
Abstract
Vitiligo, a chronic autoimmune skin disorder characterized by refractory depigmentation, has inconsistent associations with various biomarkers and diseases due to confounding factors. Here, we conduct a comprehensive umbrella review and comparative analysis to evaluate the validity and strength of evidence from observational studies on vitiligo. 103 meta-analyses and 150 Mendelian randomization (MR) analyses are included, spanning categories including cardiometabolism, cancer, autoimmune, dermatosis, psychiatry/neurology/senses, and biomarkers/lifestyle. Evidence grading reveals seven convincing meta-analysis findings: five factors (fasting blood glucose, Graves’ disease, thyroid antibodies, cataracts, and glaucoma) are associated with an increased risk of vitiligo, while vitiligo is related to two conditions (a decreased risk of overall cancer and an increased risk of inflammatory bowel disease). Future similar research is unlikely to alter these findings according to fail-safe number. Among them, the protective effect of vitiligo on overall cancer risk is also supported by causal associations from MR evidence, indicating a reassuring cancer risk in vitiligo. This study establishes an evidence hierarchy for vitiligo, which may inform multidisciplinary management strategies.
Similar content being viewed by others


Introduction
Vitiligo is a chronic autoimmune skin disease characterized by refractory depigmentation affecting approximately 1.3% of the adult population1. The typical clinical manifestation of vitiligo is white, non-scaly patches which significantly affect patients’ emotional well-being, daily life, and psychosocial health2. Emerging research increasingly recognizes that the effect of vitiligo in the body extends beyond its cutaneous manifestations, as it may be accompanied by elevated biomarkers, organ-specific diseases, and even systemic conditions, such as thyroid disorders and metabolic syndrome3,4. Observational studies have identified numerous potential associations between vitiligo and diseases, biomarkers, and risk or protective factors. Categorizing and assessing the credibility of these associations is crucial for advancing the understanding of and improving existing management strategies.
However, evidence supporting these associations varies greatly. This lack of clarity hinders the development of comprehensive and evidence-based management strategies for patients with vitiligo. These observational studies may be subject to biases such as residual confounding, excess significance bias, and selective reporting, which could potentially overestimate the observed effect sizes5,6. Even meta-analyses that aim to synthesize existing evidence, may yield conflicting conclusions. As an observational method, Mendelian randomization (MR) studies provide unbiased effect estimates and minimize the influence of reverse causation and confounding factors commonly encountered in epidemiological settings by leveraging genetic variations as proxies for exposure7. However, for the same association in MR studies on vitiligo, two different results can be obtained owing to variations in data sources and the selection criteria for instrumental variables8,9. Therefore, both approaches lack rigorous evidence with respect to validity and strength.
In this study, we performed a comprehensive umbrella review to establish an evidence hierarchy and systematically evaluate observational associations and causal relationships reported in meta-analyses and MR studies. This dual-direction evaluation encompassed: (1) exposures as risk/protective factors for vitiligo, and (2) vitiligo itself as a risk/protective factor for other conditions. By integrating and comparing findings from meta-analyses and MR analyses, we aimed to provide more robust evidence and deepen the understanding of vitiligo as a complex and multifaceted disease.
Results
Selection and characteristics of included meta-analyses
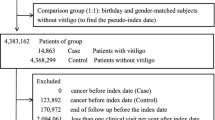
Based on an initial search across four databases for observational systematic reviews and meta-analyses (SRMAs) on vitiligo, 8674 articles were identified (Fig. 1). Following the exclusion of duplicate and irrelevant studies, 46 SRMAs were eligible for overlapping associations screening. Ultimately, 103 unique associations derived from 28 SRMAs were retained for the main analysis. Detailed reasons for the inclusion and exclusion of overlapping associations are provided in Supplementary Data 1.

Flow diagram visually summarizing the screening and selection processes. A Screening for eligible observational meta-analyses. B Screening for eligible Mendelian randomization studies. Abbreviations: SRMA, systematic review and meta-analysis; MR, Mendelian randomization; DMRdb, Disease-centric Mendelian Randomization database.
These 103 meta-analyses investigated the associations between 85 exposures and vitiligo, in addition to the associations between vitiligo and 18 outcomes. These associations could be categorized as follows: cardiometabolism (n = 19, including 18 exposures and 1 outcome); cancer (n = 4, all outcomes); autoimmune (n = 25, including 20 exposures and 5 outcomes); dermatosis (n = 11, including 4 exposures and 7 outcomes); psychiatry/neurology/senses (n = 20, all exposures); biomarkers/lifestyle (n = 23, all exposures); and other (n = 1, 1 outcome, achalasia) (Fig. 2). The number of primary studies per association ranged from 2 to 31. Three associations included only cohort studies, reporting effect sizes as hazard ratios, whereas others included case-control, cross-sectional, cohort baseline, or mixed designs, with effect sizes reported as mean difference, standardized mean difference, odds ratio (OR), or risk ratio (RR).

A Associations between 85 factors and the risk of vitiligo. B Associations between vitiligo and the risk of 18 conditions. Different colors represent different categories, and the size of the circles for factors/conditions indicates the strength of evidence—larger circles correspond to stronger evidence. AITD autoimmune thyroid disease, GD Grave’s disease, HT Hashimoto’s thyroiditis, TPOAb anti-thyroperoxidase antibodies, TgAb anti-thyroglobulin antibodies, T1DM diabetes mellitus type 1, AAA anti-adrenal antibodies, MS multiple sclerosis, MG Myasthenia gravis, SS Sjogren’s syndrome, RA sheumatoid arthritis, SLE systemic lupus erythematosus, ANA antinuclear antibodies, AMA anti-mitochondrial antibody, ASMA anti-smooth muscle antibody, UC ulcerative colitis, IBD inflammatory bowel disease, PA Pernicious anemia, APCA anti-parietal cell antibody, BMI Body Mass Index, MetS metabolic syndrome, DM diabetes mellitus, HOMA-IR Homeostatic Model Assessment of Insulin Resistance, FBG fasting blood glucose, HDL high-density lipoprotein, LDL low-density lipoprotein, TC total cholesterol, TG triglyceride, HTN hypertension, DBP Diastolic Blood Pressure, SBP Systolic Blood Pressure, AA alopecia areata, AD atopic dermatitis, LS lichen sclerosus, LP lichen planus, CU chronic urticaria, LPP lichen planopilaris, DLE discoid lupus erythematosus, NMSC non-melanoma skin cancer, RPE retinal pigment epithelium, TFBUT tear film breakup time, OSDI Ocular Surface Disease Index, SFCT subfoveal choroidal thickness, IOP intra-ocular pressure, SOD superoxide dismutase, GPx glutathione peroxidase, MDA Malondialdehyde, CRP C-reactive protein, VC vitamin C, VE vitamin E, VD vitamin D, 25(OH)D 25-hydroxyvitamin D, 25(OH)D3 25-hydroxyvitamin D3, VB12 vitamin B12, SRD substance−related disorder, ARD alcohol−related disorder.
