
Abstract
Global cross-country socioeconomic inequalities in all-cause age-standardized mortality (SIAM) have persisted over decades, but major contributing causes and risk factors remain unclear. Here, we quantified contributions of 288 causes and 84 risk factors to SIAM using the Global Burden of Disease Study 2021 (GBD 2021). From 1990 to 2021, communicable, maternal, neonatal, and nutritional diseases’ contribution fell from 81.2% to 56.6%, while non-communicable diseases’ contribution from 13.2% to 27.8%. The top five causes of death contributing to SIAM in 2021 were COVID-19 (17.9%), stroke (9.4%), tuberculosis (7.3%), lower respiratory infections (7.0%), and diarrheal diseases (5.5%). The top five risk factors contributing to SIAM in 2021 were household air pollution from solid fuels (17.2%), high systolic blood pressure (9.9%), unsafe sex (4.6%), high fasting plasma glucose (4.4%), and unsafe water sources (4.2%). Overall, this study provides policymakers with data to promote global health equity by targeting key causes and risk factors contributing to cross-country mortality inequality.
Similar content being viewed by others

Introduction
Health inequalities associated with socioeconomic status are a persistent global concern, with profound implications for social justice, economic development, and public health policies1,2,3. These inequalities are particularly pronounced when comparing mortality rates and disease burdens across countries or regions, where socioeconomic status (measured by indicators like income per capita or development indices) plays a critical role3,4,5. Although global public health policies have made substantial progress in reducing cross-country health inequalities in recent years, health disparities between different socioeconomic groups remain significant, particularly in certain diseases, such as infectious diseases, malnutrition, cardiorespiratory, and digestive diseases2,3,4,5,6,7,8,9,10.
To understand cross-country health inequalities, it is essential to decompose them by specific causes of death and risk factors. This helps identify which diseases or health risks are most responsible for the observed inequalities, enabling targeted interventions and health policies to narrow these gaps11. For instance, communicable diseases and injuries disproportionately affect lower-income countries, while non-communicable diseases might show different patterns, influenced by risk factors like tobacco use or physical inactivity4,12. Some national studies, such as those in Iran and South Korea, have examined mortality inequalities by causes of death, identifying key contributors like accidents and external causes13,14. Several global studies have also evaluated socioeconomic disparities in burdens caused by specific diseases4,6,8,9,10. However, there has been no comprehensive global analysis on cross-country socioeconomic inequality in mortality by a wide range of causes and risk factors over an extended period.
To address this research gap, we need country-level comparable and standardized mortality data by causes and risk factors. The Global Burden of Disease (GBD) study has been the best available data resource for this purpose. GBD 2021 integrates diverse data sources, such as vital registration, surveys, censuses, and surveillance systems, into a unified modeling framework to produce comparable all-cause and cause-specific (for 288 causes of deaths) mortality estimates across 204 countries and territories from 1990 to 202115. Exposures of more than 80 risk factors and their attributable disease burden are assessed using the Comparative Risk Assessment framework, which links exposure distributions with dose–response functions to quantify population-attributable mortality rates and disease burdens16.
In this work, leveraging standardized and comparable mortality data from GBD 2021, we comprehensively quantified the global cross-country socioeconomic inequalities in mortality rates from 1990 to 2021, as well as the specific contributions of 288 causes of death and 84 risk factors. By doing so, we provided detailed insights into the key drivers to these inequalities, informing more targeted and effective global health equity strategies.
Results
Overall socioeconomic inequality in all-cause mortality
We observed persistent global socioeconomic inequalities in all-cause age-standardized mortality (SIAM) from 1990 to 2021, as indicated by the negative correlations between all-cause age-standardized mortality (ASM) and socio-demographic index (SDI) (Fig. 1a), as well as the decreasing ASM with increasing SDI categories (Fig. 1b). Overall, SDI could explain 51–65% (model R2:0.51–0.65) of variations in all-cause age-standardized mortality in 1990, 2000, 2010, 2019, and 2021 (Table 1). The SIAM quantified as the Beta value showed an improving trend from 1999 to 2019 but then reversed during 2020 and 2021 due to the COVID-19 (Fig. 1c). As a result, the largest SIAM was observed in 2021, with each 0.1-unit increase in SDI associated with a 225.0 per 100,000 residents (95% CI: −233.2 to −216.8) decrease in ASM (Table 1).

