
Abstract
Background
Current risk assessments of cardiovascular disease (CVD) outcomes attributable to transportation noise rely on estimates from the 2018 WHO Environmental Noise Guidelines. Since the publication of these guidelines, several studies have been conducted to determine the association between transportation noise sources and CVD; however, recent meta-analyses have not derived updated exposure-response functions.
Objective
We reviewed epidemiological evidence linking long-term exposure to road traffic, railway, and aircraft noise with non-fatal and fatal myocardial infarction, ischemic heart disease, stroke, and ischemic stroke, and derived exposure-response functions using the conventional and Burden of Proof (BoP) methodologies.
Methods
We systematically searched databases for cohort or case-control studies that determined the associations between non-fatal and/or fatal myocardial infarction, ischemic heart disease, stroke, and ischemic stroke and long-term exposure to road traffic, railway, aircraft noise in general populations. Exposure-response functions were generated using the conventional natural cubic splines and Burden of Proof Risk Function approaches.
Results
Twenty-six studies met our eligibility criteria. Road traffic noise was associated with 1% increase in the combined risk of stroke incidence and mortality (RR = 1.01, 95%CI: 1.00–1.02, p-value = 0.04), and with 5% increase under the BoP framework (RR = 1.05, 95%UI: 1.03–1.07). Railway noise was associated with 1% increase in myocardial infarction outcomes (RR = 1.01, 95%CI: 1.01–1.01, p-value < 0.0001), and with 16% increase under the BoP framework (RR = 1.16 95%UI: 1.07–1.26). Of the twelve risk-outcome pairs examined, five showed no evidence of association, four showed weak evidence, and the remainder lacked credible evidence or did not meet the BoP criteria. Compared with the natural splines approach, the BoP framework produced more plausible exposure-response curves.
Significance
This study adds to the existing literature by providing a comprehensive comparison of the association between long-term exposure to transportation noise sources and CVD outcomes using both conventional and BoP methodologies.
Impact statement
This is the first study to apply the conventional meta-regression and Burden of Proof methodologies to systematically quantify and evaluate associations between long-term exposure to transportation noise sources (i.e., road traffic, railway, and aircraft) and combined risk of fatal and non-fatal cardiovascular disease outcomes, including myocardial infarction, ischemic heart disease, stroke, and ischemic stroke. The application of these two approaches to deriving exposure-response functions provides additional insights into the quantification of the burden of disease attributable to transportation noise. Our findings using the Burden of Proof framework on transportation noise and CVD outcomes advance the integration of an additional environmental risk factor and propose new risk-outcome pairs for potential inclusion in the Global Burden of Disease study.
Similar content being viewed by others


Introduction
Transportation noise has emerged as a major environmental stressor that not only increases the risk of sleep disturbance and noise annoyance but also contributes to cardiovascular diseases (CVD), such as ischemic heart disease (IHD) and stroke, as well as CVD-related risk factors, such as hypertension and obesity [1,2,3,4]. To quantify the impact of transportation noise on population health, an exposure-response function between specific transportation noise sources—such as road traffic, railway, and aircraft noise—and associated health outcomes is warranted.
The 2018 Environmental Noise Guidelines for the WHO European Region were developed by an expert panel, employing the grading of recommendations, assessment, development, and evaluation (GRADE) tool to evaluate the quality of evidence from studies examining associations between various noise sources and health outcomes, and to derive noise source-specific exposure-response functions [5]. In these guidelines, the expert panel concluded that the quality of evidence supporting the association between transportation noise and CVD outcomes varied considerably. High-quality evidence was found for the association between road traffic noise and IHD. In contrast, the evidence for the association with railway noise was considered low-quality, and that for aircraft noise was deemed very low. The expert panel also concluded that the quality of evidence linking road traffic noise to stroke was of moderate quality. However, the data collection to support the above-described conclusions covered the period from January 2000 to August 2015 [5]. Since then, several population-based studies have been conducted to determine the association between transportation noise sources and CVD outcomes, yielding different results, likely due to heterogeneity in exposure assessment methods and/or population heterogeneity in demographic characteristics and contextual factors [6,7,8,9,10].
Exposure-response functions linking transportation noise with health outcomes are traditionally established through quantitative synthesis of studies, often involving traditional meta-analyses. These analyses combine effect sizes extracted from epidemiological studies and weight them by the inverse of their variances. Between-study heterogeneity is quantified, and mixed models that account for variability between studies are employed to adjust the weighting of each estimate in the pooled analysis [11, 12]. A more recent approach to deriving exposure-response functions is the Meta-Regression-Bayesian, Regularized, Trimmed (MR-BRT), which is part of the Burden of Proof (BoP) framework [13, 14]. The MR-BRT approach facilitates the detection and removal of outliers through a standardized trimming methodology and enables the integration of heterogeneous data into one model, thereby ensuring stable estimations of exposure-response curves [13, 15, 16]. This framework also accounts for heterogeneity in effect estimates between studies that is not explained by study-level factors, such as exposure measurement error or confounding. In addition, the BoP framework includes a risk-outcome score (ROS), which quantifies the strength of evidence based upon both the magnitude of the mean effect estimate and the degree of unexplained between-study heterogeneity [16]. The application of these two approaches to deriving exposure-response functions provides additional insights into quantifying the burden of disease attributable to transportation noise.
Therefore, we aimed to conduct a systematic review that includes a qualitative synthesis and quantitative meta-analysis of existing epidemiological evidence on the association between long-term exposure to transportation noise sources (i.e., road traffic, railway, and aircraft) and CVD outcomes. These outcomes included non-fatal (measured by incidence) and fatal (measured by mortality) myocardial infarction, IHD, stroke, and ischemic stroke. We also aimed to derive and critically discuss exposure-response functions using both the conventional meta-regression and BoP approaches to obtain conservative estimates and ratings of evidence strength.
Methods
Search strategy and selection criteria
We systematically searched the literature across six bibliographic databases (PubMed, Embase, Web of Science, Cochrane Central, Scopus, and Global Index Medicus) and an additional search engine (Google Scholar) from inception to July 4, 2023. We also hand-searched the reference lists of all identified systematic reviews and meta-analyses to find additional eligible records. The search strategy, developed by an experienced librarian of the Erasmus MC, is available in the Supplementary material (pp 4). The protocol has been registered in the PROSPERO database (CRD42023444656).
