
Abstract
Several studies have evaluated PD-1 inhibitors plus chemotherapy as neoadjuvant treatment for locally advanced esophageal squamous cell carcinoma (ESCC), but comparative data with chemoradiotherapy (CRT) remain limited. This multicenter, randomized, open-label, phase 2 non-inferiority trial (REVO, NCT05007145) assessed the efficacy and safety of neoadjuvant camrelizumab plus chemotherapy (ICT) versus CRT in patients with resectable, locally advanced ESCC. A total of 104 patients were randomized to ICT (camrelizumab, nab-paclitaxel, cisplatin) or CRT (nab-paclitaxel, cisplatin, radiotherapy). The primary endpoint was pathologic complete response (pCR). ICT achieved a pCR rate of 32.7% versus 34.6% with CRT (rate ratio 0.94, 90% CI 0.6–1.49), demonstrating non-inferiority and meeting the pre-specified primary endpoint. Major pathologic response was observed in 42.3% of ICT patients and 57.7% of CRT patients, with R0 resection achieved in 100% of both groups. 1-year disease-free survival was 89.1% versus 78.2%, and 1-year overall survival was 100% versus 92.3% for ICT and CRT, respectively. Grade ≥3 treatment-related adverse events occurred in 19.2% of ICT patients and 33.3% of CRT patients, and surgical complications were reported in 31.1% and 35.9%, respectively. These findings indicate that ICT is a safe and effective neoadjuvant strategy for resectable ESCC with a more favorable safety profile.
Similar content being viewed by others

Introduction
Esophageal cancer is a global health concern, particularly in East Asia, where esophageal squamous cell carcinoma (ESCC) is the dominant type1. Following the landmark CROSS and NEOCRTEC5010 studies, neoadjuvant chemoradiotherapy (CRT) has been established as the current standard of care for locally advanced, resectable esophageal cancer2,3. Recently, neoadjuvant DCF (docetaxel, cisplatin, and 5-fluorouracil) therapy has shown an overall survival (OS) benefit for patients with resectable locally advanced ESCC4. Nevertheless, approximately half of patients still experience recurrence within five years following surgery3,4. This underscores the urgent need for more effective systemic therapies to improve OS for these patients.
Programmed cell death protein 1 (PD-1), an immune checkpoint protein that regulates T-cell activity, has emerged as a key target in cancer immunotherapy. Camrelizumab, a PD-1 inhibitor, has shown promise in treating ESCC, with its efficacy and safety established in 20185. Its approval as a standard treatment for advanced ESCC followed the phase 3 trial that confirmed improved OS and progression-free survival and comparable adverse event (AE) rates to chemotherapy6. Pathologic complete response (pCR) is defined as the absence of residual tumor at the primary tumor site and negative lymph nodes. In phase 1b and 2 trials, neoadjuvant camrelizumab combined with chemotherapy for resectable ESCC reported pCR rates reaching 39.2%7,8,9,10. Most recently, the phase 3 ESCORT-NEO study showed that the neoadjuvant combination of camrelizumab and chemotherapy resulted in elevated pCR rates in comparison to chemotherapy alone for resectable ESCC, and this approach exhibited a favorable safety profile11. Our current retrospective analysis indicated that the integration of neoadjuvant chemotherapy with immunotherapy, particularly with high-dose chemotherapy, improves pCR rates12. In another retrospective analysis, neoadjuvant immunochemotherapy (ICT) demonstrated superior 3-year OS and 3-year disease-free survival (DFS) rates compared with neoadjuvant chemotherapy in patients with resectable advanced ESCC13. Nevertheless, despite these encouraging findings, a gap remains in clinical trials that comprehensively evaluate and compare the efficacy and safety of ICT versus CRT in the management of locally advanced ESCC.
