
Abstract
Aims
The aim was to investigate the cross-sectional associations between personality traits, psychogenic needs and eating behaviour, and to describe the extent to which personality influences the association between eating behaviour and weight status.
Methods
In 2016/17, a population-based sample of 573 women in Gothenburg, Sweden aged either 38 or 50 participated in a health examination. They completed the Three-Factor Eating Questionnaire, measuring uncontrolled eating, emotional eating and cognitive restraint on a scale of zero to 100. Scores higher than 50 defined excessive eating behaviour. The Cesarec-Marke Personality Schedule was used to measure psychogenic needs, characterised by pursuits and objectives that define personality and influence actions. Extraversion and neuroticism were assessed using the Eysenck-Personality Inventory. Regression models for excessive eating behaviour and for logarithmic body mass index (BMI) as a function of standardised personality scores were adjusted for sociodemographic, lifestyle and health factors.
Results
A higher need to defend one’s status (DST) was positively associated with excessive uncontrolled eating, odds ratio (OR) = 1.44, 95% confidence interval = (1.11, 1.86) per standard deviation (SD) of DST. The need to defend one’s status was more strongly associated with excessive emotional eating, OR = 1.61 (1.18, 2.20) than neuroticism, OR = 1.45 (1.06, 1.97), in a mutually adjusted model. Needs for achievement and autonomy were associated with excessive cognitive restraint, OR = 1.39 (1.09, 1.76) and 0.78 (0.62, 0.97), respectively. Excessive emotional eating was associated with 5.3 (1.1, 9.6) % higher values of BMI when adjusted for the need of DST, which was associated with −2.7 (−4.1, −1.3) % lower BMI per SD.
Conclusions
Psychogenic needs were more closely associated with eating behaviour than personality traits. A lower need to defend one’s status and excessive emotional eating were independently associated with higher BMI, suggesting different pathways to obesity and treatment strategies.
Similar content being viewed by others

Introduction
The global prevalence of obesity remains high, and further research into the psychological underpinnings of eating behaviour is essential to develop targeted strategies for weight loss and obesity management [1]. The Three-Factor Eating Questionnaire (TFEQ) is a validated instrument for measuring eating behaviour in the general population and defines three principal domains of adverse eating behaviours: uncontrolled eating, which is characterised by the tendency to lose control over food intake and overeat, emotional eating, which describes the inclination to eat as a way of coping with dysphoric states, and cognitive restraint, which is defined as consciously restricting food intake regardless of feelings of hunger [2,3,4,5]. We have recently shown that emotional eating was the strongest correlate of various measures of adiposity in a population-based sample of women in Sweden [6]. Previous studies on the relationship between personality and eating behaviour have mainly focussed on the Big Five personality traits, of which neuroticism has the strongest, positive association with emotional eating and eating disorders [7]. Higher levels of neuroticism or extraversion and lower levels of conscientiousness have also been linked to higher BMI [8]. Knowledge about the association between personality traits and eating behaviour may inform the psychiatric treatment of overeating and obesity. However, the Big Five personality traits are considered to be innate characteristics that remain stable throughout life [9], limiting the possibility to modify these aspects of unhealthy weight status.
Psychogenic needs present an alternative model for describing personality that are more closely linked to the motives that lead to certain behaviours and that may be more amenable to treatment and change. Psychogenic needs are assessed using the Cesarec-Marke Personality Schedule (CMPS), which is the Swedish version of the Edwards Personal Preference Scale [10]. According to Murray’s theory of personality two sets of needs are defined in humans [11]. The primary needs are centred upon basic biological requirements such as food, water and sex. The secondary or ‘psychogenic’ needs are characterised by goals and pursuits such as affiliation, nurturance, and dominance. Secular changes in psychogenic needs were observed in cohorts of 38- and 50-year-old women, who participated in the 1968 and 2004 examinations of the Population Study of Women in Gothenburg (PSWG), with higher scores for the needs of achievement, dominance, aggression and exhibition in the more recent cohort [12]. This pattern was also observed in a study of 75-year-old men and women examined in 1976 and 2005. The latter study also showed that the gender gap in the values for the need of achievement, the desire to accomplish something challenging, had decreased [13]. This could be due to societal change, where women increasingly occupy a more dominant position. Consequently, one might assume that psychogenic needs are also changeable in the individual, but longitudinal studies of psychogenic needs are lacking.