Without any geographical restrictions, we considered published papers if they met the following criteria: (i) cohort or case-control studies that determined the association between non-fatal and/or fatal major CVD outcomes, and long-term transportation noise source (i.e., road traffic, railway, aircraft) in general populations; (ii) studies that quantified a relative measure of association or number of cases and non-cases among exposed groups versus non-exposed comparators; (iii) studies that quantified the association for a certain increase in noise exposure (dB), either categorically or by assuming linearity (i.e. the risk in increase remains constant per noise exposure interval), and accounted for uncertainty; (iv) studies that explicitly reported on the noise exposure levels (e.g., 24 h average sound levels weighted with a penalty of 5 dB for evening time noise and 10 dB for nighttime noise; day-evening-night noise level (Lden)) and defined how and when the studied exposure was modeled; (v) studies that explicitly defined the studied disease outcomes based on the International Classification of Diseases codes; and (vi) studies published in English. It should be noted that if multiple publications reported on the same population, we considered the one with the longest follow-up duration, and consequently, the greatest number of disease cases. Details on the case definitions and exposure assessment criteria considered can be found in the Supplementary material (pp 5). We excluded cross-sectional, ecological, animal, and case studies, as well as publications, such as editorials, letters-to-the-editor, commentaries, and conference proceedings that lacked essential information (e.g., effect sizes and/or appropriate uncertainty information).
Data screening and extraction
After removing duplicates, we applied the above criteria to screen the titles and abstracts of all identified records, as well as the full texts of potentially eligible records. Two reviewers (PC & JH) independently conducted title/abstract screening using the EndNote 21 software. One researcher (PC) manually searched the reference lists of all identified systematic reviews and meta-analyses in order to detect additional studies. PC & EG documented all eligible records in an Excel spreadsheet, shared it with an expert in the field (GMA), and discussed the main reasons for inclusion/exclusion. PC, EG, JH & GMA discussed any disagreements arising from the eligibility criteria.
In addition, PC & EG used a validated data extraction form developed by the Global Burden of Disease (GBD) researchers to extract data pertaining to study characteristics, disease outcome, sources of noise exposure, adjusted confounders, and effect sizes and their uncertainty (Supplementary material pp 7). Where available, we extracted effect size estimates from models adjusted for factors including age, sex, socio-economic status, and correlated exposures, such as particulate matter smaller than 2.5 μm in aerodynamic diameter (PM2.5) and nitrogen dioxide (NO2). When multiple estimates were available, we prioritized those derived from the most adjusted models (i.e., models that accounted for air pollutants) over those that did not. In cases where transportation noise exposure was measured both as Lden and Lnight (i.e., equivalent continuous sound pressure level when the reference time interval is the night), the former was prioritized due to its overlap with the latter. PC, JH, GMA, and EG discussed any disagreements arising from data extraction items. It should be noted that researchers engaged in every stage of the review process received training from GBD researchers.
Methodological quality
Two reviewers (PC & EG) independently evaluated the methodological quality of the included papers using the Newcastle-Ottawa Scale (NOS) [17]. The NOS utilizes a nine-point scale, assigning points across three main domains: selection of participants (four points), comparability of cohorts or case-control groups (two points), and assessment of outcomes and adequacy of follow-up (three points). We classified studies into three categories based on their methodological quality: low (score: 0–3 points), medium (score: 4–6 points), and high (score: 7–9 points). Any disagreements were resolved by consensus.
Data analysis and synthesis
Systematic review
A narrative synthesis was conducted by classifying studies according to their study characteristics (e.g., year of publication, geographical location, methodological quality, model adjustments, risk-outcome pairs assessed, and CVD outcomes covered) and whether they examined non-fatal or fatal events.
Data pre-processing
Records were deemed appropriate for meta-analysis if at least three independent studies had an equivalent exposure, disease outcome, and health indicators, and if they reported the same or equivalent effect statistics, thereby enabling meaningful and interpretable pooling of estimates. Risk measures were reported in varying formats (i.e., categorical or continuous values). To ensure consistency, we standardized these measures by converting categorical data to a common 10 dB increment and scaling the midpoints to the Lden indicator [18]. These standardized values were modeled against the associated risk measure using the dosresmeta package [19]. A detailed description of the conversion process is available in the Supplementary material (pp 15).
Conventional meta-analyses and meta-regression
Fixed-effects models were fitted, and between-study heterogeneity was quantified with Cochran’s Q and I [2] statistics (Supplementary material pp 16). If the p-value associated with the heterogeneity test was lower than 0.05, a random-effects model was preferred. Publication and reporting bias were assessed with visual inspection of funnel plots. Relative risk (RR) estimates, 95% confidence intervals (95%CI), and I [2] were reported. In an additional step, a meta-regression was employed to model log(RR) against noise exposure levels using natural cubic splines [20]. To characterize the shape of the relationship between exposure and the log(RR), splines with three knots were used to account for potential non-linear trends across the noise exposure range. Exposure-response functions were plotted from meta-regression results. It should be noted that studies trimmed from the MR-BRT approach were excluded from the conventional meta-analyses and meta-regression, facilitating comparisons between the two approaches. Supplemental conventional meta-analyses on major fatal and fatal CVD outcomes, without pooling trimmed estimates, were conducted (Supplementary material pp 20). All statistical analyses were performed using R version 4.3.2 [21].
Burden of proof (BoP) framework
We applied the GRADE guidelines to create a series of binary covariates capturing potential sources of bias [22]. Across all risk-outcome pairs analyzed, the covariates primarily included those measuring the representativeness of the study sample; whether exposure was measured at the overall population or a subpopulation only; risk of selection bias; reverse causation; and estimates uncontrolled for major confounders (Supplementary material pp 14). The potential effect of bias covariates was tested using the MR–BRT automated covariate selection process, which applies a LASSO strategy to identify statistically significant covariates at a threshold of 0.05 [16, 23]. To quantify between-study heterogeneity, the framework accounts for within-study correlations, overall study variability, and the influence of a limited number of studies. The Fisher information matrix, along with the final uncertainty estimate, was then generated to quantify the posterior uncertainty associated with the fixed effect (as in the conventional meta-analytical approach) [13]. RR estimates, with and without adjustment for between-study heterogeneity, were presented with corresponding 95% uncertainty intervals (95%UI). Publication and reporting bias were assessed with visual inspection of funnel plots (as in the conventional meta-analytical approach). To characterize the shape of each exposure-risk association, knots were placed anywhere within the 5th and 95th percentiles of the data; shape constraints were applied to ensure that the resulting exposure-response functions were concave down and exhibited monotonic behavior. We estimated the Burden of Proof Risk Function (BPRF), reflecting the most conservative estimate of the association between transportation noise sources and CVD. ROS were calculated from the BPRF as the log(BPRF) divided by 2. ROS were categorized into star-rating categories ranging from one to five; a one-star (ROS value: ≤0.0) indicates weak evidence of association, while a five-star (ROS value: >0.62) indicates very strong evidence of association [13, 16]. It should be noted that risk-outcome pairs with a zero-star association do not meet the GBD inclusion criteria and were thus excluded from further discussion. Further details of the BoP framework have been described elsewhere[16]. All statistical analyses were performed using R version 4.3.2 and Python version 3.10.4 [21, 24].
