
Abstract
Background/Objectives
Vitamin D (VD) status has been linked to the development of diabetes. However, this relationship in the context of comorbid conditions remains understudied. Additionally, ethnic disparities in nutritional status and chronic disease prevalence within rural populations are a vastly underrepresented area of research. In our previous study, we explored VD levels and depression in a rural West Texas aging sample. In the present study, we investigated the associations between diabetes, vitamin D (VD) levels, depression, and Hispanic ethnicity (HE) among a sample of aging, rural West Texans from Project FRONTIER (PF; Facing Rural Obstacles to Health Care Now Through Intervention, Education, and Research).
Subjects/Methods
A cohort of 299 PF participants (mean age 62.6 ± 11.8 years old, 70.9% female, 40.5% HE) was used. We examined relationships between diabetes diagnosis, blood-based diabetes-related biomarkers, VD level, Geriatric Depression Scale (GDS) score, and HE status. We developed a “VD-sensitive GDS score” composed of the 9 GDS questions that were significantly correlated with VD level in our previous study. We further created a complementary “VD-insensitive GDS score” composed of the remaining 21 GDS questions. Standard correlation and regression analyses were employed.
Results
VD level was significantly negatively associated with diabetes diagnosis, while VD-sensitive depression score was significantly positively associated with diabetes diagnosis. HE was associated with higher HbA1c levels, higher fasting blood glucose levels, and higher VD-sensitive depression scores.
Conclusions
In this rural West Texas cohort, diabetes was significantly associated with low VD levels and high VD-sensitive depression scores. HE was associated with higher levels of diabetes-related biomarkers and higher VD-sensitive depression scores. These disparities are crucial to consider when examining areas for healthcare improvement in West Texas, particularly among aging populations.
Similar content being viewed by others

Introduction
Diabetes mellitus (DM) is a metabolic disorder characterized by chronic hyperglycemia. The majority of cases (90–95%) involve a dysregulated response to insulin and are classified as type 2 DM [1]. Higher rates of diabetes have been reported in Hispanic populations due to factors including lower socioeconomic status, a cultural diet high in carbohydrates and saturated fat, and genetic susceptibility to insulin resistance [2, 3]. Diabetes has been linked to a variety of comorbid conditions, including depression, which is of particular concern in the aging population [4]. When considering factors contributing to the development of diabetes, many identify nutritional deficiencies as a potential link; studies have found significant associations between low vitamin D (VD) levels and diabetes [5, 6]. VD level has also been linked with comorbid conditions that frequently occur alongside diabetes; a substantial connection between low VD levels and depression has been established [7].
Just as diabetes is a worldwide health issue, vitamin D deficiency (VDD) and vitamin D insufficiency (VDI) impact diverse populations around the globe [8]. According to the Endocrine Society, VDD is defined as a 25(OH)D level of 20 ng/mL or lower, and VDI as a 25(OH)D of 21–29 ng/mL [9]. There is a particularly high prevalence of VDD/VDI amongst Hispanic populations due to factors including darker skin pigmentation, higher rates of obesity, and poorer overall health status [10]. Moreover, there is an age-dependent reduction in the body’s ability to synthesize and absorb VD [11]. Thus, it is essential to consider how nutritional status impacts the development of chronic conditions in older individuals within rural communities with large Hispanic populations, such as West Texas.
In a previous study, we examined VD level and depression in a rural West Texas aging sample from the TTUHSC-managed epidemiological study termed Project FRONTIER (PF; Facing Rural Obstacles to Health Care Now Through Intervention, Education, and Research) [12, 13]. Significant negative associations were identified between VD levels and Geriatric Depression Scale (GDS) scores, and Hispanic participants had significantly lower VD levels [12]. Other studies using PF data have explored the relationships between ethnic disparities and depression in older adults [14]. However, there remains a critical knowledge gap about the possibility that VD levels could serve as a proxy marker of diabetes and comorbid conditions in older adults. Previous research has linked VDD/VDI to increased risk of development of DM [15], yet few studies have focused on identifying these disparities in an older West Texas population with a large Hispanic demographic. Therefore, more research is necessary to elucidate relationships between these disease processes. To better identify opportunities for intervention, education, and research, this study explored the relationships between diabetes, VD level, depression, and Hispanic ethnicity (HE) in an aging West Texas cohort. A subset of the data in this study was presented in preliminary form at the 2024 Alzheimer’s Association International Conference in Philadelphia, PA, USA [16].
Materials and methods
Study population and sample
We used a cross-sectional subsample from PF, an ongoing longitudinal study in rural West Texas, which was approved by the Texas Tech University Health Sciences Center (IRB Number L06-028). Informed consent was obtained from all subjects in this study. Similar to a previous study [12], the PF cohort consisted of 299 individuals, and this cohort size was chosen to include all participants with available VD level measurements. The sample calculation was performed by identifying the number of samples in which the variable bw_vitd contained a positive number. Data were obtained from participants living in Parmer County, the only county where VD measurements were available, and represent the baseline from Visit 1 (2009–2011). Samples were deidentified (by co-author Annette Boles) to preserve patient anonymity and exported from Qualtrics into Excel format.