To our knowledge, the relationship between psychogenic needs and eating behaviour as well as their combined association with body weight has not been investigated before. Hence, we assessed the association between psychogenic needs and eating behaviour measured by the Three-Factor Eating Questionnaire in 38- and 50-year-old women, who participated in the 2016 PSWG survey. Furthermore, we examined whether previously observed associations between eating behaviour and obesity measures [6] were influenced by further adjustment for psychogenic needs. Participants also responded to the Eysenck personality inventory assessing extraversion and neuroticism [14, 15], allowing us to compare the associations of psychogenic needs and personality traits with eating behaviours and body weight.
Materials and methods
Study population and design
A population-based sample of 573 women aged 38 (n = 263) and 50 (n = 310) was retrieved from the Prospective Study of Women in Gothenburg, using the data from the most recent examination in 2016/17. Participation rates were 63% and 73% among 38- and 50-year-old women respectively [16]. The original cohort was established in 1968 with focus on menopause and cardiovascular disease, which was the reason for choosing the age strata 38, 46, 50, 54, and 60 [17]. Subsequent examinations were performed every 12th year and included new samples of 38- and 50-year-old women, to allow for the investigation of secular trends [12]. Hence, the present study is cross-sectional in nature.
Assessment of eating behaviour
Participants’ eating behaviour was self-assessed using the revised 21-item Three-Factor Eating Questionnaire (TFEQ-R21), which comprises three domains: Uncontrolled Eating (UE, 6 items), which describes loss of control over food intake in response to hunger or external stimuli; Emotional Eating (EE, 6 items), which describes overeating during periods of negative mood; and Cognitive Restraint (CR, 9 items), which describes the conscious restriction of food intake to control body weight and shape [2,3,4,5]. The raw scores were converted to a scale from zero to 100, whereby higher values indicate greater levels of the respective eating behaviour. A validated cut-off score for excessive eating behaviour is presently lacking. However, a score of 50 was proposed in previous literature [18] and has been utilised in a subsequent study [6].
Personality traits and psychogenic needs
The Cesarec-Marke Personality Schedule measures eleven psychogenic needs [10, 11, 19, 20]. The questionnaire comprises 165 yes-no items; each of the 11 psychogenic needs are represented by 15 questions, the meaning of which is described in Table 1. In addition, an acquiescence scale measures the propensity to respond affirmatively regardless of the question asked and is included as a control scale in regression models with psychogenic needs. The personality dimensions extraversion-introversion and neuroticism-stability were measured with the Eysenck Personality Inventory [14, 15]. The questionnaire includes 57 yes-no items, 24 of which measure neuroticism and a further 24 extraversion. Nine questions represent a control scale that assesses the tendency to respond with social desirability bias, often referred to as the “lie scale,” the term henceforth utilised in the current study.
Body mass index (BMI)
The physical examination included measurement of weight and height, and body mass index was calculated as weight/height2 (in units of kg/m2). BMI was further categorised into underweight (BMI < 18.5), overweight (BMI ≥ 25) and obesity (BMI ≥ 30).
Potential confounders
The participants completed a self-report questionnaire whereby information on the highest level of education was obtained, which in turn was divided into university education and lower education. The women also indicated whether they were living with a partner and answered questions on previous and current weight-loss diets. All but one of the current dieters had also been dieters in the past, so three mutually exclusive categories were defined: never, only in the past, and current dieting regardless of previous dieting. Consumption of sweets was categorised as never, a few sweets/day, and consumption several times/day. Leisure time physical activity (LTPA) was assessed in four categories, sedentary lifestyle, moderate activity ≥four hours/week, regular training and competitive sports. Coffee consumption was reported as cups/day, regardless of type of coffee or preparation method. Current tobacco use distinguished any tobacco use (cigarette, cigar, pipe, e-cigarette, moist snuff) and no tobacco use. General wellbeing was answered as a validated question on a 7-step Likert scale, with higher scores indicating better well-being [6].
