
Abstract
Rotational atherectomy (RA) is an effective, mature, and specific treatment for calcified lesions. However, the incidence of RA-related myocardial injury remains high and has not been adequately addressed. To assess the safety and efficacy of low-temperature RA-flush solution versus room-temperature RA-flush solution during RA. A total of 132 patients with moderate-to-severe calcified lesions who underwent RA were randomly assigned to the low-temperature RA-flush solution group or the room-temperature RA-flush solution group. The primary endpoint was RA-related myocardial injury, defined as any increase in myocardial biomarkers within 72 h after percutaneous coronary intervention (PCI). Secondary endpoints included RA-related myocardial infarction (MI), RA-related transient slow/no flow, or transient coronary spasm. A total of 78 patients (59.1%) had increased cardiac troponin I (cTnI) levels, and 60 patients (45.5%) had increased creatine kinase isoenzyme (CK-MB) levels after PCI. The number of patients with myocardial injury (primary endpoint), defined as elevated cTnI (47.0% vs. 71.2%, p = 0.005) or elevated CK-MB (28.8% vs. 62.1%, p < 0.001), was significantly lower in the low temperature group than in the room temperature group. The number of patients with RA-related transient slow/no flow (6.1% vs. 34.8%, p < 0.001) and transient coronary spasm (9.1% vs. 25.8%, p = 0.012) (secondary endpoints) was significantly lower in the low temperature group than in the room temperature group; no significant difference in the incidence of RA-related MI was observed between the two groups. Compared with room-temperature RA-flush solution, low-temperature RA-flush solution is associated with reduced RA-related myocardial injury in patients treated with RA.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT03701230; first submitted registration date: 09/10/2018.
Similar content being viewed by others

Introduction
With the further development of various tools, technological advances and updated treatment models, the efficacy and safety of percutaneous coronary intervention (PCI) for the treatment of complex obstructive coronary artery diseases have greatly improved;1,2 however, severe calcified lesions remain problems that cannot be completed resolved by PCI3,4,5.
Rotational atherectomy (RA) is a mature technology that has been used to treat moderate-to-severe coronary calcified lesions for a very long time6,7,8 and has been widely used in the field of PCI for more than 30 years;9 however, because RA involves differential cutting and orthogonal displacement of the friction of high-speed burrs on inelastic tissue spaces (such as calcified lesions),10,11 the RA-related complications of slow/no flow, which are caused mainly by the debris generated by RA11,12 and local thermal tissue damage (LTTD),11,13,14,15 and even secondary complications that are related to the operation, such as thrombosis induced by platelet activation, cannot be avoided11,15.
Although continuous flushing with room-temperature RA-flush solution washes debris to the distal end of coronary circulation and partially cools the RA burr and reduces the local tissue temperature, myocardial injury cannot be completely avoided7,10,11 Previous studies reported that the decrease in the speed of the RA burrs that occurs during the procedure indicates that the thermal energy that is generated by the conversion of kinetic energy to potential energy cannot be completely eliminated by the RA-flush solution, and this results in LTTD9,12,13. Therefore, we designed a randomized controlled study to compare the myocardial protective effects of low-temperature RA-flush solution and room-temperature RA-flush solution during the RA procedure to treat moderate-to-severe calcified lesions.
Methods
Study design and oversight
The LOTA II was an investigator-initiated, prospective, multicenter and randomized controlled study of patients with moderate-to-severe calcified lesions who were treated with RA; this study was conducted in 8 heart centers in China after the protocol was approved by the ethics committee at each participating site, and all patients provided written consent before receiving the assigned treatments. This trial was registered at clinicaltrials.gov (NCT03701230). A data and safety monitoring board oversaw the study, and an independent clinical-event adjudication committee, whose members were blinded to the study group assignments, evaluated all the clinical events. The executive committee and the authors guarantee the accuracy and complete reliability of the data and study protocols. The first and last authors have unrestricted access to the data, participated in the analysis and interpretation of the data, and wrote the first and subsequent drafts of the manuscript, and all the authors decided to submit the manuscript for publication. The study was funded mainly by the JiangSu Provincial (China) Health Commission Medical Research Project [ZDB2020029], which had no role in site selection, study design, or data collection, analysis or interpretation. All the study protocols were conducted in accordance with the provisions of the Declaration of Helsinki and the International Conference on Harmonization Good Clinical Practices.
