
Abstract
Little is known about the prevalence of chronic kidney disease (CKD) during the coronavirus disease 2019 (COVID-19) pandemic. We aimed to investigate the long-term trends in CKD prevalence from South Korea including the early pandemic. We used data from 108,152 Korean adults from 2007 to 2020 obtained from a representative longitudinal serial study. We defined CKD as a condition when the participant’s estimated glomerular filtration rate was < 60 mL/min/1.73 m2, or one-time spot proteinuria was ≥ 1 +, and then examined the overall trends in the prevalence of CKD. Among the included adults (n = 80,010), the overall national prevalence of CKD was 6.2%. The trend slope gradually increased from 2007 to 2019, however, there was a sudden decrease in 2020 (2007–2010, 5.1% [95% confidence interval (CI) 4.7–5.5]; 2017–2019, 7.1% [95% CI 6.6–7.6]; pandemic period, 6.5% [95% CI 5.7–7.3]; and βdiff, − 0.19; 95% CI − 0.24 to − 0.13). The prevalence of CKD among younger adults and those with poor medical utilization significantly decreased during the early pandemic. This study was the first large-scale study to investigate the longitudinal prevalence of CKD from 2007 to 2020. Further research is needed to fully understand the exact causes for this decline and to identify healthcare policy strategies for preventing and managing CKD.
Similar content being viewed by others

Introduction
The coronavirus disease 2019 (COVID-19) pandemic has significantly impacted socioeconomic conditions worldwide1. However, it is unknown whether the pandemic has had an impact on the prevalence of chronic kidney disease (CKD) in the general population2. Importantly, the belief that in-person outpatient clinic visits propagated the spread of COVID-19 had an impact on the number of outpatient clinic visits3. As the COVID-19 pandemic still has an impact on healthcare worldwide, identification of disadvantaged populations potentially limiting access to the best medical treatment is needed.
Chronic kidney disease (CKD) is a long-term condition associated with a high risk of death and is also connected to excess healthcare expenditure at advanced stages, and can ultimately require renal replacement therapy (RRT)4. CKD is a global public health problem, affecting 6.8–14.4% of the population across different countries5. The prevalence of CKD is known to increase with increasing prevalence of hypertension, diabetes, and obesity6,7. Unfortunately, CKD is clinically silent and asymptomatic until the later stages, and thus, many patients unaware of CKD prior to end stage of the condition8,9. Therefore, optimal screening via hospitals or workplaces and evidence-based management are critical to attenuate CKD progression and lower associated risks of end-stage kidney disease (ESKD) and mortality8,10. However, there is a lack of research on the prevalence of CKD during the COVID-19 pandemic. Therefore, it is necessary to conduct a long-term trend analysis based on the differences in CKD observed over before and during early stages of the COVID-19 pandemic.
Thus, the aim of this study was to evaluate the long-term nationwide prevalence of CKD among different subgroups including sociodemographic information, health-related lifestyle, and various medical conditions using nationally representative data from South Korea. Additionally, we assessed pandemic-related changes in the prevalence of CKD to examine whether the estimated prevalence of CKD in the early period of the pandemic differed from the expected level by comparing trends in the prevalence of the disease during the pre-pandemic (2007–2019) and early pandemic periods (2020).
Methods
Study population and design
This study utilized data from the Korea National Health and Nutrition Examination Survey (KNHANES) spanning from 2007 to 2020. KNHANES is a population-based nationwide longitudinal serial study that follows a multistage clustered design based on a stratified, multistage probability sampling scheme conducted by the Korea Disease Control and Prevention Agency (KDCA) for public interest11,12. In 2007, the frequency of the KNHANES has been modified from once every three years to every year in order to provide more timely statistics and diminish seasonal differences. Health interviews and examinations were conducted over 3 days in 192 primary sampling units across the country using the mobile examination center, consisting of two KNHANES-exclusive trucks12. Trained investigators performed all health examinations using validated methods and instruments calibrated periodically. This study was conducted in compliance with the ethical standards of relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects were approved by both the KDCA and Sejong University (SJU-HR-E-2020–003) institutional review board, and all anonymous participants signed a written informed consent form.