Analytic sample
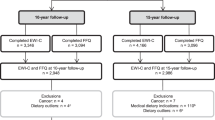
Exclusion criteria were missing values regarding BMI (n = 2), eating behaviour (n = 27), or personality scores (n = 54). Five women were excluded due to pregnancy, as this temporarily changes weight status and eating behaviour. The final analytic sample comprised observations from 485 women.
Ethical approval
Approval for the study was granted by the Regional Ethical Committee Gothenburg (258-16). The study complies with the Declaration of Helsinki and written informed consent was obtained from all participants.
Statistical analysis
The correlation between psychogenic needs and personality scores was assessed using Pearson correlation coefficients. Differences in mean values of psychogenic needs and personality scores by excessive eating behaviours was assessed using t-tests accounting for unequal variances in the two groups. We used multiple logistic regression with automatic variable selection to identify individual psychological scores and background factors associated with each type of excessive eating behaviour. Psychogenic needs and personality traits were standardised to permit the comparison of effect sizes given the different units of measurements; this was done by converting the variables into z-scores. The results were presented as odds ratio (OR) with 95% confidence interval. The area under the receiver operating characteristic curve (AUROC) was used to assess the performance of the model, where a value of 0.5 represents random prediction and the value of 1 represents classification with perfect accuracy. Multiple linear regression analyses were carried out to examine the associations between BMI and psychogenic needs, personality traits, eating behaviours, and potential confounders. As BMI had a right-skewed distribution the variable was log-transformed to ensure a normal distribution of residuals. The corresponding β-coefficients were transformed into (exp(β)-1) ×100%, which gives the percentage change in BMI when the independent variable is increased by one unit. Analyses of continuous BMI were supplemented by logistic regression of overweight and obesity, with variable selection from predictors as described above. Finally, cubic spline regression was used to illustrate the mutual associations between specific psychogenic needs, emotional eating, and BMI or the likelihood of overweight and obesity. Statistical analyses were performed using SAS v.9.4 and Matlab R2022a. The significance level was 0.05 (two-sided tests).
Results
Characteristics of the study population
The sample consisted of two age strata, women aged 38 (44%) and 50 (56%). The prevalence of overweight and obesity was given by 38% and 13%, respectively. About one-third of the women had a university education, and 79% of the women lived with a partner. Dieting was common in this sample: 70% of women had dieted or were currently dieting. Only eight percent said they led a sedentary lifestyle while 56% reported regular training or competitive sports. Eighteen percent of women currently consumed tobacco products. Mean values of scores describing eating behaviour, psychogenic needs, and Eysenck personality traits are shown in Supplementary Table S1.
Correlations between psychogenic needs and Eysenck personality traits
The mutual correlations between individual psychogenic needs and personality traits are shown in Supplementary Table S2. Two sets with three variables each were identified, the need for defence of status, guilt feelings and neuroticism as well as the needs for aggression and exhibition and extraversion, that showed positive correlations within and negative correlations between sets (|r|> 0.4). The correlation structure is further illustrated in Supplementary Fig. S1.
Associations between psychological factors and excessive eating behaviour
Women with excessive emotional eating scored higher on aggression, defence of status, guilt, succorance, acquiescence and neuroticism, and lower on extroversion and the Eysenck-lie scale compared to women without excessive emotional eating (Table 2). Several of these differences were also observed for excessive uncontrolled eating, albeit with smaller effect size. Women with excessive cognitive restraint showed higher scores for achievement, affiliation and nurturance compared to women without excessive cognitive restraint.
