
Abstract
Background
The COVID-19 pandemic significantly impacted child mental health, but data on long-term outcomes are limited. This study explored the course of psychiatric symptoms in patients with pre-existing psychopathology, assessed from both the child’s and parents’ perspectives.
Methods
A three-year multicentre-longitudinal study involving patients aged 5–18 years and their parents across 10 Italian sites. Data were collected at three time points (2020, 2021 and 2022). Statistical analyses included Exploratory Factor Analysis (EFA), Confirmatory Factor Analysis (CFA) and Linear Mixed Models (LMM) via REML.
Results
A total of 523 families participated. Factor analysis validated 3 factors for parents and 4 for children. Parents reported a low emotional well-being, positively correlated with socioeconomic status (SES); children reported better emotional well-being correlated with higher SES in 2020–2021 but not in 2022. During the pandemic, children perceived the quality of care as unsatisfactory; however, the association between SES and the perceived quality of care was less pronounced.
Conclusion
SES may have differentially influenced the long-term mental health outcomes in children and parents. Social disadvantage may be especially evident during acutely stressful periods. During the pandemic, the advantages of a higher SES in mental health care were less pronounced than expected.
Impact
-
The multi-informant perspective is extremely important to understand the impact of pandemic on the well-being of the entire family.
-
Both youths with pre-existing psychopathology and their parents show consistently low emotional well-being throughout the pandemic, indicating a persistent vulnerability that does not spontaneously normalize.
-
Youths report low satisfaction with, and perceived quality of, mental health support during the pandemic.
-
Socioeconomic status shows a dynamic and informant-specific pattern. The advantage of higher SES is less evident for care satisfaction,
-
In at risk populations family-based interventions should also address caregivers’ emotional involvement and burden.
Category of study
Clinical Research Article
Similar content being viewed by others


Introduction
The Coronavirus Disease 19 (COVID-19) was a global epidemic triggered by the SARS-CoV-2 coronavirus leading the World Health Organization (WHO) to declare it a pandemic on March 11, 2020.1 Children and adolescents experienced prolonged confinement measures, home-schooling, and social restrictions with drastic and sustained changes in their daily lives.2
Since its onset, the impact of the COVID-19 pandemic on child and adolescent mental health has gained widespread research attention suggesting that the younger generations, even if less likely to be infected, may have been more negatively impacted than adults by the long-term mental health consequences of the pandemic.3,4,5,6,7,8 The pandemic has exacerbated existing vulnerabilities in young people’s mental health,9 particularly those with neurodevelopmental difficulties or from underprivileged backgrounds.10,11 The impact on mental health was particularly pronounced in children with pre-existing conditions, such as Attention Deficit Hyperactivity Disorder (ADHD),12 autism spectrum disorders,13 intellectual disabilities,14 and eating disorders.15 Cost et al. (2022) compared both children and adolescents with and without psychiatric diagnoses during the first wave of COVID-19, showing a decline in mental health and a more pronounced deterioration in those with pre-existing diagnoses.16 Similarly, Zijlmans et al. revealed that children and adolescents with pre-existing mental or somatic health conditions faced greater challenges compared to their peers, with the impact varying according to specific psychopathological conditions.17
While many studies have assessed youth mental health during the COVID-19 pandemic, few studies have reported on the long-term trajectory of mental symptoms in patients with pre-existing mental disorders. In a 6-month longitudinal study (from April to September 2020), Raffagnato et al. (2021) examined the effects of the pandemic on the psycho-behavioral profiles of young psychiatric patients and their parents, finding that the patients had generally adapted well to the pandemic context.18 The study by Lewis et al. (2022) examined changes in trauma symptoms in adolescents with pre-existing conditions such as ADHD, anxiety, or depression across four timepoints from spring 2020 to spring 2021. These individuals presented increased vulnerability, with 25% of participants exhibiting trauma symptoms during the spring 2020 lockdown, and although symptoms decreased thereafter, 20% of adolescents maintained moderate or clinical levels of trauma symptoms through spring 2021.19
Chadi et al. (2022) reviewed data on internalizing and externalizing disorders in children and adolescents with pre-existing mental disorders,20 reporting an increase in internalizing symptoms, such as depression and anxiety, early in the pandemic, followed by a partial recovery by summer 2020.21,22 In contrast, a U.S.-based longitudinal study indicated an increase in externalizing symptoms in children between April 2020 and January 2021.23
On May 5, 2023, the WHO COVID-19 Emergency Committee declared the end of the global emergency phase of the disease.1
Given the unprecedented nature and duration of the pandemic, understanding its possible long-term effects on mental health is crucial, particularly for youth with pre-existing conditions who are more vulnerable to environmental stressors. The primary aim of our study was therefore to evaluate the clinical trajectory of internalizing and externalizing symptoms in a large cohort of Italian patients with pre-existing psychopathology across three time points: early, during the acute pandemic period and during the later pandemic stage. In the study, both the parents’ and children’s perspectives were examined and integrated. A secondary objective was to examine the association between sociodemographic status and the longitudinal trajectory of emotional well-being in both children and their parents, as these data may inform targeted interventions and resource allocation, and address health disparities within vulnerable populations.
Methods
The RISM-COVID-19-PSICO study was a three-year multicenter, longitudinal (2020–2022), observational, naturalistic study examining the impact of the COVID-19 pandemic on the mental health of children (aged 5–18 years) with pre-existing psychopathology and their families. The study followed the principles of the Declaration of Helsinki. The protocol was approved by the institutional Ethics Committee of the Department of Biomedical Sciences at the University of Cagliari (Protocol No. 18 dated: 24/06/2020. Resolution No. 1012 dated: 15/07/2020). This manuscript is reported in accordance with the STROBE guidelines (see Strobe Table in Supplementary Materials).
