
Abstract
Variants in the retinitis pigmentosa GTPase regulator (RPGR) gene are responsible for the majority of X-linked retinitis pigmentosa cases, which not only affects male patients but also some heterozygous females. Vision-related disability and anxiety of patients with RPGR-associated retinal degeneration have never been explored before. This study aimed to evaluate self-reported visual function and vision-related anxiety in a Portuguese cohort of male and female patients with RPGR-associated retinal degeneration using two validated patient-reported outcome measures. Cross-sectional data of thirty-two genetically-tested patients was examined, including scores of the Michigan retinal degeneration questionnaire (MRDQ) and Michigan vision-related anxiety questionnaire. Patients were classified according to retinal phenotypes in males (M), females with male phenotype (FM), and females with radial or focal pattern. Both M and FM revealed higher rod-function and cone-function anxiety scores (p < 0.017). Most MRDQ disability scores were higher in M and FM (p < 0.004). Overall, positive correlations (p < 0.004) were found between every MRDQ domain and both anxiety scores. In RPGR-associated retinal degeneration, males and females with male phenotype show similar levels of increased vision-related anxiety and disability. Every MRDQ visual function domain showed a strong correlation with anxiety scores.
Similar content being viewed by others


Introduction
Retinitis pigmentosa (RP) encompasses a diverse group of inherited retinal disorders characterized initially by night blindness and visual field constriction due to the loss of rod photoreceptors1,2,3. As the disease progresses, cone photoreceptors deteriorate, typically resulting in the loss of color vision, contrast sensitivity, and central vision1,2,3. Retinitis pigmentosa stands as the most prevalent inherited retinal disease (IRD) globally, affecting an estimated 1 in 4000 individuals, and X-linked retinitis pigmentosa (XLRP) accounts for 5–15% of all cases2,4. It is one of the most severe forms of RP in males, with symptoms appearing in childhood and progressing rapidly to severe vision impairment by the fourth decade of life4. Clinically significant variants in the retinitis pigmentosa GTPase regulator (RPGR) gene are responsible for 70–80% of XLRP cases1. Despite the X-linked inheritance, heterozygous females of RPGR variants may display varying degrees of severity, often with significant inter-eye asymmetry5. This phenotypic heterogeneity is thought to stem from differences in the X chromosome inactivation ratio (X lyonization)4,6. Fundus autofluorescence (FAF) is a valuable imaging technique for identifying retinal mosaicism and classifying the disease into four patterns of increasing severity: normal, radial, focal and male pattern4. Additionally, visual function correlates with retinal phenotype on FAF, with patients showing normal, focal, or radial patterns more likely to retain good visual acuity5.
The approval of Voretigene neparvovec for RPE65-associated retinal degeneration has promoted research into treatments for other IRD7. Several clinical trials are underway, aiming to deliver a healthy RPGR gene copy using adeno-associated viral vectors8,9,10. Given the severity and prevalence of this condition, effective treatments are urgently needed to prevent, halt, or reverse disease progression7,9. Female carriers of RPGR variants, who may exhibit a severe male-like phenotype, could benefit from gene replacement therapies and should be equally considered for future therapeutic approaches, as has already happened in the phase 3 LUMEOS study (NCT04671433)5,9,11.
The inexorable vision impairment associated with IRD may profoundly impact a patient’s quality-of-life (QoL), leading to higher rates of depression and anxiety12,13. Studies have shown that vision-related anxiety correlates with disability in this population14. X-linked RP imposes a particularly heavy humanistic, economic and emotional burden due to its early onset and rapid progression to blindness12. Patient-reported outcome (PRO) measures play a crucial role in assessing treatment efficacy and understanding its association with patient-perceived treatment benefits in a standardized manner3,15,16. These clinical outcome assessments convey the patient’s viewpoint on the disease’s impact on their life, and which aspects of visual dysfunction affect their emotional well-being15,16.
The Michigan Retinal Degeneration Questionnaire (MRDQ) and the Michigan Vision-related Anxiety Questionnaire (MVAQ) are two psychometrically validated PRO measures specifically developed for IRD patients, which were translated and linguistically validated for usage in Portuguese-speaking countries17. The MRDQ captures subjective disability across several domains representative of physiological visual function pathways3,15. Meanwhile, the MVAQ provides insight into vision-related anxiety, assessing the contributions of both cone and rod systems separately16.