a Association between ASM (per 100,000 population) and SDI in 1990, 2000, 2010, 2019, and 2021. Solid lines represent linear regression estimates (central estimates). Shaded bands represent 95% confidence intervals derived from linear regression of data points of 32 years. b Distribution of country-level ASM by SDI category. Box plots show the median (center line), interquartile range (IQR; box limits represent 25th and 75th percentiles), whiskers extending to 1.5× IQR, and points beyond whiskers representing outliers. c Socioeconomic inequality in ASM quantified as regression coefficient (β; change in ASM per 0.1 increase in SDI, unit: deaths per 100,000). Points represent β estimates (central estimates); error bars represent 95% confidence intervals derived from 1000 times of bootstrap simulations. d Contribution of level 1 causes to socioeconomic inequality in ASM (SIAM). e Socioeconomic inequality in ASM by level 1 risk factors. Points regression coefficients (β); error bars represent 95% confidence intervals derived from 1000 times of bootstrap simulations. f Contribution of level 1 risk factors to SIAM (%).
Contributions of specific causes of death to SIAM
We then decomposed the SIAM by causes of death and risk factors, with the contribution calculated as \(\frac{{\beta }_{{{\rm{specific}}}}}{{\beta }_{{all}}}\). The \({\beta }_{{all}}\) refers to the SIAM, while the \({\beta }_{{{\rm{specific}}}}\) refers to the socioeconomic inequality in cause- or risk-specific ASM, all presented as Beta values in tables and figures. The sum of \({\beta }_{{{\rm{specific}}}}\) for all exclusive specific causes is equal to the \({\beta }_{{all}}\) because causes of death are collectively exhaustive, and thus the contribution of all different exclusive causes of death to the SIAM can add up to 100%. However, the contributions by risk factor do not add up to 100% as they are neither mutually exclusive nor collectively exhaustive.
Among the three level 1 causes of death, CMNNDs contributed the largest proportion of the SIAM, although their contribution decreased from 81.2% (95% CI: 80.4–82.1%) in 1990 to 56.6% (95% CI: 56.0–57.1%) in 2021 (Table 1, Fig. 1c, d). Respiratory infections and tuberculosis have been the leading level 2 causes of death contributing to the SIAM from 1990 to 2021 (Fig. 2a). Their contribution decreased from 27.5% in 1990 to 21.1% in 2019 but then increased again to 32.4% in 2021 due to the impacts of COVID-19 (Figs. S1–S2). Enteric infections were the second largest level 2 cause contributing to the SIAM in 1990 (18.1%), but their contribution showed consistent downward trends and decreased to 5.9% by 2021. Similarly, the contribution of neglected tropical diseases and malaria, HIV/AIDS and sexually transmitted infections, and other infectious diseases also showed decreasing trends at least since 2004, all falling to around 5% by 2021 (Fig. S2). Decreasing trends from 1990 to 2021 were also evident for the contribution of maternal and neonatal disorders (from 8.4 to 4.8%) and the contribution of nutritional deficiencies (from 3.9 to 1.2%).

a Contribution by level 2 causes. b Contribution by level 2 risk factors Bars represent central estimates. Error bars represent 95% confidence intervals derived from 1000 times of bootstrap simulations.
However, the contribution of NCDs to SIAM rose from 13.2% (95% CI: 11.8–14.5%) in 1990 to 36.2% (95% CI: 35.1–37.2%) in 2019 and then decreased to 27.8% (95% CI: 26.7–28.7%) in 2021. Notably, the contribution of cardiovascular diseases rapidly increased (Fig. S2) and has become the second largest level 2 cause of death contributing to SIAM since 2010, with a contribution reaching 15.3% in 2021.
The contribution of injuries to SIAM showed no clear trends, all below 10% except for 1995 (about 14%). The main contributors were unintentional injuries, followed by transport injuries, self-harm, and interpersonal violence.