Summary effect size and heterogeneity between studies
Each meta-analysis was reanalyzed and the detailed results of the 103 associations are presented in Supplementary Data 2 and Supplementary Figs. 1–103. Among the 103 associations, 67 (65.05%) had statistically significant pooled random-effect estimates (P < 0.05) (Table 1). Among the 67 significant associations, 57 involved exposures related to vitiligo, and 10 were outcomes. Of the 57 exposures, 13 were identified as protective factors, whereas the remaining 44 were risk factors. In terms of the 10 outcomes, vitiligo was found to be a protective factor for one—overall cancer—whereas it was associated with increased risk in the remaining 9. Upon applying stricter thresholds (P < 10⁻³ and P < 10⁻⁶), which are considered to substantially reduce false positive findings10,11,12,13, 39 (37.86%) and 17 (16.50%) associations, respectively, remained significant.
Among the 103 associations, 63 (61.17%) and 28 (27.18%) showed substantial (I² > 50%) and low (I² < 25%) heterogeneities, respectively. Among the 77 meta-analyses eligible for the 95% prediction interval (PI) calculation (containing more than two primary studies), 9 (11.69%) excluded null effects.
Small study effects and excess significance bias
Among the 19 meta-analyses where Egger’s test yielded a P-value < 0.10, 13 included a sufficient number of studies (n ≥ 10) to ensure adequate statistical power for robust bias detection14. Moreover, evidence for small-study effects (the P-value of Egger’s test < 0.10 and pooled random effects estimate larger than the point estimate of the largest study in the meta-analysis) were identified in 11 associations.
Among the 67 significant associations, only 2 (0.03%) exhibited an excess significance bias (P < 0.10). When credibility ceilings of 5, 10, 15, and 20% were applied, 59 (88.06%), 61 (91.04%), 61 (91.04%), and 63 (94.03%) associations, respectively, remained significant.
Study quality assessment
The quality of the 28 SRMAs was assessed using the A MeaSurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)15 checklist (Supplementary Data 3). Two were rated as high, whereas the remaining (26) were classified as low or critically low. One of the reasons for the low or critically low quality of these 26 SRMAs was the failure by 25 (96.15%) to meet the criterion of regarding the presentation of a list of excluded studies, considered a critical flaw by AMSTAR 2. The quality of 19 SRMAs improved when this specific criterion was exempted, with 7 and 1 rated as moderate and high quality, respectively.
Grading of evidence
The 103 associations were graded as convincing (7; 6.80%), highly suggestive (7; 6.80%), suggestive (13; 12.62%), weak (40; 38.83%), and non-significant (36; 34.95%) (Table 1 and Supplementary Data 2).
Among the 85 associations investigating exposures related to vitiligo, 5 (5.88%) were supported by convincing evidence, 5 (5.88%) by highly suggestive evidence, 9 (10.59%) by suggestive evidence, 38 (44.71%) were classified as weak, and 28 (32.94%) were non-significant. Of the 85 exposures, 18 were cardiometabolic-related: only fasting blood glucose presented convincing evidence (higher fasting blood glucose was associated with a higher risk of vitiligo), while triglyceride levels showed suggestive evidence (higher triglyceride levels were associated with a lower risk of vitiligo). Body mass index, waist circumference, diabetes mellitus, dyslipidemia, phospholipid levels, and hypertension were not associated with a higher risk of vitiligo. The remaining 10 cardiometabolic factors were graded as weak evidence. Twenty exposures were autoimmune-related: 2—Grave’s disease and thyroid antibodies—were classified as convincing evidence; 4 as highly suggestive; 3 as suggestive; 7 as weak; and 7 as not significant. Regarding skin disease associations, both alopecia areata and atopic dermatitis provided suggestive evidence, whereas psoriasis showed weak evidence. In the psychiatry/neurology/senses associations, cataracts and glaucoma were identified as having convincing evidence of associations with vitiligo, while retinal pigment epithelium (RPE) change was classified as having highly suggestive evidence; sensorineural hypoacusis was found to have weak evidence; anxiety and anxiety disorders were classified as having weak evidence; and depression showed weak evidence, whereas depression disorders were not significantly associated with vitiligo. In the biomarker and lifestyle categories, only vitamin D and zinc were classified as having suggestive evidence, while 12 associations were considered to have weak evidence and 9 were not significant. The weak associations included 10 biomarkers (malondialdehyde, regulatory T cells [Treg]’ frequency, FOXP3, interleukin [IL]−10, IL-17, C-reactive protein, vitamin E, 25-hydroxyvitamin D, vitamin B12, and copper) and two lifestyle factors (alcohol consumption and smoking).
Of the 18 associations examining vitiligo as a potential risk or protective factor for other conditions, 2 (11.11%) were supported by convincing evidence, 2 (11.11%) by highly suggestive evidence, 4 (22.22%) by suggestive evidence, 2 (11.11%) were classified as showing weak evidence, and 8 (44.44%) were non-significant. The 18 outcomes were primarily distributed across categories such as cardiometabolism, cancer, autoimmune, dermatosis, and other. In terms of cardiometabolic outcomes, vitiligo was classified as having highly suggestive evidence for its association with diabetes. In cancer associations, vitiligo was identified as a protective factor against overall cancer, which was graded as convincing evidence; vitiligo was a risk factor for thyroid cancer, supported by suggestive evidence; and no significant association was found between vitiligo and non-melanoma skin cancer or melanoma. In autoimmune conditions, vitiligo was considered as a risk factor for inflammatory bowel disease and celiac disease, graded as having convincing and highly suggestive evidence, respectively. In dermatosis, vitiligo was classified as a risk factor for atopic dermatitis, psoriasis, and lichen sclerosus, wherein all three were graded as having suggestive evidence; the associations between vitiligo and alopecia areata/lichen planus were rated as having weak evidence. In the other group, no significant association was found between vitiligo and the risk of achalasia.