Participants included children diagnosed with psychiatric disorders according to the DSM-5 criteria, and their parents, in care at 10 Italian child and adolescent neuropsychiatry services. Informed consent was obtained from parents, and assent from children 10 years of age or older. Centers were identified within an already active collaborative research network to ensure nationwide geographic and socio-demographic variability, standardized assessments, trained staff, sufficient clinical volume, and adherence to the study timeline.
A non-probabilistic, convenience sampling method was used. All eligible children and their parents were contacted by telephone and/or were invited to participate, during their outpatient clinic visit, with actual enrollment depending on patient and caregiver availability (e.g., time or family and work-related commitments) and access to remote, internet-enabled devices, as commonly applied in clinical recruitment during the COVID-19 pandemic. This strategy was considered as the more suitable one given the longitudinal design across three time points and the clinical characteristics of the target population (i.e., children with psychopathology and their caregivers), thereby enhancing feasibility and retention over time.24,25,26,27
The psychopathological conditions included ADHD, oppositional defiant disorder/conduct disorder (ODD/CD), movement disorders (including developmental coordination disorder and Tourette syndrome), specific learning disorders, anxiety disorders, mood disorders (major or persistent depression, bipolar disorders and cyclothymia), eating disorders, obsessive-compulsive disorders (OCD), post-traumatic stress disorders, schizophrenia spectrum disorders and other psychotic disorders. Not included were patients with single-gene syndromes, meanwhile patients with a primary diagnosis of autism spectrum disorder (ASD) levels 2 and 3 and/or intellectual disability were enrolled in a separate, specifically dedicated, prospective international study.13 All participants were categorized into three distinct macro-groups (formalized as the variable “diagnostic category”) based on their pre-existing primary diagnoses: a) “Internalizing disorders”, including depressive and bipolar disorders, anxiety disorders, OCD and related disorders, and eating disorders; b) “Externalizing disorders”, including ADHD, ODD, CD, and schizophrenia spectrum disorders; c) “Other”, including learning disabilities and Tourette syndrome.
For patients with multiple comorbid diagnoses, clinicians identified a primary diagnosis corresponding to the most prevalent and functionally impairing condition, and a secondary diagnosis capturing additional comorbid disorders, based on a clinical judgment process.
The classification of complex cases reflected the dominant psychopathological dimension rather than a simple count of co-occurring diagnoses and could be identified as an internalizing, externalizing pattern or other.
Data collection
Pre-COVID clinical and sociodemographic data were collected using a clinical research form. This information included age, sex, residential area28 (e.g., rural/suburban/urban), socioeconomic status (SES) according to Hollingshead Four-Factor Index of SES,29 primary and comorbid psychiatric diagnosis according to DSM-5 criteria,30 symptoms severity rated by the Clinical Global Impression31 and the Children’s Global Assessment Scale.32 SES was computed based on parental education and occupation. Educational attainment was coded separately for each parent using a seven-level scale reflecting the highest level completed, ranging from less than seventh grade to postgraduate or professional training. Occupation was likewise coded on a nine-level scale, ranging from unskilled or menial occupations to higher executive and major professional roles. For each parent, an SES score was derived by weighting education and occupation differently, and then summing these components. The participant’s SES was calculated as the average of the two parental scores; when data were available for only one parent, that value was used directly. The resulting SES scores ranged from 8 to 66, and were subsequently grouped into five ordered categories for analytical purposes, commonly used in psychological research33: low (8–19), middle-low (20–29), middle (30–39), middle-high (40–54), and high (55–66).
Children/adolescents and their parents completed, respectively, the Young Person Covid Questionnaire (YP-CQ) and the Parent Covid Questionnaire (P-CQ), at three time-points: T0 (July–December 2020, early pandemic stage), T1 (February–March 2021, acute pandemic stage), and T2 (February–March 2022, later pandemic period). The questionnaires were self-administered by participants, without the presence or involvement of clinical personnel during completion. Parents and children completed their respective surveys independently, with no access to each other’s responses, to ensure the integrity of the individual reports. For each family, a single parent was designated to complete the parent survey, and the same parent consistently completed the questionnaire at the follow-up assessments. To avoid within-family clustering, each family contributed data for only one child. In cases where more than one sibling was in care, only the first child was included in the study.
The two questionnaires were derived from the electronic questionnaires of the project “The Coronavirus Health Impact Survey (CRISIS)”, developed through a collaboration with the National Institute of Mental Health, and the Child Mind Institute and the NYS Nathan S. Kline Institute for Psychiatric Research.34
The Italian version was created through translation and back-translation. The electronic questionnaires and their responses were stored, via the REDCap platform (https://www.project-redcap.org/), on the Cagliari University servers.
The YP-CQ consists of 30 questions aimed at evaluating the following domains: health status/COVID-19 exposure, emotions/concerns and behaviors, impact of emotions and behavior, experience of mental health care, education, and everyday life (see Appendix B).
The P-CQ consists of 66 questions aimed at assessing the following dimensions: health status/COVID-19 exposure, child’s emotions/concerns, changes in the child’s relationships, experience of mental health care for the child, childhood and education services, work-family balance, home environment, parent’s emotions/concerns, changes in the parent’s relationship, financial problems (see Appendix A).
Responses to the items in both questionnaires were evaluated on a 5-point Likert scale, ranging from 1 (improvement) to 5 (worsening).
Statistical and data analyses
The statistical analyses were carried out with the software Jamovi35 (release 2.3.28; The jamovi project. jamovi, 2024). Descriptive statistics were computed for all study variables, and their distributions were examined to assess normality and identify potential outliers.
Both the child and parent samples were randomly split into two subgroups. Explorative factorial analysis (EFA) was conducted on subsample 1 and confirmative factorial analysis (CFA) on subsample 2, the Bartlett test36 and the Kaiser-Meyer-Olkin test37,38 were employed to assess the suitability of the data. The parallel analysis and the scree plot criteria were used preliminarily to identify the number of factors to retain in the questionnaire. The Weighted Least Squares Method of factoring and the oblique promax rotation were applied.
