
Abstract
This study investigates the relationship of neutrophil–lymphocyte ratio (NLR) with the risk of all-cause and cardiovascular mortality in patients with cardiovascular disease. The data for this analysis came from 2239 participants with cardiovascular disease of the National Health and Nutrition Examination Survey conducted between 1999–2018. The optimal cutoff point for NLR was determined using maximally selected rank statistics. Survival analysis was performed using Cox regression models to assess the impact of NLR on the risk of all-cause mortality and cardiovascular mortality. Restricted cubic spline was used to visualize the association of NLR with mortality risk. Subgroup analysis was performed to examine the relationship between NLR and mortality within subgroups based on age, sex, diabetes and hypertension. During a median follow-up period of 6.7 (IQR, 3.3–10.9) years, 992 all-cause deaths occurred, including 381 cardiovascular deaths. Our study revealed that NLR is a risk factor for all-cause mortality (HR: 1.15 95%Cl: 1.11 ~ 1.19) and cardiovascular mortality (HR: 1.14 95%Cl: 1.08 ~ 1.2) among patients with cardiovascular disease. The restricted cubic spline regression analysis showed a non-linear association between NLR and all-cause mortality (p < 0.05 for nonlinearity) in cardiovascular patients. This association remained robust in subgroup analyses stratified by age, sex, diabetes, and hypertension. Conclusion NLR stands as a significant risk factor for both all-cause and cardiovascular mortality among patients with cardiovascular disease.
Similar content being viewed by others
Introduction
As population aging progresses, the high incidence of cardiovascular disease (CVD) is becoming an important public health problem1. Despite significant progress in treatment, CVD remains a major cause of mortality worldwide2,3. Inflammatory processes, including cellular immunity, critically regulate the onset, progression, and outcomes of cardiovascular disease4,5. Many inflammatory factors also could predict cardiovascular events risk.
The neutrophil–lymphocyte ratio (NLR) is an easily measurable inflammatory marker derived from routine blood draws, determined by the ratio of neutrophil count to lymphocyte count. It reflects the equilibrium between two facets of the immune system: innate (neutrophils) and adaptive (lymphocytes) immunity. Therefore, NLR has been widely studied by researchers and has been shown to be a risk predictor for numerous diseases and mortality6. In patients with coronary artery disease, NLR has proven to be a superior predictor for myocardial infarct or mortality compared to neutrophil or monocyte counts7.
Therefore, we conducted this study to investigate the association between NLR and the risks of all-cause and cardiovascular mortality in patients with cardiovascular disease from the National Health and Nutrition Examination Survey (NHANES).
Materials and methods
Study design and population
The NHANES was a nationwide research project administered by the Centers for Disease Control and Prevention (CDC) and the National Centers for Health Statistics (NCHS). The study protocol had received ethical approval from the National Centre for Health Statistics research ethics review board (ERB), and all individuals provided written informed consent at enrollment (the website is https://www.cdc.gov/nchs/nhanes/irba98.htm). All methods were performed in accordance with relevant guidelines and regulations. The study enrolled patients with cardiovascular disease aged ≥ 18 years from NHANES 1999–2018. Participants were excluded if they lacked mortality data, complete blood count parameters, essential covariate information, or if they were pregnant.
Definition of CVD
In this study, we defined CVD based on self-reported diagnoses of heart failure, coronary heart disease, angina, myocardial infarction, or stroke. The information was obtained through medical condition questionnaires during in-person interviews. Participants were asked whether they had been informed by a doctor or other health professional that they have or have had any of the following: heart failure, coronary heart disease, angina, myocardial infarction, or stroke. Those who responded “yes” to any of these inquiries were classified as individuals with CVD.
Outcomes
The primary outcomes for this study were all-cause mortality and cardiovascular mortality. Mortality status was determined using the Public-use Linked Mortality Files. Follow-up time ranged from the MEC interview date to the date of death or the end of the follow-up (December 31, 2019). All-cause death was defined as death from any cause. Cardiovascular mortality was defined using International Classification of Diseases coding, including the death caused by heart diseases (I00–I09, I11, I13, I20–I51) and cerebrovascular diseases (I60–I69).