Patients’ QoL is one of the seven priorities of the 2021–2025 National Eye Institute (NEI) Strategic Plan18,19. The authors underline the importance of incorporating patient perspectives in clinical research studies using vision-related QoL assessments based on PRO measures18,19.
To our knowledge, neither vision-related disability and anxiety nor any potential differences between males and females with RPGR-associated retinal degeneration have been explored before. The purpose of this study was to evaluate self-reported visual function and vision-related anxiety in a Portuguese cohort of male and female patients with RPGR-associated retinal degeneration using two validated PRO measures.
Materials and methods
Study design and participants
Cross-sectional study conducted at an IRD referral center in Portugal. Male and female patients with genetically confirmed RPGR-associated retinal degeneration were identified using the IRD-PT registry (retina.com.pt)20.
Ethical statement
All patients provided written informed consent. The study was approved by the ethics committee of Coimbra University Hospital (protocol no GER/001/2016) and followed the tenets of the Declaration of Helsinki for biomedical research.
Measures
We collected clinical data such as demographics (age and sex) and genetic testing results. Genetic variants were classified according to the guidelines of the American College of Medical Genetics and Genomics (ACMG).
The Early Treatment of Diabetic Retinopathy Study (ETDRS) introduced the ETDRS chart as a standardized visual acuity testing chart. Best corrected visual acuity (BCVA) was recorded as ETDRS letter score in the better-seeing eye. We used BCVA in the better-seeing eye as a surrogate for central visual function since PRO measures typically reflect binocular vision and in cases where there is a difference between eyes, visual function is primarily determined by the eye with better sight.
Ultrawidefield fundus autofluorescence (UW-FAF) was used to classify retinal phenotype (Fig. 1): normal pattern, radial pattern (radial spoke–shaped reflexes extending from the central macular area in a radial pattern), focal pattern (focal pigmentary retinopathy patchy pigmentation with a radial reflex pattern), and male pattern4. We chose to include only the FAF phenotype of the better-seeing eye in our analysis based on the reasoning described above and the fact that a significant inter-eye asymmetry is not infrequent in heterozygous females15.

Retinal phenotype classification based on UW-FAF. (a) Radial pattern, (b) focal pattern, (c) male pattern.
The MRDQ and MVAQ were developed using item response theory, factor analysis, and graded response models3,13. MRDQ measures the impact of visual impairment in daily tasks, containing 59 Likert-scaled question items across seven different dimensions: central vision, color vision, contrast sensitivity, scotopic function, photopic peripheral vision, mesopic peripheral vision, and photosensitivity3,15. On the other hand, MVAQ is a 14-item instrument with two domains: rod-function related anxiety, which included items like worrying about bumping into people/objects or walking on uneven ground at night, and cone-function related anxiety, with items such as worrying when reading or distinguishing colors13,16. Item response theory analysis results in a theta score, which represents the functional ability or anxiety of a person in the measured domain3. Theta scores are mean-centered at zero and follow a normal distribution with variance of 13. They range between − 3 and + 3, where an increasing score indicates a higher severity in disability (MRDQ) or higher levels of anxiety (MVAQ)21. All participants completed the translated and linguistically validated Portuguese version of the Michigan Retinal Degeneration Questionnaire (MRDQ) and Michigan Vision-related Anxiety Questionnaire (MVAQ), where questions were read aloud by the interviewer, according to predefined guidelines17.
Statistical analysis
Data normality was visually assessed and analyzed with the Shapiro–Wilk test. Normal distributed data was presented as mean and standard deviation (SD), and non-normal distributed data was presented as median and interquartile range (IQR). Using Kruskal–Wallis test, we searched for differences in age, BCVA of the better-seeing eye and all MRDQ and MVAQ theta scores between three groups based on FAF phenotype: males (M), females with male phenotype (FM) and females with radial or focal pattern (FRF). When a significant difference was detected, pairwise comparison was performed. Additionally, Spearman’s rank correlation was used to quantify the association between MVAQ theta scores and other variables such as age, BCVA of the better-seeing eye and MRDQ domains. Adjusted p-values according to Bonferroni correction for multiple comparison testing are presented. P-values were deemed significant if less than 0.05. All statistical analyses were performed using R 4.2.1 software (R Foundation for Statistical Computing).
Results
Thirty-two patients (50% female) from 13 families with RPGR-associated retinal degeneration were included. The cohort’s clinical and demographic characteristics are shown in Table 1.
Genetic analysis yielded 12 distinct variants in the RPGR gene, 8 of which were located in the ORF15 region. The genetic landscape of our cohort is further described in the Supplementary Table S1.