Patient selection
Consecutive patients who presented with de novo coronary artery lesions with moderate-to-severe calcification and for whom treatment with PCI combined with RA was planned at participating centers were evaluated for enrollment in the current study. Patients were included if they were > 18 years old; presented with silent ischemia, clinically stable or unstable angina, or moderate-to-severe calcified lesions detected by angiography, intravascular ultrasound or optical coherence tomography for which RA pretreatment was required before new-generation drug-eluting stent (DES) implantation; and only a single vessel lesion needed to be treated. Patients were excluded if they were diagnosed with acute myocardial infarction (MI), elevated levels of myocardial biomarkers (including creatine kinase isoenzyme (CK-MB) and cardiac troponin I (cTnI)) at baseline, clinical hemodynamic instability with cardiac shock, multiple organ failure, allergy to contrast agents, inability to tolerate dual antiplatelet therapy or anticoagulation therapy, recent infection, hepatorenal dysfunction, thrombosis in the coronary artery, spontaneous coronary dissection, or complex coronary bifurcation requiring a two-stent strategy, if they had received drug-coated balloon treatment, bioabsorbable vascular scaffold implantation, previous PCI or coronary artery bypass graft treatment, or if they were in an active stage of autoimmune disease.
Randomization
Randomization was performed by a central interactive web-based computerized system, and concealed operations were stratified based on the enrollment site, with a block size of 6 for the two groups (Fig. 1). Eligible patients were randomly assigned in a 1:1 ratio to receive either a low-temperature RA-flush solution or a room-temperature RA-flush solution during the RA procedure to treat moderate-to-severe coronary calcified lesions. Neither the operators nor the patients were blinded to the specific grouping information or treatment procedures. RA-flush solution during RA procedure was carried out randomly by the nurse who was working in cath room according to the center randomization. The outcome assessors and statisticians were also blinded to the study group assignments.
Laboratory examination and angiographic data analysis
The levels of myocardial biomarkers (including CK-MB and cTnI) in patients were measured before PCI and 8, 16, 24, 48 and 72 h after PCI. Other biomarkers, such as lipid profile and renal function, were routinely measured before PCI. Quantitative coronary analysis (QCA; Angio Plus, Pulse Medical Imaging Technology) was used offline to measure angiographic data (such as lesion length, reference vessel diameter and diameter stenosis) pre-PCI by two independent technicians who were familiar with the operating system and were blinded to patient characteristics or clinical results.
Interventional procedure
All patients received dual antiplatelet therapy (aspirin 100 mg qd plus clopidogrel 75 mg qd or ticagrelor 90 mg bid) before the PCI procedure, and a loading dose of 300 mg clopidogrel or 180 mg ticagrelor was prescribed to patients within 12 h prior to the procedure if they had not received such treatment for more than 5 days. PCI was performed according to conventional and local standards. After the decision to perform upfront RA for calcified lesions based on angiographic findings or intravascular imaging findings (intravascular imaging technique was not mandatory), an activated clotting time ≥ 300 s should be maintained after intra-arterial or intravenous heparin injection. Other anticoagulation agents (e.g., bivalirudin) and other antiplatelet therapies (e.g., glycoprotein IIb/IIIa antagonists) were not routinely recommended in this study, and those decisions were left to the discretion of the treating physician.
RA was performed with a Rotablator (Boston Scientific Corporation, 47215 Lakeview Boulevard Fremont, CA 94538, USA) according to previous experts’ consensus recommendations. The final burr size was selected in order to reach a burr/vessel ratio of 0.5 (a maximum of 0.7 if needed). The rotational speed ranged from 140,000 to 180,000 rotations/minute. The burr was placed immediately proximal to the target lesion to avoid damaging the healthy vessel wall. Gradual burr advancement using a pecking motion manipulation method with short ablation runs of 15 to 20 s per time was recommended11 Next, the RA operation was performed at intervals of more than 30 s if necessary.
Preparation of RA-flush solution before the RA procedure: According to previous consensus recommendations, an RA-flush solution cocktail with equal proportions of verapamil, nitroglycerin, and heparin (5 mg/5 mg/5000 U in 500 ml of saline) was used for all the RA procedures that were conducted in the study7,8,16 The saline was placed in the refrigerator at 0 ~ 5 ℃ or at room temperature for reserve use. Once a patient was confirmed to be enrolled in the study, the saline that was stored in the refrigerator was used to prepare the RA-flush solution for use in the low-temperature group, and the saline that was stored at room temperature was used to prepare the RA-flush solution that was used in the room temperature group. The temperature of all the RA-flush solutions was measured before and after RA in both groups.
