
Abstract
Adolescent major depressive disorder (MDD) involves complex and heterogeneous alterations in brain functional organization. A possible explanation is the disruption of individualized brain maturation during adolescence, which typically transitions from lower-order sensory to higher-order association regions. To test this hypothesis, we analyzed resting-state functional MRI data using advanced matrix decomposition techniques to extract organizational gradients, temporal dynamics, and information flow. Clustering sensory–association gradient features in our main sample (NMDD = 302 and NControls = 207; ages 11-17) revealed two subtypes. Subtype 1 showed bottom‑up (sensory‑to‑association) flow, reduced synergy but heightened redundancy in sensory cortices, and a highly modular yet globally inefficient network—patterns consistent with aberrant sensory processing and impaired integration. Subtype 2 instead displayed a top‑down (association‑to‑sensory) flow, reduced synergy in association areas, elevated redundancy in sensory regions, and network efficiency between subtype 1 and healthy controls, suggesting compensatory higher‑order engagement. Subtypes also differed in age-related changes, clinical profiles, and neurobiological processing. These patterns were largely replicated in an independent sample (NMDD = 73 and NControls = 28). Overall, the sensory-association axis distinguishes MDD subtypes, integrating functional heterogeneity, cortical dynamics, developmental trajectories, and genetic influences, offering new insights for pathophysiology and precision psychiatry.
Similar content being viewed by others


Introduction
Adolescent major depressive disorder (MDD) poses significant challenges due to the complex manner of clinical symptoms with biological substrates and may exhibit heterogeneous transitions over puberty1,2,3. These heterogeneous phenomena influence the efficacy of pharmacological and psychological interventions, complicating clinical assessments and therapeutic outcomes4. One possible reason for this heterogeneity is that the highly individualized maturation process during adolescence, including the transition from low-order sensory and unimodal areas to higher-order association regions, is disrupted in MDD. However, systematic analysis of hierarchical information interaction patterns along the cortical hierarchy in MDD remains elusive. Advanced by the development of neuroimaging techniques, especially functional MRI (fMRI), researchers can elucidate the multidimensional neural substrates5,6,7, uncover the underlying individual-level mental variability8, and identify distinct neurodevelopmental trajectories that may underlie variations in symptom presentation and treatment response9,10,11. Such functional alteration was validated across different samples with various symptom severity and was stable over time10, suggesting that intrinsic brain networks serve as heterogeneous neural biomarkers in depression.
More recently, pioneering work has revealed that large-scale cortical networks are systematically organized along multidimensional hierarchical axes, for example, the sensory-to-association (S-A) and somatomotor-to-visual (S-V) axes, as the most representative dimensionalities in the intrinsic brain organization12. These hierarchical axes have been found shifted during adolescence, with progression from lower-order sensory and unimodal regions to higher-order association regions13,14,15,16. Such extended plasticity of late-maturing association regions is a hallmark of human development15 and a key risk factor for MDD17. For instance, functional gradients in adult MDD patients exhibit significant global and focal alterations, which are associated with sensory processing, higher-order cognitive functions, and specific gene expression profiles17, indicating adult MDD subtypes could be characterized by their functional deviations18. However, healthy adolescents exhibit significant individual variability in cognitions19 and neural representation throughout development20,21, and their functional heterogeneity has not yet been fully elucidated. Here, we hypothesize that adolescent MDD could be classified into distinct neurobiological subtypes along the S-A axis, with different S-A axis features having different information interaction dynamics.
Previous studies have demonstrated that the human brain exhibits distinct sensory and association interaction via different temporal dynamics and stream profiles22,23, reflecting how the brain processes external environmental information24,25. Adolescents with MDD exhibited complex symptoms, encompassing social information processing, cognitive control, and emotion regulation functions. They could also be summarized by abnormal information processing and exchanging abilities from the external environment26,27,28,29,30. Information decomposition theory provides an expanded neural framework to explain how different MDD subtypes process external information along brain gradients and integrate symptom diversity into a unified cognitive framework, extending to transdiagnostic and comorbid issues in psychiatric disorders31,32,33,34. Furthermore, the redundant interactions between sensory and association regions shape the neurocognitive architecture, offering insights into the neural organization and information processing characteristics of different MDD subtypes35. For instance, studies have shown that dynamic synergistic measurements derived from fMRI data are significantly disrupted in patients with chronic disorders of consciousness36, further highlighting the importance of dynamic information processing patterns in psychiatric disorders. However, such temporal dynamics and stream profiles of adolescent MDD are still unclear.
In this study, we leveraged multi-site resting-state fMRI data to investigate brain functional reorganization, temporal dynamics, and information stream in adolescents with MDD compared to healthy controls (HC). We first calculated functional gradients and identified two distinct subtypes using an unsupervised machine learning pipeline. These two subtypes exhibited distinct clinical symptom patterns and were consistently reproducible across independent dataset. To further elucidate the aberrant integration patterns between sensory and association regions, we applied synergy-redundancy information decomposition to analyze the information processing modes associated with functional reorganization in these two subtypes.
Results
Distinct neurofunctional signatures of the two subtypes in adolescents with MDD
In this study, we included two independent datasets (Supplementary Table 1): an exploratory dataset comprising 302 adolescents with MDD (15.40 ± 2.09 years old, 134 females) and 207 HC (15.53 ± 1.98 years old, 82 females). All participants were right-handed, of Han Chinese ethnicity, and free from other psychiatric or major physical illnesses. Each participant’s fMRI data underwent identical quality control procedures, including the exclusion of scans with excessive head motion or image artifacts. Then, each participant’s fMRI time series was parcellated into Schaefer 400 cortical regions37 and calculated Pearson correlation to obtain functional connectivity matrices. Further, the group-level functional connectivity matrix is obtained by averaging individual functional connectivity matrices. At the group level, connectivity matrices underwent Fisher z-transformation, retaining only the top 10% of connections per region. A similarity matrix was subsequently generated using the normalized angle kernel, and the diffusion map embedding38 method was applied to extract functional gradients, yielding a group-level gradient template. The same procedure was applied to individual functional connectivity matrices, and the resulting individual gradients were aligned to the group template via Procrustes-based rotation, thereby facilitating consistent comparisons via one-way analysis of variance (ANOVA) with Tukey’s Honest Significant Difference (HSD) across groups and subtypes.
Next, we investigated various clustering solutions (from 2 to 10) of adolescent MDD’s functional gradients with a machine learning algorithm. Results showed that the best optimized clustering number was 2 (Fig. 1a) and the similarity within subtype 1 (N = 140, 15.37 ± 2.14 years old, 62 females), subtype 2 (N = 162, 15.42 ± 2.03 years old, 72 females), and HC was larger than across subtypes. To further verify the effectiveness of these two subclasses, a support vector machine (SVM) was used to classify the different groups. We found classification accuracy of subtype 1 and subtype 2 was 99.37%, subtype 1 and HC was 89.98%, subtype 2 and HC was 98.52% (Supplementary Fig. 1). To verify the robustness of the subtype classification, we further repeated the analyses using alternative methods and datasets (Supplementary Fig. 2). First, we applied hierarchical clustering to re-derive the subtypes and computed functional gradient and reorganization maps, which showed high consistency with the main analysis (subtype 1–HC: r = 0.68; subtype 2–HC: r = 0.92; subtype 2–subtype 1: r = 0.86; all pspin < 0.001). Second, we repeated the analyses with a balanced dataset, which also revealed patterns significantly correlated with the main results (subtype 1–HC: r = 0.43; subtype 2–HC: r = 0.79; subtype 2–subtype 1: r = 0.68; all pspin < 0.05). We also select the MDDs whose Hamilton Depression Rating Scale (HAMD) score is greater than 20 (N = 234). We applied the same analysis on this selected dataset, which showed high consistency with the main analysis (Supplementary Fig. 3; (subtype 1–HC: r = 0.95; subtype 2–HC: r = 0.98; subtype 2–subtype 1: r = 0.99; all pspin < 0.001). These findings demonstrate that, regardless of clustering method or sample balancing, the functional organizational differences between subtypes and healthy controls can be reliably captured, thereby confirming the stability and robustness of the subtype definitions.