As expected, BCVA of the better-seeing eye was significantly higher in the FRF group compared to males and females with a male phenotype. There was no difference in BCVA between M and FM (Table 2).
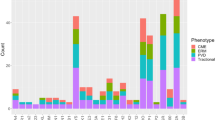
Males and females with male pattern presented higher MRDQ theta scores than the FRF group in central vision, color vision, contrast sensitivity, scotopic function, photopic and mesopic peripheral function domains (Table 2). There was no significant difference in theta scores between males and FM, except for the mesopic peripheral function domain, in which males revealed greater disability (median 0.999) than FM (median 0.014). Similarly, median MVAQ scores for rod- and cone-function related anxiety were equally higher in males and FM compared to FRF (Table 2). The distribution of MRDQ and MVAQ domain scores across the three groups are shown in Fig. 2.

Comparison of MRDQ and MVAQ scores between males, females with a male phenotype and females with a radial or focal pattern. Note: ACF = cone-function related anxiety, ARF = rod-function related anxiety, CNT = contrast sensitivity, COL = color vision, CV = central vision, FM = females with male phenotype, FRF = females with radial or focal pattern, M = males, MF = mesopic peripheral function, PF = photopic peripheral function, PS = photosensitivity, SF = scotopic function.
Regarding BCVA of the better-seeing eye, the higher the visual acuity, the lower the cone and rod anxiety thetas (Table 3). These negative correlations between BCVA and both rod- and cone-function anxiety scores are graphically depicted in Figs. 3 and 4, respectively.

Negative correlation between MVAQ rod-function anxiety and BCVA. Note: ARF = rod-function related anxiety, BCVA = best corrected visual acuity.

Negative correlation between MVAQ cone-function anxiety and BCVA. Note: ACF = cone-function related anxiety, BCVA = best corrected visual acuity.
Significant positive correlations between age and MRDQ scores related to central vision (r = 0.866; p < 0.0001), color vision (r = 0.585; p = 0.02), contrast sensitivity (r = 0.812; p = 0.0002), scotopic function (r = 0.769; p = 0.0008), photopic (r = 0.715; p = 0.003) and mesopic peripheral function (r = 0.737; p = 0.002) were found only in the male group. No significant correlations with age were observed in the FM or FRF groups.
Overall, positive correlations were found between every MRDQ domain and both rod- and cone-function related anxiety (Table 3). MRDQ mesopic peripheral function (r = 0.699; p < 0.0001) and scotopic function (r = 0.684; p < 0.0001) thetas had the strongest correlation with rod anxiety theta. MRDQ contrast sensitivity (r = 0.782; p < 0.0001) and central vision (r = 0.773; p < 0.0001) thetas had the strongest correlation with cone anxiety theta. Moreover, cone anxiety scores are positively correlated with concomitant rod anxiety scores and vice-versa (Table 3).
Discussion
By evaluating self-perceived vision-related disability and anxiety in both male and female patients, this study makes a significant and innovative contribution to the current knowledge and adds a new dimension to our understanding of RPGR-associated retinal degeneration.
We highlight the importance of PRO measures in capturing the effect of visual loss on the patient’s function, mental health and QoL. In our cohort, both males and females with a male phenotype, presented increased disability scores in domains such as central vision, color vision, contrast sensitivity, scotopic function, photopic peripheral function and mesopic peripheral function. Both rod and cone related functional domains were affected in our population, which is explained by the rapid progression of XLRP leading to secondary cone degeneration.
In the male group, we found the highest perceived disability in the domains of scotopic function and mesopic peripheral function. This result is in line with data previously published by Karuntu et al. while evaluating visual function parameters in patients with RP using MRDQ3. Additionally, similar findings were described by Marques et al. in a cohort of EYS-associated retinal degeneration, where self-reported visual function and psychosocial impact of visual loss were evaluated using MRDQ and MVAQ21. On the other hand, in our group of females with male phenotype, highest perceived disability was observed in the domains of contrast sensitivity and central vision. Interestingly, the cohort of patients studied by Karuntu et al. also presented high scores of disability in contrast sensitivity and could be present at all stages of RP3. The lowest perceived disability score in our cohort of males and females with male phenotype was photosensitivity. This is consistent with the findings of Karuntu et al., whereas in the EYS cohort of Marques et al. color vision yielded the lowest disability score3,21. In the male group, there was a positive correlation between age and several domains of visual disability. This finding is in line with the natural history of the disease, where older men present more advanced stages of the disease, corresponding to increased levels of visual disability1. Additionally, albeit nonsignificant, there seems to be a difference in age between males and females with a male phenotype. We hypothesize that this age difference in our cohort may be attributed to several factors, such as our small sample size, a later onset of symptoms in females, and a lower awareness of the disease in female patients, leading to a delayed diagnosis.
