
Abstract
Serum cytokine alterations are associated with the usage of antipsychotic medications (AP). However, few studies have been designed to longitudinally measure cytokine changes during AP exposure in individuals at clinical high risk (CHR) for psychosis. This study aimed to assess changes in levels of cytokines after initiating AP in the prodromal phase. This longitudinal study involved individuals with CHR who completed the 1-year follow-up reassessment. Individuals with CHR were grouped into those treated with AP (AP + group) and those without (AP- group). Levels of vascular endothelial growth factor (VEGF), granulocyte-macrophage colony-stimulating factor (GM-CSF), tumor necrosis factor-α (TNF-α), interleukin (IL)-1β, 2, 6, 8, and 10 were measured at baseline and 1 year after completion of the clinical assessment. This study included 88 CHR individuals (median age, 18 years and 40.9% [n = 36] women; AP- group: n = 28, AP + group: n = 60). The baseline serum levels of IL-6 were higher in the AP- group than in the AP + group (z = −2.577, p = 0.010). Self-controlled comparisons showed that VEGF (z = 3.826, p < 0.001), TNF-α (z = 2.642, p = 0.008), IL-8 (z = 2.300, p = 0.021), and GM-CSF (z = 2.346, p = 0.019) levels were significantly increased in the AP- group. In the AP + group, IL-6 (z = 3.512, p < 0.001) was significantly increased, IL-1β (z = 2.563, p = 0.010), and GM-CSF (z = 2.095, p = 0.036) were significantly decreased. Repeated-measures analysis of variance revealed a significant group × visit effect on VEGF (F = 20.348, p < 0.001), GM-CSF (F = 7.042, p = 0.013), and IL-1β(F = 4.670, p = 0.040). The findings revealed significant differences in trajectories between individuals with CHR who were and were not taking AP. There is an association between AP use in CHR individuals and differences in inflammatory and neurotrophic factor trajectories.
Similar content being viewed by others

Introduction
Antipsychotic medications (AP) represent frontline treatment options for patients with psychosis, effectively managing clinical symptoms, particularly severe hallucinations and delusions during acute phases. The impact of AP on cytokines in patients with first-episode and stabilized schizophrenia (SZ) has been extensively studied [1, 2]. Different antipsychotic drugs may yield varying effects on cytokines. For instance, Patlola et al. [3] conducted a systematic review on the effects of risperidone on cytokines in first-episode versus chronic patients with psychosis. They found a significant reduction in pro-inflammatory cytokines following risperidone treatment, with noteworthy changes in interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) levels observed mainly in chronic patients rather than first-episode psychosis (FEP) patients. However, their study revealed significant effects of disease duration. This suggests that investigating the impact of AP on cytokines in patients with post-onset psychosis may be confounded by the influence of the psychotic states on cytokine levels. Immune system dysfunction is considered a significant characteristic in psychosis, marked by substantial alterations in specific peripheral cytokine concentrations [4, 5]. A recent systematic review and network meta-analysis [6] found consistent elevation in concentrations of IL-1β, IL-1 receptor antagonist (IL-1RA), soluble interleukin-2 receptor (sIL-2R), IL-6, IL-8, IL-10, TNF-α, and C-reactive protein in individuals with acute and chronic psychosis compared to healthy controls. Hence, it remains unclear whether changes in cytokine levels are primarily influenced by the psychosis itself or by the AP exposure.
Therefore, it is conceivable that the influence of AP on cytokine levels during the clinical high risk (CHR) stage, prior to the onset of full psychosis, may be somewhat less confounded by the effects of the disease itself. However, our previous research suggests that the use of AP during the CHR stage may have more drawbacks than benefits [7, 8], with greater advantages observed in initiating AP treatment during the first episode rather than during the CHR stage [9]. In our previous investigation [7], we found that nearly 80% of individuals classified as CHR in our cohort received AP treatment. Consequently, observing the effects of AP on cytokine levels in CHR individuals in real-world settings to better understand the impact of AP on cytokines remains uncertain, since whether the effects of AP on cytokine levels in CHR individuals are similar to those observed in patients with psychosis remains unanswered.
This study utilized a longitudinally constructed real-world CHR cohort to compare the changes in cytokine levels between CHR individuals using and not using AP at baseline and 1-year follow-up, aiming to investigate the impact of AP on cytokines. The research hypothesis posits that AP usage would alter the trajectory of cytokine changes in CHR individuals, leading to a decrease in inflammatory factor levels (anti-inflammatory effects of AP [3]) and an increase in neurotrophic factor levels (neuroprotective effects of AP [10]). To achieve this, a combination of cross-sectional and longitudinal designs was employed to examine the dynamic alterations in cytokine levels, encompassing peripheral concentrations of vascular endothelial growth factor (VEGF), TNF-α, IL-8, IL-6, IL-1β, IL-10, and granulocyte-macrophage colony-stimulating factor (GM-CSF).