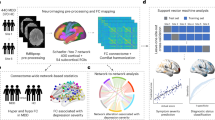
a The optimal number of subtypes for adolescent MDD was determined to be 2 using stability analysis. Points and error bars represent mean ± SD of the 1000 repetitions in the identification of the clustering stability. Similarity matrices indicate that within-subtype similarity for subtype 1 (N = 140), subtype 2 (N = 162), and health controls (HC; N = 207) is higher than across subtypes. b Functional gradient maps across subtype 1, subtype 2, and HC show a continuous spatial transition from sensory regions to association regions in all groups. c Density plots illustrate functional gradient values (number of subjects multiplied by the number of parcels with NSubtype 1 = 56,000, NSubtype 2 = 64,800, and NHC = 82,800), similarity between individual gradient and template gradient (number of subjects with NSubtype 1 = 140, NSubtype 2 = 162, and NHC = 207), and global dispersion differences (number of subjects with NSubtype 1 = 140, NSubtype 2 = 162, and NHC = 207) among subtype 1, subtype 2, and HC. Subtype 1 shows lower global gradient dispersion compared to subtype 2 (t = −3.08, pHSD = 0.002, one-sided). Box plots depict the interquartile range (IQR) and the median value of the distribution. Whiskers extend to the nearest points ± 1.5 × IQR above and below the 25th and 75th percentiles. Asterisks indicate a significant difference between box plots (*pHSD < 0.05). Group differences were compared using one-way analysis of variance (ANOVA), with head motion, age, handedness, and sex as covariates. Then, false discovery rate (FDR) with q < 5% was used to consider the multiple comparisons correction. Furthermore, post hoc analysis with Tukey’s Honest Significant Difference (HSD) was implemented to clarify the multiple comparisons among various groups. d Functional reorganization patterns were visualized through group comparisons. Subtype 1 primarily exhibited motor cortex contraction, while subtype 2 showed expansion in posterior cingulate and occipito-parietal association cortices and contraction in frontal and insula regions compared to HC. e Cognitive decoding highlights functional differences between subtype 1 and subtype 2. Subtype 1 is associated with sensory functions (e.g., movement, visual perception, and multisensory), while subtype 2 involves higher-order cognitive functions (e.g., language, pain, and sentence comprehension). Word clouds illustrate the cognitive domains linked to functional reorganization patterns in both subtypes. Source data are provided as a Source Data file.
The averaged functional gradient maps across subtype 1, subtype 2, and HC demonstrated a continuous spatial transition from unimodal to transmodal regions in all groups (Fig. 1b). The similarity between individual gradients and standard templates for subtype 1, subtype 2, and HC was: 0.59 ± 0.14, 0.58 ± 0.18 and 0.49 ± 0.23, respectively. We calculated three global scores for gradients, including loading range, individual similarity, and network dispersion (Fig. 1c). Specifically, we found subtype 1 shows lower global gradient dispersion compared to subtype 2 (t = −3.08, pHSD = 0.002), with significant distinctions in sensory and association regions. We further defined dispersion by calculating the Euclidean distance between individual regions and the manifold centroid to quantify continuous variation along spatial organization through the cortex. Regions exhibiting higher global dispersion values demonstrated greater segregation, whereas regions with lower values showed enhanced integration with proximal areas. Network-level results could be seen in Supplementary Fig. 4.
Regarding the regional comparisons, we found a contraction pattern mainly in the primary motor, auditory and visual cortices in subtype 1 compared to HC, while an expansion pattern in association cortex and a contraction pattern in frontal regions and insula region in subtype 2 compared to HC (Fig. 1d, pFDR < 0.05). Furthermore, Neurosynth-based cognition decoding results (Fig. 1e) revealed that the functional reorganization pattern of subtype 1 was sensory functions (e.g., movement, visual perception, and multisensory), while subtype 2 was mainly featured by high-order cognitions (e.g., language, pain, and sentence comprehension). In total, these results emphasize that one subtype of MDD was dominantly associated with sensory reorganization and another was associated with association reorganization. Specifically, subtype 1 was associated with sensory reorganization, characterized by the contraction in primary motor, auditory, and visual cortices and increased segregation within the sensorimotor and salience networks, while exhibiting reduced segregation in the limbic and default mode networks. In contrast, subtype 2 was linked to association network reorganization, marked by expansion pattern in posterior cingulate and occipito-parietal association cortices and enhanced segregation within higher-order networks such as the dorsal attention and control networks, significantly greater than in HC. These findings highlight the pronounced heterogeneity in functional reorganization and neural network architecture across adolescent MDD subtypes.
Two subtypes of adolescent MDD reflect different neurodynamics
Next, we investigated the neurodynamics using the regression dynamic causal model (rDCM)22,23, as suggested by previous studies23. The specific method details can be found in the “Methods” section. We found rDCM captures information flows in various regions in subtype 1, subtype 2, and HC (Fig. 2 and Supplementary Fig. 5). Here, the sensory-association information directions were used to define bottom-up (sensory to association) and top-down (association to sensory) information flow. Then, we calculated the flow ratios, defined by the outward degree between sensory regions and association regions. The flow ratios represent global bottom-up dynamics if the ratio value is larger than one, while it is top-down dynamics if this value is less than one. We found that the flow ratio values in subtype 1 (t = 3.24, p < 0.001) and subtype 2 (t = −3.68, p < 0.001) were significantly different from one via two-sided one-sample t-test. Then, we further compared the ratio values among subtype 1, subtype 2, and HC via one-way ANOVA and post hoc analysis through HSD with head motion, age, handedness, and sex as covariates. The post hoc analysis showed that the flowing ratio values in subtype 1 were significantly higher than HC (t = 7.47, pHSD < 0.001) and subtype 2 (t = 10.76, pHSD < 0.001). The flow ratio values in subtype 2 were significantly lower than HC (t = −6.47, pHSD < 0.001). Together, those results indicated that the dominant dynamic pattern in subtype 1 was more bottom-up, while in subtype 2 it was more top-down.

The flow ratio (number of subjects with NSubtype 1 = 140, NSubtype 2 = 162, and NHC = 207) values in subtype 1 were significantly higher than HC (t = 7.47, pHSD = 6.80 × 10−13, one-sided) and subtype 2 (t = 10.76, pHSD = 4.79 × 10−21, one-sided). The flow ratio values in subtype 2 were significantly lower than HC (t = −6.47, pHSD = 3.08 × 10−10, one-sided). Specifically, we examined neurodynamics using regression dynamic causal modeling (rDCM) to characterize information flow among brain regions in subtype 1, subtype 2, and HC. Bottom-up and top-down flows were defined based on sensory-to-association (bottom-up) and association-to-sensory (top-down) interactions. Flowing ratios, calculated as the outward degree from sensory to association regions, indicated predominantly bottom-up global dynamics when greater than 1 and predominantly top-down dynamics when less than 1. Box plots depict the IQR and the median value of the distribution. Whiskers extend to the nearest points ± 1.5 × IQR above and below the 25th and 75th percentiles. Asterisks indicate a significant difference between box plots (*pHSD < 0.001). Group differences were compared using one-way ANOVA, with head motion, age, handedness, and sex as covariates. Then, post hoc analysis with HSD was implemented to clarify the multiple comparisons among various groups. Source data are provided as a Source Data file.
Different neural information processing patterns in adolescent MDD subtypes
Information from the external environment is processed along a gradient toward deeper brain regions35. In this section, we applied Integrated Information Decomposition (IID) to resting-state fMRI data across different subtypes of MDD (Fig. 3a). This method allows us to quantify the extent to which information about the brain’s future trajectory is redundantly encoded by distinct brain regions, as well as the extent to which it is mediated by synergistic interactions between regions. By differentiating between synergistic and redundant interactions in the time series of Schaefer 400 brain regions, we independently ranked each brain region based on the degree of its synergistic and redundant interactions with other regions. The difference between these rankings (synergy values and redundancy values) was used to determine the relative contribution of each region to synergistic versus redundant processing, thereby establishing a redundancy-to-synergy gradient across brain regions. Positive values represent higher synergistic interactions, indicating that brain regions are more inclined to process information through cross-region synergy. In contrast, negative values indicate higher redundant interactions, reflecting a tendency for brain regions to share similar information.

a Integrated information decomposition framework illustrating synergy and redundancy along the sensory-association (S-A) axis. b Group differences in synergy-redundancy gradients (pFDR < 0.05). Subtype 1 additionally showed reduced interactions in sensory regions, including motor and auditory cortices. Direct comparisons revealed that subtype 1 had more pronounced interactions in the left frontal and temporal cortices, but reduced interactions in the right frontal and temporal cortices. c The comparison of synergy and redundancy values in sensory (left) and association (right) regions among subtype 1, subtype 2, and HC. In sensory regions, both subtypes showed reduced synergy but elevated redundancy compared to HC (synergy: subtype 1 vs. HC, t = −7.06, pHSD = 9.01 × 10−12; subtype 2 vs. HC, t = −8.18, pHSD = 4.80 × 10−15, one-sided; redundancy: subtype 1 vs. HC, t = 3.19, pHSD = 2.59 × 10−3; subtype 2 vs. HC, t = 3.98, pHSD = 2.37 × 10−5, one-sided), with subtype 1 exhibiting higher redundancy than subtype 2 (t = 4.03, pHSD = 7.07 × 10−5, one-sided). In association regions, both subtypes showed reduced synergy (subtype 1 vs. HC, t = −5.72, pHSD = 2.31 × 10−8; subtype 2 vs. HC, t = −7.64, pHSD = 3.01 × 10−14, one-sided), while subtype 2 exhibited significantly increased redundancy compared to both HC (t = 4.84, pHSD = 1.98 × 10−6, one-sided) and subtype 1 (t = 8.32, pHSD = 2.31 × 10−15, one-sided). d The comparison of global network properties among subtype 1, subtype 2, and HC. At the global level, both subtypes showed increased synergy modularity (subtype 1 vs. HC, t = 5.64, pHSD = 5.78 × 10−9; subtype 2 vs. HC, t = 3.22, pHSD = 2.25 × 10−3, one-sided), while reduced synergy efficiency (subtype 1 vs. HC, t = −6.01, pHSD = 8.08 × 10−10; subtype 2 vs. HC, t = −5.43, pHSD = 1.11 × 10−7, one-sided) and subtype 1 was significantly lower than subtype 2 (t = −3.27, pHSD = 1.72 × 10−3, one-sided). Redundancy modularity was significantly increased in both subtypes (subtype 1 vs. HC, t = 9.14, pHSD = 4.76 × 10−17; subtype 2 vs. HC, t = 11.36, pHSD = 3.55 × 10−22, one-sided), whereas redundancy efficiency showed opposite changes (t = −10.92, pHSD = 3.68 × 10−21, one-sided), with subtype 1 exceeding subtype 2 (t = 3.45, pHSD = 6.62 × 10−4, one-sided). All box plots shown in c and d have the same sample size (NSubtype 1 = 140, NSubtype 2 = 162, NHC = 207), depicting the IQR and the median value of the distribution. Whiskers extend to the nearest points ± 1.5 × IQR above and below the 25th and 75th percentiles. Asterisks indicate a significant difference between box plots (*pHSD < 0.001). Group differences were compared using one-way ANOVA, with head motion, age, handedness, and sex as covariates. Then, post hoc analysis with HSD was implemented to clarify the multiple comparisons among various groups. Source data are provided as a Source Data file.
