
Abstract
Heat waves are associated with increased fatalities from adverse cardiovascular events attributed to the negative effects of heat on cardiac function. However, scientific understanding of acute cardiac adjustments to heat has come primarily from laboratory experiments employing insulated and encapsulated heating modalities, most commonly water-perfused suits. We evaluated whether findings from those studies reflect cardiac responses during more natural exposures to hot ambient conditions simulated in climate-controlled chambers by synthesizing the findings from over 400 laboratory-based heat exposure studies (6858 participant-exposures) published between 1961–2024. Among all included studies, median (interquartile range) elevations in core temperature and heart rate from baseline to end-exposure were 0.9 (0.5–1.3)°C and 27 (15–40) beats/min. Multilevel mixed-effects meta-analyses revealed exacerbated elevations in heart rate, cardiac output, and rate pressure product (estimate of cardiac workload) and blunted falls in systolic pressure in participants heated via encapsulated modalities. Leveraging the large dataset, we also provide empirical estimates of body temperature and cardiovascular responses to a wide range of conditions experienced during heat waves. With rising global temperatures, ecologically-minded physiological research is needed to improve understanding of the effects of heat stress on cardiac responses and further the development of robust climate health models and evidence-based heat-health guidance.
Similar content being viewed by others

Introduction
Hot weather and heat waves are associated with increased fatalities from adverse cardiovascular events1,2,3. The putative pathophysiology has been summarized in numerous narrative reviews4,5,6,7,8,9. Briefly, rising core and skin temperatures elicit reflex and locally mediated vasodilation of the cutaneous vasculature to facilitate transfer of blood-borne heat to the skin where it can be dissipated to the environment10. The resultant fall in vascular resistance necessitates an elevation in cardiac output to maintain arterial pressures and systemic blood flow11. These adjustments increase myocardial strain12,13,14,15 which, when combined with heat-induced dehydration and hypercoagulability16,17, could elevate the risk of acute coronary events, particularly in persons already vulnerable to such events (e.g., older adults)4,5,6,7,8,9.
Laboratory-based heat exposure studies have played a central role in delineating the cardiovascular adjustments to acute heat stress11. The limits of those adjustments were perhaps first shown in a seminal study by Rowell et al.18, in which cardiac output rose 5–7 L/min due to a 60–80 beats/min increase in heart rate in four young men heated to the limits of thermal tolerance using an encapsulated, tube-lined garment perfused with ~48–50 °C water. Water-perfused suits have since become a mainstay of laboratory research, primarily because they allow for rapid and precise control of body temperature11, which facilitates comparisons between different populations (e.g., young and older adults)15,19,20 and physiological states (e.g., central hypovolemia and normovolemia)12,13.
The extreme cardiac responses seen in studies employing water-perfused suits18,19 are often cited in translational reviews describing the impacts of hot weather and heat waves on the heart5,6,7,8,9. However, the encapsulated and conduction-mediated design of this heating modality impedes heat dissipation, meaning that extreme hyperthermia can develop rapidly and skin temperatures often reach supra-physiological levels (≥40 °C)18,19. Consequently, it has been suggested that perfusion suits (and other encapsulated modalities) are suboptimal for translational research aimed at quantifying the cardiac strain experienced during hot weather and heat waves6,11. To address this limitation, a growing number of studies have exposed participants to hot weather simulated in specialized climate-controlled chambers21,22,23,24,25,26,27,28, which are thought to provide a more ecologically relevant exposure model6,11. However, such studies are highly resource-intensive, which makes quantifying cardiac responses to a wide range of ambient conditions challenging.
With rising global temperatures, physiological research will play an increasingly important role in the development of robust climate-health models29,30,31 and evidence-based guidance for protecting heat-vulnerable persons5,7,32,33,34. Given the pervasive use of water-perfused suits, we were concerned that the substantial body of evidence on the physiological burden of heat has, in its current form, limited use in supporting these efforts. We therefore conducted this systematic review and meta-analysis to synthesize data from laboratory-based studies evaluating the cardiac responses to acute heat stress. Our primary objective was to compare the cardiac adjustments reported in studies employing water-perfused suits and other encapsulated and/or extreme modalities (hot water immersion and sauna) with those experienced during resting exposure to high ambient temperatures in climate-controlled chambers (supplemental Table S2 overviews common modalities). The time- and resource-intensive nature of thermophysiological research and the required controls (e.g., of skin temperature and hemodynamic responses) rendered approaching this problem experimentally intractable. Conversely, a large-scale meta-analysis permitted evaluations of between-modality differences, while adjusting for relevant confounders and non-heat-related mediators of the cardiac response to different heating modalities. Leveraging the large and unique dataset also allowed us to provide empirical estimates of body temperature and cardiovascular responses in a wide range of conditions experienced during hot weather and heat waves.
Results
Flow of studies through the review and report characteristics
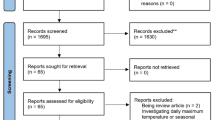
After abstract and full text screening and data extraction (Fig. 1), 438 articles met the eligibility criteria. Of these, 28 reported secondary analyses of other included studies. These were omitted from primary analyses along with 10 studies employing only radiant or conductive heating modalities or heating participants in the standing posture or in high clothing insulation35,36,37,38,39,40,41,42,43,44. Effect estimates from an additional 2 studies meeting these criteria were removed from the primary analysis, but those studies also reported data for eligible conditions45,46. The records supplement summarizes studies that could not be classified in full-text screening, eligible studies for which data could not be sourced, reports of secondary analyses, and original study reports omitted from primary analyses.

A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart showing the flow of studies through the review456. *Of 438 eligible reports, 28 reported secondary analyses of data already included in the review. These studies were not included in analyses. Data from 10 studies that only heated participants via radiant (e.g., infrared or radiofrequency) or conductive (e.g., heated blankets) heating modalities, in the standing posture, or in high clothing insulation (e.g., nuclear, biological, chemical suit) were also omitted from the primary analysis but included in sensitivity analyses.
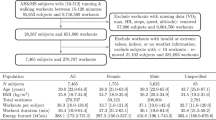
Characteristics of the 400 reports included in primary analyses are summarized in Table 112,13,16,18,21,22,23,24,25,26,27,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256,257,258,259,260,261,262,263,264,265,266,267,268,269,270,271,272,273,274,275,276,277,278,279,280,281,282,283,284,285,286,287,288,289,290,291,292,293,294,295,296,297,298,299,300,301,302,303,304,305,306,307,308,309,310,311,312,313,314,315,316,317,318,319,320,321,322,323,324,325,326,327,328,329,330,331,332,333,334,335,336,337,338,339,340,341,342,343,344,345,346,347,348,349,350,351,352,353,354,355,356,357,358,359,360,361,362,363,364,365,366,367,368,369,370,371,372,373,374,375,376,377,378,379,380,381,382,383,384,385,386,387,388,389,390,391,392,393,394,395,396,397,398,399,400,401,402,403,404,405,406,407,408,409,410,411,412,413,414,415,416,417,418,419,420,421,422,423,424,425,426,427,428,429,430,431,432,433. These studies contributed a total of 586 effect estimates of the heat-induced increase in heart rate, representing 6858 participant-heat exposures, or approximately 8526 person-hours (~1 person-year). Most of the reports originated from laboratories in North America, Europe and Japan and were published with increasing frequency starting in 1961 through to 2024 (Fig. 2).

The size of the bubbles in the top panel indicates the number of studies from each location. The color shows the geographical density, which considers both the number of studies from each location and their proximity to other study locations. The world map was generated using the opensource R package rnaturalearth491.
Included studies received a median 5 (Interquartile range: 4–5) “yes” answers on the 12 questions of the National Heart, Lung and Blood Institute Quality Tool for Before-After Studies434, though no marked differences between heating modalities were observed (Figure S24). For studies including a control trial, we also evaluated risk of bias using the Cochrane Risk of Bias Tool for Randomized Trials435. A summary is provided in Figure S25.
Effect of heating modality on cardiac responses
Heart rate (primary outcome)
Comparisons of heart rate responses between heating modalities are shown in Fig. 3. A model including a heating modality by core temperature change interaction provided the most parsimonious fit. Relative to studies that heated participants via passive exposure to hot ambient conditions in a climate chamber, the overall pattern of response was statistically significantly different in studies employing water-perfused suits (P < 0.001), water immersion (P = 0.001), and saunas (P = 0.004). Heart rate increased, on average, 26 [95% CI: 22, 29] beats/min per 1 °C rise in core temperature in the climate chamber studies. Heat-induced increases in heart rate were exacerbated in perfusion suit studies at low levels of hyperthermia (intercept difference: 7 [4, 11] beats/min; P < 0.001), though the slope of the relation between core temperature and heart rate was not statistically different between these modalities (slope difference: −3 [−7, 1] beats/min/°C; P = 0.192). At low core temperatures, heart rate was also elevated to a greater extent in water immersion (intercept difference: 8 [4, 12] beats/min; P = 0.001) and sauna studies (24 [10, 37] beats/min; P < 0.001). For these modalities, however, elevations in heart rate were blunted by 8 [3, 13], and 10 [2, 18] beats/min/°C, respectively, compared to studies performed in a climate chamber (P ≤ 0.012).

Figure shows the model-predicted relation between the change in heart rate and core temperature in studies heating participants via a climate chamber (grey, reference), water-perfused suit (red, top), water immersion (aqua, middle), and sauna (purple, bottom). Models are also adjusted for the core temperature measurement technique. Model predictions (left) are presented as means (lines) and 95% confidence intervals (shaded ribbons). The latter were produced via a sandwich estimator with small-sample correction. Analyses were also adjusted for the method used to measure core temperature. Model diagnostics are provided in supplemental Figures S27–S30 (pp 71–74). Included covariates explained a statistically significant portion of variance across included studies (omnibus test of covariates: two-sided P < 0.001). However, considerable residual heterogeneity was still observed (QE test: two-sided P < 0.001), with 93.5 [92.5, 94.4]% of total variance not explained by sampling variance (overall I2; 57.1 [50.1, 63.1]% between-study I2 and 36.4 [31.3, 41.9]% within-study I2). Model estimates and P-values (reported in the main text) were not adjusted for multiple comparisons. Individual effect estimates (right) are sized according to their weight in the meta-analytic model. The marginal distribution of individual effect estimates (unweighted) for each heating modality is depicted on the right side of the panel. The effect estimate for the seminal study by Rowell et al.18 is also highlighted, which was among the first to assess the physiological limits of cardiac responses to heat exposure and is also commonly cited in translational reviews describing heat’s effects on the heart.
Although differences in heating modality, baseline-to-end heating core temperature change, and the core temperature measurement technique explained a statistically significant portion of variance across included studies (omnibus test of covariates: P < 0.001), considerable residual heterogeneity was still observed (QE test: P < 0.001). Indeed, 93.5 [92.5, 94.4]% of the total variance was not explained by sampling variance (overall I2). Of total heterogeneity, 61% was attributable to differences between studies (57.1 [50.1, 63.1]% between-study I2), while the remaining 39% stemmed from within-study differences in extracted effect estimates (36.4 [31.3, 41.9]% within-study I2).
While adjustment for non-heat-related mediators (posture and clothing insulation), and sample demographics potentially confounding or altering cardiac responses to heating (age, sex, body mass index, climate zone) improved model fit (likelihood ratio test: P ≤ 0.041), modality model coefficients were comparable to the primary analysis (Figure S31). By contrast, when end-exposure mean skin temperature was included (likelihood ratio test: P ≤ 0.001) between-modality differences were no longer statistically significant (Figure S31). Among the additional covariates included, heart rate increased 2 [1, 3] beats/min per 1 °C increase in mean skin temperature (P < 0.001). Both posture (−4 [−6, −1] beats/min in supine vs. seated; P = 0.003) and sample mean age (−2 [−3, −2] beats/min per decade; P < 0.001) had small but statistically significant effects on heart rate (Table S18).
In sensitivity analyses (Table S19–S28, Figure S32), interpretations of the primary analysis were not markedly altered when studies omitted from the primary analysis were included, a laboratory identifier was incorporated as a random effect, or we varied the within-study correlation modeled in robust variance estimation. Findings were also robust to removal of potentially influential effect estimates, modeling non-linear associations between core temperature and heart rate, restricting suit and immersion studies to those employing full body coverage, and variation in measurement timing for heart rate, study quality, and date of publication. By contrast, between-modality differences in heart-rate responses were blunted when core temperature was replaced with estimated mean body temperature. Finally, analyses of the 51 studies including a control arm were similar when data were analyzed for the heat stress arm only (as in the primary analysis) and as the difference in heart rate responses between the heat and control arms. That said, relations between heating modalities were altered considerably in these analyses compared to primary analysis of the 400 included studies.
Cardiac output, systolic blood pressure, rate pressure product (secondary outcomes)
Cardiac output, systolic pressure, and rate pressure product in the climate chamber and perfusion suit studies are shown in Fig. 4. At any given increase in core temperature, cardiac output was elevated an average of 1.0 [0.4, 1.6] L/min in the perfusion suit studies (P = 0.003). Systolic pressure changed by −8 [−15, 0] and 2 [−2, 7] mmHg per 1 °C rise in core temperature in the climate chamber and perfusion suit studies, respectively. While those within-modality associations between systolic pressure and core temperature were not statistically significant (P ≥ 0.054), the between-modality difference in slopes was (slope difference: 10 [1, 18] mmHg/°C, P = 0.025). Heat-induced increases in rate pressure product were exacerbated 1841 [32, 3650] mmHg·beats/min/°C in the suit studies (P = 0.046).

Figure shows the model-predicted relations of the change in cardiac output (top; 79 studies, 114 effect estimates), systolic blood pressure (middle; 212 studies, 337 effect estimates), and rate pressure product (bottom; 205 studies, 303 effect estimates) as a function of the change in core temperature from baseline to end-heating in studies employing a climate chamber (gray) or perfusion suit (red) to induce heat stress. Model predictions (left) are presented as means (lines) and robust 95% confidence intervals. Analyses were also adjusted for the method used to measure core temperature. Model estimates and P-values (reported in the main text) were not adjusted for multiple comparisons. Data for hot water immersion and sauna studies are shown in supplemental Figures S33-S35 (pp 89–90), respectively. Model diagnostics are provided in supplemental Figures S35-S46 (pp 92−103). Model estimates and P-values (reported in the main text) were not adjusted for multiple comparisons. Individual effect estimates (right) are sized according to their weight in the meta-analytic model. The marginal distribution of individual effect estimates (unweighted) for each outcome modality is depicted on the right side of the panel. The effect estimate for the seminal study by Rowell et al.18 is also highlighted, which was among the first to assess the physiological limits of cardiac responses to heat exposure and is also commonly cited in translational reviews describing heat’s effects on the heart.
Secondary outcome model comparisons for hot water immersion and sauna studies are summarized in Figures S33-S34. Cardiac output was elevated, on average, 0.9 [0.2, 1.6] L/min in the immersion studies (P = 0.020), whereas reductions in systolic pressure were blunted (slope difference vs. chamber: −11 [−20, −2] mmHg/°C, P = 0.016). Despite a statistically significant overall response pattern for rate pressure product (P = 0.046), model intercept and slope coefficients were not different between modalities (P ≥ 0.145). For studies performed in a sauna, no differences in cardiac output were seen relative to the chamber studies (P = 0.562), though only 2 sauna studies reported this secondary outcome. By contrast, associations between core temperature and systolic pressure were significantly different between climate chamber and sauna studies (P = 0.001) such that systolic pressure fell 8 [0, 15] mmHg/°C in the chamber (P = 0.054) but rose 16 [8, 24] mmHg/°C in the sauna (P = 0.001; slope difference: 16 [8, 24] mmHg/°C, P = 0.001). While the overall rate pressure product response was significantly different between climate chamber and sauna studies (P = 0.001), the individual model intercept and slope coefficients were not (P ≥ 0.083).
Statistically significant residual heterogeneity was detected for all secondary cardiac outcomes (P < 0.001). The overall I2 was 92.7 [89.6, 95.0]% for cardiac output (66 [46.9, 77.0]% and 26.7 [16.7, 41.2]% between- and within-study, respectively), 92.9 [91.4, 94.3]% for systolic pressure (76.2 [70.6, 80.8]% and 16.8 [12.1, 22.8]%), and 94.0 [92.7, 95.1]% for rate pressure product (62.1 [53.4, 69.3]% and 31.9 [25.5, 39.2]%).
In sensitivity analyses, between-modality differences in cardiac output were not markedly altered when analysis was adjusted for the measurement methods employed (Table S30). That said, the method used to measure cardiac output was found to have strong impacts on model outputs (P < 0.001). Compared with more direct and invasive methods (e.g., direct Fick, thermodilution), the reported increase in cardiac output for a given rise in core temperature was reduced 1.2 [0.2, 2.2] L/min with imaging techniques (e.g., echocardiogram, magnetic resonance imaging; P = 0.026), 2.1 [1.3, 3.0] L/min with rebreathing methods (e.g., Innocor®; P < 0.001), and 1.8 [0.9, 2.6] L/min with indirect estimations (e.g., Modelflow®; P = 0.001). Like cardiac output, between-modality differences in the heat-induced change in systolic pressure were not altered when the measurement method was considered in analysis (Table S31). Again, however, the measurement method had strong influences on observed responses (P < 0.001). Relative to measurements made at the brachial artery (e.g., auscultation, oscillometry), systolic pressure was 16 [11, 22] and 7 [4, 10] mmHg/°C lower in studies employing an intra-arterial pressure transducer (P = 0.002) and indirect methods (P < 0.001), respectively. Systolic pressure (Table S32) and rate pressure product responses (Table S33) were no longer statistically significantly different between climate chamber and hot water immersion studies when core temperature was modeled using a spline (P ≥ 0.186); comparisons for the other two modalities remained statistically significant when a non-linear response function was modelled (P ≤ 0.022).
Body temperature and cardiac responses to high ambient temperatures
Associations between ambient heat index and 103 effect estimates for the heat-induced rise in core temperature and heart rate from 68 climate chamber studies are shown in Fig. 5 (1433 participant-exposures, approximately 3519 person-hours). Elevations in thermal and cardiac strain were exacerbated with increasing heat index, particularly at high levels of ambient heat stress (P ≤ 0.001). Heat-induced rises in core temperature also increased with sample age (0.05 [0.02, 0.07]°C/decade, P = 0.001) and the duration of heat exposure (0.05 [0.01, 0.10]°C/h, P = 0.027).