In this work, we conducted a multicenter, randomized, open-label, phase 2 trial (REVO) to estimate the relative efficacy and safety of camrelizumab-based ICT versus CRT in patients with resectable ESCC. We used nab-paclitaxel, an albumin-bound formulation of paclitaxel shown in our retrospective analysis to improve pCR rates12, in combination with cisplatin as the chemotherapy backbone for both treatment groups. Given the lack of consensus on the optimal number of cycles for neoadjuvant chemotherapy, we administered 2–4 cycles tailored to individual patient needs to balance efficacy and safety. ICT demonstrates a pCR rate comparable to CRT, with a lower incidence of grade ≥3 treatment-related adverse events (TRAEs). These findings indicate that ICT provides non-inferior efficacy and a more favorable safety profile compared with CRT in this patient population.
Results
Patient characteristics
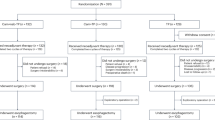
From September 1, 2021, to December 8, 2023, 104 patients were enrolled and randomized to receive either ICT (n = 52) or CRT (n = 52). Initially, the CRT group had 52 patients, but one withdrew consent prior to treatment, leaving the CRT group with 51 patients. Consequently, the intent-to-treat (ITT) populations for both groups were 52 patients each, with safety set populations of 52 for ICT and 51 for CRT (Fig. 1). The data cutoff for analysis was March 19, 2024, with a median follow-up of 18.8 months (interquartile range [IQR], 12.8–24.0 months). The median age of the patient cohort was 63 years (range, 45–74), with 78.8% of the participants being male. In terms of clinical staging, 16 patients (15.4%) were classified as stage II, 72 (69.2%) as stage III, 14 (13.5%) as stage IVA, and two (1.9%) as stage IVB. The anatomical location of the tumors was the upper thoracic esophagus in 23 patients (22.1%), the middle thoracic esophagus in 55 patients (52.9%), and the lower thoracic esophagus in 26 patients (25.0%). Baseline characteristics were similar between the two groups (Table 1).

aOf the six patients who did not complete neoadjuvant treatment, three withdrew consent, one discontinued due to physical condition, one due to medication unavailability, and one due to financial reasons. bOf the 10 patients who did not complete neoadjuvant treatment, nine discontinued due to adverse events, and one due to medication unavailability. ICT neoadjuvant immunochemotherapy, CRT neoadjuvant chemoradiotherapy.
Neoadjuvant treatment and surgical overview
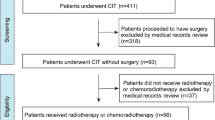
Within the ITT population, 52 patients in the ICT group and 51 in the CRT group received neoadjuvant therapy (Supplementary Table 1). The actual cycles of exposure during neoadjuvant therapy were 2.0 (IQR 2.0–3.0) in the ICT group and 2.0 (IQR 2.0–2.0) in the CRT group. Additionally, during the pandemic, shortages of nab-paclitaxel unfortunately resulted in 16 patients in the ICT group and 16 patients in the CRT group being treated with paclitaxel and corticosteroids instead. In the CRT group, besides the seven patients receiving radical CRT and the six withdrawing due to AEs, among those undergoing surgery, 35 received 40 Gy, while four received a reduced 36 Gy dose due to frailty (Supplementary Table 2).
A total of seven patients (13.5%) in the ICT group and 12 patients (25%) in the CRT group did not undergo surgery. In the ICT group, six patients refused surgery, and one had it canceled due to AEs. In the CRT group, six patients refused surgery, and six had it canceled due to AEs. In the two groups, patients primarily refused surgery due to pandemic-related concerns, symptom improvement following neoadjuvant therapy, and fear of surgery. The AEs leading to surgery cancellations predominantly included pneumonia, fatigue, decreased white blood cell count, decreased neutrophil count, decreased platelet count, and nausea (Supplementary Table 1). Eleven non-surgical patients were evaluated using CT imaging for post-treatment assessment. In the ICT group, three patients showed a partial response (PR), and one had stable disease. In the CRT group, seven patients demonstrated a PR.
Esophagectomy was performed on 45 patients (86.5%) in the ICT group, while 39 patients (75.0%) in the CRT group underwent the surgical procedure. The most frequently performed surgical procedure was the McKeown procedure, accounting for 97.8% of cases in the ICT group and 97.4% in the CRT group. In terms of surgical details, for the ICT and CRT groups, the median number of harvested lymph nodes was 45 (IQR, 13-97) and 42 (IQR, 11–88), respectively. The median duration of surgery was 315 minutes (range, 150–480) and 300 minutes (range, 90–558) (Table 2).
