
Abstract
Impairments in somatosensory function are a common and often debilitating consequence of neurological injury, with few effective interventions. Building on success in rehabilitation for motor dysfunction, the delivery of vagus nerve stimulation (VNS) combined with tactile rehabilitation has emerged as a potential approach to enhance recovery of somatosensation. In order to maximize the effectiveness of VNS therapy and promote translation to clinical implementation, we sought to optimize the stimulation paradigm and identify neural mechanisms that underlie VNS-dependent recovery. To do so, we characterized the effect of tactile rehabilitation combined with VNS across a range of stimulation intensities on recovery of somatosensory function in a rat model of chronic sensory loss in the forelimb. Consistent with previous studies in other applications, we find that moderate intensity VNS yields the most effective restoration of somatosensation, and both lower and higher VNS intensities fail to enhance recovery compared to rehabilitation without VNS. We next used the optimized, moderate intensity to evaluate the mechanisms that underlie recovery. We find that moderate intensity VNS enhances transcription of Arc, a canonical mediator of synaptic plasticity, in the cortex, and that transcript levels were correlated with the degree of somatosensory recovery. Moreover, we observe that blocking plasticity by depleting acetylcholine in the cortex prevents the VNS-dependent enhancement of somatosensory recovery. Collectively, these findings identify neural mechanisms that subserve VNS-dependent somatosensation recovery and provide a basis for selecting optimal stimulation parameters in order to facilitate translation of this potential intervention.
Similar content being viewed by others


Introduction
Vagus nerve stimulation (VNS) combined with rehabilitative training has emerged as a novel strategy to improve recovery after neurological injury1,2. This application of VNS therapy is founded on the principles of neurorehabilitation, which aims to facilitate recovery by promoting adaptive changes in neural circuits after injury. Brief bursts of electrical stimulation of the vagus nerve drive release of neuromodulators, including acetylcholine and norepinephrine, which are associated with synaptic plasticity3,4,5,6,7,8. Pairing VNS with forelimb motor training enhances synaptic connectivity changes in descending motor circuits and improves recovery across a range of preclinical models of neurological injury9,10,11,12,13,14,15,16,17. Moreover, based on a successful pivotal trial, VNS paired with upper limb rehabilitation recently received FDA approval for individuals with chronic stroke18.
Building on these findings, a series of recent studies show that a congruent approach of pairing VNS with tactile rehabilitation promotes recovery of somatosensation. VNS combined with passive mechanical stimulation of hyposensitive skin surfaces reduces detection thresholds in a rat model of profound sensory loss, indicating a restoration of an aspect of somatosensory function19,20,21,22. Highlighting the clinical potential of this approach, a case study in an individual with profound sensory loss resulting from stroke provides initial evidence that pairing VNS with tactile retraining may improve recovery of somatosensation23.
The ability to apply VNS to improve recovery of both motor and sensory function raises two overlapping questions, one theoretical and one practical. First, does VNS engage a similar underlying mechanism to enhance recovery of somatosensory function? VNS-directed recovery is known to require synaptic plasticity specific to the cortical networks engaged by the rehabilitative paradigm16,17. For instance, pairing VNS with motor training yields refinement of synaptic connectivity in corticospinal networks controlling the trained muscles17. Moreover, related studies show that VNS-dependent plasticity and recovery follows a well-described inverted-U relationship with stimulation intensity24,25,26,27,28. Consequently, stimulation intensity provides a simple, accessible means to probe whether a similar mechanism, namely, enhancement of plasticity, underlies recovery of somatosensory function.
Second, what is the best strategy to apply VNS to improve recovery? Optimization is a key step in effective translation of VNS therapy. Emerging evidence provides a basis to define the optimal strategies for the accompanying tactile rehabilitation20,21,22, but no studies directly examine the electrical stimulation parameters that yield the greatest recovery. Stimulation intensity is a critical determinant of VNS-dependent effects, thus optimizing intensity is a logical first step in developing this approach28. Both of these questions can be addressed by evaluating the effect of stimulation intensity on VNS-dependent recovery across a range of clinically-viable parameters known to predictably influence synaptic plasticity.
In our first experiment, we characterized the influence of VNS intensity on somatosensory recovery in a rat model of profound sensory loss. Mirroring results from pairing VNS with motor rehabilitation, we find that VNS exhibits an inverted-U relationship with stimulation intensity. Additionally, we provide two other lines of evidence indicating that pairing VNS with touch promotes synaptic plasticity. In our second and third experiments respectively, we found that moderate intensity VNS increases transcription of a plasticity-related gene in the cortex, and preventing plasticity abrogates VNS-dependent enhancement of somatosensory recovery. These findings help to define the mechanistic basis for VNS-dependent improvements in somatosensation and provide a basis for selecting optimal stimulation parameters.
Methods
Subjects
All methods followed the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines. 126 female Sprague–Dawley rats weighing approximately 250–300 g were included in this study (Charles River Labs). The rats were housed in a 12:12 reversed light cycle environment, and behavioral training was performed during the dark cycle to increase daytime activity levels. All handling, housing, stimulation, and surgical procedures were approved by the University of Texas at Dallas Institutional Animal Care and Use Committee (Protocols: 14-10 and 99-06) and conducted according to the protocols and guidelines.