Lesion preparation post-RA and stenting: In the absence of complications during the RA procedure, lesion preparation with noncompliant balloon predilatation was routinely performed after RA and before stenting, and any modified balloon, such as a cutting balloon or scoring balloon, was recommended for lesion preparation but notrequired17,18,19 Finally, new-generation DES implantation was performed to cover the whole lesion, followed by 1:1 noncompliant balloon postdilatation.
Follow-up
Clinical follow-up was routinely performed at 1, 3, 6 and 12 months through office visits or telephone interviews. All the procedural and clinical data were recorded in electronic case report forms, verified by independent on-site monitoring, and transmitted to a central database at Nanjing Medical University.
Study endpoints
The primary endpoint was the incidence of RA-related myocardial injury within 72 h after PCI with RA; RA-related myocardial injury was assessed based on the fourth universal definition of myocardial infarction (4th UDMI),20 according to which this condition is defined by an increase in cTnI values (> 99th percentile upper reference limit (URL)) in patients with normal baseline values (≤ 99th percentile URL). The secondary endpoints included the incidence of RA-related MI within 3 days after PCI with RA (based on the 4th UDMI, according to which this condition this defined by an increase in cTnI values more than five times the 99th percentile URL in patients with normal baseline values in conjunction with one of the following elements was needed: new changes on ischemic electrocardiograph; development of new pathological Q waves; imaging evidence of new decrease in viable myocardium or new regional wall motion abnormality in a pattern that was consistent with an ischemic etiology; angiographic findings consistent with a procedural flow-limiting complication such as coronary dissection, occlusion of a major epicardial artery or a side branch occlusion/thrombus, disruption of collateral flow, or distal embolization; or SCAI definition of type 4a MI,21 which was defined as a peak CK-MB level within 72 h of the PCI procedure that reached ≥ 10× the local laboratory URL or to ≥ 5× the URL with new pathologic Q-waves in ≥ 2 contiguous leads or new persistent LBBB, or in the absence of CK-MB data and a normal baseline cTnI level, a cTnI level within 72 h of the PCI that reached ≥ 70× the local laboratory URL or ≥ 35× URL with new pathologic Q-waves in ≥ 2 contiguous leads or new persistent LBBB, respectively), the incidence of RA-related transient slow/no flow, the incidence of RA-related transient spasm of target coronary artery, and target-vessel failure (TVF), which was defined as a composite of death due to cardiac causes, spontaneous target-vessel-related MI (TVMI), or clinically driven target-vessel revascularization (TVR) at the 1-year follow-up.
Statistical analysis
We estimated that a sample size of 132 patients in total would provide the study with at least 90% power at a two-sided significance level of 5% in order to reject the null hypothesis. The null hypothesis was that the incidence of RA-related myocardial injury would be higher in the room temperature group (expected value was 68.0%)22 based on a previous study than in the low temperature group (expected value was 34.0%), with an estimated loss of 10% in each arm during follow-up.
The baseline data are expressed as counts and percentages or means ± standard deviations. The χ2 test or Fisher’s exact test was performed to compare categorical variables. Student’s t test or the Wilcoxon rank sum test for nonnormally distributed data were performed to compare continuous variables. Primary and secondary endpoints were analyzed by Cox regression with the hazard ratio (HR) and 95% confidence interval (CI). Potential interactions between the following subgroups and randomized treatment were examined for the primary endpoint: age, sex, diabetes mellitus status, chronic kidney disease status, left ventricular EF, target lesion location, and final burr-to-vessel ratio. Time-to-first event curves were analyzed by the Kaplan–Meier approach and compared using the log-rank test. All the statistical tests were two-sided, and a P value < 0.05 was considered to indicate statistical significance. All the analyses were performed using R software for Windows version 4.1.2 (https://www.r-project.org/).
Results
Baseline clinical characteristics
From Oct 2018 to Oct 2023, a total of 132 patients with moderate-to-severe coronary calcified lesions underwent RA treatment before DES implantation, and these patients were randomly divided into groups to receive low-temperature RA-flush solution (n = 66) or room-temperature RA-flush solution (n = 66) during the RA procedure (Fig. 1). Baseline clinical data (including demographics, physical measurements, clinical risk factors, medical history, presentation at admission, and medication before PCI) were well matched between the two groups (Table 1).

