
Abstract
Introduction: Down Syndrome Regression Disorder (DSRD) is a neuropsychiatric condition causing insomnia, catatonia, encephalopathy, and obsessive-compulsive behavior in otherwise healthy individuals with Down syndrome (DS). Smaller cohorts have identified heterogenous diagnostic abnormalities which have predicted immunotherapy responsiveness although pattern analysis in a large cohort has never been performed. Methods: A multi-center, retrospective study of individuals with DSRD was performed. Individuals met international consensus criteria for DRSD and were aged 10–30 years. Clinical, demographic, and diagnostic data was extracted for all individuals. Serum studies were compared to a group of individuals with DS only. Results: A total of 164 individuals with DSRD were identified. Individuals with DSRD were more likely to have a positive antinuclear antibody, low complement 3, abnormal cytokines, and elevated ferritin levels. In a minority of individuals, EEG (30%), MRI (33%) and cerebrospinal fluid (CSF) (21%) were abnormal. Individuals with CSF abnormalities demonstrated greater disease severity at diagnosis on the BFCRS and NPI-Q (p = 0.02 and p < 0.001). Abnormalities in cytokines (p = 0.03), neuroimaging (p < 0.001), and CSF (p = 0.02) were predictive of immunotherapy responsiveness. When MRI and LP were both abnormal or when EEG, MRI and LP were all abnormal, the odds of immunotherapy responsiveness approached 100% (p = 0.01, 95%CI: 1.75–105.1, OR: 13.56 and p = 0.02, 95%CI: 1.37–86.87, OR: 10.91, respectively). Conclusions: In a population of individuals diagnosed with DSRD, abnormalities in serum cytokine levels, neuroimaging findings, and CSF analysis emerged as indicators of disease severity and responsiveness to immunotherapy.
Similar content being viewed by others


Introduction
Down syndrome (DS) is one of the most common genetic disorders and is caused by trisomy of chromosome 211. Individuals with DS are at risk for a variety of neurologic and psychiatric conditions including autism spectrum disorder (ASD), Alzheimer’s disease (AD), and Down Syndrome Regression Disorder (DSRD)2,3,4. Recently characterized in the last decade, DSRD is a condition in which otherwise healthy individuals with DS experience an acute or sub-acute functional status decline and have a myriad of symptoms including agitation, bradykinesia, catatonia, encephalopathy, insomnia, mutism, obsessive-compulsive tendencies, and the loss of ability to perform activities of daily living2,4,5,6,7,8. Persons with DSRD typically present during adolescence or young adulthood with the majority of cases developing between ages 10–30 years. The acute/subacute presentation and age at onset aids in distinguishing DSRD from other neuropsychiatric conditions which are co-morbid with DS, such as ASD and AD9,10,11.
Although the exact etiologies of DSRD remain unclear, several smaller studies have documented clear abnormalities in neuroimaging and cerebrospinal fluid (CSF) analysis6,12. In addition, these abnormalities are predictive of immunotherapy responsiveness, with rates of improvement as high as 80%.6,7,12,13, This diagnostic-therapeutic gap, is felt to indicate the possibility of multiple unknown mechanisms for DSRD. One proposed hypothesis for neurologic disease in individuals with DSRD is overactivation of JAK/STAT signaling cascades, which has been demonstrated in persons with DS and can be attributed to the multiple interferon receptor genes located on chromosome 21 and has been proposed as a possible mechanism for DSRD14,15. Given the underlying chronic inflammatory state of persons with DS and the documented clinical improvement of individuals with DSRD receiving immunotherapy, it is possible that DSRD may have an underlying autoimmune or inflammatory pathogenesis, although this has not been explicitly identified at this time.
This study sought to systematically evaluate the presence of clinically available diagnostic abnormalities in the serum, CSF, and neuroimaging of individuals with DSRD and determine if these abnormalities were predictive of subsequent immunotherapy responsiveness.
Results
In total, 203 individuals met inclusion criteria for the study although complete data sets were only available on 164 (81%). Of the 39 individuals without complete data sets, 29 (74%) had no LP data available, 7 (18%) had incomplete MRI sequencing performed or had neuroimaging done on a 1.5 T scanner and 3 (8%) had incomplete clinical data available. All cases with complete data sets were independently confirmed to have DSRD by the independent arbiter (100% agreement). Demographic and clinical features of the cohort are presented in Table 1. The median age of onset was 16 (interquartile range (IQR): 13–19) with a median age at diagnosis of 18 (IQR: 15-21.75) and a median age at first treatment of 19 (IQR: 15–22). There was a preceding trigger present in 53% (n = 87) of cases with infection (n = 23, 35%) or change of home/school environment (n = 22, 34%) being the most common temporal associations. Catatonia was present in 75% (n = 123) of individuals. Patients who received immunotherapy largely received IVIg (139, 85%) with smaller numbers of individuals receiving rituximab (15, 9%), steroids (14, 9%), mycophenolate mofetil (7, 4%) and tofacitinib (2, 1%). There were 13 individuals who were on more than one immunotherapy with the most frequent combination being IVIg and mycophenolate (8, 62%), IVIg and rituximab (3, 23%), and one being on IVIg and steroids (1, 8%).
