
Abstract
Widespread measles cases following the COVID-19 pandemic have threatened human health and progress towards measles elimination. While we know that the pandemic has disrupted routine measles vaccination worldwide, most settings still lack quantification of post-pandemic population immunity gaps and the feasibility of closing these gaps through supplementary immunisation activities. Using serological data (15,405 antibody measurements from 3,674 individuals) in southern China between 2013-2024, we analyse pre- and post-pandemic susceptibility profile changes in the pediatric population, and explore underlying differences and mechanisms of measles-specific immunity. We show that childbearing-age women born at a time of low measles infection risk (born between 1990-2005) had 0.39 (95% CI 0.38-0.42) log mIU/ml lower mean log-concentration in 2021-2024 compared to those born during high-risk periods (born between 1984-1989). This in turn resulted in a 0.29 (95% CI 0.27-0.52) log mIU/ml lower mean log-concentration at birth and faster antibody waning in their infants. We also observe that 9.5-10.7% pediatric susceptibility was attributed to waning vaccine-induced immunity during 2013-2024. We project a 23.5–50.0% immunity increase (from 66.6% to 92.7%) in children under 15 years following non-selective supplementary immunisation activities, supporting the key role of supplementary immunisation activities in restoring robust population immunity.
Similar content being viewed by others
Introduction
Establishing population immunity of at least 90–95% through the use of effective and safe measles-containing vaccines (MCV) has been a target set by all WHO regions to stop measles transmission. Despite averting an estimated 31.7 million deaths through MCV vaccination globally since 20001, measles transmission remains ongoing in all regions and continues to be one of the leading causes of vaccine-preventable disease burden worldwide, accounting for more than 159,073 reported cases in 2020 alone2,3. The COVID-19 pandemic presented new challenges to this already precarious situation of global measles control and elimination. From 2019 to 2021, global coverage of the first MCV dose (MCV1) declined from 86 to 81% (the lowest level since 2008), leaving about 24.7 million children unvaccinated4. The largest drop was observed in countries in the South-East Asia region (7%, resulting in an estimated 12,899 additional deaths during 2020–2030), followed by those in the African region (4%, 26,498 additional deaths) and other WHO regions (2–3%,199–2918 additional deaths)3,5,6. Along with this drop in global MCV1 coverage, measles cases and deaths increased substantially, with an estimated 9.2 million cases and 136,200 deaths in 2022, compared to 7.6 million cases and 60,700 deaths in 20202,7. Suboptimal measles epidemics, inadequate MCV1 coverage, and rising vaccine hesitancy suggest that global measles vaccination disruptions have persisted beyond the emergency phase of the COVID-19 pandemic, as evidenced by the rapid measles spread worldwide in 2023–20248,9,10.
Amid these global setbacks, measles-specific population immunity gaps must be addressed. However, identifying and quantifying these gaps has become increasingly complex following disruptions in routine MCV uptake after the COVID-19 pandemic. Population immunity is made up of infection- and vaccination-induced immunity in adults and children and maternal protection in infants. While immunity gaps in children eligible for vaccination (mainly due to undervaccination, primary vaccine failure and waning vaccine-induced immunity) is well established, pediatric immunity gaps in pre-vaccination age groups remains less well understood. We know that the magnitude of infant immunity is primarily determined by the magnitude of measles antibodies in their mothers at birth11. There is also a growing realization that there exists wide heterogeneity in antibody levels across childbearing-age women12. Currently, the extent to which vaccine versus infection history determine underlying differences in antibody levels and whether these differences contribute to pediatric immunity gaps remain unknown. Filling this knowledge gap is crucial for understanding how to restore robust population immunity from the pandemic. To understand pediatric immunity gaps in a post-pandemic setting, it is necessary to understand the exact role of maternal immunity (and its transfer to neonates), natural infection, primary and secondary vaccine failure, and missing MCV doses.
In response to the significant public health threats posed by the immunity gaps in the pediatric population, prioritising the supplementary immunisation activity (SIA) policy implementation at national or regional scale is necessary. As of June, 2025, very few countries have initiated SIAs as a key strategy to close immunity gaps in age-eligible populations, despite the World Health Organization already launching the “Measles outbreaks strategic response plan: 2021–2023” in August, 202213. Given the complexity and time-dependency of population immunity, timely evidence from modelling informed by empirical data is needed before implementing SIAs in the real world to support whether and which supplementary immunisation efforts could shift population immunity to reach the necessary levels (e.g., >90–95%), particularly in a setting with high pre-pandemic MCV coverage. In particular, we need to address methodological challenges to predicting each individual’s vaccine responses and SIA strategy-specific cumulative effects.
In this study we aim to provide overview of long-term immunity profiles among both children and childbearing-age women and how these profiles may contribute to pediatric immunity gaps before and after the COVID-19 pandemic period. To do this, we use pre- and post-pandemic measles antibody measurements from three large population-based studies conducted during 2013–2024 in Hunan province, China—a setting with consistently high MCV coverage of over 95% since the early 1990s. We also use this study location as an example to analyse susceptibility profile changes in the pediatric population and explore the optimal SIA strategies to close population immunity gaps in a post-pandemic setting with high MCV coverage. In particular, we develop mathematical models to infer individual responses to a new vaccination event, and then estimate the SIA strategy-specific effects on shifting population immunity.
