
Abstract
Older adults are at risk of committing cognitive and decision-making errors due to the decline in cognitive functions. However, the understanding of the determining factors of cognitive errors among ageing adults is limited. In this study, we explored the role of various psychiatric factors, life satisfaction, and other socioeconomic, health and behavioural risk factors of committing cognitive errors among middle-aged and older adults in India. The study utilized the data from the experimental module of the Longitudinal Ageing Study in India (LASI) Wave-1 (2017–2018) with a sample of 12,754 adults aged 45 years and above. The cognitive error was measured using logical fallacies committed in the activity-based experiments. The study employed descriptive, bivariate statistics and multivariable logistic regression models to identify the factors associated with cognitive errors among the study participants. Depression (aOR = 1.28, 99%, CI: 1.16–1.41), life satisfaction (aOR = 0.99, 99%, CI: 0.98–1.00), and cognitive impairment (aOR = 1.13, 90% CI: 1.00–1.30) were significantly associated with higher odds of committing cognitive errors among the middle-aged and older adults. Also, ageing adults with low educational levels, functional limitations, sleep disturbances, smoking history, living in rural areas and belonging to scheduled tribes had a higher probability of committing cognitive errors. However, involvement in physical activity, reading habits and social interactions reduced the odds of cognitive errors among this sample. Mental health and well-being indicators, including depression, life satisfaction, cognitive impairment, and other health and behavioural health factors, determine cognitive errors among ageing adults. Programs and policies should be initiated to address these factors, reduce cognitive errors, and ensure active ageing.
Similar content being viewed by others


Introduction
Cognitive abilities facilitate individuals in navigating complex decision-making, problem-solving, and reasoning in everyday life1. Decision-making is a dynamic skill2, and it is influenced by various factors, such as past life experiences3,4, cognitive biases5,6, individuals’ personalities7,8, and beliefs about the importance of the problem they encounter 9. A study indicated that traits related to behavioural and cognitive self-regulatory functions and cognitive flexibility are related to an increased tendency to be involved in rational thoughts7. The decision-making process is guided by internal and external factors like perceptions and environment, and cognitive bias plays a crucial role5. Decision-making is an important faculty of cognition and is associated with various life outcomes10, including cognitive errors. Cognitive error is a volatile concept, and scholars conceptualize it differently.
Cognitive errors are common in everyday life, as no system is completely foolproof, and decision-making as a process of cognition also involves mental shortcuts (heuristics) to save resources and avoid cognitive overload in a world flooded with information. Even though heuristics helps in quicker decision-making and problem-solving, they are bound to errors and biased judgments11. A heuristic procedure is a collection of steps or rules that may or may not lead to an ideal optimal solution, and the steps are usually based on one’s intuitions, good ideas and hunches, problem characteristics, and reasoning processes12. Heuristics are effective during time constraints, lack or overload of information when no optimal solution is evident, and when the problem looks familiar13. A few commonly employed heuristics during uncertainty are representativeness, availability of instances or scenarios, and adjustment from an anchor. These are highly economical and generally effective but may lead to predictable and systematic errors14.
Interestingly, there is a significant association between ageing and cognitive capacities as decision-making or the trajectory of decision-making changes with age15,16. The decline in cognitive capacities like memory17, perceptual processing18, and executive functions19 while ageing may impact the process of decision-making and lead to related errors2. The literature points out the difference in affective-motivational factors during ageing. The major focus of decision-making during a young age is gain, but changes to prevent loss in later life15,20. Also, a study found that loneliness and cognitive distortion negatively impact life satisfaction and the interconnectedness between these factors21. Psychiatric conditions such as depression22,23 and neurological issues such as cognitive impairments24,25,26 affect decision-making and cognitive errors. Interestingly, a sense of purpose acted as a psychological resource, leading to fewer cognitive failures among adults, even countering the depressive effects27.
In addition, multiple psychosocial factors influence the process of decision-making and play a role in cognitive errors among adults, including interpersonal relationships28, stress29, health status30, economic well-being31, risky lifestyle behaviours32 and physical activities33. Further, a study among older adults in Japan suggested that participation in sports club activities is related to the articulation of decisions about life-prolonging treatments34, indicating better use of cognitive resources. As the concept of neural compensation suggests, being active and keeping the neural network active while ageing helps better physical and psychological functioning35. It is important to note that educational attainment adds to the cognitive reserve and brain maintenance, ultimately improving and facilitating better cognitive functions later in life36.
It has been widely established that older adults are at higher risk of committing decision-making errors due to reduced cognitive functions, and despite these odds, they must make decisions in their everyday lives2. Strikingly, a study showed that decision-making errors increased mortality risk by 20% among older adults37. Also, cognitive errors are associated with severe anxiety and depressive symptoms in older adults38, and subjective cognitive failures were associated with anxiety, depression, and anger39. In addition, cognitive biases were persistent across all economic groups regarding financial decisions40, indicating its relevance to be addressed. Further, the dynamic process of decision-making and cognitive errors was influenced by culture41. In the Indian context, cognitive bias is investigated from the business and investors’ perspectives42,43 with a minuscule focus on the general population, leading to a significant gap in this subject matter.
This brings in the significant need to understand the determining factors of cognitive errors among middle-aged and older adults in India. The current study attempted to understand the role of depression, life satisfaction, cognitive impairment, and self-reported psychiatric/neurological conditions on cognitive errors along with covariates such as socioeconomic, demographic, health-related, behavioural risk, and other factors (the study’s conceptual framework is presented in Fig. 1). We have considered the above mentioned factors as determinants, as life satisfaction and mental health factors are generally associated with cognitive functioning and errors44,45. In the present study, we aimed to understand cognitive errors through an experimental approach (Refer to Fig. 2 for conceptualization of cognitive errors).

Summary of the conceptualization of cognitive errors and their predictors.

Conceptualization of cognitive errors.
Methods
Data and sample
The study used unit-level data from the first wave of the Longitudinal Ageing Study in India (LASI) conducted between 2017 and 2018. The data investigate the socioeconomic, health, psychosocial components, and other aspects of the ageing population in India. The LASI was funded by the Ministry of Health and Family Welfare, the Government of India, the National Institute of Aging, and the United Nations Population Fund India. The data collection was designed and executed by the International Institute for Population Sciences (IIPS) along with technical support from various institutions, including Harvard T H Chan School of Public Health (HSPH), and the University of Southern California (USC)46. LASI adopted a three-stage and four-stage sampling design for rural and urban areas.
