
Abstract
The endothelial glycocalyx is damaged in postcardiac arrest syndrome (PCAS), but the prognostic value is unknown. We aimed to observe the expression and prognostic value of glycocalyx shedding products, including syndecan-1 (SDC-1), hyaluronan (HA), and heparan sulfate (HS) in PCAS. Data on clinical and 28-day outcomes of seventy-one consecutive patients with out-of-hospital cardiac arrest (OHCA) after the return of spontaneous circulation (ROSC) were collected. SDC-1, HA, and HS were measured on days 0, 1, and 3 after ROSC. Thirty healthy individuals were controls. Glycocalyx shedding was observed in human umbilical vein endothelial cells (HUVECs) stimulated during hypoxia and reoxygenation in vitro. Within 4 h of ROSC, SDC-1 and HA levels, significantly increased. In the 28-day non-survivors, HA levels showed a gradual upward trend, SDC-1 remained at a high level, and HS levels first increased, then decreased. Kaplan–Meier curves and binary logistic regression analysis showed the prognostic value of SDC-1 levels on days 0, 1, and 3, HA levels on days 1 and 3, and HS levels on day 1. Only HS levels on day 1 showed a prognostic value for 28-day neurological outcomes. SDC-1 and HA levels were positively correlated with the no-flow time. In vitro, HUVECs showed shedding of SDC-1 and HS during a prolonged duration of hypoxia. After ROSC, SDC-1, HA, and HS levels may predict the 28-day survival after PCAS, and HS levels are associated with functional outcomes.
Similar content being viewed by others


Introduction
Despite decades of efforts, the survival rate of patients with out-of-hospital cardiac arrest (OHCA) remains poor. An analysis of 16 OHCA registries worldwide showed that survival to hospital discharge ranged from merely 3.1–20.4%, and favorable neurological outcomes ranged from 2.8 to 18.2%1. In addition to multiple organ failure (MOF), many deaths result from the withdrawal of life-sustaining treatment (WLST) owing predicted poor neurological outcomes2. Although current guidelines recommend against WLST because of its perceived poor neurological prognosis, this practice is common3. It is difficult to determine whether the resuscitation should be continued or withdrawn in a real clinical setting.
After the return of spontaneous circulation (ROSC), patients with OHCA present with critical post-cardiac arrest syndrome (PCAS), which has four major clinical manifestations: (1) neurological injury; (2) myocardial dysfunction; (3) systemic ischemia–reperfusion (IR) response that can evolve into MOF; and (4) the persistent precipitating pathology4. At the pathophysiological level, these injuries involve microcirculatory dysfunction, vascular leakage, and increased platelet and leukocyte adhesion to the endothelium. In other words, endothelial dysfunction is closely associated with pathophysiological changes in PCAS. Numerous studies have shown that endothelial dysfunction plays a crucial role in the development of ischemia–reperfusion (IR) response and MOF5,6,7,8. Hence, it is important to understand the pathophysiological changes after ROSC further and explore biomarkers that help in the clinical judgment of prognosis.
Recently, the glycocalyx has been identified as a key modulator of endothelial function, including the maintenance of endothelial barrier integrity and anticoagulant and anti-inflammatory responses9,10. The immune profile of PCAS shows a “sepsis-like” syndrome11. In sepsis, the shedding of the glycocalyx is promoted by various inflammatory mediators, including reactive oxygen species, tumor necrosis factor, heparanase, matrix metalloproteases, hyaluronidase, and serine proteases, thereby producing the main shedding products such as syndecan-1 (SDC-1), hyaluronan (HA), and heparan sulfate (HS)12. A damaged glycocalyx has been documented in PCAS and other IR injuries, such as lung, liver, and renal transplantation13,14,15,16. Thus, the clinical prognostic value of the glycocalyx shedding products in PCAS remains controversial and requires further investigation17,18,19.
In this study, we dynamically observed circulating SDC-1, HS, and HA level changes, evaluated the impact of IR on the glycocalyx of endothelial cells in vitro, and aimed to determine their clinical values in predicting survival and neurological outcomes for patients with OHCA after ROSC.