In the whole-brain hierarchical level, our results showed that redundancy-to-synergy gradient (Supplementary Fig. 6) was aligned with the sensory-to-association axis in subtype 1 (r = 0.44, pspin < 0.001), subtype 2 (r = 0.52, pspin < 0.001), and HC (r = 0.50, pspin < 0.001). This indicates that the information interactions between brain regions follow the principle of functional hierarchy across all groups, consistent with previous findings35. Compared with HC, both subtype 1 and subtype 2 exhibited greater synergy-redundancy interactions (red) primarily in temporal and frontal cortices (Fig. 3b, pFDR < 0.05). Additionally, subtype 1 showed reduced synergy-redundancy interactions (blue) in several sensory regions, including motor and auditory cortices (Fig. 3b, pFDR < 0.05). Direct comparisons between the two subtypes further revealed that subtype 1 demonstrated more pronounced synergy-redundancy interactions in left frontal and temporal cortices, while reduced synergy-redundancy interactions in right frontal and temporal cortices (pFDR < 0.05).
Furthermore, we compared the synergy and redundancy capabilities between sensory and association regions across adolescent MDD subtypes 1, subtype 2, and HC (Fig. 3c). Average synergy and redundancy matrix could be seen in Supplementary Fig. 7. Along the sensory axis, compared to HC, subtype 1 exhibited significantly reduced synergy (t = −7.06, pHSD < 0.001), and subtype 2 also showed a significant reduction (t = −8.18, pHSD < 0.001), with no significant difference observed between these two subtypes. In contrast, redundancy in the sensory regions was markedly elevated in both subtypes (subtype 1: t = 3.19, pHSD < 0.01; subtype 2: t = 3.98, pHSD < 0.001), with subtype 1 exhibiting higher redundancy levels than subtype 2 (t = 4.03, pHSD < 0.001). Along the association axis, subtype 1 showed significantly decreased synergy (t = −5.72, pHSD < 0.001), and subtype 2 also demonstrated significant decrease synergy values (t = −7.64, pHSD < 0.001). Redundancy in the association regions exhibited the opposite pattern with subtype 2 displayed significant increases redundancy values relative to HC (t = 4.84, pHSD < 0.001), and subtype 2 significantly exceeding subtype 1 (t = 8.32, pHSD < 0.001). Taken together, in the sensory regions, both subtypes exhibited reduced synergy but elevated redundancy relative to HC, with subtype 1 showing greater redundancy than subtype 2. In the association regions, both subtypes were characterized by decreased synergy, while subtype 2 showed the opposite pattern of increased redundancy, with significant differences compared to subtype 1. These findings suggest that subtype 1 tends to preserve redundancy processing in association regions while reducing synergy, whereas subtype 2 demonstrates diminished synergy coupled with elevated redundancy, reflecting distinct alterations in association-level information integration across adolescent MDD subtypes.
We further analyzed network modularity and global efficiency, where modularity measures the extent of functional segregation between brain regions, and global efficiency reflects the overall capacity for information integration. Figure 3d showed that at the global level, compared to HC, both subtypes exhibited significantly increased synergy modularity (subtype 1: t = 5.64, pHSD < 0.001; subtype 2: t = 3.22, pHSD < 0.01), with no significant difference between these two subtypes. Redundancy modularity was also significantly increased in both subtypes compared to HC (subtype 1: t = 9.14, pHSD < 0.001; subtype 2: t = 11.36, pHSD < 0.001). Network efficiency showed an opposite pattern: synergy efficiency was significantly reduced in both subtype groups compared to HC (subtype 1: t = −6.01, pHSD < 0.001; subtype 2: t = −5.43, pHSD < 0.001), and subtype 1 was significantly lower than subtype 2 (t = −3.27, pHSD < 0.01); in contrast, redundancy efficiency was significantly decreased in subtype 2 compared to HC (t = −10.92, pHSD < 0.001), with subtype 1 exceeding subtype 2 (t = 3.45, pHSD < 0.001). At the global network level, both subtypes demonstrated significantly increased synergy modularity compared to HC, but the differences between the two subtypes were minimal. Conversely, both subtypes demonstrated significantly reduced synergy efficiency. Redundancy modularity and redundancy efficiency showed opposite changes in subtype 2, with subtype 1 showing higher levels than subtype 2 for redundancy efficiency. Overall, these results indicate a general trend of increased synergistic modularity but reduced synergistic efficiency in adolescent MDD patients. Both subtypes exhibited enhanced redundancy modularity, while subtype 2 showed particularly pronounced increases in redundancy modularity and significantly decreases in redundancy efficiency compared with subtype 1. This pattern suggests that subtype 2 may rely more heavily on enhanced redundancy modularity, despite reduced efficiency, to sustain information transfer and network functionality.
In summary, both subtypes of adolescent MDD exhibited reduced synergy and increased redundancy in sensory regions, with subtype 1 showing higher redundancy than subtype 2. In association regions, both subtypes displayed decreased synergy, while subtype 2 demonstrated significantly increased redundancy compared with both HC and subtype 1. At the global level, both subtypes were characterized by increased synergy modularity but reduced synergy efficiency. Redundancy modularity was enhanced in both subtypes, whereas redundancy efficiency showed opposite changes, with subtype 1 exceeding subtype 2.
Various age effects on the functional gradient of subtype 1 and subtype 2
Adolescence demonstrates a developmental shift in functional organization13, initially characterized by a predominant segregation between sensory and motor systems, which subsequently evolves into a more integrated architecture through interactions with later-maturing regions of the association cortex that underpin higher-order cognitive processes39. Therefore, we further explored how functional gradients in two subtypes altered across ages to further clarify age effects on MDD subtypes. We found age effects (see Supplementary Table 2 for age distribution) in subtype 1, subtype 2, and HC aligned with functional hierarchy (Fig. 4). Specifically, age effects in subtype 1 followed motor/auditory-visual axis (r = 0.44, pspin < 0.001), while age effects in subtype 2 followed sensory-association axis (r = 0.58, pspin < 0.001), and age effects in HC aligned sensory-association axis (r = 0.40, pspin < 0.05) (Supplementary Fig. 8). We further examined the relationship between functional gradients and age effects in brain regions showing significant age-related effects (Supplementary Fig. 9, pFDR < 0.05). These results indicated that subtype 1 (r = 0.27, pspin < 0.05, one-sided) and subtype 2 (r = 0.37, pspin < 0.05, one-sided) remained significantly associated with the functional gradient. This indicates that different MDD subtypes exhibit specificity in age-related changes in functional gradients, showing significant deviations from the normal developmental trajectory15.

Specifically, age effects in subtype 1 follow the motor/auditory-visual axis (r = 0.44, pspin < 0.001) and in subtype 2 follow the sensory-association axis (r = 0.58, pspin < 0.001). Each point on the scatter plot (N = 400) indicates one parcel in the Schaefer 400 parcellation. Statistical significance was accessed using spin permutation of each group’s age effect map (Schaefer 400 parcellation, 1000 repetitions), respectively. Source data are provided as a Source Data file.