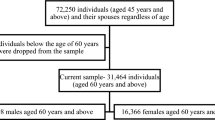
LASI included 72250 adults representing all Indian states and union territories (excluding Sikkim) aged 45 years and above. The current study considered data from the experimental module, consisting of four separate sections: time use, expectations, social connectedness, and vignettes. One of these sections was chosen randomly to collect data from each individual. This study initially considered 17253 individuals from the ‘expectation’ section. Further, after removing individuals below 45 years and other missing cases, the final sample included for analysis was 12,754 individuals. The summary of the sample selection process is presented in Fig. 3.

Sample selection procedure.
Measures
Conceptualization of cognitive errors
The “Homo Economicus” theory, widely considered the base for developing socioeconomic theories, emphasizes that humans are consistently rational, close-to-optimal agents and can solve simple and complex cognitive decision-making problems47. Social scientists in the late 20th century weighted the importance of “bounded rationality” with the support of empirical evidence asserting that humans often fail in their decision-making processes as they are not perfectly rational48,49,50. Studies indicated that the human tendency to depend on heuristic or mental shortcuts causes cognitive errors that may result in irrational decisions51. In social and behavioural sciences, people are considered incomplete Bayesians as they sometimes designate erroneous probability values about outcomes, as found in several recent studies52,53,54,55. These possibilities lead to cognitive errors.
In the present study, cognitive errors were estimated using an activity based experimental design. In the expectations module of the LASI survey, an experimental set-up was created for the study participants. Different questions were asked about the chance or the likelihood of certain events that are going to happen. For the experiment, each participant was given 10 beans in a cup and asked to choose out of them and put them onto a plate representing the likelihood of an event. The participants were further informed that adding no beans onto the plate meant the event would not happen. Adding beans increases the likelihood of the event happening. Adding ten beans onto the plate means the participant is sure that the event will happen. Additionally, the interviewer demonstrated the experiment by creating a hypothetical question about the likelihood of a cold in the coming year. In this hypothetical example, participants were informed that if the participant think about the chance that there will have a cold in the next year; if the participant put 4 beans onto the plate, it means that out of 10 people who are exactly like the participant, 4 would have a cold in the next year. It also means that 6 out of those 10 people would not have a cold in the next year. Along with this hypothetical example, the interviewer has demonstrated the case by putting 4 beans onto the plate. Once the participant understood the method of participation in the experiment, the following question was asked in the actual experiment.
“Suppose that you and I decide to play a game of Ludo against each other.”
The responses by the participants regarding the likelihood of winning and losing were collected in two phases. In the first phase, the participants were asked to pick the number of beans that reflects how likely they think it is that:
-
(a)
They will win the game….
-
(b)
They will lose the game….
In the second phase, the participants were taught the concept of conditional probability, and responses were collected as in the first phase. In the second phase, the participants were informed that since only two outcomes are possible at the end of the Ludo game, i.e., either win or lose, it means that they may win the game with a given probability [equivalent to the number of beans added to the plate] and the remaining is the probability of loss. Mathematically, it can be expressed as follows.
In the above expressions (1) and (2), X represents the number of beans added to the plate. Technically, the events, win and loss, are mutually exclusive and dependent. It can be expressed as follows.
The cognitive errors were estimated when the participants committed “logical fallacy”. In other words, cognitive errors occurred when the participants deviated from the basic understanding of probability rules. Such deviations from the basic logic can be classified as (exclusive) “disjunction fallacy”56. Study participants who responded in line with the probability logic (i.e., the sum of beans placed in the plate for both win and loss was equal to ten) were considered not committed cognitive errors in the first phase. The remaining participants were taught the basic concept of conditional probability and then considered for the second phase of the experiment. For this, participants were informed that the sum of beans placed onto the place for both win and loss should be 10. We also identified participants with cognitive errors when they repeated the “logical fallacy” in the second phase. Those who did not commit such “logical fallacy” in the second phase were considered cases of non-cognitive errors. A summary of the conceptual framework of the experimental design is presented in Fig. 2.
Predictor variables
Depression: Previous studies established that depression is a decisive factor that may negatively affect cognitive ability57,58,59. The present study considered depression symptoms as a primary predictor variable of cognitive errors. In this study, depression was measured using the Center for Epidemiological Studies Depression (CESD) score. A short version of the depression measurement tool (CESD-10) consisting of 7 negative and 3 positive feelings questions was employed in the survey. The total score from these 10 questions was calculated after reversing the score of the positive questions (on a 0–10 scale). We classified individuals with “depression symptoms” if the CESD score was 4 and above, and less than 4 was classified as “no depression symptoms”60.
Life satisfaction: Life satisfaction level is an established associated factor of cognitive ability. Studies indicated that life satisfaction prevents cognitive impairment risk among the ageing population61. Studies also indicated that life dissatisfaction is associated with the risk of dementia62. In the present study, the participants’ life satisfaction was assessed based on five questions in the survey. The five questions include: (i) In most ways, my life is close to ideal, (ii) The conditions of my life are excellent, (iii) I am satisfied with my life, (iv) So far, I have got the important things I want in life, and (v) If I could live my life again, I would change almost nothing. Response to each of these questions was collected on a seven scale with a value of 1 representing “strongly disagree”, 2 representing “somewhat disagree”, 3 representing “slightly disagree”, 4 representing “neither agree nor disagree”, 5 representing “slightly agree”, 6 representing “somewhat agree”, and 7 representing “strongly agree”. The scores from all five questions were combined, and a life satisfaction score ranging between 5 and 35 was created, with a higher score representing a higher level of life satisfaction. Additionally, the internal consistency and reliability was assessed and the result indicated that the scale is a good measurement tool of life satisfaction with a Cronbach Alpha value of 0.90.
Cognitive impairment: Studies indicated the importance of cognitive impairment and showed that individuals with cognitive impairment are at multiple risks, including the decline of functional ability, memory loss, and other psychiatric disorders63,64. In the present study, cognitive impairment was measured as recommended by LASI using a set of questions on memory (word recall test), orientation (time and place), arithmetic function (number counting and computation), executive function (paper folding and drawing test) and object naming65. The composite cognitive score ranged between 0 and 43, with a higher score for improved cognitive functions. We classified the lowest 10% as having low cognitive status66.
