
Abstract
Postoperative pain is a common concern following root canal treatments (RCT), impacting both patients and oral health practitioners. This systematic review and meta-analysis aimed to evaluate the effectiveness of laser treatment modalities in reducing postoperative pain compared to conventional methods after primary and secondary RCT in permanent mature teeth. A search of three electronic databases (PubMed, ScienceDirect, and The Cochrane Library) was conducted, using a broad range of keywords and terms. Gray literature and manual searches were conducted to complement the search. The inclusion criteria included randomized clinical trials based on the objective of the secondary study. A minimum sample size of 10 participants per group and a clearly defined criterion for postoperative pain assessment were required. The characteristics of the included studies were presented as tables. The Cochrane collaboration tool RoB 2.0 was used to assess the risk of bias within each study. Two reviewers extracted the data and assessed the studies independently, and discrepancies were resolved through consultation with a third reviewer. A random-effects model was employed for meta-analysis to estimate the overall effect measure. Heterogeneity was evaluated using Cochran’s Q test and the I2 index. Publication bias was explored via Funnel plots and Egger’s test. Subgroup analyses and meta-regression were conducted to assess variations among laser methods and examine the influence of independent factors. The significance threshold for all analyses was set at 5% (α = 0.05). Intraoral laser therapy demonstrated no significant advantage over conventional treatments but consistently outperformed placebo, particularly from 4 to 72 h post-treatment. Low-level laser therapy provided slight pain reduction in the first 8 h, though its effectiveness diminished in retreatment scenarios. Photodynamic therapy and laser disinfection showed marginal benefits, especially shortly after treatment, with reduced efficacy in longer-term or retreatment contexts. Further research is needed to explore different applications of laser modalities and assess distinct prognostic factors in more detail.
Similar content being viewed by others

Introduction
Root canal treatment (RCT) is a dental procedure prescribed to address infected or damaged tooth pulp, involving the process of pulp removal, thorough root canal cleaning, shaping, precise filling, and a secure seal to prevent further infection1,2. One frequently encountered challenge following RCT is the occurrence of postoperative pain or flare-ups3. This discomfort originating from these endodontically-treated teeth (ETT) can arise from various factors, including lingering infection, inflammation, or irritation of surrounding tissues during the procedure4,5. Symptoms of postoperative pain commonly include discomfort, swelling, and mild to moderate pain6,7.
Postoperative pain management after RCT comprises diverse strategies and interventions aimed at alleviating discomfort and pain arising after medical or surgical procedures4,8. These strategies fall into two primary categories: pharmacological and non-pharmacological approaches. Pharmacological options involve the use of non-steroidal anti-inflammatory drugs (NSAIDs)9, acetaminophen10, long-acting anesthetics11, and intracanal medications12. While these pharmacological approaches offer benefits, oral health professionals must carefully consider the most suitable approach for individual patients while minimizing associated medication risks13,14. Consequently, the demand for non-pharmacological adjunct therapies, such as anxiety reduction protocols15, cryotherapy16, and intracanal laser therapy17,18, has increased.
Among these adjunctive therapies for patients with ETT, laser and light-activated treatments have demonstrated remarkable versatility, offering a multitude of applications and methodologies19,20. These involve various treatments and techniques used to mitigate postoperative pain after endodontic procedures, including irrigation activation with Er: YAG lasers21, canal disinfection utilizing Nd: YAG or diode lasers17, photodynamic therapy (PDT)22, and photobiomodulation (PBM) or low-level laser therapy (LLLT)23. Reported benefits of such therapeutic approaches involve different light wavelengths being absorbed by tissue chromophores, resulting in cyclooxygenase-2 suppression and enhanced clearance of pain-inducing substances24,25. Moreover, laser treatment influences plasma membrane permeability to ions like sodium, potassium, and calcium26,27. This modulation in permeability reduces C fiber activity while elevating neuron action potentials, offering a molecular explanation for post-laser pain reduction26,27.
Previous reviews have examined the effects of laser treatments in endodontics, yet limitations exist in their scope and focus. Elafifi-Ebeid et al. (2023)28 restricted their analysis to studies on initial RCT, excluding those on root canal retreatment (re-RCT), and concentrated solely on intracanal laser irradiation, omitting LLLT and PBM. Guerreiro et al. (2021)29 included studies on LLLT but did not compare different laser treatment modalities, while Chen et al. (2019)30 focused exclusively on LLLT without considering other laser therapies. Meire et al. (2023)31 evaluated various adjunctive treatment modalities, such as ozone therapy and ultrasonically activated irrigation (UAI), without a sole emphasis on laser treatments. Lastly, Alonaizana & AlFawaz (2019)32 examined the impact of PDT on postoperative endodontic pain management, but their systematic review had significant limitations, including a limited number of included studies and a qualitative analysis approach, and many of the clinical studies lacked specific control or comparison groups, making it challenging to determine the true impact. Therefore, the present systematic review aimed to assess the efficacy of various laser-dependent treatment modalities in diminishing postoperative pain subsequent to primary and secondary RCTs in comparison to conventional methods, according to the available randomized clinical trials and perform a meta-analysis.
Materials and methods
Protocol and registration
This systematic review is registered in the PROSPERO international prospective database of systematic reviews in health and social care under the registration identification number CRD42023415417. The secondary study adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, ensuring comprehensive and transparent reporting33.
Eligibility criteria
Population, Intervention, Comparison, Outcome, Timing, and Setting (PICOTS), were used to structure research questions and define key elements. The primary research question guiding this review is: “To what extent do various laser-dependent treatment modalities effectively reduce postoperative pain following both primary and secondary root canal treatments in comparison to conventional methods?”.
Search strategy
An electronic search was conducted across three different databases: PubMed (National Center for Biotechnology Information, U.S. National Library of Medicine), ScienceDirect (Elsevier, Relx Group plc.), and The Cochrane Library (John Wiley & Sons, Ltd). This search was conducted without imposing any language or publication date restrictions, thus ensuring the inclusion of a broad spectrum of relevant literature. In addition, gray literature search was performed in three grey engines: CADTH’s Grey Matters (https://greymatters.cadth.ca/), the European database on medical devices from the European Commission (https://ec.europa.eu/tools/eudamed/#/screen/home), and The New York Academy of Medicine Library (https://catalog.nyam.org/cgi-bin/koha/opac-search.pl).
A manual search complemented the search to ensure a thorough exploration and identification of relevant information. Two review authors (H.S and R.A) carried out the search process and study inclusion. In instances where a consensus was not readily reached between the two review authors, a third review author (F.E. or K.I.A.) served as an impartial arbitrator to resolve any discrepancies. The following search keywords were utilized to formulate the search strategy.