Covariates
Participants’ baseline data was collected through questionnaires and laboratory tests, including age (years), sex (male or female), race /ethnicity (non-Hispanic white, non-Hispanic black, Mexican American, and others), education level (less than high school, high school or equivalent, and college or above), marital status (married or living with a partner; never married; widowed, divorced, separated). Poverty-income ratio (PIR) categorized as ≤ 1.30, 1.31–3.50, > 3.50, and unknown. Never smokers were defined as individuals who reported smoking less than 100 cigarettes in their entire life. Those who had smoked more than 100 cigarettes in their lifetime and were currently smoking were categorized as current smokers. Individuals who had smoked more than 100 cigarettes but had ceased smoking at the time of the survey were labeled as former smokers. The drinking status (yes or no) depends on whether participants consumed 12 or more drinks per year. Because there were relatively few individuals with a BMI < 18.5 kg/m2, BMI were grouped into three categories based on their BMI values: < 25, 25–30, and > 30 kg/m2. A diagnosis of diabetes was determined by criteria as follows: self-reported diagnosis of diabetes, use of insulin or oral hypoglycemic drugs, fasting blood glucose levels ≥ 7.0 mmol/L, random blood glucose or two-hour oral glucose tolerance test (OGTT) blood glucose levels ≥ 11.1 mmol/L, or glycated hemoglobin A1c (HbA1c) levels ≥ 6.5%. Hypertension was defined as meeting one or more of the following criteria: self-reported hypertension, systolic blood pressure equal to or greater than 140 mmHg, diastolic blood pressure equal to or greater than 90 mmHg, or current use of antihypertensive medications. Data regarding age, gender, and serum creatinine were utilized to calculate eGFR using the CKD Epidemiology Collaboration (CKD-EPI) equation8. Low-density lipoprotein cholesterol (LDL), total cholesterol (TC), serum creatinine, and HbA1c levels and blood cell counts were obtained from laboratory test results. The medications, including beta-blockers, renin–angiotensin–aldosterone system blockers (RAS blockers), and statins, were obtained from participant-reported prescription medicines taken in the past month.
Statistical analysis
The optimal cutoff point for NLR corresponding to the most significant association with survival outcomes was determined using maximally selected rank statistics facilitated by the ‘survminer’ package. Participants were divided into higher and lower NLR groups based on the cutoff point. Continuous variables are presented as mean ± SD or median (interquartile range, IQR), depending on their distribution. Categorical variables are expressed as numbers (n) and percentages (%). To compare continuous variables between groups, the independent samples Student’s t-test or Mann–Whitney U-test was performed based on the distribution normality, while categorical data were compared using the chi-square test. An analysis of multivariable Cox regression models was applied to investigate the relationship between NLR and mortality among individuals with CVD. Model 1 was a crude model. Model 2 was adjusted for age, sex, race/ethnicity, education level, marital status, and poverty income ratio. Model 3 was the main model and included Model 2 variables plus smoking status, drinking status, BMI category, diabetes, hypertension, LDL cholesterol, and eGFR. Sensitivity analysis was conducted by adding the three medications, beta-blockers, RAS blockers, and statins, to Model 3 for multivariate Cox regression analysis. Mortality outcomes were assessed using Kaplan–Meier survival curves stratified by NLR categories and evaluated with the log-rank test. We employed a restricted cubic spline model to generate smooth curves, enabling the exploration of potential nonlinear dose–response relationships between NLR and mortality. Nonlinearity was assessed using a likelihood ratio test, comparing a model with only a linear term to a model with both linear and cubic spline terms. Subgroup analysis was performed to examine the relationship between NLR and mortality within distinct subgroups. Interactions among subgroups were evaluated using the likelihood ratio test. All analyses were performed using the statistical packages R (http://www.R-project.org, The R Foundation) and Free Statistics software versions 1.9.2, and a two-tailed p < 0.05 was considered statistically significant.
