
Abstract
Renalase, a novel flavoprotein that is mainly expressed in the kidney and heart, plays a crucial role in hypertension. Recent studies have shown that renalase is expressed at low levels in the serum of patients with heart failure, while the role of renalase and its mechanism in cardiac failure is unclear. Adult Sprague-Dawley (SD) rats were used to investigate the role and function of renalase in the pathological process of transverse aortic constriction (TAC)-induced heart failure. Renalase-human protein chip analysis showed that renalase was directly associated with P38 and extracellular signal-regulated protein kinase 1/2 (ERK1/2) signaling. We further used lentivirus-mediated RNA interference to study the role of renalase in the progression of pathological ventricular hypertrophy and found that renalase inhibition attenuated the noradrenaline-induced hypertrophic response in vitro or the pressure overload-induced hypertrophic response in vivo. Recombinant renalase protein significantly alleviated pressure overload-induced cardiac failure and was associated with P38 and ERK1/2 signaling. These findings demonstrate that renalase is a potential biomarker of hypertrophy and that exogenous recombinant renalase is a potential and novel drug for heart failure.
Similar content being viewed by others

Introduction
Heart failure is a very common cardiovascular disease worldwide and is the advanced stage of other cardiovascular diseases. One of most common risk factors for heart failure is hypertension. In China, a recent study reported that more than 320 million Chinese adults had hypertension [1,2,3]. Approximately 30–40% of these cases were complicated by left ventricular hypertrophy (LVH) [4], and those patients with LVH could become candidates for heart failure at the end stage of the disease. Therefore, controlling the development of LVH at the early stage and slowing the development of heart failure at the end stage are currently the most efficient treatment strategies for patients with hypertension [5]. Although an increasing number of medicines and techniques have been used to alleviate the pathological progression of heart failure [6], the pathophysiological mechanism is complex and has still not been completely elucidates. Novel targets or new medications also offer hope for patients with heart failure.
Renalase is a flavoprotein that is primarily expressed in the kidneys and heart and was first discovered in 2005 [7, 8]. Further research has shown that renalase degrades catecholamines and regulates blood pressure and cardiac function [9]. Many researchers have hypothesized that renalase is associated with cardiomyocyte energy metabolism because the molecular structure of renalase includes flavin adenine dinucleotideand amine oxidase [10]. An increasing number of studies have demonstrated that renalase is involved in multiple pathophysiological processes in the heart, including cardiac ischemic injury [11,12,13,14]. Consequently, our earlier study showed that recombinant renalase protected cardiomyocytes against ischemia and reperfusion injury induced by blocking the left anterior descending coronary artery in a rat model [15]. Recent studies have shown that renalase is markedly expressed in melanoma and pancreatic cancer cells and that renalase is a survival factor that promotes cancer cell growth and proliferation [16, 17]. Other studies have shown that renalase plays a key role in cardiac remodeling or coronary heart disease and might be a biomarker for heart failure [14, 18, 19]. However, whether and how renalase affects the pathological process of hypertrophy or heart failure is unclear.
Our preliminary experiments showed that renalase was highly expressed in hypertrophic cardiac tissue and reduced in the serum and cardiac tissue of model rats during heart failure; however, whether renalase is involved in the development of chronic pressure overload-induced cardiac hypertrophy and cardiac failure has not been examined to date. Additionally, whether exogenous recombinant renalase is a potential therapeutic treatment for heart failure is unclear. Therefore, our aims for the present study were as follows: to explore whether renalase expression was altered in the context of pressure overload-induced heart failure and to demonstrate how renalase participates in modulating the development of heart failure. Our study may provide a basic theory and target for improving cardiac hypertrophy and the early treatment of heart failure.
Materials and methods
Animals and heart failure model
For our experiments, we used Sprague-Dawley (SD) rats (10 weeks of age, male, ~220 g); all animals were according to the national standard at the animal experimental center, and we performed transverse aortic constriction (TAC) on rats in the operation group at 14 weeks of age. Our animal protocol was approved by the Animal Care and Use Committee of The Third Xiangya Hospital, Central South University.
