
Abstract
Intrahepatic cholangiocarcinoma (ICC) is a highly malignant liver tumor associated with a dismal prognosis, largely due to chemotherapy resistance. However, the mechanisms underlying gemcitabine (GEM) resistance in ICC remain poorly understood. In this study, we established three GEM-resistant cell models and evaluated their resistance by assessing cell proliferation, cell cycle arrest, and DNA damage. GEM-resistant cells exhibited significant tolerance to GEM-induced growth inhibition, reduced cell cycle arrest, and decreased DNA damage compared to parental cells. We then explored potential resistance mechanisms and found that pathways and targets such as epithelial-mesenchymal transition, PI3K/Akt, p53R2, and IGF-1R did not show a significant correlation with ICC resistance. Interestingly, our findings suggested that reactive oxygen species might promote GEM resistance in ICC. In conclusion, we characterized a GEM-resistant ICC model, which can be employed to investigate alternative resistance mechanisms and explore new treatment approaches.
Similar content being viewed by others

Introduction
Intrahepatic cholangiocarcinoma (ICC) is a highly malignant liver tumor originating from the epithelial cells of the secondary and higher-order bile ducts, accounting for 10–15% of all liver malignancies1,2. Compared to hepatocellular carcinoma, ICC is a more malignant tumor with a worse prognosis3. Although advances in diagnostic methods have recently increased the detection rate of ICC, the overall prognosis remains poor4,5, and ICC ranks highly among the most malignant tumors in China and has high mortality rates.
The primary reason for its poor prognosis is that most patients are diagnosed at an advanced stage of the disease, limiting the opportunity for curative surgery6,7. Even among the few early-stage patients eligible for surgical resection, the postoperative recurrence rate is exceedingly high8,9. Treatment regimens centered around gemcitabine (GEM) have demonstrated effectiveness in improving the prognosis for unresectable patients10,11. However, ICC patients are prone to developing acquired drug resistance during treatment, those who initially respond well to treatment often experience reduced sensitivity to GEM chemotherapy, diminishing its overall effectiveness12. Therefore, investigating the intrinsic mechanisms underlying acquired GEM resistance in ICC may help improve the survival of ICC patients in clinical scenarios.
GEM is a nucleoside analog chemotherapeutic prodrug that relies predominantly on cellular uptake by nucleoside transporters (ENTs and CNTs)13. Once inside the cell, it undergoes activation via phosphorylation catalyzed by deoxycytidine kinase14,15. GEM is structurally similar to deoxycytidine and exerts its anti-cancer effects by inhibiting ribonucleotide reductase, effectively impeding de novo DNA synthesis16,17. This inhibition triggers cell cycle arrest in the G0/G1 phase, ultimately culminating in its anticancer effects. Numerous studies have unveiled GEM resistance mechanisms in pancreatic cancer, highlighting factors such as impaired drug transport and metabolism, activation of alternative DNA repair pathways, apoptosis resistance, and involvement in epithelial-mesenchymal transition (EMT)16,18. However, the current understanding of GEM resistance in ICC remains limited. Therefore, exploring the mechanisms that drive GEM resistance could potentially reveal the key molecules involved. In this study, we established three GEM-resistant ICC cell lines, verified their resistance, and initiated a preliminary investigation into the mechanisms that may lead to acquired resistance in ICC.
Materials and methods
All methods used in this study were performed in accordance with the relevant guidelines and regulations. All experimental protocols were approved by Shaoxing People’s Hospital.
Reagents
GEM was obtained from Shaoxing People’s Hospital (Zhejiang, China). The DNA damage kit (C2035S), cell cycle kit (C1052), HRP-conjugated secondary antibodies (A0216 and A0208), PMSF (ST506), enhanced BCA protein assay kit (P0010), RIPA lysis buffer (P0013B), crystal violet (C0121), primary antibodies against PCNA (AF1363), and Occludin (AF7644) were purchased from Beyotime Institute of Biotechnology (Shanghai, China). Primary antibodies against PI3K (#4249), p-PI3K (#4228), p-Akt (#4060), E-Cadherin (#3195), N-Cadherin (#13116), β-catenin (#8480), Vimentin (#5741), Snail (#3879), ZEB1 (#3396), ZO-1 (#8193), Bcl-2 (#15071), Bax (#2772), and β-actin (#3700) were procured from Cell Signaling Technology (Boston, USA). Primary antibodies against Akt (10176-2-AP) and SOD2 (66474-1-Ig) were acquired from Proteintech (Wuhan, China). CCK-8 was obtained from MCE (Monmouth Junction, NJ, USA). The ROS assay kit (S0033S) was obtained from Beyotime (Shanghai, China). The RNA extraction kit (RN001) was bought from Yishan Biotechnology (Shanghai, China). The PrimeScript RT reagent kit (RR047) and TB Green (RR420) were received from TaKaRa (Dalian, China). Matrix (082724) was purchased from Xiamen Mogengel Biotech (Xiamen, China). All primers were synthesized by Sangon Biotechnology (Shanghai, China).