Clinical profiles in two adolescent MDD subtypes
Next, we probed the clinical symptoms in two subtypes (Fig. 5), including HAMD, Hamilton Anxiety Scale (HAMA), and Childhood Trauma Questionnaire (Supplementary Table 3, CTQ). Those questionnaires effectively capture the severity of depressive symptoms, anxiety levels, and early-life stressors, respectively. These measures comprehensively reflect key clinical aspects of adolescent MDD, such as mood dysregulation, emotional distress, and vulnerability due to childhood trauma. Previous studies have demonstrated that threat-related CTQ dimensions predominantly affect primary sensory cortices (e.g., visual and auditory systems)40, whereas neglect dimensions and the CTQ total score are closely associated with functional abnormalities in higher-order association networks (e.g., default mode network, frontoparietal network). Our results showed that both HAMD (NSubtype 1 = 140, NSubtype 2 = 162, t = 3.74, p < 0.001) and HAMA (NSubtype 1 = 103, NSubtype 2 = 114, t = 2.07, p = 0.04) of subtype 1 were significantly higher than subtype 2 (Fig. 5a). CTQ-T was significantly different in subtype 1 and subtype 2 (NSubtype 1 = 24, NSubtype 2 = 28, t = 3.03, pFDR < 0.05). More specifically, items including CTQ-EI (t = 2.67, pFDR < 0.05) and CTQ-PI (t = 3.16, pFDR < 0.05) (Fig. 5b) in subtype 1 were significantly higher than in subtype 2. In summary, subtype 1 exhibited significantly higher depressive and anxiety symptom severity, alongside elevated levels of childhood trauma—particularly emotional and physical neglect—compared to subtype 2. These findings underscore distinct clinical profiles between the two adolescent MDD subtypes.

a Clinical symptoms were significantly different in subtype 1 and subtype 2. Specifically, HAMD (number of subjects with NSubtype 1 = 140 and NSubtype 2 = 162) in subtype 1 was significantly higher than subtype 2 (t = 3.74, p = 2.20 × 10−4, one-sided). HAMA (number of subjects with NSubtype 1 = 103 and NSubtype 2 = 114) in subtype 1 was significantly higher than subtype 2 (t = 2.07, p = 0.04, one-sided). b CTQ was significantly different in subtype 1 (N = 24) and subtype 2 (N = 28). Specifically, CTQ-EI (t = 2.67, pFDR = 0.013, one-sided), CTQ-PI (t = 3.16, pFDR = 0.006, one-sided) and CTQ-T (t = 3.03, pFDR = 0.0067, one-sided) in subtype 1 were significantly higher than in subtype 2. Note that CTQ-EA means Emotional Abuse, CTQ-EI means Emotional Neglect, CTQ-PA means Physical Abuse, CTQ-PI means Physical Neglect, CTQ-SA means Sexual Abuse, CTQ-T means Total Score, HAMD means Hamilton Depression Rating Scale and HAMA means Hamilton Anxiety Scale. All box plots shown in a and b depict the IQR and the median value of the distribution. Whiskers extend to the nearest points ± 1.5 × IQR above and below the 25th and 75th percentiles. Asterisks indicate a significant difference between box plots (*p < 0.05). Group differences were compared using two-sample t-test, respectively, regressing out the influence of head motion, age, sex, and handedness. Then, FDR (q < 5%) was used to consider the multiple comparisons correction. Source data are provided as a Source Data file.
Molecular mechanisms and genetic mechanisms of functional reorganization
Finally, we performed spatial correlation analyses to investigate the alignment between molecular/cellular maps and functional reorganization maps for the subtypes (Fig. 6a). These normative molecular and cellular maps, derived from the Neuromaps platform41,42, representing the spatial distribution of 19 neurotransmitter receptors and transporters. Spatial correlations enable us to identify which neurotransmitter systems are aligned with the sensory-to-association reorganization axis across different episodes. Specifically, negative associations indicated that higher cell or neurotransmitter density was more related to sensory reorganization, while positive correlations were associated with the reorganization of association regions. We found that the functional reorganization of subtype 1 and subtype 2 was both significantly related to excitatory receptors such as mGluR5, and inhibitory receptors (e.g., 5HT1b, CB1, D2, MOR) (Fig. 6a). These findings suggest that distinct receptors contribute differentially to the functional reorganization processes in sensory versus association regions, potentially reflecting regional-specific adaptations.

a Spatial correlations between functional reorganization patterns and normalized neurotransmitter receptor and transporter maps revealed distinct associations in subtype 1 and subtype 2. Subtype 1 and subtype 2 both showed strong correlations with excitatory receptors such as mGluR5, and inhibitory receptors (e.g., 5HT1b, CB1, D2, MOR). b Gene enrichment analyses highlighted distinct molecular processes for each subtype. Subtype 1 was enriched in processes related to regulation of synapse organization, neuron projection development, regulation of plasma membrane-bounded cell projection organization, positive regulation of cell adhesion, and metabolism of lipids. Subtype 2 was enriched in processes associated with intracellular protein transport, RNA splicing, regulation of cellular response to stress, cancer pathways, and positive regulation of cellular component biogenesis. Source data are provided as a Source Data file.
Furthermore, we implemented enrichment analyses for subtype 1 and subtype 2 (Fig. 6b). Gene enrichment analysis highlighted distinct molecular processes for each subtype. Subtype 1 was enriched in processes related to regulation of synapse organization, neuron projection development, regulation of plasma membrane-bounded cell projection organization, positive regulation of cell adhesion, and metabolism of lipids. Subtype 2 was enriched in processes associated with intracellular protein transport, RNA splicing, regulation of cellular response to stress, cancer pathways, and positive regulation of cellular component biogenesis. Together, these results suggest that subtype 1 may be linked to mechanisms of neuronal growth and structural plasticity, whereas subtype 2 may be associated with processes supporting synaptic efficiency and cellular stress responses. The p-values could be seen in Supplementary Fig. 10.
Together, these findings reveal that the functional reorganization patterns observed across adolescent MDD subtypes were closely aligned with the cortical distribution of chemical neuromodulator systems, providing insights into potential molecular biomarkers that could guide future therapeutic strategies.
Replication of key findings
Finally, we replicated the depression subtypes via an independent Characterization and Treatment of Adolescent Depression (CAT-D) open dataset (Supplementary Tables 1 and 4). This validation dataset consists of 73 adolescents with MDD (16.80 ± 1.22 years old, 31 females) and 28 HC (16.82 ± 1.40 years old, 12 females). All participants underwent an identical preprocessing pipeline, including fMRI quality control, parcellation into the Schaefer 400 parcellation, functional connectivity computation, and gradient extraction. These standardized procedures enabled group- and subtype-level comparisons as well as clustering analyses, ensuring the robustness of functional reorganization patterns. Our results revealed that optimization of the subtype number was also two (Supplementary Fig. 11a). The functional gradient of subtype 1 (N = 33, 16.84 ± 1.51 years old, 13 females) was associated with motor areas contraction, and subtype 2 (N = 40, 16.75 ± 0.75, years old, 18 females) was related to association areas expansion, which were consistent with the two subtypes in exploration dataset (subtype 1: r = 0.35, subtype 2: r = 0.51, HC: r = 0.53; all pspin < 0.001, Supplementary Fig. 11b, c). Subtype 1 had a higher Kiddie Schedule for Affective Disorders and Schizophrenia (KSADS) Z-scores (t = 3.41, p < 0.05, Supplementary Fig. 12a), higher Z-scores for exercise (t = 2.28, p < 0.05, Supplementary Fig. 12b) and higher concentration difficulty Z-scores (t = 2.37, p < 0.05, Supplementary Fig. 12c) than subtype 2. Taken together, these findings suggest that, in the CAT-D dataset, subtype 1 is more closely related to alterations in primary sensory processes, whereas subtype 2 is predominantly associated with impairments in higher-order cognitive functions.
Discussion
Our study identified two distinct subtypes of adolescent MDD: subtype 1, characterized by sensory region reorganization, exhibiting a bottom-up information flow pattern, heightened network segregation, and reduced integrative capacity; subtype 2, characterized by association region reorganization, displaying a top-down information flow pattern and better integration. Both subtypes demonstrated age-related alterations in functional gradients, significantly deviating from normal developmental trajectories. In information processing, subtype 1 showed lower synergy and higher redundancy in sensory regions relative to HC, whereas subtype 2 exhibited lower synergy in association regions and reduced redundancy in sensory regions relative to subtype 1. Clinically, subtype 1 presented with more severe symptoms, especially higher depressive and anxiety symptom severity. In molecular-levels, subtype 1 linked to molecular mechanisms involved in neuronal growth and structural plasticity, while subtype 2 was closely associated with processes that regulate synaptic efficiency and cellular stress responses. In summary, our study proposes a binary hierarchical model systematically characterizing the neurophenotypes of adolescent MDD subtypes, offering critical insights into the unique neurobiological mechanisms driving each subtype. This model captures the complex interplay between sensory and association brain regions, integrates developmental and genetic factors, and underscores its significance for precision psychiatry.
First of all, our results identify subtype 1 as primarily involving sensory-region reorganization with bottom-up information flow, and subtype 2 as driven by association-region reorganization with relatively enhanced top-down information flow. These findings converge with previous proposed theory, which highlights a continuous gradient of brain functions along the S-A axis and underscores its close links to general perception and cognition12. Crucially, the observed subtypes resonate with the well-documented individual variability in functional gradients during adolescence14,15,19, suggesting that divergent neurodevelopmental trajectories may underlie their distinct S-A axis profiles. Furthermore, previous studies emphasize that sensory regions play a pivotal role in information segregation and robustness, whereas association regions facilitate integrative and flexible processes35,36,43. Our results robustly validate this framework, demonstrating that subtype 1 reflects a sensory-driven, bottom-up processing bias, while subtype 2 exhibits association-mediated top-down dominance. By leveraging multisite multimodal data and advanced machine learning, we provide empirical evidence for the heterogeneous neurobiological substrates of adolescent MDD.