The top one level 3 causes of death contributing to the SIAM were all infectious diseases over 1990–2021, which were diarrheal diseases (17.1% of SIAM) in 1990, HIV/AIDS (13.6%) in 2000, tuberculosis (10.9%) in 2010, and COVID-19 (17.9%) in 2021 (Fig. 3). Other infectious diseases are also among the top ten diseases contributing to SIAM, mainly including lower respiratory infections, and malaria, and their contributions were all decreasing over time. Among NCDs, stroke had become the second largest contributor of SIAM since 2010 and ranked the first during 2012–2019 (Figs. S3–S5). Among injuries, road injuries were consistently one of the top 20 causes of death contributing to SIAM, although its contribution was relatively small (<2%). The contributions of all detailed causes of death to the SIAM are presented in Table S1.

a–e were the top 20 level 3 causes in 1990, 2000, 2010, 2019, and 2021, respectively. Bars represent central estimates. Error bars represent 95% confidence intervals derived from 1000 times of bootstrap simulations.
Contribution of specific risk factors to SIAM
Overall, over half of the SIAM (i.e., Beta values for all causes) were contributed by all GBD 2021 risk factors (i.e., Beta values for all risk factors) in 1990, 2000, and 2010, although this contribution proportion decreased to 42.2% (95% CI: 41.7–42.6%) in 2021 (Table 1, Fig. 1f). Environmental/occupational risk factors explained the largest proportion of SIAM, followed by behavioral risk factors, and metabolic risk factors. The contribution of environmental/occupational and behavioral risk factors to SIAM saw significant decreases: from 41.8% and 28.2% in 1990, to 26.3% and 19.4% in 2021, respectively. However, the contribution of metabolic risk factors showed a clear increasing trend from 4.0% in 1990 to 16.0% in 2021 (Table 1).
The leading level 2 risk factors contributing to SIAM were air pollution (contribution: about 20% of SIAM, slight decrease from 21.9% in 1990 to 17.9% in 2021) (Figs. S6–S7), child and maternal malnutrition (rapid decrease from 22.6 to 6.9%), and unsafe water, sanitation, and handwashing (rapid decrease from 19.6 to 6.9%) (Fig. 2b). Notable increasing trends were observed for the contributions of high systolic blood pressure (from 1.4% in 1990 to 9.9% in 2021), dietary risks (2.3–6.4%), high fasting plasma glucose (1.6–4.4%), and kidney dysfunction (1.8–3.4%).
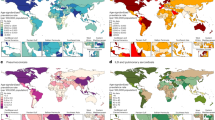
Among all level 3 risk factors, particulate matter air pollution was consistently the top risk factor contributing to SIAM, and its contribution only slightly decreased from 1990 to 2021 (Fig. 4, Figs. S8–9). It should be noted that the contribution to SIAM of this risk factor was dominated (>95%) by the contribution of household particulate matter air pollution from solid fuels, rather than ambient (i.e., outdoor) particulate matter air pollution (Table S2).

a–e were the top 20 level 3 risk factors in 1990, 2000, 2010, 2019, and 2021, respectively. Bars represent central estimates. Error bars represent 95% confidence intervals derived from 1000 times of bootstrap simulations. The particulate matter air pollution can be specified as two level 4 risk factors: “household air pollution from solid fuels” and “ambient particulate matter pollution”. From Table S2, it is clear that the contribution of particulate matter air pollution was largely (>95%) contributed by household air pollution from solid fuels (i.e., indoor particulate matter air pollution caused by burning solid fuels).
Child growth failure was the second-highest contributor to SIAM in 1990, but its ranking decreased to 9th by 2021 (Fig. S10). Similarly, the rankings of unsafe water sources, unsafe sanitation, and no access to a handwashing facility also dropped significantly over the three decades. By contrast, high systolic blood pressure and high fasting plasma glucose had risen to the second and fourth leading risk factors contributing to SIAM by 2021.
Sensitivity analyses by removing 5% countries with the highest relative uncertainty of all-cause mortality estimates (indicating low-quality data) showed highly consistent estimates of Beta and SIAM contributions with those of our main analyses (all agreement R2 > 0.999, Fig. S11).