Cell culture
The human ICC cell line HCCC-9810 and RBE were acquired from the Chinese Academy of Science Shanghai Branch Cell Bank (Shanghai, China), while the HuH28 cell line was obtained from our laboratory. HCCC-9810 cells were cultured in RPMI-1640 medium, and HuH28 and RBE cells were cultured in DMEM medium. All cells were supplemented with 10% fetal bovine serum during culture and were maintained in an incubator containing 5% CO2 at 37 °C.
Induction of GEM-resistant cell lines
GEM-resistant ICC cells were established by subjecting them to increasing concentrations of GEM over time. Initially, the cells were exposed to a drug concentration of 1 nM for 72 h. The surviving cells were subsequently cultivated in drug-free medium until they reached 80% confluence. These cells were then maintained at this drug concentration until they grew steadily and were exposed to a 10-fold higher drug concentration. This process was repeated for nine months, after which the cells were cryopreserved in liquid nitrogen for another three months and then revived. The resistance of these cells to GEM was assessed using the CCK-8 assay.
Chemosensitivity assay
To assess chemosensitivity, the cells were plated in 96-well plates at a density of 4 × 103 cells per well and incubated in medium containing different concentrations of GEM for 48 h. After adding CCK-8 to each well, the plates were further incubated at 37 °C for 2 h. Cell viability was determined by measuring the absorbance at 450 nm with a microplate reader (Molecular Devices Co., San Jose, CA, USA).
Cell growth assay
To evaluate cell growth, 2,000 viable ICC cells were seeded in 96-well plates, and cell proliferation was assessed using CCK-8. The GEM concentrations in the treatment groups for HCCC-9810, HuH28, and RBE cells were 1, 0.025, and 0.025 µM, respectively. Cell viability was measured every 24 h, and a microplate reader was used to determine proliferation rates. Five replication wells from each cell were analyzed.
Colony formation assay
After counting, cells were seeded in 6-well plates at a density of 1,000 cells per well and cultured overnight. The ICC cells were then treated with different concentrations of GEM. After 10 days, the cells were fixed with 4% paraformaldehyde and stained with 0.01% crystal violet.
Cell cycle analysis
For cell cycle analysis, the cells were seeded in a 6 cm dish and starved in serum-free medium for 24 h. After an additional 24 h in GEM-containing medium, the cells were harvested, washed with cold phosphate-buffered saline (PBS), fixed in 70% ethanol at 4 °C overnight, and then treated with RNase A and propidium iodide (PI) in the dark. After incubation at 37 °C and avoidance of light for 30 min, the samples were tested using flow cytometry (Beckman Coulter, Fullerton, CA, USA) and analyzed by FCSExpress 3.0 software.
DNA damage detection assay
The extent of cellular DNA damage was detected using the DNA damage kit. In brief, the cells were cultured in 96 wells with or without GEM for 24 h, fixed for 15 min, and blocked with immunostaining blocking solution for 30 min. The cells were then incubated with a monoclonal anti-γ-histone H2AX antibody overnight at 4 °C, followed by incubation with anti-rabbit 488 for 1 h. The nuclei were stained with DAPI, and fluorescence was captured using a Leica confocal microscope system.
3D spheroid growth
Cell seeding was performed in 96-well round-bottom plates (ultra-low attachment), and 1,000 viable cells were suspended in 90 µL of medium containing 5% Matrigel. The plates were incubated overnight to form spheroids after centrifugation at 700 rpm for 5 min. The next day, 10 µL of medium containing GEM was added to the culture. The spheroids underwent imaging after 14 days, and the volumes were calculated with the following formula: volume = 4/3π*b2*c (b = semi-major axis, c = semi-minor axis). Five replication wells from each cell were analyzed.
ROS detection assay
ROS levels were detected using a ROS assay kit (S0033S, Beyotime, China). Briefly, the cells were suspended in diluted DCFH-DA (prepared at 1:10000 in serum-free culture medium) after trypsin digestion and then incubated at 37 °C for 20 min. To facilitate optimal probe-cell interaction, the suspension was gently inverted every 3 to 5 min. The cells were rinsed three times with serum-free culture medium to effectively remove residual DCFH-DA. Finally, the cells’ ROS was detected by the Beckman CytoFLEX S flow cytometer (Beckman Coulter, USA), and data were analyzed on the FlowJo v10.5.0 software.
siRNA transfection
To downregulate SOD2 expression in HCCC-9810 and HuH28 cell lines, SOD2-targeting siRNA (5’-CTGGGAGAATGTAACTGAA-3’) was purchased from RiboBio (Guangzhou, China). Control siRNA was also sourced from RiboBio, with the sequence remaining undisclosed. Before transfection, cells were seeded in dishes to achieve 70–90% confluence. Transfection was performed using Lipofectamine 3000 (Invitrogen, USA, L3000015) following the manufacturer’s instructions.
Real-time polymerase chain reaction
The cells were seeded in 35 mm dishes at 30% confluence. The total RNA was extracted with the RNA extraction kit when cells density achieved 90% confluence, and RNA concentration was determined by NanoDrop 2000. cDNA was prepared using the PrimeScript RT Reagent Kit with gDNA Eraser. The resulting cDNA was subjected to 45 rounds of quantitative real-time PCR on a Lycle-480 detector. Gene expression was assessed by the 2−ΔΔCT quantification method for three biological replications. The primer sequences required for the experiments are listed in Table 1.