Endpoints
In the ITT population, for the primary endpoint, the pCR rate was 32.7% (17/52) in the ICT group, comparable to the 34.6% (18/52) observed in the CRT group (ratio of pCR rates [RR], 0.94, 90% confidence interval [CI], 0.6–1.49). The lower limit of the RR did not encompass the 0.5 non-inferiority threshold, thereby demonstrating non-inferiority and meeting the primary endpoint. For secondary endpoints, the MPR rate was 42.3% (22/52) in the ICT group and 57.7% (30/52) in the CRT group, respectively. According to the Becker criteria, 17 patients (32.7%) in the ICT group achieved TRG 1a, whereas 18 patients (34.6%) in the CRT group had TRG 1a tumors (Table 3 and Supplementary Table 3). A post-hoc subgroup analysis of pCR rate based on baseline characteristics is depicted in Supplementary Fig. 1. The pCR rates were similar between the ICT and CRT groups across various subgroups, consistent with the primary result.
The surgical outcomes and survival rates were generally similar between the ICT and CRT groups. In the surgery set, the pCR rate was 37.8% (17/45) in the ICT group and 46.2% (18/39) in the CRT group (Supplementary Table 4). The rates of R0 resection were identical at 100% for both groups (Table 2). Moreover, the ICT group had 30 patients (66.7%) achieve a downstage, compared to 31 patients (79.5%) in the CRT group (Supplementary Table 5). As some patients received paclitaxel, we compared the pCR rates of paclitaxel and nab-paclitaxel in the ICT and CRT groups. No obvious difference of paclitaxel or nab-paclitaxel was found between the two groups (Supplementary Table 6). The OS and DFS have not yet matured. In the ICT group, the 1-year DFS rate was 89.1% (95% CI: 72.96–95.83), while the CRT group had a 1-year DFS rate of 78.2% (95% CI: 56.98–89.79). The ICT group achieved a 1-year OS rate of 100.0% (95% CI: 100.00–100.00) and a 2-year OS rate of 86.3% (95% CI: 64.25–95.20). In contrast, the CRT group reported a 1-year OS rate of 92.3% (95% CI: 80.79–97.04) and a 2-year OS rate of 81.6% (95% CI: 59.47–92.38) (Supplementary Fig. 2).
Safety
The CRT group had a similar incidence of all-grade TRAEs but a higher rate of grade ≥3 TRAEs and treatment discontinuations compared to the ICT group. The incidence of TRAEs was 96.2% (50/52) in the ICT group and 100% (51/51) in the CRT group. Grade ≥ 3 TRAEs occurred in 19.2% (10/52) of the ICT group and 33.3% (17/51) of the CRT group (Table 4). Treatment discontinuation due to TRAEs was rare in the ICT group (1.9%, 1/52) but more common in the CRT group (15.7%, 8/51), with one CRT patient dying from a severe infection due to Grade IV myelosuppression (Supplementary Table 7). The most common grade ≥3 TRAEs in the ICT group were decreased white blood cell count (13.5%), decreased neutrophil count (3.8%), and decreased platelet count (1.9%) compared to decreased white blood cell count (21.6%), decreased neutrophil count (9.8%), and decreased platelet count (7.8%) in the CRT group. Immune-related AEs (irAEs) affected 34.6% (18/52) of the ICT group, with grade ≥3 irAEs in 3.8% (2/52). The most common irAE was reactive cutaneous capillary endothelial proliferation, all graded as Grade 1-2 (Table 4). Additionally, the AEs associated with nab-paclitaxel plus cisplatin, paclitaxel plus cisplatin, and nab-paclitaxel plus paclitaxel and cisplatin in the ICT and CRT groups are detailed in Supplementary Tables 8–11.