Peripheral nerve injury (PNI)
All animals underwent transection and repair of the median and ulnar nerves to generate chronic sensory loss, as described in previous studies17,29,30. Animals were deeply anesthetized with ketamine hydrochloride (50 mg/kg, IP), xylazine (20 mg/kg, IP), and acepromazine (5 mg/kg) and supplemented as necessary to maintain areflexia. The animal was placed in a supine position, and a sagittal incision was made 1 cm proximal to the elbow of the right forelimb. The surrounding tissue was blunt dissected to expose, separate, and transect the median and ulnar nerves. The proximal and distal nerve stumps were sutured 1 mm from the ends of an 8 mm saline-filled polyurethane tube (Micro-Renathane 0.095’’ I.D 0.066’’ O.D., Braintree Scientific, Inc., Braintree, MA), resulting in a 6 mm gap between nerve stumps. The skin incision was sutured and covered in a triple antibiotic ointment. After surgery, animals were given subcutaneous injections of sustained release buprenorphine (10 mg/kg) and 10 ml of a solution of lactated ringers with 5% dextrose. Animals were outfitted with an Elizabethan collar for 4 days to prevent autophagia. Animals were allowed to recover for 8 weeks prior to the resumption of behavioral testing.
Vagus nerve cuff implantation
All animals were implanted with a stimulating cuff electrode on the left cervical vagus nerve, according to standard procedures17,20,29. Animals were anesthetized and placed in a stereotaxic apparatus to stabilize the skull. A midline incision was made to expose the surface of the skull. Four holes were drilled surrounding lambda, and bone screws were inserted to anchor a two-channel connector to the skull using acrylic. The animal was then removed from the stereotaxic apparatus and placed in a supine position. An incision was made 2 mm anterior and 2 mm lateral to the top of the sternum, and blunt dissection exposed the left cervical vagus nerve. After the nerve was isolated from the carotid artery, a stimulating cuff electrode was placed around the vagus nerve. The stimulating cuff was constructed of a 3 mm polyurethane tube (Micro-Renathane 0.039’’ I.D 0.079’’ O.D., Braintree Scientific, Inc., Braintree, MA) and 2, 0.01 mm diameter multi-stranded platinum-iridium wires (Sigmund Cohn Corp., Mt. Vernon, NY) spaced 1 mm apart and covering a 270° arc inside the cuff, as previously described31. Leads were tunneled subcutaneously to the head-mounted connector. All incisions were sutured closed, and the two-channel connector was enclosed in acrylic. After surgery, animals were given subcutaneous injections of buprenorphine (1.2 mg/kg) and 10 ml of a solution of lactated ringers with 5% dextrose. Additional details and description of the cuff and headstage are included in Supplementary Fig. 1.
Cuff functionality
We used two methods to ensure effective nerve activation, as in our previous studies25,26,27. VNS-dependent activation of the Hering-Breuer reflex was used to confirm correct placement and functionality of the stimulating cuff electrode. If five trains of stimulation (0.8 mA, 30 Hz, 100 microsecond pulse width, up to 5 train duration, with an inter-stimulus duration of 30 s) failed to decrease blood oxygen saturation, the cuff electrode was determined to be nonfunctional31. Cuff functionality was assessed at time of implant and on the last day of therapy. If the cuff was nonfunctional at implant, the cuff electrode was replaced, and if the cuff was nonfunctional after therapy completion, the animal was excluded from the study. As an additional measure to confirm cuff functionalize, we monitored cuff impedance during each session of stimulation using a digital oscilloscope. If stimulation voltage exceeded 40 V peak-to-peak, the animal was excluded from the study. Cuff impedance was stable for the duration of the study (Supplementary Fig. 2).
Tactile rehabilitation
8 weeks after PNI, 85 animals were allocated into one of 8 groups to receive tactile rehabilitation paired with VNS. 60 animals were included in the first experiment investigating the effect of current amplitude on recovery groups (No VNS (n = 15), Low VNS (n = 15), Moderate VNS (n = 15), High VNS (n = 15)). 15 animals were included in the second experiment, which examined the effect of moderate intensity VNS on plasticity-related gene expression (Arc No VNS (n = 7), Arc Moderate VNS (n = 8)). 10 animals were included in the third experiment to determine the necessity of plasticity for recovery (ACh+; Moderate VNS (n = 4), ACh−; No VNS (n = 6)).
Tactile rehabilitation began 9 weeks after PNI and was delivered similar to previous studies19,21,22. Animals received one session of rehabilitation daily, 4 days per week, for up to 5 weeks. Animals were placed in an acrylic booth (14 × 15 cm) with a mesh floor. The headstage was connected to an isolated pulse stimulator to deliver fixed current-controlled parameters for VNS therapy (Model 2100, A-M Systems, Sequim, WA, ± 100 V). Approximately every 10 s, a small paintbrush was applied to ventral surface of the right, previously denervated paw, to provide a mechanical stimulus. A short burst of VNS was triggered by a button press to coincide with the delivery of mechanical stimulation. Each stimulation consisted of a 500 ms train of 100 us biphasic pulses delivered at 30 Hz. VNS intensity was delivered as appropriate for each group: 0 mA (no VNS), 0.4 mA (low intensity), 0.8 mA (moderate intensity), or 1.2 mA (high intensity), with all other stimulation parameters held constant. All animals received 200 tactile VNS pairings per session, as in previous studies20,21,22,29. Additional details and description of the stimulation set up are included in Supplementary Fig. 1.
