
Abstract
Spontaneous bleeding into soft tissues was a common complication of anticoagulant therapy among critically ill patients during the COVID-19 pandemic. This study sought to evaluate the impact of different treatment methods on survival among COVID-19 patients with active or self-resolved spontaneous bleeding into soft tissues. Methods used to treat CT-confirmed spontaneous hematomas in COVID-19 patients included nonoperative management (NOM), angiography (AG) with transarterial embolization (TAE) and open surgery (OS). A total of 227 participants with spontaneous hematomas into soft tissues were enrolled in this retrospective single-center study at a COVID-19-hospital between March 3, 2020 and March 3, 2022. NOM was used in 144 patients, including 51 patients with extravasation on CT; 60 patients with extravasation on CT were subjected to AG, which was followed by TAE in 41 patients. Open surgery was performed on 23 patients. The choice of treatment strategy did not have any effect on 30-day mortality among patients with extravasation. Mortality did not differ between the OS, NOM and AG/AG+TAE groups (p = 0.094). In the multivariate logistic regression model, OS and NOM did not increase the risk of death, in comparison with AG, respectively (OR 1.53 [95% CI: 0.35-7.37]; p = 0.579 and OR 1.39 [95% CI: 0.53–3.72]; p = 0.501).
Similar content being viewed by others
Introduction
Spontaneous bleeding (hematomas) into the anterior abdominal wall, retroperitoneal space or other soft tissues is a common complication of anticoagulant therapy1.
Before the COVID-19 pandemic, reports of spontaneous hematomas were sporadic, and the total number of observations did not exceed a few hundred2,3.
During the pandemic, administration of therapeutic doses of anticoagulants to COVID-19 patients with no previous exposure to these medications increased the incidence of spontaneous soft tissue bleeding and worsened their prognosis4,5.
According to some reports, bleeding into soft tissues often develops in patients with severe COVID-19, impaired mental status and immobility that complicate its timely diagnosis6. The main diagnostic test for spontaneous bleeding is a CT scan; it can detect the presence of active bleeding and determine the size of the hematoma. Extravasation of a contrast agent into a hematoma is recognized as a radiographic criterion of ongoing bleeding7. However, the clinical significance of extravasation in patients with spontaneous bleeding may require additional study.
Non-operative management is the preferred treatment option for spontaneous hematomas8. Extravasation of a contrast agent, hemodynamic instability and a progressive decrease in blood hemoglobin are indications for Transarterial Embolization (TAE)9. TAE is technically feasible in most patients, but there is no compelling evidence that it ensures better survival than nonoperative treatment. Besides, it is not clear what management tactic should be applied in the absence of obvious angiographic signs of extravasation. Embolization of the vessels suspicious for bleeding has been proposed in1. However, we have not found any publications that compare “preventive” embolization to nonoperative treatment. Open surgery is rarely performed for spontaneous hematomas in patients with COVID-19 and is associated with high mortality. Indications for open surgery are open to debate10.
The aim of the study was to evaluate the effect of different treatment methods on the survival rate of COVID-19 patients with ongoing or self-resolved spontaneous bleeding into soft tissues.
Materials and methods
This study was reviewed and approved by the Institutional Review Board (IRB). Written informed consent was obtained from all study participants. Ethics approval number for the study is 11 dated December 6, 2023. The study was conducted in accordance with the current guidelines and regulations.
In a previous study, we had evaluated the significance of specific CT features of coagulopathy in predicting the dynamics of spontaneous bleeding into soft tissues in 60 patients with COVID-1911. The current study with a larger patient sample expands on our previous work and analyzes survival.
This retrospective single-center study enrolled patients with spontaneous soft tissue bleeding admitted for COVID-19 to the hospital of Kommunarka Moscow Multidisciplinary Clinical Center (Russia) between March 1, 2020 and March 1, 2022. During the pandemic, about 55,000 patients with confirmed COVID-19 were treated at this hospital.
The following inclusion criteria were applied: patients of both sexes aged 18 years or older with confirmed COVID-19 and spontaneous bleeding into the abdominal and thoracic walls, retroperitoneal space or limbs confirmed by CT.