Self-reported psychiatric/neurological conditions: We further considered the study participants’ self-reported neurological or psychiatric problems diagnosis. We classified individuals as having neurological or psychiatric problems if they have reported a physician diagnosis of any neurological or psychiatric problems among depression, Alzheimer’s/Dementia, unipolar/bipolar disorders, convulsions, Parkinson’s, etc.
Socioeconomic and demographic factors: The study considered a range of covariates that could potentially affect cognitive errors. The socioeconomic and demographic factors consist of age categories (45–59 years, 60–69 years and 70 years and above), gender (male and female), education in years (no schooling, up to 5 years, 6–10 years and above 10 years), and social class, which includes Scheduled Tribes (ST), Scheduled Caste (SC), Other Backward Class (OBC) and Others. We have also considered the household economic status that was categorized as poorest, poor, middle, richer and richest; living arrangement (living alone, with spouse and others and with others); marital status (in a union and not in a union) and residency type (rural and urban). We have also included study participants’ social interaction, which could determine their cognitive ability. Social interaction was categorized as ‘yes’ if the participants visited relatives/friends and as ‘no’ if otherwise. The household economic status was measured based on the expenditure data of each household on 11 food and 29 non-food items after standardizing the expenditure to a 30-day reference period65.
Health–related factors: It was well established that health factors significantly contribute to cognitive errors67,68. The health-related factors include self-rated health (SRH), Activities of Daily Living (ADL), Instrumental Activities of Daily Living (IADL), and morbidity status. The response to the SRH question was categorized into “good” by combining very good, good, and fair and “poor” by combining poor and very poor. The ADL and IADL consist of six and seven types of difficulties in various aspects of everyday functioning, respectively. ADL was measured using questions on six types of difficulties in dressing, walking, bathing, eating, using the toilet, and getting out of bed. IADL was measured using seven questions on difficulties in performing cooking, shopping, making telephone calls, taking medications, doing work around the house/gardening, managing money, and movement. ADL and IADL were classified as “low” if the difficulty was reported in performing at least one of the ADL and IADL items, respectively69. The morbidity status was measured based on the presence of some diseases as reported by the participants among the nine diseases listed; the responses were classified as “no disease”, “one disease”, and “multimorbidity”. The major diseases considered include hypertension, diabetes, cancer, chronic lung diseases, chronic heart diseases, stroke, arthritis, any neurological or psychiatric issues, and high cholesterol. In addition, we have considered hearing loss and sleep disturbances among the study participants. Hearing was assessed based on any hearing problem reported among the study participants. Sleep disturbances of the study participants were measured based on the Jenkin’s Sleep Scale (JSS) and considered a continuous variable. The measure indicated a good reliability (Cronbach’s Alpha = 0.82).
Behavioural-risk factors: The literature suggests that involvement in behavioural risk factors such as smoking and drinking alcohol, in the long run, impairs cognitive abilities later in life70,71. The current study considers alcohol consumption (yes and no), smoking (yes and no), and involvement in physical activity (yes and no) as behavioural risk factors.
Other factors: Studies indicated that reading habits reduce cognitive impairment72 and prevent cognitive decline among older adults73. This study includes a component about reading habits from the social activities section of the LASI data. The reading habit was assessed using the survey question, ‘How often, if at all, do you read books/newspapers/magazines?’ and the responses were classified into ‘daily readers, ‘read sometimes’, and ‘never readers’.
Statistical analysis
In the present study, we conducted descriptive statistics and bivariate analysis to report the characteristics of the study sample. Further, multivariable logistic regression was employed to estimate the odds of committing cognitive errors on respondents’ background characteristics. First, we examined the association between depression, life satisfaction, cognitive impairment, and self-reported psychiatric/neurological conditions with cognitive errors independently and estimated the crude odds ratio. We have considered other confounding variables in the full model (and estimated the adjusted odds ratio), including socioeconomic and demographic factors, health-related factors, behavioural risk factors, and others. The results were presented as odds ratio, and 90%, 95%, and 99% confidence intervals were considered for drawing conclusions. All the statistical analysis was performed using Stata Version 16.
Results
The study tries to uncover the factors determining cognitive errors among ageing adults in India. The main factors considered in the study are depression, life satisfaction, cognitive impairment, and neurological conditions, along with covariates such as socioeconomic and demographic factors, health-related factors, behavioural risk factors, and other factors like reading.
The descriptive characteristics of the study variables are presented in Table 1 (N = 12754). The results indicated that 27.49% of adults had depression, 11.44% had cognitive impairment, and about 2% had neurological conditions. The mean score on life satisfaction was 23.93. More than 50% of the study participants were aged 45–59 years old, and nearly 52% of the total sample were females. It was found that 45.37% of participants had no formal schooling. The major proportion of the sample belonged to OBC social background (44.76%), and an approximately equal proportion of older adults belonged to different categories of household economic status: poorest (20.79%), poorer (21.26%), middle (20.65%), richer (18.58) and richest (18.73%). In addition, about 76.18% of the study participants were in a marital union. A majority of the study participants were rural residents (67.98%). About 16.33% reported poor self-reported health status. About 15% and 35% of the sample reported low ADL and IADL statuses, respectively. More than half of the participants had no morbidity conditions (53.95%). About 57% of the participants did not engage in physical activity (57.05%). It was found that 38.09% and 15.13% were ever smokers and consumers of alcohol. Just above 15% of the study participants reported being daily readers.
Table 2 indicates the bivariate analysis of cognitive errors with depression, cognitive impairment, neurological condition, and other baseline characteristics. The results indicated that ageing adults with depression symptoms had committed cognitive errors than those with no depression symptoms (26.75% Vs 21.12, p < 0.01). It was also revealed that participants who reported cognitive impairment had a higher prevalence of cognitive errors than participants with no cognitive impairment (30.00% Vs 21.72%, p < 0.01). Similarly, it was found that cognitive errors were high among participants who reported any neurological condition in comparison with those who did not report any neurological condition (36.41% Vs 22.39%, p < 0.01).