To determine which of the personality scores were independently associated with excessive eating behaviours, we performed logistic regression with automatic variable selection among psychological factors and potential confounders. Table 3 shows that the need to defend one’s status was associated with higher odds of excessive uncontrolled eating in a model including the Eysenck-lie scale and sweet consumption. The need for defence of status was also associated with excessive emotional eating, with one SD higher z-DST being associated with 61% higher odds for excessive emotional eating. The magnitude of the association with DST was greater than the equally positive association with neuroticism. Only psychogenic needs were selected in a model for excessive cognitive restraint, with the need for achievement being associated with higher odds, and the need for autonomy with lower odds of excessive cognitive restraint.
In sensitivity analyses we tested the associations of individual questions that form the respective psychogenic needs and the neuroticism scale. A positive answer to the question ‘do you often think about situations that have been embarrassing for you?’ more than doubled the odds for excessive uncontrolled eating, OR = 2.64 (1.53, 4.54), adjusted for sweet consumption and the Eysenck-lie scale (AUROC = 0.74). The same question was also associated with excessive emotional eating, OR = 2.18 (1.19, 3.99), as was the question ‘do you find it difficult to maintain your self-confidence when you are together with confident and superior people?’, OR = 3.01 (1.63, 5.56), adjusted for sweet consumption and dieting behaviour (AUROC = 0.81). No single item from the neuroticism scale was associated with excessive emotional eating in a model including the items of DST described above. Among questions for achievement and autonomy the individual question ’do you want to achieve something important?’ was most strongly associated with excessive cognitive restraint, OR = 2.33 (1.24, 4.37). In the same model, two questions contributing to the need for autonomy (in inverse direction), ‘do you have the feeling that your opinions and perceptions are almost always in line with what people in general think and feel?’ and ‘do you think that the person who goes his own way without taking into account prevailing opinions will sooner or later fail?’ were associated with the outcome, OR = 1.61 (1.00, 2.60) and OR = 1.79 (1.06, 2.99), respectively, adjusted for sweet consumption and dieting behaviour (AUROC = 0.76).
Is the association between eating behaviour and BMI influenced by personality traits or psychogenic needs?
To characterise the association between eating behaviour and BMI, two analyses were conducted using both the continuous scores and the dichotomised versions representing excessive eating behaviour (Table 4). To assess the extent to which these associations were confounded by psychological factors, each model was run with and without adjustment for personality traits and psychogenic needs. We performed linear regression with backward variable selection among psychological factors and covariates, retaining the variables for eating behaviour.
The results showed a general consistency in the associations between log-BMI and the continuous and dichotomised eating-behaviour scores. Using the continuous scores, participants were found to have 2.7% higher BMI values per SD of emotional eating in the basic model, and 2.9% higher BMI when further adjusted for psychological factors, while other domains of eating behaviour were not associated with BMI (left columns in Table 4). From the set of psychological factors, only defence of status acquiescence were selected. The inverse association between defence of status and BMI was also observed after excluding acquiescence, with an effect size of −2.3 (−3.6, −1.0) % per SD. Further adjustment for neuroticism showed that the inverse association between DST and BMI, −2.3 (−3.8, −0.9) %, was stronger than the equally inverse association with neuroticism, −1.5 (−3.1, 0.1) %.
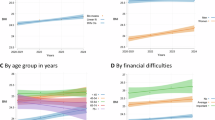
The same covariates were selected in models that contained excessive eating behaviours (right columns in Table 4). Excessive emotional eating was associated with 4.3% higher BMI compared to non-excessive eating behaviour, and this increased to 5.3% when adjusted for DST and ACQ. Overall, past and current dieting were associated with higher BMI, while higher education, living with a partner, and higher physical activity were associated with lower BMI. Positive associations with emotional eating and negative associations with DST in mutually adjusted regression models were also observed with respect to risk for overweight and obesity (Fig. 1).

Spline regression for risk of overweight /obesity as a function of emotional eating behaviour (A, B) and defence of status (C, D)a. aLogistic regression using restricted cubic splines (ref = median) in models including emotional eating (EE), need for defence of status (DST), living with a partner, dieting behaviour, and physical activity (LTPA). Only linear terms of EE and DST were statistically significant.