Figure shows the model-predicted relation between the change in core temperature (top, red) and heart rate (bottom, purple) with increasing heat index in studies exposing participants to ambient heat stress in a climate chamber (k = 68 studies, n = 103 effect estimates). Model predictions are presented as means (lines) and robust 95% confidence intervals (shaded ribbons). Heat index was modeled via a restricted cubic (natural) spline. Predictions for a model in which heat index was included as a linear term are also shown (dark grey dashed lines). Models were adjusted for sample mean age and the duration of heat stress. Model outputs are shown for a hypothetical study with a sample mean age of 27 years and 100 min of heat exposure (based on the sample size-weighted medians of the analyzed studies). Model diagnostics are provided in supplemental Figures S51–S66 (pp 112–127). Model estimates and P-values (reported in the main text) were not adjusted for multiple comparisons. Individual effect estimates (grey bubbles) are sized according to their weight in the meta-analytic model. The marginal distribution of the individual effect estimates (unweighted) is depicted on the right side of the panel.
For the secondary outcomes (Table S34), linear associations between heat index and cardiac output and systolic blood pressure were not statistically significant (P ≥ 0.193). For the latter, however, we observed significant effects of age and duration. Systolic pressure was reduced 1 [1, 2] mmHg per decade increase in age (P < 0.001) and 1 [0, 1] mmHg per hour of exposure (P = 0.021). Rate pressure product was elevated 257 [45, 469] mmHg·beats/min/5 °C heat index (P = 0.021) but not influenced by age or heating duration (P ≥ 0.236).
Discussion
We synthesized the findings of over 400 laboratory-based studies to compare heat-induced changes in heart rate, cardiac output, systolic pressure, and rate pressure product between studies using encapsulated and extreme heating modalities and those exposing participants to hot ambient conditions in a climate-controlled chamber. The employed modality had marked effects on cardiac responses. Of key importance, water-perfused suits, the most common passive heating modality in thermophysiological research, were associated with exacerbated cardiac responses compared to resting exposure in climate chambers. While perfusion suits play an integral role in mechanistic investigations, our findings suggest that they are less useful for quantifying the cardiac effects of more natural exposures. Ecologically-minded studies simulating or conducted in real-world settings are needed to improve scientific understanding of the cardiac impacts of hot weather and support the development of robust climate-health models. As a step toward this goal, we provide empirical quantifications of the acute thermal and cardiac strain experienced in conditions reflective of deadly heat waves.
Following foundational work by Rowell et al.18,357,436, water-perfused suits quickly became the most common heating modality in research evaluating the cardiovascular adjustments supporting thermoregulation and homeostasis during acute heat stress11. In addition to their accessibility, their popularity is owed to their encapsulated design, which, when combined with the high thermal conductivity of water perfused in near-direct contact with the skin, allows for precise control of body temperature. While these features have clear benefits for mechanistic research (Table S2), we questioned whether perfusion suits provide a suitable model for evaluating the cardiovascular consequences of more natural heat exposures like those occurring during hot weather and heat waves6. To address this knowledge gap, we leveraged data from over 400 studies conducted over 60 years to evaluate how cardiac responses were modified by the employed heating modality. As anticipated, we found exacerbated elevations in heart rate, cardiac output, and rate pressure product along with blunted reductions in systolic pressure in studies using perfusion suits compared to those exposing participants to hot conditions in climate-controlled chambers (Figs. 2–4).
These findings have important implications for translational efforts directed at linking cardiovascular adjustments to acute environmental heat stress11 with the elevated risk of cardiovascular events seen during heat waves1,2. Discussions in this area have focused on the profound cardiovascular strain observed in studies using water-perfused suits4,5,6,7,8,9, most commonly the early work by Rowell et al.18 which showed increases in cardiac output of 5-7 L/min. Our analyses, however, suggest that rises in cardiac output do not surpass 3 L/min when participants are heated with a climate chamber. In fact, only 1 in 14 effect estimates of the heat-induced elevation in cardiac output in the chamber studies exceeded 2.0 L/min (Fig. 4)26,27,70,140,157,164,226,229,244,284,346,392,405 and those data were collected under extreme conditions (42 °C, 70% relative humidity)70. Further, despite comparable heart rate responses (Fig. 3), systolic pressure and rate pressure product were elevated >10 mmHg and >1800 mmHg·beats/min in perfusion suits relative to chamber studies at core temperature elevations >1.0 °C (Fig. 4), differences that, on average, exceeded previously suggested thresholds for clinical significance21. These findings highlight that while perfusion suits have played a central role in developing mechanistic understanding of the physiological adjustments to extreme heat11, they have limited utility for quantifying the cardiovascular burden of hot weather and heat waves.
Extreme increases in skin temperature are the most likely explanation for the exacerbated cardiac strain seen with perfusion suits. In our primary analyses, we normalized cardiac responses to the rise in core temperature, the most relevant body temperature when discussing the clinical implications of heat4,5,6,7,8,9. However, cardiovascular adjustments are also influenced by skin temperatures through autonomic- and locally-mediated mechanisms acting to facilitate blood redistribution from the central to peripheral circulation to aid in heat dissipation378,437,438. Since perfusion suits heat participants by passing hot water over the skin surface, cutaneous heat gain is substantial6,11. As a result, skin temperatures often reach levels considerably higher than those seen during exposure to hot conditions where the skin can readily participate in heat exchange (Figure S83). Our secondary analyses clearly demonstrate the importance of skin temperature. While correcting for posture, worn clothing, and participant demographics had little impact on heart rate differences between heating modalities, adjusting for skin temperature nullified between-modality differences (Figure S31).
Some translational reports have acknowledged skin temperature’s role in cardiovascular adjustments to heat. For example, in their review on heat waves and cardiovascular health, Kenney et al.9 cite the >40 °C skin temperatures achieved in the work by Rowell et al.18, as the key mechanism underpinning the observed doubling of cardiac output. However, skin temperatures of this magnitude are unlikely to develop outside of the laboratory. In conditions experienced in most hot weather and heat waves, evaporation of sweat ensures continual skin-environment heat transfer in unencapsulated persons (e.g., wearing summer clothing), limiting potential rises in skin temperature. This can be seen in the modality-specific distributions of average end-exposure skin temperatures. Over half of the analyzed perfusion suit studies reported skin temperatures exceeding 38.0 °C compared to less than 15% of the climate chamber studies (Figure S84). While there were some examples of skin temperatures in a climate chamber approaching those seen in water-perfused suits, they were measured in wet-bulb temperatures of 36–39 °C (heat index 80–96 °C)67,166,377. In these conditions, thermoregulation is impossible30. Thus, even if modality-related differences in skin temperature are accounted for, the marked whole-body hyperthermia induced by perfusion suits severely limit their generalizability to naturally occurring hot weather.
Our broad inclusion criteria also allowed us to explore differences in cardiac responses between climate chambers and other extreme heating modalities (Table S2). Compared to resting exposure in a climate chamber, heat-induced elevations in heart rate were blunted with water immersion (Fig. 3), whereas cardiac output was elevated, particularly at lower increases in core temperature (Figure S34; differences in systolic pressure and rate pressure product were not statistically significant when non-linear responses were considered, Tables S32–S33). Given the apparently similar body temperature distributions between the two modalities (Figure S83), elevated cardiac output in the immersion studies is likely related to the hydrostatic effects of water immersion, which promote blood displacement to the central circulation, supporting cardiac filling pressure439, increasing stroke volume for a given heart rate440,441.
We also found that at small increases in core temperature, average heart rates were elevated considerably in studies heating participants in a sauna relative to those employing climate chambers (Fig. 3). The high ambient temperatures and/or humidities generated by saunas are a likely explanation for these findings (Figure S5), as even very short exposures (~15 min) can cause highly elevated skin temperatures (Figure S83). Interestingly, however, changes in systolic pressure followed opposing response patterns, increasing with core temperature in the sauna studies but falling in climate chamber studies (Figure S34). It could be that heat-induced reductions in arterial pressure are established over durations longer than those typical of sauna studies. Another possibility is that studies performed in climate chambers are more likely to enroll older adults (Figure S22), who, on average, experience greater reductions in systolic pressure during heat exposure (Table S34). While both explanations are consistent with our data (Figure S85), further investigation is required to establish their validity. Underpinning mechanism(s) notwithstanding, the disparate findings between relatively similar heating modalities, both involving resting exposure to hot conditions, further underscores that cardiac responses to heat stress are complex and are often not readily generalizable across populations and contexts.
With the planet warming rapidly, there is growing demand for climate-health models predicting how changes in climate systems affect the health of individuals29,30,31 as well as for evidence-based heat-mitigation strategies for protecting at-risk groups5,7,32,33,34. Central to these efforts is a need for robust physiological data describing how environmental conditions (e.g., air temperature, humidity, air flow, solar radiation) and other factors (e.g., health conditions, socioeconomic status, physical activity) influence body temperature regulation, cardiovascular function, and susceptibility to adverse health events. However, physiological inputs for recently proposed models have generally been based on select studies, often with few participants exposed to conditions unreflective of hot weather. This severely limits their utility, as model inferences can be highly sensitive to the methods used to derive key inputs33. It is therefore our view that a more systematic approach synthesizing large amounts of physiological data is needed to better quantify relations between environmental factors, personal characteristics, and physiological outcomes. Such an approach would also benefit rational physiological models (e.g., the human energy/heat balance models described in references31,33) in deriving key inputs and defining their uncertainty for use in sensitivity analyses.
As a step toward this goal, we quantified core temperature and cardiac responses across a wide range of ambient conditions based on data collected from over 1400 participant-heat exposures in climate-controlled chambers. These analyses highlight that considerable hyperthermia and cardiovascular strain can be experienced during exposure to heat wave conditions. As an illustrative example, Fig. 6 presents model estimates for hypothetical groups of young and older adults resting for 2 h in peak conditions measured during recent extreme heat waves. During even a short and sedentary exposure, our model predicts that resting core temperature can exceed 38.0 °C, commonly recommended as the safe upper limit in occupational contexts442, while heart rates can surpass 100 beats/min and blood pressure can be reduced by as much as 10 mmHg, on average, in older adults (though the 95% confidence intervals are also consistent with group mean systolic blood pressures as low as ~95 mmHg). The contribution of such reductions in blood pressure to heat-related cardiovascular mortality and morbidity is an important area for future exploration. Translational discussions on the mechanisms underpinning increased cardiac risk during heat exposure tend to focus on tachycardia-induced elevations in cardiac strain4,5,6,7,8,9. However, acute hypotension may precipitate end-organ malperfusion, leading to myocardial infarction and ischemic strokes443,444,445, the risks for both of which are elevated during hot weather1,446.

Figure shows model predictions (points) and robust 95% confidence intervals (error bars) for hypothetical groups (studies) of young (mean age: 25 years; sample weighted median below 65 years) and older adults (mean age: 70 years; sample weighted median above 65 years) resting for 2 h in peak conditions measured in recent heat waves in British Columbia, Canada (2021, gray)493, Bangkok, Thailand (2023, aqua)494, Asaluyeh, Iran (2022, purple)495, and Sikkim, India (2022, blue)496,497. Predictions are presented as means (points) and robust 95% confidence intervals (error bars) produced by adding the estimated change in each variable from the models presented in Fig. 5 (core temperature and heart rate, k = 68 studies, n = 103 effect estimates) and supplemental Table S34 (systolic pressure; k = 34 studies, n = 55 effect estimates) to the sample-weighted model median baseline values (grey horizontal lines).
Though somewhat crude, ours are among the first empirical estimates of heat strain to systematically consider the breadth of physiological data collected using highly specialized equipment and, perhaps more importantly, quantify uncertainty in model outputs. That said, there are important knowledge gaps that must be addressed to improve the utility and generalizability of such empirical models. Although accounting for design characteristics and demographic factors and between-modality differences in skin temperature reduced unexplained variance, most notably on the between-study level, considerable heterogeneity was still detected (Figure S86). These findings highlight the well-established variability in physiological responses to heat stress447,448,449. Delineating sources of this variation, particularly under ecologically relevant exposure conditions and durations (e.g., over several hours to days)449,450, is needed to not only improve our understanding of heats effects on the body, but also to identify factors for improving the accuracy and representativeness of physiological models.
It is important that future studies and analyses collect and consider data from individuals and locations most vulnerable to heat stress. For example, while age-related increases in heat-vulnerability and associated cardiovascular mortality are well-established2,3,6, 90% of our dataset, including studies aimed at defining responses to simulated heat waves or evaluating cooling strategies for protecting vulnerable groups32,33, was comprised of studies in adults, predominantly males, with mean ages under 50 years (Figure S22). Relatedly, few studies have assessed physiological responses in participants with heat-sensitive chronic health conditions447 and fewer still under environmental conditions relevant to the general population (e.g., those experienced during hot weather)6. Because of this, we excluded studies with participants reporting diagnosis of, or taking medications for, chronic health conditions linked with heat vulnerability. Future research and analyses should also evaluate the impacts of chronic diseases and associated medications on cardiac responses under ecologically relevant conditions, especially in light of recent research showing that age-associated functional decline and multimorbidity are associated with increased risk of heat-related hospitalization and deaths451,452. Finally, the geographical areas most strongly represented in our dataset (Fig. 1) are not those facing the most immediate threats of extreme heat and climate change (e.g., countries highlighted in Fig. 6). Research is needed to expand understanding of cardiovascular responses to heat exposure to encompass a greater range of climate regions (and associated differences in natural acclimatization among inhabitants), particularly those in the Global South. More studies performed in ecologically relevant environmental conditions would also allow for more thorough consideration of environmental factors like solar radiation and airflow33,453 and facilitate the expansion of models from resting conditions to incorporate physical activity (e.g., activities of daily living)454.
Another consideration is that not all studies reported data for secondary cardiac outcomes. Cardiac output, for instance, was reported in only ~20% of studies, and almost two-thirds of effect estimates were derived from participants heated using perfusion suits. This resulted in wide confidence intervals for estimates of the average heat-induced change in cardiac output and between-modality differences (Fig. 4). A likely contributor to this uncertainty is variation in employed measurement techniques. While Rowell et al.18 measured cardiac output using the highly accurate dye dilution technique (described in reference455). Common estimation techniques like Modelflow® can underestimate cardiac output in hyperthermic individuals relative to more direct methods like thermodilution (which is similar to dye dilution)313. Compared to direct methods, cardiac output was ~1–2 L/min lower when measured via imaging techniques (e.g., echocardiogram), rebreathing, or other indirect methods like Modelflow® (Table S30). However, direct measurements were almost entirely restricted to studies employing perfusion suits (Figure S87). While it is unlikely that measurement technique explains the large differences in cardiac output between Rowell et al.18 and the reviewed climate chamber studies, the lack of direct measurements in the latter further highlights the challenges in using extant laboratory data to inform our understanding of the real world.
Laboratory-based heat exposure research is becoming increasingly leveraged in the development of climate-health models and evidence-based heat-health guidance. However, our findings suggest that the substantial body of evidence on the cardiovascular burden of heat has, in its current form, limited use in supporting these efforts. Ecologically minded physiological research, conducted in both laboratories and natural settings, is urgently needed to develop and refine empirical physiological models and facilitate linkages to larger health databases and heat-health action plans and policies.
Methods
This review was prospectively registered (PROSPERO: CRD42020192887) and conducted and reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines456. The full review protocol, statistical analysis plan, and supporting analyses, are provided in the supplemental materials.
Literature search and study eligibility criteria
Cochrane search strategies were employed to identify eligible studies457. PubMed, Embase, Web of Science, and the Cochrane Central Register of Controlled Trials were searched from database inception until January 9th, 2023, for terms related to different laboratory-based passive (non-exercising) heating modalities, indices of body core temperature, and cardiac outcomes. Search criteria for each database are reported in Table S1 of the supplemental materials (pp 3–5). Systematic searches were supplemented with hand-searches of reference lists from topical narrative reviews and PubMed performed until February 8th, 2024.
Predefined criteria for population, exposure (intervention), comparator, and outcomes, (PECOs) were used to identify eligible studies457,458. Included studies needed to be published in a peer-reviewed journal. Conference papers were ineligible. There were no limits on date of publication. Given the size of the review, we decided not include study reports without an already available English translation.
Population
The population of interest was adults aged ≥18 years without reported acute or chronic disease linked with heat vulnerability (e.g., heart disease). Relatively few studies have evaluated thermal and cardiovascular responses to heat exposure in persons with chronic health conditions. We therefore opted to exclude such reports. Studies including individuals with risk factors for cardiovascular disease (e.g., hypertension, hypercholesteremia, cigarette smoking, obesity, etc.) were included, and we did not restrict inclusion based on sex/gender, anthropometric characteristics, habitual physical activity participation, or aerobic fitness.
Exposure
Studies were eligible if they included a passive (resting) heat stress intervention (no physical activity) using any heating modality (supplemental Table S2 provides an overview of common modalities) without concurrent continuous secondary intervention (e.g., intravenous saline infusion). All studies needed to report an index of core temperature (e.g., rectal temperature, oral temperature) and only those in which core temperature increased ≥0.1 °C were included. This ensured that only heat stress studies, and not studies using water-perfused suits or water immersion for other reasons (e.g., cold-stress, central volume manipulation) were included. Studies with acute secondary interventions (e.g., isometric hand grip, cognitive function tests) were included provided that resting data were reported and the intervention was not expected to influence resting responses. Secondary exposure variables included mean skin temperature and mean body temperature (weighted average of core and skin temperatures459).
Comparator
Included studies were required to report cardiovascular outcomes prior to and at the end of the heat stress intervention. Data from studies that included a non-heat stress control arm (e.g., rest in a thermoneutral environment, temperate water immersion) were also included for use in sensitivity analyses (described below).
Outcomes
All studies needed to report heart rate (primary outcome). Secondary outcomes included cardiac output, stroke volume, systolic blood pressure, and rate pressure product (an index of cardiac work calculated as heart rate × systolic pressure).
Study screening, data extraction, and risk of bias assessment
Study screening, data extraction, and risk of bias assessments were independently performed by at least two review authors. Disagreements were resolved via group consensus. Screening was conducted using commercially available software460. Relevant data on experimental design, participant characteristics, and study outcomes were extracted using a custom spreadsheet based on a previously tested form461. A full list of extracted variables is included in supplemental Tables S5–S11. A similar form was used to record study quality and risk of bias assessments (Tables S12–S14).