Mechanosensory withdrawal threshold testing
Mechanosensory withdrawal thresholds were assessed in all animals according to standard procedures20,29. Testing was performed in an acrylic chamber (19.5 × 9.6 cm) with a mesh wire floor. Animals were allowed to acclimate to the behavioral chamber for 30 min before testing commenced. Mechanical withdrawal thresholds of the left and right forepaws were tested using a dynamic plantar aesthesiometer (Cat. No. 37450; Ugo Basile, Lugano, Switzerland). The actuator filament (0.5 mm diameter) was positioned against the plantar surface of the forepaw, and a linearly increasing force was applied (20-s ramp time, 50 g maximal force). The force at which paw withdrawal occurred was captured for analysis. Testing alternated between the left and right forepaws, with a minimum of 1 min between consecutive tests. Trials resulting in paw withdrawal due to spontaneous exploratory activity were excluded from analysis. Assessments were collected before injury, before rehab, and once weekly during rehab.
Cylinder asymmetry testing
Spontaneous forelimb use was measured using the cylinder task as previously described20,29. Animals were placed in a transparent Plexiglas cylinder (20 cm diameter) and allowed to freely explore for 3 min. Video was recorded from directly underneath the cylinder through a clear sheet of acrylic. The total number of left and right forepaw contacts with the wall during rearing was recorded. The relative use of the injured right forepaw was evaluated with an asymmetry index, calculated as (right/[left + right]) × 100. Assessments were collected before injury, before rehab, and once weekly during rehab by experimenters blinded to experimental conditions of the animals.
Toe spread assessment
Toe spread analysis was performed to measure weight bearing using the stamp and paper method as previously described20,29. The forepaws of the animals were coated in a layer of nontoxic ink, and the animals walked across a sheet of paper. The paper was scanned, digitized, and scored using ImageJ software (NIH, Bethesda, MD). Three footprints from both the left and right paw were analyzed by a blinded experimenter. The distance between the center of the second and fifth digits was measured and recorded for each print. Assessments were performed before injury, before rehab, and on the last week of rehab by experimenters blinded to the groups.
mRNA sequencing
One day after the last tactile rehabilitation session, rats were decapitated and the forelimb section of the contralateral somatosensory cortex was rapidly dissected in ice-cold dissection buffer and homogenized using Precellys Minlys Tissue Homogenizer (Bertin-instruments, P000673-MLYS0-A). Samples were homogenized at 10 s intervals (medium speed) for 10 min, at 4 °C, in Precellys homogenizing CKMix tubes. RNA was performed on all samples using the Direct-zol RNA Microprep kit (R2060, Zymo Research) according to the manufacturer’s instructions. RNA was eluted with 30 µL of RNase free water. RNA yield was quantified using a Nanodrop system (Thermo Fisher Scientific), and RNA quality was determined by a fragment analyzer (Advanced Analytical Technologies).
Total RNA from 15 cortical samples was purified using TRIzolTM (ThemoFisher) and subjected to Tru-seq stranded mRNA library preparation according to the manufacturer’s instructions (Illumina). Tru-seq total RNA library kit with ribosomal RNA depletion was used to generate sequencing libraries. After standardizing the amount of cDNA per sample, the libraries were sequenced on an Illumina NextSeq500 sequencing platform with 75-bp single-end reads in multiplexed sequencing experiments, yielding a median of 22.3 million reads per sample. mRNA library preparation and sequencing were done at the Genome Center in The University of Texas at Dallas Research Core Facilities.
Cortical cholinergic depletion
Cholinergic lesions were performed at the time of vagus nerve cuff implantations, similar to previous reports4,32,33,34. Rats were anesthetized with ketamine hydrochloride (80 mg/kg, i.p.) and xylazine (10 mg/kg, i.p.), and given supplemental doses as needed to maintain anesthesia levels. After placing the rat in a stereotaxic frame (David Kopf Instruments, Tujunga, CA) burr holes were drilled bilaterally over the nucleus basalis. Rats received injections of either conjugated 192-IgG-saporin (Advanced Targeting Systems, San Diego, CA) to selectively lesion cholinergic neurons in the basal forebrain, or vehicle injections of an untargeted antibody and saporin, which does not enter cells and induce cell death. 192-IgG-saporin or vehicle (0.375 mg/mL in saline) were injected through a pulled glass needle at 0.1 µL/min using a Nanoliter 2010 injector (World Precision Instruments, Sarasota, FL). Injections were made at the following sites (site 1&2: 0.3 µL, AP: − 1.4, ML: ± 2.5, DV: − 8.0; sites 3&4: 0.2 µL, AP: − 2.6, ML: ± , DV: − 7.0 mm). The needle remained in place for 4–5 min after each injection to allow for diffusion and prevent backflow. Burr holes were sealed with bone wax.
Exclusion criteria
41 animals were excluded from the study. Animals were excluded for the following reasons, which were pre-defined and consistent with our prior studies: pre-injury withdrawal threshold was above 15 g (n = 7), post-injury withdrawal threshold was below 15 g (n = 15), failure of the stimulating cuff (n = 5), failure of the headstage (n = 4), autophagia (n = 2), or mortality prior to completion of the full course of rehabilitation (n = 8). After exclusions, 85 rats were included in 1 of 8 groups (‘No VNS’ (n = 15), ‘Low VNS’ (n = 15), ‘Moderate VNS’ (n = 15), ‘High VNS’ (n = 15), ‘Arc No VNS’ (n = 7), ‘Arc VNS’ (n = 8), ‘ACh+; VNS’ (n = 4), ‘ACh−; VNS’ (n = 6)).