Research and reporting practices
This study complies with both the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Supplementary material pp 24) and the GATHER (Supplementary material pp 27) guidelines [25, 26]. All code used for both the conventional meta-regression (https://github.com/egonzato/noisecvds_meta-analysis) and MR-BRT analyses (https://github.com/ihmeuw-msca/burden-of-proof/) are publicly available.
Results
Literature review
After removing duplicates, we identified a total of 1339 relevant records through electronic database searches, gray literature, and handsearching. The full texts of 153 articles were systematically reviewed and led to the final inclusion of 26 unique studies (Fig. 1).

Flowchart of the literature search and study selection.
Study characteristics and methodological quality assessment
Of the 26 studies considered eligible, the vast majority (n = 25) were conducted at a single-country level, with 23 performed in European countries (Table 1 & Supplementary Fig. S1, Supplementary material pp 19) [6, 8, 27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46]. The lowest number of studies was conducted in the United States (n = 1) [47] and Canada (n = 2) [48, 49], whereas the highest number of studies was conducted in Denmark (n = 8) [30, 33, 35, 36, 40,41,42,43], followed by Germany (n = 5)[27, 37, 38, 44, 46]. The risk-outcome pair that was studied the most was road traffic noise and myocardial infarction (n = 16) [6, 27,28,29, 31,32,33,34, 36, 38, 41, 43,44,45, 48, 49], followed by road traffic noise and stroke (n = 11)[6,7,8, 29,30,31,32, 34, 35, 37, 39, 40]. The risk-outcome pairs involving railway (n = 3) and aircraft noise (n = 4) were the least studied (Table 1 & Supplementary Fig. S2, Supplementary material pp 19). Regarding model adjustments, all studies controlled for age and gender, while a few accounted for lifestyle attributes, thereby limiting adjustments to socio-demographic variables (e.g., highest attained level of education, income). More than half of the studies (n = 14) controlled for one or more air pollutants, with PM2.5 being the most commonly adjusted pollutant. Out of the 26 studies, the majority (n = 19) were classified as high-quality[6,7,8, 29, 30, 32,33,34,35,36,37,38,39,40, 42, 43, 47,48,49]. The remaining studies were classified as medium-quality [27, 28, 31, 41, 44,45,46], primarily due to limitations in outcome definition [28, 45] and/or inaccuracies in defining cases and controls [27, 44, 46].
Conventional meta-analyses and meta-regression: estimation of exposure-response relationships
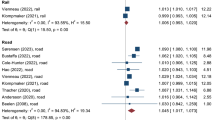
Figures 2–5 depict the results of conventional meta-analyses, including forest plots, exposure-response curves, and funnel plots for all transportation noise sources and major CVD. We found a 2, 1, and 2% increase in risk per 10 dB for myocardial infarction associated with road traffic noise (RR = 1.02, 95%CI: 1.00–1.05 95%CI, p-value = 0.08), railway noise (RR = 1.01, 95%CI: 1.01–1.01, p-value < 0.0001), and aircraft noise (RR = 1.02, 95%CI: 0.99–1.05, p-value = 0.14), respectively (Fig. 2A–Ci). Heterogeneity was high for the association between road traffic noise and myocardial infarction (I2 = 87%), with a prediction interval of 0.94–1.11, and for between aircraft noise and myocardial infarction (I2 = 77%), with a prediction interval of 0.95–1.09. Heterogeneity was low for the association between railway noise and myocardial infarction (I² = 21%), for which a fixed-effects model was applied (Fig. 2A–Ci). The exposure-response curves for road traffic and aircraft noise exhibited a relatively stable pattern across the exposure range, while a more pronounced increase in risk was observed above 60 dB for railway noise (Fig. 2A–Cii). There was no visual evidence of publication or reporting bias in studies determining the association between road traffic noise and myocardial infarction (Fig. 2Aiii), whereas a slight asymmetry was observed in the funnel plot for railway noise and myocardial infarction (Fig. 2Biii).

A Road traffic noise, B railway noise, C aircraft noise. (i) Forest plot of underlying relative risk (RR) data, (ii) log(RR) exposure-response function; and (iii) modified funnel plot showing the residuals (relative to 0) on the x axis and the estimated standard error and between-study heterogeneity on the y axis. Note: Meta-regression was performed using relative risk estimates associated with each noise exposure category to construct the exposure-response function (ii). Estimates from the same study were interpolated and pooled into a single estimate (per 10 dB increase), which was then pooled in the meta-analysis.

A Road traffic noise, B aircraft noise. (i) Forest plot of underlying relative risk (RR) data, (ii) log(RR) exposure-response function; and (iii) modified funnel plot showing the residuals (relative to 0) on the x axis and the estimated standard error and between-study heterogeneity on the y axis. Note: Meta-regression was performed using relative risk estimates associated with each noise exposure category to construct the exposure-response function (ii). Estimates from the same study were interpolated and pooled into a single estimate (per 10 dB increase), which was then pooled in the meta-analysis.

A Road traffic noise, B railway noise, C aircraft noise. (i) Forest plot of underlying relative risk (RR) data, (ii) log(RR) exposure-response function; and (iii) modified funnel plot showing the residuals (relative to 0) on the x axis and the estimated standard error and between-study heterogeneity on the y axis. Note: Meta-regression was performed using relative risk estimates associated with each noise exposure category to construct the exposure-response function (ii). Estimates from the same study were interpolated and pooled into a single estimate (per 10 dB increase), which was then pooled in the meta-analysis.

A Road traffic noise, B railway noise, C aircraft noise. (i) Forest plot of underlying relative risk (RR) data; (ii) log(RR) exposure-response function; and (iii) modified funnel plot showing the residuals (relative to 0) on the x axis and the estimated standard error and between-study heterogeneity on the y axis. Note: Meta-regression was performed using relative risk estimates associated with each noise exposure category to construct the exposure-response function (ii) Estimates from the same study were interpolated and pooled into a single estimate (per 10 dB increase), which was then pooled in the meta-analysis.