Materials and methods
Participants and setting
The present study is a component of the ShangHai At Risk for Psychosis-extended (SHARP-extended) program, which involved 131 help-seeking first-visit participants recruited consecutively from the Shanghai Mental Health Center (SMHC) between January 1, 2020, and August 8, 2023. This research focused on individuals at CHR for psychosis and was conducted at a single site, the SMHC in China. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human subjects/patients were approved by the Internal Review Board of the SMHC (Approval No. 2017-36 R). INFORMED consent was obtained from all participants during the recruitment stage. For participants under the age of 18, written parental INFORMED consent was obtained, and adolescents provided verbal assent. The research was conducted in accordance with the Declaration of Helsinki.
The SMHC serves as China’s largest outpatient facility for medication management and psychotherapy, catering to patients from various regions across the country. In this study, a total of 394 individuals meeting the criteria for CHR were identified through face-to-face interviews utilizing the Structured Interview for Prodromal Syndromes (SIPS) [11, 12]. Eligible participants ranged from 13 to 45 years of age at baseline—chosen because the CHR state predominantly affects adolescents and young adults, with psychosis transition likelihood decreasing significantly after 45 years—and had received a minimum of 6 years of primary education. Exclusion criteria encompassed individuals with severe somatic diseases (diseases that may affect immune function, interfere with cytokine detection or pose risks to follow-up safety, including but not limited to uncontrolled diabetes, active autoimmune diseases, malignant tumors) such as cancer, as well as those with mental retardation, developmental disorders, or substance abuse. Notably, during recruitment and follow-up assessments, we confirmed no participants had a history of smoking; combined with the young age of the cohort (median 18 years) and strict exclusion of severe somatic diseases, this ensured no participants had significant medical comorbidities that could influence cytokine levels. Due to study design constraints, body mass index data were not collected.
Out of the 131 individuals identified with CHR, 88 participants (67.2%) completed 1-year face-to-face reassessments using the SIPS along with blood sample recollection. Thirty-three individuals did not complete the 1-year follow-up assessments, and ten were lost to follow-up. Comprehensive details regarding the study procedures, settings, and measurement implementation can be found elsewhere [13,14,15,16]. A notable aspect of our sample was the psychotropic naivety of all participants upon study entry. They underwent clinical assessment without prior treatment for any psychiatric disorder.
Criteria and assessments
We employed the SIPS to identify individuals meeting criteria for CHR, based on one of the following prodromal syndrome criteria: (1) Brief Intermittent Psychotic Syndrome, (2) Attenuated Positive Symptom Syndrome, or (3) Genetic Risk and Deterioration Syndrome. The SIPS comprises 19 items designed to assess four symptom domains: positive symptoms, negative symptoms, disorganized symptoms, and general symptoms. Additionally, the Global Assessment of Functioning (GAF) scale was utilized to evaluate the patients’ overall psychological, social, and occupational functioning during the SIPS interview. In our previous studies, [14, 15] the Chinese version [16] of SIPS, which was developed by the SHARP team, also demonstrated good inter-rater reliability (intraclass correlation coefficient r = 0·96, p < 0·01 for the SIPS total score) and validity (26·4% converted to psychosis in the following 2 years) in China. The first author is SIPS certified through Yale University-sponsored SIPS training.
Psychosis conversion, the primary outcome of this study, was assessed using the Presence of Psychotic Symptoms (POPS) criteria [17] derived from the SIPS. Conversion was specifically defined by the presence of a positive symptom rated at level “6,” indicating severe and psychotic, which is either dangerous, disorganized, or occurs for at least an hour a day on average over four days a week, totaling at least 16 h overall.