Statistics
The data was first tested for normality using the Kolmogorov–Smirnov test (KS test). Upon testing distributional variance using the Kolmogorov–Smirnov test, we found that the mean and variance of our data were the same as a normal distribution, so we used parametric statistical comparisons. Mechanical withdrawal thresholds were analyzed using a two-way repeated measures ANOVA, followed by post hoc Bonferroni-Corrected unpaired t-test where appropriate. Paired t-test were used to compare measurements within subjects from pre-injury to week eight post-injury time points, where applicable. An unpaired t-test was used to analyze Arc transcript levels. A Pearson’s correlation coefficient was used evaluate association of Arc levels and magnitude of recovery. In the figures, data are presented as mean ± standard error of the mean (SEM).
Results
We first sought to determine whether pairing VNS with tactile rehabilitation would improve somatosensory function in a current intensity-dependent manner. To do so, all rats underwent transection and repair of their median and ulnar nerves to induce chronic hyposensitivity in the ventral forepaw. As expected, withdrawal thresholds of the injured forepaw were significantly elevated 8 weeks after nerve injury (Fig. 1A; Before Injury v. After Injury; Paired t-test, t(58) = 1.67, p = 1.42 × 10–25).

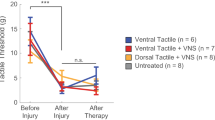
Moderate VNS improves recovery of somatosensory thresholds. (A) Nerve injury worsens withdrawal thresholds in all groups, indicative of chronic hyposensation. Moderate VNS paired with tactile rehabilitation (n = 15) enhances recovery compared to no stimulation with equivalent tactile rehabilitation after therapy (n = 15). Low (n = 15) and high (n = 15) intensity VNS fail to produce equivalent improvements in recovery. (B) Only moderate intensity VNS produces significant improvements in recovery. (C) Moderate intensity VNS results in the greatest proportion of animals exhibiting full recovery of withdrawal thresholds after therapy. *Indicates p < 0.05.
Animals were then assigned to groups and underwent 4 weeks of daily tactile rehabilitation with VNS delivered at a fixed low, moderate, or high intensity or no stimulation, as appropriate for their group. Group analysis of withdrawal threshold recovery revealed a significant effect of group (1-way repeated measures ANOVA, No VNS v. Low VNS v. Moderate VNS v. High VNS; F[4, 228] = 7.75, p = 7.3 × 10–3. No differences in withdrawal thresholds were observed across groups prior to beginning rehabilitation (Fig. 1A; Unpaired t-tests, No VNS v. Low VNS v. Moderate VNS v. High VNS; t(30) = 1.70, p = 0.84, t(30) = 1.70, p = 0.71, t(30) = 1.70, p = 0.99). Consistent with previous reports, Moderate VNS paired with tactile rehabilitation significantly decreased withdrawal thresholds compared to equivalent tactile rehabilitation without VNS (Fig. 1A; Unpaired t-test, No VNS After Therapy v. Moderate VNS After Therapy, t(28) = 1.70, p = 3.2 × 10–3). These findings confirm that pairing moderate intensity VNS with tactile rehabilitation improves recovery of somatosensory function.
We next tested if VNS delivered at lower or higher intensities would similarly improve recovery. Low intensity VNS delivered at 0.4 mA failed to improve recovery compared to no stimulation (Fig. 1A; Unpaired t-test, No VNS After Therapy v. Low VNS After Therapy, t(28) = 1.70, p = 0.33). Similarly, High VNS did not improve recovery compared to no stimulation (Fig. 1A; Unpaired t-test, No VNS After Therapy v. High VNS After Therapy, t(29) = 1.70, p = 0.12). At the end of therapy, the Moderate VNS group was the only group to demonstrate a significant percent recovery over No VNS (Fig. 1B; One-way ANOVA, F[3, 55], = 4.45, p = 7.2 × 10–3; Unpaired t-tests, Percent Recovery No VNS v. Low VNS, v. Moderate VNS, and High VNS; t(27) = 1.70, p = 0.12; t(28) = 1.70, p = 8.7 × 10–3; t(28) = 1.70, p = 0.14). Additionally, when we stratified animals by the magnitude of somatosensory recovery, a chi-squared test of independence revealed that moderate intensity VNS resulted in a greater proportion of fully recovered animals (as defined by a > 90% restoration of pre-injury withdrawal threshold), with 93% of animals demonstrating full recovery compared to the No VNS group where only 7% of animals completely recovered (Fig. 1C; χ2 Test for Independence, Degree of Recovery: No VNS v. Moderate VNS; χ2 (2, N = 30) = 12.1, p = 2.3 × 10–3). Low and high intensity VNS resulted in approximately 65% of animals with full recovery but the proportion of animals who made a complete recovery did not statistically differ from the No VNS group (Fig. 1C; χ2 Test for Independence, Degree of Recovery: No VNS v. Low VNS and High VNS; χ2 (2, N = 29) = 3.06, p = 0.22; X2 (2, N = 30) = 3.45, p = 0.18). These findings define an inverted-U relationship between stimulation intensity and recovery of somatosensory function.
We next tested if VNS-dependent improvements in somatosensory function would generalize to other measures of forelimb sensorimotor function. No improvements in forelimb use during spontaneous exploration or weight bearing were observed across groups (Fig. 2A, 1-way repeated measures ANOVA, F[1,49] = 0.12, p = 0.73; Fig. 2B, 1-way repeated measures ANOVA, F[1,51] = 2.1 × 10–4, p = 0.99). These findings suggest that VNS benefits do not generalize.