The sudden decrease in SIAM in 1994 and some moderate decreases in SIAM during 2010–2012 can be explained by the Rwanda genocide of 1994, the 2010 Haiti earthquake, and the 2011 Somalia famine, as detailed in Fig. S13.
Discussion
To the best of our knowledge, this is by far the most comprehensive assessment of the causes of death and risk factors contributing to the global SIAM. We found consistent global SIAM from 1990 to 2021, with the largest inequality seen in 2021 due to COVID-19. CMNNDs were the largest contributors to SIAM, and their impacts remained significant despite notable decreases in three decades. Respiratory infections and tuberculosis remained the leading level 2 causes, with their contribution peaking in 2021 due to COVID-19. Conversely, contributions from enteric infections, neglected tropical diseases, malaria, HIV/AIDS, maternal and neonatal disorders, and nutritional deficiencies declined significantly. NCDs saw a rising contribution, with cardiovascular diseases emerging as the second largest level 2 contributor. The contribution of injuries showed no clear trend.
Regarding risk factors, environmental/occupational risk factors (e.g., air pollution) contributed to the largest proportion of SIAM, followed by behavioral risk factors (e.g., child and maternal malnutrition), but they both decreased significantly in contribution, while the contribution of metabolic risk factors (e.g., high systolic blood pressure) increased markedly. Particulate air pollution, particularly from household sources, was consistently the top contributing risk factor of SIAM, though its dominance slightly waned, while high systolic blood pressure rose to the second leading contributing risk factor by 2021.
The decreasing contribution of CMNNDs to SIAM reflects global improvements in addressing those issues, particularly in low- and middle-income countries15. Such improvement is driven by progress made in reducing key risk factors for these diseases, including child and maternal malnutrition, unsafe water, sanitation, and handwashing, and unsafe sex, etc., as supported by our results (Fig. 2), which aligns well with the achievements of the United Nations Millennial Development Goals17. Despite overall progress, infectious diseases remained the top contributors to SIAM over the years, with COVID-19 being the leading contributor in 2021. The emergence of COVID-19 has reversed some of the gains made in reducing inequality in infectious disease mortality. This finding underscores the need for improving public health systems capable of responding to pandemics and other emerging infectious disease outbreaks in less developed countries, e.g., through improving vaccine access and human resources for health.
The rising contribution of NCDs highlights a shift in the drivers of global health inequality. This shift is consistent with the classical epidemiological transition theory, first proposed by Abdel Omran in 1971, which describes a long-term shift in disease patterns whereby pandemics of infection are gradually displaced by degenerative and man-made diseases as primary causes of death as societies develop economically18. The GBD study has reported such transitions in many countries, where NCDs become more prevalent as infectious diseases are controlled19. Our findings suggest that such epidemiological transition varies significantly by socioeconomic level, aligning with critiques of Omran’s original linear models, which noted that observed transitions often do not follow a single pathway across all countries20. Specifically, less developed countries often experience a “protracted and polarized” transition, where they carry a dual burden of persistent infectious diseases alongside the rising prevalence of NCDs. This is supported by our results that the socioeconomic inequality in infectious diseases remained significant in recent years, while the inequality in NCDs had risen significantly over the three decades. Given that the countries at the high or low end of the SDI scales almost did not change over the three decades (Fig. S12), these results suggest that less developed countries tended to have experienced slower decreases of infectious diseases while similar or even faster increases in NCDs, making them bear the dual burden of infectious diseases and NCDs in recent years. Public health policies, guided by the broader health transition framework that incorporates social and behavioral determinants of health21, need to address this growing dual challenge through effective prevention and management of NCDs (particularly cardiovascular diseases) while maintaining vigilance against infectious diseases. The prevention and management strategies include but are not limited to lifestyle interventions, early detection, and improved healthcare services22.
The significant decrease in the proportion of SIAM explained by environmental/occupational and behavioral risk factors, alongside the increase in metabolic risk factors, indicates changing risk profiles over time23. The enduring impact of environmental risks, notably household air pollution, underscores the urgency of clean energy initiatives in low- and middle-income countries24,25. Previous studies have suggested that transitioning from solid cooking fuels (coal or charcoal, wood, crop residues, and dung) to cleaner energy sources can effectively reduce household air pollution and the associated health consequences26,27. Our study suggests that promoting such clean energy initiatives in low- and middle-income countries tends to improve global health equity as well.