Antipsychotic exposure and groups
The current study is a naturalistic follow-up investigation [7, 18, 19], involving no additional intervention or financial compensation. The assumption of AP usage was documented by researchers during follow-up assessments, corroborated by family members, and verified through clinician reports and medical records. Information regarding medication usage was systematically recorded, including the types of antipsychotics, drug response, and duration of reduction or withdrawal. Specifically, individuals with CHR who had received AP treatment for at least 2 weeks [20, 21], with a minimum equivalent dose of 5 mg of olanzapine [22], were classified into the AP + group. Specifically, individuals with CHR in the AP + group had taken APs with an olanzapine-equivalent mean dose of 10.7 mg (standard deviation [SD] = 5.6 mg) for a mean duration of 45.7 weeks (SD = 12.7 weeks). During the 1-year follow-up, individuals with CHR were prescribed various types of AP, including aripiprazole (n = 20), olanzapine (n = 18), risperidone (n = 8), amisulpride (n = 4), paliperidone (n = 2), quetiapine (n = 2) and multiple APs (n = 6). To explore whether different AP types affect cytokine changes, we conducted subgroup analyses focusing on the three most commonly used APs (aripiprazole, olanzapine, risperidone) due to limited sample sizes in other AP subgroups. Using Kruskal-Wallis H tests, we compared baseline-to-1-year changes in key cytokines among the three subgroups. No significant differences in the magnitude of cytokine changes were observed across the three AP types (all p > 0.05). A small group of participants took psychoactive medication other than antipsychotic (27 individuals took antidepressants, with a fluoxetine-equivalent [23] dose of 29.7 mg [SD = 13.1], and the mean administration duration was 21.7 [SD = 12.9] weeks). To rule out potential confounding of antidepressant use on cytokine changes, we conducted a sensitivity analysis: subgroup analyses of baseline-to-1-year cytokine changes were performed within the AP- and AP + groups, stratified by antidepressant use (yes/no). Results showed no significant differences in the direction or magnitude of cytokine changes between subgroups with and without antidepressants (all p > 0.05), indicating antidepressant use did not substantially confound the observed cytokine trajectories.
Measurement of cytokine levels
Venous blood samples were obtained both at baseline and during the 1-year follow-up period [24, 25]. Collection was conducted in the morning after participants had fasted for a minimum of 3 h. Ten mL of peripheral venous blood were drawn into anticoagulant-free tubes. After 1 h at room temperature, the samples underwent centrifugation at 1,710 g for 20 min at 4 °C to separate the serum. The serum was then stored at −80 °C until analysis. Analysis was performed using enzyme-linked immunosorbent assay with the Human HS Cytokine Premixed Kit (Catalog#: FCSTM09-10, USA) following the manufacturer’s instructions. Duplicate measurements were taken for each sample. The concentrations of VEGF, TNF-α, IL-8, IL-6, IL-1β, IL-10, and GM-CSF were expressed as pictograms of protein per milliliter of serum (pg/mL). Calibration of all data was conducted using standard curves generated for each cytokine.
Statistical analysis
CHR individuals were categorized based on their antipsychotic assumption during the follow-up period into two groups: AP- and AP + . Quantitative variables were presented as mean (standard deviation) for normally distributed data and median (interquartile range) for non-normally distributed data. Qualitative variables were expressed as frequencies (%). The normality of inflammatory variables’ distribution was assessed using the Kolmogorov-Smirnov test, revealing non-normal distribution for all cytokine variables. Group comparisons were conducted using χ2 tests for categorical variables and independent t-tests or Mann-Whitney tests for continuous variables. Changes in cytokine levels between baseline and 1-year follow-up were compared using the paired sample Wilcoxon signed rank test for non-normally distributed continuous variables; effect sizes for significant changes were calculated as r values using the formula r = z/\(\sqrt{n}\) (z = Wilcoxon z-statistic, n = sample size per group). Trajectories of cytokine levels between the AP- and AP + groups were evaluated using repeated-measures analysis of variance (RMANOVA). RMANOVA with a factorial design (2 visits × 2 groups) was employed to assess significant interactions between visit (baseline and 1-year) and group (AP- and AP + ) regarding their effects on cytokine levels. Effect size was evaluated using η2, with values of 0.01 indicating a small effect, 0.06 indicating a medium effect, and 0.14 indicating a large effect. To account for the potential influence of psychosis conversion on cytokine trajectories, we further adjusted the RMANOVA model by including conversion status (converter/non-converter) as a covariate.
To enhance the readability and logical flow of the results section in this document, the following presentation structure was implemented: (1) First, report baseline demographic and clinical characteristics and their group comparisons to establish cohort comparability; (2) second, describe changes in clinical characteristics at the 1-year follow-up to track temporal shifts in the cohort’s clinical profile; (3) third, present within-group changes in cytokine levels (via Wilcoxon signed-rank tests) to highlight subgroup-specific temporal trends; (4) finally, report RANOVA results (main effects of group and time, visit × group interactions) and corresponding post-hoc analyses to synthesize longitudinal group differences in cytokine trajectories.
Results
Baseline demographic, clinical and cytokine characteristics
The baseline characteristics of the AP- and AP + groups are summarized in Table 1. Most variables showed no statistically significant differences. However, the AP + group had more males (χ2 = 4.477, p = 0.034) than the AP- group. Additionally, the level of IL-6 (z = −2.577, p = 0.010) was higher in the AP- group than in the AP + group.