Western blot analysis
The cells were seeded in 60 mm dishes at 30% confluence. Total protein was extracted from ICC cells using RIPA lysis buffer when cells density achieved 90% confluence. After quantified via the BCA kit, 30 µg of protein sample was subject to electrophoresis on a 10% SDS–PAGE gel and transferred onto a polyvinylidene fluoride membrane. The membrane was blocked and incubated with a primary antibody, followed by incubation with a horseradish peroxidase-conjugated secondary antibody. Immunoreactive bands were visualized using a chemiluminescence solution (Millipore, Temecula, CA, USA), and β-actin was used as endogenous control.
Data collection
In our study, we identified a published dataset GSE116118 (https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi? acc=GSE116118), in the GEO database using “intrahepatic cholangiocarcinoma” and “drug resistance” as keywords, specifying the species as “Homo sapiens”. This dataset includes paired samples of parental ICC and GEM-resistant ICC cells. Additionally, our laboratory data, labeled as DGSR-ICC, comprises three samples each of parental and GEM-resistant ICC cells.
Identification of differentially expressed genes
We processed the GSE116118 dataset and our laboratory dataset DGSR-ICC using the R language (Version 4.3.0), which involved removing batch effects from each group’s data (using the sva package, Version 3.35.2) and normalization. The R package limma (Version 3.56.2) was used to detect Differentially Expressed Genes (DEGs) in the parental and resistant groups of both datasets. For the GEO dataset GSE116118, the criteria for selecting DEGs were a p-value < 0.05 and |log2 fold change| > 1; for the laboratory dataset DGSR-ICC, the criteria were a p-value < 0.05 and |log2 fold change| > 0.6. We visualized the differential analysis results with volcano plots using the R package ggrepel (Version 0.9.3) and used the R package pheatmap (Version 1.0.12) for heatmap visualization of gene expression in each dataset. Subsequently, we analyzed the intersecting DEGs from both datasets, created Venn diagrams, and visualized the expression differences of the Common DEGs (Co-DEGs) using line charts.
Enrichment analysis of DEGs
We conducted Gene Ontology (GO) enrichment analysis on the DEGs of our dataset using the R package clusterProfiler (Version 4.8.3). A p-value < 0.05 was considered statistically significant. For the GO enrichment analysis results, we visualized the top 10 pathways with the smallest p-values in bar charts. All visualizations were generated using the R package ggplot2 (Version 3.4.3).
Statistical analysis
Data were presented as the means ± SD. Student’s t-test was used to determine the statistical significance between the two groups. One-way ANOVA followed by the Tukey–Kramer adjustment was used to examine differences among multiple groups. All statistical analyses were conducted using SPSS v21.0 (IBM, Armonk, NY, USA) and GraphPad Prism 8.3.0 (GraphPad, Bethesda, MD, USA). A p-value < 0.05 was considered statistically significant.
Results
Establishment of GEM resistance in ICC cell lines
GEM-resistant ICC cell lines were established by methods outlined in Materials and Methods. The sensitivity of cells to GEM is depicted in Fig. 1A. Notably, GEM-resistant lines exhibited a significant increase in tolerance to GEM-induced toxicity compared to the parental cell lines. However, it is important to note that the degree of resistance varied among the three cell lines, with HCCC-9810 displaying the highest resistance, followed by HuH28 and RBE.
Given that cell viability resulted from a short treatment with GEM for 48 h, proliferation assays were performed to further confirm the stability of proliferation in GEM-resistant cell lines. Our results revealed that each GEM-resistant cell line at the maintenance of GEM remained capable of sustained growth despite a modest inhibition of proliferation compared to the parent (Fig. 1B).
Additionally, we performed a clonal formation assay, which showed that GEM-resistant ICC cells could steadily proliferate in the presence of GEM (Fig. 1C).

Establishment of GEM resistance in ICC cell lines. (A) Cell viability curves for parental and resistant ICC cells after 48 h of GEM. (B) Cell growth curves of parental and resistant ICC cells with or without GEM. (C) Colony formation ability of parental and resistant ICC cells with or without GEM. HCCC-9810, HuH28, and RBE were treated with GEM at concentrations of 1, 0.025, and 0.025 µM, respectively. GEM: gemcitabine; P-GEM (-)/(+): parental ICC cell without/with GEM; R-GEM (-)/(+): resistant ICC cell without/with GEM. *P<0.05; **P<0.01 versus parental ICC cells.
Diminished G0/G1 cell cycle arrest and tumorigenicity inhibition in GEM-resistant cell lines
Cell cycle distribution of the parental and GEM-resistant cells was determined by flow cytometry analysis. As displayed in Fig. 2A, after incubation with GEM for 24 h, a significant G0/G1 phase arrest (G0/G1-phase cells represented 92.55%±1.22%, 80.1%±2.27%, and 86.58%±3.74% of the HCCC-9810, HuH28, and RBE GEM-incubated parental cells, respectively, and only 66.89%±6.88%, 54.9%±3.02%, and 43.3%±9.14% of the respective controls.) was observed in parental cells, rendering them incapable of proliferation. In contrast, GEM-resistant cells proliferated normally, with no difference in cell cycle distribution compared to that of the GEM-free culture.