Methods
Study participants
This observational study was approved by the Yantai Affiliated Hospital of Binzhou Medical University’s Medical Ethics Committee (F-KY-0022-20161201-01). The patients’ close relatives and healthy controls provided written informed consent for study participation before enrollment. Between January 2020 and October 2022, patients who experienced OHCA and were admitted to the emergency department were evaluated for potential enrollment. The inclusion criteria were as follows: ROSC greater than 12 h and Glasgow coma scale scores < 8 after resuscitation. The exclusion criteria were as follows: age < 18 years; obvious signs of infection of any organ or tissue before OHCA, such as fever, obvious skin abscesses, soft tissue infection, or obvious abnormality of humoral tests or radiographic images indicative of infection after hospitalization; and terminal disease stages. Criteria for PCAS case withdrawal: after communicating with the guardians about the patients’ conditions, the patients' vital signs were extremely unstable, the clinical assessment of the risk of death in a short period of time was extremely high, the assessment of cerebral function was poor, or there was a need for prolonged hospitalization which may be a large economic burden, and the guardian voluntarily gave consent for treatment withdrawal. All the patients received treatment per the 2019 International Consensus on Cardiopulmonary Resuscitation Guidelines20. In this study, the patients received target temperature management (TTM). TTM was initiated within one hour of ROSC. The temperature was maintained at 36 °C for 72 h.
Healthy individuals were recruited from the physical examination center of Yantai Affiliated Hospital of Binzhou Medical University and enrolled as controls. The underlying diseases of the healthy population were effectively managed before study enrollment.
All methods used were performed in accordance with the relevant guidelines and regulations.
Data collection
Information on demographics, resuscitation data, and clinical and laboratory data were recorded. Acute physiology and chronic health evaluation (APACHE) II and sequential organ failure assessment (SOFA) scores were used to determine severity. For patients with OHCA, we analyzed serum samples taken at admission (within 4 h after ROSC, day 0), day 1 (12–36 h after ROSC), and day 3 (60–84 h after ROSC) for SDC-1, HA, and HS concentrations. During follow-up, we collected 28-day survival and favorable neurological outcomes data, which were defined as cerebral performance categories (CPC) 1–2.
Determining SDC-1, HS, and HA concentrations
Serum SDC-1, HS, and HA concentrations were assessed via ELISA according to the manufacturer’s instructions. The following ELISA kits were used: SDC-1 (Diaclone, Besançon Cedex, France), HS (US Biological Life Sciences), and HA (R&D Systems).
Impact of hypoxia and reoxygenation (H/R) on the endothelial cell glycocalyx
In order to intimate the impact (ischemia–reperfusion) IR on endothelial cell glycocalyx, an in vitro hypoxia and reoxygenation (H/R) model was constructed21,22. HUVECs were placed in an anoxic (1% O2, 5% CO2) incubator at 37 °C for 12 or 24 h in a sugar-free incomplete medium (Gibco, USA). Subsequently, the medium was replaced with an equivalent quantity of high-sugar complete media, and the cells were then returned to a standard cell culture incubator (21% O2, 5% CO2) at 37 °C for 6 h. The HUVECs were collected for subsequent studies.
Terminal deoxynucleotidyl transferase dUTP nick end labeling and flow cytometry analysis for apoptosis analysis
The terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) assay kit (Vazyme Biotech, China) was used according to the manufacturer’s instructions. HUVECs were fixed in 4% paraformaldehyde for 15 min and treated with 20 g/ml proteinase K for 20 min. The cells were then placed in an equilibration buffer for 30 min. The samples were then dropwise added to 50 μl of terminal deoxynucleotidyl transferase incubate, incubated for 60 min at 37 °C in the dark, and then twice rinsed with PBS. The cell nuclei were stained with DAPI (Invitrogen, USA). The results were analyzed using a fluorescence microscope (Olympus, Japan).
Annexin V-fluorescein isothiocyanate (FITC) and propidium iodide (PI) apoptosis detection kits (Immunoway, USA) were used for flow cytometry analysis. Briefly, 2 × 105 HUVECs were collected and resuspended in annexin V binding buffer. After staining with annexin V-FITC and PI, apoptotic cells were examined using flow cytometry (CytoFLEX LX, Beckman, USA).
Immunofluorescence
After different pre-treatments, HUVECs were fixed using a 4% paraformaldehyde solution. The cells were then sealed with BSA. Subsequently, the cells were incubated overnight with primary antibodies against HS (Biotechnology, Switzerland) and SDC-1 (Immunoway Biotechnology, USA). This was followed by incubation with the corresponding FITC secondary antibody. DAPI was used to stain the nuclei. Finally, images were captured using a fluorescence microscope.