The method to induce heat stress (i.e. the heating modality) was extracted and classified as either ambient exposure in a climate chamber, water-perfused suit, water immersion, or sauna (Table S2). Body temperature (exposure) and cardiovascular (outcome) data were extracted as mean and dispersion (e.g., standard deviation or error, 95% confidence interval) before and at the end of the heat stress intervention (and control intervention, if included) and/or the change score and its dispersion (i.e., the baseline-end difference). Data were extracted for all eligible experimental conditions. If studies employed a multi-stage protocol wherein body core temperature was stabilized (clamped) at multiple levels of heat stress, data for each level were extracted. Otherwise, only the pre- and end-heating data were recorded. For studies with multiple experimental trials in which drinking water was provided during heating, only the condition eliciting the smallest fluid loss (change in body weight) was included. Open-source software was used to extract numerical data presented in graphical format462. For studies that met the inclusion criteria but did not present core temperature and heart rate data in a usable format, the corresponding author was contacted (supplemental Box S1).
Information on numerous additional study-level variables was also extracted, including participant characteristics and posture, duration of heat stress, additional indices of body temperature (mean skin temperature and mean body temperature), indices of body fluid status (change in body weight and/or plasma volume), and methods of exposure/outcome ascertainment. Regarding the latter, the body location in which core temperature was measured was recorded and grouped into three categories: i) direct, slow-responding (rectum, gastrointestinal tract); ii) direct, fast-responding (pulmonary artery, esophagus, or tympanic membrane); or iii) indirect (oral cavity, aural canal). This was done to account for differences in the absolute and temporal responses to body heating among common core temperature indices (see “Meta-analyses” below)459. Ascertainment methods for all exposure and outcome variables are described in supplemental Table S9 (pp 17–18).
The quality of studies including only a heat stress arm were assessed using the National Heart, Lung and Blood Institute Quality Tool for Before-After Studies434. Risk of bias in the controlled studies was evaluated using the revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2)435. Information on the use of these scales along with adaptations made for the current review are described in the supplement (Tables S12–S14).
Meta-analyses
Individual study effect estimates (unit of analysis)
Analyzed effect estimates were the change in heart rate (primary outcome) and secondary cardiac outcomes from pre-heating (baseline) values to the end of heating. If the baseline-to-end-heating change and its standard deviation were not directly reported, they were derived from data presented for the baseline and end-heating timepoints463. Data presented in figures were extracted using open-source software (WebPlotDigitizer)462. Secondary variables reflecting a composite of other exposures (e.g., mean body temperature) or outcomes (e.g., cardiac output, rate pressure product) were imputed from the composite variables if sufficient data were available (Tables S15–S16). Secondary outcomes reported in the main article included cardiac output, systolic pressure, and rate pressure product, with analyses for stroke volume confined to the supplement.
Modifying effect of heating modality on cardiac responses
We evaluated how the employed heating modality modified heat-induced cardiac responses in a series of multilevel mixed-effects meta-analyses. Robust variance estimation was used to account for statistical dependencies among effect estimates derived from the same study and to correct for small sample bias464. This approach allows for inclusion of multiple estimates from individual studies in a single analysis, increasing statistical power to evaluate the contribution of study-level covariates (e.g., heating modality) to the observed variation in study findings (heterogeneity)464,465.
The analysis of each cardiac outcome followed the general workflow for meta-analyses with complex dependency structures466. First, an approximate variance-covariance matrix of the sampling variance of dependent effect estimates was constructed. A unique identifier for study (study id) was used as the clustering variable and the within-study correlation was assumed constant at 0.6 (different values were considered in sensitivity analyses, described below)464. The resultant variance-covariance matrix was then used in a series of multilevel mixed-effects meta-analyses, which differed with respect to prespecified covariates (fixed effects). Model 1 included heating modality as a categorical predictor (4 levels: ambient exposure in a climate chamber [reference], water-perfused suit, water immersion, sauna). To account for differences in the level of heat strain, model 2 included, in addition to heating modality, the baseline-to-end heating change in core temperature (in °C), and the core temperature measurement technique as a categorical predictor (three levels: direct-slow [reference], direct-fast, indirect). Model 3 was identical to model 2 except an interaction term between heating modality and core temperature change was specified. All models included a multilevel random effects structure with an effect identifier nested within the study identifier467,468. Variance components (random effects) for all models were initially derived using the maximum likelihood (ML) estimator. Models were then compared using Akaike’s Information Criterion (AIC)469 and the most parsimonious (lowest AIC) was refit using the restricted maximum likelihood (REML) variance estimator470.
Approximate normality and homogeneity of model residuals were assessed via visual inspection of residual diagnostic plots. Identifiability of the variance components (random effects) was evaluated using profile likelihood plots466. After confirming the models were well specified, robust confidence intervals and significance tests were obtained using a cluster-robust (sandwich) estimator with small-sample correction471,472. Modification of cardiac responses by heating modality was interpreted with respect to significance tests considering both the overall pattern of response between the climate chamber studies and other heating modalities (i.e., omnibus test of both model intercept and slope coefficients) and the individual model coefficients for the between-modality differences in intercept and slope (per °C change in the pre-end heating rise in core temperature). Statistical significance was taken as a two-sided robust P < 0.050. No adjustments were made for multiple comparisons.
Residual heterogeneity was assessed via the QE test and the I2 statistic473,474,475. The latter was evaluated for the overall model as well as individually at the between- and within-study levels. Influence statistics were generated to identify effect estimates with potentially undue influence on model outputs (Cook’s distances and differences in regression coefficient values (DFBETAS))476. Relations between model residuals and their associated standard errors were visualized using funnel plots477.
Potential mediators and confounders of heat-induced changes in heart rate
In secondary analyses, we evaluated the association between heating modality and heart rate (primary outcome), controlling for potential non-heat stress-related mediators and confounders of this relation. A directed acyclic graph (DAG) describing assumed relations between these factors is provided in supplemental Figure S21 (pp 63). Three models were produced. Model 4 included the same covariates from the best-fitting model amongst models 1–3 along with participant posture (2 levels: seated [reference], supine) and the level of clothing insulation (2 levels: low [reference], medium). Model 5 was comprised of the same covariates as model 4, as well as participant characteristics known to influence thermoregulatory function. These included age (in years), sex (proportion of females in sample), body mass index (in kg/m2), and climate zone (Köppen climate classifications478), which was taken as a proxy for natural heat acclimatization (4 levels: temperate [reference], continental, tropical, polar). Model 6 included the same covariates as model 5 along with end-heating mean skin temperature (in °C) also included. These analyses allowed us to isolate the extent to which modality-related differences in heat strain explained the primary findings.
Body temperature and cardiac responses to high ambient temperatures
A secondary goal of this project was to leverage the large number of captured studies to provide empirical estimates of the thermal and cardiac strain that may be experienced in hot weather and heat waves. To achieve this, we modeled associations between ambient heat index (apparent temperature index considering both air temperature and humidity) and core temperature, heart rate, and secondary cardiac outcomes in studies exposing participants to ambient heat stress in a climate chamber (see supplement pp 66). For core temperature and heart rate, separate models were produced with heat index included as a linear term and as a restricted cubic (natural) spline with knots placed at the 10th, 50th, and 90th quantiles479. Analyses for all other outcomes included only the linear term. Models for core temperature, heart rate, systolic pressure, and rate pressure product were adjusted for sample mean age (in decades) and heating duration (in hours). Analysis was restricted to experimental conditions with heat index ≤80 °C, the highest value ever recorded480.
Sensitivity analyses
A series of sensitivity analyses were conducted to evaluate the robustness of our findings to key assumptions made in data processing and analysis (see supplement pp 66–69). For heart rate, we evaluated whether findings were robust to: a) inclusion of the studies omitted from the primary analysis, b) consideration of laboratory in the multilevel random effect structure, c) variation in the within-study correlation input in robust variance estimation, d) removal of potentially influential effect estimates flagged in influence analyses, e) differences in the bodily coverage of perfusion suits and water immersion in studies that employed those modalities, f) inclusion of covariates describing when the baseline and end-heating measurements were procured, g) modeling non-linear associations between core temperature and heart rate, h) replacing core temperature with estimated mean body temperature, i) including a covariate for study quality, j) including a covariate for publication date, and k) whether the outcome was analyzed as the pre-end heating change or the between-arm difference in studies including a control group. We also evaluated whether findings of secondary analyses were altered by the technique used to measure l) cardiac output and m) systolic blood pressure, and when modeling non-linear associations between core temperature and n) systolic pressure and o) rate pressure product.
All data processing and statistical analyses were performed using R (Version 4.2.0, R Core team)466,481,482,483,484. The full analysis plan is provided supplemental materials (pp 30–69). R was also used for all data visualizations484,485,486,487,488,489,490,491,492.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The meta-analytic dataset and record supplement is available at: https://github.com/robdmeade/csrma.
Code availability
Analytical code is available at: https://github.com/robdmeade/csrma.
References
Alahmad, B. et al. Cardiovascular mortality and exposure to heat in an inherently hot region: implications for climate change. Circulation 141, 1271–1273 (2020).
Bunker, A. et al. Effects of air temperature on climate-sensitive mortality and morbidity outcomes in the elderly; a systematic review and meta-analysis of epidemiological evidence. EBioMedicine 6, 258–268 (2016).
Scovronick, N. et al. Temperature-mortality associations by age and cause: a multi-country multi-city study. Environ. Epidemiol. 8, e336 (2024).
Khraishah, H. et al. Climate change and cardiovascular disease: implications for global health. Nat. Rev. Cardiol. 19, 798–812 (2022).
Chaseling, G. K., Morris, N. B. & Ravanelli, N. Extreme heat and adverse cardiovascular outcomes in Australia and New Zealand: What do we know? Heart Lung Circ. 32, 43–51 (2022).
Meade, R. D. et al. Physiological factors characterizing heat-vulnerable older adults: a narrative review. Environ. Int. 144, 105909 (2020).
Chaseling, G. K. et al. Extreme heat and cardiovascular health: what a cardiovascular health professional should know. Can. J. Cardiol. 37, 1828–1836 (2021).
Ebi, K. L. et al. Hot weather and heat extremes: health risks. Lancet 398, 698–708 (2021).
Kenney, W. L., Craighead, D. H. & Alexander, L. M. Heat waves, aging, and human cardiovascular health. Med. Sci. Sports Exerc. 46, 1891–1899 (2014).
Kenny, G. P. & Jay, O. Thermometry, calorimetry, and mean body temperature during heat stress. Compr. Physiol. 3, 1689–1719 (2013).
Crandall, C. G. & Wilson, T. E. Human cardiovascular responses to passive heat stress. Compr. Physiol. 5, 17–43 (2015).
Crandall, C. G. et al. Effects of passive heating on central blood volume and ventricular dimensions in humans. J. Physiol. 586, 293–301 (2008).
Lucas, R. A., Sarma, S., Schlader, Z. J., Pearson, J. & Crandall, C. G. Age-related changes to cardiac systolic and diastolic function during whole-body passive hyperthermia. Exp. Physiol. 100, 422–434 (2015).
Hausfater, P. et al. Elevation of cardiac troponin I during non-exertional heat-related illnesses in the context of a heatwave. Crit. Care 14, R99 (2010).
Barry, H. et al. The effect of heat exposure on myocardial blood flow and cardiovascular function. Ann. Intern. Med. 177, 901–910 (2024).
Keatinge, W. R. et al. Increased platelet and red cell counts, blood viscosity, and plasma cholesterol levels during heat stress, and mortality from coronary and cerebral thrombosis. Am. J. Med. 81, 795–800 (1986).
Meyer, M. A. et al. Hypercoagulability in response to elevated body temperature and central hypovolemia. J. Surg. Res. 185, e93–e100 (2013).
Rowell, L. B., Brengelmann, G. L. & Murray, J. A. Cardiovascular responses to sustained high skin temperature in resting man. J. Appl. Physiol. 27, 673–680 (1969).
Minson, C. T., Wladkowski, S. L., Cardell, A. F., Pawelczyk, J. A. & Kenney, W. L. Age alters the cardiovascular response to direct passive heating. J. Appl Physiol. 84, 1323–1332 (1998).
Bach, A. J. et al. Experimental research in environmentally induced hyperthermic older persons: a systematic quantitative literature review mapping the available evidence. Temperature 11, 4–26 (2023).
Morris, N. B., English, T., Hospers, L., Capon, A. & Jay, O. The effects of electric fan use under differing resting heat index conditions: a clinical trial. Ann. Intern. Med. 171, 675–677 (2019).
Morris, N. B. et al. A preliminary study of the effect of dousing and foot immersion on cardiovascular and thermal responses to extreme heat. JAMA 322, 1411–1413 (2019).
Cramer, M. N., Huang, M., Moralez, G. & Crandall, C. G. Keeping older individuals cool in hot and moderately humid conditions: wetted clothing with and without an electric fan. J. Appl Physiol. 128, 604–611 (2020).
Meade, R. D. et al. Effects of daylong exposure to indoor overheating on thermal and cardiovascular strain in older adults: A randomized crossover trial. Environ. Health Perspect 132, 27003 (2024).
Meade, R. D. et al. Body core temperature after foot immersion and neck cooling in older adults exposed to extreme heat. JAMA 331, 253–253 (2024).
Meade, R. D. et al. Efficacy of cooling centers for mitigating physiological strain in older adults during daylong heat exposure: A laboratory-based heat wave simulation. Environ. Health Perspect 131, 67003 (2023).
Meade, R. D. et al. Physiological responses to 9 hours of heat exposure in young and older adults. Part I: body temperature and hemodynamic regulation. J. Appl. Physiol. 135, 673–687 (2023).
Fisher, J. T. et al. Cardiovascular responses to orthostasis during a simulated 3-day heatwave. Sci. Rep. 12, 19998 (2022).
Vanos, J. K., Baldwin, J. W., Jay, O. & Ebi, K. L. Simplicity lacks robustness when projecting heat-health outcomes in a changing climate. Nat. Commun. 11, 6079 (2020).
Vecellio, D. J., Kong, Q., Kenney, W. L. & Huber, M. Greatly enhanced risk to humans as a consequence of empirically determined lower moist heat stress tolerance. Proc. Natl. Acad. Sci. USA 120, e2305427120 (2023).
Vanos, J. et al. A physiological approach for assessing human survivability and liveability to heat in a changing climate. Nat. Commun. 14, 7653 (2023).
Jay, O. et al. Reducing the health effects of hot weather and heat extremes: from personal cooling strategies to green cities. Lancet 398, 709–724 (2021).
Meade, R. D., Notley, S. R., Kirby, N. V. & Kenny, G. P. A critical review of the effectiveness of electric fans as a personal cooling intervention in hot weather and heatwaves. Lancet Planet Health 8, e256–e269 (2024).
Meade, R. D. et al. Human heat resilience in a warming climate: Biophysical and physiological underpinnings of heat vulnerability and personal cooling strategies. One Earth 7, 1343–1350 (2024).
Michikami, D. et al. Attenuated thermoregulatory sweating and cutaneous vasodilation after 14-day bed rest in humans. J. Appl. Physiol. 96, 107–114 (2004).
Ftaiti, F. et al. Effect of hyperthermia and physical activity on circulating growth hormone. Appl. Physiol. Nutr. Metab. 33, 880–887 (2008).
Stephenson, L. A., Kolka, M. A., Allan, A. E. & Santee, W. R. Heat exchange during encapsulation in a chemical warfare agent protective patient wrap in four hot environments. Aviat. Space Environ. Med. 59, 345–351 (1988).
O’Hearn, K. et al. Heat exposure increases circulating fatty acids but not lipid oxidation at rest and during exercise. J. Therm. Biol. 55, 39–46 (2016).
Goulet, E. D. B. et al. Impact of mild hypohydration on muscle endurance, power, and strength in healthy, active older men. J. Strength Cond. Res. 32, 3405–3415 (2018).
Yadav, S., Verma, V. & Abinav, Impact of Sarvanga Ruksha Svedana on physiological, hematological and biochemical parameters in young healthy subjects: an exploratory study. J. Nat. Rem. 20, 249–261 (2020).
Barley, O. R., Chapman, D. W., Mavropalias, G. & Abbiss, C. R. The influence of heat acclimation and hypohydration on post-weight-loss exercise performance. Int J. Sports Physiol. Perform. 15, 213–221 (2020).
Drummond, P. D. Thermoregulatory response to passive body heating in borderline hypertension. Clin. Auton. Res. 3, 233–238 (1993).
Jensen, B. H. et al. Visual function and retinal vessel diameters during hyperthermia in man. Acta Ophthalmol. 95, 690–696 (2017).
Glazachev, O. S. et al. Whole-body repeated hyperthermia increases irisin and brain-derived neurotrophic factor: a randomized controlled trial. J. Therm. Biol. 101, 103067–103067 (2021).
Kominami, K., Noda, K., Takahashi, N., Izumi, T. & Yonezawa, K. Cardiovascular reactions for whole-body thermal therapy with a hot pack and Waon therapy. Int J. Hyperth. 37, 184–191 (2020).
Ohnaka, T., Tochihara, Y., Kubo, M. & Yamaguchi, C. Physiological and subjective responses to standing showers, sitting showers, and sink baths. Appl. Hum. Sci. 14, 235–239 (1995).
Wilson, T. E., Cui, J. & Crandall, C. G. Absence of arterial baroreflex modulation of skin sympathetic activity and sweat rate during whole-body heating in humans. J. Physiol. 536, 615–623 (2001).
Carter, S. J., Herron, R. L., Akers, S. Z. & Bishop, P. A. Acetylsalicylic acid does not alter thermo-effector responses during mild whole-body passive heat stress in young men. Int J. Hyperth. 31, 319–324 (2015).
Pearson, J. et al. Active and passive heat stress similarly compromise tolerance to a simulated hemorrhagic challenge. Am. J. Physiol. Regul. Integr. Comp. Physiol. 307, R822–R827 (2014).
Kamijo, Y., Lee, K. & Mack, G. W. Active cutaneous vasodilation in resting humans during mild heat stress. J. Appl. Physiol. 98, 829–837 (2005).
Hoekstra, S. P., Bishop, N. C., Faulkner, S. H., Bailey, S. J. & Leicht, C. A. Acute and chronic effects of hot water immersion on inflammation and metabolism in sedentary, overweight adults. J. Appl. Physiol. 125, 2008–2018 (2018).