Subsequently, the cultivation of HCCC-9810 and HuH28 cells in 3D spheroids was employed to mimic the tumor formation capacity in vitro. The findings indicated that parental cells exhibited smaller spheroid sizes when subjected to GEM than the resistant cohort (Fig. 2B).

Diminished G0 /G1 cell cycle arrest and tumorigenicity inhibition in GEM-resistant cell lines. (A) Representative flow cytometry histograms depicting cellular distribution clusters with GEM in parental and resistant ICC cells, categorized into distinct cell cycle phases (G0/G1, S, and G2/M) based on PI staining intensity. (B) Detection of spherical growth of parental and resistant ICC cells after GEM treatments. HCCC-9810, HuH28, and RBE were treated with GEM at concentrations of 1, 0.05, and 0.05 µM, respectively. **P<0.01 versus parental ICC cells without GEM.
Reduced H2AX phosphorylation induced by GEM in resistant cell lines
Upon entry into the cell, GEM is activated to a triphosphate form and binds to replicating DNA19. This incorporation induces partial chain termination and replication fork stalling, as detected by H2AX phosphorylation20,21. To determine whether GEM-induced replication arrest differed between the parental and resistant cells, immunofluorescence assays were performed to detect H2AX phosphorylation. As presented in Fig. 3, γ-H2AX foci were observed in the nuclei of nearly all parental cells, whereas they were rarely observed in the nuclei of GEM-resistant cells. These results indicate that GEM-induced DNA damage was substantially attenuated in GEM-resistant cell lines.

Reduced H2AX phosphorylation induced by GEM in resistant cell lines. HCCC-9810, HuH28, and RBE were treated with GEM at concentrations of 1, 0.05, and 0.05 µM, respectively. Green fluorescence represents cells with DNA damage.
GEM resistance was independent of PI3K/Akt and EMT pathway in ICC cell lines
Numerous signaling pathways, including PI3K/AKT and EMT, have been implicated in the resistance of cholangiocarcinoma cells to apoptosis when exposed to GEM, oxaliplatin, cisplatin, and 5-FU22,23,24. In light of these observations, we conducted this study by scrutinizing the disparities in the expression of PI3K/Akt, EMT pathway components, and apoptosis-related proteins before and after developing secondary drug resistance (Fig. 4). Unfortunately, no meaningful variations in the expression of relevant genes were observed among different ICC cells.
The ribonucleotide reductase p53R2 is responsible for supplying nucleotides crucial for the repair of damaged DNA25. IGF-1R is a tyrosine kinase receptor activated by its ligand IGF-1 and elevated insulin levels, which was overexpressed in human cholangiocarcinoma cell lines and tumor biopsy samples26. The expression levels of both are reported to be closely linked with the efficacy of GEM. Accordingly, we conducted a comparative analysis of p53R2 and IGF-1R expression levels in parental and resistant cells, but our findings revealed no statistically significant disparities (Fig. 4A).
Consequently, it can be inferred that the aforementioned targets may not contribute to developing GEM resistance in ICC. This further instigated our investigation into the novel mechanisms underlying GEM resistance in ICC.

GEM resistance was independent of PI3K/Akt and EMT pathway in ICC cell lines. (A) Detection of the mRNA expression levels of the EMT pathway, PI3K/Akt axis, IGF-1R, p53R2, Bcl-2, and Bax between the parental and resistant ICC cells. (B) Western blot analysis of protein expression related to the EMT pathway and the PI3K/Akt signaling axis. HCCC-9810-P: HCCC-9810 parental cell; HCCC-9810-R: HCCC-9810 GEM-resistant cell. *P<0.05; **P<0.01 versus parental ICC cells.
High tolerance to oxidative stress was associated with ICC cell resistance
ROS primarily include superoxide anions, hydroxyl radicals, and hydrogen peroxide. Excessive ROS accumulation can disrupt protein function, induce lipid peroxidation, and cause DNA damage, thereby promoting the development of various diseases, including cancer27,28. Notably, SOD2, a metalloenzyme that shields cells from ROS-induced damage29 exhibited a significant increase following GEM treatment in ICC cells (Fig. 5A). This upregulation hints at the potential significance of oxidative stress in the context of chemotherapy. Using the flow cytometry assay, we detected that the basal ROS of GEM-resistant cells was notably higher compared to those in parental cells. Interestingly, the extent of ROS increase in GEM-resistant cells upon exposure to GEM was not as pronounced as that observed in parental cells (Fig. 5C). This led us to hypothesize that prolonged exposure to GEM conferred resistance to oxidative stress to these cells, allowing them to endure elevated ROS levels by enhancing their antioxidant capacity. The result of SOD2 expression in GEM-resistant cells provided preliminary support to the mentioned hypothesis (Fig. 5B).
To further clarify the effect of ROS on GEM sensitivity, we performed ROS intervention within ICC cells. Knockdown of SOD2 further enhanced drug resistance in ICC cells (Fig. 5D). These findings collectively indicate the pivotal role of ROS in promoting the development of GEM resistance in ICC.