Follow-up clinical and cytokine characteristics
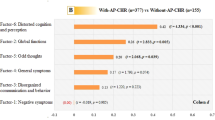
The 1-year follow-up characteristics of the AP- and AP + groups are summarized in Table 2. The AP + group exhibited a higher severity level of negative symptoms (t = −2.123, p = 0.037) and disorganization symptoms (t = −2.105, p = 0.038) compared to the AP- group.
Self-controlled comparisons of cytokine levels
The paired sample Wilcoxon tests (Fig. 1) showed that VEGF (z = 3.826, p < 0.001, r = 0.408), TNF-α (z = 2.642, p = 0.008, r = 0.282), IL-8 (z = 2.300, p = 0.021, r = 0.245), and GM-CSF (z = 2.346, p = 0.019, r = 0.250) levels were significantly increased in the AP- group. In the AP + group, IL-6 (z = 3.512, p < 0.001, r = 0.449) was significantly increased, IL-1β (z = 2.563, p = 0.010, r = 0.327) and GM-CSF (z = 2.095, p = 0.036, r = 0.267) were significantly decreased.

GM-CSF, granulocyte-macrophage colony-stimulating factor; IL-10, interleukin (IL)-10; IL-1β, interleukin (IL)-1beta; IL-6, interleukin (IL)-6; IL-8, interleukin (IL)-8; TNF-α, tumor necrosis factor-α; VEGF, vascular endothelial growth factor; The paired Wilcoxon test was used for self-controlled analysis. The level of statistical significance was set at a two-tailed p value of 0.05. Effect sizes (r values) were calculated as (r = z/\(\sqrt{n}\) (n = 28 for AP- group, n = 60 for AP + group); r ≥ 0.5 indicates large effect, 0.3 ≤ r < 0.5 indicates medium effect, 0.1 ≤ r < 0.3 indicates small effect.
Changes of clinical and cytokine factors
After a 1-year follow-up, data analyzed using the RMANOVA model (Table 3) revealed a significant group × visit effect on VEGF (F = 20.348, df = 1, p < 0.001), GM-CSF (F = 7.042, df = 1, p = 0.013), and IL-1β (F = 4.670, df = 1, p = 0.040). No significant group effect was observed for both clinical and cytokine variables. However, a significant visit effect was noted on all clinical variables, VEGF (F = 4.902, df = 1, p = 0.035), and TNF-α (F = 5.412, df = 1, p = 0.028).
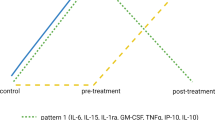
To interpret the significant time × group interactions, post-hoc pairwise comparisons were conducted to assess within-group changes from baseline to follow-up. For VEGF, levels increased significantly in the AP- group, whereas no significant change was observed in the AP + group. This indicates that AP use may mitigate the natural upward trend of VEGF in non-AP users. For IL-1β, the AP- group showed no significant change, while the AP + group exhibited a significant decrease. This suggests that AP use is associated with reduced IL-1β levels over time. For GM-CSF, the AP- group had a significant increase in levels, whereas the AP + group had a significant decrease. This demonstrates opposing trajectory patterns based on AP use (Fig. 2).

GM-CSF, granulocyte-macrophage colony-stimulating factor; IL-10, interleukin (IL)-10; IL-1β, interleukin (IL)-1beta; IL-6, interleukin (IL)-6; IL-8, interleukin (IL)-8; TNF-α, tumor necrosis factor-α; VEGF, vascular endothelial growth factor; RMANOVA, repeated measures analysis of variance.
When including conversion status as a covariate in the RMANOVA model, the core group × visit interactions reflecting AP effects remained robust, confirming AP use drives cytokine trajectory differences independent of psychosis conversion. For conversion status-related effects, there were no significant between-subject differences in baseline cytokine levels by conversion status (all p > 0.05); among within-subject time × conversion status interactions, only IL-10 showed significance (F = 4.107, p = 0.046), while all other cytokines had no significant conversion-related time-dependent changes (all p > 0.05). Notably, IL-10 had no significant AP-related trajectory differences in the original model, so its conversion-related interaction does not affect core conclusions about AP.
Discussion
This study aimed to investigate the association between AP use and cytokine profiles in the CHR state. To the best of our knowledge, this is the first study to examine the impact of AP on cytokines in CHR individuals. The findings revealed comparable baseline characteristics between the AP- and AP + groups, with the only notable differences being a higher proportion of males and lower levels of IL-6 observed in the AP + group. No significant differences were observed in other variables. Dynamic changes in cytokine levels during the follow-up period showed significant increases in VEGF, TNF-α, IL-8, and GM-CSF levels in the AP- group, while IL-6 levels significantly increased and IL-1β and GM-CSF levels decreased in the AP + group. Consistent with our hypothesis, there was an association between AP use and differences in the trajectory of cytokine changes. Moreover, significant differences were observed in the change trajectories of VEGF, IL-1β, and GM-CSF between the two groups, with increases in the AP- group and decreases in the AP + group.