Sensitivity analyses were performed to obtain a detailed picture of the association between DST and BMI. Spline regression showed an inverse J-shaped association for log-BMI as a function of DST but the positive association with BMI at the upper end of the DST spectrum was not statistically significant (Supplementary Fig. S2). The non-linear association between neuroticism and log-BMI was weaker than for DST and log-BMI (not shown).
Discussion
Summary of results
In this study of women aged 38 and 50, eating behaviour measured by the Three-Factor Eating Questionnaire was found to be associated with both psychogenic needs and personality traits. However, only defence of status was associated with excessive uncontrolled eating in mutually adjusted models, while defence of status and neuroticism were both positively associated with excessive emotional eating. Models for excessive cognitive restraint found a positive association with the need for achievement and a negative association with the need for autonomy. Regression models for body mass index confirmed that emotional but not uncontrolled or restrained eating behaviours was positively associated with BMI. The strength of the association between emotional eating and BMI was not reduced when further adjusted for psychological factors. Defence of status was most strongly associated with body weight and showed negative associations with BMI, overweight, and obesity despite its positive correlation with emotional eating behaviour. Independent associations of BMI with high emotional eating and low defence of status could indicate different psychological dispositions underlying excess body weight, which in turn require different therapeutic approaches.
Associations between psychological factors and eating behaviour
The need to defend one’s status was the predominant correlate of both uncontrolled and emotional eating behaviours, offsetting associations with other psychological factors. The exception was the neuroticism scale that contributed to excessive emotional eating independently of DST. Neuroticism and the need for DST share aspects of self-consciousness and emotional instability but their correlation was only moderate. However, psychogenic needs in general, and the need for DST in particular almost always assess the quality of interactions with other people, whereas the Eysenck neuroticism scale assesses states of dysphoric mood irrespective of reason or cause. Consequently, specific problems such as rumination about embarrassing situations or low self-confidence in the presence of confident and superior people may be more directly related to overeating than mood and psychosomatic symptoms assessed with the neuroticism scale. The link between neuroticism and emotional eating has been observed before [7, 21,22,23], but the new finding that it is associated with the need for defence of status could help to identify and treat specific causes for over-eating.
Although cognitive restraint was not associated with body weight, it is interesting to note that a higher need for achievement and a lower need for autonomy were independently associated with restrained eating behaviour. While the need to master difficult tasks may include maintaining a healthy diet, a reduced need for autonomy could be a sign of sensitivity to the opinions and habits of others, which also promotes restrained eating behaviour. To our knowledge, this is the first time that associations between personality scores and restrained eating behaviour have been examined in a population-based sample that also took into account confounding factors such as dieting.
Associations of psychological factors and eating behaviours with weight status
The results for the continuous scores of the Three-Factor Eating Questionnaire (TFEQ) in relation to BMI are consistent with our previous study [6], with minor differences due to fewer observations and covariates not included here. The main result was that emotional eating was the predominant eating behaviour associated with obesity in middle-aged women independent of uncontrolled or restrained eating and of confounders including dieting behaviour. The positive association between emotional eating and BMI is now confirmed in regression models adjusting for psychological factors of which the need to defend one’s status was the most important. Since DST correlated positively with emotional eating, one might have expected it to be at least partly responsible for the association between emotional eating and BMI. However, the opposite was observed: since low but not high DST was associated with higher BMI as well as overweight and obesity, including DST in the model for BMI or weight status strengthened the association with emotional eating. The latter is formally a result of negative confounding, as the associations of DST with emotional eating and BMI point in opposite directions. Consequently, high levels of emotional eating and low defence of status are independent risk factors and may account for different mechanisms behind the development of excess body weight. While emotional eating by definition and by association with elevated BMI may represent overeating in response to dysphoric mood states [23, 24], the mechanism underlying a low need for defence of status and body weight is less clear. It is possible that a low need for defence of status or low neuroticism is associated with a lower basal metabolic rate [25, 26], which favours sedentary behaviour and accumulation of excess weight.