Laboratory results for individuals with DSRD and DSwR are reported in Table 2. Multiple serum labs were elevated in individuals with DSRD compared to individuals with DSwR and included antinuclear antibody (ANA) (p < 0.001, 95%CI: 3.49–9.11), complement 3 (C3) (p = 0.02, 95%CI: 1.16–5.98), cytokines (p = 0.03, 95%CI: 1.55–9.55), erythrocyte sedimentation rate (ESR) (p < 0.001, 95%CI: 3.13–9.18), and ferritin (p = 0.04, 95%CI: 1.05–3.54). The most frequently elevated cytokines in the DSRD cohort were soluble interleukin (IL) 2 receptor (sIL2r) (67%), IL-6 (22%), and IL-10 (30%), with only sIL2-R being statistically significant compared to individuals with DSwR (p = 0.04, 95%CI: 1.09–92.1). Individuals with DSwR were noted to have TNF-alpha abnormalities more frequently than individuals with DSRD (p = 0.04, 95%CI: 0.02–0.92). The median time to nadir of symptoms was significantly shorter (four weeks) in individuals with cytokine abnormalities than in those without (nine weeks) (p = 0.02, 95%CI: 1.17–3.67). Other lab-based abnormalities were not associated with clinical or demographic data or with disease severity.
Neurodiagnostic data is also reported in Table 2. The rate of EEG abnormalities was 30% (n = 40), with the large majority being diffuse bilateral slowing (33/40, 83%). Neuroimaging abnormalities were detected in 33% (n = 54) of individuals, with the majority having bilateral susceptibility-weighted imaging (SWI) signal abnormalities in the basal ganglia (40/54, 74%). Representative imaging findings are presented in Fig. 1. Compared to a cohort of individuals with DSwR who had neuroimaging performed for any reason outside of the neonatal period, there was a statistically significant higher incidence of T2 signal prolongation and gradient echo sequences (GRE)/SWI signal abnormalities (p < 0.001, 95%CI: 1.70–5.87). The rate of abnormalities on lumbar puncture was 21% (n = 34). The most frequent abnormalities in the cerebrospinal fluid were elevated CSF protein and elevated IgG index which were present in seven individuals each (14%). Independently, there were seven individuals with both elevations in CSF total protein and IgG index (7%). Individuals with DSRD who had CSF abnormalities demonstrated greater disease severity at diagnosis with a median BFCRS of 29 and NPI-Q total score of 45 compared to those without which were 21 and 30, respectively (p = 0.02, 95%CI: 1.07–2.64; p < 0.001, 95%CI: 1.39–6.21). This difference was not observed in individuals with EEG (p = 0.41 and p = 0.66) or MRI (p = 0.37 and p = 0.22) abnormalities.
Individuals with DSRD and diagnostic abnormalities were noted to have disease severity differences and unique clinical phenotypes (Table 3). No serum biomarkers were predictive of the presence of catatonia or more severe clinical symptomatology as defined by the BFCRS ≥ 20 and NPI-QSS ≥ 10. The presence of either MRI and LP abnormalities was predictive of the presence of catatonia (p = 0.02, 95%CI: 1.13–2.35 and p = 0.03, 95%CI: 1.34–3.46, respectively), BFCRS > 20 (p = 0.04, 95%CI: 1.36–2.49 and p = 0.03, 95%CIL 1.09–2.97, respectively) although only LP was predictive of elevated NPI-QSS ≥ 10 (p < 0.001, 95%CI: 2.63–4.69). The presence MRI and LP abnormalities in the same individual was associated with catatonia (p = 0.01, 95%CI: 1.87–3.98), BFCRS ≥ 20 (p = 0.02, 95%CI: 1.63–3.65) and NPI-QSS ≥ 10 (p = 0.02, 95%: 1.43–3.07). Symptoms of DSRD were not associated with the presence or absence of any diagnostic test with the exception of movement disorder which was associated with abnormalities on MRI (p = 0.02, 95%CI: 1.21–2.69) and LP (p = 0.04, 95%CI: 1.09–3.79), similar to findings of those with catatonia.