Result
Baseline characteristics
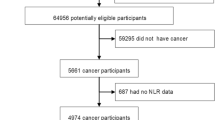
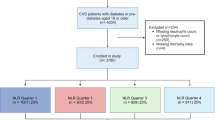
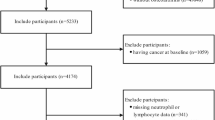
A total of 2239 participants with CVD were enrolled in the study, with Fig. 1 providing a detailed flowchart outlining the meticulous process of participant selection. Based on maximally selected rank statistics, the optimal NLR cutoff value is determined to be 2.89. Consequently, participants were divided into higher NLR group and lower NLR group. The baseline characteristics of the patients grouped based on NLR were listed in Table 1 and Supplementary Table S1 online. The study cohort had a mean age of 66.6 ± 12.6 years, with 1277 participants (57.0%) being male.

Flowchart of participants selection.
Association of NLR with mortality
During a median follow-up of 6.7 (IQR 3.3–10.9) years, there were a total of 922 occurrences of all-cause mortality, including 381 cardiovascular deaths. In the model 1 (unadjusted model), NLR was significantly associated with an increased risk of all-cause mortality (hazard ratio (HR): 1.22 95%Cl: 1.18 ~ 1.25) and cardiovascular mortality (HR: 1.21 95%Cl: 1.16 ~ 1.26). After multivariate adjustment, model 3 showed that each one-unit increase in the NLR was associated with a 15% higher risk of all-cause mortality and 14% higher risk of cardiovascular mortality. As a categorical variable, the higher NLR group had 1.57 and 1.66 times the risk of all-cause and cardiovascular mortality compared to lower NLR group (Table 2). Kaplan–Meier analysis showed that the survival rate for the higher NLR group was significantly lower than that of the lower NLR group for both all-cause and cardiovascular mortality (p < 0.0001) (Fig. 2). The sensitivity analysis showed that adding medications(beta-blockers, RAS blockers, and statins) into Model 3 as covariates resulted in findings consistent with the main results, confirming the robustness of the outcomes. (see Supplementary Table S2 online).

Kaplan–Meier curves of all-cause mortality and cardiovascular mortality among participates with CVD. Kaplan–Meier curves of the survival rate and the number of at-risk cardiovascular patients with higher and lower NLR values (NLR breakpoint: 2.89). (A) All-cause mortality. (B) Cardiovascular mortality.
Subgroup analyses
In subgroup analyses stratified by sex, age, diabetes, hypertension, a consistently observed association was found between higher NLR and increased risks of all-cause and cardiovascular mortality (Fig. 3). Furthermore, no significant interaction was observed between the aforementioned factors and NLR (p for interaction > 0.05). These findings suggest that the association between elevated NLR and higher mortality risk remains consistent across subgroups of potential confounders.

Subgroup analysis of the associations between neutrophil–lymphocyte ratio and mortality Notes: Adjusted for age, sex, race/ethnicity, educational level, marital status, poverty income ratio, smoking statues, drinking status, body mass index category, diabetes, hypertension, low density lipoprotein-cholesterol cholesterol, estimated glomerular filtration rate.
Nonlinear regression of NLR and mortality
The RCS curve in Fig. 4A illustrates the association between continuous NLR and the risk of all-cause mortality in participants with CVD. The result showed a positive non-linear association between NLR and all-cause mortality (nonlinear p = 0.024), characterized by a J-shaped curve with an initial plateau followed by an upward trend. RCS analysis in Fig. 4B demonstrated a linear correlation between NLR and cardiovascular mortality (nonlinear p = 0.087), with a curve exhibiting a similar pattern to that in Fig. 4A.

Restricted cubic spline models of neutrophil–lymphocyte ratio with mortality The association of neutrophil–lymphocyte ratio (NLR) with all-cause (A) and cardiovascular mortality (B) among cardiovascular patients visualized by restricted cubic spline analysis (NLR breakpoint: 2.89). Notes: Adjusted for age, sex, race/ethnicity, educational level, marital status, poverty income ratio, smoking statues, drinking status, body mass index category, diabetes, hypertension, low density lipoprotein-cholesterol cholesterol, estimated glomerular filtration rate. Only 99% of the data is displayed.