VNS-dependent recovery does not generalize to other measures of forelimb function. None of the tested VNS paradigms improved recovery of (A) volitional forelimb use during exploratory behavior or (B) weight bearing during locomotion. n.s. denotes no significant difference. n = 15 for each group.
The finding that VNS-dependent recovery exhibits an inverted-U relationship with stimulation intensity provides circumstantial evidence that plasticity may underlie recovery. In our second and third experiments, we sought to probe this mechanism more directly. Prior studies show that VNS paired with other forms of training modulates expression of proteins associated with synaptic plasticity, including Activity-regulated cytoskeleton-associated protein (Arc)35,36,37. Our second experiment assessed whether VNS paired with tactile rehabilitation increased the expression of Arc transcript in cortex compared to tactile rehabilitation without VNS in a separate cohort of animals. Because moderate intensity VNS produced the largest improvement in recovery, we utilized this parameter set in the subsequent experiments. A separate cohort of animals underwent one week of tactile therapy with either moderate intensity VNS (n = 8) or no stimulation (n = 7). Moderate VNS paired with tactile rehabilitation significantly increased Arc transcript levels in cortex compared to equivalent tactile training with no stimulation (Fig. 3A; Unpaired t-test, Arc No VNS v. Arc VNS; t(13) = 2.62, p = 0.021). Additionally, Arc transcript levels were weakly, but significantly, correlated with the degree of recovery (Fig. 3B; Pearson correlation, r2 = 0.27, p = 0.0492). The full RNAseq dataset is available in Supplementary Table 1. These observations are consistent with a scenario in which VNS-directed plasticity enables recovery.

VNS increases Arc mRNA transcript levels. (A) VNS paired with tactile rehabilitation (n = 8) significantly increases the levels of Arc mRNA in cortex compared to equivalent tactile rehabilitation without VNS (n = 7). (B) Arc mRNA levels are weakly, but significantly, correlated with the degree of forelimb somatosensory recovery. *Indicates p < 0.05. Data are presented as mean ± SEM in panel A, and panel B shows datapoints from individual subjects.
If indeed cortical plasticity underlies VNS-dependent recovery of somatosensory function after nerve injury, then manipulations that prevent this plasticity should block recovery. In our third experiment, we directly explored this in a separate cohort of animals using IgG-192-saporin to deplete forebrain acetylcholine, a common technique known to abrogate plasticity4,38. Animals underwent nerve injury as in the initial experiment and were randomized to receive either IgG-192-SAP injections to deplete acetylcholine (ACh-; Moderate VNS, n = 6) or vehicle injections (ACh + ; Moderate VNS, n = 4). All animals received equivalent moderate intensity VNS paired with tactile rehabilitation. ANOVA revealed a significant effect of treatment (1-way repeated measures ANOVA, VNS; ACh + v. VNS; ACh−, F[6,48] = 4.19; p = 2.9 × 10–5). After VNS therapy, animals with depletion of acetylcholine demonstrated significantly worse recovery compared to animals with intact cholinergic signaling (Fig. 4; Unpaired t-test, After Therapy; ACh+; VNS v. ACh−; VNS, t(8) = 9.93, p = 8.93 × 10–6). These findings are consistent with the hypothesis that VNS enhances somatosensory recovery by directing synaptic plasticity.

Blocking plasticity prevents VNS-dependent enhancement of somatosensory recovery. VNS paired with tactile rehabilitation significantly improves recovery of forelimb somatosensation in control rats (ACh+; VNS, n = 4). Depletion of forebrain acetylcholine, which blocks cortical plasticity, significantly impairs VNS-dependent recovery (ACh−; VNS, n = 6). **Indicates p < 0.001 across groups. Data are presented as mean ± SEM.
Discussion
In our first experiment, we characterized the effects of stimulation intensity on VNS-dependent enhancement of somatosensory recovery in a rat model of chronic sensory loss. Consistent with prior studies, we find that VNS, delivered at a moderate stimulation intensity, combined with tactile rehabilitation enhances recovery of forelimb somatosensory function. Higher and lower stimulation intensities fail to produce comparable improvements in recovery. The inverted-U relationship between stimulation intensity and recovery suggests that VNS-dependent enhancement of plasticity may underlie recovery. Consistent with this, we next show that VNS paired with tactile training enhances the levels of Arc transcript in somatosensory cortex, and that preventing plasticity blocks VNS-dependent recovery. Together, findings from these experiments reveal mechanisms that underlie VNS-dependent improvements in somatosensation and provide guidance to select optimal stimulation parameters for future use.
The core finding of this study confirms that moderate intensity VNS paired with tactile rehabilitation enhances recovery of somatosensation. These findings corroborate previous studies demonstrating VNS-dependent somatosensory improvements in both preclinical models and a pilot study in an individual with stroke, all of which utilize moderate intensity stimulation19,20,21,22,23. Additionally, we observe that lower and higher stimulation intensities fail to generate significant improvements in somatosensory recovery compared to tactile rehabilitation without stimulation. The findings provide a straightforward basis for selection of stimulation intensity for future use of this approach. Combined with prior work characterizing the parameters regarding timing and dose of VNS therapy21,22, as well as the influence of the paired tactile stimuli20, this study adds a critical dimension to optimizing VNS therapy for clinical implementation.