Sensitivity analysis
The sensitivity analyses of study quality, ethnicity, and study design are presented in Supplementary Data 4, 5, and 6, respectively. High-quality original studies (Newcastle–Ottawa Scale [NOS] score ≥7) were pooled, revealing that 17 analyses had altered evidence levels. Among these, three analyses were upgraded, including associations with autoimmune thyroid disease (AITD), systemic lupus erythematosus, and RPE changes. The sensitivity analysis of European populations showed 13 changes, with no upgrades. In the sensitivity analysis of study design, no changes in the evidence grading were observed between results from all available studies and those restricted to cohort studies.
Meta-regression analysis
Meta-regression analyses were conducted to explore the moderating effects of various factors, including study year, mean age, and the proportion of females, on the associations. Results were primarily related to cardiometabolism. The results showed that the association between fasting blood glucose and vitiligo strengthened with more recent study years, with a slope of 0.05 (95% confidence interval [CI] = [0.02, 0.09]). Similarly, the association between systolic blood pressure and vitiligo also increased with study year (slope = 0.08, 95% CI = [0.00, 0.16]). The meta-regression analysis also revealed that high-density lipoprotein (HDL) had a slightly stronger protective effect with increasing age (slope = 0.02, 95% CI = [0.00, 0.05]). Regarding diastolic blood pressure, the percentage of females in the study was positively associated with the strength of the relationship with vitiligo (slope = 2.18, 95% CI = [0.43, 3.93]). Additional meta-regression results are provided in Supplementary Data 7.
Number of additional studies required to change the current meta-analytic evidence
Among the 67 meta-analyses that provided convincing, highly suggestive, suggestive, and weak evidence, the median fail-safe number (FSN) was 115, with a wide range from 2 to 2509. When stratified by the strength of evidence, the median FSN was 170 (ranging from 17 to 367) for convincing evidence, 40 (ranging from 16 to 602) for highly suggestive evidence, 324 (ranging from 6 to 2250) for suggestive evidence, and 78 (ranging from 2 to 2509) for weak evidence (Supplementary Data 8).
In the 27 meta-analyses graded as providing convincing, highly suggestive, or suggestive evidence, the FSN consistently exceeded the number of included primary studies, indicating that the statistical significance of these summary estimates is unlikely to be altered by the addition of more studies with null results. Among the 40 meta-analyses with weak evidence, 4 (10%) (the associations between anti-adrenal antibodies/antinuclear antibodies/pernicious anemia/alcohol consumption and vitiligo) had an FSN that was equal to or smaller than the number of included primary studies, which suggests that these associations may be more susceptible to change.
MR studies
The initial literature search identified 119 articles (Fig. 1). Following the removal of duplicate and irrelevant studies, 30 MR studies were included. Additionally, 12 available MR results were extracted from the Disease-centric Mendelian Randomization database (DMRdb)16 by comparing the 103 associations reported in the meta-analyses. The results from the DMRdb were combined with the associations generated from 30 MR studies to screen for overlap, yielding 150 unique associations. A detailed list of the study selection process is provided in Supplementary Data 9.
All MR studies were derived from European populations with quality scores of 8–10 stars, indicating high research quality (Supplementary Data 10). The MR results were categorized into six major groups based on the associations from meta-analyses. However, some MR results were classified into other categories, including blood counts, infection markers, metabolites, microorganisms, and environmental factors. The 150 associations were classified as follows: robust evidence (n = 14), probable evidence (n = 72), suggestive evidence (n = 6), insufficient evidence (n = 57), or non-evaluable (n = 1). Among the 14 associations with robust evidence, there were 7 outcomes: type 1 diabetes mellitus, cardiovascular disease, psoriasis arthritis, non-melanoma skin cancer, basal cell carcinoma, squamous cell carcinoma, and melanoma, as well as 7 exposures: BAFF-R on CD20 − CD38 − B cells, CD28 + CD45RA- CD8dim T cell %T cells, folate, coffee intake, EBV ZEBRA antibody, 1,5-anhydroglucitol, and mannitol. All MR results are listed in Supplementary Data 11.
Comparative analysis between meta-analyses and MR studies
After thoroughly comparing the results of the meta-analyses and MR analyses, we identified 35 associations from the meta-analyses and 53 from the MR analyses that could be directly compared. A detailed comparison of the results is provided in (Supplementary Data 12). Six associations were significant in both methods (Fig. 3): three exposures (AITD, triglycerides, and depression) and three outcomes (alopecia areata, psoriasis, and overall cancer [MR provided results for lung, liver, ovarian, breast, and kidney cancers]). However, these associations were not simultaneously graded as the highest level of evidence in both meta-analysis and MR studies.

There are six pairs of associations that are significant and directionally consistent across both meta-analysis and MR studies, irrespective of evidence grades. Published MR studies provide associations of vitiligo with lung, liver, ovarian, kidney, and breast cancers, rather than with overall cancer. N denotes the number of primary studies included in meta-analyses and the number of single-nucleotide polymorphisms used as instruments in MR analyses. Blue squares represent the effect sizes from meta-analyses, and green squares represent the effect sizes from MR studies. Meta-analyses are conducted using a random-effects model. All statistical tests are two-sided and unadjusted for multiple comparisons. MR data are directly sourced from published studies and not calculated in this analysis. Source data are provided as a Source Data file. MR Mendelian randomization, OR odd ratio, HR hazard ratio, SMD standardized mean difference; ES effect size, CI confidence interval, AITD autoimmune thyroid disease, TG triglyceride, AA alopecia areata.
No additional or consistent evidence emerged from subgroup comparisons of European populations.