Statistical analysis
All data were analyzed using the SPSS Version 27.0 software (SPSS, Chicago, IL, USA). For normally distributed data, continuous variables were presented as mean ± sd. Variables were expressed as median (25–75th percentiles) for skewed-distribution data. The Kruskal–Wallis test was applied for multigroup comparisons, and the Mann–-Whitney U test was used for between-group comparisons. Wilcoxon signed-rank test was used for paired sample comparisons. Qualitative variables were compared using a continuity table, followed by the chi-square test. The generalized estimated equation was used for dynamic analysis. The optimal thresholds of SDC-1, HS, and HA concentrations were determined using receiver operating characteristic (ROC) curves according to the Youden index. Using optimal thresholds, Kaplan–Meier survival curves were plotted, and log-rank tests were applied to compare survival distributions. The diagnostic abilities of SDC-1, HS, and HA were evaluated by the area under the curve (AUC). The z-test was used to compare the AUCs. Binary logistic regression was used to identify the variables associated with 28-day mortality and CPC 1–2. Correlations were analyzed using Spearman rank correlation. All statistical tests were two-tailed, and a P value of less than 0.05 was considered statistically significant.
Results
Characteristics of Enrolled Subjects
Totally, thirty healthy individuals and 71 patients with OHCA participated in this study. The demographics and clinical characteristics of the two groups are shown in Table 1. Serum samples were collected on day 0 in 71 patients, day 1 in 64 patients, and day 3 in 43 patients, respectively. Based on 28-day survival and favorable neurological outcome, OHCA patients were divided into survivor and non-survivor groups; CPC 1–2 and CPC 3–5 groups. Comparisons of the clinical characteristics between the different groups are shown in Tables 2 and 3.
Changes in SDC-1, HS, and HA concentrations within 4 h after ROSC
Within 4 h after ROSC, SDC-1, and HS concentrations, but not HA, were higher in the OHCA group than in the healthy control group (data not shown). Furthermore, SDC-1 and HS levels in both survivors and non-survivors in the CPC 1–2 and CPC 3–5 groups were higher than those in the healthy control group (Fig. 1A,B,D,E). Comparatively, no significant differences in HA levels were found between the groups (Fig. 1C,F).

Circulating syndecan-1, heparan sulfate, and hyaluronan expression in patients with OHCA 4 h after ROSC. (A–C): Serum concentrations of syndecan-1, heparan sulfate, and hyaluronan in healthy individuals, survivors, and non-survivors. (D–F): Serum concentrations of syndecan-1, heparan sulfate, and hyaluronan in healthy individuals, patients with CPC 1–2 and 3–5. * P < 0.05 between two groups, ** P < 0.001. CPC: cerebral performance category; OHCA: out-of-hospital cardiac arrest; ROSC: after return of spontaneous circulation.
In the first 3 days after ROSC, the evolution of both SDC-1 and HA levels, but not the HS level, was significantly different between 28-day survivors and non-survivors. At all three time points, SDC-1, HS, and HA levels in survivors persisted at low levels. In non-survivors, SDC-1 persisted at higher levels, and the HA level showed a slightly upward trend, whereas HS levels first increased and then decreased (Fig. 2A–C). In CPC 1–2 group, HA and SDC-1 levels first increased then decreased, whereas HS levels first decreased and then increased (Fig. 2D–F). However, only the HS level on day 1 showed differences between the groups (Fig. 2E).

Circulating syndecan-1, heparan sulfate and hyaluronan expression in patients with OHCA in the first three days after ROSC. (A–C) Time course of serum concentrations of syndecan-1, heparan sulfate, and hyaluronan by 28-day survival status. (D–F): Time course of serum concentrations of syndecan-1, heparan sulfate and hyaluronan by favorable neurological outcome. * P < 0.05 compared with survivors or patients with CPC 1–2. CPC: cerebral performance category; OHCA: out-of-hospital cardiac arrest; ROSC: after return of spontaneous circulation.