Assessment of covariates and ascertainment of CKD
Sociodemographic information (age, sex, region, education, household income, and body mass index [BMI]), health-related lifestyle (smoking status), and various medical conditions were queried or self-reported. BMI (kg/m2) was calculated by dividing body weight (kg) by the square of height (m), and laboratory test results from blood and urine samples, including kidney function, were collected. The laboratory result data quality control program monitored the performance of all analytical values to meet the standard target of accuracy12. Medical conditions were applicable when participants self-reported diabetes mellitus, hypertension, dyslipidemia, myocardial infarction or ischemic heart disease, gastrointestinal malignancies, lung cancer, breast cancer, or uterine and cervical cancers. We classified residential areas into large cities and rural areas, including small- and medium-sized cities11,13. Educational level was divided into three categories: middle school or lower, high school, and college or higher14. Household income was categorized into quartiles: low, lower-middle, higher-middle, and high income. BMI was subdivided into three categories: underweight or normal BMI (< 23.0 kg/m2), overweight (23.0–25.0 kg/m2), and obese (≥ 25.0 kg/m2) with respect to Asia–Pacific BMI15,16. Current smoking was defined as smoking at least once within the last 30 days. Kidney function was assessed via estimated glomerular filtration rate (eGFR), calculated using the Chronic Kidney Disease Epidemiology Collaboration equation17. We defined CKD as a condition when the eGFR of the participant was lower than 60 mL/min/1.73 m2, one-time spot proteinuria was ≥ 1 + on a urine dipstick test according to Kidney Disease: Improving Global Outcomes practice guidelines18.
Statistical analyses
KNHANES data analysis was performed between 2007 and 2020 following the protocol for a clustered, multi-stage, stratified sampling design to ensure a representative sample in Korea11. At first, we examined the overall trends in CKD during the study period (2007–2020) along with the age-standardized prevalence in overall CKD. The pre-pandemic period of the KNHANES cycle was set for four consecutive periods (2007–2010, 2011–2013, 2014–2016, and 2017–2019) to stabilize the data19. All analyses were stratified for the following baseline covariates: age, sex, residential area (urban and rural), educational level (middle school or lower, high school, and college or higher), household income (low, lower-middle, higher-middle, and high), BMI group (underweight or normal BMI, overweight, and obese), current smoking, outpatient clinic use within two weeks of the time of the survey, and medical condition (diabetes mellitus, hypertension, dyslipidemia, myocardial infarction or ischemic heart disease, gastrointestinal malignancies, lung cancer, breast cancer, or uterine and cervical cancer).
The baseline characteristics of the study participants were analyzed as weighted means with 95% confidence intervals (CIs) and frequencies with weighted proportions. We conducted a weighted complex sampling analysis using linear and logistic regression models. The trend difference was derived from the difference between β-coefficients before and after the pandemic to understand the trend of change in the prevalence of CKD during the entire period (2007–2020). The odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using logistic regression models comparing the prevalence of CKD from 2007 to 2019 with 2020. Our next endpoint was whether the trends in the prevalence of CKD differed between the population who visited the outpatient clinic and those who did not visit the in-person clinic during the early COVID-19 pandemic era. All analyses were performed using SAS version 9.4 (SAS Inc., Cary, NC, USA)20,21. Statistical significance was defined as a two-sided P-value less than 0.05.
Results
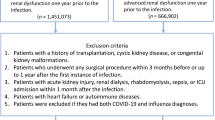
Of the subjects participating in the KNHANES 2007–2020 (total N = 108,152), we excluded those who (1) were under 19 years of age (excluded N = 23,889); (2) had missing data on covariates (e.g., household income) included in the multivariable model (excluded N = 909); and (3) did not have data for CKD ascertainment based on eGFR or proteinuria (excluded N = 3344). Thus, the final number of subjects for the analysis was 80,010.
Table 1 shows the general characteristics of the study participants. CKD accounted for 6.2% (unweighted n = 6105) adults of the total subjects, with 51.8% being females. A total of 50.0% (95% CI 48.3–51.6) of CKD group was 65 years or older, compared to 12.8% (95% CI 12.4–13.2) of the non-CKD group. The proportion of subjects with CKD in rural areas was higher than in those without CKD. The lower educational attainment group and the low quartile of household income group with CKD showed a higher proportion than those without CKD.