Bridging the evidence gap: MR analyses of convincing meta-analytic findings
Seven convincing associations were identified, supported by meta-analyses: five factors —fasting blood glucose, Graves’ disease, thyroid antibodies, cataracts, and glaucoma—were associated with an increased risk of vitiligo, whereas vitiligo itself was related to two conditions—a decreased risk of overall cancer and an increased risk of inflammatory bowel disease (see Table 2 for details). Among these seven associations, the causal relationships between Graves’ disease, cataracts, glaucoma, and vitiligo have been investigated in MR studies but were graded as insufficient evidence. No MR study has investigated the causal relationship between vitiligo and overall cancer, although MR studies have explored the causal relationships between vitiligo and cancers in specific anatomical sites. Additionally, the causal relationships between fasting blood glucose and vitiligo, thyroid antibodies and vitiligo, and vitiligo and inflammatory bowel disease have not yet been addressed in MR studies.
To fill this gap in the existing evidence, we conducted MR studies to explore the causal relationships between fasting blood glucose and vitiligo, vitiligo and overall cancer, and vitiligo and inflammatory bowel disease (the causal relationship between thyroid antibodies and vitiligo was not analyzed due to the lack of available single nucleotide polymorphisms [SNPs]). The results indicated that vitiligo is causally associated with a reduced risk of overall cancer (inverse variance weighted [IVW] OR = 0.96, 95% CI = [0.94, 0.97]) (Supplementary Data 13). SNPs commonly associated with cancer-related risk factors such as smoking and those directly linked to cancer were excluded, and the final instrumental variables used are listed in Supplementary Data 14. Sensitivity analyses showed that the weighted median, simple mode, and weighted mode methods yielded results similar to the IVW method. However, MR-Egger was not significant, and thus, the evidence was rated as probable evidence. No evidence of directional pleiotropy was found using either the MR-Egger intercept (P = 0.611) or MR-PRESSO (P = 0.115). Furthermore, no heterogeneity was observed. In the leave-one-out analysis, excluding individual SNPs from the main two-sample MR analysis did not affect the robustness of the primary results (Supplementary Fig. 104). No causal association was found between fasting blood glucose and vitiligo or between vitiligo and inflammatory bowel disease. The meta-analysis results for the convincing associations and the MR findings are compared in Fig. 4.

After conducting three additional MR studies to bridge the evidence gap, six convincing meta-analytic associations were explored in MR analyses. The MR analysis confirmed a causal relationship between vitiligo and a reduced risk of overall cancer, which were rated as probable evidence. N denotes the number of primary studies included in meta-analyses and the number of single-nucleotide polymorphisms used as instruments in MR analyses. Blue squares represent the effect sizes from meta-analyses, and green squares represent the effect sizes from MR studies. Meta-analyses are conducted using a random-effects model. All statistical tests are two-sided and unadjusted for multiple comparisons. MR data of GD to vitiligo, cataract to vitiligo, and glaucoma to vitiligo are directly sourced from published studies and not calculated in this analysis. For FBG to vitiligo, vitiligo to IBD, and vitiligo to overall cancer, MR analyses are conducted using the inverse-variance weighted method, as these were not available in published studies. Source data are provided as a Source Data file. MR Mendelian randomization, OR odd ratio, HR hazard ratio, SMD standardized mean difference, ES effect size, FBG fasting blood glucose, GD Grave’s disease, IBD inflammatory bowel disease, ES effect size, CI confidence interval.
Discussion
In this comprehensive umbrella review, we reanalyzed 103 observational associations of vitiligo reported in meta-analyses and systematic reviews across six categories: cardiometabolism, cancer, autoimmune, dermatosis, psychiatry/neurology/senses, and biomarkers/lifestyle factors. Seven associations were graded as having convincing evidence: five factors associated with vitiligo risk (fasting blood glucose, Graves’ disease, thyroid antibodies, cataracts, and glaucoma) and two wherein vitiligo was linked to the risk of two other conditions (overall cancer and inflammatory bowel disease).
Among the 103 meta-analyses, 67 (65.05%) were statistically significant using the random-effects model. However, the potential for bias necessitates cautious interpretation17. Thus, we conducted a series of statistical tests and sensitivity analyses to examine the stability of these associations. Based on varying conditions, namely P < 10⁻⁶, a sample size of >1000 cases, P < 0.05 in the largest study, I² < 50%, absence of small study effects, a PI excluding the null, no evidence of excess significance bias, and P < 0.05 under a 10% credibility ceiling, 67 associations were identified with considerable uncertainty. Therefore, assessing causal relationships using MR studies may be necessary. Observational studies provide evidence of a correlation for MR, which, in turn, helps validate causal relationships18.
We found that vitiligo may have a potential protective effect against certain internal cancers, namely ovarian, lung, liver, kidney, and breast cancers. This result is based on convincing evidence from meta-analyses as well as probable and suggestive evidence from MR studies. A recently published cohort study involving 25,008 patients with vitiligo also reached similar conclusions regarding cancer risk19. Previous genome-wide association studies have identified multiple genetic susceptibility loci associated with the development of vitiligo, including HLA genes involved in abnormal antigen presentation, the FOXP3 gene related to immune suppression, and the GZMB gene associated with T-cell cytotoxicity20,21. These genetic variants may exert protective effects against tumor development. Moreover, Tregs are present in almost all cancers and represent a major mechanism of tumor immune evasion22,23. Some studies have also found that patients with vitiligo exhibit fewer Tregs and a weaker IL-10 signaling pathway24, which was also observed in our study. This downregulation of immune suppression may render tumors more vulnerable to immune attacks. The appearance of vitiligo on the skin may indicate reduced susceptibility to certain internal cancers. In clinical practice, this finding allows the adjustment of cancer risk assessment strategies based on the patient’s vitiligo status, thereby providing a potential biomarker for cancer risk evaluation. This insight may offer potential directions for personalized disease management and the development of advanced anticancer therapeutic strategies.
Interestingly, although several MR studies have suggested that vitiligo may have a protective effect against the development of non-melanoma and melanoma skin cancers25,26,27, epidemiological studies have not reached a consistent conclusion28,29,30. This discrepancy indicates that this issue remains controversial. Based on the best available evidence, our umbrella review of meta-analysis results indicates that vitiligo does not confer protective effects against skin tumors, including melanoma, which share similar antigens targeted by vitiligo-associated CD8 + T cells. However, MR studies have also suggested the presence of such protective effects. This discrepancy is understandable from the perspective of skin tumor pathogenesis. As the body’s first barrier against external environmental factors, the skin is influenced by various exposures, such as sunlight, friction, and chemicals. Ultraviolet (UV) radiation can induce DNA damage in skin cells, triggering carcinogenesis31 and activating Tregs to exert immunosuppressive effects. UV exposure is a major factor in skin cancer development, and factors such as friction are critical contributors to melanoma formation. In patients with vitiligo, the impact of environmental factors on skin tumor development may significantly outweigh the genetic predisposition associated with the disease.