Variables and measurements
Variables were collected using a standardized medical examination, fasting blood work at a local CLIA-certified hospital, detailed interview/medical history, and neuropsychological testing. Visits were not aligned to a specific season or time of year. Other than the absence of a VD measurement, there were no exclusion criteria in this observational study. PF variables were requested from the TTUHSC Garrison Institute on Aging. 298 samples had all variables, including vitamin D measurements (bw_vitd). However, one sample did not have HbA1c, GDS score, VD-sensitive GDS score, and VD-insensitive GDS scores; however, it was included when possible.
Diabetes-related variables requested include HbA1c (bw_hgba1), fasting blood glucose (bw_gluc), and consensus diagnosis of diabetes (cdx_mdca). A fasting bloodwork test from Parmer County Hospital was used to measure fasting blood glucose and HbA1c level. While the consensus diagnosis of diabetes did not specify whether participants had type 1 or type 2 DM, based on national rates and participant demographic characteristics it is assumed a large majority in the cohort classify as type 2 DM. Consistent with this idea, only a single participant (1/299) was explicitly mentioned as having type 1 DM. HbA1c levels were parsed into No Diabetes Range (<5.7% or <39 mmol/mol), Pre-Diabetes Range (5.7–6.4% or 39–46 mmol/mol), and Diabetes Range (≥6.5% or ≥48 mmol/mol), while fasting blood glucose levels were parsed into No Diabetes Range ( < 100 mg/dL), Pre-Diabetes Range (100–125 mg/dL), and Diabetes Range (≥126 mg/dL) [17].
Serum 25-hydroxyvitamin D measurements were requested. Following Endocrine Society guidelines [9], VD level was subcategorized into VD deficiency (VDD) ( ≤ 20 ng/mL), VD insufficiency (VDI) (21–29 ng/mL), and VD sufficiency (VDS) (30–38 ng/mL). A “high sufficient” (VDHS) (>38 ng/mL) category was established due to evidence of additional benefits of VD beyond those associated with sufficiency [18].
In our previous study [12], the GDS total (gds_sumt) (ranging from 0 to 30 points) was used to assess depressive symptoms. From the GDS, we derived a “VD-sensitive GDS score” (gds_VDS-RM) composed of 9 GDS questions that were significantly correlated with VD levels [12]. Here, we further created a complementary “VD-insensitive GDS score” (gds_VDI-RM) composed of the remaining 21 GDS questions that were not significantly correlated with VD in our previous study. Depressive symptoms were corroborated with consensus diagnosis of depression (cdx_psya).
Hispanic ethnicity was determined based on self-reported ethnicity, which included the following categories: Mexican, Mexican American, or Chicano, Puerto Rican, and Other Hispanic Origin. A binary variable (ds_16_3-JL, HE = 1, non-HE = 0) was created to group together HE participants (n = 121) to compare to non-HE participants (n = 178).
The 299 PF sample was further categorized into four groups based on comorbidity status informed by consensus diagnosis: neither diabetes nor depression (n = 184), only diabetes (n = 53), only depression (n = 47), and both diabetes and depression (n = 15).
Statistical analyses
Statistical comparisons and graphics were generated with GraphPad Prism 10. A normality test (Shapiro-Wilk test) was performed with all collected variables. Shapiro-Wilk test for normality indicated VD levels (W = 0.8976), HbA1c levels (W = 0.6102), fasting blood glucose levels (W = 0.6287), consensus diabetes diagnosis (W = 0.5180), GDS total (W = 0.8495), VD-sensitive GDS (W = 0.7457), VD-insensitive GDS (W = 0.8737), and HE status (W = 0.6231) were all (p < 0.0001) not normally distributed; therefore, we used nonparametric analyses for statistical comparisons.
Spearman’s correlation, simple logistic regression, and multiple logistic regression analyses were used. The nonparametric Kruskal-Wallis test with post hoc Dunn’s multiple comparisons test were used to compare fasting blood glucose, HbA1c, VD levels, and GDS scores between the no diabetes range, pre-diabetes range, and diabetes range participants. To investigate differences between these three groups, we categorized participants based on their fasting blood glucose level corresponding with no diabetes range, pre-diabetes range, and diabetes range, and we then used each participant’s associated VD level and GDS score to conduct the comparisons. The Mann-Whitney U test was employed for nonparametric comparisons between HE and non-HE groups. All Mann-Whitney tests were two-tailed. A Chi-square test was conducted to compare HE status and comorbidity status via nonparametric analysis of a contingency table. A Chi-square test was also used to compare HE status and diabetes range status via nonparametric analysis of a contingency table. When comparing HE status and VD subcategory for participants with diabetes, due to the small sample size in which the expected values were not all greater than 1, Chi-square assumptions were not met; therefore, Fisher’s exact test was conducted for a nonparametric analysis of this contingency table.
Cohen’s d was calculated to display effect sizes for the Mann-Whitney comparisons. The effect sizes are classified as follows: small (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8) [19].