SDC-1, HS, and HA levels as independent predictors for 28-day prognosis
ROC analyses showed that SDC-1 on days 0, 1, and 3, HA on days 1 and 3, and HS on day 1 were discriminatory predictors of 28-day mortality (Supplemental Fig. 1A–C). With the designated cut-off value of SDC-1 (125.0, 114.0, and 107.0 ng/mL on day 0, 1, and 3 respectively), HA (236.0 ng/mL on day 1 and 354.0 ng/mL on day 3), and HS (2798 ng/mL on day 1), those biomarkers showed relatively high positive predictive value (Supplemental Table 1).
Comparatively, only the HS level on day 1, not SDC-1 or HA level, predicted 28-day CPC 1–2 (Supplemental Fig. 1D-F). With the designated cut-off value of 2355 ng/ml, HS levels on day 1 showed 100% sensitivity, 48.2% specificity, 22.2% positive predictive value, 100% negative predictive value, and 57.8% accuracy.
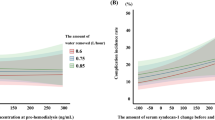
Kaplan–Meier curves were plotted according to the cut-off values determined by the Kaplan–Meier curves. After ROSC, patients with OHCA with SDC-1, HA, and HS levels higher than the optimal thresholds had a lower probability of 28-day survival (Fig. 3A–F) and a lower probability of favorable neurological outcomes (Fig. 3G).

Circulating SDC-1, HS and HA for discriminating 28-day survival and favorable neurologic outcome in the first three days after ROSC. According to optimal thresholds determined using receiver operating characteristic curves, Kaplan–Meier survival curves of SDC-1 levels (on days 0, 1, and 3), HA (on days 1 and 3), and HS (on day 1) showed statistically different survival outcomes (A–F) and neurologic outcomes (G). CPC: cerebral performance category; SDC-1: Syndecan-1; HA: hyaluronan; HS: heparan sulfate; ROSC: after return of spontaneous circulation.
In addition, binary logistic regression analysis revealed that SDC-1 levels on days 0, 1, and 3; HA levels on days 1 and 3; and HS on day 1 were significantly associated with all-cause mortality. Even after adjusting for age, sex, initial cardiac rhythm, and APACHE II scores, these biomarkers remained independent prognostic factors (Table 4).
Correlation between glycocalyx shedding products and ischemic hypoxia
After OHCA, no flow led to systematic ischemic hypoxia. The correlation between the duration of ischemic hypoxia and the level of glycocalyx shedding products was analyzed. SDC-1 and HA levels on days 0, 1, and 3, but not HS levels, showed a significant positive correlation with no-flow time (Supplemental Fig. 2).
Impact of H/R on endothelial apoptosis and the shedding of glycocalyx
H/R model of HUVECs was constructed in vitro. TUNEL staining results showed that HUVECs showed apoptosis after H/R, which was most significant at 24 h (Fig. 4A,B). Flow cytometry tests showed early and late apoptosis in endothelial cells, which was exacerbated by prolonged hypoxia (Fig. 4C). Similarly, immunofluorescence showed that the HS (Fig. 4D,F) and SDC-1 (Fig. 4E,G) expression decreased after hypoxic treatment for 12 h and was further aggravated after hypoxic treatment for 24 h.

Impact of H/R on endothelial apoptosis and the shedding of glycocalyx. Representative TUNEL staining (green) for HUVECs apoptosis in the control, H/R 12 h, and H/R 24 h groups and nuclei were stained with DAPI (blue) (A). Scale bar = 100 μm. The quantification of TUNEL-positive cells is displayed (B). Apoptosis of HUVECs treated with H/R using flow cytometry (C). Immunofluorescence showed HS (D,F) and SDC-1 (E,G) expression. Magnifcation 200 × , scale bar, 50 μm. H/R: Hypoxia and reoxygenation. Data represent the mean ± SD of three independent experiments. * P < 0.05; ** P < 0.01.
Discussion
Glycocalyx damage is involved in endothelial dysfunction in PCAS. However, the dynamic changes and prognostic value of the glycocalyx shedding products remain poorly understood. In this study, we explored the value of circulating SDC-1, HA, and HS levels as biomarkers for evaluating the prognosis of patients with PCAS. We found that serum SDC-1, HA, and HS levels increased after ROSC and showed different trends in patients corresponding to 28-day survival rates or neurological outcomes in the first three days. Furthermore, using optimal cut-off values, SDC-1, HA, and HS level showed significantly different curves regarding 28-day mortality and were independent predictive factors for 28-day survival. In addition, HS levels on day 1 had different Kaplan–Meier curves for 28-day neurological outcomes. After ROSC, SDC-1 and HA levels showed a positive correlation with the no-flow time. Finally, after prolonged hypoxia, HUVECs showed increased apoptosis and exacerbated shedding of SDC-1 and HS in vitro.