Eligibility criteria
Only randomized clinical trials comparing laser-dependent treatment modalities to conventional methods for reducing postoperative pain following primary or secondary root canal treatment were considered. The primary outcome of interest was postoperative pain, which had to be assessed using well-defined criteria. Inclusion criteria required a minimum sample size of 10 participants per group, and all interventions had to be performed on mature permanent teeth.
Data extraction
After reviewing the titles and abstracts of the search results, articles that potentially met the inclusion criteria were subjected to full-text examination. The following study characteristics and data were extracted: study name, sample size, age, sex, diagnosis, laser treatment method, instrument for documenting postoperative pain, pain scale measurement, anesthetic type, tooth type, and treatment type. Postoperative pain assessments were categorized into seven distinct time points: 4–6 h, 8 h, 12 h, 24–30 h, 48–72 h, 4–5 days, and 7 days post-treatment. Pain severity was further stratified into four levels using the quantitative data from the pain assessment instrument: no pain (0), mild pain (0.1–3.9) or (1–39), moderate pain (4-6.9) or (40–69), and severe pain (7–10) or (70–100). In cases of disagreement, consensus was achieved through discussions involving two review authors (H.S and R.A), with a third review author (F.E. or K.I.A.) providing resolution when needed.
Quality assessment
To assess the risk of bias, two review authors (H.S and R.A) independently conducted quality assessments for each of the included studies. Given that this review exclusively considered randomized clinical trials, the evaluation of bias risk followed The Cochrane Collaboration’s RoB 2.0 tool34. Discrepancies were resolved through consultation with a third review author (F.E. or K.I.A.).
Statistical analysis
Our quantitative analysis comprised several key components, which included meta-analysis, heterogeneity analysis, publication bias assessment, and subgroup analysis. The meta-analysis was conducted using a random-effects model. This allowed us to estimate the overall effect measure, specifically the raw rate of patients experiencing null or mild pain, for both the laser and conventional treatment groups. To estimate heterogeneity, we utilized a restricted maximum likelihood estimator.
Our findings were visually represented using forest plots, complete with 95% confidence intervals. To further assess heterogeneity among the studies, we applied Cochran’s Q test. Additionally, we calculated the I² index, which signifies the proportion of between-studies variability relative to the total variability. The funnel plot analysis was conducted to explore the potential presence of publication bias. To measure the impact of such bias, Egger’s test was applied. Throughout the analyses, a significance level of 5% (α = 0.05) was applied. We utilized R 3.5.1, a statistical computing software, for all calculations and data processing35. Subgroup analysis was undertaken for several comparisons:
Comparison between laser and control groups. Odds ratio (OR) was calculated as the effect measure, expressed as log OR due to its symmetric and normal characteristics. This analysis was conducted using a random-effects model, yielding corresponding Z statistics, p-values, and 95% confidence intervals, all visualized through forest plots.
Comparison between individual laser methods. We utilized the ‘Log OR’ from each study to assess the benefits of specific laser methods compared to their respective control groups. This standardized measure allowed for direct comparison between different articles. A mixed-effects model (meta-regression) was used with the moderator variable ‘type of laser method.’
Effect of other factors. A meta-regression analysis was conducted using mixed-effects models to assess the influence of various moderator variables. These included mean age, gender distribution (% of males), anesthetic solution, tooth type (% in different positions), and the type of RCT. R² was calculated to quantify the extent to which each factor explained between-studies variability.
Results
Study selection
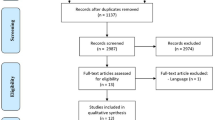
The study selection process was structured as depicted in Fig. 1 of the PRISMA flow diagram. Initially, the comprehensive literature search based on a strategy featuring including relevant keywords and MeSH terms (Table 1), resulted in a substantial pool of 7,288 studies aimed at addressing our focused research inquiry. To ensure the integrity of our dataset, diligent removal of duplicate entries was performed, resulting in the elimination of 7,198 redundant studies. Subsequently, the remaining studies underwent a rigorous assessment based on their titles and abstracts, applying the predefined inclusion criteria. Thereafter, this rigorous evaluation process culminated in the identification of 21 studies that merited comprehensive scrutiny through full-text analysis. Within this subset, four studies were deemed ineligible and were consequently excluded (Table 2). Ultimately, this qualitative synthesis encompassed a comprehensive review of the findings from the remaining 17 studies, which were included in the final qualitative synthesis.

PRISMA flow diagram: visual representation of the study selection process.
Study characteristics
Summary of the included studies is presented in Table 3, comprising randomized clinical trials that compared the efficacy of laser-dependent treatment modalities to conventional methods for mitigating postoperative pain after both primary and secondary root canal procedures. The laser wavelength and activation protocols of the included studies are presented in Table 4. Among the various laser treatment modalities, PDT and PBM were most frequently investigated, appearing in 7 and 5 studies, respectively. Additionally, three studies examined disinfection of the root canal system using Diode or Nd: YAG lasers, while two studies focused on irrigation activation with Er: YAG lasers.
Regarding the assessment of postoperative pain, the Visual Analogue Scale (VAS) emerged as the predominant instrument, as it was used in 12 out of the 17 studies. Other utilized instruments incorporated the Verbal Rating Scale (VRS), Numerical Rating Scale (NRS), Heft Parker pain survey, and evaluation of pain on percussion. These studies collectively form the basis for our comprehensive analysis of the effectiveness of laser-dependent treatment modalities in alleviating postoperative pain following root canal treatments.
Risk of bias assessment
The Cochrane collaboration tool RoB 2.0 was used to assess the risk of bias across the included studies. Of the 17 studies reviewed, 10 demonstrated an overall low risk of bias across all assessed domains (Fig. 2). In contrast, four studies received an assessment of “some concern” in specific domains, thus, were rated with an overall assessment of “some concerns.”

Risk of bias assessment via Cochrane’s collaboration tool RoB 2. Domains: D1, Randomization process; D2, Deviations from intended intervention; D3, Missing outcome data; D4, Measurement of the outcome; D5, Selection of the reported result. Assessors’ judgement: , High;
, High; , Some concerns;
, Some concerns; , Low.
, Low.
Furthermore, three studies were identified as having an overall high risk of bias (Fig. 2). Among these studies, the most frequently observed domain with a high risk of bias was the “deviation from intended interventions,” followed by “measurement of outcome,” and subsequently, “selection of reported results.” A comprehensive summary of the risk of bias assessment for all 17 studies is presented in Supplementary Table 1.
Findings form the quantitative analysis
Normalization included mapping scores from different pain scales (VRS, NRS, and Heft Parker) onto a common scale for unified comparison with the VAS. This facilitated a comprehensive synthesis of diverse pain assessment metrics.
