
Abstract
Research on articular cartilage has primarily focused on athletes, particularly regarding increased metatarsal cartilage thickness in high-impact sports, with limited studies in military settings. This study examined Air Force Academy cadets, who experience unique mechanical demands on their hands. A total of 30 senior male cadets (age: 23.14 ± 0.51 years; height: 174.07 ± 3.14 cm; weight: 70.20 ± 6.63 kg) were evaluated based on their hand/wrist injury history, categorizing them into those with an injury history (IH; n,17) and non-injury history (NIH; n,13). Various assessments included body composition, hand grip strength, hand length, and ultrasonography, applying a validated tool (Michigan Hand Outcomes Questionnaire). Ultrasound measurements showed that the IH group had thicker cartilage than the NIH group in the index, ring, and little fingers, indicating the need for improved ergonomics in cockpit design and enhanced training protocols to mitigate injury risks among pilots.
Similar content being viewed by others


Introduction
Understanding the effects of mechanical loading and physical activity on articular cartilage has drawn increasing interest in recent years. This interest is primarily driven by evidence that excessive or abnormal joint loading elevates the risk of developing osteoarthritis, whereas moderate levels of exercise are beneficial for maintaining joint health1. Articular cartilage, a thin connective tissue at the ends of long bones, possesses viscoelastic properties essential for absorbing shocks and evenly distributing mechanical loads2,3. Previous studies have reported that athletes participating in high-impact and load-intensive sports, such as weightlifting and volleyball, exhibit increased metacarpal cartilage thickness4. However, comparable research on military populations, particularly Air Force cadets facing unique mechanical demands, remains scarce.
Air Force pilots, similar to athletes, engage in physically demanding activities. Pilots regularly perform resistance training to counteract the effects of gravitational acceleration, dedicating significant effort in maintaining skeletal muscle mass5. However, the most critical aspect of a pilot’s physical activity is operating the aircraft, which relies heavily on hand function. Previous research has shown that hand grip strength and the structural features of the hand (e.g., palm width and finger length) play pivotal roles in flight control accuracy and endurance6. Consequently, pilots may risk joint deformation due to intensive physical activity and repetitive mechanical demands. Assessing hand function and structural characteristics is particularly important for populations such as cadets at the Air Force Academy who routinely perform tasks requiring precise manual control of flight systems. Furthermore, understanding the subtle variations in hand function could inform strategies to enhance performance, improve grip mechanics, and reduce the risk of injuries. While studies on athletes have provided insights into cartilage adaptations to mechanical stress, similar investigations in military populations, particularly Air Force cadets, are limited. This study addresses this gap by exploring this specific group’s unique mechanical and functional demands.
Ultrasonography has emerged as a reliable tool for assessing joint cartilage owing to its noninvasive nature, absence of ionizing radiation, and capacity to provide real-time evaluations. It is particularly effective in measuring cartilage thickness in various joints, including the metacarpophalangeal joints4. The current study used ultrasonography to obtain precise measurements of the metacarpal cartilage thickness, which were complemented by assessments of functional outcomes, including grip strength and hand dexterity. Additionally, the participants completed the Michigan Hand Outcomes Questionnaire (MHQ), which provided valuable insights into self-reported hand function.
This study aimed to expand upon existing research by focusing on a novel population of cadets at the Air Force Academy who face unique mechanical demands on their hands. Through this investigation, we sought to provide comprehensive insights into the structural and functional adaptations of the hands in response to the rigorous training. Ultimately, the findings of this study will provide meaningful guidance for designing targeted training protocols and ergonomic interventions to improve hand function and reduce the risk of cartilage-related injuries in Air Force Academy cadets.
Results
Participants’ demographic characteristics and MHQ scores
Table 1 summarizes the participants’ demographic characteristics and MHQ scores based on their injury history. The analysis using an independent sample t-test revealed a statistically significant difference in the reported hand pain between the injury history (IH; n,17) and non-injury history (NIH; n,13) groups (p = 0.033). No statistically significant differences were observed in the other factors, including hand function, work performance, activities of daily living, aesthetics, or patient satisfaction.