Study flowchart.
Target lesion characteristics and interventional properties
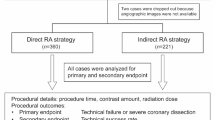
Most of the target lesions (approximately 84.1%) were located in the left anterior descending artery, and approximately 87.9% of the lesions were long (lesion length ≥ 30 mm), with an average diameter stenosis of approximately 78.5% and an average reference vessel diameter of approximately 3.24 mm. None of the target lesion characteristics (including lesion length, reference diameter or diameter stenosis) differed between the two groups (Table 2). Most patients (approximately 80%) were treated with a planned RA strategy, with a similar final burr size of approximately 1.66 ± 0.18 mm, but the final burr-to-vessel size ratio, as determined by QCA, was approximately 0.5, with no significant difference between the two groups (0.51 ± 0.05 vs. 0.51 ± 0.05, p = 0.977). Even though the initial RA burr speed was significantly in the lower temperature group than in the room temperature group (161181.82 + 1983.85 rpm vs. 160196.97 + 1026.12 rpm, p < 0.001), other RA procedure data (such as the maximal RA burr speed deceleration, the ratio of the RA burr speed deceleration that exceeded 5000 rpm, and the total RA time) were similar between the two groups. Only the initial temperature (2.08 ± 1.02 °C vs. 22.63 ± 1.29 °C, p < 0.001) of the RA-flush solution at the beginning of the RA procedure and the final temperature (6.06 ± 1.91 °C vs. 22.86 ± 1.32 °C, p < 0.001) of the RA-flush solution at the end of the RA procedure were significantly lower in the low-temperature group than in the room temperature group. There were no significant differences between the two groups in terms of lesion preparation after RA (such as the use of common balloons, noncompliant balloons, modified balloons, maximal predilatation balloon size, and maximal predilatation pressure), stent characteristics (such as the number of stents per lesion, total stent length per lesion, and average stent diameter), or postdilatation features (such as the maximal postdilatation balloon size and maximal postdilatation pressure). Additionally, no cases of RA-related coronary perforation were observed in the two groups.
Primary endpoint and secondary endpoints
All patients were monitored for myocardial biomarkers every 12 h after PCI for 72 h and peaks value were recorded for further analysis. According to the 4th UDMI definition, 78 patients (59.1%) had increased cTnI levels, and 60 patients (45.5%) had increased CK-MB levels. The incidence of myocardial injury (primary endpoint), which was defined as elevated cTnI levels (47.0% vs. 71.2%, p = 0.005) or elevated CK-MB levels (28.8% vs. 62.1%, p < 0.001), was significantly lower in the low temperature group than in the room temperature group (Fig. 2; Table 3). Regardless of the criteria for RA related myocardial injury (increased cTNI in Fig. 3a or CK-MB in Fig. 3b), subgroups analysis (such as gender, age, hypertension, diabetes, clinical presentation, lesion location, and final burr size) all showed an advantage (or trend toward advantage) in low temperature group in reducing myocardial injury. The incidence of total RA-related MI (secondary endpoint) was only 0.8% according to the SCAI criteria of elevated CK-MB levels post-PCI or 3.0% according to the 4th UDMI criteria of elevated cTnI levels post-PCI. Interestingly, the incidence of RA-related transient slow/no flow (6.1% vs. 34.8%, p < 0.001) and transient coronary spasm (9.1% vs. 25.8%, p = 0.012) was significantly lower in the low temperature group than in the room temperature group. The incidence of the clinical outcome of TVF at the 1-year follow-up was 6.8%, and the differences in total TVF (p = 0.167) and each component of cardiac death (p = 1.000), TVMI (p = 1.000) and clinically driven TVR (p = 0.167) between the two groups were not significant (Fig. 4; Table 3).

Primary and secondary endpoints. (A) The incidence of myocardial injury (primary endpoint) was significantly lower in the low-temperature RA-flush solution group than in the room-temperature RA-flush solution group. (B) The incidence of RA-related MI (secondary endpoint) based on the SCAI criteria or the 4th UDMI criteria was not significantly different between the two groups. CK-MB creatine kinase isoenzyme, cTnI cardiac troponin I, MI myocardial infarction, RA rotational atherectomy, SCAI Society for Cardiovascular Angiography and Interventions, UDMI universal definition of myocardial infarction, URL upper reference limit.