Moreover, we observed that rod- and cone-function related anxiety scores were greater in males and females with male pattern, which is consistent with the self-perceived visual disability revealed by the MRDQ analysis. This hypothesis is supported by significant positive correlations found between anxiety scores and every MRDQ domain and BCVA. To date, very few studies have delved into the patient burden and psychosocial aspect of XLRP. In a review study, Chivers et al. described that people with RP reported a heavy psychosocial burden, having difficulty undertaking activities of daily living and maintaining independence12. Furthermore, they inferred from RP studies that XLRP ought to be associated with a greater burden than other forms of RP, with a greater impact on patients’ mental health due to the younger age of those affected and more rapid progression to advanced disease12. The significant correlations found in our study between self-perceived visual disability and vision-related anxiety are consistent with previous studies with IRD patients by Jayasundera et al. and Popova et al.13,14. Furthermore, our findings suggesting a stronger correlation of scotopic function with rod-function anxiety, and central vision with cone-function anxiety, correspond to the results presented by Popova et al. and highlight the interconnection of the phenomena measured by these two PRO questionnaires13.
By including female carriers of RPGR variants, this study underscores phenotype heterogeneity, showing that females with a male phenotype may experience similar levels of self-perceived disability and vision-related anxiety as males. It has been well documented that female carriers with a severe phenotype often face significant visual impairment early in life4,5. Including female carriers of RPGR variants in future studies is crucial for enhancing disease understanding and developing targeted therapies for both men and women1,4,5. The inclusion of standardized PRO measures in clinical trials and studies is essential for better representing the impact of visual loss on patients’ function and mental health, thereby providing adequate support1,3.
One limitation of this study is its cross-sectional nature, which prevents us from inferring about disease progression. Secondly, the sample size is relatively small as expected in a rare disease, and it is unequally distributed between the three groups analysed. Consequently, the statistical power to draw significant conclusions and detect any differences between groups is inevitably hindered. Thirdly, we acknowledge that using visual acuity as a surrogate of central visual function and biomarker of disease severity has its limitations and does not fully encompass all functional dimensions of vision. Lastly, our results may be influenced by ascertainment bias, as the cohort was drawn from an IRD referral center, where patients with more severe symptoms are more likely to be referred.
In conclusion, this is the first study to explore self-reported disability and vision-related anxiety using validated PRO measures in both males and females with RPGR-associated retinal degeneration. Our findings highlight the significant visual and psychological impairments experienced by female carriers of RPGR variants and underscore the need for a holistic approach to patient care. The MRDQ results can guide personalized low vision rehabilitation, while identifying patients with higher anxiety levels using the MVAQ can direct psychological interventions. This study demonstrates that males and females with a male phenotype show similar levels of increased vision-related anxiety and self-perceived visual disability, with rod- and cone-function related anxiety correlating positively with MRDQ domains and BCVA. Utilizing PRO measures like MRDQ and MVAQ enhances our understanding and supports more targeted, patient-centered therapeutic interventions.
Data availability
The datasets generated and analyzed during the current study are not publicly available due to the sensitive nature of the research supporting data but are available from the corresponding author on reasonable request.
References
Lam, B. L. et al. A systematic literature review of disease progression reported in RPGR-associated X-linked retinitis pigmentosa. Retina (Philadelphia, Pa) 44, 1–9 (2024).
Nguyen, X. T. et al. RPGR-associated dystrophies: Clinical, genetic, and histopathological features. Int. J. Mol. Sci. 21, 835 (2020).
Karuntu, J. S., Nguyen, X. T. & Boon, C. J. F. Correlations between the Michigan retinal degeneration questionnaire and visual function parameters in patients with retinitis pigmentosa. Acta Ophthalmol. https://doi.org/10.1111/aos.16601 (2023).
Nanda, A., Salvetti, A. P., Clouston, P., Downes, S. M. & MacLaren, R. E. Exploring the variable phenotypes of RPGR carrier females in assessing their potential for retinal gene therapy. Genes 9, 643 (2018).