The present findings further illuminate distinct developmental patterns in the two subtypes. Both subtypes show age-related shifts in functional gradients. Specifically, subtype 1 follows a gradient from motor/auditory-to-visual axis, while subtype 2 aligns more closely with the sensory-to-association axis, diverging from the typical adolescent progression toward higher-order association networks. Prior research has underlined that adolescence is a critical window for the protracted maturation of association regions19, crucial to advanced cognitive and socioemotional integration15. Our results suggest that subtype 1 excessive reliance on sensory cortex development might heighten sensitivity to external stimuli, whereas subtype 2 shows a partial “compensatory” enhancement in association regions that nonetheless remains suboptimal. Such discrepancies in the developmental timetable and region-specific maturation processes provide novel insights into the pathophysiology and clinical course of adolescent MDD44,45.
Our synergy–redundancy analysis indicates that subtype 1 has reduced synergy within sensory regions but higher redundancy in sensory regions relative to HC, whereas subtype 2 exhibits lower synergy in higher-order association regions while showing reduced redundancy in sensory areas. These data align with the conceptual framework, wherein synergy reflects emergent information gained through cross-regional integration, whereas redundancy provides robustness and error tolerance35,36,43. Subtype 1 presents reduced synergy in sensory regions that may lead to insensitivity to external stimuli, diminishing affective and stress responses46,47,48. Conversely, subtype 2 exhibits reduced synergy in higher-order cognitive circuits, suggesting a diminished basic regulation of emotional and cognitive functions, leading to deficits in higher-order cognitive information processing49,50. Such synergy–redundancy differentials support our gradient-based findings and lay a theoretical foundation for precision-targeted interventions.
Clinically, we observed pronounced differences in symptomatology between the two subtypes. Subtype 1 presents more severe depressive and anxious symptom profiles, including higher HAMD and HAMA scores, as well as a history of CTQ, particularly in emotional and physical neglect. CTQ provides a natural bridge between sensory systems and association cortices, offering a behavioral and developmental framework to interpret our findings on the differentiation between sensory processing and higher-order cognitive networks. These findings align with Kaczkurkin et al.51,52,53 on the susceptibility conferred by early pubertal transitions and heightened psychosocial stress, as well as54, who underscore the enduring impact of adverse early-life events. In subtype 1, the global disruption in the environment may foster greater network segregation and diminished integrative capacity55. Subtype 2, despite showing reductions in synaptic efficiency and neuronal excitability, tends to manifest relatively milder clinical symptoms, potentially reflecting partial compensation in association regions for inadequate functional integration56,57,58,59. These clinical distinctions underscore the tight link between functional reorganization profiles and disease severity, suggesting that future therapeutic strategies should be tailored to subtype-specific clinical features.
At the molecular and genetic levels, subtype 1 is likely underpinned by molecular mechanisms involved in neuronal growth and structural plasticity, whereas subtype 2 appears to be characterized by processes that regulate synaptic efficiency and cellular stress responses. These findings converge with prior evidence60 and further reveal that the roles of neuromodulatory systems in brain functional organization and they align with15, which postulates that divergences in gene expression profiles during cortical maturation may underlie susceptibility to psychiatric conditions61. The differential molecular mechanisms imply that subtype 1 may exhibit more pervasive deviations in cellular and synaptic architecture62, whereas subtype 2 shows greater deficits in neuronal processing and signal transmission63,64,65. Overall, by integrating functional neuroimaging, developmental, and molecular approaches, this work clarifies the heterogeneous neural mechanisms underlying adolescent MDD and highlights novel directions for precision medicine and personalized interventions, such as the identification of molecular biomarkers to guide pharmacological or other therapeutic strategies.
Several limitations warrant consideration in the current study. First, we did not account for the potential influences of brain structure in our analysis. Second, we did not examine the impact of medication on brain structure and function in individuals with MDD, which is a common challenge in psychiatric research. Also, the receptor, cellular, and gene expression maps used in this study were derived from group-averaged data in previous studies, without accounting for individual variability. Future research should aim to validate these findings by incorporating individual-level differences. Moreover, given that pharmacological treatment may exert heterogeneous effects across different subtypes of adolescent MDD, future studies should carefully account for medication status when investigating brain structure and function. Such considerations will be essential to disentangle medication-related influences from subtype-specific neural alterations.
Methods
Exploratory dataset 1
Participants in the MDD group (N = 302, 15.40 ± 2.09 years old, 134 females) were experiencing their first depressive episode, with no history of manic or hypomanic episodes, and had not received antidepressant treatment prior to the study. Participants who had a Hamilton Depression Rating Scale (HAMD-24) score greater than 17 (25.11 ± 5.63), were Han Chinese, right-handed, and aged 11–17 years. They had not taken any psychotropic, sedative, or analgesic medications in the month preceding the study. Exclusion criteria included a history of neurological disorders (e.g., epilepsy, multiple sclerosis) or significant physical illnesses (e.g., heart disease, cancer), the presence of other psychiatric disorders or borderline personality disorder, intracranial mass, family history of mental illness or self-harm, severe head trauma resulting in loss of consciousness, substance or alcohol abuse, contraindications to MRI (e.g., pacemakers, metal implants), and an inability to cooperate during MRI scanning. HC were age- and sex-matched volunteers (N = 207, 15.33 ± 1.77 years old, 86 females) recruited from the community. Inclusion criteria for the HC included Han nationality, right-handedness, and an age range of 11–17 years. Exclusion criteria for HC mirrored those of the MDD group. More details of data collection and quality control can be seen in the Supplementary Materials and Supplementary Tables 1–4.
This study received approval from the Ethics Committee of Renmin Hospital, Wuhan University, Wuhan, China, and adhered to the principles of the Declaration of Helsinki (2002). Written informed consent was obtained from all participants and their legal guardians after a thorough explanation of the study’s objectives and procedures.
Replication dataset 2
We also replicated results of Exploratory Dataset 1 using the Characterization and Treatment of Adolescent Depression (CAT-D) from OpenNeuro (ds004627)66. The details could be seen in the Supplementary Materials as well as66. After quality control, we included 73 adolescents with MDD (16.80 ± 1.22 years old, 31 females) and 28 HC (16.82 ± 1.40 years old, 12 females) (see Supplementary Materials and Supplementary Table 1).
Data preprocessing, quality control, and functional connectome
Raw DICOM files from all datasets were converted to Brain Imaging Data Structure (BIDS)67 format using HeuDiConv v0.13.1. Structural and functional preprocessing for the MDD dataset were conducted with fMRIPrep 23.0.268 and Numpy69 as its underlying framework. Key anatomical preprocessing steps included intensity normalization, brain extraction, tissue segmentation, surface reconstruction, and spatial normalization. Functional data preprocessing involved head motion correction, slice-time correction, and co-registration. The functional time series were then parcellated according to the Schaefer 400×7 parcellation and subjected to a confound removal process via Nilearn, following the “simple” strategy outlined by ref. 70. This involved high-pass filtering, removal of motion and tissue signals, detrending, and z-scoring. Subsequently, functional connectivity matrices were calculated for each participant using zero-lag Pearson correlation coefficients. The details of data quality control can be seen in the Supplementary Data quality control.
Functional hierarchy definition
We employed BrainSpace (version 0.1.10; https://github.com/MICA-MNI/BrainSpace) to derive cortex-wide functional connectome gradients, adhering to default parameters. Consistent with prior study12, the top 10% of weighted connections per region were retained post-z-transformation of the data. An affinity matrix was constructed using a normalized angle kernel to capture connectivity profile similarities between regions. Diffusion map embedding approach38, a robust non-linear manifold learning technique, was utilized to extract functional gradients from the high-dimensional functional connectome for each participant. Individual gradient maps were then aligned to template gradients derived from the group average connectome.
Subtypes definition
To define subtypes of adolescent MDD, we conduct a data-driven approach on function gradients via a machine learning model. Specifically, we applied k-means clustering to analyze the first functional gradient in adolescents with MDD. The optimal number of clusters was identified based on the clustering stability71. We perturbed the data by sampling 80% of the whole dataset and generated two subsample datasets72. We then clustered these two subsample datasets respectively and calculated the stability. Noted that stability was measured by the similarity of two cluster indices based on overlap of samples in these two subsample datasets. Stability was rigorously assessed by averaging stability over performing 1000 iterations on the MDD sample, ensuring the robustness of the identified subtypes. Finally, we repeated the whole process and revised the cluster number to ensure the stability of each cluster number. The cluster number was defined by the value with the largest stability.
To validate the specificity of these network patterns, we employed both similarity matrices across participants and other supervised machine learning techniques to assess their ability to differentiate between depressive subtypes. Specifically, we utilized a Support Vector Machine (SVM) with a radial basis kernel to classify subtype 1, subtype 2, and HC. The data were divided into training and testing sets using leave-one-out cross-validation. Model performance was evaluated using accuracy and the area under the receiver operating characteristic (ROC) curve (AUC), with the entire process repeated 1000 times to ensure robustness.