Surgical complication rates were similar between the ICT and CRT groups, but the CRT group had a higher 30-day postoperative mortality rate. Surgical complications occurred in 31.1% (14/45) of patients treated with ICT and 35.9% (14/39) of patients treated with CRT, with Clavien-Dindo grade ≥ 3 complications in 15.6% (7/45) and 12.8% (5/39), respectively. Postoperative pneumonia was the main complication, with grade ≥ 3 complications in 11.1% (5/45) of the ICT group and 10.3% (4/39) of the CRT group (Supplementary Table 12). The CRT group had a 30-day postoperative mortality rate of 5.1% (2/51), including one case due to severe pneumonia and another due to septic shock. In contrast, the ICT group reported no cases of 30-day and 90-day postoperative mortality (Table 2).
Discussion
The REVO study was a phase 2 trial that evaluated the efficacy and safety of ICT versus CRT in patients with locally advanced ESCC. The pCR rate in the ICT group was 32.7%. The CRT group had a pCR rate of 34.6%, which was similar to the 32% pCR rate reported for neoadjuvant chemoradiotherapy in a meta-analysis of locally advanced ESCC14. This result preliminarily demonstrated that the pCR rate with ICT was not inferior to CRT, supporting the hypothesis of equivalent pCR probabilities. This is evidenced by an RR of 0.94 with the 90% CI of 0.60 to 1.49, whose lower boundary did not encompass the predefined non-inferiority threshold of 0.5. Given concerns regarding the tolerability of CRT, neoadjuvant chemotherapy is more commonly used in clinical practice, despite its relatively low pCR rate, typically ranging from 2.9% to 9.0%14,15,16. Compared to CRT, ICT requires shorter hospital stay, is more accessible in settings with limited radiotherapy resources, avoids radiation-related toxicities, and reduces the number of clinic visits. Therefore, these findings highlight the considerable therapeutic potential of ICT as a treatment strategy for locally advanced ESCC.
Although the ITT analysis showed similar pCR rates between the ICT and CRT groups, the surgery set demonstrated a higher pCR rate in the CRT group (46.2%, 18/39) compared to the ICT group (37.8%, 17/45). However, this apparent difference is likely attributable to the lower number of operated patients in the CRT group, which had a higher non-surgery rate (23.5% vs 13.5%). Furthermore, the CMISG1701 study demonstrated a higher pCR rate with CRT (27.7% vs 2.9% for neoadjuvant chemotherapy) but found no OS benefit17. Similarly, the NeoRes trial reported minimal OS differences despite a superior pCR rate with CRT (28% vs 9%)16. The JCOG1109 trial indicated that adding radiotherapy to CF did not significantly improve OS, while neoadjuvant DCF offered both a higher pCR (18.6% vs 2.2%) and OS benefit4. Thus, the relationship between pCR and prolonged survival outcomes remains unclear. Neoadjuvant immunotherapy aims to enhance systemic immunity against tumor antigens, potentially eliminating micrometastases to prevent postoperative relapse18. However, most current trials are comparing ICT to neoadjuvant chemotherapy, including reported phase 2 studies and the phase 3 ESCORT-NEO/NCCES01 study, as well as ongoing phase 3 studies such as NCT04848753 and KEYSTONE-00219. Our multicenter, randomized, open-label REVO trial uniquely assessed the non-inferiority of ICT compared to CRT. Whether the ICT group can prolong OS compared to CRT will be reported in further follow-up, making these results highly anticipated.
In China, the TP regimen (paclitaxel and cisplatin) is favored due to its good tolerance among patients. Corticosteroids are commonly administered before paclitaxel to mitigate side effects and manage dose-response; however, studies suggest that corticosteroids may negatively impact survival outcomes in patients receiving checkpoint blockade therapy20,21,22. Nab-paclitaxel, a steroid-free formulation, simplifies administration and has shown higher pCR and MPR rates when combined with immunotherapy and platinum-based chemotherapy compared to standard paclitaxel12. In this study, we utilized the NP regimen (nab-paclitaxel and cisplatin). However, during the pandemic, some patients regrettably received paclitaxel due to nab-paclitaxel shortages. While the CROSS and JCOG1109 trials used a higher radiation dose of 41.4 Gy2,4, the NEOCRTEC5010 trial used 40 Gy, and approximately 13% of patients received a dose below 40 Gy due to treatment-related toxicities3,23. In this study, during the neoadjuvant therapy, due to frailty concerns, four patients (10.3%) received a reduced dose of 36 Gy, while the majority (35 patients, 89.7%) received 40 Gy. Notably, the pCR and MPR rates were similar between patients receiving 36 Gy and those receiving 40 Gy.