The inverted-U relationship of VNS intensity has been reported across a broad range of contexts, from memory enhancement to extinction learning to motor recovery28,39,40,41. A number of explanations could account for this phenomenon, but two likely schema, which have been described extensively in prior literature, involve either desensitizing or functionally opposing action of neuromodulatory networks39. Regardless of the specific molecular pathways, the pervasive occurrence of this phenomenon implies that VNS likely engages a common, central mechanism. Synaptic plasticity is a common denominator linking prior studies of VNS, such that VNS exhibits an inverted-U relationship with cortical plasticity25,26,27, and the effective parameters mirror those for VNS-dependent recovery of forelimb function28. We hypothesized that a similar enhancement of plasticity, when combined with tactile rehabilitation, would underlie recovery of somatosensory function. The observation of the inverted-U relationship reported here provides initial, though indirect, evidence of this mechanism.
This claim is bolstered by two experiments that more directly examine VNS-dependent plasticity. First, we observed that moderate VNS paired with tactile rehabilitation enhances expression of Arc transcript in the somatosensory cortex compared to tactile rehabilitation without VNS. Arc is an immediate early gene implicated in many canonical forms of synaptic plasticity37,42. The increase in Arc observed here is consistent with prior studies that report changes in Arc mRNA and protein levels with VNS delivery35,36. Moreover, the correlation of Arc mRNA levels and VNS-dependent enhancement of somatosensory recovery suggests that plasticity underlies recovery. If so, then manipulations that prevent plasticity should consequently block VNS-dependent recovery. We explored with hypothesis in a third experiment using targeted immunodepletion of acetylcholine, a technique known to prevent VNS-dependent plasticity17. We find that acetylcholine depletion blocks VNS-dependent enhancement of somatosensory recovery. Taken together, these three lines of evidence, the inverted-U relationship with intensity, the VNS-driven increase in Arc levels, and the abrogation of recovery when plasticity is limited, strongly indicate that VNS-dependent plasticity underlies recovery of somatosensory function.
These data corroborate a large body of literature pertaining to the mechanisms engaged by VNS therapy3,4,5,6,7,8,16,17,25,26,27,28,41. The general concept is that VNS drives phasic neuromodulatory release throughout the central nervous system to reinforce concurrent neural activity associated with rehabilitative training. Based on the necessity of neuromodulator release in the CNS and the stimulation intensity needed for VNS-dependent plasticity and recovery, it is likely that these actions are mediated by afferent (i.e., ascending) Aδ fibers in the vagus nerve. Future studies could utilize fiber-specific activation, such as with optogenetics, to more directly define the contribution of different classes of fibers. A clearer understanding of the target fibers, coupled with a validated biomarker, could provide a means to individualize stimulation in future applications. Additionally, given prior studies showing that implantation and nerve manipulation can have a detrimental impact on fibers in the vagus43,44, this may provide a means to ensure that any fiber damage does not inhibit the effects of VNS therapy.
VNS therapy recently received FDA approval to improve recovery of upper limb arm and hand function in individuals with chronic stroke, and a number of other applications of this approach are rapidly emerging. As VNS therapy is increasingly developed and translated to clinical use, a clear understanding of the mechanisms that underlie recovery is important for optimization. The findings from this study clarify the mechanisms engaged by VNS therapy to promote recovery of somatosensory function and provide clear guidelines for selecting effective stimulation parameters for future studies.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Engineer, N. D. et al. Targeted vagus nerve stimulation for rehabilitation after stroke. Front. Neurosci. 2019, 13. https://doi.org/10.3389/fnins.2019.00280 (2019).
Hays, S. A., Rennaker, R. L. & Kilgard, M. P. Targeting plasticity with vagus nerve stimulation to treat neurological disease. Prog. Brain Res. 207, 275–299. https://doi.org/10.1016/B978-0-444-63327-9.00010-2 (2013).
Hulsey, D. R. et al. Parametric characterization of neural activity in the locus coeruleus in response to vagus nerve stimulation. Exp. Neurol. 298, 21. https://doi.org/10.1016/j.expneurol.2016.12.005 (2016).
Hulsey, D. R. et al. Reorganization of motor cortex by vagus nerve stimulation requires cholinergic innervation. Brain Stimul. 9, 174–181. https://doi.org/10.1016/j.brs.2015.12.007 (2016).
Hulsey, D. R., Shedd, C. M., Sarker, S. F., Kilgard, M. P. & Hays, S. A. Norepinephrine and serotonin are required for vagus nerve stimulation directed cortical plasticity. Exp. Neurol. 320, 112975. https://doi.org/10.1016/j.expneurol.2019.112975 (2019).
Bowles, S. et al. Vagus nerve stimulation drives selective circuit modulation through cholinergic reinforcement. Neuron 110, 2867-2885.e7. https://doi.org/10.1016/J.NEURON.2022.06.017 (2022).
Mridha, Z. et al. Graded recruitment of pupil-linked neuromodulation by parametric stimulation of the vagus nerve. Nat. Commun. 12, 1–14. https://doi.org/10.1038/s41467-021-21730-2 (2021).
Collins, L., Boddington, L., Steffan, P. J. & McCormick, D. Vagus nerve stimulation induces widespread cortical and behavioral activation. Curr. Biol. 31, 2088-2098.e3. https://doi.org/10.1016/j.cub.2021.02.049 (2021).