To estimate functional reorganization across various MDD subtypes, we implemented one-way analysis of variance (ANOVA) to compare the functional organization pattern between MDD subtypes and HC, respectively, with head motion, age, handedness, and sex as covariates. Then False Discovery Rate (FDR, q < 5%) was used to consider the multiple comparisons correction. Furthermore, post hoc analysis with Tukey’s Honest Significant Difference (HSD) was implemented to clarify the multiple comparisons among various MDD subtypes.
Dispersion of functional reorganization
In this section, we used the Schaefer 400 parcellation as well as its associated Yeo’s seven functional network solution, including the visual network (VN), somatomotor network (SMN), dorsal attention network (DAN), ventral attention network (VAN), limbic (LIB), frontoparietal network (FPN), and default-mode network (DMN). We calculated global dispersion as the Euclidean distance between individual regions and the manifold centroid. This metric, which corresponds to eccentricity, provides a quantitative measure of whole-brain integration and segregation. Regions exhibiting higher global dispersion values demonstrated greater segregation, whereas regions with lower values showed enhanced integration with proximal areas. To assess within-network organization, we defined a dispersion metric to assess the degree of gradient dispersion within each functional network. Using the VN, SMN, DAN, VAN, LIB, FPN, and DMN as boundaries, we averaged the gradient values within each network to establish a central reference. The dispersion was then calculated by measuring the distance between the gradient of each node and the central reference. Finally, we compared the gradient dispersion values across different MDD subtypes and HC within each resting-state network using the two-sample t-test.
Cognition decoding for functional reorganization
We then further estimated the cognition relevance of functional reorganization patterns among various adolescent subtypes using Neurosynth73. We used twenty cognition maps from previous studies12, which represented sensory functions and high-order cognition. Then we correlated them with functional gradient difference maps between adolescent MDD subtypes and HC via Pearson correlation.
Top-down and bottom-up information flow in various subtypes
We further explore information flow along the sensory-association axis. Top-down was first defined as information flow from association to sensory regions, and bottom-up as information flow from sensory regions to association regions19. Information flow was measured by regression dynamic causal model (rDCM)22,23 and graph theory measurement. Then we calculated the ratio between the average outward in sensory regions and association regions, respectively. This ratio value represents top-down flow when it is less than one, while bottom-up flow when it is larger than one. Finally, the flow ratio in both MDD subtypes and HC was compared using one-way ANOVA, with head motion, age, handedness, and sex as covariates. Then, post-hoc analysis with HSD was implemented to clarify the multiple comparisons among various groups.
Synergy and redundancy: integrated information decomposition
The Integrated Information Decomposition (IID) framework35 integrates key concepts from Integrated Information Theory (IIT) and Partial Information Decomposition (PID) to parse information flow in neural systems74. Specifically, IID builds on Shannon’s Mutual Information (MI) by quantifying the dependency between two variables and decomposing the information that two sources provide about a target into unique, redundant, and synergistic components. Synergistic information represents insights derived only when both sources interact, while redundant information reflects insights that are independently contributed by each source35. This decomposition framework sheds light on how brain regions collectively contribute to future states, highlighting the roles of synergy and redundancy in integrating and coordinating neural processes. To address the limitations of the original IIT measure of integrated information (Φ), which could yield negative values in redundancy-dominated systems, Mediano and colleagues introduced a revised measure (Φ_R) that incorporates redundancy75. This revised measure ensures non-negativity and provides a more robust metric for assessing the extent to which “the whole is greater than the sum of its parts,” specifically by focusing on synergistics76. In total, this approach is particularly relevant for understanding brain network dynamics in a more nuanced way, where brain regions are identified as either “gateways”, contributing to integration via synergistic interactions, or “broadcasters”, contributing to the distribution of redundant information.
Therefore, using the IID framework on time series data parcellated with the Schaefer 400 × 7 parcellation, we generated for each participant a 400 × 400 synergy matrix and a 400 × 400 redundancy matrix, respectively, indicating the synergistic and redundant relationships among different brain regions.
Gradient of redundancy-to-synergy relative importance
In our analysis, we constructed synergy and redundancy networks across regions of interest ROIs in the brain and evaluated the relative contribution of each ROI to these interactions. First, we computed the nodal strength for each brain region, which reflects the total sum of its connections in the group-averaged matrix. We then ranked all 400 regions by their nodal strength, assigning higher ranks to regions with stronger connections in both synergy and redundancy networks35. By subtracting each region’s redundancy rank from its synergy rank, we derived a gradient score that ranges from negative to positive values. A negative score indicates a stronger association with redundancy (i.e., a higher redundancy ranking than synergy), while a positive score suggests greater involvement in synergistic processes. This gradient reflects relative differences in the balance of synergy and redundancy within the brain, helping to reveal how individual brain regions participate in either integration or redundancy, depending on the broader network dynamics.
Graph-theoretic profiles for synergy and redundancy properties
Modularity and efficiency are critical metrics for understanding the functional roles of synergy and redundancy networks in the brain. Modularity quantifies the degree to which nodes cluster into functional modules, reflecting the organization of network architecture. In synergy networks, high modularity indicates robust inter-regional integration, facilitating global information processing, whereas in redundancy networks, high modularity emphasizes distributed independent contributions, supporting localized functional stability. The reduced modularity may signify disrupted functional segregation, leading to impairments in cognitive and emotional regulation. Efficiency, on the other hand, assesses the brain’s information exchange capacity, with local efficiency capturing short-range information transfer and supporting specific regional functions, while global efficiency measures the capacity for long-range integration across the brain. In MDD, decreased global efficiency suggests impaired integration, whereas increased local efficiency may indicate compensatory mechanisms. Together, modularity and efficiency provide insights into network dysfunction in MDD subtypes, elucidating the balance between integration and segregation, and highlighting distinct neural mechanisms35. Therefore, in this study, we further calculated modularity and efficiency of synergy and redundancy matrices for each individual. Finally, we compared those network properties in both MDD subtypes and HC using one-way ANOVA, with head motion, age, handedness, and sex as covariates. Then, post hoc analysis with HSD was implemented to clarify the multiple comparisons among various groups.
Age association in various subtypes of adolescent MDD
To further elucidate the age-related effects on functional reorganization patterns across different subtypes of adolescent MDD, we calculated the Pearson correlation between age and the functional gradient in each parcellated brain region for each subtype and the HC group. These age-effect maps were subsequently generated, reflecting how age influences the functional gradient within different brain regions across subtypes. Additionally, we computed the age effects for standard sensory-association and auditory/motor-visual axes, which were defined by the functional connectome from 100 healthy adults in the Human Connectome Project77. We also validated the correlation between MDD subtypes’ age effect maps and functional gradient axes calculated with HC (Supplementary Fig. 13). These maps provided a comparative framework for examining how adolescent MDD subtypes deviate from normal developmental trajectories, shedding light on the neurodevelopmental dynamics underlying the disorder and its relation to age-specific brain reorganization.
Clinical symptom association in various subtypes of MDD
To further validate the clinical association of various subtypes, we compared HAMD, Hamilton Anxiety Rating Scale (HAMA), and Childhood Trauma Questionnaire (CTQ) between MDD subtype 1 and subtype 2 via two-sample t-test, respectively, regressing out the influence of head motion, age, sex, and handedness.
Enrichment analysis of functional reorganization in subtypes
Cell type fractions were deconvolved from microarray samples downloaded from the Allen Human Brain Atlas (AHBA; http://human.brain-map.org/)78. To study how the functional reorganization is regulated by genes, we combined AHBA and the precise brain connectivity pattern for analysis. Regional microarray expression data were obtained from six post-mortem brains (age = 42.50 ± 13.38 years; male/female = 5/1) with 3702 spatially distinct samples. We used the Abagen toolbox41 (https://github.com/netneurolab/abagen) to process and map the data to 400 parcellated brain regions from the Schaefer 400 parcellation. We further correlated the two subtypes’ functional reorganization maps with the gene expression cortical patterns.
Then we tested whether transcriptionally dysregulated genes in postmortem brain tissue of messenger RNA are expressed most in cortical regions that are associated with gradient abnormalities across different subtypes. Metascape analysis (https://metascape.org/gp/index.html#/main/step1) automated meta-analysis tool to identify and interpret common or unique pathways across 40 independent knowledge bases79. The most significantly functional reorganization patterns related genes were input into the Metascape website, and the obtained enrichment pathways were thresholded for significance at 5%, corrected by the FDR, and null model test.
Receptor mechanism of functional reorganization of various subtypes
Receptor densities were assessed through the utilization of PET tracer investigations encompassing a total of 19 receptors and transporters spanning nine neurotransmitter systems. This data, recently shared by Hansen and colleagues (https://github.com/netneurolab/hansen_receptors)60. The neurotransmitter systems include dopamine (D1, D2, DAT), norepinephrine (NET), serotonin (5-HT1a, 5-HT1b, 5-HT2a, 5-HT4, 5-HT6, 5-HTT), acetylcholine (α4β2, M1, VAChT), glutamate (mGluR5, NMDA), GABA (GABAa/bz), histamine (H3), cannabinoid (CB1), and opioid (MOR)41. Volumetric PET images were aligned with the MNI 152 nonlinear 2009 (version c, asymmetric) template. These images, averaged across participants within each study, were subsequently parcellated into the Schaefer 400 parcellation. Receptors/transporters exhibiting more than one mean image of the same tracer (5-HT1b, D2, VAChT) were amalgamated using a weighted average60.