The rising contribution of metabolic risk factors, such as high systolic blood pressure and high fasting plasma glucose, reflects the growing impact of lifestyle-related conditions. Public health policies should focus on promoting healthy lifestyles, improving access to preventive healthcare, and addressing social determinants of health to reduce the burden of these risk factors and promote health equity28.
Our study addressed a complex question that involves multiple dimensions, including country, year, causes of death, and risk factors. While we acknowledge that a single, complex statistical model (e.g., panel regressions, machine learning models) could potentially capture all interactions between different dimensions simultaneously, we finally employed a series of annual cross-country linear regressions for each specific cause of death and risk factors. This simple approach is sustainable for several key reasons. First, this approach aligns with the established methodology for inequality metrics within the GBD framework, serving as a direct, interpretable variant of the widely used slope index of inequality approach in health equity research2. This consistency ensures our findings are comparable to a large body of existing literature1,2,29. Second, running separate, granular models for each of the 288 causes of death and 84 risk factors allowed us to isolate and rank the precise, time-varying contribution of each specific driver to the overall SIAM, providing highly actionable insights for policymakers that might be obscured by a single, all-encompassing panel regression model. Finally, the resulting β coefficient offers enhanced interpretability and transparency, as it is easily understood as the change in deaths per 100,000 residents associated with each 0.1 increase in SDI, making the metric more accessible for a general public health audience and practical for policy implementation.
Overall, our findings of persistent global SIAM, with higher mortality in lower SDI regions, align well with extensive existing literature documenting the social gradient in health outcomes2,30. However, our granular, cause- and risk-specific approach goes beyond previous studies by identifying specific emerging drivers of inequality. By systematically quantifying the contribution of 288 causes of death and 84 risk factors to the SIAM from 1990 to 2021 with robust GBD data and a comparable inequality metric, we have made major progress compared with previous studies that only evaluated overall inequality or inequality in certain specific diseases or risk factors1,2,3,4,5,6,7,8,9,10. The long temporal span captured major health transitions, including the rise of NCDs, HIV/AIDS epidemic’s decline and COVID-19’s emergence, offering a dynamic view of inequality trends and the shift in major drivers of health inequality. Our findings validate and complement the epidemiological transition theory from the perspective of inequality: the contribution of CMNNDs to health inequality has decreased over time, while that of NCDs has risen. Despite the comprehensive analysis, several limitations of this study should be acknowledged. The data quality of GBD estimates varied across countries and tended to be lower in low-SDI settings, which may introduce bias in the inequality analyses3. However, our sensitivity analysis by removing 5% countries with low-quality mortality data showed highly consistent (R2 > 0.999 compared with the main analyses, Fig. S11), suggesting our findings are generally robust against low data quality settings. The GBD risk factors could only explain about half of the SIAM, suggesting there are many omitted risk factors (e.g., conflicts, natural disasters, climate change, biodiversity loss) that warrant further investigation. Our cross-country inequality analyses cannot assess within-country or between-individual socioeconomic disparities. Further subnational or individual-level studies are required to address this gap.
In conclusion, this study illuminates the evolving landscape of cross-country socioeconomic inequality in mortality from 1990 to 2021, highlighting a persistent mortality inequality but shifting major contributors. These findings offer a vital evidence base for reducing global health inequities, urging policymakers to act more decisively to bridge the mortality gap across socioeconomic divides.
Methods
This study is a secondary analysis of publicly available, de-identified, aggregated data from GBD 2021 and does not involve human participants. Therefore, ethics approval, informed consent, and participant compensation were not required. This study complies with the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER).
Data collection
We collected data on the socio-demographic index (SDI), ASM, and ASM attributable to 288 causes of death and 84 risk factors, for 204 countries or territories during 1990–2021 from the GBD 202115,23. SDI is an integrated index that measures the social and economic development of a country (or territory), combining data on the economy, education, and fertility rate, with a range from 0 to 1 (where a higher value indicates better socioeconomic status).31 GBD 2021 classified 204 countries and territories into five SDI categories: low, low-medium, medium, medium-high, and high. ASM refers to mortality rates standardized according to a common age structure, allowing for comparison across countries with different age distributions.