TAC was used to establish the pressure overload-induced left ventricular hypertrophy and heart failure model. Rats in the operation group were anesthetized via an intraperitoneal injection of 10% chloral hydrate (3 ml/kg), and normal breathing was maintained by tracheal cannula (tidal volume = 2–3 ml/100 g; frequency = 60–80 times/minute; respiration ratio = 1:1). The chest was opened, the aorta was separated, and a silk suture was used to ligate the arterial segment between the truncus brachiocephalicus and aortic root. The constriction maintained ~70% of the original diameter of the aorta (note: less than 70% of the diameter easily leads to sudden cardiac arrest). Blood samples were collected by the medial canthal vein, separated by centrifugation (3000 rpm, 10 min) and then stored at –80 °C. General data were collected, including basic information (age, weight, heart rate, and blood pressure).
Echocardiography evaluation
All rats were examined by echocardiography at 4 weeks and 8 weeks after TAC before tissues were harvested. A 10S pediatric ultrasound system (Toshiba, Japan) was used in M-mode with a 10-MHz probe. All data were measured from the short axis of the LV at the basalis posterior. The echocardiography measurements were obtained from three beats and averaged. Some data reflect the extent of left ventricular hypertrophy and cardiac function, including left ventricular posterior wall thickness (LVPWT), left ventricular end diastolic diameter (LVDd), ejection fraction (EF), and left ventricular fraction shortening (FS).
A low-expression renalase gene model
A low-expression renalase gene model was established by lentivirus-mediated RNA interference as described in our previously published paper. The lentivirus titer was 5E + 9 TU/ml (GeneChem, Shanghai, China), the vector was GV118 (10.3 kb), and the oligonucleotide sequence was U6-MCS-Ubi-EGFP. The screened LV-RNLS-RNAi oligonucleotide (200 µl and 2E + 9 TU/ml) was injected into the pericardial cavity to inhibit renalase gene expression in heart tissue [20]. Another group of rats was treated with exogenous recombinant renalase (Proteintech, Wuhan, China) by subcutaneous injection (1.5 mg/kg, once a week from the 6th week to the 8th week after TAC) [15].
Renalase-human protein chip analysis
We used HuProt™ human protein chips to screen possible proteins that bound to renalase and examined potential targets to determine molecular mechanisms. These high-throughput screening chips were designed and produced by Wayen Biotechnologies (Shanghai, China). HuProtTM 20 K included 49,152 dots, exclude 3,374 negative dots and 1,536 positive dots and obtained 44,242 dots. The results represented 19,851 proteins, each protein had one repeat, and then GenePixTM Pro v6.0 analyzed the results.
H9C2 cell culture and treatment
H9C2 cells (Central Laboratory of the Third Xiangya Hospital) were cultured in DMEM (Invitrogen, Shanghai) containing 10% fetal bovine serum, HEPES (20 mmol/l), and penicillin-streptomycin (100 U/l). H9C2 cells were stimulated with norepinephrine (NE), and H9C2 cells were transfected with the designed and screened plasmids packaged with renalase gene interference sequences. The plasmid vector was GV102 (GeneChem, Shanghai, China), and the designed target sequence was CCCAGCAACTGGAAACCAT (details in Supplementary Tables).
Histological analysis and staining
Heart tissues were harvested at 4 weeks and 8 weeks after TAC for hematoxylin and eosin (HE) and Masson staining.
Quantitative real-time polymerase chain reaction (PCR) and western blotting
PCR and western blot analyses of cardiac tissue were performed in accordance with standard methods previously published in our earlier paper [21] (the gene primers used in this study are shown in the Supplementary Tables). Anti-renalase monoclonal antibodies were used as primary antibodies (ProTech, China). Anti-Erk, anti-p-p38, and anti-p-Erk primary antibodies were purchased from Cell Signaling Technology (CTS, China), and the anti-β-MHC primary antibody was purchased from Abcam (Guangzhou, China). Horseradish peroxidase (HRP)-labeled immunoglobulin G (IgG) (CW-Biotech, China) antibodies were used as secondary antibodies, and western blotting was performed to measure renalase protein expression in heart tissues.