Marques, J. P. et al. Genetic spectrum, retinal phenotype, and peripapillary RNFL thickness in RPGR heterozygotes. Graefe’s Arch. Clin. Exp. Ophthalmol. 261, 867–878 (2023).
Gocuk, S. A., Jolly, J. K., Edwards, T. L. & Ayton, L. N. Female carriers of X-linked inherited retinal diseases: Genetics, diagnosis, and potential therapies. Prog. Retinal Eye Res. 96, 101190 (2023).
Wongchaisuwat, N. et al. Retinitis pigmentosa GTPase regulator-related retinopathy and gene therapy. Saudi J. Ophthalmol. Off. J. Saudi Ophthalmol. Soc. 37, 276–286 (2023).
Lam, B. L. et al. Assessment of visual function with cotoretigene toliparvovec in X-linked retinitis pigmentosa in the randomized XIRIUS phase 2/3 study. Ophthalmology https://doi.org/10.1016/j.ophtha.2024.02.023 (2023).
de la Camara, C.M.-F., Cehajic-Kapetanovic, J. & MacLaren, R. E. Emerging gene therapy products for RPGR-associated X-linked retinitis pigmentosa. Expert Opin. Emerg. Drugs 27, 431–443 (2022).
von Krusenstiern, L. et al. Changes in retinal sensitivity associated with cotoretigene toliparvovec in X-linked retinitis pigmentosa with RPGR gene variations. JAMA Ophthalmol. 141, 275–283 (2022).
National Library of Medicine. Gene Therapy Trial for the Treatment of X-Linked Retinitis Pigmentosa Associated with Variants in the RPGR Gene. https://www.clinicaltrials.gov/study/NCT04671433 (2024).
Chivers, M. et al. The burden of X-linked retinitis pigmentosa on patients and society: A narrative literature review. ClinicoEcon. Outcomes Res. CEOR 13, 565–572 (2021).
Popova, L. T. et al. Effects of duration and number of symptoms on vision-related anxiety in patients with inherited retinal diseases. Ophthalmic Genet. 44, 11–18 (2021).
Jayasundera, K. T. et al. Construct validity of inherited retinal disease-specific patient-reported outcome measures. Am. J. Ophthalmol. 248, 116–126 (2023).
Lacy, G. D. et al. The Michigan retinal degeneration questionnaire: A patient-reported outcome instrument for inherited retinal degenerations. Am. J. Ophthalmol. 222, 60–68 (2021).
Lacy, G. D. et al. The Michigan vision-related anxiety questionnaire: A psychosocial outcomes measure for inherited retinal degenerations. Am. J. Ophthalmol. 225, 137–146 (2021).
Marques, J. P. et al. Portuguese translation and linguistic validation of the Michigan retinal degeneration questionnaire and the Michigan vision-related anxiety questionnaire in a cohort with inherited retinal degenerations. Ophthalmic Genet. 43, 137–139 (2022).
Chiang, M. F. The 2021 National Eye Institute Strategic Plan: relating vision to health and quality of life. JAMA Ophthalmol. 139, 1263–1265 (2021).
Chiang, M. F. & Tumminia, S. J. The 2021 National Eye Institute Strategic Plan: Eliminating vision loss and improving quality of life. Ophthalmology 129, 12–14 (2022).
Marques, J. P. et al. Design, development and deployment of a web-based interoperable registry for inherited retinal dystrophies in Portugal: The IRD-PT. Orphanet J. Rare Dis. 15, 304 (2020).
Marques, J. P. et al. Self-reported visual function and psychosocial impact of visual loss in EYS-associated retinal degeneration in a Portuguese population. Ophthalmic Genet. 44, 334–340 (2023).
Author information
Authors and Affiliations
Contributions
N.G., O.C. and J.P.M. were involved in study concept, design and acquisition of data. N.G. analyzed and interpreted the data, and wrote the draft of the manuscript. J.P.M., C.O., C.H.A., R.S. and J.M. were contributors in writing and critically revising the manuscript. All authors edited and approved the final version of the manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gouveia, N., Chukwunalu, O., Oliveira, C. et al. Exploring self-reported visual function and vision-related anxiety in patients with RPGR-associated retinal degeneration. Sci Rep 14, 15189 (2024). https://doi.org/10.1038/s41598-024-66170-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-66170-2
Keywords
This article is cited by
-
Self-reported visual function and in-depth swept-source optical coherence tomography features of cystoid macular edema in retinitis pigmentosa
International Journal of Retina and Vitreous (2024)