High tolerance to oxidative stress was associated with ICC cell resistance. (A) SOD2 expression was upregulated after exposure to GEM. (B) SOD2 expression in parental and GEM-resistant cells. (C) Detection of the levels of ROS in parental and resistant ICC cells with or without GEM treatment. Δ value = (median value with GEM) – (median value without GEM). (D) Inhibition of SOD2 expression by si-RNA enhanced the resistance of ICC cells to GEM treatment. *P<0.05; **P<0.01 versus the negative group.
MAPK cascade was a candidate pathway for the molecular mechanisms of GEM resistance in ICC
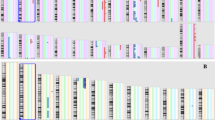
Indeed, to delve deeper into the molecular mechanisms of GEM resistance in ICC, a comprehensive transcriptomic analysis of the established resistant cell lines was performed. Through stringent threshold screening, we identified 60 downregulated genes and 19 upregulated genes (Fig. 6). GO enrichment analysis revealed a significant association of these differentially expressed genes with the negative regulation of the MAPK cascade (Fig. 6E). Notably, Chiara Varamo et al. attempted to construct the ICC-resistant cell line MT-CHC01R1.5 to screen for GEM resistance. We aimed to elucidate the molecular targets involved in ICC resistance through a larger-scale resistant cell line, considering the high heterogeneity of ICC. Collaborating with the dataset GSE116118, we found differential expression in ANKRD1, AP1AR, BMP2, CAB39L, CDCA3, CTH, DUSP5, EIF4A2, GDPD1, HJURP, HMBOX1, PSMC3, RB1CC1, SLC25A36, and USP53 (Fig. 6D). Therefore, our future research will focus on exploring the relationship between these DEGs and ROS.

Analysis of gene transcriptome dataset from ICC resistant and parental cell lines. (A) Heatmap of DEGs in our constructed dataset of GEM-resistant cell lines versus the GEO dataset GSE116118. (B) Volcano plot of DEGs. (C) Venn diagram of DEGs. (D) Expression of DEGs in the crossover between DGSR-ICC and GSE116118. (E) Go description of DGSR-ICC.
Discussion
Over the past four decades, ICC incidence has surged by over 140%30. However, only 20–30% of patients are eligible for curative resection, and the 5-year survival rate is 20–35%31. For advanced-stage patients, the combination chemotherapy regimen of GEM and cisplatin has long held the mantle of being the most effective first-line treatment32. Nevertheless, drug resistance typically occurs within a few months. Few therapeutic options are left after first line chemotherapy failure, and less than half of patients receive a second-line treatment in a disease characterized by an elevated attrition rate between chemotherapy lines33. Therefore, the mechanisms involved in the acquired resistance of ICC to GEM need to be urgently investigated. In this study, we validated the acquired resistance in HCCC-9810, HuH28, and RBE cells through prolonged exposure to GEM. We assessed resistance based on cell proliferation, cell cycle arrest, and DNA damage. Importantly, the acquired resistance properties are proved durable. As described, even after being cryopreserved in liquid nitrogen for three months, these cells maintain a high level of tolerance to GEM, confirming the reliability of the GEM-resistant cell model.
EMT is a well-established process closely linked to cell migration and invasion. Moreover, it plays a pivotal role in fostering drug resistance34,35. Lu et al. discovered that the combined action of heparin and GEM facilitated EMT in biliary tract cancer cells, inducing drug resistance36. Interestingly, the drug resistance was reversed when interventions were conducted to block the EMT process. This observation implies that EMT is a crucial factor in GEM resistance among cancer cells. Meanwhile, Yamada found that the interaction between interleukin-6 and transforming growth factor β1 can influence EMT and consequently affect cancer cell resistance24. In our GEM-resistant model of ICC, GEM resistance was not shown to be mediated by the EMT pathway. The expression of EMT-related genes fluctuates inconsistently among different cells and is likely attributed to the distinct biological characteristics of biliary tract malignancies, which encompass ICC, extrahepatic cholangiocarcinoma, and gallbladder cancer. However, it is worth noting that the mRNA levels of E-Cadherin and Claudin-1 were significantly upregulated in the RBE resistant cell line. Considering the relatively low baseline expression levels of both genes in HCCC-9810 and HuH28, some of the differential expressions may not be as apparent. Perhaps expanding the variety of ICC cell samples could help address this limitation.
It has been reported that increased expression of p53R2 may serve as a predictive indicator for resistance to GEM in cholangiocarcinoma37. Inhibition of IGF-1R function holds promise as an adjunctive approach for cholangiocarcinoma treatment, as it exhibits activity against biliary tract cancer cells in vitro and potentiates the efficacy of GEM38. Therefore, we investigated several pathways and targets, including PI3K/Akt, p53R2, and IGF-1R. However, the results failed to reveal any significant differences.
ROS are closely associated with drug resistance39. They can activate various intracellular antioxidant mechanisms to counter their detrimental effects. These resistance mechanisms often involve multiple transcription factors and signaling pathways that promote cell survival, ultimately leading to the development of drug-resistant phenotypes in cancer cells40. For instance, exposure of cancer cells to chemotherapy drugs can elevate ROS levels, cause the buildup of misfolded proteins, and provoke endoplasmic reticulum stress. In response, cells induce autophagy to degrade misfolded proteins, enabling their survival and the acquisition of drug resistance41. In platinum-resistant ovarian cancer cells, the Keap1/Nrf2/p62 pathway induces the expression of downstream transcription factors, allowing cells to evade apoptosis triggered by ROS and consequently acquire drug resistance42.