Results
Baseline demographic characteristics
The demographic and baseline characteristics of our PF sample are presented in Table 1. VD values ranged from 7.2 to 91.0 ng/mL, and the majority of participants (61.5%) were classified as VDD or VDI. The overall mean VD level was 28.5 ± 12.4 ng/mL, the mean HbA1c level was 6.0 ± 1.1% (42.2 ± 12.4 mmol/mol), and the mean fasting blood glucose level was 109.4 ± 33.6 mg/dL (mean ± SD). Subcategory averages (mean ± SD) are represented in Table 1. A detailed representation of the distribution of HbA1c levels and fasting blood glucose levels is shown in Fig. 1A and Fig. 1B, respectively. To further compare across DM categories, we used the Kruskal-Wallis test to demonstrate significant differences in the HbA1c levels between the no diabetes, pre-diabetes, and diabetes range participants (p < 0.0001; Fig. 1C); post hoc analysis using Dunn’s multiple comparisons test showed significant differences between all 3 comparisons: no diabetes vs. pre-diabetes (p < 0.0001), pre-diabetes vs. diabetes (p < 0.0001), and no diabetes vs. diabetes (p < 0.0001). When analyzing fasting blood glucose levels using the same method, both the Kruskal-Wallis test (p < 0.0001) and Dunn’s multiple comparisons test (p < 0.0001 for all 3 comparisons) showed similar significance across all categories (Fig. 1D).

A HbA1c levels among 299 PF participants. Histogram of frequency vs. HbA1c levels, parsed into No Diabetes Range (green, <5.7% or <39 mmol/mol), Pre-Diabetes Range (yellow, 5.7–6.4% or 39–46 mmol/mol), and Diabetes Range (red, ≥6.5% or ≥48 mmol/mol;bin width: 0.1%). B Fasting blood glucose levels among 299 PF participants. Histogram of frequency vs. fasting blood glucose levels, parsed into No Diabetes Range (green, <100 mg/dL), Pre-Diabetes Range (yellow, 100–125 mg/dL), and Diabetes Range (red, ≥126 mg/dL;bin width: 4 mg/dL). C HbA1c levels were significantly different between the No Diabetes Mellitus (DM), pre-DM, and DM range participants (p < 0.0001). Post hoc analysis showed significant differences (p < 0.0001) for all 3 comparisons: No DM vs. pre-DM, pre-DM vs. DM, and No DM vs. DM. D Fasting blood glucose levels were significantly different between the No DM, pre-DM, and DM range participants (p < 0.0001). Post hoc analysis showed significant differences (p < 0.0001) for all 3 comparisons: No DM vs. pre-DM, pre-DM vs. DM and No DM vs. DM. ****p < 0.0001.
Relationships between VD Levels, diabetes, and GDS
VD level was significantly negatively correlated with HbA1c level (rs = −0.24; p < 0.0001) and fasting blood glucose level (rs = −0.27; p < 0.0001; Fig. 2A). Further analysis also showed a significant negative association between VD level and diabetes diagnosis (Likelihood ratio test, G2 = 7.58; p = 0.0059; OR = 0.9652; Fig. 2B).

A Spearman correlation matrix of measured variables. VD levels were significantly negatively correlated with HbA1c (p < 0.0001) and fasting blood glucose levels (p < 0.0001). VD-sensitive GDS (VD-S GDS) total was significantly positively correlated with fasting blood glucose levels (p = 0.013). VD-I GDS = VD-insensitive GDS. B. Simple logistic regression of the relationship between VD level and diabetes diagnosis (Likelihood ratio test, G2 = 7.58; p = 0.0059). C Simple logistic regression of the relationship between VD-S GDS and diabetes diagnosis (Likelihood ratio test, G2 = 6.514; p = 0.0107). D Simple logistic regression of the relationship between VD-I GDS and diabetes diagnosis (Likelihood ratio test, G2 = 1.205; p = 0.2724). Dotted lines indicate 95% confidence intervals. E There were significant differences in the VD levels of participants with fasting blood glucose values in the No Diabetes Mellitius (No DM) range versus those in the pre-DM range (p = 0.0147), as well as between those in the No DM range versus the DM range (p = 0.0002). F There was a significant difference in the VD-S GDS scores between those in the No DM range versus the DM range (p = 0.0403). ***p < 0.001; *p < 0.05.
We found that VD-sensitive GDS total was significantly positively correlated with fasting blood glucose level (rs = 0.144; p = 0.013; Fig. 2A). However, both GDS total and VD-insensitive GDS total were not significantly correlated (p > 0.05) with either of the blood-based diabetes biomarkers. Further assessment of the relationship between VD-sensitive GDS total and diabetes diagnosis showed a significant positive association (Likelihood ratio test, G2 = 6.514; p = 0.0107; OR = 1.185; Fig. 2C). To further distinguish VD-sensitive GDS total from VD-insensitive GDS total, we found there was no significant association between VD-insensitive GDS total and diabetes diagnosis (Likelihood ratio test, G2 = 1.205; p = 0.2724; OR = 1.042; Fig. 2D).
Comparing across categories (see Fig. 1C, D), we also found significant differences in the VD levels of participants with fasting blood glucose values in the no diabetes range compared to those in the pre-diabetes range (p = 0.0147; Fig. 2E), as well as significant differences in VD levels between those in the no diabetes range versus the diabetes range (p = 0.0002; Fig. 2E). However, there was no significant difference between the pre-diabetes range and diabetes range VD levels.
Finally, we also found significant differences in the VD-sensitive GDS scores between those in the no diabetes range versus the diabetes range (p = 0.0403; Fig. 2F); no significant differences were found between the pre-diabetes range and diabetes range, as well as between the pre-diabetes range and no diabetes range groups. We did not find significant differences (p > 0.05) among the three diabetes status groups when comparing VD-insensitive GDS scores and GDS total scores (data not shown).