Hand morphological structures and features
Independent and paired sample t-tests were used for ultrasonography analysis. Ultrasonography findings revealed that the mean cartilage thicknesses on the second, third, fourth, and fifth fingers of the dominant hand in the IH group were 0.38 ± 0.05 mm, 0.36 ± 0.05 mm, 0.37 ± 0.05 mm, and 0.39 ± 0.09 mm, respectively. The corresponding values for the non-dominant hand were 0.39 ± 0.08 mm, 0.37 ± 0.07 mm, 0.36 ± 0.09 mm, and 0.37 ± 0.06 mm, respectively. Ultrasonography showed that the average cartilage thicknesses for the second, third, fourth, and fifth fingers of the dominant hand in the NIH group were 0.31 ± 0.03 mm, 0.33 ± 0.06 mm, 0.31 ± 0.05 mm, and 0.32 ± 0.06 mm, respectively. The corresponding measurements in the non-dominant hand were 0.32 ± 0.05 mm, 0.32 ± 0.05 mm, 0.35 ± 0.08 mm, and 0.34 ± 0.10 mm, respectively. When comparing ultrasound measurements based on injury history, participants in the IH group exhibited thicker cartilage than those in the NIH group across all digits. Statistically significant differences were observed for the index (D2, p < 0.001), ring (D4, p = 0.011), and little fingers (D5, p = 0.012). (Fig. 1).

Analysis includes: (A) index finger; (B) middle finger; (C) ring finger; and (D) little finger. Solid and patterned bars represent findings for the right and left hands, respectively. Categories: 1, injury history; 2, non-injury history.
For the dominant hand in the IH group, the hand grip strength (HG) was 43.34 ± 5.66, total length was 18.49 ± 0.50, and width was 8.87 ± 0.43, and for the non-dominant hand, the HG was 41.61 ± 6.19, total length was 18.51 ± 0.57, and width was 8.83 ± 0.42. For the dominant hand in the NIH group, the HG was 45.15 ± 6.63, total length was 18.28 ± 1.04, and width was 8.71 ± 0.70, and for the non-dominant hand, the HG was 42.02 ± 5.63, total length was 18.21 ± 0.95, and width was 8.79 ± 0.70. The NIH group showed higher measurements for HG in both hands; however, the difference was not statistically significant. Also, the IH group demonstrated a longer overall hand length than the NIH group; however, the difference was not statistically significant (Fig. 2).

Analysis includes: (A) full hand length; (B) total hand width; (C) thumb; (D) index finger; (E) middle finger; (F) ring finger; (G) little finger. Solid bars represent measurements from the right hand, while patterned bars represent measurements from the left hand. Categories: 1, injury history; 2, non-injury history.
Correlation analysis with regression variables
Table 2 presents the results of the hierarchical regression analysis examining the relationship between injury history and measurement variables. Model 1 included only the dynamometer measurements (F = 4.240, p = 0.004), whereas Model 2 included the dynamometer measurements and MHQ scores as independent variables (F = 2.456, p = 0.047). In Model 1, the dominant hand’s index finger (D2) showed statistical significance (B = −5.664; β = −0.630; t = −3.608; p = 0.002). Similarly, in Model 2, D2 remained statistically significant (B = −5.112; β = −0.569; t = −2.683; p = 0.017). The Durbin-Watson statistic for the models was 0.827, and all variables had variance inflation factor (VIF) values below 5, except for non-dominant HG.0
Finally, the correlation analysis revealed statistically significant relationships between injury history and the cartilage thickness of several digits: D2 (p < 0.001), D4 (p = 0.011), D5 (p = 0.017), and the index finger of the non-dominant hand (N2, p = 0.009). The strongest correlation was observed for D2 (Table 3).
Discussion
The National Aeronautics and Space Administration reported that hand dimensions such as hand width and finger length significantly affect the control range and force transmission required during aircraft operations7. Aircraft controls are highly complex mechanical devices that require precise pilot management to ensure safe and effective operation. Ergonomically designed interfaces such as sticks and throttles are crucial to minimize pilot fatigue and facilitate seamless manipulation during flight8. These design principles are further reinforced by standards such as MIL-STD-1472G by the United States (US) Department of Defense and the Federal Aviation Administration Human Factors Design Standard, emphasizing the importance of adjustable and ergonomically optimized controls8,9. These controls must accommodate various anthropometric profiles to support diverse pilot populations and maintain operational efficiency. Additionally, a study by Wagner et al. revealed that hand force increases under stress10, suggesting its potential utility as a non-invasive workload indicator for pilots during flight operations. These studies underscore the importance of integrating ergonomic considerations into cockpit design to enhance pilot performance and flight safety.