The ICT group exhibited a toxicity profile consistent with prior studies, without introducing new safety concerns6,7,8,9,10. This group primarily experienced hematological toxicities and mild irAEs, with few grade ≥3 events, indicating a safe and manageable treatment. In contrast, the CRT group faced higher hematological toxicity rates and a greater need to discontinue therapy due to AEs. The ICT group also had fewer surgery cancellations due to AEs. While both groups had similar postoperative complication rates, only the CRT group had 30-day postoperative mortality. These results suggest that the ICT group had a better safety profile and required less intensive management than the CRT group.
This study, while informative, has several limitations. These include a relatively small patient cohort, the absence of central confirmation of pCR, and the lack of blinding for pathologists to treatment assignment. Additionally, this trial was conducted during the pandemic, which impacted patient decision-making regarding surgery and resulted in lower surgery rates. Importantly, AEs in the CRT group further reduced surgical conversion. Although the pandemic disrupted treatment protocols, both groups maintained the standard of care. The study lacked comprehensive biomarker data, with many patients’ PD-L1 status unknown. Biomarker and patient-reported outcomes are now being collected for further insights. Additionally, OS and DFS have not yet matured, and thus, the relationship between pCR and OS requires further follow-up for validation. To address these limitations, we plan to expand the sample size and initiate a phase 3 trial to solidify the evidence for the treatments’ efficacy and safety.
In conclusion, the study’s findings indicate that ICT achieved pCR rates similar to those of CRT while demonstrating a better safety profile. This similarity in pCR rates, along with the enhanced safety of ICT, supports its non-inferiority to CRT as a treatment option for patients with locally advanced ESCC. The preliminary survival data are promising and emphasize the need for further investigation; additional survival data are eagerly anticipated to confirm these encouraging trends.
Methods
Study design and participants
This was a multicenter, open-label, randomized, phase 2 clinical trial conducted at five hospitals across China. Eligible patients were aged 18-75 years, with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. They had stage T1b-4aN1-3M0-1 (with supraclavicular metastasis only) or stage T3-4aN0M0-1 ESCC (with supraclavicular metastasis only) according to the 8th edition of the American Joint Committee on Cancer (AJCC) staging system. Patients were treatment-naïve for ESCC and had no history of other cancers. Adequate organ function was required before registration, and patients were expected to be candidates for R0 resection. The first patient was enrolled on September 1, 2021, and the last patient enrolled on December 8, 2023. Sex of participants was determined by self-report.
The protocol and informed consent were approved by the institutional review boards of the Fujian Cancer Hospital (the ethical approval number: K2021-107-02). Written informed consent from all participants was obtained before starting the study. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. The trial was registered on ClinicalTrials.gov (NCT05007145) and followed the Consolidated Standards of Reporting Trials (CONSORT) guidelines for reporting. Details of the study protocol are provided in the Supplementary Note.
Randomization and masking
Eligible patients were randomized in a 1:1 ratio to the CRT group or ICT group via a central randomization process. Randomization was restricted to achieve balanced sample sizes between groups. A computer-generated system at Fujian Cancer Hospital managed the randomization process, with group assignments determined through the registration system by simple randomization. Participants were enrolled by investigators, and group allocation was not masked to participants, investigators, or outcome assessors.
Procedure
The ICT regimen included camrelizumab (200 mg on day 1), nab-paclitaxel (125 mg/m² on days 1 and 8), and cisplatin (75 mg/m² on day 1) administered intravenously every 3 weeks for 2–4 cycles. The surgical team assessed individual needs to balance safety and efficacy, guiding the decision to administer 2–-4 cycles of chemotherapy. The CRT regimen included the same chemotherapy regimen for two cycles plus 40 Gy of radiotherapy. Radiotherapy was delivered using 3D conformal technology, with a total of 20 fractions amounting to a cumulative dose of 40 Gy over a five-week period. In cases where nab-paclitaxel was not available, paclitaxel (175 mg/m² on day 1) could be used as a substitute.