In our study sample of CHR individuals, we observed a more pronounced effect of AP on VEGF levels. Specifically, in the AP- group, VEGF levels significantly increased after 1 year, whereas the changes in VEGF levels were minimal in the AP + group. Additionally, there were significant differences in the trajectory of VEGF changes between the two groups. This finding is inconsistent with previous research in patients with SZ [26]. A major topic in the literature regarding the role of VEGF in SZ revolves around whether the VEGF molecular pathway is involved in the mechanism of action of AP. Several studies [27, 28] have reported higher serum VEGF levels in patients with SZ treated with AP compared to controls. This evidence suggests that AP therapy may exert its action by directly and/or indirectly increasing serum VEGF levels, possibly by inducing VEGF gene expression in brain areas critical to the pathophysiology of SZ [29, 30]. The discrepancy in research conclusions may primarily relate to the stage of psychosis. CHR represents the prodromal phase of the illness, whereas SZ represents the later stage. In the CHR stage, baseline VEGF levels may not be abnormal [31], leading to minimal changes with AP use. Conversely, in the AP- group, the significant increase in VEGF levels suggests that individuals in the CHR stage may possess self-regulatory mechanisms under conditions of stress and inflammation imbalance [24]. This notion is supported by Ye et al. [32, 33], who found no baseline VEGF abnormalities in CHR individuals and reported a trend of VEGF elevation in unmedicated CHR participants over follow-up—consistent with our observation of significant VEGF increase in the AP- group and minimal changes in the AP + group.
In terms of inflammatory factors, we observed an overall increase in cytokine levels among individuals with CHR, regardless of whether they were in the AP + or AP- group. Particularly noteworthy were the elevated levels of TNF-α in the AP- group and IL-6 in the AP + group. The only exception was a decrease in IL-1β levels in the AP + group, while the AP- group showed a trend towards an increase (p = 0.06), with significant differences observed in the trajectory of changes between the two groups. Numerous studies [34], including meta-analyses [35], have reported elevated levels of IL-6 in various phases of SZ, with the majority of patients receiving AP treatment [36]. For instance, Hartwig et al. [37] identified increased levels of soluble IL-6 receptors in a clinical two-sample Mendelian randomization study, suggesting a compensatory response to elevated IL-6 levels in SZ. Similarly, multiple studies have reported elevated levels of TNF-α and IL-8, other pro-inflammatory cytokines, in SZ [38, 39] and CHR populations [32].
The IL-1 family, including IL-1β, represents major pro-inflammatory cytokines. While many studies have reported elevated IL-1β levels in SZ [40], particularly among those receiving atypical APs, findings regarding IL-1β in SZ have not been consistent. For example, a meta-analysis by Potvin et al. [41] in 2008 found no significant alterations in IL-1β levels in both in vivo and in vitro studies. Interestingly, a study [42] observed decreased levels of IL-1β in first-episode drug-naïve patients with a disease duration of less than 2 years, suggesting that the trajectory of IL-1β changes may differ among early-stage patients. Furthermore, GM-CSF is recognized as a crucial hematopoietic growth factor and immune modulator, exerting profound effects on the functional activities of various circulating leukocytes [43]. In this study, GM-CSF levels increased in the AP- group while decreased in the AP + group, indicating differential trajectories of change. This observation suggests that AP may have indirect anti-inflammatory effects. However, the results of this study also imply that the effects of AP on inflammatory factors in CHR individuals are complex, potentially characterized by a pattern of changes rather than being solely determined by a few factors.
Despite its novelty, the present study has several limitations: (1) The CHR cohort was followed up naturally, and the types, doses, and durations of AP use could not be controlled. Although all patients were prescribed atypical AP, it remains unknown whether different types of AP have different effects on cytokines, posing a confounding factor. As a naturalistic real-world study, we were unable to randomize participants to AP + or AP- groups, and AP use was non-random (potentially tied to clinical judgment of illness severity or transition risk). While Table 1 shows no significant baseline differences between groups in SIPS subscales (SIPS-P, SIPS-N, SIPS-D, SIPS-G) or total score (all p > 0.05)—suggesting baseline illness severity may have limited impact—this non-random assignment still introduces the possibility of unmeasured confounding (e.g., uncaptured clinical factors influencing AP prescription). Additionally, we categorized participants into AP + or AP- based on overall 1-year exposure, without collecting granular data on short-term AP use fluctuations or within-participant switches between AP + and AP- status. This binary grouping cannot capture the nuanced impact of dynamic AP exposure patterns on cytokine changes. (2) The sample included in the analysis had a poor sex balance, with males being more likely to use AP than females. This disparity might reduce statistical power and bias the results. Supplementary analysis showed only baseline IL-1β in the AP- group was higher in males than females (z = −1.974, p = 0.048); no other gender-related cytokine differences existed in either the AP- or AP + group, so this single difference did not confound core AP-related cytokine trajectory comparisons. (3) Due to limited resources, only VEGF, a neurotrophic factor-related cytokine, was included in the study, and the trajectories of change for other factors are unknown. Our focus on VEGF alone means conclusions about neurotrophic factor trajectories should be interpreted with caution, as we cannot rule out that other neurotrophic factors may exhibit different change patterns in response to AP. (4) The CHR status was followed up for only 1 year, and some individuals with CHR may transition to psychosis beyond this timeframe. Although the study primarily focused on the CHR state, there may be differences in conversion rates between the AP + and AP- groups in the future [44], particularly within 2 to 3 years, leading to mismatch between the two groups.