Metabolic syndrome is characterized by abdominal obesity, insulin resistance, hypertension, and dyslipidemia32. Among its components, our study presents convincing evidence of an association between vitiligo and elevated fasting glucose levels. Additionally, the association between vitiligo and diabetes is supported by highly suggestive evidence, but MR studies did not show significant results, suggesting a lack of robust causality. However, the causal relationship between type 1 diabetes and vitiligo was significant and bidirectional. For triglycerides, the association was significant according to both study approaches; however, the levels of evidence were rated as suggestive and probable, indicating the potential of bias. These findings suggest that the confirmation of these associations requires further investigation and robust evidence. Although an increasing number of studies have highlighted the relationship between vitiligo and metabolic syndrome33,34, our study indicated that not all components show consistently strong associations. The underlying mechanisms may involve similarities in the pathophysiological processes shared by vitiligo, such as genetic predisposition, pro-inflammatory signaling pathways, and increased oxidative stress35. Further large-scale longitudinal studies, MR analyses, and molecular mechanistic studies are required to clarify the causal relationships underlying these associations. Therefore, in the clinical management of cardiometabolic health in patients with vitiligo, findings of impaired glucose metabolism and dyslipidemia should attract attention, particularly elevated fasting glucose levels, because these associations are supported by strong evidence.
Our findings largely confirm previous findings, primarily within the autoimmune category. Numerous studies have repeatedly emphasized the close relationship between AITDs and vitiligo36,37. In our umbrella review, Graves’ disease and thyroid antibodies were classified based on convincing evidence. Although the MR results could not identify the specific type of AITDs contributing to the genetic predisposition to vitiligo, we recommend that screening for thyroid antibodies should be included as a routine examination for patients with vitiligo to monitor potential thyroid dysfunction. In addition, the association between vitiligo and inflammatory bowel disease has been graded as convincing evidence, although no relevant MR studies have been conducted to verify the causal relationship further. Whether this association involves overlapping autoimmune mechanisms or pathways and whether it arises from genetic evidence or modifiable non-genetic factors is unclear, attention to gastrointestinal conditions in patients with vitiligo is warranted.
We identified convincing evidence supporting the associations of two ocular diseases (glaucoma and cataract) with vitiligo, whereas MR studies did not show significant causal relationships. This suggests that these two ocular diseases may not have a direct causal relationship with vitiligo and that the potential reverse causal relationship remains unclear. One possible explanation is that these associations could be linked to RPE change, which was classified as highly suggestive evidence in our study. Melanocytes are present in the RPE38, and a CD8 + T cell-mediated attack on melanocytes is a hallmark of vitiligo39. Dysfunctional changes in the RPE may exacerbate intraocular metabolic dysregulation. Further research is required to explore the mechanisms underlying these associations.
The meta-regression analysis results suggest that factors such as study year, sex ratio, and age might play a moderating role in the relationship between cardiometabolism exposures and vitiligo. Our analysis found that compared to earlier studies, more recent research has shown stronger associations between exposures such as fasting blood glucose, systolic blood pressure, and HDL with vitiligo. These changes might be partly attributed to a growing recognition of vitiligo as a disease linked to other systems, along with the increasing incorporation of various indicators and tests into the management and research of vitiligo patients. Furthermore, age and sex might modulate the relationship between certain cardiometabolic indicators and vitiligo, underscoring the importance of considering these demographic factors in both health management across the life course and study design.
Despite being a comprehensive umbrella review providing one of the most extensive evaluations of observational associations in vitiligo research, our study has some limitations that are worth mentioning. First, the methodological framework of umbrella reviews inherently relies on the synthesis of existing SRMAs. This reliance may result in the systematic exclusion of recently published primary studies that have not yet been incorporated into the SRMAs. Second, according to the AMSTAR 2 assessment, the low quality of these SRMAs was primarily due to the failure to meet the criterion regarding the provision of a list of excluded studies. However, in the process of screening overlapping associations, we carefully examined each SRMA for every exposure-outcome pair and selected the SRMA that included the largest number of primary studies for re-analysis. This approach helped mitigate the potential issue of important primary studies being overlooked due to insufficient literature search and selection in the original SRMAs. Additionally, by conducting a re-analysis of all meta-analyses, we were able to identify and address potential statistical errors in the original SRMAs. Despite these efforts, we recommend conducting more robust and methodologically sound systematic reviews to provide stricter and more reliable evidence regarding these associations. Third, not all meta-analyses included corresponding MR studies to interpret causality. Although MR research has emerged as a growing area of interest with an increasing number of publications, we recommend that MR studies be designed and conducted based on epidemiological research results. The results of MR studies that lack biological plausibility or are unsupported by observational studies should be interpreted with caution. Future research should aim to strengthen the evidence base by incorporating high-quality systematic reviews and well-designed MR studies. Further intervention and causal studies are required, along with extensive collaboration, to conduct investigations involving larger and more diverse populations to achieve more definitive conclusions and enhance the generalizability of findings.
In conclusion, this umbrella review provides a comprehensive evaluation of the observational evidence related to vitiligo and compares the observed associations with genetic causal estimates available from MR analyses, wherever possible. Based on the best available evidence, we compiled an evidence hierarchy that holds the potential to offer valuable guidance for the future integrated management of patients with vitiligo.
Methods
Study design
This study followed PRISMA guidelines (Supplementary Data 15) and was registered in PROSPERO (CRD42024609508). Observational meta-analyses served as the main analysis, and their findings were compared with results from MR studies. The entire workflow is shown in Fig. 5 and Supplementary Fig. 105.

Flow diagram illustrating the data analysis procedures for different types of studies. MR Mendelian randomization, FSN fail-safe number.
Data search and selection
We systematically searched PubMed, Embase, Web of Science, and the Cochrane Library for observational SRMAs and MR studies on vitiligo up to November 5, 2024. Detailed search strategies are provided in Supplementary Method 1. Two independent researchers screened titles, abstracts, and full texts, resolving discrepancies through discussion with a third researcher. The reference lists of all included studies were manually reviewed to identify any potentially eligible studies. Additionally, in order to obtain more comparisons, we supplemented our analysis with MR results from the DMRdb16, based on the results from included meta-analyses.