We observed a slight, not significant, increase in the risk for IHD associated with road traffic noise (RR = 1.01, 95%CI: 0.96–1.07, p-value = 0.64), while the association between aircraft noise and IHD was negligible (RR = 1.00, 95%CI: 1.00–1.01, p-value = 0.34, Fig. 3A, Bi). Heterogeneity was high for the association between road traffic noise and IHD (I² = 92%), and the prediction interval contained 1.0 (0.87–1.17). Not enough point estimates were available to determine the association between railway noise and IHD.
We also found no significant association between stroke and railway noise (RR = 1.00, 95%CI: 1.00–1.01, p-value = 0.08 & I2 = 50%) and aircraft noise (RR = 1.01, 95%CI: 0.99–1.02, p-value = 0.42 & I2 = 0%), while a 1% increase in risk was observed for road traffic noise (RR = 1.01, 95%CI: 1.00–1.02, p-value = 0.04 & I2 = 83%), (Fig. 4A–Ci). The greatest heterogeneity was estimated for the association between road traffic noise and stroke (I² = 83%), and the corresponding prediction interval contained 1.0 (0.98–1.04). The exposure-response curve for road traffic noise and stroke showed a gradual increase across the exposure range (Fig. 4Aii), whereas the curve for railway noise and stroke followed an exponential pattern (Fig. 4Bii). In contrast, the curve for aircraft noise and stroke remained flat, with a slight decrease beyond 55 dB (Fig. 4Cii). A 5% increase in ischemic stroke risk was associated with exposure to aircraft noise (RR = 1.05, 95%CI: 1.02–1.08, p-value = 0.0006 & I2 = 0%, Fig. 5Ci). The exposure-response curve for aircraft noise and ischemic stroke displayed a slight upward trend above 50 dB (Fig. 5Cii). We found no evidence of publication bias in studies examining the association between road traffic and stroke (Fig. 4Aiii), nor in studies on road traffic and ischemic stroke (Fig. 5Aiii).
Burden of Proof (BoP) framework: estimation of exposure-response relationships
Table 2 shows the estimates of all identified risk-outcome pairs. Figures 6–9 illustrate the results of the BoP framework, including log(RR) functions, RR functions, and funnel plots, for transportation noise sources and major CVD outcomes. Among the assessed risk-outcome pairs, four had a two-star rating, suggesting that exposure to transportation noise sources increases the risk of a given CVD outcome by 0-15% which can be interpreted as weak evidence. For example, myocardial infarction showed a two-star association with railway noise (RR = 1.16, 95%UI inclusive between-study heterogeneity: 1.07–1.26, ROS = 0.02, BPRF = 1.04) and with aircraft noise (RR = 1.09, 95%UI inclusive between-study heterogeneity: 1.01–1.18, ROS = 0.01, BPRF = 1.02), Table 2. Among the two-star associations, the largest number of studies was found for the association between road traffic noise and stroke (n = 10 studies, RR = 1.05, 95%UI inclusive between-study heterogeneity: 1.03–1.07, ROS = 0.01, BPRF = 1.02, Table 2 & Fig. 8A).

A Road traffic noise, B railway noise, C aircraft noise. (i) Log(RR) function; (ii) RR function; and (iii) modified funnel plot showing the residuals (relative to 0) on the x axis and the estimated standard error and between-study heterogeneity on the y axis.

A Road traffic noise, B aircraft noise. (i) log(RR) function; (ii) RR function; and (iii) modified funnel plot showing the residuals (relative to 0) on the x axis and the estimated standard error and between-study heterogeneity on the y axis.

A Road traffic noise, B railway noise, C aircraft noise. (i) Log(RR) function; (ii) RR function; and (iii) modified funnel plot showing the residuals (relative to 0) on the x axis and the estimated standard error and between-study heterogeneity on the y axis.

A Road traffic noise, B railway noise, C aircraft noise. (i) Log(RR) function; (ii) RR function; and (iii) modified funnel plot showing the residuals (relative to 0) on the x axis and the estimated standard error and between-study heterogeneity on the y axis.
The BPRF analysis yielded a one-star rating for five risk-outcome pairs (e.g., aircraft noise and ischemic stroke, RR = 1.15, 95%UI inclusive between-study heterogeneity: 0.92–1.45, ROS = −0.01, BPRF = 0.98, Table 2), indicating that exposure to transportation noise sources is weakly associated with certain CVD outcomes. Among the one-star associations, the largest number of studies was found for the association between road traffic noise and myocardial infarction (n = 15 studies, RR = 1.10, 95%UI inclusive between-study heterogeneity: 0.79–1.56, ROS = −0.07, BPRF = 0.87, Table 2) and for road traffic noise and ischemic stroke (n = 10 studies, RR = 1.05, 95%UI inclusive between-study heterogeneity: 0.99–1.11, ROS = 0.00, BPRF = 1.00, Table 2). The RR function for railway noise and IHD could not be estimated due to insufficient data, while ROS and BPRF estimation for aircraft noise and IHD and stroke was not feasible due to non-detectable between-study heterogeneity (I2 = 0%). None of the covariates examined was significant across the assessed risk-outcome pairs.
The mean risk curves either increased sharply (e.g., railway noise and myocardial infarction, Fig. 6B; road traffic noise and IHD, Fig. 7A; railway noise and ischemic stroke, Fig. 9B), increased steadily (e.g., road traffic noise and myocardial infarction, Fig. 6Aii & road traffic noise and ischemic stroke, Fig. 9Aii) or plateaued (e.g., aircraft noise and myocardial infarction, Fig. 6Cii & aircraft noise and stroke, Fig. 8Cii). Most funnel plots (Figs. 6–9iii) showed that, after trimming, the residual standard error—reflecting both variance and between-study heterogeneity—fell within the expected range of the model. However, slight asymmetry was observed in the funnel plot for railway noise and myocardial infarction (Fig. 6Biii).
Discussion
This is the first study to apply the conventional meta-regression and MR-BRT approach to quantify and evaluate associations between long-term exposure to transportation noise sources (i.e., road traffic, railway, and aircraft) and combined risk of non-fatal and fatal CVD outcomes, including myocardial infarction, IHD, stroke, and ischemic stroke. Of the 26 studies included, most were cohort studies conducted in Europe and focused on road traffic noise. Long-term exposure to road traffic and railway noise was significantly associated with increased risk of stroke and myocardial infarction, respectively. These two risk-outcome pairs showed the strongest and most consistent associations across both the conventional meta-regression and MR-BRT approach; however, the strength of evidence was classified as weak. Differences in curve shapes were observed, with the conventional meta-regression approach allowing the curves to fluctuate in response to the input estimates, and the MR-BRT approach producing smoother and more plausible exposure-response curves.