In this study, significantly increased SDC-1 and HS levels were observed in the circulation within 4 h after ROSC. At present, limited data on glycocalyx shedding product kinetics have shown rapidly increasing characteristics. Circulating SDC-1 was significantly increased in patients with OHCA after ROSC and in experimental settings17,18,23,24. A rapid increase in serum SDC-1 and HS levels has been observed in patients undergoing major vascular surgery via cardiopulmonary bypass with hypothermic circulatory arrest, representing global ischemia25. Glycocalyx shedding is often thought to be strongly affected by ischemia–reperfusion (IR)16,26.In a pig heart IR model study, even a 20-min no-flow warm ischemia followed by 20-min reperfusion caused obvious SDC-1 and HS shedding in the coronary vein27. In rat models, a considerable increase in plasma SDC-1 levels was observed 120 min after cardiac arrest28. The plasma levels of HS and SDC-1, the main components of the glycocalyx, increased after major aortic surgery or prolonged intra-aortic balloon inflation and subsequent reperfusion, suggesting that both cause documented glycocalyx damage25,29.
We further observed differences in the glycocalyx shedding products between the different prognostic groups. After ROSC, SDC-1 and HS levels, were higher in non-survivors and in patients with unfavorable neurological outcomes. Furthermore, we observed dynamic changes in these biomarkers in the first three days after ROSC. For 28-day survival, generalized estimated equation analysis revealed that SDC-1, HA, and HS levels had significant main effects. In non-survivors, the HA level showed a gradual slight upward trend, SDC-1 levels remained high, and the HS level first increased and then decreased. This implies that the glycocalyx degradation products have different metabolic profiles. Dynamic changes in SDC-1 and HS levels in patients are controversial17,18,19. In addition, a study that included 15 patients with OHCA found that non-survivors within 30 days had higher SDC-1 and HA expression within 48 h after ROSC18. However, another study, which included 25 patients with OHCA, found that SDC-1 and HS, but not HA, were highly expressed in non-survivors17. Recently, a study that included 71 patients with OHCA showed that elevated serum HS and HA levels in the early stages after ROSC predicted 30-day mortality, and SDC-1 level did not contribute to outcome prediction19. Different inclusion criteria and patient heterogeneity among these studies may have led to different findings. Some studies have shown that SDC-1, HA, and HS levels in different samples exhibit diverse dynamic changes in different clinical contexts14,30. Additionally, on day 3, the HA level did not significantly increase, whereas SDC-1 and HS levels trended downward, which may be owing to patients with high SDC-1, HS, and HA levels dying within 3 days after ROSC.
Optimal cut-off values determined by ROC curves, Kaplan–Meier curves, and binary logistic regression analysis showed the prognostic values of SDC-1, HA, and HS levels. HA levels on day 1 had the highest AUC, but the AUCs of the three biomarkers did not show any statistical differences (data not shown). PCAS and sepsis destroy the endothelial glycocalyx31,32 and share similar immunological profiles11. In sepsis, SDC-1, HA, and HS levels have different prognostic values33,34,35. Studies with larger sample sizes may help to differentiate the prognostic abilities of different biomarkers.
Glycocalyx degradation affects the integrity of the blood–brain barrier36,37,38. We found that only the HS level showed a prognostic value for neurological outcomes. In this study, patients with OHCA were from a district where emergency medical services were not well developed. However, the witnesses lacked first-aid skills, and did not guarantee effective chest compressions. Therefore, the no-flow time of some patients was relatively long, and the low-flow time could not be assessed. Thus, only 8 patients with OHCA had favorable neurological outcomes. The relatively small sample size may have led to a bias in the statistical results. Futhermore, in a recent study of 22 patients with CPC 1–2 scores, HS levels were also shown to be a potential predictive marker for 30-day neurological outcomes19. In addition, glycocalyx degradation leads to blood–brain barrier dysfunction and brain edema after hypoxic cardiac arrest in rats, and elevated serum HS levels seem to be associated with poor neurological functional outcomes19,39. Nevertheless, a plasma analysis of individuals with acute ischemic stroke who are receiving intravenous thrombolysis has revealed that an increase in the glycocalyx damage marker SDC-1 is associated with a worse prognosis40.