About 4–6 weeks after the neoadjuvant treatment, patients were re-evaluated with a CT scan of the chest and upper abdomen or a PET-CT. Curative resection was performed if no evidence of metastatic disease was detected. The surgical procedure comprised esophagectomy and lymph node dissection, with the McKeown approach and a total two-field lymphadenectomy recommended24. Both minimally invasive and open techniques for esophagectomy were considered acceptable.
Outcomes
The primary endpoint was pCR, which was assessed by local pathologists at each institution without central confirmation. pCR was defined as the absence of residual tumor at the primary tumor site (tumor regression grade 1a according to the Becker criteria) and negative lymph nodes. The histological regression grade of the primary tumor was evaluated using the Becker criteria25. Secondary endpoints included MPR rate (defined as fewer than 10% residual viable tumor cells in the primary tumor), R0 resection rate, ypTNM staging according to the 8th edition of the AJCC, OS, DFS, AEs, and surgical complications. The study meticulously documented all AEs, postoperative complications, and postoperative mortality within 30 and 90 days. AEs were graded and recorded in accordance with the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 5.026. Postoperative complications were classified according to the standards of the Esophageal Complications Consensus Group, with severity graded using the CD classification27,28.
PD-L1 expression was evaluated using immunohistochemistry (PD-L1 IHC 28-8 pharmDx assay) on formalin-fixed paraffin-embedded tissue from pro-treatment endoscopic biopsies29. The assessment used the Counted Positive Squamous cells (CPS), calculated by dividing the number of PD-L1-positive staining cells by the total viable tumor cells and multiplying by 100.
Statistical analysis
This randomized trial was designed to validate the non-inferiority of ICT compared to CRT with respect to the primary endpoint of pCR. The assumed true pCR rates for both groups were set at 0.35, based on the NEOCRTEC5010 study23. A non-inferiority threshold of 0.5 in regarding RR by comparing the ICT to the CRT was established to ensure that ICT would not be deemed inferior while preserving over 70% of CRT’s efficacy. With a power of 0.8 and a significance level (α) of 0.05 by using the score test, the sample size for each group was calculated to be 51 participants. This resulted in a total of 102 participants needed for the study, allocated in a 1:1 ratio. The sample size was determined using NCSS&PASS version 15.0. The null hypothesis was that the RR was no greater than 0.5.
The efficacy analysis adhered to the ITT principle, including all randomized participants. The study population comprised subjects who had received at least one dose of the study medication. The 95% CIs for the pCR and MPR rates were computed using the Clopper-Pearson method. Differences in pCR rates (RDs), RRs, and odds ratios (ORs), along with their corresponding 95% (for RDs and ORs) or 90% (for RRs) CIs (WALD method), were calculated by comparing the pCR rates of ICT to CRT groups. Post hoc subgroup analyses of pCR were conducted based on baseline characteristics, with rate differences estimated and presented in a forest plot for each subgroup comparison. All statistical analyses were performed using SAS software version 9.4.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The clinical data generated and analyzed in this study are not publicly available due to data privacy laws and ethical restrictions. Access to the raw data can be granted to qualified researchers for non-commercial academic purposes. Requests for access should be sent to the corresponding author, Dr. Shuoyan Liu (shuoyanliu2010@163.com), and should include a brief research proposal and evidence of institutional ethical approval. All requests will be reviewed within four weeks. The protocol of this study is provided in the Supplementary Information. Source data are provided with this paper.
References
Sung, H. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 71, 209–249 (2021).
Eyck, B. M. et al. Ten-year outcome of neoadjuvant chemoradiotherapy plus surgery for esophageal cancer: the randomized controlled CROSS trial. J. Clin. Oncol. 39, 1995–2004 (2021).
Yang, H. et al. Long-term efficacy of neoadjuvant chemoradiotherapy plus surgery for the treatment of locally advanced esophageal squamous cell carcinoma: The NEOCRTEC5010 randomized clinical trial. JAMA Surg. 156, 721–729 (2021).