The inverse association between DST and, to a lesser extent, neuroticism with BMI or obesity appears to contradict previous reports of positive associations between neuroticism and weight status in both sexes [27], and among women when sex-stratified analyses were presented [8, 28,29,30]. However, a meta-analysis of nine international cohort studies found no overall association between neuroticism as measured by the Five-factor model and the prevalence or incidence of obesity, but the heterogeneity between studies was large [31]. In a recent population study from Germany a positive association between neuroticism and obesity in covariate-adjusted models was observed in men but not in women [32]. In our study, there was a U-shaped association between the need for DST and BMI, with a weak positive association at high levels of DST (Supplementary Fig. S2) but only the inverse association was observed in confounder-adjusted models. The use of self-reported anthropometric data [27,28,29, 32] and not testing for nonlinearity or effect modification by gender may contribute to the discrepancy between the present and previous results, but differences in the content of personality measures may be even more important: Sutin and Terracciano [33] discuss that scales measuring the anger and impulsivity aspects of neuroticism tend to show positive associations with BMI [8], whereas scales assessing emotional vulnerability show more variability, including inverse associations [26]. The latter may well apply to our results, as the psychogenic need to defend one’s status is strongly associated with the vulnerability facet of neuroticism.
Interventions targeting underlying thought patterns rather than eating behaviours per se, such as cognitive behavioural therapy [34, 35] and mindfulness-based approaches [36], have been shown to be successful in reducing emotional eating and excess body weight. In contrast, patients with weight problems and low levels of neuroticism or need for defence of status, who do not display the typical signs of emotional eating, may benefit from more conventional methods of weight loss, including a healthier diet and a more physically active lifestyle. It is hypothesised that high self-confidence and low sensitivity to the thoughts of others protect these individuals from the pressure to conform to contemporary body image and dieting culture, and part of this association is mediated by a low basal metabolic rate [25, 26]. Supplementary Fig. S3 illustrates the proposed risk factors of obesity as well as their treatment.
Strengths and limitations
The data in this study was taken from the Population Study of Women in Gothenburg, which consists of a relatively large sample of working-age women, with a high participation rate by today’s standards (68%). The objective assessment of anthropometry is a strength of the study that distinguishes it from other studies using self-reported weight and height, which carries the risk of under-reporting. The adjustment of regression models for the control variables ‘acquiescence’ and ‘the propensity to give socially desirable answers’ is another strength. One of the limitations of the study is that it only included female participants. While emotional eating behaviour is most strongly related with weight status in women, uncontrolled eating may be more decisive in men [37], and there may be gender differences with respect to the psychogenic needs as well. Furthermore, the study is cross-sectional, rendering it difficult to establish causality. Longitudinal studies examining weight development after the treatment of psychological problems, e.g. through cognitive behavioural therapy, could help to understand whether psychogenic needs give rise to excessive eating behaviour or vice versa.
Conclusions
This study identified specific psychological factors underlying excessive eating behaviours, which both supports the psychogenic cause of overeating and gives directives for its treatment. For the middle-aged women studied here, the need to defend one’s status and aspects of neuroticism were shown to be associated with excessive emotional eating, a behaviour that also correlates with obesity. The highly specific questions underlying the assessment of psychogenic needs may inform the treatment of emotional eating and unhealthy body weight. The association between low need for defence of status and excessive body weight independent of emotional eating was a novel finding that illustrates the heterogeneity of risk factors for overweight and obesity. While not directly linked with eating behaviour it should be the subject of future studies.
Data availability
The data sets used and analysed during the current study are available from the corresponding author upon reasonable request.
References
Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–81.
de Lauzon B, Romon M, Deschamps V, Lafay L, Borys JM, Karlsson J, et al. The three-factor eating questionnaire-R18 is able to distinguish among different eating patterns in a general population. J Nutr. 2004;134:2372–80.
Anglé S, Engblom J, Eriksson T, Kautiainen S, Saha MT, Lindfors P, et al. Three factor eating questionnaire-R18 as a measure of cognitive restraint, uncontrolled eating and emotional eating in a sample of young Finnish females. Int J Behav Nutr Phy. 2009;6:41.