Certain serum and neurodiagnostic studies were predictive of immunotherapy responsiveness in individuals with DSRD (Table 4). With regards to blood-based testing, only cytokine abnormalities were predictive of subsequent immunotherapy responsiveness (p = 0.03, 95%CI: 1.12–6.43, OR: 2.68). C3 levels trended towards significance but did not meet threshold (p = 0.07, 95%CI: 0.93–4.80, OR: 2.11). In general, neurodiagnostic tests were highly predictive of subsequent immunotherapy responsiveness. Abnormalities in neuroimaging (p < 0.001, 95%CI: 3.15–20.17, OR: 7.98) and LP (p = 0.02, 95%CI: 1.18–10.82, OR: 3.58) were the most statistically significant testing abnormalities that predicted immunotherapy responsiveness, while abnormalities on EEG were not predictive (p = 0.25, 95%CI: 0.72–3.43, OR: 1.57). When MRI and LP were both abnormal or when EEG, MRI and LP were all abnormal, the odds of immunotherapy responsiveness approached 100% (p = 0.01, 95%CI: 1.75–105.1, OR: 13.56 and p = 0.02, 95%CI: 1.37–86.87, OR: 10.91, respectively). However, this effect was largely driven by neuroimaging abnormalities in this cohort. Maximum change on the NPI-Q total score and BFCRS for diagnostic biomarkers associated with immunotherapy responsiveness are presented in Table 5. The maximum nadir of both the NPI-Q and BFCRS was statistically different for cytokines, MRI, LP, and when these neurodiagnostics were combined for all but cytokines impact on the BFCRS (p = 0.35, 95%CI: 0.23–1.25). NPI-Q subfields were also analyzed to determine if there was any unique association between diagnostic biomarkers and subfield scores but none were independently statistically significant.

SWI signal abnormality in the basal ganglia of individuals with DSRD. Legend: white arrows correspond to SWI signal abnormalities in the bilateral basal ganglia.
The time between the onset of symptoms of DSRD and capture of neurodiagnostic abnormalities was also assessed (Fig. 2). The timing of study obtainment with reference to symptom onset is provided in Supplement A. The highest rate of abnormality capture was in the first six months from onset of symptoms (64% for serum cytokines, 53% for EEG, and 59% for cerebrospinal fluid). Notably, neuroimaging abnormalities were lowest in the first six months of symptom onset at just 13%. As demonstrated in Fig. 2, the likelihood of abnormality capture for serum cytokines, EEG, and CSF declined dramatically after 24 months from symptom onset, whereas the likelihood of neuroimaging abnormalities increased over time to a peak of 41% in individuals with > 36 months between symptom onset and study obtainment.

Likelihood of lab or neurodiagnostic study capture at various time points after symptom onset.
Discussion
In a large cohort of individuals with DSRD, elevated rates of abnormalities in serum cytokines, neuroimaging, and CSF were identified. In individuals with these diagnostic abnormalities, a more severe disease phenotype and an elevated rate of responsiveness to immunotherapy was observed. These diagnostic biomarkers, when found alone or in combination, can help justify the use of early immune treatments in individuals with DSRD. This data builds on existing work in smaller and more heterogeneous cohorts6 and has the potential to create a basis for biomarkers of disease activity in persons with DSRD.
Inflammation in individuals with DS is well-established and has been linked to the triplication of genes on chromosome 21—particularly several interferon receptor genes14,15,16,17,18. Although not consistently thought of as an inflammatory disease, many of the co-morbid autoimmune and rheumatoid disorders that individuals with DS experience11,19 have recently been linked to overactive interferon responses and T-cell dysregulation14,16,18,20,21,22. This is manifested in clinical observations across a variety of pathologies and organ systems23,24,25,26,27,28,29. Both interferon overactivity and T-cell dysregulation could have an effect in the central nervous system (CNS) and might explain some of the biomarkers observed in this study and patients’ responses to immunotherapy. While further research into the role of immune dysregulation in the CNS in individuals with DSRD is necessary, this data is supported by a large evidence base of systemic immune dysregulation in persons with DS.
One of the most significant findings from this study is that multiple diagnostic biomarkers are predictive of both disease severity and immunotherapy responsiveness in individuals with DSRD. While this has been reported previously, prior studies were in a much smaller and more heterogenous cohort of which not all individuals had comprehensive testing6. When multiple diagnostic biomarkers were abnormal, the rates of greater disease severity at baseline, overall rates of response to immunotherapy and degree of response to immunotherapy on the NPI-Q and BFCRS were increased, which potentially indicates more severe inflammatory disease in this sub-population. Notably, the combination of both neuroimaging and CSF abnormalities yielded a greater than 13-fold increased likelihood of response to immunotherapy. That said, a significant amount of this increased likelihood of response is driven by neuroimaging abnormalities, which may be the more specific study to predict response. As such, these results may provide clinicians with the necessary data to warrant the use of early immunotherapy in individuals with these patterns in diagnostic studies.