This study shows that substantial new evidence on transportation noise sources and major CVD outcomes has emerged since the publication of the 2018 WHO Environmental Noise Guidelines [5]. Our conventional meta-analysis yielded a pooled RR estimate of 1.01 (95%CI: 1.00–1.02) per 10 dB Lden for the association between road traffic noise and stroke. This risk is lower compared to a recent systematic review and meta-analysis that reported a RR estimate of 1.025 (95%CI: 1.009–1.041) for road traffic noise and stroke incidence [50]. The difference in RR likely reflects variations in study inclusion criteria and/or differences in weighting approaches. However, when applying the MR-BRT approach, which accounts for study-specific deviations and down-weights inconsistent evidence, we found more robust evidence of the association of road traffic noise with stroke (RR = 1.05, 95%UI: 1.03–1.07).
Furthermore, our conventional meta-analysis identified a positive association between road traffic noise and myocardial infarction (RR = 1.02, 95%CI: 1.00–1.05), whereas the MR-BRT approach produced a higher estimate (RR = 1.10, 95%UI: 0.79–1.56) for this association. The wider 95%UI, compared with those (typically) reported in traditional meta-analyses, reflects the inclusion of unexplained heterogeneity beyond between-study heterogeneity in mean effects [13, 16]. Our conventional meta-analysis results are consistent in direction and magnitude with those of previous meta-analyses reporting modest but statistically significant associations; however, differences in study inclusion criteria and model adjustments may limit direct comparability [50, 51]. For example, inconsistent adjustments for correlated traffic-related exposures have previously been found. The major challenge is that transportation noise and air pollution correlate, reflecting that traffic is the main source of both exposures. Eminson et al. found no strong evidence that air pollution confounds the associations between traffic noise and CVD outcomes, whereas Pershagen et al. found that PM2.5, but not NO2, confounded the traffic noise-related associations [50, 52]. One possible explanation for these inconsistent findings is that disentangling the effects of both transportation noise and air pollution exposures requires a high-quality assessment of both in order to avoid one exposure being estimated more precisely than the other. Some studies have therefore recommended deriving two-pollutant effect estimates when correlations between air pollutants are low [53, 54]. Inclusion of highly correlated air pollutants when deriving two-pollutant effect estimates can attenuate the true long-term effects of noise. Sørensen et al. reported that long-term exposure to NO2 and road traffic noise was associated with increased risk of CVD outcomes in both single- and two-pollutant models, while Osborne et al. reported that combined exposure to both noise and air pollution was associated with increased risk of major adverse CVD events [55, 56]. Experimental studies are needed to further examine the effects of simultaneous exposure to traffic noise and air pollution and to address how these exposures interact at a mechanistic level.
Consistent with previous systematic reviews and meta-analyses, we identified only two studies examining the association between railway noise and myocardial infarction [57,58,59]. Our conventional meta-analysis showed a minimal effect of a 10 dB Lden increase in railway noise exposure on the combined risk of myocardial infarction incidence and mortality (RR = 1.01, 95%CI: 1.01–1.01), whereas the MR-BRT approach yielded a RR estimate of 1.16 (95%UI: 1.07–1.26). The estimate derived from the conventional meta-analysis was lower than the hazard ratio (HR) reported for fatal myocardial infarction in a large Danish and Swedish cohort study (HR = 1.08, 95%CI: 0.99–1.17), whereas the one derived from the MR-BRT was higher [60].
We also found aircraft noise as a potential environmental risk factor for the combined risk of ischemic stroke incidence and mortality; our conventional meta-analysis yielded a RR estimate of 1.05 (95%CI: 1.02–1.08), whereas the MR-BRT yielded a RR estimate of 1.15 (95%UI: 1.11–1.26). Ischemic stroke accounts for approximately two-thirds of all incident strokes and has previously been reported to be significantly associated with transportation noise sources, such as road traffic noise [61, 62]. Noise-induced endothelial dysfunction is a recognized biological mechanism that increases thrombotic risk and contributes to the development of ischemic stroke [63]. In a nationwide cohort study from Switzerland, Héritier et al. found significant positive associations of both road traffic and aircraft noise with ischemic stroke mortality, but not with stroke in general [10]. Similar findings have also been reported in the same cohort with longer follow-up time [6].
This study revealed marked differences between the conventional meta-regression and the MR-BRT approach. These differences were particularly evident in risk-outcome pairs with limited underlying evidence, which demonstrates the strength of the MR-BRT approach in generating more robust and plausible effect estimates when input data are sparse or scattered. Differences were further evident in the exposure-response curves: those derived using natural cubic splines were non-smooth and less interpretable compared to those derived with the MR-BRT approach. Using Bayesian priors, the MR-BRT approach reduces the influence of outliers, producing smoother curves and showing a consistent increase in risk, particularly at higher exposure levels (e.g., road traffic noise-IHD and aircraft noise-IHD pairs, Fig. 3A, Bii & Fig. 7A, Bii). Future conventional meta-regression analyses should acknowledge the methodological limitations of natural cubic splines in modeling exposure-response functions, particularly when comparing region-specific curves that may be affected by differences in noise exposure levels, study design, and/or confounding factors.
In this study, we pooled estimates from studies reporting either disease incidence or mortality. This approach is consistent with the BoP framework, which supports a unified risk estimate under specific conditions: when a common biological mechanism is presumed, when only incidence or mortality data are available, or when no statistically significant difference is observed between the two outcomes [16, 64]. Chronic stress, sleep disturbance, vascular inflammation, and endothelial dysfunction have been proposed as key biological pathways linking environmental noise to CVD [58, 65]. Although these mechanisms likely contribute to both non-fatal and fatal events, mortality is also influenced by additional factors, such as comorbidities and access to healthcare. Thus, combining morbidity and mortality outcomes in meta-analyses may mask differential risks. Nevertheless, in our stratified analyses, we observed similar pooled RR for road traffic noise and non-fatal myocardial infarction (RR = 1.04, 95%CI: 0.98-1.11, Supplementary Fig. S3, Supplementary material pp 18) and fatal myocardial infarction (RR = 1.04, 95%CI: 1.03-1.05, Supplementary Fig. S4, Supplementary material pp 18). We also observed that road traffic noise was the most frequently studied transportation noise source, and that its associations with CVD outcomes exhibited greater between-study heterogeneity than those observed for railway and aircraft noise. This heterogeneity may reflect the broader range of geographical and urban settings in which road traffic noise has been studied, leading to variation in study population composition, the quality of the noise exposure assessment, and the extent and quality of adjustment as well as other unmeasured sources of bias. By contrast, data on aircraft and railway noise remain limited primarily due to monitoring challenges [66, 67]. These challenges increase the risk of underrepresenting affected populations. For instance, railway noise is a relatively rare exposure, affecting a limited proportion of the population. We also observed substantial variability across studies in the noise indicators used to assess participant exposure, including methods used to quantify exposure and the predictive models used to map noise exposure across urban grids [68]. Lden should continue to be regarded as the preferred noise indicator for measuring exposure, as its standardized nature allows for more consistent comparisons of findings [18]. In addition, most of the included studies were conducted in Denmark, Germany, and Sweden—countries that have long recognized environmental noise as a significant public health concern. More efforts, including regulatory and legislative changes, are needed across the European region in order to achieve the European Union’s zero pollution action target: “reducing the share of people chronically disturbed by transport noise by 30%” [69, 70].