Subgroup meta-analyses assessed the efficacy of combined intraoral laser therapy relative to control groups (conventional treatment and placebo) over several time periods (Fig. 3). While laser therapy was marginally more effective than conventional treatment at 8 h (Fig. 3b), 24–30 h (Fig. 3d), and 48–72 h (Fig. 3e), these differences were not statistically significant. However, laser therapy significantly outperformed placebo consistently up to 48 h. For instance, there were significant statistical differences at several time intervals: at 4 to 6 h, the odds ratio (OR) was 11.1 (95% CI: 2.69–45.6) with p < 0.001; at 8 h, the OR was 12.9 (95% CI: 252.1-660003) with p < 0.001; at 12 h, the OR was 11.2 (95% CI: 2.51–49.9) with p = 0.002; and at 24 h, the OR was 15.9 (95% CI: 1.34–190.6) with p = 0.029. Particularly, when comparing combined controls, laser therapy demonstrated a significant advantage from 4 to 72 h.

Subgroup meta-analysis comparing intraoral laser therapy to conventional treatment and placebo at intervals: (a) 4–6 h, (b) 8 h, (c) 12 h, (d) 24–30 h, (e) 48–72 h, and (f) 7 days.
LLLT was evaluated solely against placebos, without comparison to conventional treatments. The analysis differentiated effects in initial RCT, re-RCT, and combined scenarios across several intervals (Fig. 4). Although results were not statistically significant at any time point, combined data showed a marginal preference for LLLT at 4–6 h (OR = 1.92 [95%CI: 0.29–12.9]; p = 0.501) and 8 h (OR = 1.29 [95%CI: 0.34-5.00]; p = 0.702). Conversely, LLLT was slightly less favorable at 48–72 h (OR = 0.73 [95%CI: 0.16–3.22]; p = 0.672), particularly in the re-RCT scenario (OR = 0.64 [95%CI: 0.11–3.71]; p = 0.618).

Subgroup meta-analysis of low-level laser therapy versus placebo for managing postoperative pain analyzing initial root canal treatment and retreatment scenarios across intervals: (a) 4–6 h, (b) 8 h, (c) 12 h, (d) 24–30 h, (e) 48–72 h, and (f) 7 days. Note: The 4 to 5-day interval has been excluded from the diagram due to insignificance and space constraint.
Figure 5 illustrates a meta-analysis comparing PDT to conventional treatment and placebo over three time-intervals: 24–30 h, 48–72 h, and 7 days. PDT showed a marginally better outcome than conventional treatment at 24–30 h (Fig. 5a; p = 0.597) and placebo at the same interval (Fig. 5b; p = 0.143), though these differences were not statistically significant.

Subgroup meta-analysis of photodynamic therapy compared with placebo andconventional treatments for postoperative pain management at specific intervals: (a) 24-30 hrs with conventional treatment, (b) 24-30 hrs with placebo, (c) 48-72 hrs withconventional treatment, (d) 48-72 hrs with placebo, (e) 7 days with conventionaltreatment, and (f) 7 days with placebo.
In the subgroup meta-analyses assessing laser disinfection post-operativepain, only placebos served as controls due to the absence of conventionaltreatments in the available literature. Initial RCTs and re-RCTs were analyzedboth separately and together (Fig. 6). Laser disinfection showed a significantbeneficial effect in most RCT intervals, except at 7 days. In contrast, lasers inre-RCT studies had neutral effects. Remarkably, the earliest time interval (i.e.,12 hrs) included only RCTs, showing a substantial benefit from lasers (Fig. 6a;OR = 11.2 [95%CI: 2.51-49.9]; p = 0.001). However, the latest time interval (i.e., 7days) did not demonstrate significant differences (Fig. 6d; OR = 4.48 [95%CI:0.66-30.3]; p = 0.124). For combined RCT and re-RCT results, significantadvantages of laser disinfection over placebo were observed at 24-30 h Fig. 6b; OR = 11.0 [95%CI: 2.56-47.9]; p = 0.001) and 48-72 h Fig. 6c;OR = 6.69 [95%CI: 1.27-35.5]; p = 0.025).

Subgroup meta-analysis of disinfection versus placebo for postoperative pain in root canal treatment (RCT) and retreatment (re-RCT) scenarios across various intervals: (a) placebo at 12 h in RCT, (b) placebo at 24–30 h in RCT, (c) placebo at 24–30 h in both RCT and re-RCT, and (d) placebo at 7 days in RCT.
In the subgroup analysis for irrigation activation using Er: YAG, data were available for only two time-intervals: one study at 24–30 h and another at 48–72 h, both comparing the laser to conventional treatments as the control group (Fig. 7). The first interval showed no significant differences (p = 0.314), whereas the second interval demonstrated significant improvements with the laser (p < 0.001).

Subgroup analysis for irrigation activation using Er: YAG versus conventional for postoperative pain in root canal treatment scenarios across various intervals: (a) At 24–30 h and (b) At 48–72 h.
Meta-regression analyses compared the efficacy of combined laser treatments at the 24–30-h interval against conventional treatments and placebo (Suppl. Fig. S1a), as well as against these combined controls (Suppl. Fig. S1b). The first meta-regression revealed that lasers significantly reduced pain compared to placebo, showing a 32.4% higher rate of ‘no/mild pain’ in the laser group (p = 0.036). No significant differences were observed between laser and conventional methods (p = 0.172) or between conventional and placebo methods (p = 0.658). The second meta-regression also indicated significant improvements with lasers, with a 28.9% increase in ‘no/mild pain’ rates compared to combined controls (p = 0.026). Additionally, a meta-regression analysis s conducted to assess the impact of various independent factors, including mean age, gender distribution (percentage of males), anesthetic solution, tooth position diversity (percentage of different positions), and treatment type. Among these factors, only tooth position showed a statistically significant influence, indicating that upper maxillary teeth achieved superior outcomes when treated with laser modalities (p = 0.079).
Discussion
Postoperative pain following endodontic procedures is a significant concern for both patients and oral health providers40. The incidence of acute pain after RCT can vary widely, ranging from 1–65%41. This wide range can be attributed to the multifactorial nature of pain41. The primary cause of postoperative pain after RCT in ETT is the inflammatory response triggered by injury to the periapical tissues42,43. Such injury can result from mechanical, chemical, and microbial factors42,43. Endodontic interventions, through the disruption of periapical tissues, may induce therelease inflammatory mediators into the periapical tissues, including prostaglandins, leukotrienes, bradykinin, platelet-activating factor, and substance P, all of which can directly stimulate or sensitize nociceptors, leading to pain44– 46. To enhance patient comfort and the overall success of RCTs, general dental practitioners and endodontists utilize various measures to minimize these contributing factors. These measures include the use of appropriate techniques, medications, and materials, as well as patient education and communication, which are essential for managing expectations and addressing any concerns related to post-treatment pain40,44. Thus, the present systematic review and meta-analysis represent an effort in evaluating the effectiveness of laser treatment modalities in reducing postoperative pain after both primary and secondary endodontic treatments compared to conventional methods.