Multiple logistic regression for diabetes diagnosis
In multivariate analyses, diabetes diagnosis was found to be trending towards significance with VD level (OR = 0.9727, p = 0.0504) and VD-sensitive GDS total (OR = 1.142, p = 0.0509; Table 2).
Relationships between Hispanic ethnicity, diabetes, and VD-sensitive GDS Total
HE participants had significantly higher HbA1c levels (6.3 ± 1.4% or 45 ± 15 mmol/mol) compared to non-HE counterparts (5.8 ± 0.9% or 40 ± 9.7 mmol/mol; p = 0.0006; Cohen’s d = 0.381; Fig. 3A) as well as significantly higher fasting blood glucose levels (114.5 ± 35.3 mg/dL) compared to non-HE participants (105.9 ± 32.1 mg/dL; p = 0.0034; Cohen’s d = 0.255; Fig. 3B).

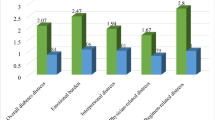
A HbA1c levels were significantly higher in Hispanic ethnicity (HE) compared to non-HE participants (p = 0.0006). B Fasting blood glucose levels were significantly higher in HE than non-HE participants (p = 0.0034). C. Differences in the distribution of HE and non-HE groups across diabetes range status (Chi-square test, X2(2, 299) = 9.501; p = 0.0086). D Differences in the distribution of HE and non-HE groups across VD strata amongst participants with a consensus diabetes diagnosis (Fisher’s exact test, p = 0.0031). Error bars indicate upper and lower limits. Legend: Vitamin D deficient (VDD, red), vitamin D insufficient (VDI, yellow), vitamin D sufficient (VDS, green), vitamin D high sufficient (VDHS, cyan). E Differences in the distribution of HE and non-HE groups across comorbidity status. There was a significant association found between HE status and comorbidity status (Chi-square test, X2(3, 299) = 23.94; p < 0.0001). F VD-sensitive GDS scores were significantly higher in HE compared to non-HE participants (p < 0.0001). Asterisks denoted by ****p < 0.0001; ***p < 0.001; **p < 0.01.
Multiple logistic regression for Hispanic ethnicity
In multivariate analysis, HE was significantly associated with VD (OR = 0.9208, p < 0.0001), VD-sensitive GDS total (OR = 1.421, p < 0.0001), HbA1c (OR = 1.940, p = 0.0079), and fasting blood glucose (OR = 0.9842, p = 0.0349; Table 3).
Relationships between Hispanic ethnicity, comorbidity status, and VD subcategory
We found a significant association between HE status and diabetes range status (Chi-square test, X2(2, 299) = 9.501; p = 0.0086; Fig. 3C). Amongst participants who had a diabetes diagnosis but not a depression diagnosis, the distribution of HE and non-HE groups across VD strata indicated significance (Fisher’s exact test, p = 0.0031; Fig. 3D). In terms of comorbid disparities, there was a significant association found between HE status and comorbidity status (Chi-square test, X2(3, 299) = 23.94; p < 0.0001; Fig. 3E). Finally, HE participants also had higher VD-sensitive GDS totals (2.2 ± 2.4) compared to non-HE participants (0.8 ± 1.4; p < 0.0001; Cohen’s d = 0.735; Fig. 3F).
Discussion
This study provides new evidence of an association between diabetes, depression, and VD level in an aging West Texas sample. Analysis revealed significant negative correlations between VD level and both diabetes biomarkers (Fig. 2A), while logistic regression supported a negative association between VD level and diabetes diagnosis (Fig. 2B). Previous research has shown that low VD levels are associated with DM [5, 6], therefore, our findings are consistent with current research that indicates a robust relationship between VD levels and diabetes prevalence.
To build on our previous study [12] a VD-sensitive depression score was used to explore its relationship with diabetes. We found a significant positive correlation between VD-sensitive depression score and fasting blood glucose (Fig. 2A), a significant positive association between VD-sensitive depression score and diabetes diagnosis (Fig. 2C). Of note, VD-insensitive GDS total was not significantly associated with diabetes diagnosis (Fig. 2D), and therefore, nutritional status may introduce a nuanced link in the relationship between diabetes and depressive symptoms.
We further found that participants with fasting blood glucose levels in the pre-diabetes range had significantly different VD levels compared to those in the no diabetes range (Fig. 2E); this warrants further research into the association between nutritional status and the risk of developing a pre-diabetes clinical profile. Investigating this factor may provide key insight into the pathology of the pre-diabetes clinical profile and may inform preventative measures to prevent the progression from pre-diabetes to diabetes. Across these same three categories, we discovered a significant difference in VD-sensitive depression scores between the no diabetes and diabetes range participants (Fig. 2F). However, the difference was less pronounced between the no diabetes and pre-diabetes categories, suggesting a stronger relationship between VD levels and diabetes measures than VD-sensitive GDS. Based on the sensitivity of VD to diabetes and depression, these results imply that the depressive symptoms that are significantly associated with VD level may be connected through diabetes, warranting investigation into the mechanistic role of VD linking metabolic and mental disease processes. To further corroborate the statistical analysis within the context of diabetes, we conducted a multiple logistic regression analysis, which demonstrated that diabetes diagnosis was trending towards significance in association with VD level and VD-sensitive depression score (Table 2).