(a) Subgroup analysis of RA-related myocardial injury based on cTNI increase. (b) Subgroup analysis of RA-related myocardial injury based on CK-MB increase. LAD Left anterior descending, LCX left circumflex, RCA right coronary artery, OR odd ratio.

Clinical outcomes at the 1-year follow-up. MI myocardial infarction, TVF target vessel failure, TVMI target vessel-related MI, TVR target vessel revascularization.
Discussion
The LOTA-II study is the first to investigate clinical protection of the myocardium during RA treatment for moderate-to-severe coronary calcified lesions with low-temperature RA-flush solution compared with room-temperature RA-flush solution. The major finding of this study is that the use of low-temperature RA-flush solution during the RA procedure significantly improves myocardial protection compared to room-temperature RA-flush solution by reducing the incidence of CK-MB and cTnI elevation. Moreover, the incidences of RA-related transient slow/no flow and transient coronary spasm were significantly lower in the low temperature group than in the room temperature group. There was no apparent difference in the incidence of RA-related MI between the groups.
RA has developed into a useful tool for the management of moderate-to-severe calcified coronary lesions; it is performed by advancing a rotating abrasive burr to ablate stiff plaques. Although various effective methods for treating calcification are constantly emerging, RA remains an irreplaceable technique in PCI for coronary calcified lesions, especially lesions that cannot be passed by even the smallest balloons3,6,7,8 In addition to the more effective methods for treating calcified lesions, such as noncompliant ballooning, cutting or scoring ballooning, or intravascular lithotripsy, the mechanism of which mainly involves the cracking of calcified lesions, RA involves a mechanism of modification and debulking. The friction that occurs during the high-speed RA procedure has long been recognized to generate heat; this heat might be reduced partly by the successful cooling effect of continuous flushing with RA-solution,13,15 and the unique iatrogenic LTTD and its adverse consequences have not been considered. It is difficult to determine the consequences of LTTD due to the quantitative index of local heat production, so very few studies on this correlation have been published. However, the theory that greater RA speed deceleration leads to greater heat generation has been confirmed15 Therefore, the consensus recommendation is to avoid the deceleration of burr speed exceeding 5000 rpm during the RA procedure; interestingly, 100% of the RA procedures that were performed in our study exceeded this standard, even with continuous infusion of traditional RA-flushing solution6,7,8 Based on previous studies, LTTD is inevitable and might cause myocardial injury13,15 We speculated that the underlying mechanism is as follows: (1) friction between the RA burr and calcified lesions can generate debris that is released into distal coronary circulation, resulting in microembolism; (2) inevitable LTTD, which is caused by RA speed deceleration, especially in severe stenosis calcified lesions, further exacerbates RA speed deceleration, increases heat generation, and leads to more LTTD; and (3) the cooling effect of room-temperature RA-flush solution is weak. Inspired by the idea of the potential protective effects of cardiac hypothermia during coronary artery bypass surgery,23 although subsequent studies showed that mild hypothermia did not provide better myocardial protection than full normothermia,24 the safety of local pretreatment of the myocardium with hypothermia allowed us to establish interventions for maintaining local coronary tissues at low temperature. Another interesting finding from this study is as follows: the incidence of 1-year clinically driven TVR in the low-temperature group showed a downward trend (although it did not reach statistical significance), which may indicate that the local protection of hypothermia during RA may affect the long-term prognosis. The underlying mechanism is speculated to be related to the reduced thermal damage of the local tissue derived by RA in the low-temperature group, and the local inflammatory response after PCI is also less severe. Therefore, we designed this randomized controlled study to investigate whether low-temperature RA-flush solution can achieve greater myocardial protection through a better cooling effect than can room-temperature RA-flush solution during the RA procedure.