Conversely, multiple diagnostic studies were found to have no bearing on disease severity or therapeutic response in individuals with DSRD and included ANA, TPO antibodies, thyroglobulin antibodies, CRP, ESR, ferritin, and EEG. These tests are obtained during the standardized work up of DSRD although may be of limited clinical significance beyond ruling out mimics of the disease. Some labs, such as ANA, TPO, and thyroglobulin antibodies may be elevated indiscriminately in individuals with DS14,23,30,31, and thus are not predictive of pathology in DSRD. Other labs such as CRP, ESR and ferritin are considered acute phase reactants and thus may not be continually elevated in individuals with DSRD across the disease course. Finally, EEG has previously been a weak marker of DSRD pathology, and while a non-invasive biomarker of disease, the high rates of EEG abnormalities in individuals with DSwR make determination of an abnormal study in an individual with DSRD challenging6. In addition, while serum cytokines were dysregulated and were weakly predictive of immunotherapy responsiveness, these were not consistent with any particular interferon-mediated cascade. As such, this pro-inflammatory milieu may point less towards interferon signaling abnormalities as the primary etiology of DSRD. While exciting from an intervention standpoint, the diagnostic patterns reported are neither sensitive nor specific for DSRD, and a singular predictive testing abnormality to diagnose or treat DSRD has not yet been identified.
Finally, a temporal correlation between the presence or absence of diagnostic abnormalities in individuals with DSRD was also observed in this study. In general, serum and CSF changes were more likely to be present early after symptom onset, however, neuroimaging studies were more likely to be abnormal several months later. These findings, particularly for cytokine, EEG and CSF abnormalities, may indicate a transient “active” process in individuals with DSRD early in the disease course. This has been observed in other neuroinflammatory disorders previously, particularly with the presence of biomarkers, antibodies32,33, and EEG findings34,35. Interestingly, neuroimaging was more likely to be abnormal with time, particularly with regards to abnormalities on SWI. This finding is notable in that the presumed etiology of SWI signal abnormality is interferon-driven, akin to individuals with Aicardi Goutières syndrome36,37, another type I interferonopathy. In these cases, increased interferon receptor gene expression may lead to chronic over-activation of interferon pathways, which may increase the likelihood of an “interferon signature” on neuroimaging. Overall, these data highlight the importance of early collection of diagnostic testing that could predict subsequent immunotherapy responsiveness in individuals with DSRD.
Research on DSRD has been rapidly expanding over the last half decade, with considerable resources actively invested in the search for sensitive and specific serum, neurodiagnostic, and CSF biomarkers. An important observation from this data is that the diagnostic signatures reported in DSRD are consistent with an inflammatory process in some individuals. This has been observed in other interferonopathies38,39 and neuroimmunologic conditions40,41. Specifically, serum biomarkers of inflammation such as complement, cytokines, erythrocyte sedimentation rate, and ferritin frequently paired with neuroimaging biomarkers consistent with interferon dysregulation (SWI signal on MRI) and CSF biomarkers of inflammation, all of which were predictive of immunotherapy responsiveness. When multiple diagnostic biomarkers were abnormal, the rates of response to immunotherapy rose further, potentially indicating more severe inflammatory disease in this sub-population. While this study demonstrates inflammatory patterns across multiple diagnostic modalities, a singular predictive testing abnormality to diagnose and treat DSRD has not been identified.
DSRD remains a complex condition and this study is not without limitations. Firstly, this study was retrospective. Selection and severity bias is present in the exclusion of patients who did not undergo neurodiagnostic work up for their clinical symptoms. This is further compounded by the fact that clinical investigations were performed at tertiary academic medical centers which also increases the potential for severity bias. Investigators involved in this study were early adopters of immunotherapy in persons with DSRD, and thus both a referral and selection bias in favor of use of immunotherapeutic use may be present. Similarly, as the primary centers involved in this study do not offer electroconvulsive therapy (ECT), there were no patients in this cohort who had received this therapy during the study period. Given that prior studies by this study group have showed a high rate of response to this therapeutic intervention6, future studies will need to include centers where these patients are followed and treated. Severity bias could also decrease the likelihood of response to any therapy. Although this study demonstrates that neuroimaging is predictive of response to immunotherapy and is advised early in the clinical presentation, it is important to note that these studies are more likely to be abnormal as time with symptoms increases which is different than other neurodiagnostic studies. Further, defining a response to immunotherapy as improvement of greater than 50% on the BFCRS and NPI-Q skews clinical improvements to catatonia (movement abnormalities) and neuropsychiatric symptoms as opposed to cognitive and functional improvements. As such some patients may have improved outside of these domains and may have not been captured using these objective metrics. In addition, testing for immune biomarkers in individuals in the DSwR cohort was clinical and may have increased the likelihood of detection in this group as clinical studies would have been ordered for diagnostic evaluation (presumably inflammatory or autoimmune disease). Similarly, EEG and LP results in individuals with DSwR were excluded from analysis due to high pre-test probability of abnormality. In sampling 100 EEGs of individuals with DS referred for any reason, 76% were abnormal. The most common reasons for referral were observed seizure(s) (n = 70, 70%) and seizure-like event (n = 23, 23%). In sampling 50 lumbar punctures of individuals with DS, 77% of studies were abnormal with the most common indications being concern for meningitis (n = 39, 78%) and refractor status epilepticus (n = 6, 12%). The important need for true DSwR EEG and LP data is not unrealized by the study team and this research is underway at this time. An important finding in this data is that nearly all individuals treated with immunotherapy received IVIg which has very broad mechanisms of action ranging from B-cell to T-cell mediated function42. This is critically important to consider as the less specific mechanisms of action may allow for both greater rates of immunotherapy responsiveness and may alter sensitivity and specificity of the diagnostics assessed in this study. Uniform therapeutic algorithms do not exist for DSRD at this time although the development of standardized approaches to the management of DSRD may also improve the ability to prospectively determine long-term responses to the treatments detailed in this study. As this study relied on physician discretion for selection of therapies, this could have impacted the study findings, as noted above. Finally, the authors note that given the rare nature of DSRD, small study populations limit the generalizability of these findings, and clinicians must evaluate each case individually.