Trends of prevalence in patients with CKD
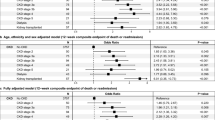
The prevalence of CKD in adults was examined using KNHANES data over 14 years in subgroups according to sex, area of residence, education level, household income, BMI, current smoking status, outpatient clinic use, and medical conditions. The slope gradually increased from 2007 to 2019; however, there was a sudden decrease in 2020, as shown in Fig. 1. The weighted prevalence of CKD increased from 5.1% (95% CI 4.7–5.5) in 2007–2010 to 7.1% (95% CI 6.6–7.6) from 2017 to 2019, and then decreased to 6.5% (95% CI 5.7–7.3) in 2020 (Table 2). Similarly, the age-standardized prevalence of CKD increased from 4.0% (95% CI 3.7–4.3) in 2007–2010 to 6.3% (95% CI 5.6–7.1) from 2017 to 2019, and then decreased to 5.0% (95% CI 4.1–6.0) in 2020 (Table 2). The downward slope during the early COVID-19 period presented a consistent tendency in subgroups by age (19–64 years [βdiff, − 0.27; 95% CI − 0.34 to − 0.19]), sex (male [βdiff, − 0.20; 95% CI − 0.28 to − 0.13] and female [βdiff, − 0.18; 95% CI − 0.25 to − 0.11]), residential area (urban [βdiff, − 0.15; 95% CI − 0.24 to − 0.07] and rural [βdiff, − 0.21; 95% CI − 0.29 to − 0.14]), educational attainment (middle school or lower [βdiff, − 0.09; 95% CI − 0.16 to − 0.02], high school [βdiff, − 0.27; 95% CI − 0.37 to − 0.17], and college or higher [βdiff, − 0.39; 95% CI − 0.50 to − 0.29]), household income (low [βdiff, − 0.24; 95% CI − 0.34 to − 0.15], lower-middle [βdiff, − 0.22; 95% CI − 0.32 to − 0.11], higher-middle [βdiff, − 0.17; 95% CI − 0.28 to − 0.07], and high [βdiff, − 0.10; 95% CI − 0.21–0.00, P < 0.05]), BMI group (underweight or normal [βdiff, − 0.20; 95% CI − 0.28 to − 0.12], overweight [βdiff, − 0.13; 95% CI − 0.23 to − 0.03], and obese [βdiff, − 0.20; 95% CI − 0.29 to − 0.12]), current smoking status (no [βdiff, − 0.20; 95% CI − 0.26 to − 0.13], yes [βdiff, − 0.17; 95% CI − 0.25 to − 0.09]), and medical conditions (those without [βdiff, − 0.26; 95% CI − 0.34 to − 0.18], those with [βdiff, − 0.07; 95% CI − 0.13–0.00, P < 0.05]).

Nationwide 14-year trends and prevalence of CKD among Korean adults, 2007–2020 (n = 80,010).
Although we compared trends before and during the early stage of COVID-19 pandemic, there was no significant difference in the slopes of the older adult and outpatient clinic visit groups. The odds of CKD in females decreased during the early COVID-19 pandemic from 2007 to 2019 (OR 0.75; 95% CI 0.63–0.89).
Differences in prevalence trends in patients with chronic kidney disease according to outpatient clinic visits
The prevalence of CKD in participants who did not visit the outpatient clinic within 2 weeks is presented in Table 3. Similar to the results in Table 2, the prevalence of participants without outpatient clinic visits increased until 2019 but stagnated in 2020 in most subgroups. In Table 3, the overall β values were positive in the pre-pandemic period and neutral in the early pandemic period, representing a statistically significant decrement in the trend difference of prevalence (βdiff, − 0.27; 95% CI − 0.33 to − 0.20). The increasing trend in the prevalence of CKD during the pre-pandemic period was consistent regardless of sex, residential area, educational attainment, household income, BMI group, current smoking status, and medical condition. Older adults showed no significant change in β both prior to and during the COVID-19 pandemic. Diminishing trends were observed in certain subgroups of participants during the early pandemic period: age 19 to 64 years, college or higher, and BMI ≥ 25.0 kg/m2. The βdiff in the prevalence of CKD in all subgroups without outpatient clinic utilization, except for older adults, were negative.