We included SRMAs that provided pooled effect sizes evaluating associations between vitiligo and risk or protective factors, biomarkers, or comorbidities using case-control, cross-sectional, or cohort studies. For studies on diseases, both those evaluating vitiligo as an exposure and an outcome were included. Narrative reviews, studies without synthesized data, and those with insufficient data for analysis, original research articles, and conference abstracts were excluded. Language restrictions were not imposed.
For the MR studies, eligibility required an assessment of causal relationships between vitiligo and risk or protective factors, biomarkers, or comorbidities. Similarly, MR studies that analyzed vitiligo as either an exposure or an outcome were included. Studies using data from two non-overlapping populations of the same ethnicity were included40; others were excluded.
Overlapping associations screening
We distinguished between associations where vitiligo was considered an outcome (i.e., lifestyle, biomarkers, or conditions as exposures) and those where vitiligo was considered an exposure (i.e., other conditions as outcomes). We screened for overlapping associations to identify instances where multiple SRMAs addressed the same association (exposure-outcome pairs), in order to avoid redundancy. If more than one SRMA reported the same association, we prioritized the one with the highest number of primary studies that involved non-overlapping populations41,42. In cases where multiple SRMAs included the same number of primary studies, we selected the SRMA with a higher number of cohort studies, a larger sample size, and more recent publications. For MR studies, we selected those providing the best available evidence based on the data sources for exposure and outcome, sample size, and quality of instrumental variables. Two researchers independently conducted the article’s inclusion and exclusion criteria, and disagreements were resolved through discussion with a third researcher.
Data extraction
Two authors independently extracted the following data for each SRMA, including the first author’s name, publication year, exposure, outcome, quality assessment tool, number of cases, number of original studies, design of the original studies, analytical metrics, maximum adjusted effect estimate from individual studies, and 95% CI.
For MR studies, data included the first author’s name, publication year, exposure, outcome, sources of exposure and outcome, ethnicity of exposure and outcome populations, criteria for single nucleotide polymorphism (SNP) selection, number of SNPs, MR analysis method, OR with a corresponding 95% CI or beta value, and P value. Data extraction was performed independently by two researchers, followed by crosschecking to ensure accuracy.
Data analysis
The statistical hypotheses were defined based on the directionality of each association. For analyses where vitiligo was the outcome (i.e., evaluating exposures as risk/protective factors for vitiligo), the null hypothesis (H₀) stated no association between the exposure and vitiligo, while the alternative hypothesis (H₁) posited a statistically significant association (two-sided test). For analyses where vitiligo was the exposure (i.e., examining vitiligo as a risk/protective factor for other conditions), H₀ assumed no association between vitiligo and the outcome, with H₁ asserting a significant link. We re-analyzed each SRMA using available studies that involved non-overlapping populations, employing effect metrics (such as OR and RR) consistent with those used in the original studies. A random-effects model, based on the DerSimonian–Laird method, was applied. Pooled effect estimates and P values were calculated using effect estimates and 95% CIs from individual studies, with statistical significance defined as P < 0.05. Heterogeneity was assessed using I2 and τ2 statistics, where τ2 quantified the true variation in the summary effect estimate, while I2 measured the proportion of variance attributable to true differences in effect sizes. Heterogeneity was considered substantial if I2 > 50%.
Small study effect was considered present when both the Egger regression asymmetry test indicated publication bias (P < 0.10), and the random effects summary effect size was larger than the effect size reported in the largest study within the meta-analysis. For meta-analyses with more than two studies, outliers were identified and removed to recalculated pooled effect estimates. Additionally, 95% PIs were computed to reflect the range of expected effect sizes in future studies.
We applied credibility ceilings of 5%, 10%, 15%, and 20% in each meta-analysis to account for the potential methodological limitations in observational studies that could result in spurious findings43. Additionally, we assessed the excess significance bias, which is a measure of publication bias that compares the expected number of statistically significant studies with the observed number44. Excess significance bias was considered significant at P < 0.10.
Study quality assessment
The AMSTAR 2 tool was used to assess the quality of observational SRMAs15. In each meta-analysis, primary studies reporting NOS scores of ≥7 were classified as high quality. When alternative tools were used or quality assessments were absent, we independently evaluated studies using the NOS. For MR studies, quality was assessed following the Strengthening the Reporting of Mendelian Randomization Studies guidelines40,45. All quality assessments were conducted independently by two researchers, with disagreements resolved through discussion with a third.
Evidence grading
Meta-analyses were categorized into five levels based on their strength and robustness: convincing (Class I), highly suggestive (Class II), suggestive (Class III), weak (Class IV), and not significant (NS), following the approach used in previous umbrella reviews46,47. Specifically, the evidence grading criteria were as follows: If the association was supported by a highly significant random-effects (P < 10⁻⁶, a threshold considered to substantially reduce false positive findings)10,11,12,13, a sample size of more than 1000 cases, P < 0.05 in the largest study, I² < 50%, absence of small study effects, a PI excluding the null, no evidence of excess significance bias, and P < 0.05 under a 10% credibility ceiling, it was classified as robust evidence; highly suggestive evidence was considered when more than 1,000 cases were included, and a highly significant random-effects (P < 10⁻⁶) was observed; associations with a random-effects P < 10−3 and more than 1000 cases were graded as suggestive evidence; the remaining significant associations with P < 0.05 were considered weak evidence.
For MR studies, we adopted the evidence grading from previous MR reviews48, classifying evidence as robust, probable, suggestive, and insufficient (Supplementary Fig. 106).
Sensitivity analysis
In this umbrella review, sensitivity analyses were conducted to evaluate the effects of study quality, ethnicity, and study design on the results and evidence grading. First, we restricted the analysis to high-quality original studies (NOS ≥ 7) to assess differences from the main analysis and their impact on evidence grading. Second, sensitivity analyses were performed including only studies involving European populations to investigate the potential influence of ethnicity on evidence classification. Additionally, after reviewing the designs of the primary studies included in each SRMA, we focused exclusively on cohort studies, excluding other study designs. This aimed to identify discrepancies between results from all available studies and those restricted to cohort studies. Notably, studies where both exposure and outcome were solely derived from baseline data in cohort studies were not classified as true cohort studies.