We observed the effects of IR on the glycocalyx shedding. SDC-1 and HA levels were positively correlated with the no-flow times. Interestingly, no significant correlation was found between the HS levels and no-flow time. Patient heterogeneity is a potential explanation. However, HS levels in patients with OHCA, even in the survivor subgroup, were higher than those in healthy individuals. Therefore, it is reasonable to conclude that IR injury leads to HS shedding. We constructed an H/R endothelial model in vitro to imitate the IR process, and flow cytometry and TUNEL staining documented that endothelial cells were damaged. With prolonged hypoxia, endothelial cells in the 24 h hypoxia group presented more significant shedding of SDC-1 and HS than 12 h of the hypoxia group, which implied that more severe IR led to more obvious destruction of the glycocalyx.
This study had some limitations. First, we did not conduct further observations for longer periods. Dynamic observation for a longer duration would clarify the significance of SDC-1, HA, and HS expression in PCAS. However, the probability of patient death and infection increases over time. Reduced sample numbers and infections affected the analysis of the glycocalyx-shedding products. Second, owing to the small number of patients with favorable neurological outcomes, we were unable to adequately evaluate the prognostic values of SDC-1, HA, and HS levels for favorable neurological outcomes.
Conclusions
This study simultaneously showed dynamic changes in circulating SDC-1, HA, and HS levels during the early period after ROSC. After ROSC, SDC-1, HA, and HS levels were independent predictors of 28-day survival, and HS levels on day 1 showed prognostic value for neurological outcomes. Furthermore, with prolonged hypoxia, endothelial cells show more severe glycocalyx shedding. In summary, IR leads to endothelial glycocalyx destruction, and its shedding products have prognostic values for patients with OHCA after ROSC, indicating that the endothelial glycocalyx is a potential therapeutic target for the treatment of PCAS.
Data availability
The data sets supporting the conclusions of this article are included within the article.
References
Kiguchi, T. et al. Out-of-hospital cardiac arrest across the World: First report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation 152, 39–49. https://doi.org/10.1016/j.resuscitation.2020.02.044 (2020).
Dragancea, I. et al. Protocol-driven neurological prognostication and withdrawal of life-sustaining therapy after cardiac arrest and targeted temperature management. Resuscitation 117, 50–57. https://doi.org/10.1016/j.resuscitation.2017.05.014 (2017).
Elmer, J. et al. Association of early withdrawal of life-sustaining therapy for perceived neurological prognosis with mortality after cardiac arrest. Resuscitation 102, 127–135. https://doi.org/10.1016/j.resuscitation.2016.01.016 (2016).
Nolan, J. P. et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation 79, 350–379. https://doi.org/10.1016/j.resuscitation.2008.09.017 (2008).
Bro-Jeppesen, J. et al. Endothelial activation/injury and associations with severity of post-cardiac arrest syndrome and mortality after out-of-hospital cardiac arrest. Resuscitation 107, 71–79. https://doi.org/10.1016/j.resuscitation.2016.08.006 (2016).
Herrera-Zelada, N., Zuniga-Cuevas, U., Ramirez-Reyes, A., Lavandero, S. & Riquelme, J. A. Targeting the endothelium to achieve cardioprotection. Front. Pharmacol. 12, 636134. https://doi.org/10.3389/fphar.2021.636134 (2021).
Aird, W. C. The role of the endothelium in severe sepsis and multiple organ dysfunction syndrome. Blood 101, 3765–3777. https://doi.org/10.1182/blood-2002-06-1887 (2003).
Hilbert, T. & Klaschik, S. The angiopoietin/TIE receptor system: Focusing its role for ischemia-reperfusion injury. Cytokine Growth Factor Rev. 26, 281–291. https://doi.org/10.1016/j.cytogfr.2014.10.013 (2015).
Joffre, J., Hellman, J., Ince, C. & Ait-Oufella, H. Endothelial responses in sepsis. Am. J. Respir. Crit. Care Med. 202, 361–370. https://doi.org/10.1164/rccm.201910-1911TR (2020).
Foote, C. A. et al. Endothelial glycocalyx. Compr. Physiol. 12, 3781–3811. https://doi.org/10.1002/cphy.c210029 (2022).