GBD 2021 divided 288 causes of death into four levels15. Level 1 included three broad categories: Communicable, Maternal, Neonatal, and Nutritional Diseases (CMNNDs), non-communicable diseases (NCDs), and injuries. Level 2 further broke these categories down into 22 specific subcategories, such as cardiovascular diseases under the NCDs. Level 3 refined these subcategories into specific diseases, such as stroke under cardiovascular diseases, and level 4 provided even more detailed classifications (e.g., distinguishing ischemic stroke and subarachnoid hemorrhage within the stroke category). This hierarchical classification enabled a detailed and comprehensive analysis of mortality from various causes of death.
Similarly, GBD 2021 also categorized 88 risk factors into four levels to systematically assess the impact of various types of risk factors on mortality23. At the broadest level, level 1 encompasses categories such as environmental, behavioral, and metabolic factors. As levels progress, risk factors were defined and categorized with increasing specificity. For instance, “Environmental/occupational risks” in level 1 includes “Air pollution” in Level 2, and this can be specified as “Particulate matter pollution” in Level 3, which could be further specified as “Ambient particulate matter pollution” and “Household air pollution from solid fuels” in Level 4. Because the GBD did not make the risk-specific ASM of four risk factors (nitrogen dioxide pollution, occupational noise, occupational ergonomic factors, and bullying victimization) openly available, we did not include these four risk factors in our analyses. As a result, 84 risk factors were included. However, the “All risk factors” still refers to the sum of all exclusive risk factors in GBD 2021.
Statistical analyses
For each year, we quantified socioeconomic inequality in ASM, using a linear regression approach with the equation below31:
where\(\,{{ASM}}_{i}\) is the age-standardized mortality rate in the country or territory i; \(\alpha\) is the intercept; \({{{\rm{\varepsilon }}}}_{i}\) is the residual error. The socioeconomic inequality in ASM was quantified as the regression coefficient \(\beta\), presented as changes in ASM (unit: 1/100,000, or 1 death per 100,000 residents each year) associated with each 0.1 increase in SDI. The regression coefficients (Beta values) were estimated separately for each calendar year. Here, the Beta value, as a metric of socioeconomic inequality in mortality, is similar to the widely used Slope Index of Inequality (SII), and both of them can reflect the overall socioeconomic inequality pattern32. However, the Beta value provides a tangible rate of change (deaths per 100,000 residents per 0.1 SDI) that is more intuitive for public health communication and policy planning, offering much better interpretability than SII, which represents a theoretical gap between the extreme ends of a ranked hierarchy that may not exist in reality1. Because the main aim of the regression is to obtain a measure of the socioeconomic inequality in mortality, rather than to quantify the relationship between SDI and mortality, we did not add any other covariates (i.e., not considering any confounding effects) in the regression model, which is a standard approach for estimating the slope index of inequality29.
With Eq. (1), we quantified global socioeconomic inequality in all-cause ASM (\({\beta }_{{{\rm{all}}}}\)), with all-cause ASM as the dependent variable. We also quantified socioeconomic inequality in cause- or risk-factor-specific ASM (\({\beta }_{{{\rm{specific}}}}\)) by setting ASM attributable to a specific cause of death or risk factor as the dependent variable.
Then the contribution of each specific cause of death or risk factor to the overall socioeconomic inequality in mortality in each year was calculated as \(100\%\times \frac{{\beta }_{{{\rm{specific}}}}}{{\beta }_{{{\rm{all}}}}}\). We used a bootstrap approach to quantify the uncertainties, i.e., 95% CI of the \({\beta }_{{{\rm{all}}}}\), \({\beta }_{{{\rm{specific}}}}\), and contributions. Briefly, for each simulation, we randomly selected the country-specific all-cause and cause- or risk-factor-specific ASM from their distributions estimated by GBD assuming independent normal distributions (i.e., mean at point estimate, standard error approximated by range of 95% CI divided by 3.92). We obtained the \({\beta }_{{{\rm{all}}}}\) and \({\beta }_{{{\rm{specific}}}}\) for each simulation using the regression approach mentioned above. This simulation was repeated 1000 times, and the 2.5th and 97.5th percentiles of the 1000 simulated \(\frac{{\beta }_{{{\rm{specific}}}}}{{\beta }_{{all}}}\) were reported as the 95% CI of the contribution.