In our research, we explored the impact of GEM exposure on parental cells, and found that the crucial antioxidant enzyme SOD2 exhibited upregulation. Additionally, we measured ROS levels in ICC cells and found that the cells displayed a marked rise in their ROS levels. Intriguingly, resistant cells exhibited higher baseline ROS levels than their parental counterparts, but their response to drug-induced ROS escalation was less pronounced. These findings suggest a plausible connection between drug resistance and ROS. To elucidate the role of ROS in acquired drug resistance in ICC, we reduced SOD2 levels in ICC cells. Surprisingly, this intervention resulted in an even greater enhancement of GEM resistance in both the parental and resistant cells. These results underscore that ROS may actively contribute to developing drug resistance in ICC. Targeting ROS levels could potentially act as a therapeutic strategy to counter acquired resistance in this particular type of cancer.
MAPK signaling plays a pivotal role in the development of chemotherapy resistance in cancer. The activation of MAPK pathways contributes to tumor cell survival by inhibiting apoptosis, enhancing DNA repair, and promoting drug efflux43. However, our study found that in drug-resistant cells, differentially expressed genes negatively regulate the MAPK pathway, implying a positive correlation between MAPK activation and chemotherapy sensitivity. A previous study showed that MAPK inhibition with SB202190 promoted cisplatin resistance in ovarian cancer cells44. This discrepancy may reflect the cell-type and condition-dependent nature of MAPK signaling.
In fact, during the development of chemotherapy resistance, tumor cells often accumulate mutations that confer a survival advantage under selective drug pressure. In our study, we observed differential gene expression in drug-resistant ICC cells, likely due to the acquisition of specific mutations. These mutations may enhance DNA repair mechanisms. As mentioned above, the differential expression of E-Cadherin and Claudin-1 in RBE-resistant cells, but not in HCCC-9810 and HuH28, may reflect underlying genetic differences between cell lines, which influence their response to treatment. This highlights the complex interaction between genetic mutations, gene expression, and the development of drug resistance. By comparing our differentially expressed genes with the GSE116118 dataset, we identified 15 genes with consistent expression trends. Notably, genes like DUSP5 and HJURP have been implicated in chemoresistance in breast and ovarian cancers45,46,47. However, the involvement of other differentially expressed genes in ICC chemoresistance remains to be determined. Further research is needed to investigate whether the observed gene expression changes are related to specific mutations and how these mutations contribute to resistance mechanisms.
In summary, the findings of this study indicate a valuable chemoresistance model, providing an indispensable foundation for further in-depth research into the intrinsic mechanisms of GEM resistance in ICC.
Data availability
The datasets analyzed and raw data during the current study are available from the corresponding author on reasonable request.
References
Yao, J., Liang, X., Liu, Y., Li, S. & Zheng, M. Trends in incidence and prognostic factors of two subtypes of primary liver cancers: a Surveillance, Epidemiology, and end results-based Population Study. Cancer Control. 29, 10732748211051548. https://doi.org/10.1177/10732748211051548 (2022).
Sung, H. et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71, 209–249. https://doi.org/10.3322/caac.21660 (2021).
Deng, G. et al. Tumor burden score dictates prognosis of patients with combined hepatocellular cholangiocarcinoma undergoing hepatectomy. Front. Oncol. 12, 977111. https://doi.org/10.3389/fonc.2022.977111 (2022).
Brindley, P. J. et al. Cholangiocarcinoma. Nat. Rev. Dis. Primers. 7, 65. https://doi.org/10.1038/s41572-021-00300-2 (2021).
Zhu, A. X. et al. Final overall survival efficacy results of Ivosidenib for patients with Advanced Cholangiocarcinoma with IDH1 mutation: the phase 3 Randomized Clinical ClarIDHy Trial. JAMA Oncol. 7, 1669–1677. https://doi.org/10.1001/jamaoncol.2021.3836 (2021).
Du, J. et al. CircNFIB inhibits tumor growth and metastasis through suppressing MEK1/ERK signaling in intrahepatic cholangiocarcinoma. Mol. Cancer. 21, 18. https://doi.org/10.1186/s12943-021-01482-9 (2022).
Liu, X. et al. Local and abscopal responses in advanced intrahepatic cholangiocarcinoma with low TMB, MSS, pMMR and negative PD-L1 expression following combined therapy of SBRT with PD-1 blockade. J. Immunother Cancer. 7, 204. https://doi.org/10.1186/s40425-019-0692-z (2019).
Wang, C. et al. Specific risk factors contributing to early and late recurrences of intrahepatic cholangiocarcinoma after curative resection. World J. Surg. Oncol. 17 https://doi.org/10.1186/s12957-018-1540-1 (2019).
Doussot, A. et al. Recurrence patterns and Disease-Free Survival after Resection of Intrahepatic Cholangiocarcinoma: preoperative and postoperative prognostic models. J. Am. Coll. Surg. 223 https://doi.org/10.1016/j.jamcollsurg.2016.05.019 (2016).