Bartolomé, I. et al. Acute effect of exposure to extreme Heat (100 ± 3 °C) on lower limb maximal resistance strength. Int. J. Environ. Res. Public Health 19, 10934 (2022).
Chaseling, G. K. et al. The acute effect of heat exposure on forearm macro- and microvascular function: impact of measurement timing, heating modality and biological sex. Exp. Physiol. 108, 221–239 (2022).
Shimodozono, M. et al. Acute effects of a single warm-water bath on serum adiponectin and leptin levels in healthy men: a pilot study. Int J. Biometeorol. 56, 933–939 (2012).
Kaldur, T. et al. The acute effects of passive heat exposure on arterial stiffness, oxidative stress, and inflammation. Medicina 52, 211–216 (2016).
Hu, Q., Zhu, W., Zhu, Y., Zheng, L. & Hughson, R. L. Acute effects of warm footbath on arterial stiffness in healthy young and older women. Eur. J. Appl. Physiol. 112, 1261–1268 (2012).
Hemingway, H. W. et al. Acute heat exposure protects against endothelial ischemia-reperfusion injury in aged humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 322, R360–R367 (2022).
Coombs, G. B. et al. Acute heat stress reduces biomarkers of endothelial activation but not macroor microvascular dysfunction in cervical spinal cord injury. Am. J. Physiol. Heart Circ. Physiol. 316, H722–H733 (2019).
Rissanen, J. A., Häkkinen, K., Laukkanen, J. A. & Häkkinen, A. Acute hemodynamic responses to combined exercise and sauna. Int. J. Sports Med. 41, 824–831 (2020).
Brunt, V. E. et al. Acute hot water immersion is protective against impaired vascular function following forearm ischemia-reperfusion in young healthy humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 311, R1060–R1067 (2016).
Romero, S. A. et al. Acute limb heating improves macro- and microvascular dilator function in the leg of aged humans. Am. J. Physiol. Heart Circ. Physiol. 312, H89–H97 (2017).
Engelland, R. E., Hemingway, H. W., Tomasco, O. G., Olivencia-Yurvati, A. H. & Romero, S. A. Acute lower leg hot water immersion protects macrovascular dilator function following ischaemia-reperfusion injury in humans. Exp. Physiol. 105, 302–311 (2020).
Campbell, H. A. et al. Acute physiological and psychophysical responses to different modes of heat stress. Exp. Physiol. 107, 429–440 (2022).
Keller, D. M. et al. Acute volume expansion preserves orthostatic tolerance during whole-body heat stress in humans. J. Physiol. 587, 1131–1139 (2009).
Ko, Y., Seol, S. H., Kang, J. & Lee, J. Y. Adaptive changes in physiological and perceptual responses during 10-day heat acclimation training using a water-perfused suit. J. Physiol. Anthropol. 39, 10 (2020).
Peçanha, T., Forjaz, C. L. M. & Low, D. A. Additive effects of heating and exercise on baroreflex control of heart rate in healthy males. J. Appl. Physiol. 123, 1555–1562 (2017).
Périard, J. D., Racinais, S. & Thompson, M. W. Adjustments in the force-frequency relationship during passive and exercise-induced hyperthermia. Muscle Nerve 50, 822–829 (2014).
Nelson, M. D. et al. Aerobic fitness does not influence the biventricular response to whole body passive heat stress. J. Appl Physiol. 109, 1545–1551 (2010).
Kenney, W. L. et al. Age and hypohydration independently influence the peripheral vascular response to heat stress. J. Appl Physiol. 68, 1902–1908 (1990).
Gagnon, D. et al. Age modulates physiological responses during fan use under extreme heat and humidity. Med Sci. Sports Exerc 49, 2333–2342 (2017).
Oue, A. et al. Age-related attenuation of conduit artery blood flow response to passive heating differs between the arm and leg. Eur. J. Appl Physiol. 118, 2307–2318 (2018).
Wang, J., Solianik, R., Eimantas, N., Baranauskiene, N. & Brazaitis, M. Age-related difference in cognitive performance under severe whole-body hyperthermia parallels cortisol and physical strain responses. Medicina 59, 1665–1665 (2023).
Minson, C. T., Wladkowski, S. L., Pawelczyk, J. A. & Kenney, W. L. Age, splanchnic vasoconstriction, and heat stress during tilting. Am. J. Physiol. 276, R203–R212 (1999).
Scremin, G. & Kenney, W. L. Aging and the skin blood flow response to the unloading of baroreceptors during heat and cold stress. J. Appl. Physiol. 96, 1019–1025 (2004).
Roine, R. et al. Alcohol and sauna bathing: effects on cardiac rhythm, blood pressure, and serum electrolyte and cortisol concentrations. J. Intern. Med. 231, 333–338 (1992).
Keller, D. M., Sander, M., Stallknecht, B. & Crandall, C. G. alpha-Adrenergic vasoconstrictor responsiveness is preserved in the heated human leg. J. Physiol. 588, 3799–3808 (2010).
Fischer, M. et al. Altered cardiac β1 responsiveness in hyperthermic older adults. Am. J. Physiol. Regul. Integr. Comp. Physiol. 323, R581–R588 (2022).
Desvaux, B., Abraham, P., Colin, D., Leftheriotis, G. & Saumet, J. L. Ankle to arm index response to exercise and heat stress in healthy subjects. Clin. Physiol. 16, 1–7 (1996).
Kellogg, D. L., Zhao, J. L., Wu, Y. & Johnson, J. M. Antagonism of soluble guanylyl cyclase attenuates cutaneous vasodilation during whole body heat stress and local warming in humans. J. Appl. Physiol. 110, 1406–1413 (2011).
Schlader, Z. J., Okada, Y., Best, S. A., Fu, Q. & Crandall, C. G. Arterial stiffness during whole-body passive heat stress in healthy older adults. Physiol. Rep. 7, e14094 (2019).
Vogelsang, T. W. et al. Atrial natriuretic peptide and acute changes in central blood volume by hyperthermia in healthy humans. Open Neuroendocrinol. J. 5, 1–4 (2012).
Arnold, R. W. & Nadel, E. R. The attenuating effect of heat and hypovolemia on the human diving response. Alsk. Med. 35, 199–203 (1993).
Levitt, E. L., Keen, J. T. & Wong, B. J. Augmented reflex cutaneous vasodilatation following short-term dietary nitrate supplementation in humans. Exp. Physiol. 100, 708–718 (2015).
Metzler-Wilson, K. et al. Augmented supraorbital skin sympathetic nerve activity responses to symptom trigger events in rosacea patients. J. Neurophysiol. 114, 1530–1537 (2015).
Marciniak, R. A., Wahl, C. A. & Ebersole, K. T. Autonomic nervous system response to far-infrared sauna exposure in firefighters. Ann. Work Expo. Health 66, 356–367 (2022).
Madeira, L. G., Passos, R. L. F., Souza, J. F. D., Rezende, N. A. & Rodrigues, L. O. C. Autonomic thermoregulatory dysfunction in neurofibromatosis type 1. Arq. Neuro Psiquiatr. 74, 796–802 (2016).
Schlader, Z. J., Gagnon, D., Lucas, R. A., Pearson, J. & Crandall, C. G. Baroreceptor unloading does not limit forearm sweat rate during severe passive heat stress. J. Appl. Physiol. 118, 449–454 (2015).
Yamazaki, F., Kawahara, C., Soga, I., Yamada, S. & Hamasaki, K. Baroreflex control of heart rate during heating in subjects with low orthostatic tolerance. Aviat. Space Environ. Med. 74, 1237–1242 (2003).
Cui, J., Wilson, T. E. & Crandall, C. G. Baroreflex modulation of sympathetic nerve activity to muscle in heat-stressed humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 282, R252–R258 (2002).
Bartnicki, C., Waśkiewicz, J. & Dubrawski, R. Behaviour of some physiological indexes depending on the age of people exposed to short action of humid heat under experimental conditions. Biul. Inst. Med. Morsk. Gdan. 20, 37–49 (1969).
Apte, C. V., Dikshit, M. B. & Prasad, B. A. Beta-adrenoreceptor blockade attenuates heat-induced tachycardia,but not the tolerance to the stress. Indian J. Physiol. Pharm. 36, 149–154 (1992).
Ogoh, S. et al. Blood flow distribution during heat stress: cerebral and systemic blood flow. J. Cereb. Blood Flow. Metab. 33, 1915–1920 (2013).
Aoki, K., Ogawa, Y. & Iwasaki, K. Blunted cutaneous vasoconstriction and increased frequency of presyncope during an orthostatic challenge under moderate heat stress in the morning. Eur. J. Appl. Physiol. 114, 629–638 (2014).
Takamata, A., Mack, G. W., Stachenfeld, N. S. & Nadel, E. R. Body temperature modification of osmotically induced vasopressin secretion and thirst in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 269, R874–R880 (1995).
Jenssen, T. G., Haukland, H. H. & Burhol, P. G. Brain-gut peptides in sauna-induced hyperthermia. Acta Physiol. Scand. 132, 519–523 (1988).
Yamazaki, F., Monji, K., Sogabe, Y. & Sone, R. Cardiac and peripheral vascular responses to head-up tilt during whole body thermal stress. J. UOEH 22, 147–158 (2000).
Brothers, R. M. et al. Cardiac systolic and diastolic function during whole body heat stress. Am. J. Physiol. Heart Circ. Physiol. 296, H1150–H1156 (2009).
Lucas, R. A., Pearson, J., Schlader, Z. J. & Crandall, C. G. Cardiopulmonary and arterial baroreceptor unloading during passive hyperthermia does not contribute to hyperthermia-induced hyperventilation. Exp. Physiol. 100, 1309–1318 (2015).
Crandall, C. G., Etzel, R. A. & Farr, D. B. Cardiopulmonary baroreceptor control of muscle sympathetic nerve activity in heat-stressed humans. Am. J. Physiol. 277, H2348–H2352 (1999).
Bühring, M., Kemmerer, K. & Kappos, A. Cardiovascular and respiratory function values in hyperthermia: the effect of beta-receptor blockade with bunitrolol. Klin. Wochenschr. 60, 617–623 (1982).
Kukkonen-Harjula, K. et al. Cardiovascular effects of Atenolol, Scopolamine and their combination on healthy men in Finnish sauna baths. Eur. J. Appl Physiol. Occup. Physiol. 69, 10–15 (1994).
Koroxenidis, G. T., Shepherd, J. T. & Marshall, R. J. Cardiovascular response to acute heat stress. J. Appl Physiol. 16, 869–872 (1961).
Allison, T. G., Maresh, C. M. & Armstrong, L. E. Cardiovascular responses in a whirlpool path at 40 degrees C versus user-controlled water temperatures. Mayo Clin. Proc. 73, 210–215 (1998).
Keller, D. M. et al. Carotid baroreceptor stimulation alters cutaneous vascular conductance during whole-body heating in humans. J. Physiol. 577, 925–933 (2006).
Krnjajic, D., Allen, D. R., Butts, C. L. & Keller, D. M. Carotid baroreflex control of heart rate is enhanced, while control of mean arterial pressure is preserved during whole body heat stress in young healthy men. Am. J. Physiol. Regul. Integr. Comp. Physiol. 311, R735–R741 (2016).
Crandall, C. G. Carotid baroreflex responsiveness in heat-stressed humans. Am. J. Physiol. Heart Circ. Physiol. 279, H1955–H1962 (2000).
Oehler, R. et al. Cell type-specific variations in the induction of hsp70 in human leukocytes by feverlike whole body hyperthermia. Cell Stress Chaperones 6, 306–315 (2001).
Shibasaki, M., Secher, N. H., Selmer, C., Kondo, N. & Crandall, C. G. Central command is capable of modulating sweating from non-glabrous human skin. J. Physiol. 553, 999–1004 (2003).
Lee, J. F. et al. Cerebral vasoreactivity: impact of heat stress and lower body negative pressure. Clin. Auton. Res. 24, 135–141 (2014).
Perry, B. G., Korad, S. & Mündel, T. Cerebrovascular and cardiovascular responses to the Valsalva manoeuvre during hyperthermia. Clin. Physiol. Funct. Imaging 43, 463–471 (2023).
Low, D. A. et al. Cerebrovascular responsiveness to steady-state changes in end-tidal CO2 during passive heat stress. J. Appl. Physiol. 104, 976–981 (2008).
Lee, K. et al. Change in spontaneous baroreflex control of pulse interval during heat stress in humans. J. Appl Physiol. 95, 1789–1798 (2003).
Fujii, N. et al. Changes in arterial blood pressure elicited by severe passive heating at rest is associated with hyperthermia-induced hyperventilation in humans. Eur. J. Appl Physiol. 113, 51–62 (2013).
Pilch, W. et al. Changes in the lipid profile of blood serum in women taking sauna baths of various duration. Int J. Occup. Med. Environ. Health 23, 167–174 (2010).
Machado-Moreira, C. A. et al. The cholinergic blockade of both thermally and non-thermally induced human eccrine sweating. Exp. Physiol. 97, 930–942 (2012).
Francisco, M. A., Gibson, B. M., Simmons, G. H., Halliwill, J. R. & Minson, C. T. Cholinergic nerve contribution to cutaneous active vasodilation during exercise is similar to whole body passive heating. J. Appl. Physiol. 134, 933–940 (2023).
Cui, J. et al. Chronic heart failure does not attenuate the total activity of sympathetic outflow to skin during whole-body heating. Circ. Heart Fail. 6, 271–278 (2013).
Greaney, J. L., Stanhewicz, A. E. & Kenney, W. L. Chronic statin therapy is associated with enhanced cutaneous vascular responsiveness to sympathetic outflow during passive heat stress. J. Physiol. 597, 4743–4755 (2019).
Zahorska-Markiewicz, B. et al. Circadian variations in psychophysiological responses to heat exposure and exercise. Eur. J. Appl. Physiol. Occup. Physiol. 59, 29–33 (1989).
Schultz Martins, R. et al. The clamping of end-tidal carbon dioxide does not influence cognitive function performance during moderate hyperthermia with or without skin temperature manipulation. Front. Psychol. 12, 788027–788027 (2021).
Crandall, C. G. et al. Colloid volume loading does not mitigate decreases in central blood volume during simulated haemorrhage while heat stressed. J. Physiol. 590, 1287–1297 (2012).
Wingo, J. E., Low, D. A., Keller, D. M., Kimura, K. & Crandall, C. G. Combined facial heating and inhalation of hot air do not alter thermoeffector responses in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 309, R623–R627 (2015).
Klein, J. C., Crandall, C. G., Brothers, R. M. & Carter, J. R. Combined heat and mental stress alters neurovascular control in humans. J. Appl. Physiol. 109, 1880–1886 (2010).
Ishibashi, K., Maeda, T., Higuchi, S., Iwanaga, K. & Yasukouchi, A. Comparison of cardiovascular response to sinusoidal and constant lower body negative pressure with reference to very mild whole-body heating. J. Physiol. Anthropol. 31, 30–30 (2012).
Iwase, S. et al. A comparison of head-out mist bathing, with or without facial fanning, with head-out half-body low-water level bathing in humans–a pilot study. Int J. Biometeorol. 58, 999–1005 (2014).
Pilch, W. et al. Comparison of physiological reactions and physiological strain in healthy men under heat stress in dry and steam heat saunas. Biol. Sport 31, 145–149 (2014).
Allison, T. G. & Reger, W. E. Comparison of responses of men to immersion in circulating water at 40.0 and 41.5 degrees. C. Aviat. Space Environ. Med. 69, 845–850 (1998).
Wijayanto, T. et al. Comparison of thermoregulatory responses to heat between Malaysian and Japanese males during leg immersion. Int J. Biometeorol. 55, 491–500 (2011).
Morrison, S. A., Ainslie, P. N., Lucas, R. A., Cheung, S. S. & Cotter, J. D. Compression garments do not alter cerebrovascular responses to orthostatic stress after mild passive heating. Scand. J. Med. Sci. Sports 24, 291–300 (2014).
Tamm, M. et al. The compression of perceived time in a hot environment depends on physiological and psychological factors. Q J. Exp. Psychol. 67, 197–208 (2014).
Gibbons, T. D. et al. Contribution of the carotid body to thermally mediated hyperventilation in humans. J. Physiol. 600, 3603–3624 (2022).
Cabanac, M. & White, M. D. Core temperature thresholds for hyperpnea during passive hyperthermia in humans. Eur. J. Appl. Physiol. Occup. Physiol. 71, 71–76 (1995).
Crandall, C. G. & MacLean, D. A. Cutaneous interstitial nitric oxide concentration does not increase during heat stress in humans. J. Appl. Physiol. 90, 1020–1024 (2001).
Crandall, C. G., Musick, J., Hatch, J. P., Kellogg, D. L. Jr & Johnson, J. M. Cutaneous vascular and sudomotor responses to isometric exercise in humans. J. Appl. Physiol. 79, 1946–1950 (1995).
Wingo, J. E., Low, D. A., Keller, D. M. & Crandall, C. G. Cutaneous vascular responses to hypercapnia during whole-body heating. Aviat. Space Environ. Med. 79, 1081–1085 (2008).
Inoue, Y. et al. Cutaneous vasodilation response to a linear increase in air temperature from 28 degrees C to 40 degrees C in prepubertal boys and young men. J. Physiol. Anthropol. 28, 137–144 (2009).
Fujii, N. et al. Cyclooxygenase-1 and -2 modulate sweating but not cutaneous vasodilation during exercise in the heat in young men. Physiol. Rep. 6, e13844–e13844 (2018).
Tian, X., Fang, Z. & Liu, W. Decreased humidity improves cognitive performance at extreme high indoor temperature. Indoor Air 31, 608–627 (2021).
Abraham, P., Leftheriotis, G., Desvaux, B., Saumet, M. & Saumet, J. L. Diameter and velocity changes in the femoral vein during thermal stress in humans. Clin. Physiol. 14, 15–21 (1994).
Cramer, M. N., Hieda, M., Huang, M., Moralez, G. & Crandall, C. G. Dietary nitrate supplementation does not influence thermoregulatory or cardiovascular strain in older individuals during severe ambient heat stress. Exp. Physiol. 105, 1730–1741 (2020).
Hashizaki, T. et al. Differences in serum IL-6 response after 1 °C rise in core body temperature in individuals with spinal cord injury and cervical spinal cord injury during local heat stress. Int. J. Hyperth. 35, 541–547 (2018).
Bartnicki, C., Ejsmont, W. & Dubrawski, R. Differences of some physiological reactions in women and men exposed to the effect of high environmental temperature. Biul. Inst. Med. Morsk. Gdan. 20, 45–49 (1969).