Adrie, C. et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation 106, 562–568. https://doi.org/10.1161/01.cir.0000023891.80661.ad (2002).
Pergolizzi, C., Franchi, F., Taccone, F. S., Preiser, J. C. & Scolletta, S. Potential nutritional and pharmacological treatment of glycocalyx alterations during sepsis. Minerva Anestesiol. 89, 341–350. https://doi.org/10.23736/S0375-9393.22.16834-3 (2023).
Schiefer, J. et al. Glycocalyx damage within human liver grafts correlates with graft injury and postoperative graft function after orthotopic liver transplantation. Transplantation 104, 72–78. https://doi.org/10.1097/TP.0000000000002838 (2020).
Sladden, T. M. et al. Endothelial glycocalyx shedding predicts donor organ acceptability and is associated with primary graft dysfunction in lung transplant recipients. Transplantation 103, 1277–1285. https://doi.org/10.1097/TP.0000000000002539 (2019).
Duni, A. et al. The endothelial glycocalyx as a target of ischemia and reperfusion injury in kidney transplantation-where have we gone so far?. Int. J. Mol. Sci. https://doi.org/10.3390/ijms22042157 (2021).
Abassi, Z., Armaly, Z. & Heyman, S. N. Glycocalyx degradation in ischemia-reperfusion injury. Am. J. Pathol. 190, 752–767. https://doi.org/10.1016/j.ajpath.2019.08.019 (2020).
Grundmann, S. et al. Perturbation of the endothelial glycocalyx in post cardiac arrest syndrome. Resuscitation 83, 715–720. https://doi.org/10.1016/j.resuscitation.2012.01.028 (2012).
Bogner-Flatz, V. et al. On-the-scene hyaluronan and syndecan-1 serum concentrations and outcome after cardiac arrest and resuscitation. Mediators Inflamm. 2019, 8071619. https://doi.org/10.1155/2019/8071619 (2019).
He, D. et al. Serum glycocalyx markers in patients after cardiac arrest: Association with outcomes. Zhonghua Yi Xue Za Zhi 104, 63–68. https://doi.org/10.3760/cma.j.cn112137-20230829-00322 (2024).
Soar, J. et al. 2019 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: Summary from the basic life support; advanced life support; pediatric life support; neonatal life support; education, implementation, and teams; and first aid task forces. Circulation 140, e826–e880. https://doi.org/10.1161/cir.0000000000000734 (2019).
Zhang, X. et al. Propofol inhibits myocardial injury induced by microvesicles derived from hypoxia-reoxygenated endothelial cells via lncCCT4-2/CCT4 signaling. Biol. Res. 56, 20. https://doi.org/10.1186/s40659-023-00428-3 (2023).
Ali Sheikh, M. S. The mir-21 inhibition enhanced HUVEC cellular viability during hypoxia-reoxygenation injury by regulating PDCD4. Mediators Inflamm. 2022, 9661940. https://doi.org/10.1155/2022/9661940 (2022).
Chaban, V. et al. Complement activation is associated with poor outcome after out-of-hospital cardiac arrest. Resuscitation 166, 129–136. https://doi.org/10.1016/j.resuscitation.2021.05.038 (2021).
Langeland, H. et al. The inflammatory response is related to circulatory failure after out-of-hospital cardiac arrest: A prospective cohort study. Resuscitation 170, 115–125. https://doi.org/10.1016/j.resuscitation.2021.11.026 (2022).
Rehm, M. et al. Shedding of the endothelial glycocalyx in patients undergoing major vascular surgery with global and regional ischemia. Circulation 116, 1896–1906. https://doi.org/10.1161/circulationaha.106.684852 (2007).
Zhang, Y. N., Wu, Q., Zhang, N. N. & Chen, H. S. Ischemic preconditioning alleviates cerebral ischemia-reperfusion injury by interfering with glycocalyx. Transl. Stroke Res. 14, 929–940. https://doi.org/10.1007/s12975-022-01081-w (2023).
Chappell, D. et al. Antithrombin reduces shedding of the endothelial glycocalyx following ischaemia/reperfusion. Cardiovasc. Res. 83, 388–396. https://doi.org/10.1093/cvr/cvp097 (2009).