Conclusions
This study investigated the effects of AP on both inflammatory and neurotrophic factor responses in individuals with CHR status, representing the first examination of its kind in this population. The findings revealed significant differences in trajectories between individuals who were and were not taking AP, indicating that VEGF, IL-1β, and GM-CSF decreased in CHR individuals using AP, while they increased in those without AP usage. These results suggest that AP usage may influence both inflammatory and neurotrophic factor trajectories in CHR individuals. Future directions to build on this work include collecting granular short-term AP use data for shorter observation window analyses, enrolling larger cohorts to enable within-participant pre/post AP comparisons, expanding measured cytokines, and conducting longer follow-up to link AP-related cytokine changes to long-term outcomes like psychosis conversion.
Data availability
The dataset(s) generated during the current study are not publically available due to ethical restrictions but are available from the corresponding author on reasonable request.
References
Lin C, Chen K, Yu J, Feng W, Fu W, Yang F, et al. Relationship between TNF-alpha levels and psychiatric symptoms in first-episode drug-naive patients with schizophrenia before and after risperidone treatment and in chronic patients. BMC Psychiatry. 2021;21:561.
Chen D, Li H, Zhao Q, Song J, Lin C, Yu J. Effect of risperidone treatment on insulin-like growth factor-1 and interleukin-17 in drug naive first-episode schizophrenia. Psychiatry Res. 2021;297:113717.
Patlola SR, Donohoe G, McKernan DP. Anti-inflammatory effects of 2nd generation antipsychotics in patients with schizophrenia: a systematic review and meta-analysis. J Psychiatr Res. 2023;160:126–36.
Zhang Y, Shi H, Yang G, Yang Y, Li W, Song M, et al. Associations between expression of indoleamine 2, 3-dioxygenase enzyme and inflammatory cytokines in patients with first-episode drug-naive Schizophrenia. Transl Psychiatry. 2021;11:595.
Engh JA, Ueland T, Agartz I, Andreou D, Aukrust P, Boye B, et al. Plasma levels of the cytokines B cell-activating factor (BAFF) and a proliferation-inducing ligand (april) in schizophrenia, bipolar, and major depressive disorder: a cross sectional, multisite study. Schizophr Bull. 2022;48:37–46.
Halstead S, Siskind D, Amft M, Wagner E, Yakimov V, Shih-Jung Liu Z, et al. Alteration patterns of peripheral concentrations of cytokines and associated inflammatory proteins in acute and chronic stages of schizophrenia: a systematic review and network meta-analysis. Lancet Psychiatry. 2023;10:260–71.
Zhang T, Xu L, Tang X, Wei Y, Hu Q, Hu Y, et al. Real-world effectiveness of antipsychotic treatment in psychosis prevention in a 3-year cohort of 517 individuals at clinical high risk from the SHARP (ShangHai At Risk for Psychosis). Aust N. Z J Psychiatry. 2020;54:696–706.
Zhang T, Raballo A, Zeng J, Gan R, Wu G, Wei Y, et al. Antipsychotic prescription, assumption and conversion to psychosis: resolving missing clinical links to optimize prevention through precision. Schizophrenia. 2022;8:48.
Zhang T, Xu L, Wei Y, Tang X, Hu Y, Cui H, et al. When to initiate antipsychotic treatment for psychotic symptoms: At the premorbid phase or first episode of psychosis?. Aust N. Z J Psychiatry. 2021;55:314–23.
Chen AT, Nasrallah HA. Neuroprotective effects of the second generation antipsychotics. Schizophr Res. 2019;208:1–7.
Miller TJ, McGlashan TH, Rosen JL, Cadenhead K, Cannon T, Ventura J, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. 2003;29:703–15.