The CFA was used for the second random subsample (respectively for parents and children), using as a method Diagonally Weighted Least Squares (DWLS) estimation.39 We assessed the goodness of fit for two models: considering a single factor solution (model 1), then applying the correlated factor solutions, identified in the previous EFA (model 2).
Test-retest validity was appraised with Pearson’s r coefficients of correlation, between the factors scores calculated at the 3 time points (at T0, T1 and T2).
The relationship between sociodemographic characteristics (age and SES) and questionnaire factors was calculated using the non/parametric Spearman’s Rho correlation.
For both parent- and child-report data, we first evaluated whether attrition at T2 was associated with any systematic baseline differences between completers (“stayers”) and non-completers (“leavers”). To this end, a descriptive attrition analysis compared key baseline characteristics—namely age, SES, area of residence, baseline factor scores, and the completion of the parent baseline questionnaire—for stayers vs leavers.
To investigate potential sources of missingness and assess the plausibility of the Missing At Random (MAR) assumption, we conducted a binary logistic regression predicting dropout at T2 from baseline covariates. Dropout was modestly associated with certain observed variables (e.g., age and area of residence), but not with the factor variables, supporting the use of model-based approaches under MAR.
We explored the nature of missingness in two further ways: assessing whether missingness was related to observed data (supporting MAR assumptions); conducting Little’s MCAR test (results reported in the Appendices Children and Parents).
Finally, we applied linear mixed-effects models (LMMs) to analyze changes in outcome scores across time and factors, accounting for intra-individual variability and center-level clustering. Accordingly, we fitted Linear Mixed-Effects Models (LMMs) estimated via Restricted Maximum Likelihood (REML), which are appropriate for handling incomplete longitudinal data under MAR when covariates related to missingness are included. No listwise deletion or multiple imputation was applied, and all available data were included in the models to preserve statistical power and minimize bias.
Although SES could be treated as a continuous variable, using a categorical specification avoids imposing linearity assumptions and facilitates the examination of interaction effects (e.g., SES × factor, SES × time).
Results
A total of 523 families (n = 983 participants) were enrolled (Table 1, Fig. 1). Rates of questionnaire completion and loss to follow-up, for both children and parents, are presented in the flow diagram (Fig. 2). From baseline to T2, the dropout rate was 59.1% (309/523). The patients (340 males and 183 females) had a mean age of 12.8 years (SD = 2.9). At baseline, 34.4% (n = 172) were attending primary school, 31.2% (n = 156) in lower secondary school, and 34.4% (n = 172) upper secondary school.

Circle size is proportional to the number of enrolled families at each site.

The flow diagram shows the number of subjects who completed the questionnaires at the three selected time points.
Most (53.5%, n = 272) lived in urban areas, 38.0% (n = 193) in suburban, and 8.3% (n = 42) in rural areas. SES was available for 462 families. Socio-demographic characteristics are shown in Table 2.
Based on the 3 diagnostic categories, 30.1% of the patients (n = 152) had an internalizing disorder, 58.8% (n = 297) an externalizing disorder, and 11.1% (n = 56) other disorders (Table 3). Furthermore, 48.6% (n = 254) had only one psychiatric diagnosis, while the remaining 51.4% (n = 269) had at least another comorbid disorder.
At baseline, 9.2% (n = 48) were receiving pharmacotherapy, 25.4% (n = 133) non-pharmacological treatment, 41.3% (n = 216) both pharmacological and non-pharmacological interventions, and 108 (20.6%) no specific intervention. Data about treatment were unavailable for 18 children (3.4%).
Exploratory factor analysis and confirmatory factor analysis
Parents sample
In the parents’ subsample, the explorative factor analysis (EFA) with oblique rotation (promax) was conducted on 20 items of the questionnaire. The graphical criterion based on the scree-plot and the results of the parallel analysis40 suggested a factorial structure defined by 3 factors (see Fig. S1 and Table S1 for eigenvalues and Table S2 for factor loadings after rotation in online Supplementary Materials). The items included in the factor analysis for parents’ report are underlined in Appendix A.
Three factors had eigenvalues over Kaiser’s criterion of 1 and, in combination, explained 36.1% of the total variance. The items that loaded strongly on the same factors suggest the following interpretations: Factor 1 (Child Emotionality) captures parents’ perceptions of their child’s emotional and psychological states; Factor 2 (Parent Emotionality) reflects parents’ own emotional responses and psychological adjustments; and Factor 3 (Child Concerns) represents the parents’ observations of their child’s specific worries and fears (see Table S2, in online Supplementary Materials).
A further CFA confirmed the three-factor structure, consistent with the results of the EFA (see Table S4 and S5 in online Supplementary Materials).
Children/adolescents sample
In the children/adolescents’ first subsample, an explorative factor analysis (EFA) with oblique rotation was conducted on the 17 items. The EFA identified four factors with eigenvalues greater than 1, explaining 41.2% of the total variance (see Fig. S2 for scree-plot, Table S6 for eigenvalues and Table S7 for factor loadings in online Supplementary Materials). The items included in the factor analysis for the child report are indicated by underlining in Appendix B.
Four factors were retained in the final analysis and were interpreted as follows: Factor 1 (Child/Adolescent Emotionality) reflects the emotional well-being and psychological states of children/adolescents, including happiness, anxiety, sleep quality, and agitation; Factor 2 (Mental Health Support) captures the perception of changes in the quality and quantity of mental health services and satisfaction with such support; Factor 3 (Child/Adolescent Behavior) represents behavioral difficulties, such as irritability, aggression (both exhibited and experienced), and challenges in self-regulation; and Factor 4 (Child/Adolescent Concerns) encompasses specific worries, particularly those related to health and contagion risks.
In the subsequent Confirmatory Factor Analysis (CFA) (carried out in the second subsample) the four-factor model identified from the previous EFA was confirmed, demonstrating alignment with the results of the explorative approach (see Tables S8 and S9 in online Supplementary Materials).