The present study also provides significant information regarding health disparities amongst older Hispanics in West Texas. Regarding ethnic disparities, group comparisons showed HE participants had significantly higher HbA1c (Fig. 3A) and fasting blood glucose levels (Fig. 3B). There was a significant association between HE status and diabetes range status (Fig. 3C). In our previous study [12], VD levels were significantly lower in HE individuals, highlighting a disparity in nutritional status. Lower VD levels and higher diabetes biomarker levels in Hispanic populations are corroborated through other studies that have identified a negative association between VD status and diabetes in Hispanic cohorts [15, 20]. Our previous study [12] found that depression scores were significantly positively associated with HE status, so in this study we specifically looked at VD-sensitive depression scores and their relationship to HE. To supplement the statistical analysis in the context of HE, we conducted a multiple logistic regression, which demonstrated that HE was significantly associated with VD level, VD-sensitive depression score, HbA1c level, and fasting blood glucose level (Table 3).
We are particularly interested in the role of VD in diabetes prevention. Since we found a significant association between VD level and diabetes (Fig. 2B), we sought to explore differences in VD level amongst HE and non-HE participants with diabetes. A significant association was found between VD category and HE status; of note, over half of HE individuals were in the VD deficient category (Fig. 3D). This further supports evidence that Hispanics are at a greater risk of VDD and suggests this disparity has a robust prevalence within the West Texas diabetes population. We also found a significant association between HE status and comorbidity status (Fig. 3E). Of note, over half of HE individuals had either diabetes, depression, or both. HE individuals had significantly higher VD-sensitive depression scores (Fig. 3F), indicating greater depressive symptoms and underscoring that HE status may exacerbate VD-sensitive disease pathology. Other studies confirm significantly high levels of diabetes and depression amongst HE individuals [2, 3, 21], and this highlights a critical disparity amongst this high-risk underserved population. It is well-known that diabetes and depression occur frequently together [4]; however, the link between nutritional status and these comorbidities remains understudied. Due to the observational nature of this study, we cannot claim causation; however, we can identify significant correlations between these variables. Further research is necessary to gain a deeper understanding of the association between various comorbidities and VD status.
Since low VD levels have been linked to diabetes in various studies, this raises the question as to whether VD supplementation could be used in the prevention and/or treatment of diabetes. A meta-analysis of 47 randomized control trials (RCTs) found VD supplementation (median dose 4000 IU/day, median trial duration 4 months) significantly reduced fasting blood glucose levels in individuals without diabetes, however there was no significant effect on the incidence of type 2 DM; the VD level of the supplementation group was 16.5 ng/mL at baseline and 32.9 ng/mL after treatment [22]. Another study found that in patients with both pre-diabetes (identified by a fasting plasma glucose levels between 100–125 mg/dL) and hypovitaminosis D (determined by a serum 25(OH)D levels less than 30 ng/mL), high-dose vitamin D (50,000 IU/week for 3 months followed by 50,000 IU/month for 3 months) supplementation reduced the risk of progression towards diabetes and improved insulin sensitivity [23]. In the supplementation group, VD level was 13 ng/mL at baseline, 41 ng/mL at 3 months, and 36 ng/mL at 6 months. These studies suggest that VD supplementation in individuals classified as VD deficient may reduce risk factors associated with the progression to diabetes.
Studies conducted in patients with diabetes show variable effects based on the VD status of participants. A meta-analysis of 20 RCTs with type 2 DM patients showed that VD supplementation (average dose: short-term subgroup = 3000 IU/day; long-term subgroup = 1833 IU/day; median study duration 3 months) significantly reduced insulin resistance and decreased fasting blood glucose in the VD deficient subgroup [24]. The increase in VD levels of the VD deficient subgroup was significant following supplementation (weighted mean difference 12.7 ng/mL). This study suggests that VD supplementation in patients with diabetes who are in the VD deficient category could gain the most benefit.
The appropriate supplemental dose of VD is a point of debate; while the Endocrine Society recommends 1500–2000 IU/day for adults to maintain VD levels above > 30 ng/mL [9], differences in dosing exist across supplementation studies, and this variability results in conflicting conclusions. A meta-analyses of 35 RCTs reported that VD supplementation (median dose 3332 IU/day, median duration 16 weeks) showed no decreased risk of progression to diabetes; the overall baseline VD level across all groups was 17.8 ng/mL, while after treatment the supplementation group VD level increased by approximately 18.7 ng/mL [25]. This relatively low median dose, compared to other studies of VD supplementation, points to a potential explanation for the ineffective intervention. Notably, the high-dose VD study (50,000 IU/week for 3 months followed by 50,000 IU/month for 3 months) yielded significant results in reducing the progression to diabetes. Thus, dose variability may contribute to the conflicting results presented in the current literature.
In addition, there is much variability in the demographic characteristics of participants who receive VD supplementation, with some studies not selecting for VDD/VDI participants. In studies exploring the risk of progression to diabetes, one study showed no decreased risk of diabetes associated with VD supplementation (4000 IU/day) [26]. The baseline VD level of the supplementation group was 27.7 ng/mL, and after 24 months of treatment the average VD level in this group was 54.3 ng/mL. The baseline VD level was not in the deficient category, which could provide a potential reason why this dose may not have had a significant effect in this cohort. Another note is that 9.3% of this study’s participants identified as HE background, and a more diverse distribution of ethnicities may have produced different results [26]. In studies of people diagnosed with type 2 diabetes, one study found that after 6 months of VD supplementation (40 000 IU/week), there was no significant difference in fasting blood glucose and HbA1c levels [27]. Of note, the baseline VD level amongst the supplementation group was 24 ng/mL, which falls into the VDI category, and the average VD level change from baseline in this group was 23.4 ng/mL. This raises the question as to whether VD supplementation shows the most benefit in patients with diabetes who are classified as VDD as earlier postulated, and therefore supplementation in these studies failed to produce significant effects in non-VDD participants. Further research is needed to explore how dose and VD status interact to produce significant changes.