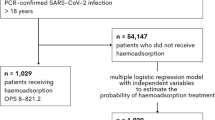
A total of 256 originally qualifying patients were evaluated for the exclusion criteria: patients with bleeding due to trauma or iatrogenic injury, intracavitary or parenchymal bleeding, incomplete CT examination (Fig. 1).

Study design. Angiography, AG; Nonoperative management, NOM.
Patient characteristics
A total of 227 patients were included in the study; data from their medical records was saved to an electronic database.
CT procedure
Two hundred seventeen patients (95.6%) underwent four-phase contrast-enhanced CT scans, 10 (4.4%) underwent nonenhanced CT scans. Accumulation of the contrast agent in the hematoma in any CT phase was considered extravasation.
All the patients underwent a 64 or 128-slice four-phase contrast-enhanced CT scan of the chest and the abdomen. The contrast agent (80–100 ml) was injected into a peripheral vein through a catheter at 4.0–4.5 ml/s using a syringe injector. Extravasation was defined as leakage of the contrast agent from a blood vessel’s lumen and its accumulation in soft tissues in the arterial (20–30 s) after bolus administration of the contrast agent), venous (40–60 s) or delayed (180 s) phase.
Management of bleeding
The following treatment modalities were used: nonoperative management (NOM), open surgery (OS) and angiography (AG) with transarterial embolization (TAE).
NOM was used in 144 (63.4%) patients: 93 patients without extravasation and 51 patients with extravasation confirmed by CT. Therapy included withdrawal of anticoagulants, blood transfusion and treatment of organ failure.
Transarterial angiography (AG) was performed in 60 (26.4%) patients with CT-confirmed extravasation. Of them, 41 patients underwent TAE.
Patients with hematomas of the anterior abdominal wall underwent selective angiography of the inferior epigastric artery. Patients with hematomas of the thoracic wall (the pectoralis major and the pectoralis minor muscles) underwent angiography of the thoracoacromial artery, lateral and internal thoracic arteries. Angiography of iliolumbar artery, the deep circumflex iliac artery and lumbar arteries was performed on patients with hematomas located in the retroperitoneal space (the iliopsoas muscle region). The procedures were conducted by 7 interventional radiologists with 2 to 25 years of professional experience. During angiography, extravasation was detected in 27 patients (45% of all the patients (n=60) subjected to AG). Those 27 patients received TAE (“therapeutic” embolization). In addition, 14 (23.3%) patients who had no signs of extravasation on AG underwent preventive embolization of a potential source of bleeding (“preventive” TAE). The rest 19 patients without signs of extravasation on AG did not undergo TAE.
The following equipment and materials were used for transarterial angiography: Innova IGS 530 System (General Electric Medical Systems, USA); Omnipaque 350 (General Electric Healthcare, USA) or Ultravist-370 (Bayer, Germany) contrast media. The target arteries were embolized with either microspheres delivered through diagnostic catheters (C1-2, JR, IM) or coils delivered through microcatheters. Microsphere embolization was performed on 30 (73.2%) patients, and coiling, on 9 (21.9%) patients. A combination of different embolizing agents was used on 1 (2.4%) patient.
Open surgery was performed on 23 (10.1%) patients; of them, 5 had no signs of extravasation on CT. The median time from CT to surgery was 617.5 (IQR=248.822) minutes.
Control of bleeding
The control of the hematoma size was performed after 6-12 hours by ultrasound in 153 (67.4%) patients. Initial NOM failed in 30 (26.5%) patients with CT-confirmed extravasation; these patients ended up having AG and TAE.
Object of study
In this work, we study the prognostic value of CT-confirmed extravasation and treatment methods for spontaneous bleeding into soft tissues in patients with COVID-19, including OS, NOM, AG with TAE. Clinical groups (NOM, AG/AG + TAE, OS) were compared by the size and location of the hematoma and by duration and severity of COVID-19. The severity of COVID-19 was evaluated using the Temporary Methodological Recommendations by the Russian Ministry of Health12. We also compared arterial blood pressure between the groups, their clinical laboratory parameters (Hb, etc.), severity of coagulopathy, the frequency of plasma transfusion, and some other parameters. The functional status and morbidity were compared using the NEWS2, APACHE II, and SOFA scoring systems.