Correlation with sociodemographic characteristics
The factors at all time points were also correlated with age and SES. Correlation analyses were performed for both parent and adolescent groups using the non-parametric Spearman’s Rho coefficient. Within the parent questionnaire, no significant correlation between the child’s age and any factor was found. A higher SES was associated with better emotional well-being in children/adolescents, measured by the “Child Emotionality” factor, in both 2020 (T0: Rho = −0.197, p = 0.001) and 2021 (T1: Rho = 0.141, p = 0.034), with a progressively decreasing correlation coefficient, indicating a weakening of the relationship between the two variables. This correlation disappeared entirely in 2022. In contrast, the “Parent Emotionality” factor correlated with SES at all time points showing a stronger correlation in 2022 compared to previous years (T0: Rho = −0.100, p = 0.037; T1: Rho = −0.134, p = 0.045; T2: Rho = −0.230, p = 0.001). A higher SES was also significantly associated with lower parent-reported Child Concerns, but only in 2021 (T1: Rho = −0.156, p = 0.019).
In the patients’ questionnaire, older adolescents reported a more positive perception of mental health services (T0: Rho = 0.142, p = 0.002); this relationship was present only in 2020 but not in 2021 or 2022.
Similarly to the findings in parents, a significant correlation was observed between SES and the “Child Emotionality” factor in both 2020 (T0: Rho = −0.101, p = 0.032) and 2021 (T1: Rho = −0.155, p = 0.033), while no correlation was found in 2022: higher SES was associated with greater emotional and psychological well-being as self-reported by adolescents. A significant association between SES and behavioral difficulties and self-regulation challenges emerged only in 2021, with participants from higher socioeconomic backgrounds exhibiting fewer behavioral problems and better self-regulatory capacities (T1: Rho = −0.155, p = 0.033).
Linear mixed-model analysis on parent survey
To examine the effects of psychological and contextual variables on the outcome across the three time points, we employed Linear Mixed-Effects Models (LMMs) using restricted maximum likelihood estimation (REML). Given the hierarchical structure of the data—with repeated measures nested within individuals—a random intercept was specified for participant ID to account for within-subject dependencies.41
Model evaluation and selection: in the initial phase, we evaluated a model that included a random intercept for the geographic area of residence, in addition to the participant-level intercept. However, this more complex model did not improve model fit over the simpler model with participants as the sole random effect (χ²(1) = 0.00, p = 1.00), and the variance component for area was estimated as zero. Therefore, the area random effect was excluded from the final model in favor of parsimony and to avoid overparameterization. This decision was also supported by model comparison metrics (ΔAIC = +2.0), indicating no benefit in retaining the additional random term.
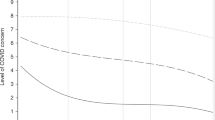
Final model specification: the fixed effects in the final model included: time (2020, 2021, 2022), questionnaire psychological factor (Child Emotionality, Parent Emotionality, Child Concerns), SES (treated as ordinal), diagnostic category (treated as categorical), parental participation at baseline, area of residence, age (standardized), the interaction between questionnaire psychological factor and SES. The random intercept was specified for each participant. The final model demonstrated satisfactory convergence, and no issues related to multicollinearity or singularity were identified. Residual diagnostics suggested acceptable model fit. The statistical modeling workflow is reported in Appendix Parents. No significant effects were found for time, diagnostic category, parental participation at T0, and area of residence, suggesting that these variables did not meaningfully contribute to variation in the outcome in this model. However, although SES plays a significant role overall, its influence is attenuated in the context of Child Concerns (Table 4; Fig. 3).

Lines show model-predicted scores for each factor across socioeconomic status (SES) levels (1 = low to 5 = high). Factors were defined as F1 = Child Emotionality, F2 = Parent Emotionality, and F3 = Child Concerns. Scores were slightly higher (indicating greater impairment) at lower SES levels and slightly lower at higher SES levels, although differences were small. Child Emotionality and Parent Emotionality did not differ substantially from each other, whereas Child Concerns showed markedly lower scores than the other factors.
Although area of residence was initially considered as a hierarchical level, its contribution was found to be negligible and excluded to retain a parsimonious model.
Linear mixed-model analysis on child/adolescent survey
In parallel with the procedure applied in the parent sample, to evaluate the criterion validity of the factor scores within the child-report sample, we conducted linear mixed-effects models (LMMs) to examine changes over time, differences among factor types, and the role of covariates including SES, clinical characteristics, and parental participation. The model accounted for repeated measures within individuals and recruitment center clustering.
Model selection and specification
Model comparison procedures were conducted using likelihood-ratio tests (LRT) under Maximum Likelihood (ML) estimation to determine the optimal random-effects structure and the necessity of including interaction terms.
Final model specification
The final model included random intercepts and random slopes for time at the individual level, random intercepts for center (Cat_site); the fixed effects included factors (Child Emotionality, Mental Health Support, Child Behavior, Child Concerns), time, SES, age (scaled), parental participation at baseline, diagnostic category, and area of residence; an interaction term between factor and SES level, based on theoretical and empirical grounds.
Model comparisons confirmed the appropriateness of including random slopes for time (ΔAIC = –6.5, p = 0.0049), while the inclusion of the factor × SES interaction improved model fit, albeit marginally (ΔAIC = –4.4, p = 0.075), thus retained for interpretive purposes (See Appendix Children).
No significant changes were detected over time at the group level, and neither age, diagnostic category, nor area of residence were significant predictors in this model. The Mental Health Support factor was associated with significantly higher scores, while Child Behavior and Child Concerns related to Covid-19 infection were consistently lower than the Child Emotionality factor. SES showed a strong main effect, with children from intermediate SES levels (2–4) scoring significantly lower indicating a better psychological condition (Table 5). Significant interaction effects emerged for the Mental Health Support factor with SES levels 2, 3, and 4, indicating that the expected SES gradient was less pronounced for this factor (Table 6).