Sensitivity analyses of MR studies were incorporated into the evidence grading process to evaluate the robustness and reliability of the results.
Meta-regression analysis
For meta-analyses that included 10 or more primary studies, we conducted random-effects meta-regression analyses to explore potential influence of factors including study year, mean age, and the proportion of females on the associations observed in the main analysis. The year, mean age or the proportion of females was used as the moderator (independent variable) in the analysis, employing the restricted maximum likelihood approach.
Calculation of FSN
In statistically significant meta-analyses, we estimated the number of future studies of average null effect and average weight required to render the overall summary estimate non-significant by calculating Rosenberg’s FSN49. A larger FSN indicates that a substantial number of unpublished, non-significant studies would be needed to nullify the observed effect, suggesting that the current meta-analytic findings are more robust and less likely to be overturned50,51. We calculated the median FSN and its range for each level of evidence (convincing, highly suggestive, suggestive, and weak), and compared these values with the number of included primary studies in each meta-analysis.
Comparative analysis
We compared statistical significance, directional consistency, and evidence grading for associations examined in both meta-analyses and MR studies. As all MR studies involved European populations, ethnicity-specific subgroup results from the meta-analyses were compared with MR study findings to identify additional results from the same background.
Additional MR analyses of meta-analytically convincing evidence
For associations rated as convincing (Class I) in the meta-analyses, we systematically assessed the availability of comparable MR studies. In cases where no suitable MR evidence was identified, we conducted additional MR analyses to address the gap in causal inference. Detailed methodologies for these additional analyses are provided in Supplementary Method 2.
All statistical analyses were conducted using R (version 4.4.1; R Foundation, Vienna, Austria) with the “meta”, “metafor”, “TwoSampleMR” and “MRPRESSO” packages. All the tests were two-sided.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The data used to support the findings of this study are collected from already published studies and are available within the article and its supplementary information. Source data are provided with this paper. Data collection form is available at the figshare (https://doi.org/10.6084/m9.figshare.29377397). Source data are provided with this paper.
Code availability
The analysis code has been publicly available in an open-access repository (https://github.com/Alexxyz123/umbrella-review-of-vitiligo).
References
Bibeau, K. et al. Vitiligo prevalence and quality of life among adults in Europe, Japan and the USA. J. Eur. Acad. Dermatol. Venereology: JEADV 36, 1831–1844 (2022).
Bibeau, K. et al. Mental health and psychosocial quality-of-life burden among patients with vitiligo: findings from the global VALIANT Study. JAMA Dermatol. 159, 1124–1128 (2023).
Chuang, K. W. & Chang, H. C. Association between vitiligo and metabolic syndrome: A systematic review and meta-analysis. J. der Dtsch. Dermatologischen Ges. = J. Ger. Soc. Dermatology: JDDG 20, 218–221 (2022).
Park, S. K. et al. Association between eight autoimmune diseases and thyroid cancer: a nationwide cohort study. Thyroid.: Off. J. Am. Thyroid. Assoc. 34, 206–214 (2024).
Ioannidis, J. P. Why most discovered true associations are inflated. Epidemiol. (Camb., Mass.) 19, 640–648 (2008).
Ioannidis, J. P. Why most published research findings are false. PLoS Med. 2, e124 (2005).
Emdin, C. A., Khera, A. V. & Kathiresan, S. Mendelian randomization. Jama 318, 1925–1926 (2017).
Liu, J., Xu, Y., Liu, Y., Zhu, Y. & Li, X. Associations between type 1 diabetes and autoimmune skin diseases: Mendelian randomization analysis. Heliyon 10, e32781 (2024).
Zhao, L., Hu, M. & Li, L. Identifying the genetic associations between diabetes mellitus and the risk of vitiligo. Clin., Cosmet. investigational Dermatol. 17, 2261–2271 (2024).
Johnson, V. E. Revised standards for statistical evidence. Proc. Natl Acad. Sci. USA 110, 19313–19317 (2013).
Benjamin, D. J. et al. Redefine statistical significance. Nat. Hum. Behav. 2, 6–10 (2018).
Sterne, J. A. & Davey Smith, G. Sifting the evidence-what’s wrong with significance tests?. BMJ (Clin. Res. ed.) 322, 226–231 (2001).
Janiaud, P. et al. Validity of observational evidence on putative risk and protective factors: appraisal of 3744 meta-analyses on 57 topics. BMC Med. 19, 157 (2021).
Sterne, J. A. et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ (Clin. Res. ed.) 343, d4002 (2011).
Shea, B. J. et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ (Clin. Res. ed.) 358, j4008 (2017).
Zheng, X. et al. DMRdb: a disease-centric Mendelian randomization database for systematically assessing causal relationships of diseases with genes, proteins, CpG sites, metabolites and other diseases. Nucleic Acids Res.https://doi.org/10.1093/nar/gkae853 (2024).
Yang, Z. et al. Maternal adiposity and perinatal and offspring outcomes: an umbrella review. Nat. Hum. Behav. 8, 2406–2422 (2024).
Cui, H. et al. Risk factors for prostate cancer: An umbrella review of prospective observational studies and mendelian randomization analyses. PLoS Med. 21, e1004362 (2024).
Schonmann, Y., Cohen, N. T. & Czarnowicki, T. Evaluating cancer risk in a large cohort of 25,008 patients with vitiligo: Insights from a comprehensive cohort population-based study. J. Am. Acad. Dermatology, https://doi.org/10.1016/j.jaad.2024.11.043 (2024).
Jin, Y. et al. Genome-wide association studies of autoimmune vitiligo identify 23 new risk loci and highlight key pathways and regulatory variants. Nat. Genet. 48, 1418–1424 (2016).
Shen, C. et al. Genetic Susceptibility to Vitiligo: GWAS Approaches for Identifying Vitiligo Susceptibility Genes and Loci. Front. Genet. 7, 3 (2016).
Moreno Ayala, M. A., Li, Z. & DuPage, M. Treg programming and therapeutic reprogramming in cancer. Immunology 157, 198–209 (2019).
Kang, J. H. & Zappasodi, R. Modulating Treg stability to improve cancer immunotherapy. Trends cancer 9, 911–927 (2023).