Just as VD supplementation is being studied in the prevention and treatment of diabetes, it has also been implicated in clinical studies of depression. Various reviews of clinical trials found VD supplementation showed positive results in those with a depression diagnosis (range from 200 IU/day to 10 000 IU/day) [28, 29]. However, other clinical studies show no benefit of VD supplementation on depression (range from 1200 IU/day to 2000 IU/day) [30, 31], and therefore a definitive benefit cannot be currently confirmed [12].
People who identify as Hispanic are largely underrepresented in clinical trials, which is why intentional inclusion of Hispanic cohorts must be prioritized in future clinical studies. As mentioned, Hispanics have been identified as having an increased risk of VDD/VDI [10], and genetic differences in VD binding protein have been implicated in this increased risk [32]. Therefore, understanding the potential differences in VD metabolism/signaling across ethnicities would further inform studies investigating the efficacy of VD supplementation across ethnic subgroups. Since there is no conclusive evidence determining the exact benefits of VD supplementation in terms of preventative care for individuals at high-risk for developing diabetes or as part of treatment for current patients with diabetes, more experimental studies are necessary to determine the clinical significance of VD supplementation.
Rural West Texas has a high proportion of older HE individuals, making it crucial to address the prevalence of diabetes, VDD/VDI, and depression in this high-risk group. Research indicates that culturally tailored approaches to diabetes education in Hispanic populations are effective; however, limited resources in underserved rural areas hinder the implementation of such community-based programs [2, 33]. HE populations are at a high risk for VDD/VDI [12, 34]. As discussed, achieving VD sufficiency may help prevent diabetes and depression among high-risk individuals, but current research shows mixed results regarding effect sizes and optimal dosing. Since VDI/VDD is also linked to increased risks of hypertension, dyslipidemia, and cardiovascular events [35], addressing VDD/VDI through VD supplementation in West Texas could provide broad benefits in reducing health disparities in the region.
Future research regarding VD supplementation in the aging population must also consider the potential benefits on cognitive functions. We are currently investigating the relationship between VD status and neuropsychological functioning in the cohort analyzed in this study, specifically the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). Using a similar cohort, Singer and colleagues [36] found that HE individuals show significantly lower RBANS total scores compared to non-HE participants, a finding that is supported by previous research [14, 37] and further highlights an area of disparity that warrants attention. We have previously investigated various dimensions of RBANS in depth, as it is composed of twelve subtests that assess five cognitive domains: attention, language, visuospatial/constructional abilities, immediate memory, and delayed memory, finding relationships to mental health, marital status, pain, age, and education [36, 38,39,40,41]. In future studies, we intend to explore nutritional supplementation as a preventative intervention for dementia and cognitive decline in the elderly in West Texas.
Limitations of our study should be considered. First, no PF variables were available that measured time spent outside, exposure to sunlight, skin pigmentation, or VDR gene polymorphisms. On this note, since visits were not aligned to a specific season or time of year, this could have influenced the measured VD levels due to seasonal sunlight exposure. Second, since HE is a self-reported measure that could be impacted by social/cultural factors not explicitly included, and misclassification bias cannot be completely ruled out. Third, since this is a cross-sectional correlative study, causal (and reverse causal) relationships cannot be determined or inferred. Finally, these findings may or may not be generalizable to the West Texas population due to using a convenience sampling technique when obtaining participant samples.
Conclusion
Our study provides significant data regarding the relationship between diabetes, vitamin D, depression, and Hispanic ethnicity in a West Texas cohort. Significant results revealed diabetes diagnosis to be associated with lower VD levels, and diabetes diagnosis was further associated with increased VD-sensitive depression score. HbA1c levels, fasting blood glucose levels, and VD-sensitive depression levels were significantly higher amongst HE vs. non-HE participants in this study, identifying major health disparities in this region of Texas. The importance of highlighting health disparities is rooted in the fact that healthcare gaps in underserved populations must first be identified to appropriately target education, outreach, and eventual interventions throughout West Texas.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. Portions of this data were presented in poster form at the Alzheimer’s Association International Conference in Philadelphia, Pennsylvania on July 29th, 2024.
References
Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2004;27:s5-s10.
Idrogo M, Mazze R. Diabetes in the Hispanic population. Postgrad Med. 2004;116:26–36.
Aguayo-Mazzucato C, Diaque P, Hernandez S, Rosas S, Kostic A, Caballero AE. Understanding the growing epidemic of type 2 diabetes in the Hispanic population living in the United States. Diab/Metab Res Rev. 2019;35:e3097.
Randväli M, Toomsoo T, Šteinmiller J. The main risk factors in type 2 diabetes for cognitive dysfunction, depression, and psychosocial problems: a systematic review. Diabetology. 2024;5:40–59.
Afzal S, Bojesen SE, Nordestgaard BG. Low 25-hydroxyvitamin D and risk of type 2 diabetes: a prospective cohort study and metaanalysis. Clin Chem. 2013;59:381–91.