A similar pattern was observed for the Child Concerns × SES interaction: children in lower SES still scored significantly lower (better perceived mental health support) though this was moderated slightly by the interaction term. The plot of estimated marginal means (EMMs) shows diverging SES trajectories across factors: Mental Health Support demonstrates relative SES invariance (flat lines across SES levels), Child Behavior and Child Concerns factor show steeper gradients, consistent with SES sensitivity (Fig. 4).

Lines show model-predicted scores for each factor across socioeconomic status (SES) levels (1 = low to 5 = high). Factors were defined as F1 = Child Emotionality, F2 = Mental Health Support, F3 = Child Behavior, and F4 = Child Concerns. Although modest, a factor-by-SES interaction was observed for Child Emotionality and Child Behavior, whereas predicted scores largely overlapped across SES levels for Mental Health Support. Overall, Child Emotionality scores were higher than those for Child Concerns and Child Behavior.
Random-effect individual variability was considerable. In particular, inter-individual variability in time-related change was virtually negligible in 2021, but became more evident in 2022, indicating meaningful between-subject heterogeneity in longitudinal trajectories despite the lack of a significant group-level mean change over time.
The contribution of center-level clustering was low but retained to account for site-specific recruitment variability. The small but non-zero center variance supports model specification that includes center as a random effect.
Discussion
This study represents one of the most extended longitudinal investigations about the psychological impact of the COVID-19 pandemic on children and adolescents with pre-existing psychopathological conditions, incorporating perspectives from both children and their parents up to the later phase of the pandemic.
The psychological and behavioral symptom profiles remained relatively stable across the various phases of the pandemic, without significant fluctuations in response to the various public health measures enacted. These results align with previous reports of emotional and behavioral stability in early stages of the pandemic, suggesting adaptability and resilience.18,42 Conversely, an increase in parental stress was observed in the initial phase of the pandemic (spring 2020),42,43 followed by a decrease in internalizing problems and post-traumatic stress symptoms during the summer months.18
Our findings diverge from other longitudinal studies that reported fluctuating symptom patterns during the pandemic in children and adolescents with neuropsychiatric disorders. An increase in internalizing symptoms during stricter lockdown phases, followed by signs of recovery, has been reported.21,22 Externalizing disorders and behavioral symptoms, such as oppositional behaviors and temper outbursts, were linked to reduced opportunities for socialization and diminished parental and peer support.23 It should be noted, however, that these studies focused on the early stage of the pandemic without assessing long-term course.
In our study, parents reported that their children had relatively low levels of concern about getting infected with COVID-19 although a high impact on emotional state (Emotionality factor), including sadness, vulnerability, or emotional distress. Patients with internalizing symptoms did not differ from subjects with externalizing disorders. In line with parents’ surveys, children and adolescents reported low emotional well-being in spite of low concerns about COVID-19 contagion. Similarly, O’Connor et al. with their CRISIS survey administered between May 2020 and April 2021 found high levels of negative mood and of concern about COVID-19 infection.44
Although our study did not include pre-pandemic data, our findings are consistent with a deterioration in emotional well-being found in other studies. Thomson et al. (2023) reported elevated levels of anxiety in children as perceived by parents compared to pre-pandemic periods.45 Likewise, Panchal et al. (2023) found a significant increase in anxiety and depression, particularly among children with pre-existing psychopathology, based on parental reports.46
Our study demonstrates a clear convergence across informants (parents and children), suggesting a shared perception of emotional difficulties. Interestingly, parents’ self-reported emotional well-being was comparable to the level of emotional well-being they attributed to their children, suggesting that the pandemic’s impact affected the entire family. Existing literature documents in fact an increased family stress during the pandemic, likely driven by the heightened caregiving burden associated with school closures, job loss or employment changes, financial insecurity, and deteriorations in children’s mental health.47 Moreover, as reported in qualitative studies, many families had to compensate for reductions in services support, taking on an even more central role in addressing their children’s mental health needs.48
In the self-report questionnaire, despite a negative emotional state, children reported relatively few behavioral difficulties, such as irritability and aggressive behaviors. Importantly, in accordance with Kourgiantakis et al.,48 children reported low perceived quality of—and low satisfaction with—mental health support services expressing negative evaluations of the quality of care received during the pandemic period. Several studies reported, in fact, a reduction in access to services from the early phases of the pandemic.49,50,51
Finally, our data indicate the dynamic nature of the relationship between SES and mental health in both patients and their parents during the entire course of the pandemic.
Several studies have highlighted the influence of SES on the developmental trajectories and mental well-being of children,52 and these effects may be further exacerbated by prolonged stress.53 However, the existing literature shows mixed evidence. SES was not associated with psychopathology in Argentine youth,54 but the sample was primarily composed of middle- to upper-class families, potentially buffering the impact of economic inequalities.
Our findings align with those reported by Davico et al. (2024) and Conti et al. (2020), confirming the relevance of SES in shaping the psychological well-being of both young patients55,56 and their parents. These results are consistent with O’Connor et al., who showed that greater difficulties were experienced by children and adolescents from more socioeconomically disadvantaged backgrounds.44 Expanding on these short-term reports, our study shows that higher SES was associated with better emotional child well-being, during the first two years of the pandemic (2020–2021), a relationship that weakened in 2022. Conversely, in parents, the link between SES and emotional well-being strengthened over time, underscoring the cumulative impact of economic pressures and increasing family responsibilities on adults.
Notably, our data indicate that the benefits associated with higher SES are attenuated when considering children’s self-rated perceived quality of mental health support, suggesting the pandemic and the resulting reorganization of services may have dampened socioeconomic inequalities. During the pandemic, emergency services were reducing routine service provision and continuity of care.51 In this context, low satisfaction with mental health care services may reflect system-wide limitations in availability and organizational discontinuity, potentially affecting even higher-SES families for whom the opportunity to compensate through private care may also have been constrained.
