prognosis, and high-quality sleep can accelerate patient recovery, improve their quality of life, and enhance their overall prognosis. Effective nursing interventions can improve the sleep quality of patients after lumbar disc herniation surgery and reduce pain severity22. Hu et al.23 reported that effective interventions can improve postoperative sleep quality following corrective surgery for ankylosing spondylitis. The results of this study showed that, after intervention, the study group had lower PSQI scores in daytime dysfunction, use of sleep medications, sleep disorders, sleep efficiency, sleep duration, time to fall asleep, and sleep quality compared to the control group (P < 0.05), indicating that collaborative pain management involving both medical and nursing staff can effectively improve the sleep quality of patients in the perioperative period of lumbar spine surgery. This may be partly because collaborative pain management by medical and nursing staff, in the implementation process, alleviates pain intensity, which can eliminate the cause of poor sleep quality.
Self-efficacy theory suggests that the relationship between an individual’s self-efficacy and their level of behavior is a dynamic development with mutual interaction and mutual promotion. The greater the self-efficacy an individual possesses, the higher the predictive ability and the greater the positive impact on the persistence and effort in their behavior. Patients with lumbar disc herniation may experience reduced psychological tolerance due to pain, restricted function, and symptoms such as limb numbness, which increase their stress, especially in patients with concurrent functional limitations, which can reduce their willingness to communicate with others, increase stress, and lead to reduced self-efficacy24. Effective nursing interventions can significantly improve the treatment outcomes of patients with lumbar postoperative syndrome25. These interventions can also reduce patient pain, improve lumbar function, and increase patient self-efficacy and quality of life. The results of this study demonstrated that, after intervention, the study group had better pain management, physical function, and symptom coping compared to the control group (P < 0.05). This indicates that collaborative pain management involving both medical and nursing staff can effectively increase pain management, physical function, and symptom coping in patients in the perioperative period of lumbar spine surgery, enhancing their self-efficacy. These results may be because in the implementation process, medical and nursing staff work together to provide targeted pain management interventions according to the patient’s pain intensity. They also combine health education interventions, effectively adjusting patient compliance, and thereby enhancing self-efficacy. Research conducted by Gong Shuwei and others indicated that targeted nursing interventions can enhance the lumbar spine function of postoperative lumbar patients. Our study showed that, after the intervention, the study group exhibited fewer subjective symptoms, improved bladder function, fewer restrictions in daily activities, and fewer clinical signs compared to the control group (P < 0.05). This suggests that collaborative pain management involving both medical and nursing staff can effectively alleviate subjective symptoms, improve bladder function, reduce limitations in daily activities, and improve clinical signs in patients in the perioperative period of lumbar spine surgery, thus aiding the recovery of lumbar spine function. The reason for this may be that in the process of implementing collaborative pain management, a well-established mechanism of medical-nursing coordination and communication is established. This includes forming nursing intervention teams, providing joint training for medical and nursing staff, making collaborative assessments and decisions, and jointly intervening in patient care. By enhancing effective medical-nursing communication and cooperation, they are able to share their respective treatment and nursing tasks without lacking communication. This approach provides patients with a collaborative, integrated, and systematic medical service process, ultimately leading to effective recovery of lumbar spine function.
The effect of surgery on lumbar disc herniation is clear. However, due to the influence of symptoms and the general fear of surgical treatment, patients often have negative emotions such as anxiety and depression during the perioperative period, which affects the efficacy of patients26. There were no differences in anxiety score and depression score between the two groups before the intervention, indicating our measures to avoid bias arising from psychological effect worked. Yuksel et al.26 found that nursing intervention can effectively improve the psychological state of patients with lumbar disc herniation. Tang et al.27 found that the application of effective nursing intervention in patients with lumbar disc herniation can improve lumbar function, relieve pain symptoms and improve the psychological state of patients. The study showed that anxiety score and depression score in the study group was lower than those in the control group after the intervention, indicating that collaborative pain management by healthcare providers could effectively reduce the anxiety and depression scores of patients during the perioperative period of lumbar surgery, improve the psychological state of patients, and increase the confidence of patients in the treatment of diseases. In the implementation process of collaborative pain management by healthcare, medical staff coordinated and cooperated to provide patients with health education lectures on perioperative pain of lumbar spine surgery before operation and answer the patients’ questions, which strengthened the patients’ cognition of pain, effectively alleviated the patients’ fear of surgery, and improved the patients’ psychological state. The study also showed that patients’ satisfaction was higher in the study group than that in the control group after the intervention, suggested that suggested that collaborative pain management by healthcare can effectively improve the scores of nursing communication, nursing system, nursing service and nursing environment for patients during lumbar spine perioperative period, and improve the nursing satisfaction of patients. In the implementation process of collaborative pain management by healthcare, doctors and nurses adopted a proactive attitude to communicate with patients, and effectively relieved the pain of patients, which were beneficial for improving patients’ satisfaction.