The literature on laser treatments in endodontics has various limitations. Meire et al.31 evaluated several adjunctive treatment modalities, such as ozone therapy and UAI, without exclusively focusing on laser treatments. Guerreiro et al. (2021)29 included studies on LLLT but did not compare different laser treatment methods. Elafifi-Ebeid et al. (2023)28 limited their analysis to RCT studies, excluding re-RCT, and focused solely on intracanal laser irradiation, overlooking LLLT and PBM. Chen et al. (2019)30 emphasized LLLT exclusively, neglecting other laser therapies. Lastly, Alonaizana & AlFawaz (2019)32 appraised the impact of PDT on postoperative endodontic pain management but faced limitations, including a scarcity of studies and a qualitative analysis approach, with many clinical studies lacking specific control or comparison groups.
Laser applications in reducing postoperative pain in endodontics consist of various techniques. These techniques range from external laser application to the apices of affected teeth, as seen in PBM or LLLT47,48, to disinfecting the canals through the activation of a photosensitizer using a laser with a specific wavelength, as in the case of PDT49,50, or simply disinfecting the radicular canal or activating irrigation solution using a direct laser source like Er: YAG (Fig. 7) or Diode lasers21,51. Our meta-analyses suggest that various laser treatments may have advantages in reducing postoperative pain compared to conventional techniques. These methods show potential benefits, particularly in the early postoperative intervals, and often outperform placebo treatments. However, the current evidence has some limitations, and further studies are needed to confirm these findings51– 62. PBM, in particular, is a therapeutic technique involving the application of low levels of red and near-infrared light to stimulate cellular processes47,48. PBM functions by reducing the production of inflammatory prostaglandins, interleukin 1β, and TNF-alpha63,64, which are known to contribute to the inflammatory processes often associated with pain. In the current meta-analysis, PBM significantly reduced postoperative pain following endodontic procedures when compared to conventional techniques. Notably, PBM was the most frequently employed laser treatment modality, with 7 studies utilizing this technique23,53,55,51,60,61,65 This prevalence suggests the ease of use, safety, and the non-toxic, non-allergenic nature of PBM treatment.
PDT is a medical treatment that involves the use of a photosensitizer, a light-sensitive compound placed inside the radicular canal, typically in the form of a gel or liquid49,50. Once applied, a specific wavelength of light is directed onto the treated area, activating the photosensitizer. This activation process leads to the generation of singlet oxygen and other reactive oxygen species (ROS)66,67, highly reactive compounds that can damage and effectively kill bacterial cells66,67. Furthermore, PDT has been found to influence the permeability of the cell membrane to ions such as calcium (Ca2+), sodium (Na+), and potassium (K+). These alterations can impact various cellular processes, including signal transduction and membrane potential26,27, leading to the enhanced degradation of the bradykinin peptide, a contributor to inflammation reduction, particularly pain reduction26,27. Additionally, changes in permeability can boost the activity of cellular receptors, potentially triggering the production of natural pain-relieving endorphins26,27. The findings from the present secondary study demonstrated the effectiveness of PDT in reducing postoperative pain following endodontic procedures. These results are consistent with a prior review by Alonaizana & AlFawaz (2019)32, which examined the impact of PDT on postoperative endodontic pain management. However, it is important to note that the previous review had limitations, including a limited literature search involving only 30 studies. Additionally, the review by Alonaizana & AlFawaz (2019)32 includes various types of clinical studies without specific control or comparison groups to assess the effect of PDT. Moreover, no statistical analysis was performed to determine the true impact of the qualitative data collected.
Our meta-analysis findings indicate that while intracanal laser therapy does not show a significant improvement over conventional treatments, it consistently outperforms placebo and demonstrates notable benefits when combined with controls, particularly in the short-term postoperative period (4 to 72 h). Subgroup analyses reveal that LLLT shows a slight, albeit non-significant, preference for pain reduction at 4–6 and 8 h post-treatment. However, its effectiveness diminishes over longer periods, especially in re-RCTs. These findings are corroborated by meta-regression analyses at 24–30 h, where laser treatments significantly improved ‘no/mild pain’ outcomes compared to placebo and combined controls (Suppl. Fig. S1a). This aligns with previous studies suggesting that LLLT can provide short-term pain relief, likely due to its anti-inflammatory effects and the promotion of cellular repair mechanisms68,69.
Our analysis indicates that PDT marginally outperforms conventional treatment and placebo at 24–30 h, though the results were not statistically significant (Fig. 5). The mechanism of PDT involves the activation of photosensitizers by light, producing reactive oxygen species that can reduce bacterial load and inflammation70. While these biological effects suggest a potential for pain reduction, our data suggests that the clinical benefits of PDT for postoperative pain management in endodontics are limited and require further investigation. Laser disinfection showed significant pain reduction shortly after treatment in root canal therapies, particularly in the early postoperative intervals. However, there were no significant benefits in retreatment scenarios or over extended periods, such as seven days (Fig. 6). The immediate pain relief observed may be attributed to the bactericidal effects of lasers, which can reduce the microbial load within the root canal system, thereby decreasing inflammation and pain71,72. However, the lack of sustained pain relief over longer periods suggests that the initial benefits of laser disinfection are transient.
The risk of bias assessment across the included studies indicated ‘some concerns’ (Fig. 2), primarily due to the limited number of studies available for certain comparisons and potential methodological weaknesses. This demonstrated the need for more high-quality randomized controlled trials to confirm the efficacy of laser therapies in postoperative pain management.
From a clinical perspective, the findings suggest that while laser therapies, particularly LLLT and laser disinfection, can provide short-term pain relief following endodontic procedures, their long-term benefits are less clear. Practitioners may consider incorporating these modalities as adjunctive treatments for immediate postoperative pain management, especially in cases where conventional methods are insufficient. However, the limited long-term effectiveness observed warrants cautious application and emphasizes the need for continued research to optimize these therapies for clinical use.
In the present meta-analysis, the utilization of Er: YAG laser, particularly through the activation of irrigation solution, has emerged as a more efficacious approach when compared to other laser treatment modalities. This superiority can be attributed to the fact that laser systems, such as the Er: YAG laser, result in minimal extrusion of the irrigation solution from the apical foramen73,74. This reduced liquid extrusion is of significant advantage, as excessive extrusion may precipitate postoperative complications. Furthermore, laser-activated irrigation techniques have been demonstrated to generate remarkably low intra-canal pressure, typically not exceeding central venous blood pressure (approximately 5.88 mmHg)75,76 The maintenance of such low intra-canal pressure is considered advantageous as it mitigates the risk of complications associated with high-pressure irrigation. Additionally, as previously elucidated, lasers in general, and laser-activated irrigation specifically, have shown effectiveness in eradicating and disinfecting bacteria within the root canal system, notably eliminating Enterococcus faecalis, a common bacterium found in infected root canals77,78. This antimicrobial action not only contributes to enhanced disinfection during RCT procedures but also potentially results in diminished postoperative pain originated form these ETT. However, it is necessary to acknowledge that further clinical studies directly comparing these different laser treatment modalities are requisite to draw a definitive conclusion regarding their comparative effectiveness in reducing postoperative pain in endodontic procedures79,80.