Coombs, G. B. et al. Distinct contributions of skin and core temperatures to flow-mediated dilation of the brachial artery following passive heating. J. Appl. Physiol. 130, 149–159 (2021).
Otani, H. et al. Diurnal effects of prior heat stress exposure on sprint and endurance exercise capacity in the heat. Chronobiol. Int. 35, 982–995 (2018).
Pullinger, S. A. et al. Diurnal variation in repeated sprint performance cannot be offset when rectal and muscle temperatures are at optimal levels (38.5 degrees C). Chronobiol. Int. 35, 1054–1065 (2018).
Lynn, A. G., Gagnon, D., Binder, K., Boushel, R. C. & Kenny, G. P. Divergent roles of plasma osmolality and the baroreflex on sweating and skin blood flow. Am. J. Physiol. Regul. Integr. Comp. Physiol. 302, R634–R642 (2012).
Amano, T., Fujii, N., Kenny, G. P., Inoue, Y. & Kondo, N. Do nitric oxide synthase and cyclooxygenase contribute to sweating response during passive heating in endurance-trained athletes? Physiol. Rep. 5, e13403 (2017).
Stapleton, J. M. et al. Do older adults experience greater thermal strain during heat waves? Appl. Physiol. Nutr. Metab. 39, 292–298 (2014).
Vejby Christensen, H. & Petersen, E. S. Effect of body temperature and hypoxia on the ventilatory CO2 response in man. Respir. Physiol. 19, 322–332 (1973).
Gaudio, R. Effect of cool-dehumidified inspired air on the physiologic responses to a hot, humid environment. Aerosp. Med. 40, 254–257 (1969).
Shibasaki, M., Namba, M., Oshiro, M., Crandall, C. G. & Nakata, H. The effect of elevations in internal temperature on event-related potentials during a simple cognitive task in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 311, R33–R38 (2016).
Whitham, M., Laing, S. J., Jackson, A., Maassen, N. & Walsh, N. P. Effect of exercise with and without a thermal clamp on the plasma heat shock protein 72 response. J. Appl. Physiol. 103, 1251–1256 (2007).
Fujii, N., Danquah, M. O., Meade, R. D., Nishiyasu, T. & Kenny, G. P. The effect of exogenous activation of protease-activated receptor 2 on cutaneous vasodilatation and sweating in young males during rest and exercise in the heat. Temperature 5, 257–266 (2018).
Rutherford, M. M. et al. Effect of extracellular hyperosmolality on sweat rate during metaboreflex activation in passively heated young men. Am. J. Physiol. Regul. Integr. Comp. Physiol. 322, R1–R13 (2022).
Bandopadhyay, P., Banerjee, P. K., Dikshit, M. B. & Iyer, M. E. Effect of glucose electrolyte ingestion on physiological changes due to severe heat stress. Indian J. Physiol. Pharm. 33, 163–167 (1989).
Ganio, M. S. et al. Effect of heat stress on cardiac output and systemic vascular conductance during simulated hemorrhage to presyncope in young men. Am. J. Physiol. Heart Circ. Physiol. 302, H1756–H1761 (2012).
Niimi, Y. et al. Effect of heat stress on muscle sympathetic nerve activity in humans. J. Auton. Nerv. Syst. 63, 61–67 (1997).
Tsuji, B. et al. Effect of hypocapnia on the sensitivity of hyperthermic hyperventilation and the cerebrovascular response in resting heated humans. J. Appl. Physiol. 124, 225–233 (2018).
Crandall, C. G., Levine, B. D. & Etzel, R. A. Effect of increasing central venous pressure during passive heating on skin blood flow. J. Appl. Physiol. 86, 605–610 (1999).
Tsuji, B., Honda, Y., Fujii, N., Kondo, N. & Nishiyasu, T. Effect of initial core temperature on hyperthermic hyperventilation during prolonged submaximal exercise in the heat. Am. J. Physiol. Regul. Integr. Comp. Physiol. 302, R94–R102 (2012).
Iwase, S., Kawahara, Y., Nishimura, N. & Sugenoya, J. Effect of micro mist sauna bathing on thermoregulatory and circulatory functions and thermal sensation in humans. Int. J. Biometeorol. 60, 699–709 (2016).
Ganio, M. S., Brothers, R. M., Shibata, S., Hastings, J. L. & Crandall, C. G. Effect of passive heat stress on arterial stiffness. Exp. Physiol. 96, 919–926 (2011).
Moyen, N. E. et al. Effect of passive heat stress on arterial stiffness in smokers versus non-smokers. Int. J. Biometeorol. 60, 499–506 (2016).
Simmons, S. E., Saxby, B. K., McGlone, F. P. & Jones, D. A. The effect of passive heating and head cooling on perception, cardiovascular function and cognitive performance in the heat. Eur. J. Appl. Physiol. 104, 271–280 (2008).
Coburn, J. W., Reba, R. C. & Craig, F. N. Effect of potassium depletion on response to acute heat exposure in unacclimatized man. Am. J. Physiol. 211, 117–124 (1966).
Iwanaga, K. et al. Effect of precooling on heat tolerance of resting men in a hot environment: comparison with seasonal effect on it. Ann. Physiol. Anthropol. 8, 151–154 (1989).
Brandenberger, G., Follenius, M. & Oyono, S. Effect of propranolol on aldosterone response to heat exposure in sodium-restricted men. J. Endocrinol. Investig. 3, 395–400 (1980).
Opaszowski, B. H., Busko, K. & Blachnio, D. Effect of rehydration on hormonal responses to heat exposure in a Finnish sauna bath. Biol. Sport 18, 193–208 (2001).
Gryka, D., Pilch, W., Szarek, M., Szygula, Z. & Tota, Ł. The effect of sauna bathing on lipid profile in young, physically active, male subjects. Int. J. Occup. Med. Environ. Health 27, 608–618 (2014).
Fujii, N., Tsuji, B., Honda, Y., Kondo, N. & Nishiyasu, T. Effect of short-term exercise-heat acclimation on ventilatory and cerebral blood flow responses to passive heating at rest in humans. J. Appl. Physiol. 119, 435–444 (2015).
Pilch, W., Szygula, Z. & Torii, M. Effect of the sauna-induced thermal stimuli of various intensity on the thermal and hormonal metabolism in women. Biol. Sport 24, 357–373 (2007).
Wilson, T. E. & Ray, C. A. Effect of thermal stress on the vestibulosympathetic reflexes in humans. J. Appl. Physiol. 97, 1367–1370 (2004).
Bundgaard-Nielsen, M., Wilson, T. E., Seifert, T., Secher, N. H. & Crandall, C. G. Effect of volume loading on the Frank-Starling relation during reductions in central blood volume in heat-stressed humans. J. Physiol. 588, 3333–3339 (2010).
Wang, H. et al. Effect of voluntary electric fan use on autonomic and perceptual responses to lower leg passive heating in humans. J. Therm. Biol. 118, 103724–103724 (2023).
Fujii, N. et al. Effect of voluntary hypocapnic hyperventilation on cutaneous circulation in resting heated humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 303, R975–R983 (2012).
Ono, J. et al. Effect of water bath temperature on physiological parameters and subjective sensation in older people. Geriatr. Gerontol. Int. 17, 2164–2170 (2017).
Nakamitsu, S. et al. Effect of water temperature on diuresis-natriuresis: AVP, ANP, and urodilatin during immersion in men. J. Appl. Physiol. 77, 1919–1925 (1994).
Brothers, R. M., Wingo, J. E., Hubing, K. A., Coso Del, J. & Crandall, C. G. Effect of whole body heat stress on peripheral vasoconstriction during leg dependency. J. Appl. Physiol. 107, 1704–1709 (2009).
Wilson, T. E., Cui, J. & Crandall, C. G. Effect of whole-body and local heating on cutaneous vasoconstrictor responses in humans. Auton. Neurosci. 97, 122–128 (2002).
Ray, U. S. & Roy, R. Effect of yoga breathing manuevers (Shitali and Sitkari Pranayama) on heat stress management. Complement Med. Res. 12, 182–188 (2021).
Ko, Y., Kang, J., Seol, S. H. & Lee, J. Y. Effectiveness of skin-heating using a water-perfused suit as passive and post-exercise heat acclimation strategies. J. Therm. Biol. 93, 102703–102703 (2020).
Lovell, R., Madden, L., McNaughton, L. R. & Carroll, S. Effects of active and passive hyperthermia on heat shock protein 70 (HSP70). J. Amino Acids 34, 203–211 (2008).
Wallace, P. J. et al. The effects of acute dopamine reuptake inhibition on cognitive function during passive hyperthermia. Appl Physiol. Nutr. Metab. 46, 511–520 (2021).
Hedley, A. M., Climstein, M. & Hansen, R. The effects of acute heat exposure on muscular strength, muscular endurance, and muscular power in the euhydrated athlete. J. Strength Cond. Res. 16, 353–358 (2002).
Yamazaki, F., Sagawa, S., Torii, R., Endo, Y. & Shiraki, K. Effects of acute hyperthermia on the carotid baroreflex control of heart rate in humans. Int. J. Biometeorol. 40, 200–205 (1997).
Lucas, R. A., Cotter, J. D., Morrison, S. & Ainslie, P. N. The effects of ageing and passive heating on cardiorespiratory and cerebrovascular responses to orthostatic stress in humans. Exp. Physiol. 93, 1104–1117 (2008).
Ota, A. et al. The effects of aging on the distribution of cerebral blood flow with postural changes and mild hyperthermia. Eur. J. Appl. Physiol. 119, 1261–1272 (2019).
Shastry, S., Minson, C. T., Wilson, S. A., Dietz, N. M. & Joyner, M. J. Effects of atropine and L-NAME on cutaneous blood flow during body heating in humans. J. Appl. Physiol. 88, 467–472 (2000).
Suzurikawa, J., Fujimoto, S., Mikami, K., Jonai, H. & Inoue, T. Effects of back cooling with Peltier devices on thermoregulatory responses in a hot environment. IEEJ Trans. Electr. Electron Eng. 11, 832–834 (2016).
Koda, M. et al. Effects of bathing in hot water on portal hemodynamics in healthy subjects and in patients with compensated liver cirrhosis. Intern. Med. 34, 628–631 (1995).
Fujii, N. et al. Effects of chemoreflexes on hyperthermic hyperventilation and cerebral blood velocity in resting heated humans. Exp. Physiol. 93, 994–1001 (2008).
Ohko, H. et al. The effects of endurance exercise combined with high-temperature head-out water immersion on serum concentration of brain-derived neurotrophic factor in healthy young men. Int. J. Hyperth. 38, 1077–1085 (2021).
Kobayashi, Y., Ando, Y., Okuda, N., Takaba, S. & Ohara, K. Effects of endurance training on thermoregulation in females. Med. Sci. Sports Exerc. 12, 361–364 (1980).
Sohar, E., Shoenfeld, Y., Shapiro, Y., Ohry, A. & Cabili, S. Effects of exposure to Finnish sauna. Isr. J. Med. Sci. 12, 1275–1282 (1976).
Mündel, T., Hooper, P. L., Bunn, S. J. & Jones, D. A. The effects of face cooling on the prolactin response and subjective comfort during moderate passive heating in humans. Exp. Physiol. 91, 1007–1014 (2006).
Nakata, H., Namba, M., Kakigi, R. & Shibasaki, M. Effects of face/head and whole body cooling during passive heat stress on human somatosensory processing. Am. J. Physiol. Regul. Integr. Comp. Physiol. 312, R996–R1003 (2017).
Wilson, T. E. et al. Effects of heat and cold stress on central vascular pressure relationships during orthostasis in humans. J. Physiol. 585, 279–285 (2007).
Hohnsbein, J., Piekarski, C., Kampmann, B. & Th, N. Effects of heat on visual acuity. Ergonomics 27, 1239–1246 (1984).
Brothers, R. M., Zhang, R., Wingo, J. E., Hubing, K. A. & Crandall, C. G. Effects of heat stress on dynamic cerebral autoregulation during large fluctuations in arterial blood pressure. J. Appl. Physiol. 107, 1722–1729 (2009).
Cui, J. et al. Effects of heat stress on thermoregulatory responses in congestive heart failure patients. Circulation 112, 2286–2292 (2005).
Dunbar, S. L. & Kenney, W. L. Effects of hormone replacement therapy on hemodynamic responses of postmenopausal women to passive heating. J. Appl. Physiol. 89, 97–103 (2000).
Yamashita, K. & Tochihara, Y. Effects of hyperoxia on thermoregulatory responses during feet immersion to hot water in humans. J. Physiol. Anthropol. Appl. Hum. Sci. 22, 181–185 (2003).
Zuo, C., Luo, L. & Liu, W. Effects of increased humidity on physiological responses, thermal comfort, perceived air quality, and Sick Building Syndrome symptoms at elevated indoor temperatures for subjects in a hot-humid climate. Indoor Air 31, 524–540 (2021).
Iwase, S. et al. Effects of isotonic and isometric exercises with mist sauna bathing on cardiovascular, thermoregulatory, and metabolic functions. Int J. Biometeorol. 58, 1109–1117 (2014).
Hoekstra, S. P. et al. The effects of local versus systemic passive heating on the acute inflammatory, vascular and glycaemic response. Appl. Physiol. Nutr. Metab. 46, 808–818 (2021).
Launay, J. C. et al. Effects of modafinil on heat thermoregulatory responses in humans at rest. Can. J. Physiol. Pharm. 80, 796–803 (2002).
Shastry, S., Dietz, N. M., Halliwill, J. R., Reed, A. S. & Joyner, M. J. Effects of nitric oxide synthase inhibition on cutaneous vasodilation during body heating in humans. J. Appl. Physiol. 85, 830–834 (1998).
Nakata, H., Oshiro, M., Namba, M. & Shibasaki, M. Effects of passive heat stress on human somatosensory processing. Am. J. Physiol. Regul. Integr. Comp. Physiol. 309, R1387–R1396 (2015).
Kuwahara, T. et al. Effects of physical training on heat loss responses of young women to passive heating in relation to menstrual cycle. Eur. J. Appl. Physiol. 94, 376–385 (2005).
Ogawa, Y., Kamijo, Y. I., Ikegawa, S., Masuki, S. & Nose, H. Effects of postural change from supine to head-up tilt on the skin sympathetic nerve activity component synchronised with the cardiac cycle in warmed men. J. Physiol. 595, 1185–1200 (2017).
Strbák, V. et al. Effects of sauna and glucose intake on TSH and thyroid hormone levels in plasma of euthyroid subjects. Metabolism 36, 426–431 (1987).
Brazaitis, M. et al. Effects of severe whole-body hyperthermia on ovarian hormone and extracellular Hsp72 responses in young adult women. Int. J. Hyperth. 36, 660–665 (2019).
Yaicharoen, P., Wallman, K., Morton, A., Bishop, D. & Grove, R. J. The effects of warm-up on intermittent sprint performance in a hot and humid environment. J. Sports Sci. 30, 967–974 (2012).
Faerevik, H. & Reinertsen, R. E. Effects of wearing aircrew protective clothing on physiological and cognitive responses under various ambient conditions. Ergonomics 46, 780–799 (2003).
Pranskunas, A. et al. Effects of whole body heat stress on sublingual microcirculation in healthy humans. Eur. J. Appl Physiol. 115, 157–165 (2015).
Crandall, C. G., Zhang, R. & Levine, B. D. Effects of whole body heating on dynamic baroreflex regulation of heart rate in humans. Am. J. Physiol. Heart Circ. Physiol. 279, H2486–H2492 (2000).
Tan, X. R. et al. Elevated brain temperature under severe heat exposure impairs cortical motor activity and executive function. J. Sport Health Sci. 13, 233–244 (2023).
Morton, J. P. et al. Elevated core and muscle temperature to levels comparable to exercise do not increase heat shock protein content of skeletal muscle of physically active men. Acta Physiol. 190, 319–327 (2007).
Pearson, J., Lucas, R. A. & Crandall, C. G. Elevated local skin temperature impairs cutaneous vasoconstrictor responses to a simulated haemorrhagic challenge while heat stressed. Exp. Physiol. 98, 444–450 (2013).
Pearson, J., Lucas, R. A. I., Schlader, Z. J., Gagnon, D. & Crandall, C. G. Elevated skin and core temperatures both contribute to reductions in tolerance to a simulated haemorrhagic challenge. Exp. Physiol. 102, 255–264 (2017).
Hess, H. W. et al. Elevations in sweat sodium concentration following ischemia-reperfusion injury during passive heat stress. J. Appl Physiol. 134, 1364–1375 (2023).
Brothers, R. M., Ganio, M. S., Hubing, K. A., Hastings, J. L. & Crandall, C. G. End-tidal carbon dioxide tension reflects arterial carbon dioxide tension in the heat-stressed human with and without simulated hemorrhage. Am. J. Physiol. Regul. Integr. Comp. Physiol. 300, R978–R983 (2011).
Shibasaki, M. et al. Endogenous nitric oxide attenuates neutrally mediated cutaneous vasoconstriction. J. Physiol. 585, 627–634 (2007).
Kellogg, D. L., Zhao, J. L. & Wu, Y. Endothelial nitric oxide synthase control mechanisms in the cutaneous vasculature of humans in vivo. Am. J. Physiol. Regul. Integr. Comp. Physiol. 295, H123–H129 (2008).
Trezza, B. M. et al. Environmental heat exposure and cognitive performance in older adults: a controlled trial. Age 37, 43–43 (2015).
Stachenfeld, N. S., Silva, C. & Keefe, D. L. Estrogen modifies the temperature effects of progesterone. J. Appl. Physiol. 88, 1643–1649 (2000).
White, M. D., Johnston, C. E., Wu, M. P., Bristow, G. K. & Giesbrecht, G. G. Ethanol ingestion prolongs orthostatic intolerance in hyperthermic humans. Aviat. Space Environ. Med. 69, 577–582 (1998).
Yamamoto, S., Iwamoto, M., Inoue, M. & Harada, N. Evaluation of the effect of heat exposure on the autonomic nervous system by heart rate variability and urinary catecholamines. J. Occup. Health 49, 199–204 (2007).
Notley, S. R. et al. Evidence for age-related differences in heat acclimatisation responsiveness. Exp. Physiol. 105, 1491–1499 (2020).