While using baseline SES is supported by national trends57,58 and the relative stability of core SES components in Italy, the lack of repeated SES measurements over follow-up limits our ability to capture potential individual-family level socioeconomic fluctuations. Socioeconomic conditions can vary over time, especially under economic uncertainty, affecting children’s developmental, behavioral, and educational outcomes. Changes in employment, income, or occupational status can alter family SES.59,60 Consequently, using baseline SES may oversimplify socioeconomic trajectories and their potential influence on child outcomes.
Several factors have, however, influenced children’s emotional well-being during the COVID-19 pandemic, independently of SES. For instance, unhealthy lifestyle habits such as low levels of physical activity and prolonged exposure to digital media, and adverse family environment including parental mental health difficulties.61 Conversely, other factors, such as parenting style and the quality of parental emotional investment have been identified as mediators in the association between SES and children’s emotional symptoms.62
Parents, too, were deeply affected by lockdown measures. The need to simultaneously manage work, household responsibilities, and childcare—often without external support—constituted a major source of stress, potentially compromising their ability to provide the emotional stability needed by their children.63
These findings call for a deeper reflection on how different generations may be shaped by distinct risk factors and underscore the complexity of psychosocial realities, which cannot be adequately explained through simple, linear causal models. Instead, there is a growing need for integrative and systemic frameworks capable of capturing the interplay among socioeconomic, environmental, familial, and individual variables, thereby informing more nuanced theoretical models and guiding future research.
Strengths of the study
This study was the first to examine the long-term course of psychiatric symptoms and well-being of children and adolescents with pre-existing psychopathology during COVID-19 pandemic.
The broad geographic distribution across Italy, involving 10 child and adolescent neuropsychiatry centers, enabled the inclusion of a sizable and geographically diverse sample of the population.
The sample size in this heterogeneous cohort allowed for the diversification across diagnostic categories, providing an opportunity for differentiated analysis of symptom trajectories.
Limitations
The non-probabilistic, convenience-based recruitment strategy might have introduced selection bias. In addition, nonresponse bias cannot be ruled out, as completers differ.44 Therefore, p-values and confidence intervals should be interpreted cautiously—as measures of uncertainty under the model—rather than definitive evidence for population-level inference. These points may limit the external validity of the study and warrant caution when generalizing the results to broader clinical or community populations.
The dropout rate is noteworthy. However, the data analysis supports a Missing At Random (MAR) assumption based on observed associations between dropout and baseline covariates.
There was heterogeneity among clinical sites as to the number of participants. Unmeasured site-level factors (e.g., service organization, local resources, or contextual differences) may have contributed to outcome variability.
Accounting for within-family changes in SES over the study period can represent an important limitation. For these reasons, we underscore the need for future studies to incorporate more dynamic and context-sensitive SES measures (e.g., employment loss, remote schooling burden, access to digital resources) to trace socioeconomic changes over time and better model their implications for developmental outcomes. Finally, due to the absence of a control group, it cannot be concluded that the observed patterns are specific to the patients with pre-existing psychopathology.
Conclusions
Overall, our data support the hypothesis that the pandemic simultaneously affected (i) the emotional well-being of children and adolescents and their parents, (ii) the perceived quality of mental health care, and (iii) the structure of socioeconomic inequalities, attenuating some advantages typically associated with more privileged conditions among younger service users.
This study may inform social interventions and support policies in managing crises and promoting the psychological well-being of minors and adults, and guide future research on individualized intervention strategies in at-risk youth populations.
Data availability
Data are available in the Supplementary Materials or on request to the corresponding author.
References
Fitzpatrick, O., Carson, A. & Weisz, J. R. Using Mixed Methods to Identify the Primary Mental Health Problems and Needs of Children, Adolescents, and Their Caregivers during the Coronavirus (COVID-19) Pandemic. Child Psychiatry Hum Dev. Dec. 52, 1082–1093 (2021).
Koenig, J. et al. The impact of COVID-19 related lockdown measures on self-reported psychopathology and health-related quality of life in German adolescents. Eur Child Adolesc Psychiatry Jan. 32, 113–122 (2023).
Meherali, S. et al. Mental Health of Children and Adolescents Amidst COVID-19 and Past Pandemics: A Rapid Systematic Review. Int J Environ Res Public Health Mar 26 18, 3432 (2021).
Clemens, V. et al. Potential effects of “social” distancing measures and school lockdown on child and adolescent mental health. Eur Child Adolesc Psychiatry Jun. 29, 739–742 (2020).
Solmi, M. et al. Physical and mental health impact of COVID-19 on children, adolescents, and their families: The Collaborative Outcomes study on Health and Functioning during Infection Times - Children and Adolescents (COH-FIT-C&A). J Affect Disord. 299, 367–376 (2022).
Panda, P. K. et al. Psychological and Behavioral Impact of Lockdown and Quarantine Measures for COVID-19 Pandemic on Children, Adolescents and Caregivers: A Systematic Review and Meta-Analysis. J Trop Pediatr. 67, fmaa122 (2021).
Scheiner, C., Seis, C., Kleindienst, N. & Buerger, A. Psychopathology, Protective Factors, and COVID-19 among Adolescents: A Structural Equation Model. Int J Environ Res Public Health. 20, 2493 (2023).
Pedrini, L. et al. Adolescents’ mental health and maladaptive behaviors before the Covid-19 pandemic and 1-year after: analysis of trajectories over time and associated factors. Child Adolesc Psychiatry Ment Health 16, 42 (2022).
Kirič, B., Leben Novak, L., Lušicky, P. & Drobnič Radobuljac, M. Suicidal Behavior in Emergency Child and Adolescent Psychiatric Service Users Before and During the 16 Months of the COVID-19 Pandemic. Frontiers in Psychiatry. 13, 893040 (2022).