Miller TJ, McGlashan TH, Rosen JL, Somjee L, Markovich PJ, Stein K, et al. Prospective diagnosis of the initial prodrome for schizophrenia based on the structured interview for prodromal syndromes: preliminary evidence of interrater reliability and predictive validity. Am J Psychiatry. 2002;159:863–5.
Zhang T, Li H, Woodberry KA, Seidman LJ, Chow A, Xiao Z, et al. Interaction of social role functioning and coping in people with recent-onset attenuated psychotic symptoms: a case study of three Chinese women at clinical high risk for psychosis. Neuropsychiatr Dis Treat. 2015;11:1647–54.
Zhang T, Li H, Woodberry KA, Seidman LJ, Zheng L, Li H, et al. Prodromal psychosis detection in a counseling center population in China: an epidemiological and clinical study. Schizophr Res. 2014;152:391–9.
Zhang TH, Li HJ, Woodberry KA, Xu LH, Tang YY, Guo Q, et al. Two-year follow-up of a Chinese sample at clinical high risk for psychosis: timeline of symptoms, help-seeking and conversion. Epidemiol Psychiatr Sci. 2017;26:287–98.
Zheng L, Wang J, Zhang T, Li H, Li C, Jiang K. The Chinese version of the SIPS/SOPS: a pilot study of reliability and validity. Chin Ment Health J. 2012;26:571–6.
McGlashan T, Walsh B, Woods S The Psychosis-Risk Syndrome: Handbook for Diagnosis and Follow-up. New York;Oxford University Press:2010.
Zhang T, Wang J, Xu L, Wei Y, Tang X, Hu Y, et al. Further evidence that antipsychotic medication does not prevent long-term psychosis in higher-risk individuals. Eur Arch Psychiatry Clin Neurosci. 2022;272:591–602.
Zhang T, Xu L, Li H, Cui H, Tang Y, Wei Y, et al. Individualized risk components guiding antipsychotic delivery in patients with a clinical high risk of psychosis: application of a risk calculator. Psychol Med. 2021;52:3412–21.
Levine SZ, Leucht S. Early symptom response to antipsychotic medication as a marker of subsequent symptom change: an eighteen-month follow-up study of recent episode schizophrenia. Schizophr Res. 2012;141:168–72.
Schennach-Wolff R, Seemuller FH, Mayr A, Maier W, Klingberg S, Heuser I, et al. An early improvement threshold to predict response and remission in first-episode schizophrenia. Br J Psychiatry. 2010;196:460–6.
Leucht S, Samara M, Heres S, Davis JM. Dose equivalents for antipsychotic drugs: The DDD method. Schizophr Bull. 2016;42(Suppl 1):S90–94.
Hayasaka Y, Purgato M, Magni LR, Ogawa Y, Takeshima N, Cipriani A, et al. Dose equivalents of antidepressants: evidence-based recommendations from randomized controlled trials. J Affect Disord. 2015;180:179–84.
Zhang T, Wei Y, Zeng J, Ye J, Tang X, Xu L, et al. Interleukin-2/interleukin-6 imbalance correlates with conversion to psychosis from a clinical high-risk state. Psychiatry Clin Neurosci. 2023;77:62–3.
Zhang T, Zeng J, Wei Y, Ye J, Tang X, Xu L, et al. Changes in inflammatory balance correlates with conversion to psychosis among individuals at clinical high-risk: a prospective cohort study. Psychiatry Res. 2022;318:114938.
Rampino A, Annese T, Torretta S, Tamma R, Falcone RM, Ribatti D. Involvement of vascular endothelial growth factor in schizophrenia. Neurosci Lett. 2021;760:136093.
Pillai A, Howell KR, Ahmed AO, Weinberg D, Allen KM, Bruggemann J, et al. Association of serum VEGF levels with prefrontal cortex volume in schizophrenia. Mol Psychiatry. 2016;21:686–92.
Balotsev R, Koido K, Vasar V, Janno S, Kriisa K, Mahlapuu R, et al. Inflammatory, cardio-metabolic and diabetic profiling of chronic schizophrenia. Eur Psychiatry. 2017;39:1–10.
Katsel P, Roussos P, Pletnikov M, Haroutunian V. Microvascular anomaly conditions in psychiatric disease. Schizophrenia - angiogenesis connection. Neurosci Biobehav Rev. 2017;77:327–39.
Lopes R, Soares R, Coelho R, Figueiredo-Braga M. Angiogenesis in the pathophysiology of schizophrenia - a comprehensive review and a conceptual hypothesis. Life Sci. 2015;128:79–93.
Zhang T, Zeng J, Wei Y, Ye J, Tang X, Xu L, et al. Changes in inflammatory markers in clinical high risk of developing psychosis. Neuropsychobiology. 2023;82:104–16.