Duarte PAS, Palmeira L, Pinto-Gouveia J. The Three-Factor Eating Questionnaire-R21: a confirmatory factor analysis in a Portuguese sample. Eat Weight Disord St. 2020;25:247–56.
Cappelleri JC, Bushmakin AG, Gerber RA, Leidy NK, Sexton CC, Lowe MR, et al. Psychometric analysis of the Three-Factor Eating Questionnaire-R21: results from a large diverse sample of obese and non-obese participants. Int J Obes. 2009;33:611–20.
Mehlig K, Sliwa P, Blomstrand A, Farhan L, Hällström T, Hange D. Eating Behaviors and Adiposity Indicators - Observations from the 2016/17 Examination of the Population Study of Women in Gothenburg. Int J Gen Med. 2024;17:2101–11.
Gilmartin T, Gurvich C, Sharp G. The relationship between disordered eating behaviour and the five factor model personality dimensions: A systematic review. J Clin Psychol. 2022;78:1657–70.
Sutin AR, Ferrucci L, Zonderman AB, Terracciano A. Personality and obesity across the adult life span. J Pers Soc Psychol. 2011;101:579–92.
Atherton OE, Sutin AR, Terracciano A, Robins RW. Stability and Change in the Big Five Personality Traits: Findings From a Longitudinal Study of Mexican-Origin Adults. J Personal Soc Psychol. 2022;122:337–50.
Cesarec Z, Marke S. Mätning av psykogena behov med frågeformulärsteknik. (Manual of the Cesarec-Marke Personality Schedule; CMPS). Stockholm, Skandinaviska Testförlaget, 1968.
Murray HA. Explorations in Personality. New York: Oxford University Press; 1938.
André M, Lissner L, Bengtsson C, Hällström T, Sundh V, Björkelund C. Cohort differences in personality in middle-aged women during a 36-year period. Results from the Population Study of Women in Gothenburg. Scand J Public Heal. 2010;38:457–64.
Billstedt E, Waern M, Falk H, Duberstein P, Östling S, Hällström T, et al. Time Trends in Murray’s Psychogenic Needs over Three Decades in Swedish 75-Year-Olds. Gerontology. 2017;63:45–54.
Eysenck HJ. A Short Questionnaire for the Measurement of 2 Dimensions of Personality. J Appl Psychol. 1958;42:14–7.
Eysenck HJ, Eysenck SBG. Manual of the Eysenck personality inventory. London: University of London Press LTD; 1964.
Rödström K, Weman L, Sandin L, Hange D, Björkelund C. Is it possible to investigate menopausal age? A comparative cross-sectional study of five cohorts between 1968 and 2017 from the Population Study of Women in Gothenburg, Sweden. Menopause. 2020;27:430–6.
Bengtsson C, Ahlqwist M, Andersson K, Bjorkelund C, Lissner L, Soderstrom M. The Prospective Population Study of Women in Gothenburg, Sweden, 1968-69 to 1992-93 - A 24-year follow-up study with special reference to participation, representativeness, and mortality. Scand J Prim Health. 1997;15:214–9.
Chacko SA, Chiodi SN, Wee CC. Recognizing disordered eating in primary care patients with obesity. Prev Med. 2015;72:89–94.
Murray HA. Explorations in Personality, 1963. J Proj Tech Pers Ass. 1964;28:172.
Piedmont RL, Mccrae RR, Costa PT. An Assessment of the Edwards Personal Preference Schedule from the Perspective of the 5-Factor Model. J Pers Assess. 1992;58:67–78.
Elfhag K, Morey LC. Personality traits and eating behavior in the obese: poor self-control in emotional and external eating but personality assets in restrained eating. Eat Behav. 2008;9:285–93.
Keller C, Siegrist M. Does personality influence eating styles and food choices? Direct and indirect effects. Appetite. 2015;84:128–38.
Tan CC, Chow CM. Stress and emotional eating: The mediating role of eating dysregulation. Pers Indiv Differ. 2014;66:1–4.