Singh, S. et al. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 293, 113429 (2020).
Dessain, A. et al. Mental health during the COVID-19 pandemic in children and adolescents with ADHD: A systematic review of controlled longitudinal cohort studies. Neurosci Biobehav Rev. 156, 105502 (2024).
Vibert, B. et al. CRISIS AFAR: an international collaborative study of the impact of the COVID-19 pandemic on mental health and service access in youth with autism and neurodevelopmental conditions. Mol Autism. 14, 7 (2023).
Maulana, G., Khalilullah, K. & Yufika, A. The Impact of COVID-19 Pandemic on People with Intellectual Disabilities: A Literature Review. J. Asian Soc. Sci. Res. 3, (2021).
Graell, M. et al. Children and adolescents with eating disorders during COVID-19 confinement: Difficulties and future challenges. Eur Eat Disord Rev. 28, 864–870 (2020).
Cost, K. T. et al. Mostly worse, occasionally better: impact of COVID-19 pandemic on the mental health of Canadian children and adolescents. Eur Child Adolesc Psychiatry. 31, 671–684 (2022).
Zijlmans, J. et al. Mental and Social Health of Children and Adolescents With Pre-existing Mental or Somatic Problems During the COVID-19 Pandemic Lockdown. Front Psychiatry. 12, 692853 (2021).
Raffagnato, A. et al. The covid-19 pandemic: a longitudinal study on the emotional-behavioral sequelae for children and adolescents with neuropsychiatric disorders and their families. Int J Environ Res Public Health. 18, 9880 (2021).
Lewis, J. et al. Prospective Examination of Psychological Trauma Among Adolescents During the COVID-19 Pandemic. Psychol Trauma. Mar. 15, 404–414 (2023).
Chadi, N., Ryan, N. C. & Geoffroy, M. C. COVID-19 and the impacts on youth mental health: emerging evidence from longitudinal studies. Can J Public Health. 113, 44–52 (2022).
Barendse, M. E. et al. Longitudinal change in adolescent depression and anxiety symptoms from before to during the COVID-19 pandemic. J Res Adolesc. 33, 74–91 (2023).
Breaux, R. et al. Prospective impact of COVID-19 on mental health functioning in adolescents with and without ADHD: protective role of emotion regulation abilities. J Child Psychol Psychiatry. 62, 1132–1139 (2021).
Rosen, M. L. et al. Promoting youth mental health during the COVID-19 pandemic: A longitudinal study. PLoS One. 16, e0255294 (2021).
Bornstein, M. H., Jager, J. & Putnick, D. L. Sampling in developmental science: Situations, shortcomings, solutions, and standards. Developmental Review 33, 357–370 (2013).
Etikan, I., Musa, S. A. & Alkassim, R. S. Comparison of convenience sampling and purposive sampling. American Journal of Theoretical and Applied Statistics 5, 1–4 (2016).
Twisk, J. W. R. (2003). Applied longitudinal data analysis for epidemiology: A practical guide. Cambridge University Press.
Menard, S. (2008). Handbook of longitudinal research: Design, measurement, and analysis. Academic Press.
Eurostat (2019) Methodological manual on territorial typologies: 2018 edition. Luxembourg: Publications Office of the European Union. https://ec.europa.eu/eurostat/ramon/miscellaneous/index.cfm?TargetUrl=DSP_DEGURBA.
Hollingshead, A. B. Four-factor index of social status. Yale journal of Sociology. 8, 2011, 197 (1975).
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Guy, W. (1976). ECDEU assessment manual for psychopharmacology (Revised). U.S. Department of Health, Education, and Welfare; National Institute of Mental Health.
Shaffer, D. et al. A children’s global assessment scale (CGAS). Archives of General Psychiatry 40, 1228–1231 (1983).
Stefanelli, R. et al. IQ and socio-occupational functioning in relation to obsessive-compulsive symptoms severity in a clinical sample of adolescents. Sci Rep. 15, 14021 (2025).
Nikolaidis, A. et al. The Coronavirus Health and Impact Survey (CRISIS) reveals reproducible correlates of pandemic-related mood states across the Atlantic. Sci Rep. 11, 8139 (2021).
The jamovi project. (2024). jamovi (Version 2.3.28) [Computer software]. https://www.jamovi.org.
Bartlett, M. S. A Note on the Multiplying Factors for Various χ 2 Approximations. Journal of the Royal Statistical Society. Series B (Methodological) (Vol. 16, Issue 2). (1954).
Dziuban, C. D. & Shirkey, E. C. When is a correlation matrix appropriate for factor analysis? Some decision rules. In Psychological Bulletin (Vol. 81, (1974).
Kaiser, H. F. A second generation little jiffy* (Vol. 35, (1970).
Brown, T. A. Confirmatory Factor Analysis for Applied Research (Guilford Press) (2015).
Hayton, J. C. Factor retention decisions in exploratory factor analysis: A tutorial on parallel analysis. Organizational Research Methods, 191–205 (2004).
Gałecki, A. and B. T. M.-E. M. U. R. Linear Mixed-Effects Models Using R. (Springer) (2013).
De Giacomo, A. et al. Psychological impact of the SARS-CoV-2 pandemic in children with neurodevelopmental disorders and their families: evaluation before and during covid-19 outbreak among an Italian sample. Riv Psichiatr 56, 205–210 (2021).
Operto, F. F. et al. Impact of COVID-19 Pandemic on Children and Adolescents with Neuropsychiatric Disorders: Emotional/Behavioral Symptoms and Parental Stress. Int J Environ Res Public Health. 19, 3795 (2022).
O’Connor, M. et al. Socio-economic disparities in the psychosocial and economic impacts of the COVID-19 pandemic on children and young people in Australia. J Paediatr Child Health. 61, 267–276 (2025).
Thomson, K. C. et al. Parent psychological distress and parent-child relationships two years into the COVID-19 pandemic: Results from a Canadian crosssectional study. PLoS One. 18, e0292670 (2023).