Nearly three-fourths of the patients in the room temperature group and half of the patients in the low temperature group had increased cTnI levels post-PCI, even after the standardized RA procedure with the traditional recommended method. However, the rate of actual RA-related MI according to the SCAI or the 4th UDMI criteria was quite low,20,21 and no significant difference was observed between the two groups. Contrary to our traditional understanding, we did not observe more coronary spasms in the low-temperature group, and we even observed significantly fewer transient coronary spasms in the low temperature group than in the room temperature group, possibly because the low-temperature RA-flush solution can more effectively reduce coronary spasms caused by the increase in local temperature caused by the RA operation. In this study, the incidence of transient slow flow and no flow in the low temperature group was also significantly lower than that in the room temperature group. It was hypothesized that the low-temperature RA-flush solution not only reduced the local coronary temperature, which was increased due to the friction of the RA burr with the vessel wall, but also perfused the microcirculatory bed in the distal segment of the coronary artery, reducing local myocardial temperature and myocardial oxygen consumption, thereby decreasing the occurrence of RA-related slow flow and no flow. Notably, the purpose of this study was to identify a new approach for optimizing the RA operation rather than clinical benefits. Moreover, the overall burr-to-vessel ratio in this study was approximately 0.5 according to the modern concept of modification;7,8 this ratio seemed to be unable to achieve better clinical results than those of patients who were not treated with RA in previous studies25,26 However, the myocardial protective effect of low-temperature RA-flush solution is stronger than that of room-temperature RA-flush solution when the burr-to-vessel ratio is between 0.5 and 0.7. Future studies can be designed to test this hypothesis.
Study limitations
The present study has several limitations. First, it is important to note that the primary endpoint of this study was RA-related myocardial injury, which is defined as any increase in a myocardial marker post-PCI; sometimes, RA-related or other PCI procedure-related myocardial injury cannot be distinguished. Second, there was a trend toward a decrease in the incidence of RA-related MI in the low temperature group, but there was no significant difference between the two groups. As a result, this study did not conclude that the low-temperature RA-flush solution may reduce the incidence of RA-related MI compared to the room-temperature RA-flush solution. Third, most patients who were enrolled in the current study underwent planned RA treatment, and the proportion of patients who underwent unplanned RA treatment was quite low. Fourth, the application of intravascular imaging technology in this study is quite low. Fifth, COVID-19 did have a small impact on this study, but it was limited to the pace of the study (patient enrollment stalled for about half a year during the height of the epidemic) and had no impact on the quality of the study.
Conclusions
Our study showed that low-temperature RA-flush solution is a safer and more effective option for RA procedure. In the present multicenter randomized study, low-temperature RA-flush solution resulted in less myocardial injury during the RA procedure than did room-temperature RA-flush solution.
Perspectives
What is known
The incidence of RA-related myocardial injury is still high even when traditional room-temperature RA-flush solution is used in the treatment of moderate-to-severe coronary calcified lesions.
What the study adds
Low-temperature RA-flush solution is associated with lower RA-related myocardial injury in patients with moderate-to-severe calcified coronary lesions than room-temperature RA-flush solution.
Data availability
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Abbreviations
- CK-MB:
-
Creatine kinase isoenzyme
- cTnI:
-
Cardiac troponin I
- DES:
-
Drug-eluting stent
- LTTD:
-
Local thermal tissue damage
- MI:
-
Myocardial infarction
- OR:
-
Odds ratio
- PCI:
-
Percutaneous coronary intervention
- QCA:
-
Quantitative coronary analysis
- RA:
-
Rotational atherectomy
- SCAI:
-
Society for cardiovascular angiography and interventions
- SMD:
-
Standardized mean difference
- TVF:
-
Target vessel failure
- TVMI:
-
Target vessel-related MI
- TVR:
-
Target vessel revascularization
- 4th UDMI:
-
Fourth universal definition of myocardial infarction
- URL:
-
Upper reference limit
References
Alexander, G. et al. Intravascular imaging during percutaneous coronary intervention: JACC State-of-the-Art review. J. Am. Coll. Cardiol. 81 (6), 590–605. https://doi.org/10.1016/j.jacc.2022.11.045 (2023).
Jennifer, S. et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: executive summary: A report of the American college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation 145 (3), e4–e17. https://doi.org/10.1161/CIR.0000000000001039 (2022). Epub 2021 Dec 9.
Shah, M., Najam, O., Bhindi, R. & De Silva, K. Calcium modification techniques in complex percutaneous coronary intervention. Circ. Cardiovasc. Interv. 14 (5), e009870. https://doi.org/10.1161/CIRCINTERVENTIONS.120.009870 (2021). Epub 2021 Jan 14.
Ata Doost, J. et al. Janarthanan Sathananthan, Abdul Rahman Ihdayhid. Contemporary Evidence-Based diagnosis and management of severe coronary artery calcification. Heart Lung Circ. 31 (6), 766–778 (2022). Epub 2022 Feb 25.