Khodaparast, N. et al. Vagus nerve stimulation during rehabilitative training improves forelimb strength following ischemic stroke. Neurobiol. Dis. 60, 80. https://doi.org/10.1016/j.nbd.2013.08.002 (2013).
Hays, S. A. et al. Training Improves functional recovery after intracerebral hemorrhage. Stroke 45, 97–100. https://doi.org/10.1161/STROKEAHA.114.006654 (2014).
Hays, S. A. et al. The timing and amount of vagus nerve stimulation during rehabilitative training affect post-stroke recovery of forelimb strength. Neuroreport 25(9), 676–682. https://doi.org/10.1097/WNR.0000000000000154 (2014).
Khodaparast, N. et al. Vagus nerve stimulation during rehabilitative training improves forelimb recovery after chronic ischemic stroke in rats. Neurorehabil. Neural Repair 30, 676–684. https://doi.org/10.1177/1545968315616494 (2016).
Hays, S. A. et al. Vagus nerve stimulation during rehabilitative training enhances recovery of forelimb function after ischemic stroke in aged rats. Neurobiol. Aging https://doi.org/10.1016/j.neurobiolaging.2016.03.030 (2016).
Pruitt, D. T. et al. Vagus nerve stimulation delivered with motor training enhances recovery of function after traumatic brain injury. J. Neurotrauma 33, 871–879. https://doi.org/10.1089/neu.2015.3972 (2016).
Meyers, E. C. et al. Vagus nerve stimulation enhances stable plasticity and generalization of stroke recovery. Stroke 47, 710–717. https://doi.org/10.1161/STROKEAHA.117.019202 (2018).
Ganzer, P. D. et al. Closed-loop neuromodulation restores network connectivity and motor control after spinal cord injury. Elife 2018, 7. https://doi.org/10.7554/eLife.32058 (2018).
Meyers, E. C. et al. Enhancing plasticity in central networks improves motor and sensory recovery after nerve damage. Nat. Commun. 10, 1–14. https://doi.org/10.1038/s41467-019-13695-0 (2019).
Dawson, J. et al. Vagus nerve stimulation paired with rehabilitation for upper limb motor function after ischaemic stroke (VNS-REHAB): A randomised, blinded, pivotal, device trial. Lancet 397, 1545–1553. https://doi.org/10.1016/S0140-6736(21)00475-X (2021).
Darrow, M. J. et al. Restoration of somatosensory function by pairing vagus nerve stimulation with tactile rehabilitation. Ann. Neurol. 87, 194–205. https://doi.org/10.1002/ana.25664 (2020).
Darrow, M. J. et al. The tactile experience paired with vagus nerve stimulation determines the degree of sensory recovery after chronic nerve damage. Behav. Brain Res. 396, 112910. https://doi.org/10.1016/J.BBR.2020.112910 (2021).
Ruiz, A. D. et al. Vagus nerve stimulation must occur during tactile rehabilitation to enhance somatosensory recovery. Neuroscience 532, 79–86. https://doi.org/10.1016/J.NEUROSCIENCE.2023.09.015 (2023).
Ruiz, A. D. et al. Effective delivery of vagus nerve stimulation requires many stimulations per session and many sessions per week over many weeks to improve recovery of somatosensation. Neurorehabil. Neural Repair https://doi.org/10.1177/15459683231197412 (2023).
Kilgard, M. P., Rennaker, R. L., Alexander, J. & Dawson, J. Vagus nerve stimulation paired with tactile training improved sensory function in a chronic stroke patient. NeuroRehabilitation 42, 159–165. https://doi.org/10.3233/NRE-172273 (2018).
Borland, M. S. et al. Cortical map plasticity as a function of vagus nerve stimulation intensity. Brain Stimul. 9, 117. https://doi.org/10.1016/j.brs.2015.08.018 (2016).
Morrison, R. A. et al. Vagus nerve stimulation intensity influences motor cortex plasticity. Brain Stimul. 12, 256. https://doi.org/10.1016/j.brs.2018.10.017 (2019).
Morrison, R. A. et al. A limited range of vagus nerve stimulation intensities produce motor cortex reorganization when delivered during training. Behav. Brain Res. 391, 112705. https://doi.org/10.1016/J.BBR.2020.112705 (2020).
Morrison, R. A. et al. High intensity VNS disrupts VNS-mediated plasticity in motor cortex. Brain Res. 1756, 147332. https://doi.org/10.1016/J.BRAINRES.2021.147332 (2021).
Pruitt, D. T. et al. Optimizing dosing of vagus nerve stimulation for stroke recovery. Transl. Stroke Res. 12, 65–71. https://doi.org/10.1007/s12975-020-00829-6 (2021).
Darrow, M. J. et al. Restoration of somatosensory function by pairing vagus nerve stimulation with tactile rehabilitation. Ann. Neurol. 87(2), 194–205 (2020).
Meyers, E. C. et al. Median and ulnar nerve injuries reduce volitional forelimb strength in rats. Muscle Nerve 2017, 56. https://doi.org/10.1002/mus.25590 (2017).
Rios, M. U. et al. Protocol for construction of rat nerve stimulation cuff electrodes. Methods Protoc. 2019, 2. https://doi.org/10.3390/mps2010019 (2019).
Conner, J. M., Chiba, A. A. & Tuszynski, M. H. The basal forebrain cholinergic system is essential for cortical plasticity and functional recovery following brain injury. Neuron 46, 173–179. https://doi.org/10.1016/j.neuron.2005.03.003 (2005).