The trend of CKD prevalence in participants who used outpatient clinics within 2 weeks is presented in Table 4, including the prevalence for each subgroup. Overall, there was no significant difference in trend difference (βdiff, − 0.06; 95% CI − 0.15–0.03) and odds ratio (OR 0.83; 95% CI 0.66–1.05) before and at the beginning of the COVID-19 period. 19.4% (95% CI 17.2–21.7) of older adults satisfied the criteria for CKD in 2017–2019, and then only 15.0% (95% CI 11.4–18.6) accounted the for CKD population in 2020 (βdiff, − 0.08; 95% CI − 0.15–0.00; P < 0.05). βdiff were significantly negative in females (βdiff, − 0.12; 95% CI − 0.23 to − 0.01) and patients without current smoking (βdiff, − 0.18; 95% CI − 0.29 to − 0.07) with outpatient visits, respectively, and odds were also similar in females (OR 0.53; 95% CI 0.39–0.73) and those without current smoking (OR 0.47; 95% CI 0.34–0.65; Table 4). In participants with outpatient clinic use, the β of prevalence increased from 2007 to 2019 across educational levels, and a decline in βdiff was observed in those with middle school or lower (βdiff, − 0.12; 95% CI − 0.23 to − 0.01) and college or higher (βdiff, − 0.19; 95% CI − 0.38 to − 0.01), respectively. The odds for both high household income (OR 0.55; 95% CI 0.34–0.88) and underweight and normal weight (OR 0.64; 95% CI 0.45–0.91) were significantly low.
Discussion
This nationwide representative longitudinal serial study included a long-term trend analysis from 2007 to 2020. This is the first study to examine the 14-year trends in the prevalence of CKD, including the early period of COVID-19. Although the trends of both overall and age-standardized prevalence of CKD increased before the pandemic (2007–2019), the overall prevalence and age-standardized prevalence of CKD significantly decreased during the early pandemic (2020) in similar pattern. The overall trend of the prevalence of CKD in the early COVID-19 pandemic was not significantly different from that of CKD in the pre-pandemic period in older patients or patients who visited outpatient clinics. Interestingly, βdiff values of younger patients or those who did not visit the outpatient clinic were negative in the overall group.
To the best of our knowledge, this is the first study to investigate 14-year trends in the prevalence of CKD, including the early COVID-19 period, as a nationwide representative serial study. The increase in rates of overall prevalence of CKD became less steep before the outbreak of the COVID-19 pandemic in Japan, the UK, and the USA22,23,24. However, although the pre-pandemic prevalence of CKD in Korea was similar to that of the aforementioned countries, the prevalence of CKD during the COVID-19 pandemic has not yet been reported25,26.
Several possibilities exist for interpreting the remarkable decline in the prevalence of CKD, and this study observed different trends in the prevalence of CKD among different subgroups. At the time of early study design, our study predicted that outpatient clinic use would be one of the most distinct factors in the fluctuation in CKD prevalence during the early COVID-19 pandemic. In general, some people were repulsed by crowded places like hospitals or clinics at the beginning of the COVID-19 pandemic, and this study identified statistically significant difference in the prevalence of CKD on age and healthcare utilization in this society27. Additionally, considering that most countries, including South Korea, implemented a policy to telework during the COVID-19 pandemic (2020), many people stayed more inevitably at home than during the pre-pandemic era or were quarantined due to lockdown or strict social distancing28.
The changes in social life patterns since COVID-19 pandemic and the results of our study can be analyzed differently depending on the subgroup of each patient. Nevertheless, we have summarized the direction of the interpretation of this study results for several reasons. Many people may have avoided going to medical facilities for non-emergency conditions, including general outpatient visits and screening during the pandemic period27. This may have resulted in a decrease in the number of CKD cases detected during the pandemic, especially in vulnerable subgroups with low healthcare utilization early in the COVID-19 pandemic. However, this interpretation was not supported by the study design of our findings. This study used only two objective criteria of the CKD definition and maintained a standardized protocol that conducted health interviews and tests over 3 days in 192 primary sample units using the accompanying mobile test centers, which is itself a strength of the study. Therefore, this determined that the reduction in prevalence of CKD in our study is a substantial numerical change, and that a different direction of discussion is needed for this reduction.