Mitri J, Muraru MD, Pittas AG. Vitamin D and type 2 diabetes: a systematic review. Eur J Clin Nutr. 2011;65:1005–15.
Renteria K, Nguyen H, Koh GY. The role of vitamin D in depression and anxiety disorders: a review of the literature. Nutr Neurosci. 2024;27:262–70.
Wimalawansa SJ. Vitamin D deficiency: effects on oxidative stress, epigenetics, gene regulation, and aging. Biology. 2019;8:30.
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin d deficiency: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–30.
Castro JP, Penckofer S. The role of vitamin D in the health of Hispanic adults with diabetes. Hisp Health Care Int. 2014;12:90–8.
Maclaughlin J, Holick MF. Aging decreases the capacity of human skin to produce vitamin D3. J Clin Investig. 1985;76:1536–8.
Pourghaed M, Sarangi A, Ramirez-Velandia F, Kopel J, Culberson J, Ashworth G, et al. Associations between vitamin D deficiency/insufficiency and depression expose health disparities in older rural West Texans: a project FRONTIER study. Am J Geriatr Psychiatry. 2024;32:808–20.
Rebello CJ. Vitamin D and depression: racial differences suggest an alternate biomarker. Am J Geriatr Psychiatry. 2024;32:821–4.
O’Bryant SE, Hall JR, Cukrowicz KC, Edwards M, Johnson LA, Lefforge D, et al. The differential impact of depressive symptom clusters on cognition in a rural multi-ethnic cohort: a Project FRONTIER study. Int J Geriatr Psychiatry. 2011;26:199–205.
Scragg R, Sowers M, Bell C. Serum 25-hydroxyvitamin D, diabetes, and ethnicity in the Third National Health and Nutrition Examination Survey. Diab Care. 2004;27:2813–8.
McCready R, Morris C, Antwi-Adjei P, Pourghaed M, Ramirez-Velandia F, Kopel J. et al. Relationships between diabetes, vitamin D status, neuropsychological functioning, and Hispanic ethnicity in older rural West Texans: a project FRONTIER study. Alzheimeras Dement. 2025;20:e091599
Association AD. Understanding Diabetes Diagnosis 2024. Available from: https://diabetes.org/about-diabetes/diagnosis.
Greenblatt HK, Adler C, Aslam M, Welge J, Krikorian R. Vitamin D level predicts all-cause dementia. Nutr Healthy Aging. 2019;5:141–7.
Sullivan GM, Feinn R. Using effect size—or Why the P value is not enough. J Grad Med Educ. 2012;4:279–82.
Ramos-Trautmann G, González L, Díaz-Luquis G, Pérez CM, Palacios C. Inverse association between vitamin D status and diabetes in a clinic based sample of Hispanic adults in Puerto Rico. Diab Res - Open J. 2015;1:5–11.
Johnson LA, Gamboa A, Vintimilla R, Edwards M, Hall J, Weiser B, et al. A depressive endophenotype for predicting cognitive decline among Mexican American adults and elders. J Alzheimer’s Dis. 2016;54:201–6.
Tang H, Li D, Li Y, Zhang X, Song Y, Li X. Effects of vitamin D supplementation on glucose and insulin homeostasis and incident diabetes among nondiabetic adults: a meta-analysis of randomized controlled trials. Int J Endocrinol. 2018;2018:1–9.
Niroomand M, Fotouhi A, Irannejad N, Hosseinpanah F. Does high-dose vitamin D supplementation impact insulin resistance and risk of development of diabetes in patients with pre-diabetes? A double-blind randomized clinical trial. Diab Res Clin Pract. 2019;148:1–9.
Li X, Liu Y, Zheng Y, Wang P, Zhang Y. The effect of vitamin D supplementation on glycemic control in type 2 diabetes patients: a systematic review and meta-analysis. Nutrients. 2018;10:375.
Seida JC, Mitri J, Colmers IN, Majumdar SR, Davidson MB, Edwards AL, et al. Effect of vitamin D3 supplementation on improving glucose homeostasis and preventing diabetes: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2014;99:3551–60.
Pittas AG, Dawson-Hughes B, Sheehan P, Ware JH, Knowler WC, Aroda VR, et al. Vitamin D supplementation and prevention of type 2 diabetes. N Engl J Med. 2019;381:520–30.
Jorde R, Figenschau Y. Supplementation with cholecalciferol does not improve glycaemic control in diabetic subjects with normal serum 25-hydroxyvitamin D levels. Eur J Nutr. 2009;48:349–54.
Musazadeh V, Keramati M, Ghalichi F, Kavyani Z, Ghoreishi Z, Alras KA, et al. Vitamin D protects against depression: Evidence from an umbrella meta-analysis on interventional and observational meta-analyses. Pharmacol Res. 2023;187:106605.
Xie F, Huang T, Lou D, Fu R, Ni C, Hong J. et al. Effect of vitamin D supplementation on the incidence and prognosis of depression: an updated meta-analysis based on randomized controlled trials. Front Public Health. 2022;10:903547.
Okereke OI, Reynolds CF, Mischoulon D, Chang G, Vyas CM, Cook NR, et al. Effect of long-term vitamin D3 supplementation vs Placebo on risk of depression or clinically relevant depressive symptoms and on change in mood scores. JAMA. 2020;324:471.