The prevalence of cognitive errors increased with age and was significantly higher among older adults aged 70 years and above compared to those aged 45–59 years (25.1% Vs 21.70%, p < 0.05) (Fig. 4). In addition, the bivariate analysis in Table 2 indicated that female participants committed higher cognitive errors than their counterparts (23.56% Vs 21.70%, p < 0.05). The cognitive errors significantly differed across educational attainment categories, with higher prevalence among individuals with no schooling and lower prevalence among participants with more years of schooling. Cognitive errors were higher amongageing from SC backgrounds. Based on marital status, it was found that participants who were in a marital union had a lower prevalence of cognitive errors compared to their counterparts (21.99% Vs 24.85%, p < 0.01). Similarly, cognitive errors were lower among participants who maintained social interaction than their counterparts (22.00% Vs 25.74%, p < 0.01). Also, individuals in urban areas had a lower prevalence of cognitive errors than those in rural areas (21.38% Vs 23.28%, p < 0.05). It was further indicated that cognitive errors were significantly lower among participants with high IADL status and those who engaged in regular physical activities and reading.

Prevalence of cognitive errors (%) by age groups.
The results of multivariate logistic regression of cognitive errors with depression, life satisfaction, cognitive impairment, neurological condition, and other background characteristics are presented in Table 3. In the unadjusted model, the results indicated that adults with depression symptoms (cOR = 1.45, 99% CI: 1.32–1.58), cognitive impairment (cOR = 1.31, 99% CI: 1.15–1.49), and neurological condition (cOR = 1.44, 99% CI: 1.09–1.88) had higher odds of committing cognitive errors compared to their respective counterparts. Similarly, in the unadjusted model, individuals with higher life satisfaction had a significantly lower likelihood of committing cognitive errors (cOR = 0.99, 99% CI: 0.98–0.99). In the fully adjusted model, the results for all these variables showed a consistent result, with higher odds of depression symptoms (aOR = 1.28, 99% CI: 1.16–1.41), cognitive impairment (aOR = 1.13, 90% CI: 1.00–1.30) and higher likelihood with life satisfaction (aOR = 0.99, 99%, CI: 0.98–1.00). Participants with neurological conditions had higher odds of committing cognitive errors, but this was not statistically significant.
Additionally, the margin plots representing the probabilities of cognitive errors by these main variables of interest are presented in Figs. 5, 6, 7 and 8. It indicated a higher probability of cognitive errors among participants with depression symptoms, cognitive impairment, and neurological conditions and lower life satisfaction scores.

Margin plot representing the probabilities of cognitive errors with depression prevalence status.

Margin plot representing the probabilities of cognitive errors with life satisfaction score.

Margin plot representing the probabilities of cognitive errors with cognitive impairment status.

Margin plot representing the probabilities of cognitive errors with self-reported psychiatric/neurological conditions.
In terms of gender, males (aOR = 1.16, 99% CI: 1.04–1.28) had higher odds of committing cognitive errors compared to their female counterparts. Compared to participants with no formal schooling, those with more than 6–10 years of education had lower cognitive errors (aOR = 0.89, 90% CI: 0.78–1.00). Individuals from Schedules Caste, Other Backward Classes, and other social classes had lower odds of committing cognitive errors than those from the ST social class (aOR = 0.77, 99% CI: 0.68–0.89, aOR = 0.73, 99% CI: 0.63–0.82, and aOR = 0.57, 99% CI: 0.50–0.65, respectively). It was found that ageing adults from higher household economic status had higher odds of cognitive errors. In addition, individuals who were not in a marital union had a higher odd of cognitive errors than those who were in a marital union (aOR = 1.09, 95% CI: 1.00–1.21). Similarly, it was found that individuals with no social interaction had a higher odds of cognitive errors than individuals who maintained social interaction (aOR = 1.28, 99% CI: 1.15–1.43). It was also found that participants from urban areas had lower odds of cognitive errors than those from rural areas (aOR = 0.81, 99% CI: 0.74–0.89).
Based on health status, participants with low ADL status had a lower odds of cognitive errors in comparison with participants with high ADL status (aOR = 0.81, 99% CI: 0.70–0.93), whereas older adults with low IADL status had a higher odds of committing cognitive errors (aOR = 1.24, 99% CI: 1.12–1.37) in comparison with those with a high IADL status. Further, results showed that participants who were involved in regular physical activities (aOR = 0.85, 99% CI: 0.78–0.93) had lower odds of committing cognitive errors than those who did not engage in regular physical activities. It was found that participants who reported hearing loss had a higher risk of cognitive errors, but this was not statistically significant. Sleep disturbances were a significant predictor of cognitive errors, and an increase in sleep disturbances was associated with a higher likelihood of cognitive errors. The results showed that smokers had lower odds of committing cognitive errors than non-smokers. The results indicated that compared to daily readers, those engaged in reading sometimes had higher odds of cognitive errors (aOR = 1.36, 99% CI: 1.17–1.58).
Discussion
The present study, with a range of physical and psychological variables, tried to understand the predictors of cognitive errors among middle-aged and older adults in India. The findings, consistent with the literature23, suggest that depression, reduced life satisfaction, cognitive impairment, and neurological conditions lead to a higher risk of committing cognitive errors. A study suggested that the effectiveness of decision-making was reduced due to the failure to use effective strategies to decide among depressed individuals22, leading to higher cognitive errors74. Limited studies examine cognitive errors as an outcome of poor life satisfaction. Earlier studies have explored the other way by exploring the role of cognitive failures and emotional distress or loneliness on life satisfaction21,75.
In addition, a study among older adults with bipolar disorder suggested that cognitive failures, directly and indirectly, affected their quality of life76. Interestingly, these factors are interconnected, where depression could lead to cognitive impairment77 and neurological conditions impacting life satisfaction and vice-versa. Further, all these factors increase the odds of cognitive errors. In the present study, older adults who could not complete the experimental task appropriately, even after the prompt of conditional probability, may need attention in terms of neurological and psychological interventions. A study among adults with Alzheimer’s and mild cognitive impairment revealed that committing errors in a task reduced from the previous trial with correction than individuals who were not corrected, indicating adaptive control among participants78.
The present study indicated that females were involved in committing higher cognitive errors than their male counterparts. In support of our findings, a previous study showed significant gender differences in the decision-making process79, and females were more prone to commit risky decisions, especially when they are under stereotype threat80. Consistent with our findings, a study among older Japanese adults showed gender differences in cognitive decline and supported the cognitive reserve hypothesis through the role of education, intellectual experiences, and occupation81. Interestingly, educational attainment acted as a reserve and reduced the risk of committing cognitive errors in this study. In addition, a systematic review indicated the impeccable role of education on cognition across the lifespan36.