Moreover, the meta-regression analysis identified tooth position as the only factor with a statistically significant influence on the outcomes of laser treatments in endodontics, with upper maxillary teeth achieving superior results. This suggests that maxillary anterior teeth experienced significantly less postoperative pain, potentially due to the cancellous nature of the maxillary bone allowing for better laser penetration and more effective treatment and the anatomical and physiological characteristics of maxillary teeth, such as their vascularization and neural networks, may contribute to the observed pain reduction81,82. While this is the best available evidence within the limitations of our review, further research is needed to confirm these findings and elucidate the underlying mechanisms. To sum up, this meta-analysis cautiously underscores the potential of intraoral laser therapies to enhance short-term pain management after endodontic treatments.
Limitations of the secondary study
This systematic review does have some limitations, primarily originating from the grouping of various laser treatment modalities into a single category. It can be argued that the diverse applications of laser in distinct manners warrant separate examination, given the substantial differences in their mode of application. While these therapies outperform placebo and show promise in the immediate postoperative period, their long-term benefits remain uncertain.
Some conventional groups in the primary studies may include ultrasonic cleansing22,52,54 introducing a potential confounding factor as it represents an additional evaluated step.
Consequently, a comprehensive exploration of all potential prognostic factors was not feasible, despite the observed statistical homogeneity across the studies. Moreover, the absence of studies directly comparing these distinct laser treatment modalities presents a limitation.
Recommendations for future research
As a prospective recommendation for future research, it is advisable to conduct randomized clinical trials that rigorously compare the diverse laser treatment modalities within a standardized setting. These trials should establish specific parameters for laser utilization, employ a consistent tool for documenting postoperative pain, and implement strict inclusion criteria to differentiate between symptomatic and asymptomatic patients. Such an approach would contribute to a better understanding of the comparative effectiveness of these laser modalities and potentially address the limitations found in this review. Also, future research should focus on exploring the mechanisms underlying the transient effects of laser treatments to develop more effective and sustained pain management strategies in endodontics.
Conclusions
Our review assessed the efficacy of laser-based treatments for postoperative pain management in primary and secondary root canal therapies, concluding that:
-
Intraoral laser therapy showed no significant advantage over conventional treatments but consistently outperformed placebo and was truly beneficial when combined with controls from 4 to 72 h.
-
Low-level laser therapy provided slight pain reduction during the first 8 h post-treatment, with decreased effectiveness in retreatment scenarios.
-
Photodynamic therapy marginally outperformed conventional treatment and placebo at 24–30 h.
-
Laser disinfection achieved significant pain relief shortly after treatment, especially in early postoperative periods, with reduced benefits in longer-term or retreatment scenarios.
-
Meta-regression analysis indicated lasers significantly reduced pain compared to placebo, showing a 32.4% higher rate of ‘no/mild pain’ in the laser group (p = 0.036). Additionally, there were significant improvements with lasers, with a 28.9% increase in ‘no/mild pain’ rates compared to combined controls (p = 0.026).
-
Studies included had ‘some concerns’ regarding bias, with some analyses based on a limited number of studies.
-
A significant influence of tooth position as a prognostic factor was observed, with maxillary anterior teeth displaying improved outcomes with laser treatment modalities.
Therefore, the best evidence showed that potential benefits of laser treatments in reducing postoperative pain following root canal therapies. However, further research, including randomized clinical trials with standardized methodologies, is needed to explore the various laser applications and impacts of distinct prognostic factors in greater depth.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Nascimento, G. G. et al. Comparison of the effectiveness of single- and multiple-sessions disinfection protocols against endotoxins in root canal infections: Systematic review and meta-analysis. Sci. Rep. 11 (1), 1226. https://doi.org/10.1038/s41598-020-79300-3 (2021).
Sjögren, U., Figdor, D., Persson, S. & Sundqvist, G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int. Endod. J. 30, 297–306. https://doi.org/10.1046/j.1365-2591.1997.00092.x (1997).
Yoldas, O., Topuz, A., Isc¸ i, A. S. & Oztunc, H. Postoperative pain after endodontic retreatment: Single-versus two-visit treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 98, 483–487. https://doi.org/10.1016/j.tripleo.2004.03.009 (2004).
Torabinejad, M. et al. Factors associated with endodontic interappointment emergencies of teeth with necrotic pulps. J. Endod. 14, 261–266. https://doi.org/10.1016/S0099-2399(88)80181-X (1988).
Chagas Carvalho Alves, N. et al. Influence of occlusal reduction on pain after endodontic treatment: A systematic review and meta-analysis. Sci. Rep. 11 (1), 14019. https://doi.org/10.1038/s41598-021-93119-6 (2021).
Imura, N. & Zuolo, M. Factors associated with endodontic flare-ups: A prospective study. Int. Endod. J. 28, 261–265. https://doi.org/10.1111/j.1365-2591.1995.tb00311.x (1995).
Walton, R. & Fouad, A. Endodontic interappointment flare-ups: A prospective study of incidence and related factors. J. Endod. 18, 172–177. https://doi.org/10.1016/S0099-2399(06)81413-5 (1992).
Nosrat, A., Dianat, O., Verma, P., Nixdorf, D. R. & Law, A. S. Postoperative pain: An analysis on evolution of research in half-century. J. Endod. 47, 358–365. https://doi.org/10.1016/j.joen.2020.11.021 (2021).
Torabinejad, M. et al. Effectiveness of various medications on postoperative pain following root canal obturation. J. Endod. 20, 427–431. https://doi.org/10.1016/S0099-2399(06)80031-2 (1994).
Arslan, H., Gundogdu, E. C. & Sumbullu, M. The effect of preoperative administration of antihistamine, analgesic and placebo on postoperative pain in teeth with symptomatic apical periodontitis: A randomized controlled trial. Eur. Endod. J. 2–6. https://doi.org/10.5152/eej.2016.16012 (2016).
Ryan, J. L. et al. Gender differences in analgesia for endodontic pain. J. Endod. 34, 552–556. https://doi.org/10.1016/j.joen.2008.01.021 (2008).
Ehrmann, E. H., Messer, H. H. & Adams, G. G. The relationship of intracanal medicaments to postoperative pain in endodontics. Int. Endod. J. 36, 868–875. https://doi.org/10.1111/j.1365-2591.2003.00735.x (2003).