De Koning EJ, Lips P, Penninx BWJ, Elders PJ, Heijboer AC, Den Heijer M, et al. Vitamin D supplementation for the prevention of depression and poor physical function in older persons: the D-Vitaal study, a randomized clinical trial. Am J Clin Nutr. 2019;110:1119–30.
Hong J, Hatchell KE, Bradfield JP, Bjonnes A, Chesi A, Lai C-Q, et al. Transethnic evaluation identifies low-frequency loci associated with 25-hydroxyvitamin D concentrations. J Clin Endocrinol Metab. 2018;103:1380–92.
Vidal TM, Williams CA, Ramoutar UD, Haffizulla F. Type 2 Diabetes mellitus in Latinx populations in the United States: a culturally relevant literature review. Cureus. 2022;14:e23173.
Ames BN, Grant WB, Willett WC. Does the high prevalence of vitamin D deficiency in African Americans contribute to health disparities?. Nutrients. 2021;13:499.
Bizzaro G, Antico A, Fortunato A, Bizzaro N. Vitamin D and autoimmune diseases: Is vitamin D receptor (VDR) polymorphism the culprit?. Isr Med Assoc J. 2017;19:438–43.
Singer J, Rerick P, Elliott L, Fadalla C, McLean E, Jump A. et al. Investigating the relationship between marital status and ethnicity on neurocognitive functioning in a rural older population: a project FRONTIER study. J Gerontol Ser B. 2024;79:gbad126.
O’Bryant SE, Johnson L, Balldin V, Edwards M, Barber R, Williams B, et al. Characterization of Mexican Americans with mild cognitive impairment and Alzheimer’s disease. J Alzheimer’s Dis. 2012;33:373–9.
Fadalla C, Singer J, Rerick P, Elliott L, McLean E, Schneider S, et al. Neurocognitive disparities: investigating ethnicity and mental health in rural aging adults. Aging. 2025;17:33–50.
Elliott L, Singer J, Rerick P, Kelly J, Chung Yin Chan A, Molinar-Lopez V, et al. Neurocognitive functioning in Hispanic and non-Hispanic individuals in Rural West Texas: understanding the influence of age and education. Appl Neuropsychol Adult. 2025;1–13.
Chrzanowski L, Singer J, Rerick P, Elliott L, Levitt DE, Cummings C. et al. The role of inflammation, chronic pain, and hypertension on neurocognitive functioning in an underserved, rural population: a project FRONTIER study. J Clin Exp Neuropsychol. 2025;47:249–62.
Johnson LA, Gamboa A, Vintimilla R, Cheatwood AJ, Grant A, Trivedi A, et al. Comorbid depression and diabetes as a risk for mild cognitive impairment and Alzheimer’s disease in elderly Mexican Americans. J Alzheimer’s Dis. 2015;47:129–36.
Acknowledgements
The authors thank Project FRONTIER participants for their invaluable contribution to this research. The authors thank Veronica Molinar-Lopez and Project FRONTIER staff for assistance in retrieving data from Qualtrics, Dr. Duke Appiah (TTUHSC) for helpful discussions throughout the study, and Dr. Rama Chemitiganti (TTUHSC) for comments on a previous version of the manuscript. This research did not receive any specific grant funding. The study was supported by the TTUHSC School of Medicine Medical Student Summer Research Program (RM and MP). Meeting attendance and travel has previously been supported by TTUHSC School of Medicine (RM and CM) and internal funds from the TTUHSC Garrison Institute on Aging and TTUHSC Department of Pharmacology and Neuroscience (JL). Partial salary support was from grants NIH R01AG071859 (JL), R01AG073826 (JL), R15AG080446 (JS), R35CA197730 (JS), P20GM109025 (MNS), R01AG053798 (MNS), R01AG053798 (MNS), R01AG059008 (MNS and BD), U24AG057437 (MNS), ADDF GC-2013717 (MNS and BD), P20AG068053 (MNS), R01AG073212 (MNS and BD), and GR-ARPA-BNF-010123 (MNS).
Author information
Authors and Affiliations
Contributions
RM, MP, FRV, JL, PA, GA, AS, AB, CM, JK, JC, JS, MNS, VN, BD, and ACS made substantial contributions to the conception and design of the work. RM, MP, PA, and JL played important roles in interpreting the results. RM, MP, PA, and CM drafted the work. RM, FRV, JL, GA, AS, AB, JK, JC, JS, MNS, VN, BD, and ACS critically revised the work for its intellectual content and data interpretation.
Corresponding author
Ethics declarations
Competing interests
MNS is a consultant for Roche-Genentech, Eisai, Lilly, Synaptogenix, NeuroTherapia, Signant Health, Novo Nordisk, Prothena, Anavex, Cognito Therapeutics, GSK, and AbbVie. BD is a consultant for Lighthouse Pharmaceuticals.
Ethics approval and consent to participate
All methods were performed in accordance with the relevant guidelines and regulations. Project FRONTIER was approved by the Texas Tech University Health Sciences Center (IRB Number L06-028). Informed consent was obtained from all participants in this study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
McCready, R., Morris, C., Antwi-Adjei, P. et al. Relationships between diabetes, vitamin D status, depression, and Hispanic ethnicity: a project FRONTIER study. Nutr. Diabetes 16, 1 (2026). https://doi.org/10.1038/s41387-025-00409-3
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41387-025-00409-3