Conclusions
In a sizable population of individuals diagnosed with DSRD and undergoing extensive laboratory and neurodiagnostic evaluations, a notable prevalence of abnormalities was observed. Marked deviations in serum cytokine levels, neuroimaging findings, and CSF analysis emerged as indicators predictive of disease severity and responsiveness to immunotherapy. These findings may serve as valuable biomarkers guiding the selection of subsequent therapeutic interventions for this complex condition. Notably, the heightened likelihood of detecting abnormalities within the initial six months following symptom onset underscores the critical importance of prompt recognition and thorough investigation in managing DSRD effectively. Early identification not only facilitates timely intervention but also offers invaluable insights for comprehensive study and understanding of this debilitating disorder. A larger, prospective, study is warranted in this unique population.
Methods
IRB and data availability
This study was approved by the Children’s Hospital Los Angeles Human Subjects Protection Program and Institutional Review Board (IRB). Given the retrospective nature, assent and consent were waived by the Children’s Hospital Los Angeles IRB. All methods were performed in accordance with the relevant guidelines and regulations. The datasets used and analyzed during the current study available from the corresponding author on reasonable request from qualified investigators with IRB approval.
Participants and study design
All individuals evaluated in the DS neurology clinic at Children’s Hospital Los Angeles between July 1st, 2019, and December 31st, 2023, were eligible for this study. Inclusion criteria for the DSRD cohort included age between 10 and 30 years at the time of symptom onset, diagnosis of either possible or probable DSRD per expert consensus guidelines43, and completion of clinical neurodiagnostic studies (electroencephalogram (EEG), magnetic resonance imaging (MRI) of the brain, and lumbar puncture (LP)). Confirmation of diagnosis was performed by an arbiter with clinical experience in evaluating individuals with DSRD and with no knowledge of the case (MK). Exclusion criteria which included, age < 10 or > 30 years at the time of symptom onset, active cardiac or pulmonary disease, frequent infections (defined as more than two infections requiring antibiotics or antivirals per year), a history of neoplasia or receipt of chemotherapy, structural brain malformation on neuroimaging, active or a history of epilepsy (excluding febrile seizure), current use of electroconvulsive therapy and use of any immunotherapy not related to DSRD. Individuals with DSRD were excluded if they had been on any steroid or other immunotherapy within three months of baseline assessment. Individuals with co-morbid diagnosis of ASD were not excluded although they were all required to meet consensus criteria for DSRD, were diagnosed at an age less than eight years and were diagnosed at minimum three years prior to the symptom onset of DSRD, to avoid clinical overlap. All individuals with DSRD had to have serum blood work, EEG, MRI and LP performed.
A cohort of individuals with DS without regression (DSwR) were also reviewed for comparison. Inclusion criteria for the DSwR included age between 10 and 30 years at the time of lab or neurodiagnostic investigations. Individuals in the comparator cohort could not meet possible or probable criteria for DSRD nor could they have any diagnosed neoplastic, immunologic or rheumatologic condition. The study only included individuals in the DSwR cohort with labs obtained before January 1st, 2022, to avoid the possibility of including an individual who could subsequently go on to develop DSRD. Individuals could have had lab obtainment for any purpose.
Demographic data, medical history, and results of clinical and diagnostic investigations were collected through clinical documentation. A board certified neuroradiologist independently reviewed radiographic data. Individuals in the DSwR group had blood work and MRI for clinical purposes which was used for comparison. As individuals undergoing EEG or LP would be biased towards having diagnostic abnormalities (e.g., EEG being performed for a seizure disorder), these studies were not included for comparison.
Definitions of Abnormal Neurodiagnostics:
-
1.
EEG: Focal or generalized slowing, focal epileptiform discharges out of any cortex, or seizure were considered abnormal. Generalized discharges were considered abnormal although inconsistent with the diagnosis of DSRD. All patients had to have at least one prior EEG prior to the onset of DSRD symptoms that did not demonstrate these results.
-
2.
MRI: All MRIs required to be performed on a 3 Tesla (T) scanner with and without contrast administration. Any abnormality beyond a structural malformation (e.g., Chiari malformation) was considered abnormal. Patients did not require a prior “normal” MRI.
-
3.