Assessment of cell surface area
Phalloidin (Sigma, Shanghai, China) was used to stain the cytoskeleton after different treatments, and then ImageJ (v1.8.0) software was used to analyze the cell surface areas.
Statistical analysis
The data were analyzed with SPSS version 21.0 and are expressed as the mean ± SD. T-tests were used to compare means between two groups, and one-way analyses of variance (ANOVA) with S-N-K multiple comparison tests were used to compare multiple groups. If the data did not pass a normality test, we used the Kruskal-Wallis test with Dunn’s multiple comparisons test. In all cases, P < 0.05 was considered significant. All figures were made with GraphPad Prism version 6.01.
Results
Upregulated renalase levels in the serum and cardiac tissue of SD rats with left ventricular hypertrophy and significant downregulation of renalase in rats with heart failure
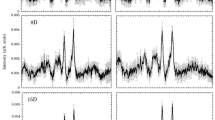
To determine whether renalase expression was gradually altered during the pathological progression of heart failure, we used TAC to establish models of LVH and heart failure (Fig. 1). SD rats developed left ventricular hypertrophy after transverse aortic constriction at ~4 weeks and then exhibited heart failure at 8 weeks. Our results showed that SD rats had significant heart failure at 8 weeks after TAC, and the EF apparently decreased (*P < 0.05 vs. sham control, n = 6). PWT increased over time\after TAC, and PWT significantly changed at 4 weeks after TAC (*P < 0.05 vs. sham control, n = 6). FS was decreased at 8 weeks after TAC (*P < 0.05 vs. v, n = 6). LVDd exhibited an adverse change (n = 6, *P < 0.05 vs. sham control). Enzyme-linked immunosorbent assay (ELISA) was used to analyze renalase levels in the serum of SD rats with LVH or heart failure; the highest level of renalase was measured at 4 weeks after TAC, and the lowest level was measured at 8 weeks after TAC (n = 6, **P < 0.01 vs. sham control). ELISA was used to analyze norepinephrine (NE) levels in the serum of SD rats with LVH or heart failure; serum levels of NE increased during the development of heart failure (n = 6, **P < 0.01 vs. sham control). Western blot analysis of renalase and β-MHC protein expression in the cardiac tissue of SD rats with LVH or heart failure showed that β-MHC protein expression gradually increased during the development of heart failure (n = 6, **P < 0.01 vs. preoperation), while the protein expression of renalase increased during the development of LVH (n = 6, **P < 0.01 vs. preoperation) and then decreased during the progression of heart failure (n = 6, **P < 0.01 vs. at 4 weeks after TAC).

SD rats have left ventricular hypertrophy at ~4 weeks after transverse aortic constriction and then exhibit heart failure at 8 weeks. A–C Echocardiography was used to evaluate the ejection fraction (EF %), left ventricular posterior wall thickness (PWT), fractional shortening (FS %), and left ventricular end diastolic diameter (LVDd) at different periods of heart failure in rats. D SD rats had significant heart failure at 8 weeks after TAC, and the EF apparently decreased (*P = 0.0426 vs. sham control, n = 6). E PWT increased with time after TAC, and PWT significantly changed at 4 weeks after TAC (*P < 0.05 vs. sham control, n = 6). F FS decreased at 8 weeks after TAC (*P = 0.0319 vs. v, n = 6). G LVDd had an adverse change (n = 6, *P < 0.05 vs. sham control). H ELISA analysis of renalase levels in the serum of SD rats with LVH or heart failure; the highest level of renalase was measured at 4 weeks after TAC, and the lowest level was measured at 8 weeks after TAC (n = 6, **P = 0.0087 vs. sham control). I ELISA analysis of norepinephrine (NE) levels in the serum of SD rats with LVH or heart failure. The serum level of NE increased during the development of heart failure (n = 6, **P = 0.0029 vs. sham control). J–K Western blot analysis of renalase and β-MHC protein expression in cardiac tissue in SD rats with LVH or heart failure. β-MHC protein gradually increased during the progression of heart failure (n = 6, **P = 0.0021 vs. preoperation), while the protein expression of renalase increased during the development of LVH (n = 6, **P = 0.0034 vs. preoperation) and then decreased during heart failure (n = 6, **P = 0.0057 vs. at 4 week after TAC s). LVH left ventricular hypertrophy, TAC transverse aortic constriction, β-MHC myosin heavy chain.