Shibasaki, M., Kondo, N. & Crandall, C. G. Evidence for metaboreceptor stimulation of sweating in normothermic and heat-stressed humans. J. Physiol. 534, 605–611 (2001).
Caldwell, H. G. et al. Evidence for temperature-mediated regional increases in cerebral blood flow during exercise. J. Physiol. 598, 1459–1473 (2020).
Galbreath, R. W., Reger, W., Allison, T. & Butler, K. Exceeding recommended standards for safe hot tub use. J. Saf. Res. 30, 7–15 (1999).
Walter, E. et al. Exercise hyperthermia induces greater changes in gastrointestinal permeability than equivalent passive hyperthermia. Physiol. Rep. 9, e14945 (2021).
Fujii, N. et al. Exogenous activation of protease-activated receptor 2 attenuates cutaneous vasodilatation and sweating in older men exercising in the heat. Ski. Pharm. Physiol. 32, 235–243 (2019).
Eimantas, N., Ivanove, S., Solianik, R. & Brazaitis, M. Exposure to acute noxious heat evokes a cardiorespiratory shock response in humans. Int J. Hyperth. 39, 134–143 (2022).
Skinner, B. D., Lucas, R. A. I. & Lucas, S. J. E. Exposure to passive heat and cold stress differentially modulates cerebrovascular-CO(2) responsiveness. J. Appl. Physiol. 136, 23–32 (2024).
Cernych, M. et al. Exposure to total 36-hr sleep deprivation reduces physiological and psychological thermal strain to whole-body uncompensable passive heat stress in young adult men. J. Sleep Res. 30, e13055 (2020).
Schlader, Z. J., O’Leary, M. C., Sackett, J. R. & Johnson, B. D. Face cooling reveals a relative inability to increase cardiac parasympathetic activation during passive heat stress. Exp. Physiol. 103, 701–713 (2018).
Stanhewicz, A. E., Greaney, J. L., Alexander, L. M. & Kenney, W. L. Folic acid supplementation increases cutaneous vasodilator sensitivity to sympathetic nerve activity in older adults. Am. J. Physiol. Regul. Integr. Comp. Physiol. 312, R681–R688 (2017).
Gagnon, D., R, M. B., Ganio, M. S., Hastings, J. L. & Crandall, C. G. Forehead versus forearm skin vascular responses at presyncope in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 307, R908–R913 (2014).
Freemas, J. A. et al. Glomerular filtration rate reserve is reduced during mild passive heat stress in healthy young adults. Am. J. Physiol. Regul. Integr. Comp. Physiol. 323, R340–R350 (2022).
Wong, B. J., Wilkins, B. W. & Minson, C. T. H1 but not H2 histamine receptor activation contributes to the rise in skin blood flow during whole body heating in humans. J. Physiol. 560, 941–948 (2004).
Kukkonen-Harjula, K. et al. Haemodynamic and hormonal responses to heat exposure in a Finnish sauna bath. Eur. J. Appl. Physiol. Occup. Physiol. 58, 543–550 (1989).
Vähä-Eskeli, K. K., Erkkola, R. U., Seppänen, A., Poranen, A.-K. & Säteri, U. Haemodynamic response to moderate thermal stress in pregnancy. Ann. Med. 23, 121–126 (1991).
Kissen, A. T., Summers, W. C., Buehring, W. J., Alexander, M. & Smedley, D. C. Head and neck cooling by air, water, or air plus water in hyperthermia. Aviat. Space Environ. Med. 47, 265–271 (1976).
Gagnon, D. et al. Healthy aging does not compromise the augmentation of cardiac function during heat stress. J. Appl. Physiol. 121, 885–892 (2016).
Bruce-Low, S. S., Cotterrell, D. & Jones, G. E. Heart rate variability during high ambient heat exposure. Aviat. Space Environ. Med. 77, 915–920 (2006).
Yamazaki, F. & Hamasaki, K. Heat acclimation increases skin vasodilation and sweating but not cardiac baroreflex responses in heat-stressed humans. J. Appl. Physiol. 95, 1567–1574 (2003).
Price, M. & Goosey-Tolfrey, V. Heat flow of the paraplegic and able-bodied lower limb during resting heat exposure. J. Therm. Biol. 33, 255–260 (2008).
Gerrett, N., Alkemade, P. & Daanen, H. Heat reacclimation using exercise or hot water immersion. Med. Sci. Sports Exerc. 53, 1517–1528 (2021).
Kumar, Y., Chawla, A. & Tatu, U. Heat shock protein 70 as a biomarker of heat stress in a simulated hot cockpit. Aviat. Space Environ. Med. 74, 711–716 (2003).
Fujii, N., Zhang, S. Y., McNeely, B. D., Nishiyasu, T. & Kenny, G. P. Heat shock protein 90 contributes to cutaneous vasodilation through activating nitric oxide synthase in young male adults exercising in the heat. J. Appl. Physiol. 123, 844–850 (2017).
Fujii, N. et al. Heat shock protein 90 does not contribute to cutaneous vasodilatation in older adults during heat stress. Microcirculation 26, e12541 (2019).
McGarr, G. W., Fujii, N., Schmidt, M. D., Muia, C. M. & Kenny, G. P. Heat shock protein 90 modulates cutaneous vasodilation during an exercise-heat stress, but not during passive whole-body heating in young women. Physiol. Rep. 8, e14552 (2020).
Davis, S. L. & Crandall, C. G. Heat stress alters hemodynamic responses during the Valsalva maneuver. J. Appl. Physiol. 108, 1591–1594 (2010).
Binder, K., Gagnon, D., Lynn, A. G., Kondo, N. & Kenny, G. P. Heat stress attenuates the increase in arterial blood pressure during isometric handgrip exercise. Eur. J. Appl. Physiol. 113, 183–190 (2013).
Cui, J. et al. Heat stress attenuates the increase in arterial blood pressure during the cold pressor test. J. Appl. Physiol. 109, 1354–1359 (2010).
Pearson, J., Ganio, M. S., Lucas, R. A., Babb, T. G. & Crandall, C. G. Heat stress does not augment ventilatory responses to presyncopal limited lower body negative pressure. Exp. Physiol. 98, 1156–1163 (2013).
Keller, D. M., Cui, J., Davis, S. L., Low, D. A. & Crandall, C. G. Heat stress enhances arterial baroreflex control of muscle sympathetic nerve activity via increased sensitivity of burst gating, not burst area, in humans. J. Physiol. 573, 445–451 (2006).
Wilson, T. E., Cui, J., Zhang, R. & Crandall, C. G. Heat stress reduces cerebral blood velocity and markedly impairs orthostatic tolerance in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 291, R1443–R1448 (2006).
Kuhlenhoelter, A. M. et al. Heat therapy promotes the expression of angiogenic regulators in human skeletal muscle. Am. J. Physiol. Regul. Integr. Comp. Physiol. 311, R377–R391 (2016).
Brazaitis, M. et al. Heat transfer and loss by whole-body hyperthermia during severe lower-body heating are impaired in healthy older men. Exp. Gerontol. 96, 12–18 (2017).
Brothers, R. M., Keller, D. M., Wingo, J. E., Ganio, M. S. & Crandall, C. G. Heat-stress-induced changes in central venous pressure do not explain interindividual differences in orthostatic tolerance during heat stress. J. Appl. Physiol. 110, 1283–1289 (2011).
Francisco, M. A. et al. Hemodynamics of post-exercise vs. post hot water immersion recovery. J. Appl. Physiol. 130, 1362–1372 (2021).
Amin, S. B. et al. High-intensity exercise and passive hot water immersion cause similar postintervention changes in peripheral and cerebral shear. J. Appl. Physiol. 133, 390–402 (2022).
Maley, M. J. et al. Hot water immersion acutely reduces peripheral glucose uptake in young healthy males: An exploratory crossover randomized controlled trial. Temperature 10, 434–443 (2023).
Su, Y., Hoekstra, S. P. & Leicht, C. A. Hot water immersion is associated with higher thermal comfort than dry passive heating for a similar rise in rectal temperature and plasma interleukin-6 concentration. Eur. J. Appl. Physiol. 124, 1109–1119 (2023).
Fan, J. L. et al. Human cardiorespiratory and cerebrovascular function during severe passive hyperthermia: effects of mild hypohydration. J. Appl. Physiol. 105, 433–445 (2008).
Miwa, C. et al. Human cardiovascular responses to a 60-min bath at 40 degrees C. Environ. Med. 38, 77–80 (1994).
Schlader, Z. J. et al. Human thermoregulation during prolonged exposure to warm and extremely humid environments expected to occur in disabled submarine scenarios. Am. J. Physiol. Regul. Integr. Comp. Physiol. 318, R950–R960 (2020).
Lucas, R. A., Pearson, J., Schlader, Z. J. & Crandall, C. G. Hypercapnia-induced increases in cerebral blood flow do not improve lower body negative pressure tolerance during hyperthermia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 305, R604–R609 (2013).
Fonseca, S. F. et al. Hypertension is associated with greater heat exchange during exercise recovery in a hot environment. Braz. J. Med. Biol. Res 48, 1122–1129 (2015).
Kenny, G. P. et al. Hyperthermia and cardiovascular strain during an extreme heat exposure in young versus older adults. Temperature 4, 79–88 (2017).
Schlader, Z. J., Lucas, R. A., Pearson, J. & Crandall, C. G. Hyperthermia does not alter the increase in cerebral perfusion during cognitive activation. Exp. Physiol. 98, 1597–1607 (2013).
Vescovi, P. P., Coiro, V., Volpi, R., Giannini, A. & Passeri, M. Hyperthermia in sauna is unable to increase the plasma levels of ACTH/cortisol, beta-endorphin and prolactin in cocaine addicts. J. Endocrinol. Investig. 15, 671–675 (1992).
Brenner, I. K. M. et al. Immune changes in humans during cold exposure: effects of prior heating and exercise. J. Appl. Physiol. 87, 699–710 (1999).
Kaiser, B. W. et al. The impact of elevated body core temperature on critical power as determined by a 3-min all-out test. J. Appl. Physiol. 131, 1543–1551 (2021).
Brenner, I. K., Severs, Y. D., Shek, P. N. & Shephard, R. J. Impact of heat exposure and moderate, intermittent exercise on cytolytic cells. Eur. J. Appl. Physiol. Occup. Physiol. 74, 162–171 (1996).
Petrofsky, J. et al. Impact of hydrotherapy on skin blood flow: How much is due to moisture and how much is due to heat? Physiother. Theory Pr. 26, 107–112 (2010).
Alali, M. H., Vianna, L. C., Lucas, R. A. I., Junejo, R. T. & Fisher, J. P. Impact of whole body passive heat stress and arterial shear rate modification on radial artery function in young men. J. Appl. Physiol. 129, 1373–1382 (2020).
Vescovi, P. P. et al. Impaired ACTH and β-endorphin response to sauna-induced hyperthermia in heroin addicts. Acta Endocrinol. 121, 484–488 (1989).
Green, D. J. et al. Impaired skin blood flow response to environmental heating in chronic heart failure. Eur. Heart J. 27, 338–343 (2006).
Allen, D. R. et al. Impaired sweating responses to a passive whole body heat stress in individuals with multiple sclerosis. J. Neurophysiol. 118, 7–14 (2017).
Petrofsky, J. S., Besonis, C., Rivera, D., Schwab, E. & Lee, S. Impairment in orthostatic tolerance during heat exposure in individuals with Type I and Type II diabetes. Med Sci. Monit. 11, CR153–CR159 (2005).
Greaney, J. L., Stanhewicz, A. E., Proctor, D. N., Alexander, L. M. & Kenney, W. L. Impairments in central cardiovascular function contribute to attenuated reflex vasodilation in aged skin. J. Appl. Physiol. 119, 1411–1420 (2015).
Barry, H. et al. Improved neural control of body temperature following heat acclimation in humans. J. Physiol. 598, 1223–1234 (2020).
Cheng, J. L., Williams, J. S., Hoekstra, S. P. & MacDonald, M. J. Improvements in vascular function in response to acute lower limb heating in young healthy males and females. J. Appl. Physiol. 131, 277–289 (2021).
Tatár, P., Vigas, M., Jurcovicová, J., Kvetnanský, R. & Strec, V. Increased glucagon secretion during hyperthermia in a sauna. Eur. J. Appl Physiol. Occup. Physiol. 55, 315–317 (1986).
Nelson, M. D. et al. Increased left ventricular twist, untwisting rates, and suction maintain global diastolic function during passive heat stress in humans. Am. J. Physiol. Heart Circ. Physiol. 298, H930–H937 (2010).
Amano, T., Inoue, Y., Koga, S., Nishiyasu, T. & Kondo, N. Influence of exercise training with thigh compression on heat-loss responses. Scand. J. Med Sci. Sports 25, 173–182 (2015).
Gryka, D. et al. The influence of Finnish sauna treatments on the concentrations of nitric oxide, 3-nitrotyrosine and selected markers of oxidative status in training and non-training men. Int. J. Occup. Med. Environ. Health 33, 173–185 (2020).
Yamazaki, F., Takahara, K., Sone, R. & Johnson, J. M. Influence of hyperoxia on skin vasomotor control in normothermic and heat-stressed humans. J. Appl. Physiol. 103, 2026–2033 (2007).
Kenny, G. P. et al. Influence of nonthermal baroreceptor modulation of heat loss responses during uncompensable heat stress. Eur. J. Appl. Physiol. 108, 541–548 (2010).
Curtis, A. N., Walsh, M. L. & White, M. D. Influence of passive hyperthermia on human ventilation during rest and isocapnic hypoxia. Appl. Physiol. Nutr. Metab. 32, 721–732 (2007).
Gibbons, T. D. et al. Influence of the mode of heating on cerebral blood flow, non-invasive intracranial pressure and thermal tolerance in humans. J. Physiol. 599, 1977–1996 (2021).
Hussain, J. N., Cohen, M. M., Mantri, N., O’Malley, C. J. & Greaves, R. F. Infrared sauna as exercise-mimetic? Physiological responses to infrared sauna vs exercise in healthy women: A randomized controlled crossover trial. Complement Ther. Med. 64, 102798–102798 (2022).
Crandall, C. G., Shibasaki, M. & Wilson, T. E. Insufficient cutaneous vasoconstriction leading up to and during syncopal symptoms in the heat stressed human. Am. J. Physiol. Heart Circ. Physiol. 299, H1168–H1173 (2010).
D’Souza, A. W., Notley, S. R., Meade, R. D. & Kenny, G. P. Intermittent sequential pneumatic compression does not enhance whole-body heat loss in elderly adults during extreme heat exposure. Appl. Physiol. Nutr. Metab. 44, 1383–1386 (2019).
McGarr, G. W., Fujii, N., Muia, C. M., Nishiyasu, T. & Kenny, G. P. Intradermal administration of atrial natriuretic peptide attenuates cutaneous vasodilation but not sweating in young men during exercise in the heat. Ski. Pharm. Physiol. 33, 86–93 (2020).
Mallette, M. M., Hodges, G. J., McGarr, G. W., Gabriel, D. A. & Cheung, S. S. Investigating the roles of core and local temperature on forearm skin blood flow. Microvasc. Res. 106, 88–95 (2016).
Nelson, M. D. et al. Left ventricular systolic and diastolic function during tilt-table positioning and passive heat stress in humans. Am. J. Physiol. Heart Circ. Physiol. 301, H599–H608 (2011).
Heinonen, I. et al. Local heating, but not indirect whole body heating, increases human skeletal muscle blood flow. J. Appl Physiol. 111, 818–824 (2011).
Chiesa, S. T. et al. Local temperature-sensitive mechanisms are important mediators of limb tissue hyperemia in the heat-stressed human at rest and during small muscle mass exercise. Am. J. Physiol. Heart Circ. Physiol. 309, H369–H380 (2015).
Perry, B. G. & Mündel, T. Lower body positive pressure affects systemic but not cerebral haemodynamics during incremental hyperthermia. Clin. Physiol. Funct. Imaging 41, 226–233 (2021).
Koch Esteves, N., Khir, A. W. & Gonzalez-Alonso, J. Lower limb hyperthermia augments functional hyperaemia during small muscle mass exercise similarly in trained elderly and young humans. Exp. Physiol. 108, 1154–1171 (2023).
Thomas, K. N., van Rij, A. M., Lucas, S. J. E. & Cotter, J. D. Lower-limb hot-water immersion acutely induces beneficial hemodynamic and cardiovascular responses in peripheral arterial disease and healthy, elderly controls. Am. J. Physiol. Regul. Integr. Comp. Physiol. 312, R281–R291 (2017).
Lee, J. F., Harrison, M. L., Brown, S. R. & Brothers, R. M. The magnitude of heat stress-induced reductions in cerebral perfusion does not predict heat stress-induced reductions in tolerance to a simulated hemorrhage. J. Appl. Physiol. 114, 37–44 (2013).
Wilson, T. E., Cui, J. & Crandall, C. G. Mean body temperature does not modulate eccrine sweat rate during upright tilt. J. Appl. Physiol. 98, 1207–1212 (2005).
Crandall, C. G., Vongpatanasin, W. & Victor, R. G. Mechanism of cocaine-induced hyperthermia in humans. Ann. Intern. Med. 136, 785–791 (2002).
McLellan, T. M., Smith, I. F., Gannon, G. A. & Zamecnik, J. Melatonin has no effect on tolerance to uncompensable heat stress in man. Eur. J. Appl. Physiol. 83, 336–343 (2000).
Kenny, G. P. et al. Menstrual cycle and oral contraceptive use do not modify postexercise heat loss responses. J. Appl. Physiol. 105, 1156–1165 (2008).
Meendering, J. R., Torgrimson, B. N., Houghton, B. L., Halliwill, J. R. & Minson, C. T. Menstrual cycle and sex affect hemodynamic responses to combined orthostatic and heat stress. Am. J. Physiol. Heart Circ. Physiol. 289, H631–H642 (2005).
Shibasaki, M. et al. Modelflow underestimates cardiac output in heat-stressed individuals. Am. J. Physiol. Regul. Integr. Comp. Physiol. 300, R486–R491 (2011).
Cui, J. et al. Moderate whole body heating attenuates the exercise pressor reflex responses in older humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 320, R757–R769 (2021).
Aoki, K., Stephens, D. P., Zhao, K., Kosiba, W. A. & Johnson, J. M. Modification of cutaneous vasodilator response to heat stress by daytime exogenous melatonin administration. Am. J. Physiol. Regul. Integr. Comp. Physiol. 291, R619–R624 (2006).