Coyle, D. T. et al. Opioidcanalgesic dose and the risk of misuse, overdose, and death: A narrative review. Pharmacoepidemiol. Drug Saf. 27, 464–472. https://doi.org/10.1002/pds.4366 (2018).
Ather, A., Patel, B., Gelfond, J. A. L. & Ruparel, N. B. Outcome of pulpotomy in permanent teeth with irreversible pulpitis: A systematic review and meta-analysis. Sci. Rep. 12 (1), 19664. https://doi.org/10.1038/s41598-022-20918-w (2022).
Gatchel, R. J. Managing anxiety and pain during dental treatment. J. Am. Dent. Assoc. 123, 37–41. https://doi.org/10.14219/jada.archive.1992.0194 (1992).
Keskin, C., Ozdemir, O., Uzun, I. & Guler, B. Effect of intracanal cryotherapy on pain after single-visit root canal treatment. Aust. Endod. J. 43, 83–88. https://doi.org/10.1111/aej.12175 (2016).
Koba, K. et al. A clinical study on the effects of pulsed nd:YAG laser irradiation at root canals immediately after pulpectomy and shaping. J. Clin. Laser Med. Surg. 17, 53–56. https://doi.org/10.1089/clm.1999.17.53 (1999).
Kreisler, M. B., Haj, H. A., Noroozi, N. & Willershausen, B. Efficacy of low level laser therapy in reducing postoperative pain after endodontic surgery–A randomized double blind clinical study. Int. J. Oral Maxillofac. Surg. 33, 38–41. https://doi.org/10.1054/ijom.2002.0449 (2004).
Huang, Q., Li, Z., Lyu, P., Zhou, X. & Fan, Y. Current applications and future directions of lasers in endodontics: A narrative review. Bioengineering 10, 296. https://doi.org/10.3390/bioengineering10030296 (2023).
Mohammadi, Z. Laser applications in endodontics: An update review. Int. Dent. J. 59, 35–46 (2009). PMID: 19323310.
Erkan, E., Gündoğar, M., Uslu, G. & Özyürek, T. Postoperative pain after SWEEPS, PIPS, Sonic and ultrasonic-assisted irrigation activation techniques: A randomized clinical trial. Odontology 110, 786–794. https://doi.org/10.1007/s10266-022-00700-0 (2022).
Vilas-Boas, L., Cozer, V., Tawil, P. Z. & Coelho, M. S. Effect of photodynamic therapy on postoperative pain in posterior teeth with symptomatic apical periodontitis. Photodiagnosis Photodyn. Ther. 35, 102348. https://doi.org/10.1016/j.pdpdt.2021.102348 (2021).
Arslan, H., Doğanay, E., Karataş, E., Ünlü, M. A. & Ahmed, H. M. A. Effect of low-level laser therapy on postoperative pain after root canal retreatment: A preliminary placebo-controlled, triple-blind, randomized clinical trial. J. Endod. 43, 1765–1769. https://doi.org/10.1016/j.joen.2017.06.028 (2017).
Wickenheisser, V. A. et al. Laser light therapy in Inflammatory, Musculoskeletal, and Autoimmune Disease. Curr. Allergy Asthma 19, 37. https://doi.org/10.1007/s11882-019-0869- (2019).
Pires, D. et al. Low-level laser therapy (LLLT; 780 nm) acts differently on mRNA expression of anti- and pro-inflammatory mediators in an experimental model of collagenase-induced tendinitis in rat. Lasers Med. Sci. 26, 85–94. https://doi.org/10.1007/s10103-010-0811-z (2011).
Pozza, D. H. et al. Analgesic action of laser therapy (LLLT) in an animal model. Med. Oral Patol. Oral Cir. Bucal 13, 648–652. https://doi.org/10.1016/S1010-5182(08)71950-4 (2008).
Hagiwara, S., Iwasaka, H., Okuda, K. & Noguchi, T. GaAlAs (830 nm) low-level laser enhances peripheral endogenous opioid analgesia in rats. Lasers Surg. Med. 39, 797–802. https://doi.org/10.1002/lsm.20583 (2007).
Elafifi-Ebeid, H., Betancourt, P., Parada-Avendaño, I. & Arnabat-Domínguez, J. Post-endodontic pain evaluation after different intracanal laser assisted disinfection techniques. Syst. Rev. J. Clin. Exp. Dent. 15 (2), e149–e159. https://doi.org/10.4317/jced.59941 (2023).
Guerreiro, M. Y. R. et al. Effect of low-level laser therapy on postoperative endodontic pain: An updated systematic review. Complement. Ther. Med. 57, 102638. https://doi.org/10.1016/j.ctim.2020.102638 (2021).
Chen, Y. et al. Efficacy of low-level laser therapy in pain management after root canal treatment or retreatment: A systematic review. Lasers Med. Sci. 34 (7), 1305–1316. https://doi.org/10.1007/s10103-019-02793-6 (2019).
Meire, M. A., Bronzato, J. D., Bomfim, R. A. & Gomes, B. P. F. A. Effectiveness of adjunct therapy for the treatment of apical periodontitis: A systematic review and meta-analysis. Int. Endod. J. 56 (Suppl 3), 455–474. https://doi.org/10.1111/iej.13838 (2023).
Alonaizan, F. A. & AlFawaz, Y. F. Is phototherapy effective in the management of post-operative endodontic pain? A systematic review of randomized controlled clinical trials. Photodiagnosis Photodyn. Ther. 26, 53–58. https://doi.org/10.1016/j.pdpdt.2019.03.003 (2019).
Page, M. J. et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ https://doi.org/10.1136/bmj.n71 (2021). 29;372.
Sterne, J. A. C. et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 28, 366:l4898. https://doi.org/10.1136/bmj.l4898 (2019).
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. http://www.R-project.org/. (2018).
Brignardello-Petersen, R. Low-level laser therapy may reduce postoperative pain levels after root canal retreatment in patients with low preoperative pain levels. J. Am. Dent. Assoc. 149, e33. https://doi.org/10.1016/j.adaj.2017.10.014 (2018).
Barciela, B. et al. In vivo evaluation of painful symptomatology after endodontic treatment with or without the use of photodynamic therapy. J. Conserv. Dent. 22, 332–335. https://doi.org/10.4103/JCD.JCD_39_19 (2019).
Souza, M. A. et al. Influence of the apical limit of instrumentation and photodynamic therapy on the postoperative pain of lower molars with asymptomatic apical periodontitis. Photodiagnosis Photodyn Ther. 36, 102489. https://doi.org/10.1016/j.pdpdt.2021.102489 (2021).