To test the robustness of our results against the data quality of GBD estimates, we repeated the above analyses by removing countries or territories with the top 5% (i.e., 10 countries) highest relative uncertainty (calculated as standard error divided by point estimates) of the all-cause mortality rate estimates33. The results were then compared with those from our main analyses.
All data analyses were performed using R software (version 4.2.1).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The data are publicly available at https://doi.org/10.26180/30856565. Source data are provided with this paper.
Code availability
The code are public available at https://doi.org/10.26180/30856565.
References
Hosseinpoor, A. R. et al. Measuring health inequalities in the context of sustainable development goals. Bull. World Health Organ 96, 654–659 (2018).
Steinbeis, F. et al. Quantifying changes in global health inequality: the Gini and Slope Inequality Indices applied to the Global Burden of Disease data, 1990-2017. BMJ Glob. Health 4, e001500 (2019).
Zheng, Y. et al. Global health inequality: analyses of life disparity and healthy life disparity. Eur. J. Public Health 34, 225–229 (2024).
Emadi, M. et al. Global socioeconomic inequality in the burden of communicable and non-communicable diseases and injuries: an analysis on global burden of disease study 2019. BMC Public Health 21, 1771 (2021).
Yan, W. et al. Association between inequalities in human resources for health and all cause and cause specific mortality in 172 countries and territories, 1990-2019: observational study. BMJ 381, e073043 (2023).
Li, H. et al. Health inequality in the global burden of chronic obstructive pulmonary disease: findings from the global burden of disease study 2019. Int. J. Chron. Obstruct. Pulmon. Dis. 17, 1695–1702 (2022).
Deng, P. et al. Temporal trends in inequalities of the burden of HIV/AIDS across 186 countries and territories. BMC Public Health 23, 981 (2023).
Haacker, M. Contributions of declining mortality, overall and from HIV, TB and malaria, to reduced health inequality and inequity across countries. Health Policy Plan 38, 939–948 (2023).
Jiang, W. et al. Health inequalities of global protein-energy malnutrition from 1990 to 2019 and forecast prevalence for 2044: data from the Global Burden of Disease Study 2019. Public Health 225, 102–109 (2023).
Peng, J. et al. Global Inequalities in the burden of digestive diseases from 1990 to 2019: findings from the global burden of disease study 2019. Gastroenterology 166, 223–224.e1 (2024).
Sommer, I. et al. Socioeconomic inequalities in non-communicable diseases and their risk factors: an overview of systematic reviews. BMC Public Health 15, 914 (2015).
Hosseinpoor, A. R. et al. Socioeconomic inequalities in risk factors for non communicable diseases in low-income and middle-income countries: results from the World Health Survey. BMC Public Health 12, 912 (2012).
Hosseinpoor, A. R. et al. Decomposing socioeconomic inequality in infant mortality in Iran. Int. J. Epidemiol. 35, 1211–1219 (2006).
Jung-Choi, K. et al. Contribution of different causes of death to socioeconomic mortality inequality in Korean children aged 1-9: findings from a national mortality follow-up study. J. Epidemiol. Community Health 65, 124–129 (2011).
GBDCoD, C. collaborators Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 403, 2100–2132 (2024).
Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 403, 2162–2203 (2024).
Laura, K. S. The United Nations Millennium Development Goals: successes and failures from 2000 until today. United Nations Association of Australia Available at: https://www.unaa.org.au/2017/01/19/the-united-nations-millennium-development-goals-successes-and-failures-from-2000-until-today/ accessed May, 2025.
Omran, A. R. The epidemiologic transition: a theory of the epidemiology of population change. Milbank Mem. Fund. Q. 49, 509–538 (1971).
GBD 2021 Diseases and Injuries Collaborators Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 403, 2133–2161 (2024).
Frenk, J. et al. Health transition in middle-income countries: new challenges for health care. Health Policy Plann. 4, 29–39 (1989).