Ozier AD, Kendrick OW, Leeper JD, Knol LL, Perko M, Burnham J. Overweight and obesity are associated with emotion- and stress-related eating as measured by the Eating and Appraisal Due to Emotions and Stress Questionnaire. J Am Diet Assoc. 2008;108:49–56.
Terracciano A, Schrack JA, Sutin AR, Chan W, Simonsick EM, Ferrucci L. Personality, metabolic rate and aerobic capacity. PLoS One. 2013;8:e54746.
Arumae K, Mottus R, Vainik U. Beyond BMI: Personality traits’ associations with adiposity and metabolic rate. Physiol Behav. 2022;246:113703.
Magee CA, Heaven PCL. Big-Five personality factors, obesity and 2-year weight gain in Australian adults. J Res Pers. 2011;45:332–5.
Faith MS, Flint J, Fairburn CG, Goodwin GM, Allison DB. Gender differences in the relationship between personality dimensions and relative body weight. Obes Res. 2001;9:647–50.
Brummett BH, Babyak MA, Williams RB, Barefoot JC, Costa PT, Siegler IC. NEO personality domains and gender predict levels and trends in body mass index over 14 years during midlife. J Res Pers. 2006;40:222–36.
Armon G, Melamed S, Shirom A, Shapira I, Berliner S. Personality Traits and Body Weight Measures: Concurrent and Across-Time Associations. Eur J Personal. 2013;27:398–408.
Jokela M, Hintsanen M, Hakulinen C, Batty GD, Nabi H, Singh-Manoux A, et al. Association of personality with the development and persistence of obesity: a meta-analysis based on individual-participant data. Obes Rev. 2013;14:315–23.
Bagnjuk J, König HH, Hajek A. Personality Traits and Obesity. Int J Env Res Pub He. 2019;16:2675.
Sutin AR, Terracciano A. Personality and Body Weight: Mechanisms, Longitudinal Associations and Context. Pasonariti Kenkyu. 2017;26:1–11.
Stahre L, Tarnell B, Hakanson CE, Hällström T. A randomized controlled trial of two weight-reducing short-term group treatment programs for obesity with an 18-month follow-up. Int J Behav Med. 2007;14:48–55.
Stahre L, Blomstrand A, Hällström T. Effectivness of cognitive behaviour therapy targeting eating behaviour for patients with abdominal obesity in an ordinary primary health care setting. Nov Res Asp Med Med Sci. 2023;8:102–18.
Lattimore P. Mindfulness-based emotional eating awareness training: taking the emotional out of eating. Eat Weight Disord Stud Anorex Bulim Obes. 2020;25:649–57.
Cornelis MC, Rimm EB, Curhan GC, Kraft P, Hunter DJ, Hu FB, et al. Obesity Susceptibility Loci and Uncontrolled Eating, Emotional Eating and Cognitive Restraint Behaviors in Men and Women. Obesity. 2014;22:E135–E41.
Funding
This work was supported by the Swedish State under the agreement between the Swedish Government and the county council, the ALF agreement (GBG-68771) as well as by The Health & Medical Care Committee of the Region Västra Götaland (VGFOUREG-586771). Open access funding provided by University of Gothenburg.
Author information
Authors and Affiliations
Contributions
Lena Farhan: Conceptualisation, formal analysis, methodology, writing: original draft, review & editing. Dominique Hange: Conceptualisation, funding acquisition, investigation, writing: review & editing. Tore Hällström: Conceptualisation, writing: review & editing. Cecilia Björkelund: Funding acquisition, investigation, writing: review & editing. Lauren Lissner: Funding acquisition, investigation, writing: review & editing. Lisbeth Stahre: Conceptualisation, writing: review & editing. Kirsten Mehlig: Conceptualisation, data curation, formal analysis, methodology, supervision, writing: review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Farhan, L., Hange, D., Hällström, T. et al. Personality, eating behaviour, and body weight: results from the population study of women in Gothenburg 2016/17. Int J Obes 49, 1272–1279 (2025). https://doi.org/10.1038/s41366-025-01764-y
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41366-025-01764-y
