
Abstract
Background
Near vision loss (NVL) represents a major global health challenge. However, its epidemiological research is less extensive compared to that of distance vision impairment. To fill this gap, this study examined worldwide patterns in NVL prevalence and disease burden from 1990 to 2021 and forecasted trends up to 2032.
Methods
Using data from the Global Burden of Disease (GBD) 2021 study, which covers 204 countries and territories, we assessed four key epidemiological measures: prevalence, disability-adjusted life years (DALYs), age-standardised prevalence rates (ASPRs), and age-standardised DALY rates (ASDRs). Future trends through 2032 were predicted employing Bayesian age-period-cohort (BAPC) modelling.
Results
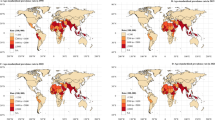
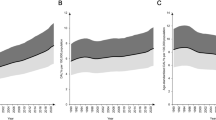
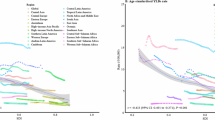
Between 1990 and 2021, global ASPRs for NVL rose by 37% (95% UI: 28–46%), and ASDRs increased by 38% (29–47%). In 2021, over 1.1 billion people worldwide were affected by NVL, leading to 11.6 million DALYs. The low-middle socio-demographic index (SDI) regions showed the highest ASPRs (16,252.9 per 100,000) and ASDRs (162.8 per 100,000), with females consistently experiencing higher rates than males. Projections suggest that ASPRs will continue to rise through 2032.
Conclusions
With the growing burden of NVL, it remains a significant global health issue. Consequently, focused allocation of resources toward NVL prevention and management is essential. Particular attention should be given to older adults and women, who are more susceptible to this condition.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 18 print issues and online access
$259.00 per year
only $14.39 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others
Data availability
The data used in this study can be derived from the GBD 2021 (Available at: https://ghdx.healthdata.org/gbd-2021).
References
Fricke TR, Tahhan N, Resnikoff S, Papas E, Burnett A, Ho SM, et al. Global prevalence of presbyopia and vision impairment from uncorrected presbyopia: systematic review, meta-analysis, and modelling. Ophthalmology. 2018;125:1492–9.
Wang Y, Lou L, Cao J, Shao J, Ye J. Socio-economic disparity in global burden of near vision loss: an analysis for 2017 with time trends since 1990. Acta Ophthalmol. 2020;98:e138–e143.
Rupert B, Jaimie DS, Seth F, Paul SB, Hugh RT, Serge R, et al. Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021;9:e130–e143.
Xu Y, Mao Y, Lin X, Gao Z, Ruan X. Trend and projection of the prevalence and burden of near vision loss in China and globally from 1990 to 2030: a Bayesian age-period-cohort modeling study. J Glob Health. 2024;14:04119.
Tahhan N, Papas E, Fricke TR, Frick KD, Holden BA. Utility and uncorrected refractive error. Ophthalmology. 2013;120:1736–44.
Frick KD, Joy SM, Wilson DA, Naidoo KS, Holden BA. The global burden of potential productivity loss from uncorrected presbyopia. Ophthalmology. 2015;122:1706–10.
Eckert KA, Carter MJ, Lansingh VC, Wilson DA, Furtado JM, Frick KD, et al. A simple method for estimating the economic cost of productivity loss due to blindness and moderate to severe visual impairment. Ophthalmic Epidemiol. 2015;22:349–55.
Reddy PA, Congdon N, MacKenzie G, Gogate P, Wen Q, Jan C, et al. Effect of providing near glasses on productivity among rural Indian tea workers with presbyopia (PROSPER): a randomised trial. Lancet Glob Health. 2018;6:e1019–e1027.
Ng Yin Ling C, Seshasai S, Chee ML, He F, Tham YC, Cheng CY, et al. Visual impairment, major eye diseases, and mortality in a multi-ethnic Asian population and a meta-analysis of prospective studies. Am J Ophthalmol. 2021;231:88–100.
Sun J, Li L, Sun J. Sensory impairment and all-cause mortality among the elderly adults in China: a population-based cohort study. Aging. 2020;12:24288–24300.
Almidani L, Miller R, Varadaraj V, Mihailovic A, Swenor BK, Ramulu PY. Vision impairment and psychosocial function in US adults. JAMA Ophthalmol. 2024;142:283–91.
Seong HJ, Kim J, Yook TM, Lee D, Chung EJ. Association between vision impairment and depression: a 9-year, longitudinal, nationwide, population-based cohort study in South Korea. Br J Ophthalmol. 2023;107:1390–4.
Shang X, Zhu Z, Wang W, Ha J, He M. The association between vision impairment and incidence of dementia and cognitive impairment: a systematic review and meta-analysis. Ophthalmology. 2021;128:1135–49.
Yamada Y, Nakashima H, Nagae M, Watanabe K, Fujisawa C, Komiya H, et al. Dual sensory impairment predicts an increased risk of postdischarge falls in older patients. J Am Med Dir Assoc. 2024;25:105123.