Natthapon Angsubhakorn, N. et al. Contemporary management of severely calcified coronary lesions. J. Pers. Med. 12 (10), 1638. https://doi.org/10.3390/jpm12101638 (2022).
Samin, K. et al. Aparna Bhave, Jeffrey W Moses. North American expert review of rotational atherectomy. Circ. Cardiovasc. Interv. 12 (5), e007448. https://doi.org/10.1161/CIRCINTERVENTIONS.118.007448 (2019).
Barbato, E. et al. Johann Sipötz, Iwar Sjögren, Gabor Suetsch, György Szabó, Mariano Valdés-Chávarri, Beatriz Vaquerizo, William Wijns, Stephan Windecker, Adam de Belder, Marco Valgimigli, Robert A Byrne, Antonio Colombo, Carlo Di Mario, Azeem latib, Christian Hamm; European association of percutaneous cardiovascular interventions. European expert consensus on rotational atherectomy. EuroIntervention 11 (1), 30–36. https://doi.org/10.4244/EIJV11I1A6 (2015).
Kenichi Sakakura, Y. et al. Clinical expert consensus document on rotational atherectomy from the Japanese association of cardiovascular intervention and therapeutics: update 2023. Cardiovasc. Interv Ther. 38 (2), 141–162. https://doi.org/10.1007/s12928-022-00906-7 (2023). Epub 2023 Jan 16.
Hansen, D. D., Auth, D. C., Vracko, R. & Ritchie, J. L. Rotational atherectomy in atherosclerotic rabbit Iliac arteries. Am. Heart J. 115 (1 Pt 1), 160–165. https://doi.org/10.1016/0002-8703(88)90532-7 (1988).
Tanush Gupta, M., Weinreich, M., Greenberg, A. & Colombo, A. L. Rotational atherectomy: A contemporary appraisal. Interv. Cardiol. 14 (3), 182–189. https://doi.org/10.15420/icr.2019.17.R1. (2019).
Matthew, I., Tomey, A. S., Kini, Samin, K. & Sharma Current status of rotational atherectomy. JACC Cardiovasc. Interv. 7 (4), 345 – 53. https://doi.org/10.1016/j.jcin.2013.12.196. (2014).
Ellis, S. G. et al. Relation of clinical presentation, stenosis morphology, and operator technique to the procedural results of rotational atherectomy and rotational atherectomy-facilitated angioplasty. Circulation 89 (2), 882–892. https://doi.org/10.1161/01.cir.89.2.882 (1994).
Gehani, A. A. & Rees, M. R. Can rotational atherectomy cause thermal tissue damage? A study of the potential heating and thermal tissue effects of a rotational atherectomy device. Cardiovasc. Intervent Radiol. 21 (6), 481–486. https://doi.org/10.1007/s002709900308 (1998).
Gholampour, S. Keyvan Hajirayat. Minimizing thermal damage to vascular nerves while drilling of calcified plaque. BMC Res. Notes. 12 (1), 338. https://doi.org/10.1186/s13104-019-4381-2 (2019).
Reisman, M. et al. Analysis of low-speed rotational atherectomy for the reduction of platelet aggregation. Cathet Cardiovasc. Diagn. 45 (2), 208–214. (1998).
Wei You, Y. et al. Post-PCI quantitative flow ratio predicts 3-year outcome after rotational atherectomy in patients with heavily calcified lesions. Clin. Cardiol. 45 (5), 558–566. https://doi.org/10.1002/clc.23816 (2022). Epub 2022 Mar 21.
Rheude, T. et al. Gert Richardt, Adnan Kastrati, Salvatore Cassese, Mohamed Abdel-Wahab. Rotational atherectomy or Balloon-Based techniques to prepare severely calcified coronary lesions. JACC Cardiovasc. Interv. 15 (18), 1864–1874. https://doi.org/10.1016/j.jcin.2022.07.034 (2022).
Samin, K. et al. Shingo Minatoguchi, Yuliya Vengrenyuk, Annapoorna Kini, Jeffrey W Moses. Rotational atherectomy combined with cutting balloon to optimise stent expansion in calcified lesions: the ROTA-CUT randomised trial. EuroIntervention 20 (1), 75–84. https://doi.org/10.4244/EIJ-D-23-00811 (2024).