Ye J, Wei Y, Zeng J, Gao Y, Tang X, Xu L, et al. Serum levels of tumor necrosis factor-alpha and vascular endothelial growth factor in the subtypes of clinical high risk individuals: a prospective cohort study. Neuropsychiatr Dis Treat. 2023;19:1711–23.
Ye J, Zhang T. Serum levels of tumor necrosis factor-alpha and vascular endothelial growth factor in the subtypes of clinical high risk individuals: a prospective cohort study [response to letter]. Neuropsychiatr Dis Treat. 2023;19:2055–6.
Lesh TA, Careaga M, Rose DR, McAllister AK, Van de Water J, Carter CS, et al. Cytokine alterations in first-episode schizophrenia and bipolar disorder: relationships to brain structure and symptoms. J Neuroinflammation. 2018;15:165.
Miller BJ, Buckley P, Seabolt W, Mellor A, Kirkpatrick B. Meta-analysis of cytokine alterations in schizophrenia: clinical status and antipsychotic effects. Biol Psychiatry. 2011;70:663–71.
Frydecka D, Krzystek-Korpacka M, Lubeiro A, Stramecki F, Stanczykiewicz B, Beszlej JA, et al. Profiling inflammatory signatures of schizophrenia: a cross-sectional and meta-analysis study. Brain Behav Immun. 2018;71:28–36.
Hartwig FP, Borges MC, Horta BL, Bowden J, Davey Smith G. Inflammatory biomarkers and risk of schizophrenia: a 2-sample mendelian randomization study. JAMA Psychiatry. 2017;74:1226–33.
Di Nicola M, Cattaneo A, Hepgul N, Di Forti M, Aitchison KJ, Janiri L, et al. Serum and gene expression profile of cytokines in first-episode psychosis. Brain Behav Immun. 2013;31:90–5.
Goldsmith DR, Rapaport MH, Miller BJ. A meta-analysis of blood cytokine network alterations in psychiatric patients: comparisons between schizophrenia, bipolar disorder and depression. Mol Psychiatry. 2016;21:1696–709.
Upthegrove R, Manzanares-Teson N, Barnes NM. Cytokine function in medication-naive first episode psychosis: a systematic review and meta-analysis. Schizophr Res. 2014;155:101–8.
Potvin S, Stip E, Sepehry AA, Gendron A, Bah R, Kouassi E. Inflammatory cytokine alterations in schizophrenia: a systematic quantitative review. Biol Psychiatry. 2008;63:801–8.
Zhu F, Zhang L, Liu F, Wu R, Guo W, Ou J, et al. Altered serum tumor necrosis factor and interleukin-1beta in first-episode drug-naive and chronic schizophrenia. Front Neurosci. 2018;12:296.
Shi Y, Liu CH, Roberts AI, Das J, Xu G, Ren G, et al. Granulocyte-macrophage colony-stimulating factor (GM-CSF) and T-cell responses: what we do and don’t know. Cell Res. 2006;16:126–33.
Zeng J, Raballo A, Gan R, Wu G, Wei Y, Xu L, et al. Antipsychotic exposure in clinical high risk of psychosis: empirical insights from a large cohort study. J Clin Psychiatry. 2022;83:21m14092.
Acknowledgements
This study was supported by the Ministry of Science and Technology of China, National Key R&D Program of China (2023YFC2506800), National Natural Science Foundation of China (82171544, 82371505, 82151314, 82101623), The Shanghai Municipal Health Commission Clinical Research Special Project (202440203), the STI 2030-Major Projects (2022ZD0208500), Shenzhen Science and Technology Plan Project (JCYJ20220530165009020), and Qingdao Science and Technology Benefit People Program (22-3-7-smjk-19-nsh).
Author information
Authors and Affiliations
Contributions
Dr. THZ, YYW, LHX, and JJW. conceptualized the study, wrote the first draft of manuscript and conducted the statistical analyses. QH, HRC, ZHY, and YYW. interviewed participants and collected and organized the primary data. MLJ, HCL, JHZ, JG, YYT, LYZ, and XCT. managed the literature searches, statistical analyses and edited the manuscript. CBL, THZ and JJW. designed the study and provided supervision in the implementation of the study. All authors have approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Research Ethics Committee of the Shanghai Mental Health Center granted ethical approval for the study (2017-36 R). INFORMED consent was obtained from all participants during the recruitment stage. For participants under the age of 18, written parental INFORMED consent was obtained, and adolescents provided verbal assent. The research was conducted in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wei, Y., Xu, L., Zhang, D. et al. Cytokine changes in clinical high risk for psychosis population following antipsychotic medication. Transl Psychiatry 16, 48 (2026). https://doi.org/10.1038/s41398-025-03763-z
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41398-025-03763-z