Kato, K. et al. Doublet chemotherapy, triplet chemotherapy, or doublet chemotherapy combined with radiotherapy as neoadjuvant treatment for locally advanced oesophageal cancer (JCOG1109 NExT): a randomised, controlled, open-label, phase 3 trial. Lancet 404, 55–66 (2024).
Huang, J. et al. Safety, Activity, and Biomarkers of SHR-1210, an Anti-PD-1 Antibody, for patients with advanced esophageal carcinoma. Clin. Cancer Res 24, 1296–1304 (2018).
Luo, H. et al. Effect of Camrelizumab vs Placebo added to chemotherapy on survival and progression-free survival in patients with advanced or metastatic esophageal squamous cell carcinoma: The ESCORT-1st Randomized Clinical trial. JAMA 326, 916–925 (2021).
Yang, W. et al. Neoadjuvant programmed cell death 1 blockade combined with chemotherapy for resectable esophageal squamous cell carcinoma. J. Immunother. Cancer 10 (2022).
Wang, Z. et al. Phase Ib trial of camrelizumab combined with chemotherapy and apatinib for neoadjuvant treatment of locally advanced thoracic esophageal squamous cell carcinoma. J. Natl. Cancer Cent. 2, 98–105 (2022).
Liu, J. et al. Multicenter, single-arm, phase II trial of camrelizumab and chemotherapy as neoadjuvant treatment for locally advanced esophageal squamous cell carcinoma. J Immunother Cancer 10 (2022).
Liu, J. et al. Neoadjuvant camrelizumab plus chemotherapy for resectable, locally advanced esophageal squamous cell carcinoma (NIC-ESCC2019): A multicenter, phase 2 study. Int J. Cancer 151, 128–137 (2022).
Qin, J. et al. Neoadjuvant chemotherapy with or without camrelizumab in resectable esophageal squamous cell carcinoma: the randomized phase 3 ESCORT-NEO/NCCES01 trial. Nat. Med. (2024).
Wang, P. et al. High-dose chemotherapy sensitizes locally advanced esophageal squamous cell carcinoma to PD-1 blockade for a higher pathological complete response rate and survival. Transl. Oncol. 36, 101736 (2023).
Wang, P. et al. Comparison of neoadjuvant chemoimmunotherapy and neoadjuvant chemotherapy for resectable esophageal squamous cell carcinoma: a retrospective study with 3-year survival analysis. J. Cancer Res Clin. Oncol. 150, 477 (2024).
Gaber, C. E. et al. Pathologic complete response in patients with esophageal cancer receiving neoadjuvant chemotherapy or chemoradiation: A systematic review and meta-analysis. Cancer Med. 13, e7076 (2024).
Samson, P. et al. Neoadjuvant Chemotherapy versus Chemoradiation prior to esophagectomy: impact on rate of complete pathologic response and survival in esophageal cancer patients. J. Thorac. Oncol. 11, 2227–2237 (2016).
Tang, H. et al. Neoadjuvant chemoradiotherapy versus neoadjuvant chemotherapy followed by minimally invasive esophagectomy for locally advanced esophageal squamous cell carcinoma: a prospective multicenter randomized clinical trial. Ann. Oncol. 34, 163–172 (2023).
Klevebro, F. et al. A randomized clinical trial of neoadjuvant chemotherapy versus neoadjuvant chemoradiotherapy for cancer of the oesophagus or gastro-oesophageal junction. Ann. Oncol. 27, 660–667 (2016).
Topalian, S. L. et al. Neoadjuvant immune checkpoint blockade: A window of opportunity to advance cancer immunotherapy. Cancer Cell 41,1551–1566 (2023).
Shang, X. et al. Pembrolizumab combined with neoadjuvant chemotherapy versus neoadjuvant chemoradiotherapy followed by surgery for locally advanced oesophageal squamous cell carcinoma: protocol for a multicentre, prospective, randomized-controlled, Phase III Clinical Study (Keystone-002). Front Oncol. 12, 831345 (2022).
Bai, X. et al. Early use of high-dose glucocorticoid for the management of irAE is associated with poorer survival in patients with advanced melanoma treated with Anti-PD-1 Monotherapy. Clin. Cancer Res. 27, 5993–6000 (2021).