Valle, J. et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl. J. Med. 362, 1273–1281. https://doi.org/10.1056/NEJMoa0908721 (2010).
Morizane, C. et al. Combination gemcitabine plus S-1 versus gemcitabine plus cisplatin for advanced/recurrent biliary tract cancer: the FUGA-BT (JCOG1113) randomized phase III clinical trial. Ann. Oncol. 30, 1950–1958. https://doi.org/10.1093/annonc/mdz402 (2019).
Marin, J. J. G. et al. Chemoresistance and chemosensitization in cholangiocarcinoma. Biochim. Biophys. Acta Mol. Basis Dis. 1864, 1444–1453. https://doi.org/10.1016/j.bbadis.2017.06.005 (2018).
Mini, E., Nobili, S., Caciagli, B., Landini, I. & Mazzei, T. Cellular pharmacology of gemcitabine. Ann. Oncol. 17 (Suppl 5), v7–12 (2006).
Yamamoto, M. et al. Roles for hENT1 and dCK in gemcitabine sensitivity and malignancy of meningioma. Neuro Oncol. 23, 945–954. https://doi.org/10.1093/neuonc/noab015 (2021).
Hu, Q. et al. dCK negatively regulates the NRF2/ARE axis and ROS production in pancreatic cancer. Cell. Prolif. 51, e12456. https://doi.org/10.1111/cpr.12456 (2018).
Binenbaum, Y., Na’ara, S. & Gil, Z. Gemcitabine resistance in pancreatic ductal adenocarcinoma. Drug Resist. Updat. 23, 55–68. https://doi.org/10.1016/j.drup.2015.10.002 (2015).
Jordheim, L. P., Sève, P., Trédan, O. & Dumontet, C. The ribonucleotide reductase large subunit (RRM1) as a predictive factor in patients with cancer. Lancet Oncol. 12, 693–702. https://doi.org/10.1016/S1470-2045(10)70244-8 (2011).
Adamska, A. et al. Molecular and cellular mechanisms of chemoresistance in pancreatic cancer. Adv. Biol. Regul. 68, 77–87. https://doi.org/10.1016/j.jbior.2017.11.007 (2018).
Huang, P., Chubb, S., Hertel, L. W., Grindey, G. B. & Plunkett, W. Action of 2’,2’-difluorodeoxycytidine on DNA synthesis. Cancer Res. 51, 6110–6117 (1991).
Ewald, B., Sampath, D. & Plunkett, W. H2AX phosphorylation marks gemcitabine-induced stalled replication forks and their collapse upon S-phase checkpoint abrogation. Mol. Cancer Ther. 6, 1239–1248 (2007).
Saiki, Y. et al. DCK is frequently inactivated in acquired gemcitabine-resistant human cancer cells. Biochem. Biophys. Res. Commun. 421 https://doi.org/10.1016/j.bbrc.2012.03.122 (2012).
Yoon, H., Min, J. K., Lee, J. W., Kim, D. G. & Hong, H. J. Acquisition of chemoresistance in intrahepatic cholangiocarcinoma cells by activation of AKT and extracellular signal-regulated kinase (ERK)1/2. Biochem. Biophys. Res. Commun. 405, 333–337. https://doi.org/10.1016/j.bbrc.2010.11.130 (2011).
Leelawat, K., Narong, S., Udomchaiprasertkul, W., Leelawat, S. & Tungpradubkul, S. Inhibition of PI3K increases oxaliplatin sensitivity in cholangiocarcinoma cells. Cancer Cell. Int. 9 (3). https://doi.org/10.1186/1475-2867-9-3 (2009).
Yamada, D. et al. Role of crosstalk between interleukin-6 and transforming growth factor-beta 1 in epithelial-mesenchymal transition and chemoresistance in biliary tract cancer. Eur. J. Cancer. 49, 1725–1740. https://doi.org/10.1016/j.ejca.2012.12.002 (2013).
Krishnaraj, J., Yamamoto, T. & Ohki, R. p53-Dependent cytoprotective mechanisms behind resistance to Chemo-Radiotherapeutic agents used in Cancer Treatment. Cancers (Basel). 15 https://doi.org/10.3390/cancers15133399 (2023).
Alvaro, D. et al. Estrogens and insulin-like growth factor 1 modulate neoplastic cell growth in human cholangiocarcinoma. Am. J. Pathol. 169, 877–888 (2006).
Cheung, E. C. & Vousden, K. H. The role of ROS in tumour development and progression. Nat. Rev. Cancer. 22, 280–297. https://doi.org/10.1038/s41568-021-00435-0 (2022).
Prasad, S., Gupta, S. C. & Tyagi, A. K. Reactive oxygen species (ROS) and cancer: role of antioxidative nutraceuticals. Cancer Lett. 387 https://doi.org/10.1016/j.canlet.2016.03.042 (2017).
Bolduc, J. A., Collins, J. A. & Loeser, R. F. Reactive oxygen species, aging and articular cartilage homeostasis. Free Radic Biol. Med. 132, 73–82. https://doi.org/10.1016/j.freeradbiomed.2018.08.038 (2019).