Statistical analysis
The obtained data was analyzed in in Statistica 12 (StatSoft, Inc.) The results are presented below as mean values (M) and standard deviations (± SD) for continuous normally distributed variables, as medians (Me) and interquartile ranges [Q1; Q3] for continuous non-normally distributed data, and as absolute values and percentage for categorical data. Normality of distribution was tested using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Normally and non-normally distributed continuous variables were compared using Student’s t-test and the Mann–Whitney U-test, respectively.
Categorical data and proportions were compared between three groups of patients using Pearson’s χ 2 test and Pearson’s χ2 test with Yates correction. Analysis of variance (ANOVA) was applied to compare the average values of quantitative parameters. The significance of differences between pairs of groups was measured by post-hoc tests. Additionally, the analyzed data was corrected for multiple comparisons using the Holm-Bonferroni method. Correlations between the risk of 30-day mortality and a number of factors were studied using multivariate logistic regressions (LASSO-regression). The significance threshold was set at p <0.05.
Results
Mortality in the general group (n=227)
Mortality was significantly higher in the open surgery group, despite the fact that 19 patients were treated with reinfusion with 707.0 ± 497.4 (100.0–2070.0) ml of red blood cells. The analysis of cumulative mortality demonstrated that open surgery had significantly worse outcomes than AG (AG+TAE) and NOM.
Outcomes among patients with and without extravasation on CT
Blood loss, hematoma volume and mortality were significantly greater in patients with extravasation (Table 1).
Patients with extravasation were more likely to have organ dysfunction and die, although in terms COVID-19 pneumonia severity they were comparable to patients without extravasation (p=0.077). The multifactorial logistic regression analysis did not confirm the presence of significant differences in the odds of 30-day death between the groups (OR 1.75 [95% CI: 0.56-5.50], p=0.332). The correlation between hematoma volume (over or under 1000 ml) and the odds of death was not confirmed (OR 0.33 [95% CI: 0.08-1.21], p=0.107).
Outcomes among patients with CT-confirmed extravasation (n=129)
Table 2 compares the outcomes of NOM, open surgery and AG/AG+TAE among patients with CT-confirmed extravasation.
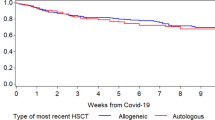
The AG/AG+TAE group was formed on the basis of the intention-to-treat principle: if a patient underwent open surgery after TAE, he/she was included in the TAE group. Similarly to the general group, the highest mortality rate was among patients undergoing open surgery. The NOM and AG/AG+TAE groups were similar (Table 2, Figs. 2, 3, 4) and did not differ significantly in terms of mortality rate.

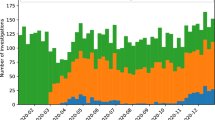
Distribution of patients by pneumonia severity. Note: ARDS, acute respiratory distress syndrome; CT, computed tomography; NOM, nonoperative management; OS, open surgery; AG/AG + TAE, angiography/angiography + transarterial embolization; bacterial pneumonia* (also includes patients with mixed pneumonia). The following grading scale was used to classify the severity of lung involvement: CT 0–0%, CT 1–1–25%, CT 2–26–50%, CT 3–51–75%, CT 4–76–100%.

Distribution of patients by severity of COVID-19. Note: NOM, nonoperative management; OS, open surgery; AG/AG + TAE, angiography/angiography + transarterial embolization.

Distribution of patients by hematoma location. Note: NOM, nonoperative management; OS, open surgery; AG/AG + TAE, angiography/angiography + transarterial embolization.
The risk of mortality did not depend on the method of treatment (Table 3).
Outcomes in the AG/AG+TAE group
There were no significant differences in mortality rates between the groups of therapeutic (n=27) and preventive embolization (n=14) and diagnostic angiography (n=19) due to the small size of the groups (Table 4).