Yamazaki, F. & Sone, R. Modulation of arterial baroreflex control of heart rate by skin cooling and heating in humans. J. Appl. Physiol. 88, 393–400 (2000).
Amano, T. et al. Modulation of muscle metaboreceptor activation upon sweating and cutaneous vascular responses to rising core temperature in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 308, R990–R997 (2015).
Hassan, E. S. Muscle damage and immune responses to prolonged exercise in environmental extreme conditions. J. Sports Med. Phys. Fit. 56, 1206–1213 (2016).
Cui, J., Wilson, T. E. & Crandall, C. G. Muscle sympathetic nerve activity during lower body negative pressure is accentuated in heat-stressed humans. J. Appl. Physiol. 96, 2103–2108 (2004).
Cui, J., Boehmer, J., Blaha, C. & Sinoway, L. I. Muscle sympathetic nerve activity response to heat stress is attenuated in chronic heart failure patients. Am. J. Physiol. Regul. Integr. Comp. Physiol. 312, R873–R882 (2017).
Cui, J. et al. Muscle sympathetic responses during orthostasis in heat-stressed individuals. Clin. Auton. Res. 21, 381–387 (2011).
Rodrigues, P., Trajano, G. S., Wharton, L. & Minett, G. M. Muscle temperature kinetics and thermoregulatory responses to 42 °C hot-water immersion in healthy males and females. Eur. J. Appl. Physiol. 120, 2611–2624 (2020).
Akerman, A. P., Meade, R. D., Notley, S. R., Rutherford, M. M. & Kenny, G. P. Myths and methodologies: reliability of non-invasive estimates of cardiac autonomic modulation during whole-body passive heating. Exp. Physiol. 106, 593–614 (2021).
Shepley, B. R. et al. Negligible influence of moderate to severe hyperthermia on blood-brain barrier permeability and neuronal parenchymal integrity in healthy men. J. Appl. Physiol. 130, 792–800 (2021).
Shibasaki, M., Rasmussen, P., Secher, N. H. & Crandall, C. G. Neural and non-neural control of skin blood flow during isometric handgrip exercise in the heat stressed human. J. Physiol. 587, 2101–2107 (2009).
Engelland, R. E., Hemingway, H. W., Tomasco, O. G., Olivencia-Yurvati, A. H. & Romero, S. A. Neural control of blood pressure is altered following isolated leg heating in aged humans. Am. J. Physiol. Heart Circ. Physiol. 318, H976–H984 (2020).
Racinais, S. & Girard, O. Neuromuscular failure is unlikely to explain the early exercise cessation in hot ambient conditions. Psychophysiology 49, 853–865 (2012).
Kellogg, D. L., Zhao, J. L. & Wu, Y. Neuronal nitric oxide synthase control mechanisms in the cutaneous vasculature of humans in vivo. J. Physiol. 586, 847–857 (2008).
Kellogg, D. L., Zhao, J. L., Wu, Y. & Johnson, J. M. Nitric oxide and receptors for VIP and PACAP in cutaneous active vasodilation during heat stress in humans. J. Appl. Physiol. 113, 1512–1518 (2012).
Hayashi, K. A novel cooling method using carbon dioxide-rich water after passive heating. J. Therm. Biol. 96, 102843–102843 (2021).
Rivas, E., Newmire, D. E. & Ben-Ezra, V. Obese type 2 diabetics have a blunted hypotensive response to acute hyperthermia therapy that does not affect the perception of thermal stress or physiological strain compared to healthy adults. Physiol. Behav. 165, 374–382 (2016).
Caldwell, A. R. et al. Obesity, but not hypohydration, mediates changes in mental task load during passive heating in females. PeerJ 2018, e5394 (2018).
Cui, J., Wilson, T. E. & Crandall, C. G. Orthostatic challenge does not alter skin sympathetic nerve activity in heat-stressed humans. Auton. Neurosci. 116, 54–61 (2004).
Barrera-Ramirez, J., McGinn, R., Carter, M. R., Franco-Lopez, H. & Kenny, G. P. Osmoreceptors do not exhibit a sex-dependent modulation of forearm skin blood flow and sweating. Physiol. Rep. 2, e00226 (2014).
Takamata, A., Nagashima, K., Nose, H. & Morimoto, T. Osmoregulatory inhibition of thermally induced cutaneous vasodilation in passively heated humans. Am. J. Physiol. 273, R197–R204 (1997).
Takamata, A., Mack, G. W., Gillen, C. M., Jozsi, A. C. & Nadel, E. R. Osmoregulatory modulation of thermal sweating in humans - reflex effects of drinking. Am. J. Physiol. Regul. Integr. Comp. Physiol. 268, R414–R422 (1995).
Reed, H. L., Pepper, S., Armstrong, D., Von Tersch, F. J. & Lewis, S. B. Oxygen saturation of brachial venous blood correlates with fingertip temperatures between 11 and 39 degrees C. Aviat. Space Environ. Med. 60, 1068–1071 (1989).
Malcolm, R. A., Cooper, S., Folland, J. P., Tyler, C. J. & Sunderland, C. Passive heat exposure alters perception and executive function. Front. Physiol. 9, 585–585 (2018).
Leppäluoto, J., Arjamaa, O., Vuolteenaho, O. & Ruskoaho, H. Passive heat exposure leads to delayed increase in plasma levels of atrial natriuretic peptide in humans. J. Appl. Physiol. 71, 716–720 (1991).
Brunt, V. E., Eymann, T. M., Francisco, M. A., Howard, M. J. & Minson, C. T. Passive heat therapy improves cutaneous microvascular function in sedentary humans via improved nitric oxide-dependent dilation. J. Appl Physiol. 121, 716–723 (2016).
Brunt, V. E., Howard, M. J., Francisco, M. A., Ely, B. R. & Minson, C. T. Passive heat therapy improves endothelial function, arterial stiffness and blood pressure in sedentary humans. J. Physiol. 594, 5329–5342 (2016).
Morrison, S., Sleivert, G. G. & Cheung, S. S. Passive hyperthermia reduces voluntary activation and isometric force production. Eur. J. Appl. Physiol. 91, 729–736 (2004).
Bender, R. W., Wilson, T. E., Hoffman, R. L. & Clark, B. C. Passive-heat stress does not induce muscle fatigue, central activation failure or changes in intracortical properties of wrist flexors. Ergonomics 54, 565–575 (2011).
Cui, J., Wilson, T. E. & Crandall, C. G. Phenylephrine-induced elevations in arterial blood pressure are attenuated in heat-stressed humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 283, R1221–R1226 (2002).
Watanabe, I., Noro, H., Ohtsuka, Y., Mano, Y. & Agishi, Y. Physical effects of negative air ions in a wet sauna. Int J. Biometeorol. 40, 107–112 (1997).
Shiraki, K., Sagawa, S., Yousef, M. K., Konda, N. & Miki, K. Physiological responses of aged men to head-up tilt during heat exposure. J. Appl Physiol. 63, 576–581 (1987).
Marszalek, A., Smolander, J., Soltynski, K. & Sobolewski, A. Physiological strain of wearing aluminized protective clothing at rest in young, middle-aged, and older men. Int J. Ind. Erg. 25, 195–202 (1999).
Gagnon, D., Romero, S. A., Ngo, H., Poh, P. Y. & Crandall, C. G. Plasma hyperosmolality attenuates skin sympathetic nerve activity during passive heat stress in humans. J. Physiol. 594, 497–506 (2016).
Shibasaki, M., Aoki, K., Morimoto, K., Johnson, J. M. & Takamata, A. Plasma hyperosmolality elevates the internal temperature threshold for active thermoregulatory vasodilation during heat stress in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 297, R1706–R1712 (2009).
Gagnon, D., Romero, S. A., Ngo, H., Poh, P. Y. & Crandall, C. G. Plasma hyperosmolality improves tolerance to combined heat stress and central hypovolemia in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 312, R273–R280 (2017).
Cernych, M., Satas, A. & Brazaitis, M. Post-sauna recovery enhances brain neural network relaxation and improves cognitive economy in oddball tasks. Int. J. Hyperth. 35, 375–382 (2019).
Wilkins, B. W., Martin, E. A., Roberts, S. K. & Joyner, M. J. Preserved reflex cutaneous vasodilation in cystic fibrosis does not include an enhanced nitric oxide-dependent mechanism. J. Appl. Physiol. 102, 2301–2306 (2007).
Rein, E. B., Filtvedt, M., Ræder, J. C. & Walløe, L. Preventing hyperthermia: a cross-over study comparing two negative pressure devices during continuous passive heat stress. J. Med. Eng. Technol. 38, 37–41 (2014).
Low, D., Purvis, A., Reilly, T. & Cable, N. T. The prolactin responses to active and passive heating in man. Exp. Physiol. 90, 909–917 (2005).
McCord, G. R., Cracowski, J. L. & Minson, C. T. Prostanoids contribute to cutaneous active vasodilation in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 291, R596–R602 (2006).
Kamijo, Y. I., Okazaki, K., Ikegawa, S., Okada, Y. & Nose, H. Rapid saline infusion and/or drinking enhance skin sympathetic nerve activity components reduced by hypovolaemia and hyperosmolality in hyperthermia. J. Physiol. 596, 5443–5459 (2018).
Rowell, L. B., Brengelmann, G. L., Blackmon, J. R. & Murray, J. A. Redistribution of blood flow during sustained high skin temperature in resting man. J. Appl. Physiol. 28, 415–420 (1970).
Nelson, M. D. et al. Reductions in cerebral blood flow during passive heat stress in humans: partitioning the mechanisms. J. Physiol. 589, 4053–4064 (2011).
Bain, A. R. et al. Regional changes in brain blood flow during severe passive hyperthermia: effects of PaCO2 and extracranial blood flow. J. Appl. Physiol. 115, 653–659 (2013).
Koch Esteves, N., Gibson, O. R., Khir, A. W. & González‐Alonso, J. Regional thermal hyperemia in the human leg: evidence of the importance of thermosensitive mechanisms in the control of the peripheral circulation. Physiol. Rep. 9, e14953(2021).
Shibasaki, M., Inoue, Y., Kondo, N., Aoki, K. & Hirata, K. Relationship between skin blood flow and sweating rate in prepubertal boys and young men. Acta Physiol. Scand. 167, 105–110 (1999).
Willmott, A. G. B. et al. The reliability of a portable steam sauna pod for the whole-body passive heating of humans. J. Therm. Biol. 118, 103743–103743 (2023).
Chapman, C. L. et al. Renal and segmental artery hemodynamics during whole body passive heating and cooling recovery. J. Appl. Physiol. 127, 974–983 (2019).
Bailey, T. et al. Repeated warm water immersion induces similar cerebrovascular adaptations to 8 weeks of moderate-intensity exercise training in females. Int J. Sports Med. 37, 757–765 (2016).
Tsuji, B. et al. Respiratory mechanics and cerebral blood flow during heat-induced hyperventilation and its voluntary suppression in passively heated humans. Physiol. Rep. 7, e13967 (2019).
Qian, S. W. et al. Resting-state brain activity predicts selective attention deficits during hyperthermia exposure. Int J. Hyperth. 37, 220–230 (2020).
Wilson, T. E. et al. Role of bradykinin type 2 receptors in human sweat secretion: Translational evidence does not support a functional relationship. Ski. Pharm. Physiol. 34, 162–166 (2021).
Shibasaki, M. et al. The role of cardiac sympathetic innervation and skin thermoreceptors on cardiac responses during heat stress. Am. J. Physiol. Heart Circ. Physiol. 308, H1336–H1342 (2015).
Takamata, A., Nagashima, K., Nose, H. & Morimoto, T. Role of plasma osmolality in the delayed onset of thermal cutaneous vasodilation during exercise in humans. Am. J. Physiol. 275, R286–R290 (1998).
Convertino, V. A., Greenleaf, J. E. & Bernauer, E. M. Role of thermal and exercise factors in the mechanism of hypervolemia. J. Appl Physiol. Respir. Environ. Exerc. Physiol. 48, 657–664 (1980).
Wong, B. J. Sensory nerves and nitric oxide contribute to reflex cutaneous vasodilation in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 304, R651–R656 (2013).
McGarr, G. W., Fujii, N., Muia, C. M., Nishiyasu, T. & Kenny, G. P. Separate and combined effects of K(Ca) and K(ATP) channel blockade with NOS inhibition on cutaneous vasodilation and sweating in older men during heat stress. Am. J. Physiol. Regul. Integr. Comp. Physiol. 317, R113–R120 (2019).
Epstein, Y., Udassin, R. & Sack, J. Serum 3,5,3’-triiodothyronine and 3,3’,5’-triiodothyronine concentrations during acute heat load. J. Clin. Endocrinol. Metab. 49, 677–678 (1979).
Jezová, D., Kvetnanský, R. & Vigas, M. Sex differences in endocrine response to hyperthermia in sauna. Acta Physiol. Scand. 150, 293–298 (1994).
Inoue, Y. et al. Sex- and menstrual cycle-related differences in sweating and cutaneous blood flow in response to passive heat exposure. Eur. J. Appl. Physiol. 94, 323–332 (2005).
Hemingway, H. W. et al. Shear stress induced by acute heat exposure is not obligatory to protect against endothelial ischemia-reperfusion injury in humans. J. Appl. Physiol. 132, 199–208 (2022).
Ihsan, M. et al. Skeletal muscle signaling following whole-body and localized heat exposure in humans. Front Physiol. 11, 839–839 (2020).
Wingo, J. E. et al. Skin blood flow and local temperature independently modify sweat rate during passive heat stress in humans. J. Appl. Physiol. 109, 1301–1306 (2010).
Kamijo, Y. et al. Skin sympathetic nerve activity component synchronizing with cardiac cycle is involved in hypovolaemic suppression of cutaneous vasodilatation in hyperthermia. J. Physiol. 589, 6231–6242 (2011).
Leppäluoto, J., Tuominen, M., Väänänen, A., Karpakka, J. & Vuori, J. Some cardiovascular and metabolic effects of repeated sauna bathing. Acta Physiol. Scand. 128, 77–81 (1986).
Cui, J., Zhang, R., Wilson, T. E. & Crandall, C. G. Spectral analysis of muscle sympathetic nerve activity in heat-stressed humans. Am. J. Physiol. Heart Circ. Physiol. 286, H1101–H1106 (2004).
Mallette, M. M., Hodges, G. J., McGarr, G. W., Gabriel, D. A. & Cheung, S. S. Spectral analysis of reflex cutaneous vasodilatation during passive heat stress. Microvasc. Res. 111, 42–48 (2017).
Cui, J. et al. Spectral characteristics of skin sympathetic nerve activity in heat-stressed humans. Am. J. Physiol. Heart Circ. Physiol. 290, H1601–H1609 (2006).
Yamazaki, F., Matsumura, F., Nagata, J., Ando, A. & Imura, T. Spontaneous arterial baroreflex control of the heart rate during head-down tilt in heat-stressed humans. Eur. J. Appl. Physiol. 85, 208–213 (2001).
Collins, K. J., Few, J. D., Forward, T. J. & Giec, L. A. Stimulation of adrenal glucocorticoid secretion in man by raising the body temperature. J. Physiol. 202, 645–660 (1969).
Hori, S., Ihzuka, H. & Nakamura, M. Studies on physiological responses of residents in Okinawa to a hot environment. Jpn J. Physiol. 26, 235–244 (1976).
Thomas, K. N., Van Rij, A. M., Lucas, S. J., Gray, A. R. & Cotter, J. D. Substantive hemodynamic and thermal strain upon completing lower-limb hot-water immersion; comparisons with treadmill running. Temperature 3, 286–297 (2016).
Shibasaki, M., Namba, M., Oshiro, M., Kakigi, R. & Nakata, H. Suppression of cognitive function in hyperthermia; From the viewpoint of executive and inhibitive cognitive processing. Sci. Rep. 7, 43528–43528 (2017).
Gerrett, N., Amano, T., Inoue, Y. & Kondo, N. The sweat glands’ maximum ion reabsorption rates following heat acclimation in healthy older adults. Exp. Physiol. 106, 302–315 (2021).
Lucas, R. A., Ganio, M. S., Pearson, J. & Crandall, C. G. Sweat loss during heat stress contributes to subsequent reductions in lower-body negative pressure tolerance. Exp. Physiol. 98, 473–480 (2013).
Machado-Moreira, C. A., Smith, F. M., van den Heuvel, AN., Mekjavic, IB. & Taylor, NA. & Sweat secretion from the torso during passively-induced and exercise-related hyperthermia. Eur. J. Appl. Physiol. 104, 265–270 (2008).
Sagawa, S., Shiraki, K., Yousef, M. K. & Miki, K. Sweating and cardiovascular responses of aged men to heat exposure. J. Gerontol. 43, M1–M8 (1988).
Gagnon, D., Schlader, Z. J. & Crandall, C. G. Sympathetic activity during passive heat stress in healthy aged humans. J. Physiol. 593, 2225–2235 (2015).
Low, D. A., Keller, D. M., Wingo, J. E., Brothers, R. M. & Crandall, C. G. Sympathetic nerve activity and whole body heat stress in humans. J. Appl. Physiol. 111, 1329–1334 (2011).
Chiesa, S. T., Trangmar, S. J. & González-Alonso, J. Temperature and blood flow distribution in the human leg during passive heat stress. J. Appl. Physiol. 120, 1047–1058 (2016).
Low, D. A. et al. Temporal thermometry fails to track body core temperature during heat stress. Med. Sci. Sports Exerc. 39, 1029–1035 (2007).
Masuda, Y. et al. Thermal and cardiovascular responses and thermal sensation during hot-water bathing and the influence of room temperature. J. Therm. Biol. 82, 83–89 (2019).
Zahorska-Markiewicz, B. Thermal and metabolic responses to heat exposure in obesity. Eur. J. Appl. Physiol. Occup. Physiol. 48, 379–385 (1982).
Ashley, C. D., Lopez, R. M., Garzon-Villalba, X. P. & Bernard, T. E. Thermal exposure limit in a simulated refuge alternative. Min. Met. Explor. 37, 179–186 (2020).
Tochihara, Y., Ohnaka, T. & Nagai, Y. Thermal responses of 6- to 8-year-old children during immersion of their legs in a hot water bath. Appl Hum. Sci. 14, 23–28 (1995).
Takeda, R. et al. Thermal sensation during mild hyperthermia is modulated by acute postural change in humans. Int. J. Biometeorol. 60, 1925–1932 (2016).