Null model
In this study, we sought to delineate the topographic correlations between common-specific network patterns and other salient neural features. To derive robust inferences, we implemented a null model designed to systematically disrupt the relationship between two topographic maps while maintaining their inherent spatial autocorrelation60. Initially, we shuffled receptor maps and assessed their relationships with common-specific network patterns. These spatial coordinates formed the foundation for generating null models, achieved by performing randomly sampled rotations and reassigning node values to the nearest resulting parcel. This procedure was repeated 1000 times to ensure robustness. Critically, the rotational transformation was first applied to one hemisphere and subsequently mirrored onto the contralateral hemisphere. The 95th percentile of occurrence frequencies from both spatial and temporal null models was designated as the threshold for statistical significance. This rigorous thresholding approach allowed us to identify meaningful topographic correlations while controlling for the intrinsic spatial autocorrelation present in the data.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The clinical data used in this study involves patient privacy concerns. Therefore, access to the data can be granted upon reasonable request to the corresponding authors. Allen Human Brain Atlas (AHBA; http://human.brain-map.org/), Neuromap (https://netneurolab.github.io/neuromaps/usage.html) could be downloaded online. Characterization and Treatment of Adolescent Depression (CAT-D) from OpenNeuro (https://openneuro.org/datasets/). Source data are provided with this paper.
Code availability
All codes used in this study were available (https://github.com/Laoma29/adolescence-MDD-subtyping-projects). Brainspace (https://brainspace.readthedocs.io/en/latest/) and ENIGMA toolbox (https://enigma-toolbox.readthedocs.io/en/latest/) could be downloaded online.
References
Cash, R. F. H. et al. Using brain imaging to improve spatial targeting of transcranial magnetic stimulation for depression. Biol. Psychiatry 90, 689–700 (2021).
Fox, M. D., Liu, H. & Pascual-Leone, A. Identification of reproducible individualized targets for treatment of depression with TMS based on intrinsic connectivity. NeuroImage 66, 151–160 (2013).
Sun, X. et al. Disrupted intersubject variability architecture in functional connectomes in schizophrenia. Schizophr. Bull. 47, 837–848 (2021).
Eiland, L. & Romeo, R. D. Stress and the developing adolescent brain. Neuroscience 249, 162–171 (2013).
Liu, X. et al. Episode-specific and common intrinsic functional network patterns in bipolar. Preprint at https://doi.org/10.1101/2024.07.26.24310655 (2024).
Liu, X. et al. Episode-specific cortical functional connectome reorganization and neurobiological correlates in bipolar disorder: a cross-sectional study. BMC Med. 23, 457 (2025).
Yang, Y. et al. Frequency-specific alteration of functional connectivity density in bipolar disorder depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 104, 110026 (2021).
Lynch, C. J. et al. Frontostriatal salience network expansion in individuals in depression. Nature 1–10 https://doi.org/10.1038/s41586-024-07805-2 (2024).
Buch, A. M. & Liston, C. Dissecting diagnostic heterogeneity in depression by integrating neuroimaging and genetics. Neuropsychopharmacology 46, 156–175 (2021).
Demeter, D. V. & Greene, D. J. The promise of precision functional mapping for neuroimaging in psychiatry. Neuropsychopharmacology 50, 16–28 (2024).
Ecker, C. & Murphy, D. Neuroimaging in autism—from basic science to translational research. Nat. Rev. Neurol. 10, 82–91 (2014).
Margulies, D. S. et al. Situating the default-mode network along a principal gradient of macroscale cortical organization. Proc. Natl. Acad. Sci. USA 113, 12574–12579 (2016).
Dong, H.-M., Margulies, D. S., Zuo, X.-N. & Holmes, A. J. Shifting gradients of macroscale cortical organization mark the transition from childhood to adolescence. Proc. Natl. Acad. Sci. USA 118, e2024448118 (2021).
Keller, A. S. et al. Personalized functional brain network topography is associated with individual differences in youth cognition. Nat. Commun. 14, 8411 (2023).
Luo, A. C. et al. Functional connectivity development along the sensorimotor-association axis enhances the cortical hierarchy. Nat. Commun. 15, 3511 (2024).
Yurgelun-Todd, D. Emotional and cognitive changes during adolescence. Curr. Opin. Neurobiol. 17, 251–257 (2007).
Xia, M. et al. Connectome gradient dysfunction in major depression and its association with gene expression profiles and treatment outcomes. Mol. Psychiatry 27, 1384–1393 (2022).
Sun, X. et al. Mapping neurophysiological subtypes of major depressive disorder using normative models of the functional connectome. Biol. Psychiatry 94, 936–947 (2023).
Pines, A. et al. Development of top-down cortical propagations in youth. Neuron 111, 1316–1330.e5 (2023).
Janssen, L. H. C., Elzinga, B. M., Verkuil, B., Hillegers, M. H. J. & Keijsers, L. The link between parental support and adolescent negative mood in daily life: between-person heterogeneity in within-person processes. J. Youth Adolesc. 50, 271–285 (2021).
Zhang, S., Baams, L., van de Bongardt, D. & Dubas, J. S. Intra- and inter-individual differences in adolescent depressive mood: the role of relationships with parents and friends. J. Abnorm. Child Psychol. 46, 811–824 (2018).
Frässle, S. et al. Regression DCM for fMRI. NeuroImage 155, 406–421 (2017).
Frässle, S. et al. Regression dynamic causal modeling for resting-state fMRI. Hum. Brain Mapp. 42, 2159–2180 (2021).
Paquola, C. et al. The architecture of the human default mode network explored through cytoarchitecture, wiring and signal flow. Nat. Neurosci. 28, 654–664 (2025).
Park, S. et al. A shifting role of thalamocortical connectivity in the emergence of cortical functional organization. Nat. Neurosci. 27, 1609–1619 (2024).
Bernaras, E., Jaureguizar, J. & Garaigordobil, M. Child and adolescent depression: a review of theories, evaluation instruments, prevention programs, and treatments. Front. Psychol. 10, 543 (2019).
Herd, T. & Kim-Spoon, J. A systematic review of associations between adverse peer experiences and emotion regulation in adolescence. Clin. Child Fam. Psychol. Rev. 24, 141–163 (2021).
Ng, M. Y. & Weisz, J. R. Annual Research Review: Building a science of personalized intervention for youth mental health. J. Child Psychol. Psychiatry 57, 216–236 (2016).
Nigg, J. T. Annual Research Review: On the relations among self-regulation, self-control, executive functioning, effortful control, cognitive control, impulsivity, risk-taking, and inhibition for developmental psychopathology. J. Child Psychol. Psychiatry 58, 361–383 (2017).
Schäfer, J. Ö, Naumann, E., Holmes, E. A., Tuschen-Caffier, B. & Samson, A. C. Emotion regulation strategies in depressive and anxiety symptoms in youth: a meta-analytic review. J. Youth Adolesc. 46, 261–276 (2017).
Dalgleish, T., Black, M., Johnston, D. & Bevan, A. Transdiagnostic approaches to mental health problems: current status and future directions. J. Consult. Clin. Psychol. 88, 179–195 (2020).
Fusar-Poli, P. et al. Transdiagnostic psychiatry: a systematic review. World Psychiatry 18, 192–207 (2019).
Jorstad, N. L. et al. Transcriptomic cytoarchitecture reveals principles of human neocortex organization. Science 382, eadf6812 (2023).
McQuaid, R. J. Transdiagnostic biomarker approaches to mental health disorders: consideration of symptom complexity, comorbidity and context. Brain Behav. Immun. Health 16, 100303 (2021).
Luppi, A. I. et al. A synergistic workspace for human consciousness revealed by integrated information decomposition. eLife 12, RP88173 (2024).
Luppi, A. I. et al. Computational modelling in disorders of consciousness: closing the gap towards personalised models for restoring consciousness. NeuroImage 275, 120162 (2023).
Schaefer, A. et al. Local-global parcellation of the human cerebral cortex from intrinsic functional connectivity MRI. Cereb. Cortex 28, 3095–3114 (2018).
Coifman, R. R. & Lafon, S. Diffusion maps. Appl. Comput. Harmon. Anal. 21, 5–30 (2006).
Xia, Y. et al. Development of functional connectome gradients during childhood and adolescence. Sci. Bull. 67, 1049–1061 (2022).
Tomoda, A., Polcari, A., Anderson, C. M. & Teicher, M. H. Reduced visual cortex gray matter volume and thickness in young adults who witnessed domestic violence during childhood. PLoS ONE 7, e52528 (2012).
Markello, R. D. & Misic, B. Comparing spatial null models for brain maps. NeuroImage 236, 118052 (2021).
Zhang, X.-H. et al. The cellular underpinnings of the human cortical connectome. bioRxiv https://doi.org/10.1101/2023.07.05.547828 (2023).