Renalase-human protein chip analysis shows that renalase plays a key role in cell growth and metabolism
We used human protein chips to further investigate the possible biological functions of renalase and the potential molecular mechanism and found that renalase may play a key role in the pathological process of heart failure. HuProtTM 20 K includes 49,152 dots, excludes 3374 negative dots and 1536 positive dots and then obtains 44,242 dots. This chip represents a total of 19,851 proteins. A total of 554 human proteins were screened, and then we used bioinformatics analysis to investigate the relationships between renalase and those proteins. Gene ontology analysis was used and included molecular function analysis, cellular component analysis, and biological process analysis. Finally, Kyoto Encyclopedia of Genes and Genomes (KEGG) was used to determine the biological function of renalase (Fig. 2).

Renalase-human protein chip analysis results show diverse biological functions. A Recombinant renalase protein was measured by WB and CBB staining. B–E Gene ontology analysis included molecular functions, cellular components, and biological processes. B Molecular function analysis showed the differential activities of proteins related to renalase; C cellular component analysis showed the functional location of renalase protein in the cell; and D biological process analysis showed that renalase protein participates in cellular metabolism. E We predicted the biological function of renalase by KEGG. F GenePixTM Pro v6.0 analyzed the chips and showed that some proteins directly bound with renalase, such as P38, Erk1/2, and mTORC1, which play key roles in the pathological process of LVH or heart failure.
Inhibition of renalase expression alleviates the noradrenaline-induced hypertrophic response by downregulating p-P38 and p-ERK1/2 expression in vitro
To explore the possible molecular mechanism of renalase, which participates in the process of hypertrophy in cardiomyocytes, were used RNA interference plasmids to inhibit renalase RNA expression during the cellular hypertrophy. Our results indicated that inhibiting renalase expression alleviated noradrenaline-induced hypertrophy in the in vitro cell model, and we found that p-P38 and p-ERK1/2 were significantly downregulated, as was renalase (Fig. 3).

Renalase (RNLS) regulates the noradrenaline (NE)-induced cardiomyocyte hypertrophic phenotype by downregulating p-P38 and p-ERK1/2 signaling in vitro. A, B Norepinephrine quickly induced cardiac cells to express renalase at a concentration of 1 µM, and the highest level of renalase occurred after NE treatment for 12 h. C, D Transfection plasmid information and inhibition efficiency. E Representative microscopic images of H9C2 cells infected with the screened plasmids, stimulated with NE (1 μM for 24 h), and stained with phalloidin and 4’,6-diamidino-2-phenylindole (DAPI, blue, nucleus; red, cytoskeleton; scale bar, 20 μm). F ImageJ software analysis of cell surface areas. Statistical analysis of the surface areas of H9C2 cells infected with interference or overexpression plasmids compared with negative control plasmids in response to NE (n = 20 cells per group; *P = 0.0359 vs. negative control plasmid; **P = 0.0072 vs. normal control). G Statistical analysis of p-P38 and p-ERK1/2 in H9C2 cells treated with NE for 24 h. H Representative western blot analysis of the phosphorylation levels of P38 and ERK1/2.
Inhibition of renalase suppresses cardiac hypertrophy by downregulating p-P38 and p-ERK1/2 expression in vivo
To further examine the role of renalase in hypertrophy, we designed and screened lentivirus-mediated RNA interference oligonucleotides of renalase genes and then established a cardiac-specific low-expression renalase model by pericardial cavity injection. This model was described in our previously published paper, and we reported the detailed methods and materials [20]. In this study, the inhibition of renalase by lentivirus-mediated shRNA obviously decreased TAC-induced left ventricular hypertrophy (Fig. 4).