Even in aircraft, which epitomize the latest technological advancements, ergonomics plays a critical role. However, the human body undergoes continuous changes owing to significant stimuli, prolonged use, and injury. Cartilage properties allow the absorption of shocks and impacts during movement, protect the underlying bone structures, and facilitate the smooth transmission of mechanical loads across joints, helping to distribute pressure evenly3. Additionally, this viscoelasticity aids joint lubrication, reduces bone friction, and enables fluid and pain-free movement11,12. However, prolonged exposure to high exercise volume or intensity can compromise the articular cartilage’s structural and functional integrity, potentially leading to joint degeneration13. Continuous mechanical loading causes fluid exudation from the cartilage, leading to morphological changes14,15. In particular, the hand is highly susceptible to deformation, and such changes can potentially impact its external structure and functional capabilities. Our findings revealed that participants in the IH group reported significantly greater hand pain and showed thicker cartilage in specific fingers than their counterparts in the NIH group. According to this study, the participants, although the absolute difference in articular cartilage thickness is only 0.5–2.0 mm, such variation is proportionally large in the small joints of the hand and wrist, where cartilage typically measures 0.3–1.0 mm and is associated with pain through joint-space narrowing and cartilage damage16. Moreover, sustained loading produces time-dependent deformation that can further compromise the tissue.
In addition, correlation analysis showed an association between IH and cartilage thickness. The correlation between the injury history and cartilage thickness, particularly in the index, ring, and little fingers, highlights the potential impact of repeated mechanical stress or trauma on the structural integrity of the hand. While transient cartilage thickening may occur as a short-term physiological response, repeated mechanical loading and injury-related stress may also induce more permanent adaptive remodeling or structural changes13,14,15. Although the ultrasound protocol in this study was rigorously standardized to minimize probe-related variability, these findings should still be interpreted as indicative rather than definitive, as functional consequences were not directly assessed in this cohort. This aligns with the findings of Möller et al., who demonstrated that ultrasonography is a sensitive and practical method for assessing cartilage thickness in finger joints. However, they also emphasized the need for consistent probe positioning and minimal transducer pressure to reduce inter-operator variability, underscoring the importance of protocol standardization for reliable interpretation of subtle cartilage changes17. Such structural changes could potentially influence a pilot’s ability to manage the nuanced controls required for modern aircraft operations, warranting further investigation in operational settings.
Furthermore, this study represents a pioneering effort to provide comprehensive anthropometric data for Asian pilots, particularly regarding hand dimensions and morphologies. Prior research has predominantly focused on Western populations, leaving a gap in ergonomic designs tailored to other groups. This study addresses this disparity. Although we found no significant differences in hand size and grip strength, according to the injury history in our research, by documenting hand size, finger length, and related metrics, we established a baseline for designing more inclusive cockpit interfaces that align with the needs of diverse pilot populations. These findings reinforce the necessity for continuous monitoring of grip strength and application of anthropometric data in cockpit design, as noted in earlier studies10.
Our findings will broaden the applicability of advanced evaluation tools that utilize technologies from the Fourth Industrial Revolution. Incorporating artificial intelligence (AI) and virtual reality (VR) into pilot assessment systems can provide real-time monitoring of hand movements and forces applied to the control interfaces. The US Air Force’s Pilot Training Next (PTN) program demonstrates how VR and AI-driven environments can tailor pilot instructions to individual skill levels and physical attributes, optimizing training efficiency and outcomes18. By continuously tracking pilot performance data, the PTN can deliver immediate feedback and adapt training modules to address specific weaknesses, ultimately reducing flight training time and cost.
When combined with biological metrics such as cartilage thickness, hand dimensions, and electromyography data, these technologies would enable a deeper analysis of hand biomechanics. For example, by integrating injury history and real-time hand stress measurements into AI-driven training simulators, the system can automatically adjust scenarios or control resistance for pilots with particular physical constraints, such as thicker cartilage or reduced grip strength. Such tools can inform the development of ergonomic cockpit interfaces, optimize pilot training programs, and enhance overall performance evaluations. While this study establishes a valuable baseline for understanding hand morphology and cartilage status in cadet pilots, its direct implications for operational performance remain to be validated. The observed differences in cartilage thickness, although statistically significant, require further exploration in the context of active-duty pilots and real-time performance metrics to determine their true functional relevance.
Nonetheless, these early findings underscore the critical need to build a comprehensive database encompassing hand dimensions, cartilage health, and functional capabilities, particularly for Asian pilots. Such data would serve as a foundational resource to optimize ergonomic cockpit design, refine anthropometry-based control systems, and tailor pilot training protocols based on individual morphological and biomechanical characteristics. When integrated into next-generation programs such as the U.S. Air Force’s PTN, these insights can help align AI- and VR-assisted flight training systems with real-world physical conditions. Additionally, applying these findings can extend the design of pilot-specific training regimens and performance evaluation systems that integrate biometric and biomechanical data to ensure optimal flight outcomes.