This study must be considered within its limitations. First, the small number of studies per risk–outcome pair precluded the derivation of stratified exposure-response functions by age, gender, and other covariates. Second, due to the relatively small number of studies analyzed per risk-outcome pair, it was not feasible to disentangle whether, or to what extent, confounders drove differences between studies. Third, this study may have introduced a potential bias by limiting inclusion to studies published in English. Fourth, this study included a limited number of studies that used physical measurements to assess exposures, which precluded sensitivity analyses comparing the impact of different assessment methods (e.g. physical measurement versus predictive models) on the association between transportation noise sources and cardiovascular disease outcomes. Nevertheless, future systematic reviews and meta-analyses should address this, as differences in exposure assessment methods may influence overall effect estimates. Although the two approaches used in the present study relied on trimmed effect estimates, differences in study weighting (i.e., inverse-variance weighting in conventional meta-analysis versus penalized regression in MR-BRT) and in the handling of residual heterogeneity likely contributed to the discrepancy in effect estimates. Our conventional meta-analysis incorporated trimmed data primarily to enable direct comparison with BPRF estimates, and also because conventional meta-analyses often overestimate risks by pooling heterogeneous data without adequately addressing outliers and study variability. The BoP framework addresses these issues, producing more precise, reliable, and conservative risk estimates that are also more robust. Given these advantages, we recommend using BoP framework risk functions in future transportation noise-specific burden-of-disease assessments. Our study contributes to the existing literature on transportation noise-related risk functions, which are quintessential to determining the burden of disease attributable to transportation noise. A landmark study that provides such population health data is the GBD study. While the most recent iteration of the GBD study has expanded the range of environmental risk factors included, such as the inclusion of ambient NO2 and non-optimal temperatures, transportation noise is currently not covered, even though it may represent a significant contributor to the global disease burden [16, 71]. Our findings using the BoP framework on transportation noise and major CVD outcomes advance the integration of an additional environmental risk factor and propose new risk-outcome pairs for potential inclusion in the GBD study.
Data availability
The appendix provides the full list of articles that informed this systematic review and meta-analysis, information about the articles, and overview of the study methodology and performed statistical analyses. All code used for the conventional meta-analyses (github.com/egonzato/noisecvds_meta-analysis) and for the MR-BRT (github.com/ihmeuw-msca/burden-of-proof) are publicly available.
References
Münzel T, Daiber A. The environmental stressors noise and air pollution are important cardiovascular risk factors. Padiatr Prax. 2019;92:171–84.
Münzel T, Sørensen M, Daiber A. Transportation noise pollution and cardiovascular disease. Nat Rev Cardiol. 2021;18:619–36.
Basner M, Babisch W, Davis A, Brink M, Clark C, Janssen S, et al. Auditory and non-auditory effects of noise on health. Lancet 2015;383:1325–32.
Persson Å, Pyko A, Stucki L, Ögren M, Åkesson A, Oudin A, et al. Long-term exposure to transportation noise and obesity: A pooled analysis of eleven Nordic cohorts. Environ Epidemiol. 2024;8:e319.
World Health Organization. Regional Office for Europe. Environmental noise guidelines for the European Region. Copenhagen: World Health Organization. Regional Office for Europe; 2018.
Vienneau D, Saucy A, Schäffer B, Flückiger B, Tangermann L, Stafoggia M, et al. Transportation noise exposure and cardiovascular mortality: 15-years of follow-up in a nationwide prospective cohort in Switzerland. Environ Int. 2022;158:106974.
Andersson EM, Ögren M, Molnár P, Segersson D, Rosengren A, Stockfelt L. Road traffic noise, air pollution and cardiovascular events in a Swedish cohort. Environ Res. 2020;185:109446.
Pyko A, Andersson N, Eriksson C, de Faire U, Lind T, Mitkovskaya N, et al. Long-term transportation noise exposure and incidence of ischaemic heart disease and stroke: a cohort study. Occup Environ Med. 2019;76:201–7.
Roswall N, Pyko A, Ögren M, Oudin A, Rosengren A, Lager A, et al. Long-term exposure to transportation noise and risk of incident stroke: a pooled study of nine Scandinavian cohorts. Environ Health Perspect. 2021;129:107002.
Héritier H, Vienneau D, Foraster M, Eze IC, Schaffner E, Thiesse L, et al. Transportation noise exposure and cardiovascular mortality: a nationwide cohort study from Switzerland. Eur J Epidemiol. 2017;32:307–15.
Muka T, Glisic M, Milic J, Verhoog S, Bohlius J, Bramer W, et al. A 24-step guide on how to design, conduct, and successfully publish a systematic review and meta-analysis in medical research. Eur J Epidemiol. 2020;35:49–60.
Thompson SG. Why sources of heterogeneity in meta-analysis should be investigated. BMJ. 1994;309:1351–5.
Zheng P, Afshin A, Biryukov S, Bisignano C, Brauer M, Bryazka D, et al. The burden of proof studies: assessing the evidence of risk. Nat Med. 2022;28:2038–44.
Zheng P, Barber R, Sorensen RJD, Murray CJL, Aravkin AY. Trimmed constrained mixed effects models: formulations and algorithms. J Comput Graph Stat. 2021;30:544–56.
Yang E, Lozano AC, Aravkin A A general family of trimmed estimators for robust high-dimensional data analysis. Electron J Statist. 2018;12:3519–53.
GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:2162–203.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality if nonrandomised studies in meta-analyses. NOS; 2012
Brink M, Schäffer B, Pieren R, Wunderli JM. Conversion between noise exposure indicators Leq24h, LDay, LEvening, LNight, Ldn and Lden: principles and practical guidance. Int J Hyg Environ Health. 2018;221:54–63.