Saha, S. K., Zhu, A. X., Fuchs, C. S. & Brooks, G. A. Forty-year trends in Cholangiocarcinoma Incidence in the U.S.: Intrahepatic Disease on the rise. Oncologist 21, 594–599. https://doi.org/10.1634/theoncologist.2015-0446 (2016).
Moris, D. et al. Advances in the treatment of intrahepatic cholangiocarcinoma: an overview of the current and future therapeutic landscape for clinicians. CA Cancer J. Clin. 73, 198–222. https://doi.org/10.3322/caac.21759 (2023).
Benson, A. B. et al. Hepatobiliary cancers, Version 2.2021, NCCN Clinical Practice guidelines in Oncology. J. Natl. Compr. Canc Netw. 19, 541–565. https://doi.org/10.6004/jnccn.2021.0022 (2021).
Filippi, R. et al. Clinical insights and prognostic factors from an advanced biliary tract cancer case series: a real-world analysis. J. Chemother. 34, 123–132. https://doi.org/10.1080/1120009X.2021.1953887 (2022).
Dong, B. et al. MiRNA-mediated EMT and CSCs in cancer chemoresistance. Exp. Hematol. Oncol. 10 https://doi.org/10.1186/s40164-021-00206-5 (2021).
Zhang, B. et al. Acetylation of KLF5 maintains EMT and tumorigenicity to cause chemoresistant bone metastasis in prostate cancer. Nat. Commun. 12, 1714. https://doi.org/10.1038/s41467-021-21976-w (2021).
Lu, Y. et al. Effect of midkine on gemcitabine resistance in biliary tract cancer. Int. J. Mol. Med. 41, 2003–2011. https://doi.org/10.3892/ijmm.2018.3399 (2018).
Sato, J. et al. Gene expression analysis for predicting gemcitabine resistance in human cholangiocarcinoma. J. Hepatobiliary Pancreat. Sci. 18, 700–711. https://doi.org/10.1007/s00534-011-0376-7 (2011).
Wolf, S., Lorenz, J., Mössner, J. & Wiedmann, M. Treatment of biliary tract cancer with NVP-AEW541: mechanisms of action and resistance. World J. Gastroenterol. 16, 156–166 (2010).
Xue, D., Zhou, X. & Qiu, J. Emerging role of NRF2 in ROS-mediated tumor chemoresistance. Biomed. Pharmacother. 131, 110676. https://doi.org/10.1016/j.biopha.2020.110676 (2020).
Pandey, V., Chaube, B. & Bhat, M. K. Hyperglycemia regulates MDR-1, drug accumulation and ROS levels causing increased toxicity of carboplatin and 5-fluorouracil in MCF-7 cells. J. Cell. Biochem. 112, 2942–2952. https://doi.org/10.1002/jcb.23210 (2011).
Liu, N. et al. The BH3 mimetic S1 induces endoplasmic reticulum stress-associated apoptosis in cisplatin-resistant human ovarian cancer cells although it activates autophagy. Oncol. Rep. 30, 2677–2684. https://doi.org/10.3892/or.2013.2771 (2013).
Park, J. S., Kang, D. H. & Bae, S. H. p62 prevents carbonyl cyanide m-chlorophenyl hydrazine (CCCP)-induced apoptotic cell death by activating Nrf2. Biochem. Biophys. Res. Commun. 464, 1139–1144. https://doi.org/10.1016/j.bbrc.2015.07.093 (2015).
Lee, S., Rauch, J. & Kolch, W. Targeting MAPK signaling in Cancer: mechanisms of Drug Resistance and Sensitivity. Int. J. Mol. Sci. 21 https://doi.org/10.3390/ijms21031102 (2020).
Mansouri, A. et al. Sustained activation of JNK/p38 MAPK pathways in response to cisplatin leads to Fas ligand induction and cell death in ovarian carcinoma cells. J. Biol. Chem. 278, 19245–19256 (2003).
Mao, M. et al. HJURP regulates cell proliferation and chemo-resistance via YAP1/NDRG1 transcriptional axis in triple-negative breast cancer. Cell. Death Dis. 13, 396. https://doi.org/10.1038/s41419-022-04833-6 (2022).
Liu, T. et al. The suppression of DUSP5 expression correlates with paclitaxel resistance and poor prognosis in basal-like breast cancer. Int. J. Med. Sci. 15, 738–747. https://doi.org/10.7150/ijms.24981 (2018).
Lan, Y., Xu, H. & Jin, L. HJURP Derived from Cancer-Associated fibroblasts promotes glutamine metabolism to Induce Resistance to Doxorubicin in Ovarian Cancer. Tohoku J. Exp. Med. 264, 31–39. https://doi.org/10.1620/tjem.2024.J041 (2024).
Author information
Authors and Affiliations
Contributions
J.L. and Y.H. carried out the experiments and created figures. J.L. wrote the original draft. W.Z. performed data analysis. J.Z. and W.Z. conducted literature retrieval. J.Y. and B.L. designed this research study and revised this manuscript. Additionally, all authors have approved the final draft.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, J., Hu, Y., Zhang, J. et al. Establishment and characterization of three gemcitabine-resistant human intrahepatic cholangiocarcinoma cell lines. Sci Rep 15, 4813 (2025). https://doi.org/10.1038/s41598-025-89423-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-89423-0