This study had the following limitations. First, the data on active pilots could not be obtained because the study was conducted using a population of cadets who were pilot trainees. In addition, our methods were limited in the ability to “prove” the pilot’s hand structure and ability to control. Therefore, follow-up studies are needed to establish the relationship between controller control and the morphological structure of the hand on active pilots.
Methods
Study participants’ details
Thirty male cadets from the Air Force Academy were recruited for the study. Participants, representing 90% of the Air Force cadet population, were fourth-year students with an average age of 23.14 ± 0.51 years, average height of 174.07 ± 3.14 cm, and average weight of 70.20 ± 6.63 kg. Participants were grouped into two categories based on their history of hand or wrist injuries: IH and NIH. Before each examination, the participants received a detailed explanation of the study’s objectives, methodology, and potential risks. They were informed of their right to withdraw from the study at any time without any consequences, and written informed consent was obtained from all participants. The study protocol was approved by the Institutional Bioethics Committee of Gachon University (approval date: November 28, 2024; approval number: 1044396-202410-HR-169-01) and adhered to the principles outlined in the Declaration of Helsinki.
Method details
The MHQ, a validated tool, was used to comprehensively assess the hand function. The MHQ evaluates six domains of hand performance: activities of daily living, pain, work performance, overall hand function, aesthetics, and patient satisfaction. The participants independently completed the questionnaire and responded based on their experience and typical hand usage.
Hand length measurements included assessment of the length of each finger, as well as the total hand length and width. HG was assessed using a grip device. Participants were instructed to hold the device with two fingers, keep their arms straight, and maintain a 15-degree angle between their torso and arms. Each participant performed three trials for both the dominant and non-dominant hands, with a sufficient rest period between trials to prevent fatigue. They then applied maximum force to the device and maintained the grip for five seconds. The highest value, measured at the nearest 0.1 kg, was recorded as the maximum grip strength of each hand9. This protocol ensured a safe and reliable representation of the maximal grip strength of each participant.
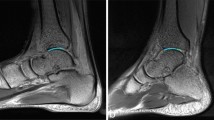
Ultrasonography was used to measure the cartilage thickness of the metacarpal heads of the second, third, fourth, and fifth digits. All measurements were performed using a high-frequency linear array transducer (SONON 500 L; Healcerion Co., Ltd., Seoul, South Korea) with a frequency range of 6–12 MHz. Participants were seated comfortably with the hand resting on a flat surface and the fingers gently flexed into a loose fist. The transducer was oriented longitudinally over each metacarpal head with no direct pressure applied to the cartilage surface. A generous amount of coupling gel was used to ensure full acoustic contact and to eliminate transducer compression artifacts. The transducer was maintained in a hover position slightly elevated above the skin to prevent deformation of the underlying tissue, while the probe angle was kept perpendicular to the cartilage surface to avoid anisotropic distortion. An experienced musculoskeletal ultrasound researcher in the field performed all imaging. The sonographer was blinded to the participants’ injury history during the measurement process to minimize bias. To enhance reliability, each site was scanned three times, and the mean value was used for analysis. The measurement sites were first localized by palpation of the metacarpophalangeal joints. Cartilage thickness was measured at the central point of the hypoechoic band corresponding to the hyaline cartilage layer, using ImageJ software (National Institutes of Health, Bethesda, MD, USA) (Fig. 3).

Ultrasonography image showing the measurement of the metacarpal cartilage thickness, accompanied by a photograph illustrating the correct positioning of the ultrasound transducer.
Statistical analysis
Data management and statistical analyses were conducted from September 1–30, 2024. Descriptive statistics (means and standard deviations) were computed in SPSS v28 (IBM Corp., Armonk, NY, USA). Between-group differences by injury history and right–left imbalance were evaluated using independent-samples t-tests and within-participant contrasts using paired-samples t-tests. Hierarchical multiple regression modeled associations among injury history, cartilage thickness, and MHQ, with model adequacy evaluated via R² and adjusted R², the Durbin–Watson statistic, and multicollinearity diagnostics (variance inflation factors, VIFs). VIFs were used to identify multicollinearity and to support the stability and interpretability of estimates. Pearson correlations quantified bivariate associations; the strength of r was classified as very weak (<0.10), weak (0.10–0.29), moderate (0.30–0.49), strong (0.50–0.69), very strong (0.70–0.89), and almost perfect (≥0.90). Statistical significance was set at p < 0.05.