Results
Childbearing-age women born at a time of low measles circulation had low antibody concentrations
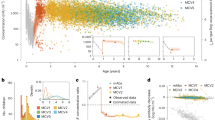
The enrolment age distribution of childbearing-age women in the mother-infant cohort in 2013–2015 (n = 555) were slightly lower than those involved in the cross-sectional study in 2021 (n = 217), with a median age of 27.4 years (interquartile range, IQR: 24.1–29.9) and 30.3 years (IQR: 25.0–35.0) respectively (p = 4.77e-08) (Table S1–S2, Fig. S1). Before determining time- and age-specific difference in measles immunity levels in all study participants, we built a Bayesian hierarchical model to assess potential testing batch-related experimental errors arising from ELISA assay. We show that both observed and model-based experimental errors fall within the range of –0.1 to 0.1 log mIU/ml (Fig. S2). Notably, no significant difference was observed between ELISA-based and error-corrected antibody concentrations across individuals estimated from this model (p = 0.205). Using error-corrected antibody measurements, we found that although childbearing-age women enroled in 2021–2024 were older than those from 2013 to 2015, and were therefore expected to have higher immunity levels due to a longer period of potential exposure to measles virus, lower log-concentrations were instead observed in this group (Fig. 1A, B). We subsequently focused on identifying which age groups contributed to the observed changes in immunity against measles. We noticed a substantially higher proportion of susceptible individuals aged 20–24 years during 2021–2024 compared to 2013–2015 (2013–2015 vs. 2021–2024: 9.8%, 95% CI 6.1–14.7% vs. 25.0%, 95% CI 14.0–38.9%; p = 0.007), whereas no significant differences in susceptibility were observed in other age groups (Fig. 1C). We next examined these individuals with paired antibody measurements from both periods (n = 84, 38.7%), and found a reduction in their log-concentrations (mean: 6.60, IQR: 5.75–7.37 log mIU/ml vs. 6.12, IQR: 5.32–6.84 log mIU/ml; p = 0.008), along with an increase in the proportion of susceptibles (6.3%, 95%CI 1.8–15.5% vs. 22.2%, 95%CI 12.7–34.5%; p = 0.022) between two periods.

A Measured antibody concentration in the years 2013–2015 (T1) and 2021–2024 (T2). Coloured points represent each individual’s antibody concentrations (n = 772). Each black point, along with an error bar, indicates the bimonthly mean antibody concentration and its 95% confidence interval. B Summary of log-concentration distribution in the years of 2013–2015 (n = 529) and 2021–2024 (n = 396). The dotted lines show the mean value of the log-concentration distribution; the black points with error bars in the inset panel show mean log-concentration and its 95% confidence interval. C The proportion of susceptible individuals aged 20–24 (n = 306), 25–34 (n = 484), and 35–49 years (n = 135) in 2013–2015 and 2021–2024 are shown by the points with error bars. Each point with error bar is the estimated mean percent susceptible and corresponding 95% confidence intervals. D Transplacental transfer of maternal antibodies. Grey points show the measured transplacental transfer ratio of log-concentrations (main panel), individual log-concentration (left subpanel) and the consistency between maternal and neonatal log-concentration (right subpanel), respectively. In the main panel, the blue line denotes the mean transplacental transfer ratio as a function of log-concentration level in birthing women using loess fit regression. In the left subpanel, observed maternal (mAb) and neonatal (nAb) mean log-concentrations are shown as blue horizontal lines, while in the right subpanel the blue line represents the regression mean. In both the main panel and right subpanel, the shaded areas denote 95% confidence intervals.
We considered that childbearing-age women’s antibody levels in 2021–2024 were unlikely to be affected by the pandemic-related vaccination delay but were likely influenced by waning immunity and changes in measles vaccination policy/transmission since the late 1980s (Fig. S3), as supported by their observed “U-shaped” immunity distributions (Fig. S4). Thus, we further use a multivariable linear regression model, which included childhood vaccination dose and infection risk as covariates, to understand the factors driving log-concentration levels in childbearing-age women. Since the unavailability of their vaccination and infection records precluded us from confirming individual vaccination/infection status, we instead categorised them into different childhood vaccination dose (born before and after 1986: MCV1 only vs. a two-dose MCV1/MCV2 strategy) and infection risk groups (determined by median measles incidence in 1984–2005: high vs. low risk for those born before and after 1990). We found that individuals who received a two-dose vaccination schedule (β = 0.66, 95%CI 0.07–1.30; p = 0.029) and those with high infection risk (β = 0.55, 95%CI 0.27–0.83; p = 1.18e-05) during childhood had higher log-concentrations compared to those with a one-dose schedule and low childhood infection risk (Table S3).
Lower child immunity in 2021–2024 compared to pre-pandemic levels was due to pandemic-related vaccination delays and waning vaccine immunity
The age and sex distribution, which are key determinants of child immunity level as shown in Table S4, are comparable among participants in three population-based studies (Table S2). The cohort children and participants in the cross-sectional study had a median age of 4.8 years (IQR: 2.2–6.9) and 5.0 years (IQR: 3.0–7.0) respectively (p = 0.166). Female/male participation percentages were close in the two cohorts [n = 1268 (48.2%) vs. 1361 (51.8%)] and the cross-sectional study [n = 133 (48.7%) vs. 140 (51.3%)] (p = 0.929), suggesting equal representation of both males and females. In addition, none of these children were officially recorded as having had measles. These similarities observed among child participants in the three studies, coupled with their exact MCV vaccination records (another key determinant of child immunity level) (n = 2902), enabled us to assess pandemic-related changes in immunity levels and MCV uptake rate in the pediatric population. In 2013–2018, we found that child bimonthly mean log-concentrations (mean: 6.65, 95%CI 6.57–6.73) (Fig. 2A) and annual MCV1 uptake rates (92.0–96.8%) (Fig. S5 subpanel) did not change significantly over time, based on serological and vaccination data from both cohort and cross-sectional studies. However they were substantially higher than those observed in the year 2021–2024 (mean: 6.21, 95% CI 5.80–6.62; MCV1 uptake rate in 2020–2021: 87.5%) (p = 0.035) (Fig. 2B).

A Measles immunity profiles in the pediatric population in the years of 2013–2018 and 2021–2024 (n = 2902). Coloured points represent each individual’s antibody concentrations. Each black point, along with an error bar, indicates the mean antibody concentration and its 95% confidence interval in the corresponding time period. B Pediatric log-concentration distribution in 2021–2024 (n = 1345) compared to those in 2013–2018 (n = 2629). The dotted lines show the mean value of the log-concentration distribution; the black points with error bars show mean log-concentration and its 95% confidence interval (subpanel). C Time variations in population susceptibility structure, respectively. D Time-specific proportions of susceptible children aged 2–3 (n = 1452), 4–5 (n = 1457), 6–7 (n = 1221) and 8–11 years (n = 1184) who received the two-dose vaccination schedule at 8 and 18 months respectively. Each point with error bar shows the estimated mean percent susceptible and corresponding 95% confidence intervals.