LP: Abnormalities were defined as having any of the following: white blood cell (WBC) count > 5 cells/mm3, total protein > 60 mg/dL, presence of oligoclonal bands, an immunoglobulin G (IgG) index of > 0.66, and/or an elevated neopterin (> 33 nmol/mL). Samples with over 1,000 red blood cells (RBC) were excluded from analysis. Patients did not require a prior “normal” LP.
Evaluations, clinical definitions and definition of therapeutic response
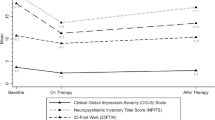
Individuals with DSRD received clinical evaluation and bloodwork at their initial visit. At this visit and all subsequent visits (every three months), individuals had a comprehensive 7-point neurologic examination, Bush-Francis Catatonia Rating Scale (BFCRS) and Neuropsychiatric Inventory Questionnaire (NPI-Q) performed. The BFCRS and NPI-Q were clinician administered. Neuroimaging and LP had to be performed within three months of the initial clinical evaluation and blood work for use.
Catatonia was defined as having at defined per the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) and required a minimum BFCRS score of three44. Severe disease was defined as having a BFCRS ≥ 20 and/or a NPI-Q severity score (NPI-QSS) ≥ 10.
All individuals in this study were treated at the discretion of the site physician. There were no uniform inclusion or exclusion criteria for individuals to receive immunotherapy although all individuals required a confirmed diagnosis of either possible or probable DSRD. Immunotherapy used to manage individuals with DSRD in this study included steroids, intravenous immunoglobulin (IVIg), mycophenolate mofetil, rituximab, or tofacitinib. A therapeutic response was defined as a > 50% improvement on either the BFCRS or NPI-Q on a subsequent evaluation compared to baseline. A therapeutic response to a particular regimen could only be made when no other therapy was used during the three-month period of evaluation.
Statistical analysis
Demographics, disease biometrics, and baseline clinical features were compared between patients with and without neurologic relapse using chi-square (χ2) or Fisher’s exact tests for categorical variables, and t-test for continuous variables. The delta BFCRS and NPI-Q total scores were generated by subtracting the lowest BFCRS and NPI-Q total score during the study period from the baseline score for each individual. To account for the influence of independent variables (demographics, disease biometrics, and baseline clinical features) on laboratory and neurodiagnostic biomarker positivity, a univariate logistic regression was used to model the association variables. Factors which differed significantly were entered into a separate multivariable logistic regression model. All analyses conducted used Stata/MP version-17.0 (StataCorp. 2021. College Station, TX: StataCorp LLC.).
Data availability
The datasets used and analyzed during the current study available from the corresponding author on reasonable request from qualified investigators with IRB approval.
References
de Graaf, G., Buckley, F. & Skotko, B. G. Estimates of the live births, natural losses, and elective terminations with Down syndrome in the United States. Am. J. Med. Genet. A. 167a, 756–767. https://doi.org/10.1002/ajmg.a.37001 (2015).
Mircher, C. et al. Acute regression in young people with Down syndrome. Brain Sci. 7 https://doi.org/10.3390/brainsci7060057 (2017).
Rosso, M. et al. Down syndrome disintegrative disorder: A clinical regression syndrome of increasing importance. Pediatrics 145 https://doi.org/10.1542/peds.2019-2939 (2020).
Worley, G. et al. Down syndrome disintegrative disorder: New-onset autistic regression, dementia, and insomnia in older children and adolescents with Down syndrome. J. Child. Neurol. 30, 1147–1152. https://doi.org/10.1177/0883073814554654 (2015).
Ghaziuddin, N., Nassiri, A. & Miles, J. H. Catatonia in Down syndrome; A treatable cause of regression. Neuropsychiatr. Dis. Treat. 11, 941–949. https://doi.org/10.2147/ndt.S77307 (2015).
Santoro, J. D. et al. Evidence of neuroinflammation and immunotherapy responsiveness in individuals with Down syndrome regression disorder. J. Neurodev Disord. 14 https://doi.org/10.1186/s11689-022-09446-w (2022).
Santoro, S. L. et al. Unexplained regression in Down syndrome: Management of 51 patients in an international patient database. Am. J. Med. Genet. A. https://doi.org/10.1002/ajmg.a.62922 (2022).
Santoro, S. L. et al. Unexplained regression in Down syndrome: 35 cases from an international Down syndrome database. Genet. Med. 22, 767–776. https://doi.org/10.1038/s41436-019-0706-8 (2020).
Santoro, J. D. et al. Alternative diagnoses in the work up of Down syndrome regression disorder. J. Autism Dev. Disord. https://doi.org/10.1007/s10803-023-06057-9 (2023).
Rivelli, A. et al. Prevalence of mental health conditions among 6078 individuals with Down syndrome in the United States. J. Patient Cent. Res. Rev. 9, 58–63. https://doi.org/10.17294/2330-0698.1875 (2022).
Chicoine, B. et al. Prevalence of common disease conditions in a large cohort of individuals with Down syndrome in the United States. J. Patient Cent. Res. Rev. 8, 86–97. https://doi.org/10.17294/2330-0698.1824 (2021).