Since the outbreak of the COVID-19 pandemic, it is possible that many individuals have made lifestyle changes, such as engaging in healthier eating habits, increased exercise, and stress reduction, which may have positively impacted kidney health and contributed to the decline in the prevalence of CKD29. Additionally, the pandemic may have influenced environmental factors, including air pollution and exposure to toxins, which could have also played a role in the decline of CKD prevalence30. On the other hand, these findings could be interpreted as a significant reduction in the prevalence of CKD in other groups, despite the fact that changes in lifestyle or environmental factors may not have had a significant impact on CKD prevalence among older individuals and those already receiving healthcare. However, as our study only included the early period of COVID-19 pandemic, it is premature to determine the contributing factors to the observed reduction. Therefore, it is essential to recognize that further research is needed to fully understand the exact causes for the decline in the prevalence of CKD during the early pandemic era.
Another possibility is that considerable number of deaths could have been the result of COVID-19 propagation among vulnerable group of patients who were approaching criteria for CKD died before a diagnosis of CKD. However, our result did not fit to this interpretation, because early explosive COVID-19 outbreak in Korea mainly focused on particular clusters such as churches in the city of Daegu and convalescent hospitals31. Due to strict social distancing and diagnostic test policies in Korea at the beginning of COVID-19 pandemic period (2020), mortality of COVID-19 was very low31. In that point of view, it is difficult to determine whether this significant decrease in the prevalence of CKD among young patients during the early pandemic period was directly caused by COVID-19 infection per se.
The strength of this study includes its national representative sampling design, including more than 80,000 adults, and the data examined from 2007 to 2020, including the early COVID-19 pandemic period. Through this dataset, we can interpret the nationwide longitudinal prevalence of CKD in Korea and understand the effect of the pandemic. This study had some limitations. First, there is a lack of evidence to conclude that the prevalence of CKD decreased during the COVID-19 pandemic because we included only the 1st year of the COVID-19 pandemic period (transitional zone). Considering the lockdown policy due to fear of new-onset airborne infection, not only the behavior of participants but also obligatory policies could be a greater factor when interpreting patterns of medical consumption in Korea. For instance, there are more opportunities for diverse physical activities than in 2020. Therefore, if nationwide data from 2021 are gathered, additional analysis of the prevalence of CKD needs to be conducted. Second, there may have been a possibility of selection bias. However, participants were encouraged to participate in KNHANES unless there were unavoidable circumstances preventing them from doing so. The response rates of the survey were 71.1% in 2019 and 71.3% in 2020, indicating that the impact of COVID-19 on response rates was negligible. Third, the two-week timeframe for outpatient visits may be a limitation of this study, as it may be too short to capture all outpatient visits. Unfortunately, additional analyses according to the duration of follow-up were not possible because the KNHANES questionnaire only includes outpatient visits within the past two weeks as a survey item, without other visit timeframes. While regular outpatient visits of chronic patients or outpatient clinic visits for a cold or fever could lead to misclassification bias, the overall interpretation of the study is not affected. Fourth, this study used a definition of CKD based on a single eGFR value check-up, which did not meet the accurate KDIGO criteria requiring at least two eGFR values measured at least 90 days apart. Lastly, we could not analyze races and ethnicities other than those of South Koreans. Hence, further research on the impact of the pandemic in other countries is needed.
This study indicated that the national prevalence of CKD before the pandemic increased; however, the prevalence during the early pandemic period significantly decreased through a long-term trend analysis among Korean adults. Interestingly, young adults and those with low medical utilization showed significantly decreased CKD prevalence during the early pandemic. This downward slope in the prevalence of CKD may be related with lifestyle modification and environmental factors as a positive impact of COVID-19 in specific population. It is important to investigate further, as understanding the factors that influence the prevalence of CKD can help to identify healthcare policy strategies to prevent and manage the condition.