Focusing on individual born since 2010 (a period with comparable measles epidemic levels and MCV uptake rate) and enroled in both cohort and cross-sectional studies, we first observed a delayed MCV1 vaccination in 2020–2021. Specifically, the median age at MCV1 administration was 8.9 months (IQR: 8.6–10.5 months), which was higher than the median in 2013–2019 (8.5 months, IQR: 8.2–8.9 months, p = 0.043) (Fig. S5). We also performed a multivariable analysis to validate the presumed child immunity differences between 2013–2018 and 2021–2024. To validate this, we stratified these children into two groups based on whether their scheduled age of receiving MCV1 occurred before or after 2020, and included this categorical variable into our multivariable analysis (Table S5). After controlling for individual age (in years) and sex, we found that child log-concentrations observed in 2021–2024 is significantly lower than those observed in 2013–2018 (\(\beta\)= −0.44, 95% CI: −0.85 to −0.02) (Fig. 2B subpanel).
We further analysed how the susceptibility structure among these children changed between the two time periods. During 2013–2018, 0.2% (n = 5), 0.7% (n = 17), and 9.5% (n = 243) susceptibility could be attributed to undervaccination, primary vaccine failure and waning immunity post-vaccination respectively (Fig. 2C). By contrast, in 2021–2024, these proportions were 0.4% (n = 8), 0.3% (n = 5) and 10.7% (n = 191) respectively, revealing an increased immunity gap in both unvaccinated and vaccinated children. For waning immunity post-vaccination, we additionally demonstrated its age-related effects using data from children who received the routine two-dose vaccination at 8 and 18 months of age (Fig. 2D). In particular, individuals enroled in 2021–2024 exhibited a progressive increase in susceptibility with age, rising from 0% at ages 2–3 years to 10.4% at ages 8–11 years.
Lower antibody concentrations in mothers results in more rapid waning of immunity in infants
To further explore the impact of the observed temporal changes in log-concentration in childbearing-age women on child antibody levels, we assessed the feasibility of using mathematical models to predict maternal antibody transfer through the placenta and child immunity dynamic changes from birth (model A). We found that model A, incorporating the exponential relationship between maternal and neonatal log-concentrations (Table S6, Fig. 1D), was capable of accurately reproducing the measured mean log-concentrations and proportion of susceptible children from birth to 10 years (Figs. 3A and S6). It also demonstrated greater parsimony while providing comparable performance in fitting individual antibody dynamics relative to the biphasic model (model C)14 (WAIC for model A and C: 6095.6 vs. 6114.8; p = 0.074) (Table S7). Using this exponential model framework, we predicted the decay dynamics of infant maternally-derived immunity, peak log-concentration increases following each routine MCV vaccination and susceptibility changes from their birth to 10 years under different scenarios: baseline (assuming mAb level consistent with its 2013–2015 level) and lower mAb scenarios (mAb level consistent with its 2021–2024 level) (Fig. S7).

The baseline scenario assumes that antibody levels in birthing women (mAb) are consistent with those observed in the mother-infant cohort in 2013–2015, while the lower mAb scenario considers mAb levels consistent with those observed in the childbearing-age women in 2021–2024. Estimated concentration or susceptibility levels in the lower mAb scenario in (A) and (B, C) are based on 10,000 simulated datasets. A Maternally derived immunity dynamics. The solid line represents the median antibody concentration or proportion of susceptible children over ages. The shaded areas represent the interquartile range of the individual concentrations or the 95% confidence intervals for the proportion of protected individuals. Each black point with error bar indicates the observed mean percent susceptible and its 95% confidence intervals. B The estimated peak log-concentration distribution following the first and second dose of measles-containing vaccine vaccination at 8 and 18 months of age. C Age-specific susceptibility changes resulting primarily from lower maternal antibody levels in individuals under 1 year of age and from vaccine failure following MCV2 vaccination at 18 months (n = 10,000). The main panel shows dose-specific susceptibility changes due to lower maternal antibody levels, while the inset panel shows the mean proportion of children susceptible to measles (abbreviated as “mean prop”) across ages, adjusted for population structure. Error bars show 95% confidence intervals.
In both modelling scenarios, we find a rapid decline in infant maternally-derived immunity, regardless of maternal immune status (Fig. S8A). Half of infants show below-threshold log-concentrations within 2 months after birth (baseline vs. lower mAb scenario: 61 vs. 48 days) (Fig. 3A). We find higher peak log-concentrations following MCV1 (mean: 6.91 log mIU/ml, IQR: 6.68–7.13 log mIU/ml; p = 1.33e-198) and MCV2 vaccination (mean: 7.24 log mIU/ml, IQR: 7.03–7.43 log mIU/ml; p = 3.65e-198) in the lower mAb scenario, compared to those observed in the baseline scenario (MCV1: 6.76, 6.51–6.99 log mIU/ml; MCV2: 7.11, 6.89–7.31 log mIU/ml) (Fig. 3B). These results are consistent with those derived from the age-specific susceptibility changes, where we find that the reduction in log-concentrations in birthing women leads to increases in the proportion of susceptible infants (mean: 7.2%, 95% CI: 2.8–11.6%), which in turn contributed to a reduction in the occurrence of secondary vaccine failure (mean: 4.3%, 95% CI: 4.1–4.5%) (Fig. 3C).
Immunity continues to decline, driven mainly by waning vaccine immunity, but can be reversed by SIAs
Based on the observed linear relationship between pre-existing log-concentrations immediately prior to vaccination and peak log-concentration increases post-vaccination (Fig. S9), we expanded model A (model B) and validated its ability to reconstruct individual vaccine responses across different pre-existing antibody levels. We found no significant difference between the measured and predicted mean log-concentrations using such a model framework (p = 0.952) (Fig. S10). We next used this model framework to infer individual immunity profiles without (baseline) and with different hypothetical SIA activities in July 2025. More specifically, we considered SIAs targeting different age groups stratified by 1-year age ranges.
We found that individual antibody concentrations and their pooled population immunity levels (defined as the proportion of children with above-threshold log-concentration) continually decrease over time if no SIA is given (Fig. 4A). We estimate that among children aged between 8 months and 14 years who are eligible to vaccination, 66.6% of them (562/844, 95%CI 63.3–69.8%) are still protected in 2025 baseline, which is lower than the 92.2% (729/791, 95%CI 90.1–93.9%) immunity observed in 2013–2018.