Inhibition of the renalase gene by lentivirus-mediated shRNA decreased TAC-induced left ventricular hypertrophy. A We used the vector and sequences of the designed LV-Rnls-RNAis to target renalase genes. B Hematoxylin and eosin (H&E) staining (scale bar, 20 μm) of cardiac tissues. C ImageJ software analysis of the cross-sectional areas and TAC treatment-induced hypertrophy (n = 6, *P = 0.0307, vs. sham group), and the inhibition of renalase by lentivirus-mediated RNAi decreased the hypertrophic response (n = 6, *P = 0.0462, vs. LV-RNAi-control). D–G Echocardiographic evaluation of the hypertrophic rat model at 4 weeks after sham or transverse aortic constriction (TAC). PWT and LVDd significantly changed after the inhibition of renalase (n = 6, *P < 0.05, vs. LV-RNAi-control), while there was no difference in either EF or FS at 4 weeks after TAC with or without LV-RNAi injection (n = 6, P > 0.05, vs. LV-RNAi-control). PWT posterior wall thickness, LVDd left ventricular end diastolic diameter, EF ejection fraction, FS fractional shortening. The data are presented as the mean ± SD. H–I The serum level of renalase was inhibited by the injection of LV-RNAi (n = 6, *P = 0.033, vs. LV-RNAi-control), and norepinephrine was significantly increased after inhibiting renalase by LV-RNAi (n = 6, *P = 0.046, vs. LV-RNAi-control). J–K WB analysis of renalase protein levels in cardiac tissue after treatment with LV-RNAi showing that LV-Rnls-RNAi obviously inhibited renalase protein levels in a rat model of TAC (n = 6, *P < 0.05, vs. LV-RNAi-control). L–M Representative western blots and quantitative results showing the phosphorylation and total protein levels of P38, extracellular signal-regulated kinase 1/2 (ERK1/2), and β-myosin heavy chain (β-MHC) in the hearts of rats in the different groups (n = 6 rats per group; *P < 0.05 vs. control groups). Protein expression was quantified and normalized to glyceraldehyde 3-phosphate dehydrogenase (GAPDH).
Exogenous recombinant renalase inhibits cardiac fibrosis and significantly improves heart function in rats with heart failure in vivo
Exogenous recombinant renalase did not promote the development of LVH, as shown by analysis of the cross-sectional areas of the left ventricles; however, exogenous recombinant renalase significantly improved cardiac function by reducing cardiac fibrosis markers, such as collagen I and III (Fig. 5).

The effect of renalase on cardiac fibrosis and heart function. A Recombinant renalase protein (RRP) was injected subcutaneously into adult SD rats, and we found that the serum level of renalase gradually increased and was sustained for 96 h (1.5 mg/kg, each rat, n = 6). B ELISA analysis of the serum level of renalase in the different groups at 8 weeks after TAC. C ELISA analysis of the serum level of NE in the different groups at 8 weeks after TAC. NE levels significantly decreased after RRP treatment (n = 6, *P = 0.0391, vs. vehicle treatment). D Masson staining (scale bar, 20 μm) of cardiac tissues. Exogenous recombinant renalase decreased cardiac fibrosis morphology. E–H Echocardiographic evaluation of the rat model with heart failure at 8 weeks after TAC. PWT and LVDd showed no changes after RRP treatment (n = 6, P > 0.05, vs. vehicle treatment), while both EF and FS were significantly increased at 8 weeks after TAC with RRP treatment (n = 6, *P < 0.05, vs. control). PWT posterior wall thickness, LVDd left ventricular end diastolic diameter, EF ejection fraction, FS fractional shortening. I mRNA levels of hypertrophic and fibrotic markers in the hearts of different groups (n = 6 per group). Collagen I and collagen III obviously changed after RRP treatment (n = 6, *P < 0.05, vs. vehicle treatment).