Follow-up CT scans were performed on 17 (11.8%) patients from the NOM group and 13 (21.7%) patients after AG/AG+TAE on the first day after a primary CT scan. The frequency of hematoma growth and extravasation on the follow-up CT scans did not differ significantly between the NOM and the AG/AG+TAE groups (3.4% vs 10%; 2.1% vs 1.7%, respectively).
Risk of death among non-operated patients (n = 144)
Among non-operated patients, significant differences in the 30-day mortality rate were associated with increasing age by one year (OR 1.14 (95% CI: 1.07–1.23); p < 0.001), BMI (OR 1.1 (95% CI: 1.01–1.20); p = 0.038), grade 4 viral pneumonia and ARDS vs. grades 0–3 pneumonia (OR 29.32 (95% CI: 6.71–182.07); p < 0.001), decrease in hemoglobin by 1 g/l (OR 0.97 (95% CI: 0.94–0.99); p = 0.020), the need for vasopressor support at the time before the onset of bleeding (OR 18.69 (95% CI: 2.42–211.26); p = 0.009) and high NEWS2 scores (OR 1.28 (95% CI: 1.02–1.64); p = 0.036). The presence of CT-confirmed extravasation did not significantly affect the mortality rate among non-operated patients.
Discussion
Spontaneous bleeding into soft tissues is a rare complication of anticoagulant therapy in critically ill patients. Despite attention to this issue, indications for its treatment and predictors of mortality have not been clearly defined yet13.
Clinical characteristics of patients and episodes of bleeding
In this study, our average patient was a elderly overweight female with CT-confirmed extravasation into the rectus abdominis or iliopsoas muscles on day 10 after the commencement of anticoagulant therapy. We have not found any published reports on the sex characteristics of patients with spontaneous bleeding, including patients with COVID-19. It is reported that the rectus abdominis and lumbar muscles are the most common sites of spontaneous bleeding into soft tissues (hematomas)14. In our study, the third most common hematoma location (23% of patients) was the thoracic wall.
CT
CT features of ongoing bleeding are not always obvious. In this study, the presence of a contrast agent in the hematoma in any CT phase was interpreted as extravasation; the same principle had been previously used by other authors and in our early work11,15. In another recent study, ongoing bleeding was defined as extravasation of a contrast agent in the arterial phase that intensifies in the venous and delayed phases. Although some patients had no extravasation in the arterial phase, it was confirmed by angiography9.
Treatment of self-resolved massive bleeding
In the absence of active bleeding, NOM is an obvious treatment choice for patients with COVID-1916. In these patients, surgery under general anesthesia is associated with increased mortality10. NOM was used in most patients without extravasation on CT and accompanied by lower mortality. Open surgeries performed on 5 patients resulted in 3 deaths despite blood reinfusion. It is not clear how endovascular embolization can improve treatment results in patients with self-resolved bleeding. In another study, preventive TAE was successful in patients without extravasation on AG1.
Treatment outcomes in patients with CT-confirmed extravasation
Open surgery
In a recent study10, only 22% of operated patients with COVID-19 complicated by spontaneous hematomas survived. Due to high mortality, the authors recommended this method only as a last resort, but did not propose criteria for choosing surgical tactics. Unfortunately, mortality rates for open surgery were the same in our study, although those patients had severe organ dysfunction and extremely large hematomas. Blood reinfusion did not improve their condition. Open surgery should not be considered a treatment of choice for patients with COVID-19 even if extravasation is confirmed by CT.
Transarterial embolization (TAE)
Extravasation suspected on CT was confirmed by AG in 45% of patients. According to some reports, the diagnostic coincidence rate between CT and AG findings is quite high15,17,18. In our study, CT and AG findings coincided in 50% of patients with hematomas of the abdominal wall and retroperitoneal space and in only 20% of patients with thoracic wall hematomas. Perhaps, this can be explained by spontaneous hemostasis due to a local spasm, hypotension or self-tamponade1. Besides, the coincidence rate may depend on the accuracy of identifying the involved artery. Some authors recommend visualizing as many blood vessels suspicious for bleeding as possible in case of abdominal wall hematomas13,19.