Cen J, Wang Q, Cheng L, Gao Q, Wang H, Sun F. Global, regional, and national burden and trends of migraine among women of childbearing age from 1990 to 2021: insights from the Global Burden of Disease Study 2021. J Headache Pain. 2024;25:96.
Qin N, Fan Y, Yang T, Yang Z, Fan D. The burden of gastric cancer and possible risk factors from 1990 to 2021, and projections until 2035: findings from the Global Burden of Disease Study 2021. Biomark Res. 2025;13:5.
Yu J, Yang X, He W, Ye W. Burden of pancreatic cancer along with attributable risk factors in Europe between 1990 and 2019, and projections until 2039. Int J Cancer. 2021;149:993–1001.
Bourne RRA, Flaxman SR, Braithwaite T, Cicinelli MV, Das A, Jonas JB, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 2017;5:e888–e897.
Zou M, Chen A, Liu Z, Jin L, Zheng D, Congdon N, et al. The burden, causes, and determinants of blindness and vision impairment in Asia: an analysis of the Global Burden of Disease Study. J Glob Health. 2024;14:04100.
Yin J, Jiang B, Zhao T, Guo X, Tan Y, Wang Y. Trends in the global burden of vision loss among the older adults from 1990 to 2019. Front Public Health. 2024; 12:1324141.
Bourne RRA, Cicinelli MV, Sedighi T, Tapply IH, McCormick I, Jonas JB, et al. Effective refractive error coverage in adults aged 50 years and older: estimates from population-based surveys in 61 countries. Lancet Glob Health. 2022;10:e1754–e1763.
Otte B, Woodward MA, Ehrlich JR, Stagg BC. Self-reported eyeglass use by US medicare beneficiaries aged 65 years or older. JAMA Ophthalmol. 2018;136:1047–50.
He M, Abdou A, Ellwein LB, Naidoo KS, Sapkota YD, Thulasiraj RD, et al. Age-related prevalence and met need for correctable and uncorrectable near vision impairment in a multi-country study. Ophthalmology. 2014;121:417–22.
Chan VF, MacKenzie GE, Kassalow J, Gudwin E, Congdon N. Impact of presbyopia and its correction in low- and middle-income countries. Asia Pac J Ophthalmol. 2018;7:370–4.
Han X, Ellwein LB, Guo X, Hu Y, Yan W, He M. Progression of near vision loss and incidence of near vision impairment in an adult Chinese population. Ophthalmology. 2017;124:734–42.
He M, Abdou A, Naidoo KS, Sapkota YD, Thulasiraj RD, Varma R, et al. Prevalence and correction of near vision impairment at seven sites in China, India, Nepal, Niger, South Africa, and the United States. Am J Ophthalmol. 2012;154:107–16.
Zebardast N, Friedman DS, Vitale S. The prevalence and demographic associations of presenting near-vision impairment among adults living in the United States. Am J Ophthalmol. 2017;174:134–44.
Jin G, Zou M, Liu C, Chen A, Sun Y, Young CA, et al. Burden of near vision loss in China: findings from the Global Burden of Disease Study 2019. Br J Ophthalmol. 2023;107:436–41.
Marmamula S, Narsaiah S, Shekhar K, Khanna RC. Presbyopia, spectacles use and spectacle correction coverage for near vision among cloth weaving communities in Prakasam district in South India. Ophthalmic Physiol Opt. 2013;33:597–603.
RamPrakash R, Lingam L. Why is women’s utilization of a publicly funded health insurance low?: a qualitative study in Tamil Nadu, India. BMC Public Health. 2021;21:350.
Sharma SK, Nambiar D, Sankar H, Joseph J, Surendran S, Benny G. Gender-specific inequalities in coverage of publicly funded health insurance schemes in Southern States of India: evidence from National Family Health Surveys. BMC Public Health. 2023;23:2414.
Chen TH, Chiu YH, Luh DL, Yen MF, Wu HM, Chen LS, et al. Community-based multiple screening model: design, implementation, and analysis of 42,387 participants. Cancer. 2004;100:1734–43.
Ferdinand DP, Nedunchezhian S, Ferdinand KC. Hypertension in African Americans: advances in community outreach and public health approaches. Prog Cardiovasc Dis. 2020;63:40–45.
Kaaya S, Eustache E, Lapidos-Salaiz I, Musisi S, Psaros C, Wissow L. Grand challenges: improving HIV treatment outcomes by integrating interventions for co-morbid mental illness. PLoS Med. 2013;10:e1001447.
Rahman A, Surkan PJ, Cayetano CE, Rwagatare P, Dickson KE. Grand challenges: integrating maternal mental health into maternal and child health programmes. PLoS Med. 2013;10:e1001442.
Author information
Authors and Affiliations
Contributions
TTG developed the concept for the manuscript, enrolment of participants, data gathering and drafting the manuscript, and conducted data analysis. XYM and XW critically verified the data obtained from the GBD database. RTC drafted and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gao, TT., Mu, XY., Wang, X. et al. The burden of near vision loss from 1990 to 2021, and projections until 2032–findings from the Global Burden of Disease Study 2021. Eye 40, 215–222 (2026). https://doi.org/10.1038/s41433-025-04134-0
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41433-025-04134-0