In addition, the risk of committing cognitive errors differed according to social class, economic status, marital status, and residence type. A previous study established that social context significantly shapes decision-making82. Further, a study suggested the differences in decision-making tendencies in the prestige-money games among the upper class and lower class83. The higher risk of cognitive errors was evident among participants from scheduled tribes might be due to various reasons, including the low level of education because, in this study, education is found to be a reserve against cognitive errors. Moreover, it is established that socioeconomic disadvantage is a risk factor for children’s cognitive development, implying its impact on life course84. Also, studies have documented that social disadvantages significantly impact health-related quality of life85, along with brain health and cognitive decline86. However, further investigations are required to establish the determinants of a higher risk of cognitive errors among the scheduled tribes.
In line with the present study, earlier studies suggested that being in a marital union and urban residency promoted cognitive abilities87,88 and reduced cognitive decline89 among older adults. These indirectly point to the role of decision-making and cognitive errors, as there is a relationship between cognitive abilities and decision-making90. In line with the study evidence, literature evidence indicates that social interaction delays cognitive decline among middle-aged and older adults91,92. In the present study, individuals with higher ADL and lower IADL had higher odds of committing cognitive errors. ADL assesses the basic functioning of daily living, including walking, dressing, and other activities that do not require higher cognitive abilities. However, IADL includes items such as making a telephone call and managing money, which require cognitive abilities. A study evidenced the impact of cognitive errors on disability among chronic lower back pain patients, and overgeneralization was the common cognitive error93. Also, functional limitations strongly predicted cognitive impairment among older adults94. In corroboration with the evidence from the study, a study conducted among the ageing population in developing countries indicated that perceived sleep quality was a significant contributor to cognitive performance95. Studies have also shown that educational attainment and involvement in physical activity can enhance cognitive performance33,96 and reduce cognitive decline in later life97. Usually, smoking is associated with poor cognitive performance98,99. However, this study’s results suggested that smoking reduced the risk of committing cognitive errors. Further, longitudinal studies might be needed to establish this association and its causes.
This study’s results support the cognitive bias theory developed by Tversky and Kahneman14, which suggests that individuals are not rational beings involved in decision-making and disobey logical rules, leading to fallacies. Further, we interpret the results to defy the concept of ‘Homo Economicus’ from the economic stand that considers human beings to be rational agents, optimizers and endure in their self-interest optimally to enhance well-being with the constraints faced100. Although individuals are expected to make rational choices every day, the outcome of these decisions is not always rational and logical due to the inbuilt heuristics. Further, we evidenced from the results that the psychosocial and health-related factors and sociodemographic variables contributed to these cognitive biases or errors.
The study results have important implications in the clinical context as they facilitate the identification of cognitive errors and their risk factors among ageing adults. This is especially crucial for providing holistic and integrated care for ageing adults. This implies the relevance of assessing psychiatric and behavioural health factors in primary health care provisions so early identification and interventions can be initiated. Further, considering cognitive errors among ageing adults, identification can facilitate better medical decision-making as it might interfere with their medical choices. In addition, the results promote the development of community programs and interventions to reduce cognitive errors and facilitate active ageing among adults by involving them in physical and social activities and improving their intellectual skills. The intellectual skills can be enhanced through context-specific adult literacy programs. We suggest that policymakers consider elevating intellectual skills and improving awareness of these basic prospects of human functioning. Future studies can focus on understanding these variables’ cause-effects through longitudinal designs and identify the cultural underpinning of cognitive biases and the regional differences in the global and Indian context. In addition, the intervention-based study would help develop and validate context-specific literacy and awareness programs for adults.
Limitations
Though this study has the strength of having a large sample size and is the first to conceptualize factors associated with committing cognitive errors among Indian adults, it has certain limitations. Firstly, the study design is cross-sectional, so the cause-and-effect relationship between the variables cannot be established. The findings only indicate the association between the variables. Secondly, the study has self-reported information regarding SRH and morbidity status. Even though the self-reported variables act as a good measure, they may be prone to biases. Third, this study does not consider cultural and regional differences in terms of cognitive errors. Future studies may use intervention-based approaches and longitudinal data.
Conclusion
The study is one of its kind and ponders the predictive factors of cognitive errors among Indian adults. Even though cognitive errors are part of everyday life, they add to the burden of ageing and are surprisingly even associated with negative psychological outcomes. This brings to the essentiality of the understanding of the determining factors of cognitive error. The study results evidenced that depression, life satisfaction, cognitive impairment, and neurological conditions, along with sociodemographic and health-related covariates, were associated with cognitive errors. It was noted that educational attainment, involvement in physical and social activities, and good quality sleep acted as reserves to inhibit and reduce cognitive errors among adults. The study results highlighted the need to enhance life satisfaction and involve adults in intellectual and physical activities, as these might delay and reduce cognitive impairment and cognitive errors. Future studies may focus on the causal relationship between these variables and developing intervention programs involving these predictive factors of cognitive errors.
Data availability
The data used for this study is available through the following website. https://www.iipsindia.ac.in/content/lasi-wave-i.
Change history
15 November 2024
A Correction to this paper has been published: https://doi.org/10.1038/s41598-024-78825-1
References
Allaire, J. C. & Gamlado, A. A. Everyday Cognition. In Encyclopedia of Geropsychology (ed Pachana, N. A.) 1–7 (Springer, Singapore, 2015). https://doi.org/10.1007/978-981-287-080-3_252-1.
Ward, E. V., Dhami, M. K. & Editorial The aging decision-maker: Advances in understanding the impact of cognitive change on decision-making. Front. Psychol. 7, (2016).
Albarracín, D. & Wyer, R. S. The cognitive impact of past behavior: Influences on beliefs, attitudes, and future behavioral decisions. J. Pers. Soc. Psychol. 79, 5–22 (2000).
Spiegel, T. Influences of personal experience in decision-making. In Exploring the Influence of Personal Values and Cultures in the Workplace 76–97 (Business Science Reference/IGI Global, Hershey, PA, US, 2017). https://doi.org/10.4018/978-1-5225-2480-9.ch005.
Acciarini, C., Brunetta, F. & Boccardelli, P. Cognitive biases and decision-making strategies in times of change: A systematic literature review. Manag. Decis. 59, 638–652 (2020).
Paulus, D., de Vries, G., Janssen, M. & Van de Walle, B. The influence of cognitive bias on crisis decision-making: Experimental evidence on the comparison of bias effects between crisis decision-maker groups. Int. J. Disaster Risk Reduct. 82, 103379 (2022).