The baseline scenario refers to no supplementary immunisation activity (SIA) occurring; “Catch-up” refers to the implementation of a selective SIA designed to vaccinate individuals of the appropriate ages who missed earlier routine vaccination; “SIA” (non-selective SIA) indicates all individuals of the target age group are immunised with a one-dose vaccination schedule, regardless of their vaccination history. <2 y: children aged 8 months to 2 years; <15 y: children aged 8 months to 14 years; 20–45 y: non-pregnant women aged 20–45 years. A Model estimates of pediatric population immunity over time. The upper and lower panels show the estimated population mean log-concentrations and proportions of protected individuals respectively. The solid line, along with the dashed area, shows the point estimates and 95% confidence intervals. B Estimated pediatric immunity levels by age group and vaccination scenarios. C Scenario-based log-concentration distributions and D proportions of protected individuals among non-pregnant women of childbearing age and their infants (n = 245). In (C), the violin plots indicate the distributions and variance of log-concentrations. Each box plot shows minimum, first quartile, median, third quartile, and maximum values. In (D), each square or point with error bar shows the observed and model-based mean proportion of protected individuals and its 95% confidence interval. In (A, C), the grey vertical dashed lines indicate the starting date of hypothetical SIAs. The grey horizontal dotted line denotes a protective threshold of 200 mIU/ml in the upper panel of (A) or the 90% population immunity threshold in the lower panel of (A, D).
Next, we project the impact of hypothetical SIAs on reducing the known immunity gaps in the pediatric population. It is worth noting that non-selective (targeting all individuals in the selected age groups) and selective SIAs (targeting individuals who missed routine doses) have a differential impact on improving immunity levels. Selective SIAs has the most significant impact on population immunity in individuals born in years with relatively lower MCV uptake rates (Fig. 4B). We observed a 9.9–16.7% immunity increase in children under 4 years old born in 2020–2024 (vaccination rate with MCV1 and MCV2: 88%), and a 4.3% immunity increase among 12-year-olds born in 2013–2014 (92%). However, we find no statistical support for the selective SIA-induced population immunity increase among individuals aged 8–11 years who were born in years with MCV1 uptake rates exceeding 95% and show a marked waning of vaccine-induced immunity. By contrast, we observe a 23.5–50.0% immunity increase in this population following non-selective SIAs, suggesting that non-selective SIA can improve immunity levels in a highly vaccinated population by boosting individual antibody concentrations post-vaccination. These results did not change after considering the uncertainties in MCV2 vaccination coverage (Fig. S11). Furthermore, we estimate that achieving 90–95% population immunity can only be done when non-selective SIA targets all children aged <15 years (Fig. 4B). Given the suboptimal immunity level in childbearing-age women (52.2%, 95% CI 45.8–58.6%) and their offspring (88.9%, 95% CI 84.3–92.6%) in 2025 baseline, we also explore if non-selective SIA could increase their immunity. We show that vaccinating non-pregnant women of childbearing age who are already immunised could significantly improve immunity levels on women themselves (82.4, 95%CI 77.1–87.0%) and their offspring (100%, 95%CI 98.5–100%), even after considering variations in maternal immune status and a reported 28.4% decrease in serum immunity in women due to pregnancy15 (Figs. 4C, D, S8B and S12).
Discussion
In this study, we characterise long-term measles immunity dynamics among children and childbearing-age women in a setting with high MCV coverage. Our analysis suggests that population immunity has decreased in both children and childbearing-age women populations in the period following the COVID-19 pandemic, with distinct driving factors. In particular, we demonstrate immunity decreases in the pediatric and childbearing-age women populations are primarily attributed to waning immunity following routine vaccination, with the pediatric population additionally affected by pandemic-related vaccination delays. Our results also indicate that in a setting with high MCV coverage and low infection risk, as vaccinated individuals get older, waning immunity becomes increasingly important in driving a population immunity gap. We observe lower maternal antibody levels higher MCV responses in infants when their mothers’ antibody levels decrease. We have explored time variations in child population susceptibility, and evaluated the feasibility of implementing SIAs to restore population immunity in highly vaccinated children and non-pregnant women of childbearing age. We find that restoring 90–95% population immunity in a highly vaccinated population solely through selective SIAs is difficult to achieve, while implementing non-selective SIA to address the immunity gap resulting from waning vaccine-induced immunity within the target age groups makes it possible.
We found that childhood measles risk is associated with antibody concentration differences in the population of childbearing-age women. The low antibody concentrations in childbearing-age women who were born at a time of low measles infection risk in region of high vaccination coverage is likely linked to a lack of exposure to circulating measles virus, which may have led to the progressive decline of antibody concentrations after receiving routine vaccination in their first two years of life. These findings have significant implications not only for the childbearing-age women we studied and their newborns, but also for a much wider population who were born during a time of sustained high MCV coverages and low measles infection risk16,17,18. Moreover, such post-vaccination immunity waning could also have implications for other regions with high measles epidemic levels and low MCV coverage, as evidenced by the progressive decline in immunity observed among childbearing-age women born before 1983 who experienced similar conditions. Our present study focused on characterising pre- and post-pandemic immunity changes in women of childbearing age and did not aim to clarify the exact mechanisms involved in determining their current immunity profile, which would require further data collection and investigation.