Data availability
The authors of this study declare that all main data within the paper are available. All other data are available upon reasonable request to the corresponding authors.
References
Nicola, M. et al. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 78, 185–193. https://doi.org/10.1016/j.ijsu.2020.04.018 (2020).
Gu, X. et al. Association of acute kidney injury with 1-year outcome of kidney function in hospital survivors with COVID-19: A cohort study. EBioMedicine 76, 103817. https://doi.org/10.1016/j.ebiom.2022.103817 (2022).
Baum, A., Kaboli, P. J. & Schwartz, M. D. Reduced in-person and increased telehealth outpatient visits during the COVID-19 pandemic. Ann. Intern. Med. 174, 129–131. https://doi.org/10.7326/m20-3026 (2021).
Hu, E. A. et al. Adherence to healthy dietary patterns and risk of CKD progression and all-cause mortality: Findings from the CRIC (Chronic Renal Insufficiency Cohort) Study. Am. J. Kidney Dis. 77, 235–244. https://doi.org/10.1053/j.ajkd.2020.04.019 (2021).
Cockwell, P. & Fisher, L.-A. The global burden of chronic kidney disease. The Lancet 395, 662–664. https://doi.org/10.1016/S0140-6736(19)32977-0 (2020).
Brück, K. et al. CKD Prevalence Varies across the European General Population. J. Am. Soc. Nephrol. 27, 2135–2147. https://doi.org/10.1681/asn.2015050542 (2016).
Liyanage, T. et al. Prevalence of chronic kidney disease in Asia: A systematic review and analysis. BMJ Glob. Health https://doi.org/10.1136/bmjgh-2021-007525 (2022).
Chen, T. K., Knicely, D. H. & Grams, M. E. Chronic kidney disease diagnosis and management: A review. JAMA 322, 1294–1304. https://doi.org/10.1001/jama.2019.14745 (2019).
Xie, Y. et al. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 94, 567–581. https://doi.org/10.1016/j.kint.2018.04.011 (2018).
Rangaswami, J. et al. Cardiorenal protection with the newer antidiabetic agents in patients with diabetes and chronic kidney disease: A scientific statement from the American heart association. Circulation 142, e265–e286. https://doi.org/10.1161/cir.0000000000000920 (2020).
Koh, H. Y. et al. Serum heavy metal levels are associated with asthma, allergic rhinitis, atopic dermatitis, allergic multimorbidity, and airflow obstruction. J. Allergy Clin. Immunol. 7, 2912–2915. https://doi.org/10.1016/j.jaip.2019.05.015 (2019).
Kweon, S. et al. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 43, 69–77. https://doi.org/10.1093/ije/dyt228 (2014).
Lee, S. W. et al. Association between mental illness and COVID-19 in South Korea: A post-hoc analysis. The lancet. Psychiatry 8, 271–272. https://doi.org/10.1016/s2215-0366(21)00043-2 (2021).
Kim, M. J. et al. Trends in body mass index changes among Korean adolescents between 2005–2020, including the COVID-19 pandemic period: A national representative survey of one million adolescents. Eur. Rev. Med. Pharmacol. Sci. 26, 4082–4091. https://doi.org/10.26355/eurrev_202206_28978 (2022).
Tan, K. C. B. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. The Lancet 363, 157–163. https://doi.org/10.1016/S0140-6736(03)15268-3 (2004).
Organization, W. H. The Asia-Pacific perspective: Redefining obesity and its treatment. (2000).
Matsushita, K. et al. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA 307, 1941–1951 (2012).
Andrassy, K. M. Comments on ‘KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease’. Kidney Int. 84, 622–623 (2013).
Lee, K. H., Yon, D. K. & Suh, D. I. Prevalence of allergic diseases among Korean adolescents during the COVID-19 pandemic: Comparison with pre-COVID-19 11-year trends. Eur. Rev. Med. Pharmacol. Sci. 26, 2556–2568. https://doi.org/10.26355/eurrev_202204_28492 (2022).
Lee, S. W. Methods for testing statistical differences between groups in medical research: Statistical standard and guideline of Life Cycle Committee. Life Cycle 2, e1. https://doi.org/10.54724/lc.2022.e1 (2022).