Weller, J., Ceschi, A., Hirsch, L., Sartori, R. & Costantini, A. Accounting for individual differences in decision-making competence: Personality and gender differences. Front. Psychol. 9, (2018).
Berthet, V., Autissier, D. & de Gardelle, V. Individual differences in decision-making: A test of a one-factor model of rationality. Personal. Individ. Differ. 189, 111485 (2022).
Dietrich, C. Decision making: Factors that influence decision making, heuristics used, and decision outcomes. Inq. J. 2, (2010).
Skagerlund, K., Forsblad, M., Tinghög, G. & Västfjäll, D. Decision-making competence and cognitive abilities: Which abilities matter? J. Behav. Decis. Mak. 35, e2242 (2022).
Dale, S. Heuristics and biases: The science of decision-making. Bus. Inf. Rev. 32, 93–99 (2015).
Laguna, M. & Martí, R. Heuristics. In Encyclopedia of Operations Research and Management Science (eds Gass, S. I. & Fu, M. C.) 695–703 (Springer US, 2013). https://doi.org/10.1007/978-1-4419-1153-7_1184.
Korteling, J. E., Brouwer, A. M. & Toet, A. A neural network framework for cognitive bias. Front. Psychol. 9, (2018).
Tversky, A. & Kahneman, D. Judgment under uncertainty: Heuristics and biases. Science 185, 1124–1131 (1974).
Samanez-Larkin, G. R. & Knutson, B. Decision making in the ageing brain: Thanges in affective and motivational circuits. Nat. Rev. Neurosci. 16, 278–289 (2015).
Tannou, T., Koeberlé, S., Aubry, R. & Haffen, E. How does decisional capacity evolve with normal cognitive aging: Systematic review of the literature. Eur. Geriatr. Med. 11, 117–129 (2020).
Nyberg, L., Lövdén, M., Riklund, K., Lindenberger, U. & Bäckman, L. Memory aging and brain maintenance. Trends Cogn. Sci. 16, 292–305 (2012).
Roberts, K. L. & Allen, H. A. Perception and cognition in the ageing brain: A brief review of the short- and long-term links between perceptual and cognitive decline. Front. Aging Neurosci. 8, 39 (2016).
Fjell, A. M., Sneve, M. H., Grydeland, H., Storsve, A. B. & Walhovd, K. B. The disconnected brain and executive function decline in aging. Cereb. Cortex 27, 2303–2317 (2017).
Depping, M. K. & Freund, A. M. Normal aging and decision making: The role of motivation. Hum. Dev. 54, 349–367 (2011).
Şi̇mşek, O., Kocak, O. & Younis, M. The impact of interpersonal cognitive distortions on satisfaction with life and the mediating role of loneliness. Sustainability 13, 20 (2021).
Leykin, Y., Roberts, C. S. & DeRubeis, R. J. Decision-making and depressive symptomatology. Cogn. Ther. Res. 35, 333–341 (2011).
Lawlor, V. M. et al. Dissecting the impact of depression on decision-making. Psychol. Med. 50, 1613–1622 (2020).
Boyle, P. A. et al. Poor decision making is a consequence of cognitive decline among older persons without Alzheimer’s disease or mild cognitive impairment. PloS One 7, e43647 (2012).
Lee, D. Decision making: From neuroscience to psychiatry. Neuron 78, 233–248 (2013).
Sun, T. et al. Decision-making under ambiguity or risk in individuals with Alzheimer’s disease and mild cognitive impairment. Front. Psychiatry 11, (2020).
Sutin, A. R., Aschwanden, D., Luchetti, M., Stephan, Y. & Terracciano, A. Sense of purpose in life and subjective cognitive failures. Personal. Individ. Differ. 200, 111874 (2023).
Uğurlar, P., Sümer, N. & Posten, A. C. The cognitive cost of closeness: Interpersonal closeness reduces accuracy and slows down decision-making. Eur. J. Soc. Psychol. 51, 1007–1018 (2021).
Porcelli, A. J. & Delgado, M. R. Stress and decision making: Uffects on valuation, learning, and risk-taking. Curr. Opin. Behav. Sci. 14, 33–39 (2017).
Chi, W. C., Wolff, J., Greer, R. & Dy, S. Multimorbidity and decision-making preferences among older adults. Ann. Fam. Med. 15, 546–551 (2017).
Posadzy, K. Social and Economic Factors in Decision Making under Uncertainty: Five Essays in Behavioral Economics (Linköping University, Linköping, Sweden, 2017). https://doi.org/10.3384/diss.diva-143035.
Davis-Stober, C. P., McCarty, K. N. & McCarthy, D. M. Decision making and alcohol: Health policy implications. Policy Insights Behav. Brain Sci. 6, 64–71 (2019).
Mandolesi, L. et al. Effects of physical exercise on cognitive functioning and well-being: Biological and psychological benefits. Front. Psychol. 9, (2018).
Kasuga, H. et al. Association between participation in sports club activities and decision-making preferences in end-of-life treatment among Japanese elderly people: A cross-sectional study. Fukushima J. Med. Sci. 67, 135–142 (2021).
Cabeza, R. et al. Cognitive neuroscience of healthy aging: Maintenance, reserve, and compensation. Nat. Rev. Neurosci. 19, 701–710 (2018).
Lövdén, M., Fratiglioni, L., Glymour, M. M., Lindenberger, U. & Tucker-Drob, E. M. Education and cognitive functioning across the life span. Psychol. Sci. Public. Interest. 21, 6–41 (2020).
Boyle, P. A., Wilson, R. S., Yu, L., Buchman, A. S. & Bennett, D. A. Poor decision making is associated with an increased risk of mortality among community-dwelling older persons without dementia. Neuroepidemiology 40, 247–252 (2013).
Caudle, D. D. et al. Cognitive errors, symptom severity, and response to cognitive behavior therapy in older adults with generalized anxiety disorder. Am. J. Geriatr. Psychiatry Off J. Am. Assoc. Geriatr. Psychiatry 15, 680–689 (2007).
Santangelo, G. et al. Subjective cognitive failures and their psychological correlates in a large Italian sample during quarantine/self-isolation for COVID-19. Neurol. Sci. 42, 2625–2635 (2021).
Ruggeri, K. et al. The persistence of cognitive biases in financial decisions across economic groups. Sci. Rep. 13, 10329 (2023).