While there is a good representation of female and male participants in our study location, one potential uncertainty in our conclusion concerns the variation in household socioeconomic status across the studies. However, given its non-confounding effect on child immunity levels (Table S4), this variation is unlikely to independently drive changes in population immunity at different time points. We also acknowledge a concern regarding the direct extrapolation of our estimated pediatric immunity level profiles, which were inherently driven by local measles antibody determinants (including local MCV coverage, measles epidemics19, MCV dose administration timing, population structure) and additional relevant factors (e.g., cellular immunity, co-infections, malnutrition, socio-economic disparities)20,21,22. Nevertheless, our conclusion regarding the increasing role of waning vaccine-induced immunity in driving a population immunity gap is likely to be broadly applicable to other high coverage settings, and is consistent with a recent study in England by Robert A et al.12. We were unable to directly relate antibody concentration levels spatially and temporally to different levels of measles incidence, vaccine coverage, social contact patterns and heterogeneous COVID-19 impacts (e.g. different local lockdown policies), as these factors had already been in effect before our study began and could not be separated due to limitations in our study design. We also found a clear impact of experimental errors on the observed antibody concentrations, highlighting the importance of rigorous assay quality control in future studies, even when standardized protocols are used. We note that the highest projected population immunity (90% or higher) in both child and childbearing-age women populations follows the implementation of non-selective SIAs. This means that SIA targeting all at-risk populations, rather than just undervaccinated individuals, may be needed. However, the trade-off between the intensified vaccination investment and benefits of improving population immunity needs to be an explicit part of supplementary immunisation strategy developments, as also pointed out by others23. Additionally, the more rapid waning of immunity in infants born by women with lower antibody concentrations may partly reflect the situation of increasing maternal age in both developed and many low- or middle-income countries (including China)24. This highlights global need for the development of more cost-effective ways to simultaneously improve infant and their mothers’ immunity, particularly in settings with low MCV coverage in young children25.
In conclusion, the immunity gaps identified in this study, particularly among individuals already vaccinated, could inform the definition of appropriate immunisation efforts based on age-specific priority targets. This is especially crucial for improving the suitability of future supplementary immunisation programmes across different sociodemographic and epidemiological settings. Our findings demonstrate that with non-selective supplementary immunisation activities in a highly vaccinated population, it is possible to restore population immunity to 90–95% or greater. However, before SIAs are implemented, operational challenges (such as vaccine hesitancy and the optimal vaccination time) need to be addressed. The success of using the proposed model to reconstruct the transplacental antibody transfer and individual immunity dynamics from birth enables its application in projecting the impact of different strategies designed to restore population immunity in settings with high MCV coverages.
Methods
Ethical approval
This study was approved by the Institutional Review Board of WHO Western Pacific Regional Office (2013.10.CHN.2.ESR), the Chinese Centre for Disease Control and Prevention (201224), and Fudan University (2019–05–0756, 2020-11-0857, 2020-11-0857-S, 2022-02-0950, and 2024-07-1142). Written informed consent was obtained from all caregivers of child participants and enroled adult participants themselves.
Study design and participants
We use epidemiological and measles serological data from two longitudinal cohorts followed in 2013-2024 respectively involving mother-infant pairs (n = 1066, referred to as the mother-infant cohort) and children aged 1–9 years (n = 4188, referred to as the child cohort), as well as an all-ages population-based cross-sectional study (n = 1016) conducted in 2021. All studies were conducted in Anhua County, Hunan Province, China, and included both male and female participants. Detailed profiles of the two cohorts have been provided elsewhere26,27,28. Participants in the three population-based studies were selected to represent local populations within designated age ranges during the study period. Enrolment and eight follow-up visits of cohort participants occurred between September 2013 and August 2024. In the mother-infant cohort, birthing women and their neonates were enroled between September 20, 2013 and October 14, 2015, and child participants were then followed at 2, 4, 6, 12, 24, and 36 months. In the child cohort, participants aged 1–9 years were enrolled between September 23, 2013 and November 25, 2013, and then followed semi-annually between February 25, 2014 and November 13, 2016. Additionally, centralised follow-ups were conducted for both cohorts between July 19 and October 31, 2021 (corresponding to the period during which the cross-sectional study was done), as well as from July 25 to August 13, 2024. For the cross-sectional study, a 2-pronged approach was used for participant recruitment, and detailed study profiles has been published elsewhere29. In brief, initial household-based enrolment was conducted in July 2021, followed by supplemental school-based enrolment in October 2021 to address shortfalls in the predefined sample size for school-age children and childbearing-age women.
Questionnaires (including socio-demographic and obstetric information) and blood sample collection were completed for each participant at each survey. Specifically, all child participants provided 2 ml venous blood samples (cord blood sample for neonates). For adult participants, 2 ml venous blood samples were collected from birthing women in the mother-infant cohort, while those in the cross-sectional study provided 4 ml venous blood samples. The selection of participants in the present study is shown below. For cohort participants, given the insufficient volume of their stored serum samples during the 2nd–6th follow-up visits, a minimum number of participants necessary to understand age-specific measles seropositivity was selected from the original cohorts (n = 2629, including 555 from the mother-infant cohort and 2074 from the child cohort)19. For participants in the cross-sectional study, individuals were selected if they are within the same age range as the cohort children (aged 0–14 years, n = 273) and birthing women (aged 20–45 years, n = 217) followed in 2013–2018 (n = 490), given the age targets of the present study. Information about the history of vaccination and infection has been extracted from participants’ vaccination cards (the official and legal documents to show the completeness of routine vaccination schedules) and official line list of measles cases respectively.
Laboratory procedure
For each blood draw of each selected participant, anti-measles virus IgG antibody concentration was measured using commercial ELISA kits (SERION ELISA classic measles virus IgG, Institut Virion/Serion GmbH, Wurzburg, Germany). All samples were diluted 1:100 in assay diluents before testing. The negative control and standard sera (from the kit) were ready to use without further dilution. The resulting optical density values were converted into concentration units (mIU/ml) based on a calibration curve generated from standard serum using SERION software. We validated the consistency of ELISA results between different testing batches by use of WHO International Standard for anti-measles serum (Fig. S2) and their consistency with the gold-standard plaque reduction neutralisation test (PRNT). The procedure of the PRNT test and the consistency between the two assays have been provided elsewhere19 and are briefly summarized in the Supplementary Text.
Statistical analyses and mathematical modelling
Characterising immunity changes before and after COVID-19 pandemic period
To explore long-term measles immunity profiles before and after the COVID-19 pandemic period, we used serological data from children aged 0-14 years and non-pregnant women of childbearing age (20–45 years) from the three population-based studies. We determined the point estimates of age- or time-specific mean concentrations and proportion of children being susceptible to measles virus infections, along with their 95% confidence intervals (95% CI). The 95% CI of mean concentrations was obtained with t distribution, while the Clopper-Pearson exact binomial confidence interval was calculated for the proportion of susceptible children. We used a generally accepted protective threshold of 200 mIU/ml to define individual immunity/susceptibility30,31. We also calculated the individual transplacental transfer ratio of maternal antibodies, which was defined as the geometric mean of the ratio of the neonate-to-mother log-concentration. We compared group means with a t-test and proportions with the χ² test or Fisher’s exact test. In addition, we built linear regression models to determine the association between maternal and neonatal log-concentrations. Linear mixed models were used to analyse which factors affected individual antibody levels in child and childbearing-age participants.