Yin, T. et al. Hydrogen gas with extracorporeal cardiopulmonary resuscitation improves survival after prolonged cardiac arrest in rats. J. Transl. Med. 19, 462. https://doi.org/10.1186/s12967-021-03129-1 (2021).
van Golen, R. F. et al. The mechanisms and physiological relevance of glycocalyx degradation in hepatic ischemia/reperfusion injury. Antioxid. Redox Signal 21, 1098–1118. https://doi.org/10.1089/ars.2013.5751 (2014).
Nemme, J. et al. Minimal shedding of the glycocalyx layer during abdominal hysterectomy. BMC Anesthesiol. 17, 107. https://doi.org/10.1186/s12871-017-0391-6 (2017).
Katsandres, S. C. et al. Inflammation, endothelial injury, and the acute respiratory distress syndrome after out-of-hospital cardiac arrest. Resusc. Plus 17, 100590. https://doi.org/10.1016/j.resplu.2024.100590 (2024).
Oshima, K., King, S. I., McMurtry, S. A. & Schmidt, E. P. Endothelial heparan sulfate proteoglycans in sepsis: The role of the glycocalyx. Semin. Thromb. Hemost. 47, 274–282. https://doi.org/10.1055/s-0041-1725064 (2021).
Benatti, M. N., Fabro, A. T. & Miranda, C. H. Endothelial glycocalyx shedding in the acute respiratory distress syndrome after flu syndrome. J. Intensive Care 8, 72. https://doi.org/10.1186/s40560-020-00488-7 (2020).
Huang, X. et al. Association between plasma glycocalyx component levels and poor prognosis in severe influenza type A (H1N1). Sci. Rep. 12, 163. https://doi.org/10.1038/s41598-021-04146-2 (2022).
Uchimido, R., Schmidt, E. P. & Shapiro, N. I. The glycocalyx: A novel diagnostic and therapeutic target in sepsis. Crit. Care 23, 16. https://doi.org/10.1186/s13054-018-2292-6 (2019).
Jin, J. et al. The structure and function of the glycocalyx and its connection with blood-brain barrier. Front. Cell Neurosci. 15, 739699. https://doi.org/10.3389/fncel.2021.739699 (2021).
Zhao, F., Zhong, L. & Luo, Y. Endothelial glycocalyx as an important factor in composition of blood-brain barrier. CNS Neurosci. Ther. 27, 26–35. https://doi.org/10.1111/cns.13560 (2021).
Yang, R., Chen, M., Zheng, J., Li, X. & Zhang, X. The role of heparin and glycocalyx in blood-brain barrier dysfunction. Front. Immunol. 12, 754141. https://doi.org/10.3389/fimmu.2021.754141 (2021).
Zhu, J. et al. Glycocalyx degradation leads to blood-brain barrier dysfunction and brain edema after asphyxia cardiac arrest in rats. J. Cereb. Blood Flow Metab. 38, 1979–1992. https://doi.org/10.1177/0271678x17726062 (2018).
Zhao, F. et al. Elevated plasma syndecan-1 as glycocalyx injury marker predicts unfavorable outcomes after rt-PA intravenous thrombolysis in acute ischemic stroke. Front. Pharmacol. 13, 949290. https://doi.org/10.3389/fphar.2022.949290 (2022).
Funding
This work was supported by funding from National Natural Science Foundation of Shandong Province (No. ZR2022MH151), Shandong Province Medical and Health Science and Technology Development Program Project (No. 2019WS336), and Yantai Science and Technology Innovation Development Program (No. 2023YD037).
Author information
Authors and Affiliations
Contributions
J.L.: Methodology, Investigation, Formal analysis, Writing—original draft, Visualization. Z.Q.: Data curation, Writing—review & editing. C.S.: Data curation, Formal Analysis. Y.Z.: Data curation, Formal Analysis. L.G.: Formal analysis, Writing—review & editing. Y.L.: Data curation. H.D.: Data curation, Methodology. W.J.: Writing-review &editing. L.Z.: Conceptualization, Supervision, Writing-review & editing. J.Y.: Funding acquisition, Project administration, Writing-review &editing.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, J., Qi, Z., Sun, C. et al. Circulating glycocalyx shedding products as biomarkers for evaluating prognosis of patients with out-of-hospital cardiac arrest after return of spontaneous circulation. Sci Rep 14, 17582 (2024). https://doi.org/10.1038/s41598-024-68738-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-68738-4