Goodman, R. S., Johnson, D. B. & Balko, J. M. Corticosteroids and cancer immunotherapy. Clin. Cancer Res 29, 2580–2587 (2023).
Arbour, K. C. et al. Impact of baseline steroids on efficacy of programmed cell Death-1 and Programmed Death-Ligand 1 blockade in patients with non-small-cell lung cancer. J. Clin. Oncol. 36, 2872–2878 (2018).
Yang, H. et al. Neoadjuvant chemoradiotherapy followed by surgery versus surgery alone for locally advanced squamous cell carcinoma of the esophagus (NEOCRTEC5010): A Phase III multicenter, randomized, open-label clinical trial. J. Clin. Oncol. 36, 2796–2803 (2018).
Kang, X. et al. 2021 NCC/CATS/CSTCVS/STM expert consensus on perioperative immunotherapy for esophageal cancer. Ann. Esophagus 4 (2021).
Langer, R. & Becker, K. Tumor regression grading of gastrointestinal cancers after neoadjuvant therapy. Virchows Arch. 472, 175–186 (2018).
Dueck, A. C. et al. Validity and reliability of the US National Cancer Institute’s Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). JAMA Oncol. 1, 1051–1059 (2015).
Low, D. E. et al. International consensus on standardization of data collection for complications associated with esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann. Surg. 262, 286–294 (2015).
Dindo, D., Demartines, N. & Clavien, P. A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 240, 205–213 (2004).
Guo, L. et al. Programmed cell death ligand 1 expression in esophageal squamous cell carcinoma: a comparative analysis of three different assays. Chin. Med J. 134, 2890–2892 (2021).
Acknowledgements
This work was supported by the National Natural Science Foundation of China (Grant No. 82002497), the Scientific and Technological Innovation Joint Capital Projects of Fujian Province (No. 2023Y9424), and Fujian Provincial Key Clinical Specialty Construction Project for Thoracic Surgical Oncology. We are grateful to all patients, their families, and the site investigators who participated in the study. We thank Wending Sun for providing medical writing support Xiaoqing Chen for assistance with statistical programming (both employed by Jiangsu Hengrui Pharmaceuticals).
Author information
Authors and Affiliations
Contributions
F.W. and S.Lu. had full access to all data in the study and took responsibility for the integrity and accuracy of the data analysis. Concept and design were by F.W., S.Lu., J.Li., P.W., and Y.C. Acquisition, analysis, or interpretation of data were by P.W., Y.C., F.W., M.C., B.Z., D.Z., Q.Z., J.W., J.C., H.C., J.Lu., W.Z., C.L., J.Che., Y.L., Y.X., R.H., M.L., P.C., H.H., H.L., X.C., H.Z., W.C., W.W., F.Z., J.Lin., C.H., N.G., J.Ya., S.Li., S.Lu., J.Li. The manuscript was drafted by P.W., Y.C., N.G., J.Ya., and S.Li. Critical review of the manuscript for important intellectual content was performed by F.W., S.Lu., P.W., and Y.C. Statistical analysis was conducted by P.W., Y.C., N.G., and J.Ya. Funding was obtained by P.W. and F.W. Administrative, technical, or material support was provided by F.W. and S.Lu., and supervision was by S.Lu. and J.Li.
Corresponding authors
Ethics declarations
Competing interests
Ni Guan, Jin Yan, and Shujun Liang are employees of Jiangsu Hengrui Pharmaceuticals. All other authors declare no conflict of interest.
Peer review
Peer review information
Nature Communications thanks Sara Lonardi and the other anonymous reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, P., Chen, Y., Wang, F. et al. Camrelizumab plus chemotherapy versus chemoradiotherapy as neoadjuvant therapy for resectable esophageal squamous cell carcinoma: Phase 2 randomized trial (REVO). Nat Commun 16, 9676 (2025). https://doi.org/10.1038/s41467-025-64660-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-64660-z
This article is cited by
-
Optimizing immunotherapy for gastrointestinal tract cancers: clinical progress and perspectives
Immunity & Inflammation (2026)