Panchal, U. et al. The impact of COVID-19 lockdown on child and adolescent mental health: systematic review. Eur Child Adolesc Psychiatry. 32, 1151–1177 (2023).
Gadermann, A. C. et al. Examining the impacts of the COVID-19 pandemic on family mental health in Canada: findings from a national cross-sectional study. BMJ Open. 11, e042871 (2021).
Kourgiantakis, T. et al. Navigating inequities in the delivery of youth mental health care during the COVID-19 pandemic: perspectives of youth, families, and service providers. Can J Public Health. 113, 806–816 (2022).
Fegert, J. M., Vitiello, B., Plener, P. L. & Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: a narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc Psychiatry Ment Health. 14, 20 (2020).
Hawke, L. D. et al. Impacts of COVID-19 on Youth Mental Health, Substance Use, and Well-being: A Rapid Survey of Clinical and Community Samples: Répercussions de la COVID-19 sur la santé mentale, l’utilisation de substances et le bien-être des adolescents : un sondage rapide d'échantillons cliniques et communautaires. Can J Psychiatry. 65, 701–709 (2020).
Petrelli, A. et al. The impact of the COVID-19 pandemic on access to mental health services and socioeconomic inequalities in Italy. Front Psychiatry. 15, 1494284 (2024).
Marmot, M. The health gap: the challenge of an unequal world. Lancet. 386, 2442–2444 (2015).
Li, W. et al. Socioeconomic inequality in child mental health during the COVID-19 pandemic: First evidence from China. J Affect Disord. 287, 8 (2021).
Andrés, M. L. et al. Parental Perceptions of Child and Adolescent Mental Health During the COVID-19 Pandemic in Argentina. Child and Youth Care Forum 51, 1195–1225 (2022).
Davico, C., et al. COVID-19 Pandemic School Disruptions and Acute Mental Health in Children and Adolescents. JAMA Network Open, e2425829 (2022).
Conti, E. et al. Behavioural and emotional changes during covid-19 lockdown in an italian paediatric population with neurologic and psychiatric disorders. Brain Sci. 10, 918 (2020).
ISTAT. Mercato del lavoro e redditi: un’analisi integrata. Anno 2022. Statistiche Focus (4 Apr 2024). https://www.istat.it/it/files/2024/04/Focus-Occupazione-e-Reddito.pdf.
ISTAT. Rapporto annuale 2022: La situazione del Paese. Roma: Istituto Nazionale di Statistica; 2022. Capitolo 2, p. 111. paragrafo 2.4.1 La dinamica del mercato del lavoro italiano nel panorama europeo.
Duncan, G. J. & Magnuson, K. Socioeconomic status and cognitive functioning: moving from correlation to causation. Wiley Interdiscip Rev Cogn Sci. May 3, 377–386 (2012).
Sirin, S. R. Socioeconomic status and academic achievement: A meta-analytic review of research. Review of Educational Research 75, 417–453 (2005).
Li, W. et al. Socioeconomic inequality in child mental health during the COVID-19 pandemic: First evidence from China. J Affect Disord. 287, 8–14 (2021).
Zhang, L., Cao, H., Lin, C. & Ye, P. Family socio-economic status and Chinese Preschoolers’ anxious symptoms during the COVID-19 pandemic: the roles of parental investment, parenting style, home quarantine length, and regional pandemic risk. Early Child Res Q. 3rd Quarter 60, 137–149 (2022).
Spinelli, M., Lionetti, F., Setti, A. & Fasolo, M. Parenting Stress During the COVID-19 Outbreak: Socioeconomic and Environmental Risk Factors and Implications for Children Emotion Regulation. Fam Process. 60, 639–653 (2021).
Acknowledgements
We would like to dedicate this manuscript to our dear friend and colleague Alessandro Zuddas who greatly contributed to promote this work and sadly passed away in July 2022. We would like to express our deepest gratitude to the parents, caregivers, and children who generously gave their time during all the course of the COVID-19 pandemic. We are equally thankful to the research and clinical teams at all participating sites for their invaluable support in gathering both the survey data and the pre-pandemic clinical phenotypic data. The contribution of Dr. Masi e Dr. Milone was supported by the Italian Ministry of Health Grant RC 2025/2026.
Funding
Open access funding provided by Università degli Studi di Cagliari within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Contributions
F.D., C.B., A.C., A.G., G.M., P.M., S.S., B.V., A.Z., S.C. contributed to study conception and design; F.D., A.C., A.A., C.B., A.C., G.M., P.M., L.N., L.T., S.V., S.S., B.V., A.Z., S.C. contributed to site coordination and participation; F.D. M.P., C.B., A.C., A.A., S.B., C.B., V.C., A.C., F.L., A.M., P.M., L.N., M.P., M.P., M.P.R., M.T., L.T., S.U., S.V., S.S., B.V. were involved in data collection; F.D., M.P., M.A., D.M., B.V., S.C. contributed to data analyses; F.D., M.P., G.A., M.A., G.A., D.M., B.V., S.C. were involved in results’ interpretation; F.D., M.P., M.A., S.C. contributed to original manuscript drafting and revisions. All authors have contributed to critical revisions of the manuscript draft for important intellectual content, and they have read and approved the manuscript. A.Z. passed away after completion of the originally submitted manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
Ethical Committee of the Department of Biomedical Sciences at the University of Cagliari (Protocol No. 18 dated: 24/06/2020. Resolution No. 1012 dated: 15/07/2020). All contributing data from each site were approved by the local Institutional Review Boards (IRB) for data collection and sharing.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Donno, F., Prandini, M., Abbracciavento, G. et al. Socioeconomic status and perception of well-being and mental health support: a three-year COVID-19 study in children with psychopathology and their parents. Pediatr Res (2026). https://doi.org/10.1038/s41390-026-04978-6
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41390-026-04978-6