Santoro, J. D. et al. Immunotherapy responsiveness and risk of relapse in Down syndrome regression disorder. Transl. Psychiatry. 13, 276. https://doi.org/10.1038/s41398-023-02579-z (2023).
Cardinale, K. M. et al. Immunotherapy in selected patients with Down syndrome disintegrative disorder. Dev. Med. Child. Neurol. 61, 847–851. https://doi.org/10.1111/dmcn.14127 (2019).
Malle, L. et al. Autoimmunity in Down’s syndrome via cytokines, CD4 T cells and CD11c(+) B cells. Nature 615, 305–314. https://doi.org/10.1038/s41586-023-05736-y (2023).
Waugh, K. A. et al. Mass cytometry reveals global immune remodeling with multi-lineage hypersensitivity to type I interferon in Down syndrome. Cell. Rep. 29, 1893–1908e1894. https://doi.org/10.1016/j.celrep.2019.10.038 (2019).
Araya, P. et al. Trisomy 21 dysregulates T cell lineages toward an autoimmunity-prone state associated with interferon hyperactivity. Proc. Natl. Acad. Sci. U S A. 116, 24231–24241. https://doi.org/10.1073/pnas.1908129116 (2019).
Pham, A. T. et al. JAK inhibition for treatment of psoriatic arthritis in Down syndrome. Rheumatology (Oxford) 60, e309–e311. https://doi.org/10.1093/rheumatology/keab203 (2021).
Sullivan, K. D. et al. Trisomy 21 causes changes in the circulating proteome indicative of chronic autoinflammation. Sci. Rep. 7, 14818. https://doi.org/10.1038/s41598-017-13858-3 (2017).
Valentini, D. et al. Medical conditions of children and young people with Down syndrome. J. Intellect. Disabil. Res. 65, 199–209. https://doi.org/10.1111/jir.12804 (2021).
Sullivan, K. D. et al. Trisomy 21 consistently activates the interferon response. Elife 5 https://doi.org/10.7554/eLife.16220 (2016).
de Jesus, A. A. et al. Distinct interferon signatures and cytokine patterns define additional systemic autoinflammatory diseases. J. Clin. Invest. 130, 1669–1682. https://doi.org/10.1172/jci129301 (2020).
Peeters, D. et al. AKT hyperphosphorylation and T cell exhaustion in Down syndrome. Front. Immunol. 13, 724436. https://doi.org/10.3389/fimmu.2022.724436 (2022).
Santoro, J. D. et al. Increased autoimmunity in individuals with Down syndrome and Moyamoya disease. Front. Neurol. 12, 724969. https://doi.org/10.3389/fneur.2021.724969 (2021).
Lai, F., Mercaldo, N., Wang, C. M., Hersch, G. G. & Rosas, H. D. Association between inflammatory conditions and Alzheimer’s disease age of onset in Down syndrome. J. Clin. Med. 10 https://doi.org/10.3390/jcm10143116 (2021).
Pepe, G. et al. Prospective evaluation of autoimmune and non-autoimmune subclinical hypothyroidism in Down syndrome children. Eur. J. Endocrinol. 182, 385–392. https://doi.org/10.1530/eje-19-0823 (2020).
Ludvigsson, J. F., Lebwohl, B., Green, P. H., Chung, W. K. & Mårild, K. Celiac disease and Down syndrome mortality: A nationwide cohort study. BMC Pediatr. 17 https://doi.org/10.1186/s12887-017-0801-4 (2017).
Ostermaier, K. K. et al. Incidence of celiac disease in Down syndrome: A longitudinal, population-based birth cohort study. Clin. Pediatr. (Phila). 59, 1086–1091. https://doi.org/10.1177/0009922820941247 (2020).
Anwar, A. J., Walker, J. D. & Frier, B. M. Type 1 diabetes mellitus and Down’s syndrome: Prevalence, management and diabetic complications. Diabet. Med. 15, 160–163. https://doi.org/10.1002/(sici)1096-9136(199802)15:2<160::Aid-dia537>3.0.Co;2-j (1998).
Pessoa, D. M. F. et al. Characteristics of type 1 diabetes mellitus in children and adolescents with Down’s syndrome in an admixed population. Arch. Endocrinol. Metab. 65, 562–569. https://doi.org/10.20945/2359-3997000000365 (2021).
Chen, M. H., Chen, S. J., Su, L. Y. & Yang, W. Thyroid dysfunction in patients with Down syndrome. Acta Paediatr. Taiwan. 48, 191–195 (2007).
da Utiyama, R. Autoantibodies in patients with Down syndrome: Early senescence of the immune system or precocious markers for immunological diseases? J. Paediatr. Child. Health. 44, 182–186. https://doi.org/10.1111/j.1440-1754.2007.01229.x (2008).
Gastaldi, M. et al. Prognostic relevance of quantitative and longitudinal MOG antibody testing in patients with MOGAD: A multicentre retrospective study. J. Neurol. Neurosurg. Psychiatry. 94, 201–210. https://doi.org/10.1136/jnnp-2022-330237 (2023).