In summary, collaborative pain management involving both medical and nursing staff can effectively alleviate pain levels, improve sleep quality, enhance self-efficacy, restore lumbar spine function, and enhance prognosis in patients in the perioperative period of lumbar spine surgery. It promotes patient recovery and can be applied in clinical practice. However, this study also has its limitations. Collaborative pain management increases the involvement of anesthetists and thus places higher demands on their professionalism and increases their workload. Anesthetists need to manage their time more efficiently.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Zhang, A. S. et al. Lumbar disc herniation: diagnosis and management. Am. J. Med. 136 (7), 645–651 (2023).
Ji, C. et al. Exploring the efficacy of intervertebral fusion and nucleus pulposus removal in treating various grades of disc herniation and assessing the significance of lumbar spine rehabilitation care. Altern. Ther. Health Med. 29 (8), 576–581 (2023).
Sınmaz, T. & Akansel, N. Experience of Pain and satisfaction with Pain Management in patients after a lumbar disc herniation surgery. J. Perianesthesia Nurs. Off. J. Am. Soc. PeriAnesthesia Nurses 36 (6), 647–655 (2021).
Sajko, T., Rotim, K., Kurtovic, B., Rotim, C. & Rotim, A. Prospective randomized appraisal of the best pain relief option after L4/L5 discectomy. Neurol. Res. 42 (12), 1003–1009 (2020).
Manietta, C., Labonté, V., Thiesemann, R., Sirsch, E. G. & Möhler, R. Algorithm-based pain management for people with dementia in nursing homes. Cochrane Database Syst. Rev. 4 (4), Cd013339 (2022).
Cheng, Z. X. et al. Chinese association for the study of pain: Expert consensus on diagnosis and treatment for lumbar disc herniation. World J. Clin. Cases 9 (9), 2058–2067 (2021).
Chiarotto, A. et al. Measurement properties of visual analogue scale, numeric rating scale, and pain severity subscale of the brief pain inventory in patients with low back pain: a systematic review. J. Pain 20 (3), 245–263 (2019).
Cheng, S. T. et al. Developing a short multidimensional measure of pain self-efficacy: the chronic pain self-efficacy scale-short form. Gerontologist 60 (3), e127–e136 (2020).
Han, Q. et al. Pittsburgh sleep quality Index score predicts all-cause mortality in Chinese dialysis patients. Int. Urol. Nephrol. 53 (11), 2369–2376 (2021).
Oshima, Y., Takeshita, K., Kato, S., Doi, T. & Matsubayashi, Y. Comparison between the Japanese orthopaedic association (JOA) score and patient-reported JOA (PRO-JOA) score to evaluate surgical outcomes of degenerative cervical myelopathy. Global Spine J. 12 (5), 795–800 (2022).
Abouammoh, M. A. Advances in the treatment of central serous chorioretinopathy. Saudi J. Ophthalmol. 29 (4), 278–286 (2015).
Dunstan, D. A. & Scott, N. Norms for Zung’s self-rating anxiety scale. BMC Psychiatry 20 (1), 90 (2020).
Xie, W., Liang, L., Lu, Y., Luo, H. & Liu, X. Deep 3D-CNN for depression diagnosis with facial video recording of self-rating depression scale questionnaire. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2007–2010 (2021).