Discussion
In the present study, we identified renalase as an important factor in cardiac hypertrophy and heart failure. The data demonstrated that renalase protein expression was significantly increased in hypertrophic cardiac tissue in rats, and there was a lack of renalase in the heart failure model. Inhibition of renalase by lentivirus-mediated low-expression RNA inhibited the hypertrophic response to TAC (transverse aortic constriction) in the rat model, whereas the level of renalase was significantly reduced in the context of heart failure, and recombinant renalase improved cardiac function and inhibited cardiac fibrosis in the heart failure model. These changes indicate that renalase may play a key role in the pathological process of LVH and pressure overload-induced heart failure. We consequently used human protein chips to further investigate the possible biological functions of renalase and found that renalase may play a key role in the pathological process of heart failure by regulating the P38 and ERK1/2 signaling pathways, and then those signals were verified in vitro and in vivo. Renalase-mediated functions were attributed to the inhibition of the P38 and ERK1/2 signaling axes. To our knowledge, this study provides the first evidence of an essential function of renalase in cardiac hypertrophy and heart failure, and recent studies have also reported that renalase is associated with adverse left atrial remodeling and disease burden in patients with atrial fibrillation [22, 23]. Therefore, renalase might be a potential therapeutic target for the pathophysiologic process of heart failure.
Renalase, a novel secreted flavoprotein with oxidoreductase activity, has been shown to degrade catecholamine and regulate blood pressure [7]. Researchers then reported that renalase was also highly expressed in cardiac tissue and regulated cardiac function in ischemia-induced heart failure in a mouse model [12]. We previously confirmed that renalase was involved in the regulation of blood pressure in spontaneously hypertensive rats [24]. Recent studies have shown that extracellular renalase signals through the plasma membrane calcium ATPase PMCA4b and activates the PI3K and MAPK pathways [25, 26]. Therefore, renalase has extracellular and intracellular functions that are dependent or independent of its enzymatic action [27]. In July 2016, researchers reported that renalase expression in a tumor was inversely correlated with disease-specific survival, suggesting a pathogenic role for renalase. Attenuation of renalase by a renalase-derived inhibitory peptide decreased melanoma cell survival, and anti-RNLS therapy blocked tumor growth in vivo in murine xenograft assays [16]. These studies suggest that renalase might have a key role in cell growth in pathogenic conditions, such as cardiac hypertrophy, and we identified the expression of renalase in hypertrophic rat hearts and serum. These results demonstrate that renalase expression is positively correlated with left ventricular hypertrophy and negatively correlated with heart failure.
In our study, we investigated the effects of renalase on myocardial hypertrophy in vitro and in vivo. We not only identified that inhibiting renalase by plasmid transfection ameliorated noradrenaline-induced H9C2 hypertrophy in vitro but also verified that downregulating the renalase gene in local cardiac tissue by lentivirus-mediated RNAi significantly alleviated TAC-induced cardiac hypertrophy in a rat model. After we confirmed the crucial role of renalase in hypertrophy in vivo and in vitro, further experiments were performed to investigate the molecular mechanism of renalase in the pathophysiological process of LVH and heart failure. Therefore, we propose that renalase alleviates the hypertrophic response by inhibiting P38 and ERK1/2, which are critical signals in cardiac hypertrophy, and our protein chip analysis also verified the relationship between renalase and those signals. During the progression from LVH to heart failure, renalase expression was significantly reduced according to decompensation. In our experiments, exogenous recombinant renalase directly affected heart failure in vivo. We first found that renalase had an additional therapeutic function in myocardial fibrosis by regulating collagen expression via P38 and ERK1/2 signaling. During the pathophysiological progression of LVH, many factors exert critical influences on myocardial cells, including neurohumoral factor-induced cell apoptosis or inflammatory reaction activation [28,29,30,31]. Renalase may be a biomarker to predict the development of hypertrophy.
In conclusion, our present work provides in vitro and in vivo evidence that the inhibition of renalase expression attenuates pressure overload-induced cardiac hypertrophy by regulating P38 and ERK1/2 signaling, and recombinant renalase protein might be a potential therapeutic medicine for controlling heart failure.
References
Lewington S, Lacey B, Clarke R, Guo Y, Kong XL, Yang L, et al. The burden of hypertension and associated risk for cardiovascular mortality in China. JAMA Intern Med. 2016;176:524–32.