Yates, J. F. & de Oliveira, S. Culture and decision making. Organ. Behav. Hum. Decis. Process. 136, 106–118 (2016).
Mohanty, S., Patnaik, B. C. M., Satpathy, I. & Sahoo, S. K. Cognitive biases and financial decisions of potential investors during Covid-19: An exploration. Arab Gulf J. Sci. Res. ahead-of-print (2023).
Choudhary, S., Yadav, M. & Srivastava, A. P. Cognitive biases among millennial Indian investors: Do personality and demographic factors matter?. FIIB Bus. Rev. 13, 106–117 (2024).
Tairi, T. Associations between cognitive errors and mental health status in New Zealand adolescents. Behav. Cogn. Psychother. 48, 280–290 (2020).
Komura, T., Cowden, R. G., Chen, R., Andrews, R. M. & Shiba, K. Estimating the heterogeneous effect of life satisfaction on cognitive functioning among older adults: Evidence of US and UK national surveys. SSM - Ment. Health 4, 100260 (2023).
International Institute for Population Sciences. Data User Guide - Longitudinal Ageing Study in India (LASI) Wave 1, 2017-18 (2020).
Blanco, F. Cognitve Bias. InEncyclopedia of Animal Cognition and Behavior. https://doi.org/10.1007/978-3-319-47829-6 (2017).
Jones, B. D. Bounded rationality. Annu. Rev. Polit. Sci. 2, 297–321 (1999).
Simon, H. A. Theories of Bounded Rationality. Decision and Organization 161–176 Preprint at (1972).
Barros, G. & Herbert, A. Simon and the concept of rationality: Toundaries and procedures. Braz. J. Polit. Econ. 30, 455–472 (2010).
Kahneman, D., Slovic, P. & Tversky, A. Judgment under Uncertainty: Heuristics and Biases (Cambridge University Press(CUP), 1982).
Besedeŝ, T., Deck, C., Sarangi, S. & Shor, M. Age effects and heuristics in decision making. Rev. Econ. Stat. 94, 580–595 (2012).
Lo, A. W. & Zhang, R. The evolutionary origin of Bayesian heuristics and finite memory. iScience 24, (2021).
Hjeij, M. & Vilks, A. A brief history of heuristics: How did research on heuristics evolve? Humanit. Soc. Sci. Commun. 10, 1–15 (2023).
Barash, J., Brocas, I., Carrillo, J. D. & Kodaverdian, N. Heuristic to bayesian: The evolution of reasoning from childhood to adulthood. J. Econ. Behav. Organ. 159 (2019).
Lu, Y. The conjunction and disjunction fallacies: Explanations of the linda problem by the equate-to-differentiate model. Integr. Psychol. Behav. Sci. 50, 507–531 (2016).
Muhammad, T. & Meher, T. Association of late-life depression with cognitive impairment: Evidence from a cross-sectional study among older adults in India. BMC Geriatr. 21, 1–13 (2021).
Yaffe, K. et al. Depressive symptoms and cognitive decline in nondemented elderly women: A prospective study. Arch. Gen. Psychiatry 56, 425–430 (1999).
Crane, M. K., Bogner, H. R., Brown, G. K. & Gallo, J. J. The link between depressive symptoms, negative cognitive bias and memory complaints in older adults. Aging Ment. Health 11, 70715 (2007).
Sebind Kumar, A. N., Thoppil, S. P., Parassery, R. P. & Kunnukattil, S. S. Brief communication screening for depression among community–dwelling elders: Usefulness of the center for epidemiologic studies depression scale. Indian J. Psychol. Med. 38, 483–485 (2016).
Zainal, N. H. & Newman, M. G. Life satisfaction prevents decline in working memory, spatial cognition, and processing speed: Latent change score analyses across 23 years. Eur. Psychiatry 65, 1–13 (2022).
Zhu, X. et al. Satisfaction with life and risk of dementia: Findings from the Korean Longitudinal Study of Aging. J. Gerontol. B Psychol. Sci. Soc. Sci. 77, 1831–1840 (2022).
Xiao, Y. et al. Cognition impairment prior to errors of working memory based on event-related potential. Front. Behav. Neurosci. 13, (2019).
Payne, T. W. & Schnapp, M. A. The relationship between negative affect and reported cognitive failures. Depress. Res. Treat.https://doi.org/10.1155/2014/396195 (2014).
International Institute for Population Sciences (IIPS), NPHCE, MoHFW,H. T. H. C. S. of P. H. (HSPH) and the U. of S. C. (USC). Longitudinal Ageing Study in India (LASI) Wave 1, 2017-18, India Report. (2020).
Pandav, R., Fillenbaum, G., Ratcliff, G., Dodge, H. & Ganguli, M. Sensitivity and specificity of cognitive and functional screening instruments for dementia: The Indo-U.S. dementia epidemiology study. J. Am. Geriatr. Soc. 50, 554–561 (2002).
Lefebvre, M. F. Cognitive distortion and cognitive errors in depressed psychiatric and low back pain patients. J. Consult. Clin. Psychol. 49, 517–525 (1981).
Kim, D. Correlation between physical function, cognitive function, and health-related quality of life in elderly persons. J. Phys. Ther. Sci. 28, 1844–1848 (2016).
Arokiasamy, P., Bloom, D., Lee, J., Feeney, K. & Ozolins, M. Longitudinal Aging Study in India: Vision, Design, Implementation, and Preliminary Findings. Aging in Asia: Findings from New and Emerging Data Initiatives (National Academies Press (US), 2012).
Cervilla, J. A., Prince, M. & Mann, A. Smoking, drinking, and incident cognitive impairment: A cohort community based study included in the Gospel Oak project. J. Neurol. Neurosurg. Psychiatry 68, 622–626 (2000).
Wu, J. et al. Relation of cigarette smoking and alcohol drinking in midlife with risk of cognitive impairment in late life: The Singapore Chinese Health Study. Age Ageing 48, 101 (2019).
Lin, Y. K., Peters, K. & Chen, I. H. Television watching, reading, cognition, depression and life satisfaction among middle-aged and older populations: A group-based trajectory modelling analysis of national data. Health Soc. Care Community 30, e5661–e5672 (2022).
Chang, Y. H., Wu, I. C. & Hsiung, C. A. Reading activity prevents long-term decline in cognitive function in older people: Evidence from a 14-year longitudinal study. Int. Psychogeriatr. 33, 63–74.