Nunes, E. C. et al. Comparison of the effect of photobiomodulation therapy and Ibuprofen on postoperative pain after endodontic treatment: Randomized, controlled, clinical study. Lasers Med. Sci. 35, 971–978. https://doi.org/10.1007/s10103-019-02929-8 (2020).
Sathorn, C., Parashos, P. & Messer, H. The prevalence of postoperative pain and flare-up in single- and multiple-visit endodontic treatment: A systematic review. Int. Endod. J. 41, 91–99. https://doi.org/10.1111/j.1365-2591.2007.01316.x (2008).
Ng, Y. L., Glennon, J. P., Setchell, D. J. & Gulabivala, K. Prevalence of and factors affecting post-obturation pain in patients undergoing root canal treatment. Int. Endod. J. 37, 381–391. https://doi.org/10.1111/j.1365-2591.2004.00820.x (2004).
Siqueira, J. F. Jr Reaction of periradicular tissues to root canal treatment: Benefits and drawbacks. Endod. Top. 10, 123–147. https://doi.org/10.1111/j.1601-1546.2005.00134.x (2005).
Siqueira, J. F. Jr & Barnett, F. Interappointment pain: Mechanisms, diagnosis, and treatment. Endod. Top. 7, 93–109. https://doi.org/10.1111/j.1601-1546.2004.00062.x (2004).
Tsesis, I., Faivishevsky, V., Fuss, Z. & Zukerman, O. Flare-ups after endodontic treatment: A meta-analysis of literature. J. Endod. 34, 1177–1181. https://doi.org/10.1016/j.joen.2008.07.016 (2008).
Mehrvarzfar, P., Shababi, B., Sayyad, R., Fallahdoost, A. & Kheradpir, K. Effect of supraperiosteal injection of dexamethasone on postoperative pain. Aust. Endod. J. 34, 25–29. https://doi.org/10.1111/j.1747-4477.2007.00076.x (2008).
Shahi, S. et al. Effect of premedication with ibuprofen and dexamethasone on success rate of inferior alveolar nerve block for teeth with asymptomatic irreversible pulpitis: A randomized clinical trial. J. Endod. 39, 160–162. https://doi.org/10.1016/j.joen.2012.10.011 (2013).
Mussttaf, R. A., Jenkins, D. F. L. & Jha, A. N. Assessing the impact of low level laser therapy (LLLT) on biological systems: A review. Int. J. Radiat. Biol. 120–143. https://doi.org/10.1080/09553002.2019.1524944 (2019).
Asnaashari, M. & Safavi, N. Application of low level lasers in dentistry (endodontic). J. Lasers Med. Sci. 57–66. PMID: 25606308 (2013).
Trindade, A. C., De Figueiredo, J. A., Steier, L. & Weber, J. B. Photodynamic therapy in endodontics: A literature review. Photomed. Laser Surg. 175–182. https://doi.org/10.1089/pho.2014.3776 (2015).
Garcez, A. S., Fregnani, E. R., Rodriguez, H. M., Nunez, S. C. & Sabino, C. P. The use of optical fiber in endodontic photodynamic therapy. Is it really relevant? Lasers Med. Sci. 79–85. https://doi.org/10.1007/s10103-012-1073-8 (2013).
Lopes, L. P. B. et al. Effect of photobiomodulation therapy on postoperative pain after endodontic treatment: A randomized, controlled, clinical study. Clin. Oral Investig. 23, 285–292. https://doi.org/10.1007/s00784-018-2435-9 (2019).
Alves-Silva, E. G. et al. The effect of photodynamic therapy on postoperative pain in teeth with primary endodontic infection. Photodiagnosis Photodyn. Ther. 37, 102700. https://doi.org/10.1016/j.pdpdt.2021.102700 (2022).
Asnaashari, M., Ashraf, H., Daghayeghi, A. H., Mojahedi, S. M. & Azari-Marhabi, S. Management of post endodontic retreatment pain with low level laser therapy. J. Lasers Med. Sci. 8, 128–131. https://doi.org/10.15171/jlms.2017.23 (2017).
Coelho, M. S., Vilas-Boas, L. & Tawil, P. Z. The effects of photodynamic therapy on postoperative pain in teeth with necrotic pulps. Photodiagnosis Photodyn. Ther. 27, 396–401. https://doi.org/10.1016/j.pdpdt.2019.07.002 (2019).
Fazlyab, M., Esmaeili Shahmirzadi, S., Esnaashari, E., Azizi, A. & Moshari, A. A. Effect of low-level laser therapy on postoperative pain after single-visit root canal retreatment of mandibular molars: A randomized controlled clinical trial. Int. Endod. J. 54, 2006–2015. https://doi.org/10.1111/iej.13608 (2021).
Genc Sen, O. & Kaya, M. Effect of root canal disinfection with a diode laser on postoperative pain after endodontic retreatment. Photobiomodul. Photomed. Laser Surg. 37, 85–90. https://doi.org/10.1089/photob.2018.4539 (2019).
Kaplan, T., Sezgin, G. P. & Sönmez Kaplan, S. Effect of a 980-nm diode laser on post-operative pain after endodontic treatment in teeth with apical periodontitis: A randomized clinical trial. BMC Oral Health 21 (22), 41. https://doi.org/10.1186/s12903-021-01401-w (2021).
Liapis, D., De Bruyne, M. A. A., De Moor, R. J. G. & Meire, M. A. Postoperative pain after ultrasonically and laser-activated irrigation during root canal treatment: A randomized clinical trial. Int. Endod. J. 54, 1037–1050. https://doi.org/10.1111/iej.13500 (2021).
Morsy, D. A., Negm, M., Diab, A. & Ahmed, G. Postoperative pain and antibacterial effect of 980 nm diode laser versus conventional endodontic treatment in necrotic teeth with chronic periapical lesions: A randomized control trial. F1000Research 7, 1795. https://doi.org/10.12688/f1000research.16794.1. (2018).
Nabi, S. et al. Effect of preoperative ibuprofen in controlling postendodontic pain with and without low- level laser therapy in single visit endodontics: A randomized clinical study. Indian J. Dent. Res. 29, 46–50. https://doi.org/10.4103/ijdr.IJDR_327_15. PMID: 29442086. (2018).
Naseri, M., Asnaashari, M., Moghaddas, E. & Vatankhah, M. R. Effect of low-level laser therapy with different locations of irradiation on postoperative endodontic pain in patients with symptomatic irreversible pulpitis: A double-blind randomized controlled trial. J. Lasers Med. Sci. 11, 249–254. https://doi.org/10.34172/jlms.2020.42 (2020).
Tunc, F., Yildirim, C. & Alacam, T. Evaluation of postoperative pain/discomfort after intracanal use of nd:YAG and diode lasers in patients with symptomatic irreversible pulpitis and asymptomatic necrotic pulps: A randomized control trial. Clin. Oral Investig. 25, 2737–2744. https://doi.org/10.1007/s00784-020-03588-8 (2021).