Lee, S. W. Regression analysis for continuous independent variables in medical research: Statistical standard and guideline of Life Cycle Committee. Life Cycle 2, e3. https://doi.org/10.54724/lc.2022.e3 (2022).
Hounkpatin, H. O. et al. Prevalence of chronic kidney disease in adults in England: Comparison of nationally representative cross-sectional surveys from 2003 to 2016. BMJ Open 10, e038423. https://doi.org/10.1136/bmjopen-2020-038423 (2020).
Nagai, K., Asahi, K., Iseki, K. & Yamagata, K. Estimating the prevalence of definitive chronic kidney disease in the Japanese general population. Clin. Exp. Nephrol. 25, 885–892. https://doi.org/10.1007/s10157-021-02049-0 (2021).
Vart, P. et al. National trends in the prevalence of chronic kidney disease among racial/ethnic and socioeconomic status groups, 1988–2016. JAMA Netw. Open 3, e207932–e207932. https://doi.org/10.1001/jamanetworkopen.2020.7932 (2020).
Park, J. I., Baek, H. & Jung, H. H. Prevalence of chronic kidney disease in Korea: The Korean national health and nutritional examination survey 2011–2013. J. Korean Med. Sci. 31, 915–923. https://doi.org/10.3346/jkms.2016.31.6.915 (2016).
Shin, H. Y. & Kang, H. T. Recent trends in the prevalence of chronic kidney disease in Korean adults: Korean National Health and Nutrition Examination Survey from 1998 to 2013. J. Nephrol. 29, 799–807. https://doi.org/10.1007/s40620-016-0280-y (2016).
Kim, J., You, M. & Shon, C. Impact of the COVID-19 pandemic on unmet healthcare needs in Seoul, South Korea: A cross-sectional study. BMJ Open 11, e045845. https://doi.org/10.1136/bmjopen-2020-045845 (2021).
Ker, D., Montagnier, P. & Spiezia, V. Measuring telework in the COVID-19 pandemic. (2021). https://doi.org/10.1787/0a76109f-en
Kovesdy, C. P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 12, 7–11. https://doi.org/10.1016/j.kisu.2021.11.003 (2022).
Liang, Z. et al. Urbanization, ambient air pollution, and prevalence of chronic kidney disease: A nationwide cross-sectional study. Environ. Int. 156, 106752. https://doi.org/10.1016/j.envint.2021.106752 (2021).
Shim, E., Tariq, A., Choi, W., Lee, Y. & Chowell, G. Transmission potential and severity of COVID-19 in South Korea. Int. J. Infect. Dis. 93, 339–344. https://doi.org/10.1016/j.ijid.2020.03.031 (2020).
Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (NRF-2021R1A2C1012120).
Author information
Authors and Affiliations
Contributions
Dr D.K.Y. had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final version before submission. Study concept and design: D.K.Y.; Acquisition, analysis, or interpretation of data: S.-Y.Y., H.W.P., D.K.Y., and K.H.J.; Drafting of the manuscript: S.-Y.Y., D.K.Y., and K.H.J.; Critical revision of the manuscript for important intellectual content: all authors; Statistical analysis: S.-Y.Y., D.K.Y., and K.H.J.; Study supervision: D.K.Y. and K.H.J. D.K.Y. supervised the study and is guarantor for this study. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Corresponding authors
Ethics declarations
Competing interests
AnK has received consultancy fees from Vifor Pharma, Otsuka, Walden Biosciences, Catalyst Biosciences, and Delta 4. The funders had no role in study design, data collection, data analysis, data interpretation, or writing of the report. All the other authors declared no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yoon, SY., Park, H.W., Kim, H.J. et al. National trends in the prevalence of chronic kidney disease among Korean adults, 2007–2020. Sci Rep 13, 5831 (2023). https://doi.org/10.1038/s41598-023-33122-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-023-33122-1
This article is cited by
-
Global burden of anticancer drug-induced acute kidney injury and tubulointerstitial nephritis from 1967 to 2023
Scientific Reports (2024)
-
National trends in rheumatoid arthritis and osteoarthritis prevalence in South Korea, 1998–2021
Scientific Reports (2023)