Macher, S. et al. Longitudinal measurement of cerebrospinal fluid neurofilament light in anti-N-methyl-D-aspartate receptor encephalitis. Eur. J. Neurol. 28, 1401–1405. https://doi.org/10.1111/ene.14631 (2021).
Shi, Y. Serial EEG monitoring in a patient with anti-NMDA receptor encephalitis. Clin. EEG Neurosci. 48, 301–303. https://doi.org/10.1177/1550059416677398 (2017).
Jeannin-Mayer, S. et al. EEG analysis in anti-NMDA receptor encephalitis: Description of typical patterns. Clin. Neurophysiol. 130, 289–296. https://doi.org/10.1016/j.clinph.2018.10.017 (2019).
Al Mutairi, F. et al. Phenotypic and molecular spectrum of Aicardi-Goutières syndrome: A study of 24 patients. Pediatr. Neurol. 78, 35–40. https://doi.org/10.1016/j.pediatrneurol.2017.09.002 (2018).
Rice, G. I. et al. Genetic, phenotypic, and interferon biomarker status in ADAR1-related neurological disease. Neuropediatrics 48, 166–184. https://doi.org/10.1055/s-0037-1601449 (2017).
Cuadrado, E. et al. Aicardi-Goutières syndrome harbours abundant systemic and brain-reactive autoantibodies. Ann. Rheum. Dis. 74, 1931–1939. https://doi.org/10.1136/annrheumdis-2014-205396 (2015).
Takanohashi, A. et al. Elevation of proinflammatory cytokines in patients with Aicardi-Goutières syndrome. Neurology 80, 997–1002. https://doi.org/10.1212/WNL.0b013e3182872694 (2013).
Culler, G., Bachman, E. & VanHaerents, S. Paraclinical serum markers as aids in the diagnosis of autoimmune encephalitis. J. Neuroimmunol. 347, 577324. https://doi.org/10.1016/j.jneuroim.2020.577324 (2020).
Hacohen, Y. et al. Paediatric autoimmune encephalopathies: clinical features, laboratory investigations and outcomes in patients with or without antibodies to known central nervous system autoantigens. J. Neurol. Neurosurg. Psychiatry. 84, 748–755. https://doi.org/10.1136/jnnp-2012-303807 (2013).
Lünemann, J. D., Nimmerjahn, F. & Dalakas, M. C. Intravenous immunoglobulin in neurology–mode of action and clinical efficacy. Nat. Rev. Neurol. 11, 80–89. https://doi.org/10.1038/nrneurol.2014.253 (2015).
Santoro, J. D. et al. Assessment and diagnosis of Down syndrome regression disorder: International Expert Consensus. Front. Neurol. 13, 940175. https://doi.org/10.3389/fneur.2022.940175 (2022).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th Ed. (2013).
Acknowledgements
This study was funded by the National Heart Lung and Blood Institute (NHLBI) and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), to whom the authors owe gratitude. The authors wish to thank the individuals and families of individuals who participated in this research.
Author information
Authors and Affiliations
Contributions
J.D.S. conceptualized the study, performed data analysis, edited tables and figures, wrote the manuscript and edited the manuscript for intellectual content.S.J., L.K., M.M.K, L.K., N.K.B, B.N.V, and L.N. performed data entry, collected study data, performed data analysis, table generation, figure generation, wrote the manuscript and edited the manuscript for intellectual content.M.M., D.N., N.A.S., A.D.B., and E.A.Q. reviewed the statistical analysis, results, and interpretations, and edited the manuscript for intellectual content.M.S.R. conceptualized the study and edited the manuscript for intellectual content.All authors reviewed the manuscript and have agreed to submit in its current form.
Corresponding author
Ethics declarations
Competing interests
Dr. Santoro receives research support from the National Institutes of Health and consulting fees from UCB, TG pharmaceuticals and Cycle Pharmaceuticals. Dr. Rafii has received grants or contracts from Eisai (AHEAD Study) and Eli Lilly (A4 Study), which were paid to his institution. He has received consulting fees from AC Immune, Corium and Ionis. He has participated on a Data Safety Monitoring Board or Advisory Board for Alzheon, Aptah Bio, Biohaven, Embic, Keystone Bio and Positrigo. All other authors reported no biomedical financial interests or potential conflicts of interest.
Legend
Cerebrospinal fluid (CSF), electroencephalogram (EEG), magnetic resonance imaging (MRI).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Santoro, J.D., Jafarpour, S., Keehan, L. et al. Diagnostic abnormalities, disease severity and immunotherapy responsiveness in individuals with Down syndrome regression disorder. Sci Rep 14, 30865 (2024). https://doi.org/10.1038/s41598-024-81819-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-81819-8
Keywords
This article is cited by
-
Serum and cerebral folate are normal in down syndrome regression disorder
Molecular Autism (2026)