Data availability
All data reported in this paper will be shared by the corresponding author upon request. The study did not generate new, unique reagents. Any additional information required to reanalyze the data reported in this paper is available from the corresponding author upon reasonable request (Jun-Young Sung, PhD [sjy7067@gmail.com]).
References
Tiderius, C. J., Svensson, J., Leander, P., Ola, T. & Dahlberg, L. dGEMRIC (delayed gadolinium-enhanced MRI of cartilage) indicates adaptive capacity of human knee cartilage. Magn. Reson. Med. 51, 286–290 (2004).
Fox, A. J. S., Bedi, A. & Rodeo, S. A. The basic science of articular cartilage: structure, composition, and function. Sports Health 1, 461–468 (2009).
Adam, C., Eckstein, F., MILZ, S. & Putz, R. The distribution of cartilage thickness within the joints of the lower limb of elderly individuals. J. Anat. 193, 203–214 (1998).
İskender, Ö et al. Ultrasonographic evaluation of the metacarpal cartilage thicknesses in weightlifters and volleyball players. Am. J. Phys. Med. Rehabil. 101, 1026–1030 (2022).
Sung, J.-Y. & Lee, K.-L. Physical strength, body composition, and G-test results of air force cadets based on nutrition knowledge differences. Sci. Rep. 14, 3083 (2024).
Department of Defense. MIL-STD-1472G: Department of Defense Design Criteria Standard – Human Engineering;http://everyspec.com/MIL-STD/MIL-STD-1400-1499/MIL-STD-1472G_39997/ 2012.
Publication, N. R. Anthropometric Volume Source Book Bibliography III: Annotated of Anthropometry. 136, NASA-RP-1024–3 (NASA, 1978). https://ntrs.nasa.gov/.
Federal Aviation Administration. Human factors design standard (HF-STD-001);https://www.hf.faa.gov/hfds/ 2018.
National physical strength awards; 2024. https://nfa.kspo.or.kr/reserve/4/selectMeasureItemListByAgeSe.kspo/. Accessed 30 Dec (2024).
Wagner, M., Sahar, Y., Elbaum, T., Botzer, A. & Berliner, E. Grip force as a measure of stress in aviation. Int. J. Aviat. Psychol. 25, 157–170 (2015).
Brody, L. T. Knee osteoarthritis: clinical connections to articular cartilage structure and function. Phys. Ther. Sport. 16, 301–316 (2015).
McNary, S. M., Athanasiou, K. A. & Reddi, A. H. Engineering lubrication in articular cartilage. Tissue Eng. (Part B Rev). 18, 88–100 (2011).
Eckstein, F., Hudelmaier, M. & Putz, R. The effects of exercise on human articular cartilage. J. Anat. 208, 491–512 (2006).
Bini, R. R. & Bini, A. F. Effects of exercise mode in knee cartilage thickness. J. Bodyw. Mov. Ther. 24, 490–495 (2020).
Halonen, K. S. et al. Deformation of articular cartilage during static loading of a knee joint – Experimental and finite element analysis. J. Biomech. 47, 2467–2474 (2014).
Saltzherr, M. S. et al. Cartilage evaluation in finger joints in healthy controls and early hand osteoarthritis patients using high-resolution MRI. Osteoarthr. Cartil. 27, 1148–1151 (2018).
Möller, I. et al. Ultrasound in the study and monitoring of osteoarthritis. Osteoarthr. Cartil. 17, S23–S28 (2009).
Forrest, N. C., Hill, R. R. & Jenkins, P. R. An Air Force pilot training recommendation system using advanced analytical methods. INFORMS J. Appl. Anal. 52, 198–209 (2021).
Acknowledgements
We would like to thank the Korean Air Force cadets who participated in the study and the officials who cooperated in the research. This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2024S1A5C3A01043381).
Author information
Authors and Affiliations
Contributions
K.K.L. and G.M.J. performed overall planning of the research, data acquisition, creation of key results, analysis and interpretation, and major drafting and revision of the manuscript submission. J.Y.S. performed data acquisition, analysis, and interpretation, overall organization, and direct supervision of the research.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lee, KL., Jeong, G.M. & Sung, JY. Morphological perspective of ergonomic implications of hand function and cartilage thickness in Air Force cadets. npj Microgravity 11, 86 (2025). https://doi.org/10.1038/s41526-025-00549-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41526-025-00549-x