Liu, Y. et al. The emerging role of regulatory T cells in the immunopathogenesis of vitiligo and implications for treatment. Br. J. Dermatol. https://doi.org/10.1093/bjd/ljae472 (2024).
Rashid, S. et al. Mendelian Randomization Analysis reveals Inverse Genetic Risks between Skin Cancers and Vitiligo. JID innovations: Ski. Sci. molecules Popul. health 3, 100217 (2023).
Wen, Y. et al. Cancer risks in patients with vitiligo: a Mendelian randomization study. J. cancer Res. Clin. Oncol. 146, 1933–1940 (2020).
Qian, H., Gong, R., Li, Y., Zhu, J. & Wang, L. A genetically informed study reveals modifiable pathways in skin cancer. J. Transl. Med. 22, 916 (2024).
Ferguson, J., Eleftheriadou, V. & Nesnas, J. Risk of melanoma and nonmelanoma skin cancer in people with vitiligo: united kingdom population-based cohort study. J. investigative Dermatol. 143, 2204–2210 (2023).
Kim, H. S. et al. The incidence and survival of melanoma and nonmelanoma skin cancer in patients with vitiligo: a nationwide population-based matched cohort study in Korea. Br. J. Dermatol. 182, 907–915 (2020).
Paradisi, A. et al. Markedly reduced incidence of melanoma and nonmelanoma skin cancer in a nonconcurrent cohort of 10,040 patients with vitiligo. J. Am. Acad. Dermatol. 71, 1110–1116 (2014).
Pfeifer, G. P. & Besaratinia, A. UV wavelength-dependent DNA damage and human non-melanoma and melanoma skin cancer. Photochemical photobiological Sci.: Off. J. Eur. Photochemistry Assoc. Eur. Soc. Photobiol. 11, 90–97 (2012).
Ndumele, C. E. et al. Cardiovascular-kidney-metabolic health: a presidential advisory from the american heart association. Circulation 148, 1606–1635 (2023).
Lee, J. H. et al. Comorbidities in Patients with Vitiligo: A Systematic Review and Meta-Analysis. J. investigative Dermatol. 143, 777–789.e776 (2023).
Kang, P., Zhang, W. G., Ji, Z. H., Shao, Z. J. & Li, C. Y. Association between vitiligo and relevant components of metabolic syndrome: a systematic review and meta-analysis. J. der Dtsch. Dermatologischen Ges. = J. Ger. Soc. Dermatology: JDDG 20, 629–641 (2022).
Hu, Z. & Wang, T. Beyond skin white spots: Vitiligo and associated comorbidities. Front. Med. 10, 1072837 (2023).
Dahir, A. M. & Thomsen, S. F. Comorbidities in vitiligo: comprehensive review. Int. J. Dermatol. 57, 1157–1164 (2018).
Fallahi, P. et al. The association of other autoimmune diseases in patients with autoimmune thyroiditis: Review of the literature and report of a large series of patients. Autoimmun. Rev. 15, 1125–1128 (2016).
Schwab, C. et al. A unifying concept of uveal pigment cell distribution and dissemination based on an animal model: insights into ocular melanogenesis. Cells, tissues, organs 201, 232–238 (2016).
Chen, J., Li, S. & Li, C. Mechanisms of melanocyte death in vitiligo. Medicinal Res. Rev. 41, 1138–1166 (2021).
Skrivankova, V. W. et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomization: The STROBE-MR Statement. Jama 326, 1614–1621 (2021).
Kyrgiou, M. et al. Adiposity and cancer at major anatomical sites: umbrella review of the literature. BMJ (Clin. Res. ed.) 356, j477 (2017).
Kalliala, I. et al. Obesity and gynaecological and obstetric conditions: umbrella review of the literature. BMJ (Clin. Res. ed.) 359, j4511 (2017).
Papatheodorou, S. I., Tsilidis, K. K., Evangelou, E. & Ioannidis, J. P. Application of credibility ceilings probes the robustness of meta-analyses of biomarkers and cancer risk. J. Clin. Epidemiol. 68, 163–174 (2015).
Ioannidis, J. P. & Trikalinos, T. A. An exploratory test for an excess of significant findings. Clin. trials (Lond., Engl.) 4, 245–253 (2007).
Larsson, S. C. & Burgess, S. Causal role of high body mass index in multiple chronic diseases: a systematic review and meta-analysis of Mendelian randomization studies. BMC Med. 19, 320 (2021).
Belbasis, L., Bellou, V., Evangelou, E., Ioannidis, J. P. & Tzoulaki, I. Environmental risk factors and multiple sclerosis: an umbrella review of systematic reviews and meta-analyses. Lancet Neurol. 14, 263–273 (2015).
Kim, J. H. et al. Environmental risk factors, protective factors, and peripheral biomarkers for ADHD: an umbrella review. Lancet Psychiatry 7, 955–970 (2020).
Markozannes, G. et al. Systematic review of Mendelian randomization studies on risk of cancer. BMC Med. 20, 41 (2022).
Rosenberg, M. S. The file-drawer problem revisited: a general weighted method for calculating fail-safe numbers in meta-analysis. evolution; Int. J. Org. evolution 59, 464–468 (2005).
Papadimitriou, N. et al. An umbrella review of the evidence associating diet and cancer risk at 11 anatomical sites. Nat. Commun. 12, 4579 (2021).
Botelho, J. et al. An umbrella review of the evidence linking oral health and systemic noncommunicable diseases. Nat. Commun. 13, 7614 (2022).
Acknowledgements
This study was supported by National Natural Science Foundation of China (82473521) (J.M.C.); National High Level Hospital Clinical Research Funding (BJ-2024-249) (J.M.C.).
Author information
Authors and Affiliations
Contributions
L.L., Y.X., W.L., and J.M.C. were involved in the original conceptualization. L.L. and Y.X. were responsible for developing the study methodology. L.L. and W.L. did the literature search. L.L. and H.L. were responsible for data curation. L.L. did the formal statistical analysis. L.L. and J.C. wrote the original draft. All authors edited and reviewed the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Russell de Souza, and the other, anonymous, reviewer for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, L., Xue, Y., Liu, W. et al. Systematic evidence grading evaluates multisystemic associations and risks of vitiligo. Nat Commun 16, 9665 (2025). https://doi.org/10.1038/s41467-025-64653-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-64653-y