In an earlier study, we analyzed specific CT signs (“hematocrit effect”, the “signal flare” phenomenon) to predict the outcomes and determine a clinical tactic in patients with spontaneous hematomas11. In that study, we concluded that "Extravasation on angiography was more often detected in patients if extravasation was confirmed on CT in the arterial phase than in the venous phase: 20 (51.3%) vs. 7 (41.2%) patients (p = 0.047)"11.
TAE versus NOM
Endovascular interventions are preferred over NOM due to their effectiveness and the low injury rate6,20. In our study, the outcomes of AG and NOM did not differ in terms of cumulative mortality. This can be explained by low mortality in patients without extravasation on CT and by the fact, that AG/AG + TAE was performed only on patients with extravasation. To exclude the influence of these two factors, further comparison was done in the group of patients with extravasation on CT. TAE is considered a life-saving procedure in case of active spontaneous bleeding into soft tissues21. Our study has not found any obvious advantage of endovascular technology, but the data we have is not sufficient for a comprehensive assessment of TAE significance.
Mortality
Mortality among our patients is probably the highest in comparison to other published studies (42%). Before the COVID-19 pandemic, the reported mortality from spontaneous bleeding into soft tissues was 27%9. It is unclear whether the observed 15% increase in mortality should be attributed to COVID-19. This study allowed us to formulate a response to the question about the leading cause of death13. Severity of a patient’s condition is the main risk factor of a bad clinical scenario. Mortality factors analyzed in various groups of patients did not correspond significantly with the volume of blood loss, the presence of active bleeding and the method of treatment.
Our study has limitations. It was a single-center retrospective study with a relatively small patient sample, so its results may have limited clinical significance for patients with COVID-19 receiving therapeutic doses of anticoagulants.
Mortality from spontaneous bleeding into soft tissues in patients with COVID-19 is largely associated with the severity of pneumonia. The heterogeneity of the groups does not allow us to make overarching conclusions or determine the optimal management strategy for spontaneous hematomas. Nevertheless, open surgery should not be considered a treatment of choice in such cases.
Data availability
Data is provided within the manuscript or supplementary information files. All the results and data of this study can be obtained from Dr. Polyaev A.Y. (apolyaev@yandex.ru) on a reasonable request.
References
Dohan, A. et al. Spontaneous soft-tissue hemorrhage in anticoagulated patients: Safety and efficacy of embolization. AJR Am. J. Roentgenol. 204(6), 1303–1310. https://doi.org/10.2214/AJR.14.12578 (2015).
Schulman, S., Beyth, R. J., Kearon, C. & Levine, M. N. Hemorrhagic complications of anticoagulant and thrombolytic treatment. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 133(6), 257S-298S. https://doi.org/10.1378/chest.08-0674 (2008).
Çolakoğlu, M. K. et al. Spontaneous abdomen and abdominal wall hematomas due to anticoagulant/antiplatelet use: Surgeons’ perspective in a single center. Ulus Travma Acil Cerrahi Derg. 26(1), 50–54. https://doi.org/10.14744/tjtes.2019.32485 (2020).
Hadid, T., Kafri, Z. & Al-Katib, A. Coagulation and anticoagulation in COVID-19. Blood Rev. 47, 100761. https://doi.org/10.1016/j.blre.2020.100761 (2021).
Ali, M. A. M. & Spinler, S. A. COVID-19 and thrombosis: From bench to bedside. Trends Cardiovasc. Med. 31(3), 143–160. https://doi.org/10.1016/j.tcm.2020.12.004 (2021).
Rogani, S. et al. Spontaneous muscle hematoma in older patients with COVID-19: Two case reports and literature review. BMC Geriatr. 20(1), 539. https://doi.org/10.1186/s12877-020-01963-4 (2020).
Dohan, A., Darnige, L., Sapoval, M. & Pellerin, O. Spontaneous soft tissue hematomas. Diagn. Interv. Imaging. 96, 789–796. https://doi.org/10.1016/j.diii.2015.03.014 (2015).
Llitjos, J. F. et al. Ilio-psoas hematoma in the intensive care unit: A multicentric study. Ann. Intensive Care. 6, 8. https://doi.org/10.1186/s13613-016-0106-z (2016).