Discussion
In our study, we observed that a higher NLR was independently predictive of increased risk of all-cause and cardiovascular mortality among patients with CVD. The association between NLR and mortality remains robust after conducting subgroup analysis. Moreover, the RCS analyses revealed non-linear positive correlations between NLR and all-cause mortality. These findings underscore the potential value of NLR as a cost-effective marker for risk stratification and prognosis assessment in clinical practice.
Neutrophils play a crucial role in the development of coronary atherosclerosis and the occurrence of cardiovascular events9. Lymphocytes are associated with a reduced risk of cardiovascular events10. NLR reflects the ratio of neutrophils to lymphocytes, representing the balance between innate and adaptive immune responses, and can be used even in patients with a normal WBC count. Previous studies have demonstrated that NLR is a risk factor for cardiovascular events and all-cause mortality11. Azab et al. found that in the NSTEMI population, NLR had superior predictive value for mortality compared to neutrophils or lymphocytes separately12. Additionally, NLR has also been found to be associated with coronary artery stenosis and plaque characteristics13. Moreover, NLR is also being investigated as a risk factor for hypertension, heart failure, and acute coronary syndrome14,15,16. NLR has also been included in many scoring systems, such as the systemic immune-inflammation index and the Naples score17,18. And these scores have been shown to be significantly associated with cardiovascular disease prognosis19. Our study confirmed the association between NLR and mortality in cardiovascular patients and the result remains robust even after subgroup analyses or adding medications in the Cox model. We also identified a non-linear relationship between NLR and all-cause mortality in this population. Additionally, the cut-off value in our study is 2.89. Different studies currently utilize varying cut-off values, and some suggested that 3 may be a reasonable cut-off point20,21.
Inflammation disfunction plays a crucial role in the progression of cardiovascular disease. As a marker of immune dysfunction, NLR is an important risk factor for cardiovascular disease. Neutrophils can release various inflammatory mediators, such as cytokines and proteases5. During the progression of atherosclerosis, neutrophils release chemotactic proteins that regulate the entry of monocytes into atherosclerotic lesions 22. Myeloperoxidase released by neutrophils leads to the oxidation of LDL and accelerates the transformation of macrophages into foam cells23. Additionally, the release of granule proteins can activate macrophages, thereby promoting cytokine secretion24. Both monocyte recruitment and macrophage activation are crucial steps in the progression of atherosclerosis. Furthermore, neutrophil infiltration into atherosclerotic plaques has been observed in atherectomy specimens from ACS patients9. Neutrophils are associated with vulnerable plaques, which are considered critical for plaque rupture25,26. As for lymphocytes, a low lymphocyte count is associated with an increased risk of developing cardiovascular events and mortality 27,28. A reduction in lymphocytes is also associated with the advancement of atherosclerosis29,30. Specifically, a reduction in T lymphocyte count is associated with poor prognosis in patients with myocardial infarction31. NLR is the ratio of neutrophils to lymphocytes, which helps explain why it is a risk factor for cardiovascular disease.
The NLR is a simple, inexpensive, and easily available parameter. However, it is important to note that NLR values may fluctuate with each measurement. Therefore, its variability must be taken into account when interpreting NLR results in clinical practice. Relying on a single indicator for disease prognosis is challenging; thus, it is crucial to account for factors such as the patient’s age, comorbid conditions, and other laboratory results. The ease of measurement and low cost make NLR a convenient tool for dynamic assessment of disease prognosis. Obtaining a baseline NLR value and monitoring changes from baseline may be useful for further assessment. As a cardiovascular risk factor, NLR can be used to stratify risk, assess severity, monitor treatment outcomes, or be incorporated into cardiovascular risk prediction models. Overall, accurate interpretation of NLR results is essential for maximizing its clinical utility.
Limitations
Firstly, despite adjusting for numerous potential confounding factors in our analysis, the possibility of residual confounding from other unknown variables cannot be entirely eliminated. Secondly, the NLR was measured at baseline, potentially limiting its ability to reflect variability over time. Furthermore, the diagnosis of cardiovascular disease in this study was based on self-reported diagnosis, which may have retrospective bias. Finally, as this study focused on individuals with cardiovascular disease in the United States, its generalizability to other populations may be limited.