Defo, K. uate B. Demographic, epidemiological, and health transitions: are they relevant to population health patterns in Africa?. Glob. Health Action 7, 22443 (2014).
NCD Countdown 2030 Collaborators NCD Countdown 2030: efficient pathways and strategic investments to accelerate progress towards the Sustainable Development Goal target 3.4 in low-income and middle-income countries. Lancet 399, 1266–1278 (2022).
Collaborators GBDRF Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 403, 2162–2203 (2024).
GBD 2021 Household Air Pollution Collaborators. Global, regional, and national burden of household air pollution, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 405, 1167–1181 (2025).
Johns, N. E. et al. The wealth (and health) of nations: a cross-country analysis of the relation between wealth and inequality in disease burden estimation. Lancet 381, S66 (2013).
Zhao, B. et al. Change in household fuels dominates the decrease in PM(2.5) exposure and premature mortality in China in 2005-2015. Proc. Natl. Acad. Sci. USA 115, 12401–12406 (2018).
Checkley, W. et al. Cooking with liquefied petroleum gas or biomass and fetal growth outcomes: a multi-country randomised controlled trial. Lancet Glob. Health 12, e815–e825 (2024).
Thomson, K. et al. The effects of public health policies on health inequalities in high-income countries: an umbrella review. BMC Public Health 18, 869 (2018).
Moreno-Betancur, M. et al. Relative index of inequality and slope index of inequality: a structured regression framework for estimation. Epidemiology 26, 518–527 (2015).
Gómez-Ugarte, A. C. et al. Reassessing socioeconomic inequalities in mortality via distributional similarities. Popul. Health Metr. 23, 7 (2025).
Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2021 (GBD 2021) Socio-Demographic Index (SDI) 1950–2021. Institute for Health Metrics and Evaluation (2024). Available at: https://ghdx.healthdata.org/record/global-burden-disease-study-2021-gbd-2021-socio-demographic-index-sdi-1950%E2%80%932021.
Khang, Y. H. et al. A publicly well-accepted measure versus an academically desirable measure of health inequality: cross-sectional comparison of the difference between income quintiles with the slope index of inequality. BMJ Open 9, e028687 (2019).
GBD 2015 Mortality and Causes of Death Collaborators Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1459–1544 (2016).
Acknowledgements
This study was supported by the National Natural Science Foundation of China (grants 42505180 and HW2024004 by RX), CQMU Program for Youth Innovation in Future Medicine (W0190 by DP), Fundamental Research Funds for the Central Universities (project No.2025CDJ-IAISZD-003 by RX), Australian Research Council (grant number DP210102076 by YG) and the Australian National Health and Medical Research Council (NHMRC, grant number GNT2000581, GNT2040897, GNT1163693, and GNT2008813 by YG; grant number GNT2009866 by SL). G.C. is supported by the Australian Research Council Discovery Early Career Researcher Award (DECRA) Fellowship (DE250100889).
Author information
Authors and Affiliations
Contributions
R.X., D.P., Y.G., and S.L. designed the study and statistical methods. DP and RX took the lead in statistical analyses, visualisation, manuscript drafting, and results interpretation. D.P., R.X., S.H., L.M., G.C., Z.Y., Y.Z., M.J.A., S.L., and Y.G. contributed to interpreting the results, revising the manuscript, and approving the submission of the manuscript for publication.
Corresponding author
Ethics declarations
Competing interests
M.J.A. holds investigator initiated grants from Pfizer, Boehringer-Ingelheim, GlaxoSmithKline, and Sanofi for unrelated research. He has undertaken an unrelated consultancy for Sanofi and received a speaker’s fee from GSK. The other authors declare no competing interests. The funding bodies did not play any role in the study design, data collection, data analyses, results interpretation, and writing of this manuscript.
Peer review
Peer review information
Nature Communications thanks the anonymous reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Peng, D., Xu, R., Hales, S. et al. Decomposition of cross-country socioeconomic inequality in mortality by 288 causes of death and 84 risk factors from 1990 to 2021. Nat Commun 17, 2586 (2026). https://doi.org/10.1038/s41467-026-70877-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-026-70877-3