Dong, C. L. W. Application of multidisciplinary teamwork combined with enhanced recovery after surgery in perioperative period of patients with lumbar disc herniation. Chin. J. Mod. Nurs. 25 (2), 137–141 (2019).
Zhu, H. et al. Percutaneous endoscopic lumbar discectomy for lumbar disc herniation with type II modic changes. World Neurosurg. 164, e143–e149 (2022).
Migliorini, F. et al. Ozone injection therapy for intervertebral disc herniation. Br. Med. Bull. 136 (1), 88–106 (2020).
Li, P. & Yang, F. Percutaneous transforaminal endoscopic discectomy for different types of lumbar disc herniation: a retrospective study. J. Int. Med. Res. 49 (10), 3000605211055045 (2021).
Wang, Y., Shen, Q. & Wang, C. Efficacy of rapid rehabilitation nursing in postoperative care in China: a meta-analysis. Rehabil.Nurs. Off. J. Assoc. Rehabil. Nurses 48 (5), 170–179 (2023).
Svensson, H. K., Olsson, L. E., Hansson, T., Karlsson, J. & Hansson-Olofsson, E. The effects of person-centered or other supportive interventions in older women with osteoporotic vertebral compression fractures-a systematic review of the literature. Osteoporos. Int. J. Establ. Result Coop. Eur. Foundation Osteoporos. Natl. Osteoporos. Foundation U. S. A. 28 (9), 2521–2540 (2017).
Simpson, M. H. & Bruckenthal, P. The current state of perioperative pain management: challenges and potential opportunities for nurses. AORN J. 104 (6s), S1–s8 (2016).
Punnoose, A. et al. Prehabilitation for patients undergoing orthopedic surgery: a systematic review and meta-analysis. JAMA Netw. Open 6 (4), e238050 (2023).
Zarei, B., Valiee, S., Nouri, B., Khosravi, F. & Fathi, M. The effect of multimedia-based nursing visit on preoperative anxiety and vital signs in patients undergoing lumbar disc herniation surgery: a randomised clinical trial. J. Perioper. Pract. 28 (1–2), 7–15 (2018).
Hu, F. et al. Improvement of sleep quality in patients with Ankylosing Spondylitis Kyphosis after corrective surgery. Spine 45 (23), E1596–e1603 (2020).
Hornung, A. L. & Baker, J. D. Resorption of lumbar disk herniation: mechanisms, clinical predictors, and future directions. JBJS Rev. 11(1). (2023).
Huan, X., Wu, L., Wang, M., Xue, D. & Tian, F. The effect of electronic moxibustion combined with rehabilitation nursing on the lumbar pain and stiffness of ankylosing spondylitis patients. Am. J. Transl. Res. 13 (5), 5452–5459 (2021).
Yuksel, A., Cetinkaya, F. & Karakoyun, A. The effect of mindfulness-based therapy on psychiatric symptoms, psychological well-being, and pain beliefs in patients with lumbar disk herniation. Perspect. Psychiatr. Care 57 (1), 335–342 (2021).
Tang, P., Zheng, Y. & Ouyang, Y. Application of multidisciplinary teamwork combined with enhanced recovery after surgery in perioperative period of patients with lumbar disc herniation. Chin. Forgein Med. Res. 21 (33), 94–97 (2023).
Funding
This study was funded by Hebei Provincial Health Department youth science and technology project (No. 20150723).
Author information
Authors and Affiliations
Contributions
Jucai Li and Shu’e Zhao contributed to the conception and design of the study. All authors participated in the clinical practice, including diagnosis, treatment, consultation and follow up of patients. Yanli Song and Yixin Zhao contributed to the acquisition of data. Dan Su and Meina Li contributed to the analysis of data. Jucai Li wrote the manuscript. Shu’e Zhao revised the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study protocol was approved by the Ethics Committee of The Third Hospital of Hebei Medical University. All participants received written and oral information prior to giving written consent, and the study was performed in accordance with the Helsinki II declaration.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, J., Song, Y., Zhao, Y. et al. The impact of collaborative pain management by healthcare providers on sleep quality and self-efficacy in perioperative lumbar surgery patients. Sci Rep 15, 5397 (2025). https://doi.org/10.1038/s41598-024-83927-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-83927-x