Conclusion
NLR stands as a significant risk factor for both all-cause and cardiovascular mortality among patients with cardiovascular disease.
Data availability
Data described in the manuscript will be made publicly and freely available without restriction at [https://www.cdc.gov/nchs/nhanes].
Abbreviations
- CVD:
-
Cardiovascular disease
- NHANES:
-
National Health and Nutrition Examination Survey
- CVD:
-
Cardiovascular disease
- NLR:
-
Neutrophil–lymphocyte ratio
References
Virani, S. S. et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 141(9), e139–e596 (2020).
Townsend, N. et al. Epidemiology of cardiovascular disease in Europe. Nature reviews Cardiology 19(2), 133–143 (2022).
Roth, G. A. et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. Journal of the American College of Cardiology 76(25), 2982–3021 (2020).
Libby, P., Nahrendorf, M. & Swirski, F. K. Leukocytes Link Local and Systemic Inflammation in Ischemic Cardiovascular Disease: An Expanded “Cardiovascular Continuum”. Journal of the American College of Cardiology 67(9), 1091–1103 (2016).
Silvestre-Roig, C., Braster, Q., Ortega-Gomez, A. & Soehnlein, O. Neutrophils as regulators of cardiovascular inflammation. Nature reviews Cardiology 17(6), 327–340 (2020).
Song, M., Graubard, B. I., Rabkin, C. S. & Engels, E. A. Neutrophil-to-lymphocyte ratio and mortality in the United States general population. Scientific reports 11(1), 464 (2021).
Horne, B. D. et al. Which white blood cell subtypes predict increased cardiovascular risk?. Journal of the American College of Cardiology 45(10), 1638–1643 (2005).
Inker, L. A. et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N Engl J Med 385(19), 1737–1749 (2021).
Naruko, T. et al. Neutrophil infiltration of culprit lesions in acute coronary syndromes. Circulation 106(23), 2894–2900 (2002).
Kofink, D. et al. Routinely measured hematological parameters and prediction of recurrent vascular events in patients with clinically manifest vascular disease. PloS one 13(9), e0202682 (2018).
Adamstein, N. H. et al. The neutrophil-lymphocyte ratio and incident atherosclerotic events: analyses from five contemporary randomized trials. Eur Heart J 42(9), 896–903 (2021).
Azab, B. et al. Usefulness of neutrophil to lymphocyte ratio in predicting short- and long-term mortality after non-ST-elevation myocardial infarction. The American journal of cardiology 106(4), 470–476 (2010).
Ateş, A. H. et al. Association of Neutrophil-to-Lymphocyte Ratio with the Severity and Morphology of Coronary Atherosclerotic Plaques Detected by Multidetector Computerized Tomography. Acta Cardiologica Sinica 32(6), 676–683 (2016).
Hong, S., He, H., Fang, P., Liu, S. & Chen, C. Association of neutrophil-to-lymphocyte ratio and risk of cardiovascular and all-cause mortality in hypertension patients. Heliyon 10(6), e27517 (2024).
Wu, C. C., Wu, C. H., Lee, C. H. & Cheng, C. I. Association between neutrophil percentage-to-albumin ratio (NPAR), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and long-term mortality in community-dwelling adults with heart failure: evidence from US NHANES 2005–2016. BMC cardiovascular disorders 23(1), 312 (2023).
Dong, C. H., Wang, Z. M. & Chen, S. Y. Neutrophil to lymphocyte ratio predict mortality and major adverse cardiac events in acute coronary syndrome: A systematic review and meta-analysis. Clinical biochemistry 52, 131–136 (2018).
Hayıroğlu, M. et al. Evaluating systemic immune-inflammation index in patients with implantable cardioverter defibrillator for heart failure with reduced ejection fraction. Pacing and clinical electrophysiology : PACE 45(2), 188–195 (2022).
Pay, L. et al. Evaluation of Naples prognostic score to predict long-term mortality in patients with pulmonary embolism. Biomarkers in medicine 18(6), 253–263 (2024).
Şaylık, F. et al. Evaluation of Naples Score for Long-Term Mortality in Patients With ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention. Angiology 75(8), 725–733 (2024).