Luppi, A. I. et al. A synergistic core for human brain evolution and cognition. Nat. Neurosci. 25, 771–782 (2022).
Anastasiades, P. G., de Vivo, L., Bellesi, M. & Jones, M. W. Adolescent sleep and the foundations of prefrontal cortical development and dysfunction. Prog. Neurobiol. 218, 102338 (2022).
Keshavan, M. S., Giedd, J., Lau, J. Y. F., Lewis, D. A. & Paus, T. Changes in the adolescent brain and the pathophysiology of psychotic disorders. Lancet Psychiatry 1, 549–558 (2014).
Canbeyli, R. Sensorimotor modulation of mood and depression: an integrative review. Behav. Brain Res. 207, 249–264 (2010).
Canbeyli, R. Sensory stimulation via the visual, auditory, olfactory and gustatory systems can modulate mood and depression. Eur. J. Neurosci. 55, 244–263 (2022).
Panzeri, S., Petersen, R. S., Schultz, S. R., Lebedev, M. & Diamond, M. E. The role of spike timing in the coding of stimulus location in rat somatosensory cortex. Neuron 29, 769–777 (2001).
Ibanez, A., Kringelbach, M. L. & Deco, G. A synergetic turn in cognitive neuroscience of brain diseases. Trends Cogn. Sci. 28, 319–338 (2024).
Robison, A. J., Thakkar, K. N. & Diwadkar, V. A. Cognition and reward circuits in schizophrenia: synergistic, not separate. Biol. Psychiatry 87, 204–214 (2020).
Kaczkurkin, A. N. et al. Dimensions of psychopathology are dissociably linked to brain structure in youth. Am. J. Psychiatry 176, 1000–1009 (2019).
Kaczkurkin, A. N. et al. Evidence for dissociable linkage of dimensions of psychopathology to brain structure in youths. Am. J. Psychiatry 176, 1000–1009 (2019).
Kaczkurkin, A. N., Raznahan, A. & Satterthwaite, T. D. Sex differences in the developing brain: insights from multimodal neuroimaging. Neuropsychopharmacology 44, 71–85 (2019).
Modabbernia, A. et al. Linked patterns of biological and environmental covariation with brain structure in adolescence: a population-based longitudinal study. Mol. Psychiatry 26, 4905–4918 (2021).
Watt, D. F. & Panksepp, J. Depression: an evolutionarily conserved mechanism to terminate separation distress? A review of aminergic, peptidergic, and neural network perspectives. Neuropsychoanalysis 11, 7–51 (2009).
Jernigan, T. L., Brown, S. A. & Dowling, G. J. The adolescent brain cognitive development study. J. Res. Adolesc. 28, 154–156 (2018).
Passarello, N. et al. Sensory processing disorders in children and adolescents: taking stock of assessment and novel therapeutic tools. Brain Sci. 12, 1478 (2022).
Peters, S. K., Dunlop, K. & Downar, J. Cortico-striatal-thalamic loop circuits of the salience network: a central pathway in psychiatric disease and treatment. Front. Syst. Neurosci. 10, 104 (2016).
Ruffini, G., Castaldo, F., Lopez-Sola, E., Sanchez-Todo, R. & Vohryzek, J. The algorithmic agent perspective and computational neuropsychiatry: from etiology to advanced therapy in major depressive disorder. Entropy 26, 953 (2024).
Hansen, J. Y. et al. Mapping neurotransmitter systems to the structural and functional organization of the human neocortex. Nat. Neurosci. 25, 1569–1581 (2022).
Wan, B. et al. Microstructural asymmetry in the human cortex. Nat. Commun. 15, 10124 (2024).
Sullivan, P. F. & Geschwind, D. H. Defining the genetic, genomic, cellular, and diagnostic architectures of psychiatric disorders. Cell 177, 162–183 (2019).
Chaudhury, D., Liu, H. & Han, M.-H. Neuronal correlates of depression. Cell. Mol. Life Sci. 72, 4825–4848 (2015).
Luscher, B., Shen, Q. & Sahir, N. The GABAergic deficit hypothesis of major depressive disorder. Mol. Psychiatry 16, 383–406 (2011).
Aan Het Rot, M., Mathew, S. J. & Charney, D. S. Neurobiological mechanisms in major depressive disorder. CMAJ 180, 305–313 (2009).
Sadeghi, N. et al. Mood and behaviors of adolescents with depression in a longitudinal study before and during the COVID-19 pandemic. J. Am. Acad. Child Adolesc. Psychiatry 61, 1341–1350 (2022).
Gorgolewski, K. J. et al. The brain imaging data structure, a format for organizing and describing outputs of neuroimaging experiments. Sci. Data 3, 1–9 (2016).
Esteban, O. et al. fMRIPrep: a robust preprocessing pipeline for functional MRI. Nat. Methods 16, 111–116 (2019).
Gorgolewski, K. et al. Nipype: a flexible, lightweight and extensible neuroimaging data processing framework in python. Front. Neuroinform. 5, 13 (2011).
Wang, H.-T. et al. Continuous evaluation of denoising strategies in resting-state fMRI connectivity using fMRIPrep and Nilearn. PLoS Comput. Biol. 20, e1011942 (2024).
Ben-Hur, A., Elisseeff, A. & Guyon, I. A stability based method for discovering structure in clustered data. In Biocomputing 2002 (eds Altman, R. B., Dunker, A. K., Hunter, L., Lauderdale, K. & Klein, T. E.) 6–17 (World Scientific, 2001).
Kuncheva, L. I. & Vetrov, D. P. Evaluation of stability of k-means cluster ensembles with respect to random initialization. IEEE Trans. Pattern Anal. Mach. Intell. 28, 1798–1808 (2006).
Yarkoni, T., Poldrack, R. A., Nichols, T. E., Van Essen, D. C. & Wager, T. D. Large-scale automated synthesis of human functional neuroimaging data. Nat. Methods 8, 665–670 (2011).
Mediano, P. A. M., Rosas, F. E., Bor, D., Seth, A. K. & Barrett, A. B. The strength of weak integrated information theory. Trends Cogn. Sci. 26, 646–655 (2022).
Mediano, P. A. M., Rosas, F. E., Barrett, A. B. & Bor, D. Decomposing spectral and phasic differences in nonlinear features between datasets. Phys. Rev. Lett. 127, 124101 (2021).
Mediano, P. A. M. et al. Integrated information as a common signature of dynamical and information-processing complexity. Chaos Interdiscip. J. Nonlinear Sci. 32, 013115 (2022).
Elam, J. S. et al. The Human Connectome Project: a retrospective. NeuroImage 244, 118543 (2021).
Shen, E. H., Overly, C. C. & Jones, A. R. The Allen Human Brain Atlas: comprehensive gene expression mapping of the human brain. Trends Neurosci. 35, 711–714 (2012).
Zhou, Y. et al. Metascape provides a biologist-oriented resource for the analysis of systems-level datasets. Nat. Commun. 10, 1523 (2019).
Acknowledgements
We acknowledge the financial support from the Grassroots Health Science and Technology Innovation Project of the Health Commission of Hubei Province. We also extend our gratitude to Drs. Wang Gaohua, Liu Zhongchun, Zha Yunfei, Wang Haibo, Qian Hong and Guo Xin from Renmin Hospital of Wuhan University, Dr. Ren Hongwei from Tianyou Hospital Affiliated to Wuhan University of Science and Technology, and Dr. Wang Sanwang and Lu Lin from Peking University for their contributions to data collection and research design. X.L. is supported by the China Scholarship Council. B.W. is supported by the International Max Planck Research School on Neuroscience of Communication: Function, Structure, and Plasticity (IMPRS NeuroCom), the Graduate Academy Leipzig, and Mitacs Globalink Research Award. G.Y. is supported by the Beijing Institute of Technology, School of Interdisciplinary Science, with the National Natural Science Foundation of China (grant numbers 82302175 and 62336002) and the National Science and Technology Innovation 2030 Program (grant numbers 2021ZD0200500 and 2021ZD0200506). This work was supported in part by the Health of Hubei Province Scientific Research Project under Grant 2020Cfb512, and by the Mental Health Research Institute of Three Gorges University: YCXL-23-11. This work was partially supported by the Beijing Institute of Technology Kunpeng&Ascend Center of Cultivation. We thank the National Center for Protein Sciences at Peking University in Beijing, China for assistance on data analysis.
Author information
Authors and Affiliations
Contributions
X.L., G.Y., and Y.G. designed research; X.L., B.W. and G.Y. analyzed the data; X.Y.W. draw the figures; X.L. and G.Y. wrote the first draft of the manuscript; X.Z., L.L., X.Y.W., S.L., R.G., R.C., X.W., X.Q.L., P.W., Y.G. and G.Y. edited the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Mingrui Xia, who co-reviewed with Xiaoyi Sun, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, X., Wan, B., Wu, X. et al. Subtypes of adolescent major depressive disorder characterized by divergent information dynamics in sensory-association cortices. Nat Commun 17, 3055 (2026). https://doi.org/10.1038/s41467-026-69697-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-026-69697-2