In addition, we analyse child population susceptibility over time based on their longitudinal vaccination records and antibody concentration predictions. For individuals who are eligible to vaccination (\(\ge\)8 months), we define their susceptibility status as follows: (1) undervaccination for those without any vaccination records and with antibody concentration lower than 10 mIU/ml over all serum samples (the estimated minimum mAb level at 8 months); (2) primary vaccine failure for those with exact vaccination dates but without post-vaccination seroconversion (i.e., the transition from seronegative to seropositive status or a fourfold antibody rise in consecutive serum samples); (3) immunity waning post-vaccination for those with exact vaccination dates and post-vaccination seroconversion but with a subsequent serum sample showing below-threshold concentration
Modelling maternally derived and vaccine-induced immunity
Correcting for potential experimental errors in antibody measurements
Before assessing how maternal immunity levels and various hypothetical SIA activities shift immunity levels in the target populations, we first characterised the impact of batch effects (random effects) on antibody concentration levels (Fig. S2A). The resulting distribution was then used as a prior for inferring batch-specific experiment errors in our Bayesian hierarchical model (Eq. 1, Table S6). Assuming that individual antibody measurements within each batch share a random effect, \({A}_{\varepsilon }\) (i.e., a constant batch-specific measurement error), individual ELISA-detectable log-concentration \({A}_{s,\varepsilon }\) can be modelled as the sum of the “true” log-concentration \({A}_{s}^{*}\) and batch effects \({A}_{\varepsilon }\) as described below:
Reconstruction of transplacental antibody transfer and infant vaccine responses
With the error-corrected antibody measurements, we then constructed models to understand the mechanisms of transplacental antibody transfer from birthing women and of antibody response dynamics in children from birth. The latter model includes the decay of maternally derived antibodies, as well as vaccine-induced peak antibody increases and subsequent decay. We specifically examined how individual immunity levels immediately prior to vaccination affects their vaccine responses, based on our previously established model frameworks26. We assume that maternally derived and vaccine-induced antibodies will decay exponentially over time. We allow for population-level decay rates of maternally derived (\(\gamma\)) and vaccine-induced antibodies (\(\lambda\)). After each vaccination, we anticipate an immediate increase in individual antibody levels, with the increased level expected to be linearly correlated with the pre-existing antibody level immediately prior to vaccination (referred to as the linear response mechanism below), as supported in our data (Fig. S9).
We first model the transplacental transfer of maternal antibodies and infant antibody dynamics using serological data from the mother-infant cohort only (model A). In light of the observed relationship between log-concentrations in birthing women and the corresponding transplacental transfer ratio (Fig. 1D), we use an exponential function to characterise transplacental transfer of maternal antibodies from birthing women, \({A}_{i,m}\), to their neonates, \({A}_{i,0}\), with a transplacental transfer ratio of \({\eta }_{i}\).
We then model the decay of infant maternally derived antibodies as Eq. (4).
To predict MCV1-induced peak increase in infant log-concentrations, we use the observed linear relationship between pre-existing log-concentration immediately prior to vaccination, \({A}_{i,\psi=1}\) (\(\psi\): dose number), and peak log-concentration increase, \({\alpha }_{i,\psi=1}\), shown in Eqs. (5)–(6).
The exponential decay of post-MCV1 log-concentrations, \({A}_{i,t,\psi=1}\), can be described as:
We also model individual MCV2-induced peak log-concentrations, \({A}_{i,t,\psi=2}\), and its subsequent log-concentration decay, shown in Eqs. (8)–(10).
where \({A}_{i,\psi=2}\) and \({\alpha }_{i,\psi=2}\) denote the pre-existing antibodies immediately prior to MCV2 and MCV2-induced peak log-concentration increase respectively.
Reconstruction of individual vaccine response across different pre-existing antibody levels
We aim to obtain the impact of various SIA activities on population immunity through aggregating their effects on individual antibody levels in the target populations. This requires a complete picture of individuals’ response mechanisms to a new vaccination event, taking into account their pre-existing antibody level immediately prior to such vaccination. To address this, we extended model A to incorporate antibody measurements in both cohorts (model B). As participants in the child cohort had antibody measurements post-MCV1 only, we instead estimate their initial log-concentration at enrolment. The decay of their initial log-concentration (\({A}_{i,\tau 0}\)) at enrolment \({\tau }_{i,0}\), as well as those from children in the mother-infant cohort (\({A}_{i,0}\)), now follows:
Then, we focus on determining the mechanisms of individual vaccine responses across different pre-existing antibody levels immediately prior to a new vaccination event \(\psi\). Supported by our data (Fig. S9), we consider two linear vaccine response mechanisms that relate individual peak log-concentration increase post-vaccination to their pre-existing log-concentrations immediately prior to vaccination. First, for individuals with below-threshold log-concentrations immediately prior to vaccination, we assume their vaccine-induced responses align with the MCV1-induced linear response mechanism (refer to Eq. (6) for details). For the second, we consider vaccine-induced responses (\({\alpha }_{i,\psi \ge 2}\)) in individuals with above-threshold log-concentrations immediately prior to vaccination (\({A}_{i,\psi \ge 2}\)) to be consistent with the post-MCV2 induced linear response mechanism, as shown in Eq. (13).
Next, we use Eq. (14) to show the decay of peak log-concentration following a new vaccination event:
Alternative model form for antibody decay
For both maternally derived and vaccine-induced antibodies, we explored an alternative biphasic model (model C) that accounts for short-term and long-term components of the antibody response, each with separate exponential rates14,32. For example, for maternal antibodies, the model can be expressed as:
where \(\delta\) is the proportion of the antibody response that is short lived, which was assumed to differ between maternally derived and vaccine-induced antibodies.
The above-mentioned model parameters have been summarised in Table S6. Model fitting was conducted in CmdStanR version 0.5.3. Each model was run with three chains of 3000 iterations each, with a warm-up period of 2000 iterations. Convergence was assessed by visual assessment of chain mixing and by R-hat convergence diagnostic. The WAIC and the expected log pointwise predictive density (ELPD) were used to compare model performance.