Barbato, E. et al. Jonathan Hill, Margaret McEntegart, Kambis Mashayekhi, Nikolasos Mezilis, Yoshinobu Onuma, Krzyszstof Reczuch, Richard Shlofmitz, Giulio Stefanini, Giuseppe Tarantini, William Wijns, Flavio L Ribichini. Management strategies for heavily calcified coronary stenoses: an EAPCI clinical consensus statement in collaboration with the EURO4C-PCR group. Eur. Heart J. 44 (41), 4340–4356. https://doi.org/10.1093/eurheartj/ehad342 (2023).
Kristian Thygesen, J. S. et al. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 40 (3), 237–269. https://doi.org/10.1093/eurheartj/ehy462 (2019).
Issam, D. et al. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: an expert consensus document from the society for cardiovascular angiography and interventions (SCAI). J. Am. Coll. Cardiol. 62 (17), 1563–1570. https://doi.org/10.1016/j.jacc.2013.08.720 (2013).
McEntegart, M. et al. Incidence of procedural myocardial infarction and cardiac magnetic resonance imaging-detected myocardial injury following percutaneous coronary intervention with rotational atherectomy. EuroIntervention 14 (7), 819–823. https://doi.org/10.4244/EIJ-D-17-01077 (2018).
Renaud Tissier, B., Ghaleh, M. V., Cohen, J. M., Downey, A. & Berdeaux Myocardial protection with mild hypothermia. Cardiovasc. Res. 94 (2), 217–225. https://doi.org/10.1093/cvr/cvr315 (2012). Epub 2011 Nov 29.
Daniel, I. et al. PROTECT investigators. Aggressive intraoperative warming versus routine thermal management during non-cardiac surgery (PROTECT): a multicentre, parallel group, superiority trial. Lancet 399 (10337), 1799–1808. https://doi.org/10.1016/S0140-6736(22)00560-8 (2022). Epub 2022 Apr 4.
Richardt, M. A. W. G. et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: the randomized ROTAXUS (Rotational atherectomy prior to Taxus stent treatment for complex native coronary artery Disease) trial. JACC Cardiovasc. Interv. 6 (1), 10–19. https://doi.org/10.1016/j.jcin.2012.07.017 (2013). Epub 2012 Dec 19.
Toelg, M. A. W. R. et al. High-Speed rotational atherectomy versus modified balloons prior to Drug-Eluting stent implantation in severely calcified coronary lesions. Circ. Cardiovasc. Interv. 11 (10), e007415. https://doi.org/10.1161/CIRCINTERVENTIONS.118.007415 (2018).
Acknowledgements
The authors acknowledge Dr. Bao-Xiang Duan as the director of the independent committee. We thank Ms. Ling Lin and Ms. Hai-Mei Xu (clinical trial coordinator) for their contributions to the completion of this study. The authors also thank Ms. Lingling Liu, Ms. Rongfang Wang, Ms. Yingying Zhao, and Ms. Wen Teng for remote monitoring and data collection throughout the study.
Funding
The LOTA-II study is a clinical program funded mainly by the JiangSu Provincial (China) Health Commission Medical Research Project [ZDB2020029].
Author information
Authors and Affiliations
Contributions
Wei You, Xiang-qi Wu, and Zhi-ming Wu wrote the main manuscript text and Yi-fei Wang, Tong-tong Shen, and Bi Tang prepared Figs. 1, 2 and 3. Tian Xu, Liang-hong Ying and De-feng Pan prepared Tables 1, 2 and 3. Song Yang, De-lu Yin, and Fei Ye designed the whole study and got funding. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Disclosures
Dr. De-lu Yin received research grants from the JiangSu provincial (China) Health Commission Medical Research Project.
Ethics committee/institutional review board
Ethics Committee of Nanjing First Hospital. Ethics number: KY20180713-04.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
You, W., Wu, Xq., Wu, Zm. et al. Safety and efficacy of low-temperature RA-flush solution in patients with moderate-to-severe calcified lesions (LOTA-II): a randomized, double-blind, multicenter study. Sci Rep 15, 18280 (2025). https://doi.org/10.1038/s41598-025-02799-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-02799-x
Keywords
This article is cited by
-
Clinical expert consensus document on rotational atherectomy from the Japanese association of cardiovascular intervention and therapeutics: update 2026
Cardiovascular Intervention and Therapeutics (2026)