Barral, M. et al. Predictors of mortality from spontaneous soft-tissue hematomas in a large multicenter cohort who underwent percutaneous transarterial embolization. Radiology. 291(1), 250–258. https://doi.org/10.1148/radiol.2018181187 (2019).
Micic, D. et al. Outcomes of open surgery for retroperitoneal hematoma in covid-19 patients: Experience from a single centre. Chirurgia (Bucur) 117(5), 526–534. https://doi.org/10.21614/chirurgia.2763 (2022).
Polyaev, A. Y. et al. Increased reliability of CT-imaging signs of bleeding into soft tissue in patients with COVID-19 for planning transarterial embolization. Abdom. Radiol. 48(3), 1164–1172. https://doi.org/10.1007/s00261-023-03810-7 (2023).
Temporary guidelines "Prevention, diagnosis and treatment of new coronavirus infection (COVID-19)" Version 13.1 (approved by the Ministry of Health of the Russian Federation on November 17, 2021) (available in Russian)
Riu, P. et al. Management of spontaneous bleeding in COVID-19 in patients: Is embolization always needed?. J. Clin. Med. 10(18), 4119. https://doi.org/10.3390/jcm10184119 (2021).
Furlan, A., Fakhran, S. & Federle, M. P. Spontaneous abdominal hemorrhage: Causes, CT findings, and clinical implications. AJR Am. J. Roentgenol. 193, 1077–1087. https://doi.org/10.2214/AJR.08.2231 (2009).
Tiralongo, F. et al. Spontaneous retroperitoneal hematoma treated with percutaneous transarterial embolization in COVID-19 Era: Diagnostic findings and procedural outcome. Tomography 8(3), 1228–1240. https://doi.org/10.3390/tomography8030101 (2022).
Elikowski, W. et al. Retroperitoneal hematoma in COVID-19 patients—Case series. Pol. Merkur Lekarski. 50(296), 118–123 (2022).
Klausenitz, C. et al. Efficacy of transarterial embolisation in patients with life-threatening spontaneous retroperitoneal haematoma. Clin. Radiol. 76(2), 157.e11-157.e18. https://doi.org/10.1016/j.crad.2020.10.003 (2021).
Tani, R. et al. The utility of transarterial embolization and computed tomography for life—Threatening spontaneous retroperitoneal hemorrhage. Jpn. J. Radiol. 37(4), 328–335. https://doi.org/10.1007/s11604-019-00815-5 (2019).
Palumbo, D., Guazzarotti, G., De Cobelli, F. Spontaneous Major Hemorrhage in COVID-19 Patients: Another Brick in the Wall of SARS-CoV-2-Associated Coagulation Disorders? J. Vasc. Interv. Radiol. 31(9), 1494–1496. https://doi.org/10.1016/j.jvir.2020.06.010 (2020)
Dunlap, R., Kisner, C., Georgiades, C. S., Demmert, A. & Lyons, G. R. Spontaneous breast hematoma as a complication of anticoagulation therapy requiring angiography and embolization. Clin. Imaging. 69, 169–171. https://doi.org/10.1016/j.clinimag.2020.07.023 (2021).
Contrella, B. N. et al. Spontaneous rectus sheath hematoma: Factors predictive of conservative management failure. J. Vasc. Interv. Radiol. 31(2), 323–330. https://doi.org/10.1016/j.jvir.2019.06.009 (2020).
Author information
Authors and Affiliations
Contributions
Conceptualization: T.A.E., M.S.V. Methodology: T.A.E., T.D.Y. Formal analysis and investigation: S.E.A. Writing—original draft preparation: P.A.Y., T.D.Y. Writing—review and editing: B.M.V., S.E.A. Supervision: S.A.V. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tyagunov, A.E., Trudkov, D.Y., Polyaev, A.Y. et al. Comparison of management options for spontaneous bleeding into soft tissues in patients with COVID-19. Sci Rep 15, 2145 (2025). https://doi.org/10.1038/s41598-025-85454-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-85454-9