Pitt B. Mark Nicholls speaks to Professor Bertram Pitt and his role as a pioneer in cardiology over the management of heart failure. Eur Heart J. 2020;41:1615–7.
Borlaug BA. Evaluation and management of heart failure with preserved ejection fraction. Nat Rev Cardiol. 2020;17:559–73.
Cuspidi C, Sala C, Negri F, Mancia G, Morganti A. Prevalence of left-ventricular hypertrophy in hypertension: an updated review of echocardiographic studies. J Hum Hypertens. 2012;26:343–9.
Shimizu I, Minamino T. Physiological and pathological cardiac hypertrophy. J Mol Cell Cardiol. 2016;97:245–62.
Bombelli M, Facchetti R, Carugo S, Madotto F, Arenare F, Quarti-Trevano F, et al. Left ventricular hypertrophy increases cardiovascular risk independently of in-office and out-of-office blood pressure values. J Hypertens. 2009;27:2458–64.
Xu J, Li G, Wang P, Velazquez H, Yao X, Li Y, et al. Renalase is a novel, soluble monoamine oxidase that regulates cardiac function and blood pressure. J Clin Invest. 2005;115:1275–80.
Luft FC. Renalase, a catecholamine-metabolizing hormone from the kidney. Cell Metab. 2005;1:358–60.
Li G, Xu J, Wang P, Velazquez H, Li Y, Wu Y, et al. Catecholamines regulate the activity, secretion, and synthesis of renalase. Circulation. 2008;117:1277–82.
Desir GV, Wang L, Peixoto AJ. Human renalase: a review of its biology, function, and implications for hypertension. J Am Soc Hypertens. 2012;6:417–26.
Desir GV. Regulation of blood pressure and cardiovascular function by renalase. Kidney Int. 2009;76:366–70.
Wu Y, Xu J, Velazquez H, Wang P, Li G, Liu D, et al. Renalase deficiency aggravates ischemic myocardial damage. Kidney Int. 2011;79:853–60.
Lee IT, Sheu WH. Serum renalase levels are predicted by brain-derived neurotrophic factor and associated with cardiovascular events and mortality after percutaneous coronary intervention. J Clin Med. 2018;7:437.
Safdar B, Guo X, Johnson C, D’Onofrio G, Dziura J, Sinusas AJ, et al. Elevated renalase levels in patients with acute coronary microvascular dysfunction - a possible biomarker for ischemia. Int J Cardiol. 2019;279:155–61.
Li X, Xie Z, Lin M, Huang R, Liang Z, Huang W, et al. Renalase protects the cardiomyocytes of Sprague-Dawley rats against ischemia and reperfusion injury by reducing myocardial cell necrosis and apoptosis. Kidney Blood Press Res. 2015;40:215–22.
Guo X, Hollander L, MacPherson D, Wang L, Velazquez H, Chang J, et al. Inhibition of renalase expression and signaling has antitumor activity in pancreatic cancer. Sci Rep. 2016;6:22996.
Hollander L, Guo X, Velazquez H, Chang J, Safirstein R, Kluger H, et al. Renalase expression by melanoma and tumor-associated macrophages promotes tumor growth through a STAT3-mediated mechanism. Cancer Res. 2016;76:3884–94.
Stojanovic D, Mitic V, Petrovic D, Stojanovic M, Ignjatovic A, Stefanovic N, et al. Association of plasma renalase and left ventricle mass index in heart failure patients stratified to the category of the ejection fraction: a pilot study. Dis Markers. 2019;2019:7265160.
Stojanovic D, Mitic V, Stojanovic M, Petrovic D, Ignjatovic A, Stefanovic N, et al. The partnership between renalase and ejection fraction as a risk factor for increased cardiac remodeling biomarkers in chronic heart failure patients. Curr Med Res Opin. 2020;36:909–19.
Li X, Lin M, Xie Z, Huang R, Chen AF, Jiang W. Establishing a low-expression renalase gene model in cardiac tissue of Sprague-Dawley rats. Herz. 2016;41:326–30.