Gama, S. K. et al. Tooth movement after infrared laser phototherapy: Clinical study in rodents. Photomed. Laser Surg. 28, S79–83. https://doi.org/10.1089/pho.2009.2618 (2010).
Pallotta, R. C. et al. Infrared (810-nm) low-level laser therapy on rat experimental knee inflammation. Lasers Med. Sci. 27, 71–78. https://doi.org/10.1007/s10103-011-0906-1 (2012).
Doğanay Yıldız, E. & Arslan, H. Effect of low-level laser therapy on Postoperative Pain in molars with symptomatic apical periodontitis: A randomized placebo-controlled clinical trial. J. Endod. 44, 1610–1615. https://doi.org/10.1016/j.joen.2018.07.002 (2018).
Xu, Y., Young, M. J., Battaglino, R. A., Morse, L. R. & Fontana, C. R. Endodontic antimicrobial photodynamic therapy: Safety assessment in mammalian cell cultures. J. Endod. 1567–1572. https://doi.org/10.1016/j.joen.2009.08.002 (2009).
Gursoy, H., Ozcakir-Tomruk, C., Tanalp, J. & Yilmaz, S. Photodynamic therapy in dentistry: A literature review. Clin. Oral Investig. 1113–1125. https://doi.org/10.1007/s00784-012-0845-7 (2013).
He, W. et al. Low-level laser therapy for closed bone fracture healing in animals: A systematic review and meta-analysis. Sci. Rep. 7 (1), 1757 (2017).
Alghamdi, K. M., Kumar, A. & Moussa, N. A. Low-level laser therapy: A useful technique for enhancing the proliferation of various cultured cells. Lasers Med. Sci. 27 (1), 237–249 (2012).
Konopka, K. & Goslinski, T. Photodynamic therapy in dentistry. J. Dent. Res. 86 (8), 694–707 (2007).
Meire, M. A. et al. Evaluation of the efficacy of four disinfection methods against the yeast Candida albicans in root canals. Int. Endod. J. 42 (4), 351–358 (2009).
Gutknecht, N. et al. Bactericidal effect of a 980-nm diode laser in the root canal wall dentin of bovine teeth. J. Clin. Laser Med. Surg. 22 (1), 9–13 (2004).
Vidas, J. et al. Comparison of apical irrigant solution extrusion among conventional and laser-activated endodontic irrigation. Lasers Med. Sci. 35, 205–211. https://doi.org/10.1007/s10103-019-02846-w (2020).
Peeters, H. H. & Mooduto, L. Radiographic examination of apical extrusion of root canal irrigants during cavitation induced by Er, Cr:YSGG laser irradiation: An in vivo study. Clin. Oral Investig. 17, 2105–2112. https://doi.org/10.1007/s00784-012-0910-2 (2013).
Peters, H. H. & De Moor, R. J. Measurement of pressure changes during laser-activated irrigant by an erbium, chromium: Yttrium, scandium, gallium, garnet laser. Lasers Med. Sci. 3, 1449–1455. https://doi.org/10.1007/s10103-014-1605-5 (2015).
Yao, K. et al. Effect of laser energy and tip insertion depth on the pressure generated outside the apical foramen during Er:YAG laser-activated root canal irrigation. Photomed. Laser Surg. 35, 682. https://doi.org/10.1089/pho.2017.4268 (2017).
Peters, O. A., Bardsley, S., Fong, J., Pandher, G. & Divito, E. Disinfection of root canals with photon-initiated photoacoustic streaming. J. Endod. 37, 1008–1012. https://doi.org/10.1016/j.joen.2011.03.016 (2011).
Olivi, G. et al. Disinfection efficacy of photon-induced photoacoustic streaming on root canals infected with Enterococcus faecalis: An ex vivo study. J. Am. Dent. Assoc. 145, 843–848. https://doi.org/10.14219/jada.2014.46 (2014).
Nathani, T. I. et al. Post-operative pain after single-visit root canal treatment using resin-based and bioceramic sealers in teeth with apical periodontitis: A randomised controlled-trial. Aust. Endod. J. 17 (2024) https://doi.org/10.1111/aej.12864. Online ahead of print.
Afrashtehfar, K. I., Jurado, C. A., Al-Hadi, D. & Shetty, K. P. Pulpotomy versus root canal treatment in permanent teeth with spontaneous pain: Comparable clinical and patient outcomes, but insufficient evidence. Evid. Based Dent. 24 (2), 54–56. https://doi.org/10.1038/s41432-023-00878-4 (2023).
Fanghänel, J. et al. The morphological and clinical relevance of mandibular and maxillary bone structures for implantation. Folia Morphol. 65 (1), 49–53 (2006).
Walker, K. E., Baldini, T. & Lindeque, B. G. Thermal conductivity of human bone in cryoprobe freezing as related to density. Orthopedics 40 (2), 90–94. https://doi.org/10.3928/01477447-20161208-01 (2017).
Acknowledgments
Open access funding provided by Ajman University and Universität Bern.
Funding
This research project received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, F.E. and K.I.A.; methodology, F.E. and J.A.G.; software, H.S. and R.A.; validation, T.A., C.A.J. and K.I.A.; formal analysis, F.E., J.A.G., J.G.O. ; investigation, H.S., R.A. and C.A.J.; resources, F.E. and K.I.A.; data curation, J.A.G., J.G.O., and C.A.J.; writing—original draft preparation, F.E., H.S. and R.A.; writing—review and editing, F.E., J.G.O., C.A.J. and K.I.A.; visualization, T.A. and J.G.O; supervision, F.E. and K.I.A.; project administration, F.E.; funding acquisition, F.E. and K.I.A. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Elmsmari, F., Shujaie, H., Alzaabi, R. et al. Lasers efficacy in pain management after primary and secondary endodontic treatment: a systematic review and meta-analysis of randomized clinical trials. Sci Rep 14, 26028 (2024). https://doi.org/10.1038/s41598-024-74998-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-74998-x
Keywords
- Dental laser applications
- Dental pain
- Dental pulp diseases
- Diode laser
- Endodontic pain relief
- Endodontic treatment
- Endodontically treated teeth
- Endodontics
- Laser therapy
- Low-level laser therapy
- Pain management
- Periapical pain
- Photobiomodulation
- Photodynamic therapy
- Postoperative pain
- Root-filled teeth
- Toothache
- Root canal therapy
This article is cited by
-
Preventive and therapeutic effects of semiconductor laser on pain in root canal treatment
European Journal of Medical Research (2025)
-
Efficacy of low-level laser as an adjunctive therapy in root canal treatment and retreatment: an umbrella review
Lasers in Medical Science (2025)