Blake, E., Dobson, K. S., Sheptycki, A. R. & Drapeau, M. The relationship between depression severity and cognitive errors. Am. J. Psychother. 70, 203–221 (2016).
Leung, P., Orgeta, V., Musa, A. & Orrell, M. Emotional distress mediates the relationship between cognitive failures, dysfunctional coping, and life satisfaction in older people living in sheltered housing: A structural equation modelling approach. Int. J. Geriatr. Psychiatry 34, 179–185 (2019).
O’Rourke, N., Sixsmith, A., Kirshner, G. & Osher, Y. Perceived cognitive failures and quality of life for older adults with bipolar disorder. J. Affect. Disord. 287, 433–440 (2021).
Culpepper, L., Lam, R. W. & McIntyre, R. S. Cognitive impairment in patients with depression: Awareness, assessment, and management. J. Clin. Psychiatry 78, 3185 (2017).
Crawford, T. J. et al. The effects of previous error and success in Alzheimer’s disease and mild cognitive impairment. Sci. Rep. 9, 20204 (2019).
Delaney, R., Strough, J., Parker, A. M. & de Bruin, W. B. Variations in decision-making profiles by age and gender: A cluster-analytic approach. Personal. Individ. Differ. 85, 19–24 (2015).
Villanueva-Moya, L. & Expósito, F. Gender differences in decision-making: The effects of gender stereotype threat moderated by sensitivity to punishment and fear of negative evaluation. J. Behav. Decis. Mak. 34, 706–717 (2021).
Okamoto, S. et al. Decomposition of gender differences in cognitive functioning: National Survey of the Japanese elderly. BMC Geriatr. 21, 38 (2021).
Bruch, E. & Feinberg, F. Decision-making processes in social contexts. Annu. Rev. Sociol. 43, 207–227 (2017).
Wang, P. & Tan, C. The effects of social class on individuals’ decision-making tendencies in a prestige-money game: Social value or instrumental value?. J. Gambl. Stud. 35, (2019).
Lee, D. & Jackson, M. The simultaneous effects of socioeconomic disadvantage and child health on children’s cognitive development. Demography 54, 1845–1871 (2017).
Hagan, K. et al. Cumulative social disadvantage and health-related quality of life: National health interview survey 2013–2017. BMC Public. Health 23, 1710 (2023).
Röhr, S. et al. Social determinants and lifestyle factors for brain health: Implications for risk reduction of cognitive decline and dementia. Sci. Rep. 12, 12965 (2022).
Liu, H., Zhang, Y., Burgard, S. A. & Needham, B. L. Marital status and cognitive impairment in the United States: Evidence from the National Health and Aging trends Study. Ann. Epidemiol. 38, 28–34e2 (2019).
Jennings, E. A., Farrell, M. T., Liu, Y. & Montana, L. Associations between cognitive function and marital status in the United States, South Africa, Mexico, and China. SSM - Popul. Health 20, 101288 (2022).
Saenz, J. L., Downer, B., Garcia, M. A. & Wong, R. Rural/urban dwelling across the life-course and late-life cognitive ability in Mexico. SSM - Popul. Health 17, 101031 (2022).
Jin, M., Ji, L. & Peng, H. The relationship between cognitive abilities and the decision-making process: The moderating role of self-relevance. Front. Psychol. 10, 1892 (2019).
Harling, G. et al. Social contact, social support, and cognitive health in a population-based study of middle-aged and older men and women in rural South Africa. Soc. Sci. Med. 260, 113167 (2020).
Hikichi, H., Kondo, K., Takeda, T. & Kawachi, I. Social interaction and cognitive decline: Results of a 7-year community intervention. Alzheimers Dement. Transl. Res. Clin. Interv. 3, 23–32 (2017).
Smith, T. W., Follick, M. J., Ahern, D. K. & Adams, A. Cognitive distortion and disability in chronic low back pain. Cogn. Ther. Res. 10, 201–210 (1986).
Zheng, J., Liu, J. & An, R. Functional limitation and cognitive impairment among 80 + year old Chinese. Australas. J. Ageing 35, 266–272 (2016).
Gildner, T. E., Liebert, M. A., Kowal, P., Chatterji, S. & Snodgrass, J. J. Associations between sleep duration, sleep quality, and cognitive test performance among older adults from six middle income countries: Results from the study on Global Ageing and Adult Health (SAGE). J. Clin. Sleep. Med. 10, 613–621 (2014).
Kumar, M., Srivastava, S. & Muhammad, T. Relationship between physical activity and cognitive functioning among older Indian adults. Sci. Rep. 12, 2725 (2022).
Law, C. K., Lam, F. M., Chung, R. C. & Pang, M. Y. Physical exercise attenuates cognitive decline and reduces behavioural problems in people with mild cognitive impairment and dementia: A systematic review. J. Physiother. 66, 9–18 (2020).
Benito-León, J., Ghosh, R., Lapeña-Motilva, J., Martín-Arriscado, C. & Bermejo-Pareja, F. Association between cumulative smoking exposure and cognitive decline in non-demented older adults: NEDICES study. Sci. Rep. 13, 5754 (2023).
Nadar, M., Sh., Hasan, A. M. & Alsaleh, M. The negative impact of chronic tobacco smoking on adult neuropsychological function: A cross-sectional study. BMC Public Health 21, 1278 (2021).
Rodriguez-Sickert, C. Homo Economicus. In Handbook of Economics and Ethics (Edward Elgar Publishing, 2009).
Funding
The authors have not received any funding to carry out this study.
Open access funding provided by Vellore Institute of Technology.
Author information
Authors and Affiliations
Contributions
C.V. conceptualized and analyzed the data. P.P. and E.P. wrote the main manuscript. T.M. supervised data analysis. Critical revision of the manuscript for intellectual content: E.P. and T.M. All authors read and approved the final draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
This study employed secondary data, Longitudinal Ageing Stusy in India (LASI), which is available publicly. Hence, ethical approval is not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error in the Abstract. Full information regarding the corrections made can be found in the correction for this Article.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Irshad, C.V., Padma Sri Lekha, P., Abdul Azeez, E.P. et al. Late-life psychiatric factors and life satisfaction are associated with cognitive errors: evidence from an experimental module of a large-scale survey in India. Sci Rep 14, 25917 (2024). https://doi.org/10.1038/s41598-024-76180-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-76180-9