Ramanathan, D., Tuszynski, M. H. & Conner, J. M. The basal forebrain cholinergic system is required specifically for behaviorally mediated cortical map plasticity. J. Neurosci. 29, 5992–6000 (2009).
Conner, J. M., Kulczycki, M. & Tuszynski, M. H. Unique contributions of distinct cholinergic projections to motor cortical plasticity and learning. Cereb. Cortex 20, 2739–2748 (2010).
Alvarez-Dieppa, A. C., Griffin, K., Cavalier, S. & McIntyre, C. K. Vagus nerve stimulation enhances extinction of conditioned fear in rats and modulates arc protein, CaMKII, and GluN2B-containing NMDA receptors in the basolateral amygdala. Neural Plast. 2016, 4273280 (2016).
Sanders, T. H. et al. Cognition-enhancing vagus nerve stimulation alters the epigenetic landscape. J. Neurosci. 39, 3454–3469. https://doi.org/10.1523/JNEUROSCI.2407-18.2019 (2019).
Nikolaienko, O., Patil, S., Eriksen, M. S. & Bramham, C. R. Arc protein: A flexible hub for synaptic plasticity and cognition. Semin. Cell Dev. Biol. 77, 33–42. https://doi.org/10.1016/J.SEMCDB.2017.09.006 (2018).
Conner, J. M., Culberson, A., Packowski, C., Chiba, A. A. & Tuszynski, M. H. Lesions of the basal forebrain cholinergic system impair task acquisition and abolish cortical plasticity associated with motor skill learning. Neuron 38, 819–829. https://doi.org/10.1016/S0896-6273(03)00288-5 (2003).
Hays, S. A., Rennaker, R. L. & Kilgard, M. P. How to Fail with Paired VNS therapy (Elsevier, 2023).
Clark, K. B., Krahl, S. E., Smith, D. C. & Jensen, R. A. Post-training unilateral vagal stimulation enhances retention performance in the rat. Neurobiol. Learn. Mem. 63, 213–216 (1995).
Souza, R. R. et al. Vagus nerve stimulation enhances fear extinction as an inverted-U function of stimulation intensity. Exp. Neurol. 341, 113718. https://doi.org/10.1016/j.expneurol.2021.113718 (2021).
Shepherd, J. D. et al. Arc/Arg3.1 mediates homeostatic synaptic scaling of AMPA receptors. Neuron 52, 475–484. https://doi.org/10.1016/J.NEURON.2006.08.034 (2006).
Agnew, W. F. & Mccreery, D. B. Considerations for safety with chronically implanted nerve electrodes. Epilepsia 31, 27–32. https://doi.org/10.1111/j.1528-1157.1990.tb05845.x (1990).
Somann, J. P. et al. Chronic cuffing of cervical vagus nerve inhibits efferent fiber integrity in rat model. J. Neural Eng. 15, 036018. https://doi.org/10.1088/1741-2552/AAA039 (2018).
Acknowledgements
We would like to thank Alfonso Reyes for the construction of VNS stimulator cuffs. We also thank Megan White, Joseph Montefalcon, Ronse Raphi, Mamoon Aslam-Syed Mian, Nikit Valmiki, Immaculate Wambugu, Ayesha Yousaf, Sakina Husain, Afaf Nabeeha, and Abhishek Sule for their help in behavioral training and testing. We would like to thank Joseph Epperson for their assistance in generating supplemental images. Finally, thank you to David Pruitt his technical expertise and guidance throughout the experimental process.
Funding
This work was supported by the National Institutes of Health NIH R01 NS094384 (SAH) and by the Department of Defense Joint Program Committee 8/Clinical and Rehabilitative Medicine Research Program and the Congressionally Directed Medical Research Programs grant W81XWH-20-1-0863 (SAH).
Author information
Authors and Affiliations
Contributions
K.M.M.: Study design, surgical procedures, behavioral tests, supervision of data collection, data analysis, preparation of the figures and manuscript. A.D.R.: Study design, surgical procedures, behavioral tests, supervision of data collection. M.J.D.: Study design, behavioral tests, supervision of data collection, data analysis, preparation of the figures. T.T.D.: Surgical procedures. S.S.: Supervision of data collection, data analysis. F.N.A. and C.M.B.: Behavioral tests. B.T.S.: Behavioral tests, data analysis. T.J.P.: Supervision. R.L.R.: Supervision. S.A.H.: Conceptualization, study design, supervision, data analysis, and manuscript revisions. M.P.K.: Project administration, conceptualization, study design, data analysis, and manuscript revisions.
Corresponding author
Ethics declarations
Competing interests
MPK has a financial interest in MicroTransponder, Inc. RLR is the co-founder and CEO of XNerve, which is developing nerve stimulation therapies. The other authors declare that no competing interests exist.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Malley, K.M., Ruiz, A.D., Darrow, M.J. et al. Neural mechanisms responsible for vagus nerve stimulation-dependent enhancement of somatosensory recovery. Sci Rep 14, 19448 (2024). https://doi.org/10.1038/s41598-024-70091-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-70091-5
This article is cited by
-
Advice for translational neuroscience: move deliberately and build things
Bioelectronic Medicine (2025)
-
Vagus nerve stimulation: innovative applications in the field of hand function rehabilitation
Cognitive Neurodynamics (2025)