Model validation
For model A, we address model validation both within the cohort participants and from a broader population perspective. In the first analysis, we predict individual antibody dynamics among child participants in the mother-infant cohort who had exact vaccination times and were followed in 2021–2024 (n = 82). This prediction is made using the parameter estimates from model A, as well as log-concentrations observed in cohort birthing women and the times of children’s vaccination. In the second analysis, we draw 10,000 random samples from the distribution with a mean and standard deviation of log-concentrations from cohort birthing women, assuming it represents the obstetric population in the real world. We then predict the dynamics of maternally derived immunity in the first year of life using the random draws and the parameter estimates. For model B, we validate its ability to predict individual vaccine response across different pre-existing antibody levels immediately prior to vaccination. This validation is based on the 10,000 random samples drawn from the distribution with a mean and standard deviation of cord blood log-concentrations in the mother-infant cohort (as the initial log-concentrations for children in both cohorts), along with the parameter estimates and vaccination times from both cohorts. In these validation analyses, we assess model performance based on the consistency between the predicted mean log-concentration or susceptibility and those derived from measurements.
Estimating the impact of maternal antibody levels on shifting pediatric immunity profiles
Given the substantial reduction in immunity levels observed in childbearing-age women in 2021–2024 compared to those in 2013–2015, we prospectively explore how this reduction in maternal antibody levels affects pediatric immunity profiles. Using the validated framework of model A, we simulate the decay of maternally derived immunity, peak log-concentration increases following MCV1/MCV2 vaccination, and long-term susceptibility changes from birth to 10 years of age. Such analysis relies on the parameter estimates from model A, random draws (n = 10,000) from birthing women’s log-concentration distribution in different scenarios (baseline: mAb level consistent with its 2013–2015 level; lower mAb scenario: mAb level consistent with its 2021–2024 level), as well as pre-defined timings of MCV1/MCV2 at 8 and 18 months of age. In these scenarios, the log-concentration distributions are presumed to represent the obstetric population during the study period. The susceptibility changes between the two scenarios are defined as the estimated proportion of susceptible children in the lower mAb scenario minus those derived from the baseline scenario.
Additionally, considering the differences in immune status in women of childbearing age—shaped by local measles epidemics and vaccination policy/coverage—we also simulated infant susceptibility changes across different immunisation groups. In particular, we classified non-pregnant women of childbearing-age into three immunisation groups. These included: (1) individuals born in 1978–1986, a period marked by high measles transmission and low coverage of a one-dose MCV schedule; (2) those born in 1987–1997, who experienced high measles transmission and low coverage of the two-dose MCV schedule administered at 8 months and 7 years; and (3) individuals born in 1998–2003, a period with continued high measles epidemic levels but relatively high coverage of the two-dose MCV schedule. For each group, we then simulated the transplacental transfer of their pre-existing immunity to newborns, followed by subsequent antibody decay, using exponential functions as described in Eqs. (2)–(4).
Assessing the impact of various SIA activities on improving population immunity
We then use the two validated models to determine the impact of various hypothetical SIA activities in July 2025 on population immunity in the target populations, including both children and non-pregnant women of childbearing age. Across different SIA scenarios, the population immunity level is determined by the proportion of individuals with above-threshold log-concentration estimates. Individual log-concentration estimates are obtained using their 2021 antibody measurements and the model parameter estimates. For children aged 0–2 years lacking antibody measurements in 2025, we instead estimate their log-concentration distributions through a simulation study. In such a simulation study, we first determined the number of participants to be included (n = 163), which was calculated using the age structure in our study location and the age-specific number of child participants with available antibody measurements from 2021. We next assigned random draws as their initial log-concentrations at birth, similar to the validation analyses. We consider the following SIA scenarios: (1) the absence of SIA (baseline); (2) selective SIA, targeting children who missed routine doses; and (3) non-selective SIA, targeting all children in the selected age groups regardless of their vaccination history. We consider both selective and non-selective SIAs targeting children with different age groups, while all non-pregnant women of childbearing age, regardless of their immune status, were assumed to receive non-selective SIA only. In the simulation study of SIA-induced antibody increases, we assumed a validated linear relationship with pre-existing antibody levels (Eq. (13)), regardless of the target populations. For childbearing-age women with different immune status, the transplacental transfer of their post-SIA immunity to newborns was modelled using exponential functions, with the relevant parameters derived from Eqs. (2)–(3).
All analyses were performed in R, version 4.2.1.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Because of privacy and ethical reasons, individual epidemiological and serological data cannot be made public, but they are available from the corresponding author (H.Y.) on request. The time frame for a response to requests is 1–2 weeks. We have provided the synthetic dataset, and aggregated de-identified data generated in this study. These datasets have been deposited in Zenodo at https://doi.org/10.5281/zenodo.1721204233. Source data are provided with this paper.
Code availability
The codes to reproduce the main results in this study have been deposited in Zenodo at https://doi.org/10.5281/zenodo.1721204233.
References
Patel, M. K. Progress toward regional measles elimination — Worldwide, 2000–2019. MMWR Morb. Mortal Wkly Rep. 69, 1246–1251 (2020).
Dixon, M. G. Progress toward regional measles elimination — Worldwide, 2000–2020. MMWR Morb. Mortal Wkly Rep. 70, 1563–1569 (2021).
Minta, A. A. et al. Progress Toward Measles Elimination — Worldwide, 2000–2023. MMWR Morb. Mortal. Wkly. Rep. 73, 1036–1042 (2024).
Fu, H. et al. Impact and cost-effectiveness of measles vaccination through microarray patches in 70 low-income and middle-income countries: mathematical modelling and early-stage economic evaluation. BMJ Glob. Health 8, e012204 (2023).
Kaur, G. Routine Vaccination Coverage — Worldwide, 2022. MMWR Morb. Mortal. Wkly. Rep. 72, 1155–1161 (2023).
Hartner, A.-M. et al. Estimating the health effects of COVID-19-related immunisation disruptions in 112 countries during 2020–30: a modelling study. Lancet Glob. Health 12, e563–e571 (2024).