Crippa A, Orsini N. Multivariate dose-response meta-analysis: the dosresmeta R package. J Stat Softw, Code Snippets. 2016;72:1–15.
Viechtbauer W. Conducting meta-analyses in R with the metafor Package. J Stat Softw. 2010;36:1–48.
R Core Team. R: a language and environment for statistical computing. 2021. https://www.R-project.org/.
Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P, et al. GRADE guidelines: 4. Rating the quality of evidence—study limitations (risk of bias). J Clin Epidemiol. 2011;64:407–15.
Tibshirani R. Regression Shrinkage and Selection Via the Lasso. J R Stat Soc Series B Methodol. 1996;58:267–88.
Foundation PS Python 3.10.4 documentation. 2024. https://docs.python.org/3.10/2024.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Stevens GA, Alkema L, Black RE, Boerma JT, Collins GS, Ezzati M, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. Lancet. 2016;388:e19–e23.
Babisch W, Beule B, Schust M, Kersten N, Ising H. Traffic noise and risk of myocardial infarction. Epidemiology. 2005;16:33–40.
Bodin T, Björk J, Mattisson K, Bottai M, Rittner R, Gustavsson P, et al. Road traffic noise, air pollution and myocardial infarction: a prospective cohort study. Int Arch Occup Environ Health. 2016;89:793–802.
Carey IM, Anderson HR, Atkinson RW, Beevers S, Cook DG, Dajnak D, et al. Traffic pollution and the incidence of cardiorespiratory outcomes in an adult cohort in London. Occup Environ Med. 2016;73:849–56.
Cole-Hunter T, Dehlendorff C, Amini H, Mehta A, Lim YH, Jørgensen JT, et al. Long-term exposure to road traffic noise and stroke incidence: a Danish Nurse Cohort study. Environ Health. 2021;20:115.
Dimakopoulou K, Koutentakis K, Papageorgiou I, Kasdagli MI, Haralabidis AS, Sourtzi P, et al. Is aircraft noise exposure associated with cardiovascular disease and hypertension? Results from a cohort study in Athens, Greece. Occup Environ Med. 2017;74:830–7.
Hao G, Zuo L, Weng X, Fei Q, Zhang Z, Chen L, et al. Associations of road traffic noise with cardiovascular diseases and mortality: Longitudinal results from UK Biobank and meta-analysis. Environ Res. 2022;212:113129.
Lim YH, Jørgensen JT, So R, Cramer J, Amini H, Mehta A, et al. Long-term exposure to road traffic noise and incident myocardial infarction: a Danish nurse cohort study. Environ Epidemiol. 2021;5:e148.
Magnoni P, Murtas R, Russo AG. Residential exposure to traffic-borne pollution as a risk factor for acute cardiocerebrovascular events: a population-based retrospective cohort study in a highly urbanized area. Int J Epidemiol. 2021;50:1160–71.
Poulsen AH, Sørensen M, Hvidtfeldt UA, Christensen JH, Brandt J, Frohn LM, et al. Concomitant exposure to air pollution, green space, and noise and risk of stroke: a cohort study from Denmark. Lancet Reg Health Eur. 2023;31:100655.
Roswall N, Raaschou-Nielsen O, Ketzel M, Gammelmark A, Overvad K, Olsen A, et al. Long-term residential road traffic noise and NO2 exposure in relation to risk of incident myocardial infarction - A Danish cohort study. Environ Res. 2017;156:80–6.
Seidler A, Wagner M, Schubert M, Dröge P, Pons-Kühnemann J, Swart E, et al. Myocardial infarction risk due to aircraft, road, and rail traffic noise. Dtsch Arztebl int. 2016;113:407–14.
Seidler AL, Hegewald J, Schubert M, Weihofen VM, Wagner M, Dröge P, et al. The effect of aircraft, road, and railway traffic noise on stroke - results of a case-control study based on secondary data. Noise Health. 2018;20:152–61.
Selander J, Nilsson ME, Bluhm G, Rosenlund M, Lindqvist M, Nise G, et al. Long-term exposure to road traffic noise and myocardial infarction. Epidemiology. 2009;20:272–9.
Sørensen M, Andersen ZJ, Nordsborg RB, Jensen SS, Lillelund KG, Beelen R, et al. Road traffic noise and incident myocardial infarction: a prospective cohort study. PLoS ONE. 2012;7:e39283.
Sørensen M, Lühdorf P, Ketzel M, Andersen ZJ, Tjønneland A, Overvad K, et al. Combined effects of road traffic noise and ambient air pollution in relation to risk for stroke? Environ Res. 2014;133:49–55.
Sørensen M, Poulsen AH, Hvidtfeldt UA, Münzel T, Thacher JD, Ketzel M, et al. Transportation noise and risk of stroke: a nationwide prospective cohort study covering Denmark. Int J Epidemiol. 2021;50:1147–56.
Thacher JD, Poulsen AH, Raaschou-Nielsen O, Hvidtfeldt UA, Brandt J, Christensen JH, et al. Exposure to transportation noise and risk for cardiovascular disease in a nationwide cohort study from Denmark. Environ Res. 2022;211:113106.
Willich SN, Wegscheider K, Stallmann M, Keil T. Noise burden and the risk of myocardial infarction. Eur Heart J. 2006;27:276–82.
Babisch W, Ising H, Gallacher JE, Sweetnam PM, Elwood PC. Traffic noise and cardiovascular risk: the Caerphilly and Speedwell studies, third phase–10-year follow up. Arch Environ Health. 1999;54:210–6.
Babisch W, Ising H, Kruppa B, Wiens D. The incidence of myocardial infarction and its relation to road traffic noise—the Berlin case-control studies. Environ Int. 1994;20:469–74.
Grady ST, Hart JE, Laden F, Roscoe C, Nguyen DD, Nelson EJ, et al. Associations between long-term aircraft noise exposure, cardiovascular disease, and mortality in US cohorts of female nurses. Environ Epidemiol 2023;7:e259.
Bai L, Shin S, Oiamo TH, Burnett RT, Weichenthal S, Jerrett M, et al. Exposure to road traffic noise and incidence of acute myocardial infarction and congestive heart failure: a population-based cohort study in Toronto, Canada. Environ Health Perspect. 2020;128:87001.
Yankoty LI, Gamache P, Plante C, Goudreau S, Blais C, Perron S, et al. Long-term residential exposure to environmental/transportation noise and the incidence of myocardial infarction. Int J Hyg Environ Health. 2021;232:113666.