Yamazaki, F. & Sone, R. Thermal stress modulates arterial pressure variability and arterial baroreflex response of heart rate during head-up tilt in humans. Eur. J. Appl. Physiol. 84, 350–357 (2001).
Machado-Moreira, C. A. & Taylor, N. A. Thermogenic and psychogenic recruitment of human eccrine sweat glands: variations between glabrous and non-glabrous skin surfaces. J. Therm. Biol. 65, 145–152 (2017).
Schwarck, J. B. et al. Thermogenic and psychogenic sweating in humans: Identifying eccrine glandular recruitment patterns from glabrous and non-glabrous skin surfaces. J. Therm. Biol. 82, 242–251 (2019).
Pallubinsky, H. et al. Thermophysiological adaptations to passive mild heat acclimation. Temperature 4, 176–186 (2017).
Solonin, Y. G. & Katsyuba, E. A. Thermoregulation and blood circulation in adults during short-term exposure to extreme temperatures. Hum. Physiol. 29, 188–194 (2003).
Suzuki, A. et al. Thermoregulatory responses are attenuated after fructose but not glucose intake. Med. Sci. Sports Exerc. 46, 1452–1461 (2014).
Low, D. A., Bailey, T. G., N, T. C. & Jones, H. Thermoregulatory responses to combined moderate heat stress and hypoxia. Microcirculation 23, 487–494 (2016).
Gass, E. M. & Gass, G. C. Thermoregulatory responses to repeated warm water immersion in subjects who are paraplegic. Spinal Cord. 39, 149–155 (2001).
de Korte, J. Q., Eijsvogels, T. M. H., Hopman, M. T. E. & Bongers, C. C. W. G. Thermoregulatory, cardiovascular and perceptual responses of spectators of a simulated football match in hot and humid environmental conditions. Sports 11, 78–78 (2023).
Allison, T. G. & Reger, W. E. Thermoregulatory, cardiovascular, and psychophysical response to alcohol in men in 40degreeC water. J. Appl. Physiol. 72, 2099–2107 (1992).
Kingma, B. R. M., Roijendijk, L. M. M., L, V. M., H, V. R. & Mhph, V. B. Time perception and timed decision task performance during passive heat stress. Temperature 8, 53–63 (2020).
Schlader, Z. J., Rivas, E., Soller, B. R., Convertino, V. A. & Crandall, C. G. Tissue oxygen saturation during hyperthermic progressive central hypovolemia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 307, R731–R736 (2014).
Huang, M. et al. Tolerance to a haemorrhagic challenge during heat stress is improved with inspiratory resistance breathing. Exp. Physiol. 103, 1243–1250 (2018).
Wong, B. J. & Fieger, S. M. Transient receptor potential vanilloid type 1 channels contribute to reflex cutaneous vasodilation in humans. J. Appl. Physiol. 112, 2037–2042 (2012).
Fujii, N. et al. TRPV4 channel blockade does not modulate skin vasodilation and sweating during hyperthermia or cutaneous postocclusive reactive and thermal hyperemia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 320, R563–R573 (2021).
Koulmann, N. et al. Use of bioelectrical impedance analysis to estimate body fluid compartments after acute variations of the body hydration level. Med. Sci. Sports Exerc. 32, 857–864 (2000).
Ganio, M. S., Brothers, R. M., Lucas, R. A., Hastings, J. L. & Crandall, C. G. Validity of auscultatory and Penaz blood pressure measurements during profound heat stress alone and with an orthostatic challenge. Am. J. Physiol. Regul. Integr. Comp. Physiol. 301, R1510–R1516 (2011).
Lee, J. F. et al. Variability in orthostatic tolerance during heat stress: cerebrovascular reactivity to arterial carbon dioxide. Aviat. Space Environ. Med. 85, 624–630 (2014).
Abraham, P., Leftheriotis, G., Desvaux, B., Saumet, M. & Saumet, J. L. Venous return in lower-limb during heat-stress. Am. J. Physiol. Heart Circ. Physiol. 267, H1337–H1340 (1994).
Zhao, M., Kuklane, K., Lundgren, K., Gao, C. & Wang, F. A ventilation cooling shirt worn during office work in a hot climate: Cool or not? Int. J. Occup. Saf. Erg. 21, 457–463 (2015).
Wilson, T. E., Kuipers, N. T., McHugh, E. A. & Ray, C. A. Vestibular activation does not influence skin sympathetic nerve responses during whole body heating. J. Appl. Physiol. 97, 540–544 (2004).
Kellogg, D. L., Zhao, J. L., Wu, Y. & Johnson, J. M. VIP/PACAP receptor mediation of cutaneous active vasodilation during heat stress in humans. J. Appl. Physiol. 109, 95–100 (2010).
Kimura, T. et al. Warmer environments increase implicit mental workload even If learning efficiency is enhanced. Front. Psychol. 11, 568 (2020).
Fujii, N. et al. Wearing graduated compression stockings augments cutaneous vasodilation in heat-stressed resting humans. Eur. J. Appl. Physiol. 117, 921–929 (2017).
Kimball, A. L., McCue, P. M., Petrie, M. A. & Shields, R. K. Whole body heat exposure modulates acute glucose metabolism. Int. J. Hyperth. 35, 644–651 (2018).
Cui, J. et al. Whole body heat stress attenuates baroreflex control of muscle sympathetic nerve activity during postexercise muscle ischemia. J. Appl. Physiol. 106, 1125–1131 (2009).
Cui, J., Blaha, C. & Sinoway, L. I. Whole body heat stress attenuates the pressure response to muscle metaboreceptor stimulation in humans. J. Appl. Physiol. 121, 1178–1186 (2016).
Littmann, A. E. & Shields, R. K. Whole body heat stress increases motor cortical excitability and skill acquisition in humans. Clin. Neurophysiol. 127, 1521–1529 (2016).
Yamazaki, F. et al. Whole body heating reduces the baroreflex response of sympathetic nerve activity during Valsalva straining. Auton. Neurosci. 103, 93–99 (2003).
Yamazaki, F., Nakayama, Y. & Sone, R. Whole-body heating decreases skin vascular response to low orthostatic stress in the lower extremities. J. Physiol. Sci. 56, 157–164 (2006).
Yamazaki, F. & Sone, R. Whole-body heating slows carotid baroreflex response in human subjects. Eur. J. Appl. Physiol. 94, 690–696 (2005).
Ferreira, F. C. et al. Women have a greater cardiac vagal withdrawal to heat stress compared to men. Temperature 10, 444–453 (2023).
National Heart Lung and Blood Institue (NHLBI). Quality Assessment Tool for before-after (pre-post) studies with no control group. in Study Quality Assessment Tools (ed. (NIH), N.I.o.H.) (National Insitutes of Health (NIH), 2014).
Sterne, J. A. C. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898 (2019).
Rowell, L. B., Detry, J. R., Profant, G. R. & Wyss, C. Splanchnic vasoconstriction in hyperthermic man–role of falling blood pressure. J. Appl. Physiol. 31, 864–869 (1971).
Chou, T.-H. & Coyle, E. F. Cardiovascular responses to hot skin at rest and during exercise. Temperature 10, 326–357 (2023).
Rowell, L. B., Murray, J. A., Brengelmann, G. L. & Kraning, K. K. 2nd Human cardiovascular adjustments to rapid changes in skin temperature during exercise. Circ. Res. 24, 711–724 (1969).
Risch, W. D., Koubenec, H. J., Gauer, O. H. & Lange, S. Time course of cardiac distension with rapid immersion in a thermo-neutral bath. Pflugers Arch. 374, 119–120 (1978).
Park, K. S., Choi, J. K. & Park, Y. S. Cardiovascular regulation during water immersion. Appl. Hum. Sci. 18, 233–241 (1999).
Christie, J. L. et al. Cardiovascular regulation during head-out water immersion exercise. J. Appl. Physiol. 69, 657–664 (1990).
McGregor, G. R., Bessmoulin, P., Ebi, K. L. & Menne, B. Heatwaves and health: guidance on warning-system development (World Meteorological Organization and World Health Organization, 2015).
Thygesen, K. et al. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 40, 237–269 (2019).
Rawlings, A. M. et al. Association of orthostatic hypotension with incident dementia, stroke, and cognitive decline. Neurology 91, e759–e768 (2018).
Yatsuya, H. et al. Postural changes in blood pressure and incidence of ischemic stroke subtypes: the ARIC study. Hypertension 57, 167–173 (2011).
Zhu, X. et al. Hourly heat exposure and acute ischemic stroke. JAMA Netw. Open 7, e240627 (2024).
Meade, R. D., Notley, S. R. & Kenny, G. P. Aging and human heat dissipation during exercise-heat stress: an update and future directions. Curr. Opin. Physiol. 10, 219–225 (2019).
Foster, J., Hodder, S. G., Lloyd, A. B. & Havenith, G. Individual responses to heat stress: implications for hyperthermia and physical work capacity. Front. Physiol. 11, 541483 (2020).
Meade, R. D. et al. Exploring the contribution of inter-individual factors to the development of physiological heat strain in older adults exposed to simulated indoor overheating. Appl. Physiol. Nutr. Metab. 49, 1252–1270 (2024).
Meade, R. D., Notley, S. R. & Kenny, G. P. Time to reach equilibrium deep body temperatures in young and older adults resting in the heat: a descriptive secondary analysis. Am. J. Physiol. Regul. Integr. Comp. Physiol. 327, R369–R377 (2024).
Xu, Z. et al. Multimorbidity and emergency hospitalisations during hot weather. EBioMedicine 104, 105148 (2024).
Xi, D. et al. Risk factors associated with heatwave mortality in Chinese adults over 65 years. Nat. Med. 30, 1489–1498 (2024).
Turner, V. K., Middel, A. & Vanos, J. K. Shade is an essential solution for hotter cities. Nature 619, 694–697 (2023).
McKenna, Z. J. et al. Age alters the thermoregulatory responses to extreme heat exposure with accompanying activities of daily living. J. Appl. Physiol. 135, 445–455 (2023).
Rowell, L. B., Marx, H. J., Bruce, R. A., Conn, R. D. & Kusumi, F. Reductions in cardiac output, central blood volume, and stroke volume with thermal stress in normal men during exercise. J. Clin. Investig. 45, 1801–1816 (1966).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of interventions (Wiley-Blackwell, 2019).
Morgan, R. L., Whaley, P., Thayer, K. A. & Schunemann, H. J. Identifying the PECO: a framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 121, 1027–1031 (2018).
Taylor, N. A., Tipton, M. J. & Kenny, G. P. Considerations for the measurement of core, skin and mean body temperatures. J. Therm. Biol. 46, 72–101 (2014).
Covidence systematic review software. Available at www.covidence.org (Veritas Health Innovation, 2020).
Reynolds, A. N., Akerman, A. P. & Mann, J. Dietary fibre and whole grains in diabetes management: Systematic review and meta-analyses. PLoS Med. 17, e1003053 (2020).
WebPlotDigitizer. Available at https://automeris.io/ (Rohatgi, A., 2017).
Borenstein, M., Hedges, L. V., Higgins, J. P. & Rothstein, H. R. Introduction to meta-analysis, (John Wiley & Sons, 2021).
Pustejovsky, J. E. & Tipton, E. Meta-analysis with robust variance estimation: expanding the range of working models. Prev. Sci. 23, 425–438 (2022).
Hedges, L. V., Tipton, E. & Johnson, M. C. Robust variance estimation in meta-regression with dependent effect size estimates. Res. Synth. Methods 1, 39–65 (2010).
Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 36, 1–48 (2010).
Assink, M. & Wibbelink, C. J. Fitting three-level meta-analytic models in R: a step-by-step tutorial. Quant. Methods Psychol. 12, 154–174 (2016).
Van den Noortgate, W., Lopez-Lopez, J. A., Marin-Martinez, F. & Sanchez-Meca, J. Three-level meta-analysis of dependent effect sizes. Behav. Res. Methods 45, 576–594 (2013).
Bozdogan, H. Model selection and Akaike’s information criterion (AIC): the general theory and its analytical extensions. Psychometrika 52, 345–370 (1987).
Zuur, A. F., Ieno, E. N., Walker, N. J., Saveliev, A. A. & Smith, G. M. Mixed Effects Models and Extensions in Ecology with R (Springer, 2009).
Tipton, E. & Pustejovsky, J. E. Small-sample adjustments for tests of moderators and model fit using robust variance estimation in meta-regression. J. Educ. Behav. Stat. 40, 604–634 (2015).
Tipton, E. Small sample adjustments for robust variance estimation with meta-regression. Psychol. Methods 20, 375–393 (2015).
Cochran, W. G. The combination of estimates from different experiments. Biometrics 10, 101–129 (1954).
Borenstein, M., Higgins, J. P., Hedges, L. V. & Rothstein, H. R. Basics of meta-analysis: I(2) is not an absolute measure of heterogeneity. Res Synth. Methods 8, 5–18 (2017).
Borenstein, M. Avoiding common mistakes in meta-analysis: Understanding the distinct roles of Q, I-squared, tau-squared, and the prediction interval in reporting heterogeneity. Res. Synth. Methods 15, 354–368 (2023).
Viechtbauer, W. & Cheung, M. W. Outlier and influence diagnostics for meta-analysis. Res Synth. Methods 1, 112–125 (2010).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634 (1997).
Kottek, M., Grieser, J., Beck, C., Rudolf, B. & Rubel, F. World map of the Köppen-Geiger climate classification updated 15, 259–263 (2006).
Harrell, F. E. Regression Modeling Strategies: with Applications to Linear Models, Logistic Regression, and Survival Analysis (Springer, 2001).
NOAA. Heat index, Vol. 2024 (National Oceanic and Atmospheric Administration 2023).
Wickham, H. et al. Welcome to the Tidyverse. J. Open Source Softw. 4, 1686 (2019).
Pustejovsky, J. clubSandwich: Cluster‐robust (sandwich) Variance Estimators with Small‐Sample Corrections. R Package Version 0.2.3 (R Foundation for Statistical Computing, 2017).
Lüdecke, D., Ben-Shachar, M. S., Patil, I., Waggoner, P. & Makowski, D. performance: an R package for assessment, comparison and testing of statistical models. J. Open Source Softw. 6, 3139 (2021).
Harrell, F. E. Jr, Harrell, M. F. E. Jr & Hmisc, D. Package ‘rms’. Vanderbilt Univ. 229, Q8 (2017).
Wickham, H. ggplot2. Wiley Interdiscip. Rev. Comput. Stat. 3, 180–185 (2011).
Aphalo, P. J. ggpmisc: Miscellaneous extensions to ‘ggplot2’. R package version 0.3.1. https://cran.r-project.org/web/packages/ggpmisc/index.html (2021).
Van den Brand, T. ggh4x: Hacks for “ggplot2.”. R Package version 0.2.1. https://cran.r-project.org/web/packages/ggh4x/index.html (2021).
Pedersen, T. L. patchwork: The Composer of Plots. R package version 1.1.1. https://CRAN.R-project.org/package=patchwork (2020).
Van Buuren, S. & Groothuis-Oudshoorn, K. Multivariate imputation by chained equations. J. Stat. Softw. 45, 1–67 (2011).
Baddeley, A., Rubak, E. & Turner, R. Spatial Point Patterns: Methodology and Applications with R (CRC press, 2015).
Massicotte, P. & South, A. naturalearth: World Map Data from Natural Earth. R package version 0.3.4. https://cran.r-project.org/web/packages/rnaturalearth/index.html (2023).
Garnier, S. et al. viridis (Lite)-Colorblind-Friendly Color Maps for R. R package version 0.6.4. https://cran.r-project.org/web/packages/viridis/index.html (2023).
Government of Canada. Hourly Data Report for June 29, 2021—Lytton, British Columbia, Vol. 2024 (Government of Canada, 2024).
Reuters. Thai Authorities Issue Extreme Heat Warnings for Dozens of Provinces (Reuters, 2023).
Domensino, B. Heat index hits 66C at Persian Gulf International Airport https://www.weatherzone.com.au/news/heat-index-hits-66c-at-persiangulf-international-airport/1392522 (Weatherzone, 2023).
Debnath, R., Bardhan, R. & Bell, M. L. Lethal heatwaves are challenging India’s sustainable development. PLOS Climate 2, e0000156 (2023).
Debnath, R. Email communication with Robert D Meade. (2024).
Acknowledgements
We are indebted to all the authors who provided data for inclusion in the review. We would also like to thank Samah Saci (Human and Environmental Physiology Research Unit) for her contributions to article screening and Profs. Heather Baer (Harvard T.H. Chan School of Public Health) and Stefania Papatheodorou (Rutgers School of Public Health) for their guidance during the completion of this work. This work was funded by the Canadian Institutes of Health Research Project Grant (399434, G.P.K., and PJT—180242, G.P.K., R.D.M., S.R.N., and A.P.A.) and the Human and Environmental Physiology Research Unit (G.P.K., all funding support was used to support postdoctoral fellows’ salaries).
Author information
Authors and Affiliations
Contributions
R.D.M., A.P.A., S.R.N., and G.P.K. conceived the research question. R.D.M., A.P.A., S.R.N., G.W.M., E.R.M., J.T.C., J.D.C., C.G.C., and G.P.K. designed the review. R.D.M. and A.P.A. performed systematic searches. R.D.M., A.P.A., S.R.N., G.W.M., E.R.M., and N.V.K. screened report titles, abstracts, and full texts, performed data extraction, and conducted quality and risk of bias assessments. R.D.M. and E.R.M. contacted authors for additional data. R.D.M. and A.Z. developed statistical analyses. R.D.M. performed analyses, created data visualizations, drafted the article and was responsible for project supervision. R.D.M., A.P.A., S.R.N., G.W.M., E.R.M., N.V.K., J.T.C., J.D.C., C.G.C., A.Z., and G.P.K. revised the article for important intellectual content and approved the final submission. All persons designated as authors meet the Nature Portfolio journals criteria for authorship, and all those who qualify are listed. Each author’s roles and responsibilities were agreed upon prior to the start of this work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Zhiwei Xu, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Meade, R.D., Akerman, A.P., Notley, S.R. et al. Meta-analysis of heat-induced changes in cardiac function from over 400 laboratory-based heat exposure studies. Nat Commun 16, 2543 (2025). https://doi.org/10.1038/s41467-025-57868-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-57868-6
This article is cited by
-
The environmental exposome in heart failure risk and progression
Nature Reviews Cardiology (2026)