Minta, A. A. Progress Toward Measles Elimination — Worldwide, 2000–2022. MMWR Morb. Mortal Wkly Rep. 72, 1036–1042 (2023).
Centers for Disease Control and Prevention. Measles Cases and Outbreaks. Measles (Rubeola) https://www.cdc.gov/measles/data-research/index.html (2025).
European Centre for Disease Prevention and Control. Threat assessment brief: Measles on the rise in the EU/EEA - Considerations for public health response. https://www.ecdc.europa.eu/en/publications-data/threat-assessment-brief-measles-rise-eueea-considerations-public-health-response (2024).
World Health Organization. A 30-fold rise of measles cases in 2023 in the WHO European Region warrants urgent action. https://www.who.int/europe/news/item/14-12-2023-a-30-fold-rise-of-measles-cases-in-2023-in-the-who-european-region-warrants-urgent-action.
Leuridan, E. et al. Early waning of maternal measles antibodies in era of measles elimination: longitudinal study. BMJ 340, c1626 (2010).
Robert, A., Suffel, A. M. & Kucharski, A. J. Long-term waning of vaccine-induced immunity to measles in England: a mathematical modelling study. Lancet Public Health 9, e766–e775 (2024).
World Health Organization. Measles outbreaks strategic response plan: 2021–2023: Measles outbreak prevention, preparedness, response and recovery. https://www.who.int/publications/i/item/9789240018600.
Salje, H. et al. Reconstruction of antibody dynamics and infection histories to evaluate dengue risk. Nature 557, 719–723 (2018).
Miller, E. M. Changes in serum immunity during pregnancy. Am. J. Hum. Biol. 21, 401–403 (2009).
Perofsky, A. C. et al. Impacts of human mobility on the citywide transmission dynamics of 18 respiratory viruses in pre- and post-COVID-19 pandemic years. Nat. Commun. 15, 4164 (2024).
Nicolay, N., Mirinaviciute, G., Mollet, T., Celentano, L. P. & Bacci, S. Epidemiology of measles during the COVID-19 pandemic, a description of the surveillance data, 29 EU/EEA countries and the United Kingdom, January to May 2020. Eur. Surveill. 25, 2001390 (2020).
Centers for Disease Control and Prevention. Assessing Measles Outbreak Risk in the United States. National Center for Immunization and Respiratory Diseases https://www.cdc.gov/ncird/whats-new/measles-outbreak-risk-in-us.html (2025).
Wang, R., Jing, W., Liu, M. & Liu, J. Trends of the Global, Regional, and National Incidence of Measles, Vaccine Coverage, and Risk Factors in 204 Countries From 1990 to 2019. Front. Med. 8, 798031 (2021).
Lanke, R. & Chimurkar, V. Measles outbreak in socioeconomically diverse sections: a review. Cureus 16, e62879 (2024).
Di Guardo, G. COVID-19: measles and antibiotic resistance are a matter of concern. Pathogens 10, 449 (2021).
Noori, N. et al. Potential impacts of mass nutritional supplementation on measles dynamics: a simulation study. Am. J. Trop. Med. Hyg. 107, 863–872 (2022).
Winter, A. K. et al. Feasibility of measles and rubella vaccination programmes for disease elimination: a modelling study. Lancet Glob. Health 10, e1412–e1422 (2022).
Hochler, H. et al. The impact of advanced maternal age on pregnancy outcomes: a retrospective multicenter study. J. Clin. Med. 12, 5696 (2023).
Flannery, D. D. et al. Measles serostatus among parturient patients at 2 Philadelphia Hospitals in 2021. JAMA 329, 682–684 (2023).
Wang, W. et al. Dynamics of measles immunity from birth and following vaccination. Nat. Microbiol. 9, 1676–1685 (2024).
Wei, X. et al. The transfer and decay of maternal antibodies against enterovirus A71, and dynamics of antibodies due to later natural infections in Chinese infants: a longitudinal, paired mother–neonate cohort study. Lancet Infect. Dis. 21, 418–426 (2021).
Yang, J. et al. Seroepidemiology of enterovirus A71 infection in prospective cohort studies of children in southern China, 2013-2018. Nat. Commun. 13, 7280 (2022).
Wu, Y. et al. Measles population immunity in Hunan, China: a serological assessment. Open Forum Infect. Dis. 12, ofaf216 (2025).
Argüelles, M. H. et al. Measles virus-specific antibody levels in individuals in Argentina who received a one-dose vaccine. J. Clin. Microbiol. 44, 2733–2738 (2006).
Bautista-López, N. L., Vaisberg, A., Kanashiro, R., Hernández, H. & Ward, B. J. Immune response to measles vaccine in Peruvian children. Bull. World Health Organ 79, 1038–1046 (2001).
White, M. T. et al. A combined analysis of immunogenicity, antibody kinetics and vaccine efficacy from phase 2 trials of the RTS,S malaria vaccine. BMC Med. 12, 117 (2014).
Wang, W. waning_immunity_source. Zenodo https://doi.org/10.5281/zenodo.17212042 (2025).
Acknowledgements
W.W. acknowledges financial support from the Young Scientists Fund of the National Natural Science Foundation of China (82304205). H.Y. acknowledges financial support from the Key Program of the National Natural Science Foundation of China (82130093). M.J. was funded by the Bill & Melinda Gates Foundation (INV-034281 and INV-016832). H.S. was supported by funding from the European Research Council (grant number: 101170844). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
H.Y. conceived, designed, and supervised the study. Q.W., S.Z., and X.Z. did the laboratory tests. W.W. collated data, performed the analysis, and wrote the first draft of the manuscript. W.W., S.C., H.S., M.J., and H.Y. discussed the results and contributed to revisions of the manuscript.
Corresponding author
Ethics declarations
Competing interests
H.Y. has received research funding from Sanofi Pasteur, Shenzhen Sanofi Pasteur Biological Products Co., Ltd, Shanghai Roche Pharmaceutical Company, and SINOVAC Biotech Ltd. None of these funds is related to this work. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention. All other authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks the anonymous reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, W., Wang, Q., Zhao, S. et al. COVID-19 pandemic and waning immunity disrupted measles population immunity and strategies to close immunity gaps. Nat Commun 16, 10966 (2025). https://doi.org/10.1038/s41467-025-65955-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-65955-x