Pershagen G, Pyko A, Aasvang GM, Ögren M, Tiittanen P, Lanki T, et al. Road traffic noise and incident ischemic heart disease, myocardial infarction, and stroke: a systematic review and meta-analysis. Environ Epidemiol. 2025;9:e400.
Khosravipour M, Khanlari P. The association between road traffic noise and myocardial infarction: a systematic review and meta-analysis. Sci Total Environ. 2020;731:139226.
Eminson K, Cai YS, Chen Y, Blackmore C, Rodgers G, Jones N, et al. Does air pollution confound associations between environmental noise and cardiovascular outcomes? - a systematic review. Environ Res. 2023;232:116075.
Strak M, Weinmayr G, Rodopoulou S, Chen J, de Hoogh K, Andersen Z, et al. Long term exposure to low level air pollution and mortality in eight European cohorts within the ELAPSE project: pooled analysis. BMJ. 2021;374:n1904.
Stafoggia M, Oftedal B, Chen J, Rodopoulou S, Renzi M, Atkinson RW, et al. Long-term exposure to low ambient air pollution concentrations and mortality among 28 million people: results from seven large European cohorts within the ELAPSE project. Lancet Planet Health. 2022;6:e9–e18.
Sørensen M, Wendelboe Nielsen O, Sajadieh A, Ketzel M, Tjønneland A, Overvad K, et al. Long-term exposure to road traffic noise and nitrogen dioxide and risk of heart failure: a cohort study. Environ Health Perspect. 2017;125:097021.
Osborne MT, Abohashem S, Naddaf N, Abbasi T, Zureigat H, Mezue K, et al. The combined effect of air and transportation noise pollution on atherosclerotic inflammation and risk of cardiovascular disease events. J Nucl Cardiol. 2023;30:665–79.
Fu X, Wang L, Yuan L, Hu H, Li T, Zhang J, et al. Long-term exposure to traffic noise and risk of incident cardiovascular diseases: a systematic review and dose-response meta-analysis. J Urban Health. 2023;100:788–801.
Münzel T, Daiber A, Engelmann N, Roosli M, Kuntic M, Banks JL. Noise causes cardiovascular disease: it’s time to act. J Expo Sci Environ Epidemiol. 2025;35:24–33.
Münzel T, Molitor M, Kuntic M, Hahad O, Röösli M, Engelmann N, et al. Transportation noise pollution and cardiovascular health. Circ Res. 2024;134:1113–35.
Pyko A, Roswall N, Ögren M, Oudin A, Rosengren A, Eriksson C, et al. Long-term exposure to transportation noise and ischemic heart disease: a pooled analysis of nine Scandinavian cohorts. Environ Health Perspect. 2023;131:17003.
GBD 2021 Stroke Risk Factor Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 2024;23:973–1003.
Vivanco-Hidalgo RM, Avellaneda-Gómez C, Dadvand P, Cirach M, Ois Á, Gómez González A, et al. Association of residential air pollution, noise, and greenspace with initial ischemic stroke severity. Environ Res. 2019;179:108725.
O’Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. 2010;376:112–23.
GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. 2024;403:2133–61.
Sørensen M, Pershagen G, Thacher JD, Lanki T, Wicki B, Röösli M, et al. Health position paper and redox perspectives - Disease burden by transportation noise. Redox Biol. 2024;69:102995.
Moudon AV. Real noise from the urban environment: how ambient community noise affects health and what can be done about it. Am J Prev Med. 2009;37:167–71.
Stansfeld SA, Matheson MP. Noise pollution: non-auditory effects on health. Br Med Bull. 2003;68:243–57.
Nijland HA, Van Wee GP. Traffic noise in Europe: a comparison of calculation methods, noise indices and noise standards for road and railroad traffic in Europe. Transport Reviews. 2005;25:591–612.
European Commission. Zero Pollution Action Plan. 2021. https://environment.ec.europa.eu/strategy/zero-pollution-action-plan_en?utm_source=chatgpt.com.
European Environmental Agency. Environmental noise in Europe 2025, No 05/2025. 2025. https://www.eea.europa.eu/en/analysis/publications/environmental-noise-in-europe-2025?activeTab=13e424cd-5934-4614-92ef-e6be8d05c441.
Clark SN, Anenberg SC, Brauer M. Global Burden of Disease from Environmental Factors. Annu Rev Public Health. 2025;46:233–51.
Acknowledgements
The authors would like to thank Maarten Engel from the Erasmus MC Medical Library for developing the search strategy. We would also like to thank Ricardo Assunção, Jurgen Buekers, Alberto Castro, Mariana Oliveira Corda, Vanessa Gorasso, Hamid Y. Hassen, Carla Martins, Axel Luyten, and Arno Pauwels for their insightful discussions on exposure-response functions and their contributions to various aspects of this study.
Funding
This study is part of the BEST-COST project, funded by the European Union’s Horizon Europe program under Grant Agreement No.101095408. The funder of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the paper. The authors had full access to all the data in the study and had final responsibility to submit for publication. Views and opinions expressed are those of the author(s) only and do not necessarily reflect those of the European Union or of HaDEA. Neither the European Union nor the granting authority can be held responsible for them.
Author information
Authors and Affiliations
Contributions
Elia Gonzato, Periklis Charalampous, and Juanita A. Haagsma developed the study design. Periklis Charalampous and Juanita A. Haagsma conducted the data screening, while Elia Gonzato and Periklis Charalampous performed the data extraction and reviewed it with Juanita A. Haagsma, Gunn Marit Aasvang, and Vanessa Garcia. Elia Gonzato, Tessa M.I. Haverkate, Michael Brauer, and Sandra Spearman carried out all statistical analyses, with Tessa MI Haverkate and Susanne Breitner-Busch assisting with the conventional meta-analyses. Elia Gonzato and Periklis Charalampous drafted the manuscript. Elia Gonzato, Tessa M.I. Haverkate, Susanne Breitner-Busch, Anette Kocbach Bølling, Gunn Marit Aasvang, Michael Brauer, Vanessa Garcia, Sandra Spearman, Brecht Devleesschauwer, Juanita A. Haagsma, and Periklis Charalampous critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gonzato, E., Haverkate, T.M.I., Breitner-Busch, S. et al. Exposure-response relationship between transportation noise and cardiovascular disease outcomes: a systematic review and meta-regression analysis. J Expo Sci Environ Epidemiol (2026). https://doi.org/10.1038/s41370-026-00856-9
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41370-026-00856-9