Li X, Jiang W, Li L, Huang R, Yang Q, Yang Y, et al. Renalase gene polymorphism in patients with hypertension and concomitant coronary heart disease. Kidney Blood Press Res. 2014;39:9–16.
Wybraniec MT, Wieczorek J, Wozniak-Skowerska I, Hoffmann A, Nowak S, Cichon M, et al. Renalase is associated with adverse left atrial remodelling and disease burden in patients with atrial fibrillation undergoing pulmonary vein isolation. Kardiol Pol. 2018;76:1232–41.
Schlaich MP, Lambert GW, Eikelis N. Renalase - a potential biomarker for risk of atrial fibrillation? Kardiol pol. 2018;76:1201–2.
Jiang W, Tan L, Guo Y, Li X, Tang X, Yang K. Effect of renal denervation procedure on left ventricular hypertrophy of hypertensive rats and its mechanisms. Acta Cir Bras. 2012;27:815–20.
Wang L, Velazquez H, Chang J, Safirstein R, Desir GV. Identification of a receptor for extracellular renalase. Plos ONE. 2015;10:e122932.
Wang Y, Safirstein R, Velazquez H, Guo XJ, Hollander L, Chang J, et al. Extracellular renalase protects cells and organs by outside-in signalling. J Cell Mol Med. 2017;21:1260–5.
Hoag MR, Roman J, Beaupre BA, Silvaggi NR, Moran GR. Bacterial renalase: structure and kinetics of an enzyme with 2- and 6-Dihydro-beta-NAD(P) oxidase activity from pseudomonas phaseolicola. Biochemistry-US. 2015;54:3791–802.
Zhao L, Cheng G, Jin R, Afzal MR, Samanta A, Xuan YT, et al. Deletion of interleukin-6 attenuates pressure overload-induced left ventricular hypertrophy and dysfunction. Circ Res. 2016;118:1918–29.
Hunter CA, Jones SA. IL-6 as a keystone cytokine in health and disease. Nat Immunol. 2015;16:448–57.
Miao R, Lu Y, Xing X, Li Y, Huang Z, Zhong H, et al. Regulator of G-protein signaling 10 negatively regulates cardiac remodeling by blocking mitogen-activated protein kinase-extracellular signal-regulated protein kinase 1/2 signaling. Hypertension. 2016;67:86–98.
Verma SK, Krishnamurthy P, Barefield D, Singh N, Gupta R, Lambers E, et al. Interleukin-10 treatment attenuates pressure overload-induced hypertrophic remodeling and improves heart function via signal transducers and activators of transcription 3-dependent inhibition of nuclear factor-kappaB. Circulation. 2012;126:418–29.
Acknowledgements
The study was supported by the National Natural Science Foundation of China (NSFC) Projects (Nos. 81800271 and 81670335) and the Natural Science Foundation of Hunan Province (No. 2019JJ50920).
Author information
Authors and Affiliations
Contributions
XL and WJ provided the general outline of the manuscript and designed the research study, XL and YW performed all experiments and wrote the manuscript, and CQ and YY verified and analyzed the raw data after the experiments. ZL provided assistance with our animal experiments.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Wu, Y., Quan, C., Yang, Y. et al. Renalase improves pressure overload-induced heart failure in rats by regulating extracellular signal-regulated protein kinase 1/2 signaling. Hypertens Res 44, 481–488 (2021). https://doi.org/10.1038/s41440-020-00599-6
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-020-00599-6
Keywords
This article is cited by
-
Renal Denervation Improves Myocardial Mitochondrial Dysfunction and Myocardial Fibrosis by Inhibiting the NE/KLF15/renalase Pathway
Molecular Neurobiology (2025)
-
Bone marrow mesenchymal stem cells-derived exosomal lncRNA GAS5 mitigates heart failure by inhibiting UL3/Hippo pathway-mediated ferroptosis
European Journal of Medical Research (2024)
-
Denervation or stimulation? Role of sympatho-vagal imbalance in HFpEF with hypertension
Hypertension Research (2023)
-
Update on Hypertension Research in 2021
Hypertension Research (2022)