Kourilovitch, M. & Galarza-Maldonado, C. Could a simple biomarker as neutrophil-to-lymphocyte ratio reflect complex processes orchestrated by neutrophils?. Journal of translational autoimmunity 6, 100159 (2023).
Buonacera A, Stancanelli B, Colaci M, Malatino L. Neutrophil to Lymphocyte Ratio: An Emerging Marker of the Relationships between the Immune System and Diseases. International journal of molecular sciences 2022, 23(7).
Soehnlein, O., Lindbom, L. & Weber, C. Mechanisms underlying neutrophil-mediated monocyte recruitment. Blood 114(21), 4613–4623 (2009).
Delporte, C. et al. Impact of myeloperoxidase-LDL interactions on enzyme activity and subsequent posttranslational oxidative modifications of apoB-100. Journal of lipid research 55(4), 747–757 (2014).
Soehnlein, O. et al. Neutrophil primary granule proteins HBP and HNP1-3 boost bacterial phagocytosis by human and murine macrophages. The Journal of clinical investigation 118(10), 3491–3502 (2008).
Silvestre-Roig, C. et al. Externalized histone H4 orchestrates chronic inflammation by inducing lytic cell death. Nature 569(7755), 236–240 (2019).
Ionita, M. G. et al. High neutrophil numbers in human carotid atherosclerotic plaques are associated with characteristics of rupture-prone lesions. Arteriosclerosis, thrombosis, and vascular biology 30(9), 1842–1848 (2010).
Núñez, J. et al. Relationship between low lymphocyte count and major cardiac events in patients with acute chest pain, a non-diagnostic electrocardiogram and normal troponin levels. Atherosclerosis 206(1), 251–257 (2009).
Zidar, D. A. et al. Association of Lymphopenia With Risk of Mortality Among Adults in the US General Population. JAMA network open 2(12), e1916526 (2019).
Major, A. S., Fazio, S. & Linton, M. F. B-lymphocyte deficiency increases atherosclerosis in LDL receptor-null mice. Arteriosclerosis, thrombosis, and vascular biology 22(11), 1892–1898 (2002).
Ducloux, D., Challier, B., Saas, P., Tiberghien, P. & Chalopin, J. M. CD4 cell lymphopenia and atherosclerosis in renal transplant recipients. Journal of the American Society of Nephrology : JASN 14(3), 767–772 (2003).
Boag, S. E. et al. T lymphocytes and fractalkine contribute to myocardial ischemia/reperfusion injury in patients. The Journal of clinical investigation 125(8), 3063–3076 (2015).
Acknowledgements
We thank all investigators and participants in the NHANES study for their contributions.
Funding
This study was not funded by any external source.
Author information
Authors and Affiliations
Contributions
GS.W. contributed to the conception and design of the work. XJ.L. and MX.L. conducted research, analyzed data and drafted the manuscript. GS.W. critically revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, X., Liu, M. & Wang, G. The neutrophil–lymphocyte ratio is associated with all-cause and cardiovascular mortality in cardiovascular patients. Sci Rep 14, 26692 (2024). https://doi.org/10.1038/s41598-024-76836-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-76836-6
Keywords
This article is cited by
-
Timing-dependent anti-inflammatory effects of empagliflozin in monocyte-derived macrophages from post-myocardial infarct patients with type 2 diabetes
Cardiovascular Diabetology (2026)
-
Association of the novel remnant cholesterol inflammatory index with acute coronary syndrome risk in hospitalized patients with diabetes: a two-center study
Scientific Reports (2026)
-
Prognostic value of neutrophil-to-lymphocyte ratio for the clinical outcomes of chronic kidney diseases: an update systematic review and meta-analysis
BMC Nephrology (2025)
-
Neutrophil-to-lymphocyte ratio as a sex-specific predictor of short-term mortality in hospitalised older adults with COVID-19: a pragmatic biomarker of inflammaging in acute vulnerability
Immunity & Ageing (2025)
-
Constructing a nomogram for short-term prognosis in postoperative patients with aneurysmal subarachnoid hemorrhage: a two-center retrospective study
Scientific Reports (2025)
