
Abstract
Herein, 4D-flow MRI was performed on the bilateral carotid arteries in a rat model of unilateral carotid artery injury to analyze changes in flow velocity, flow rate, wall shear stress (WSS), and cross-sectional area due to endothelial injury. MR images of the rat carotid artery were acquired using 7T-MRI. Seven control rats and 16 rats with right endothelial injury (VED) were used. For five of the VED models where blood flow in both the right and left common carotid arteries was confirmed, 4D-flow MRI was performed after obtaining 3D images using the time of flight method. MRI was performed to calculate the flow velocity, flow rate, WSS, and cross-sectional area of the proximal, middle, and distal carotid arteries. In all five VED models, blood flow rate and WSS were predominantly decreased at the proximal injured side compared to the ipsilateral control side (p < 0.05). The cross-sectional area of the vessel distal to the injured side of the VED model was reduced compared to that of the non-injured side (p < 0.05). A comparison of the proximal part of the uninjured side between the control group and VED model showed that the vascular cross-sectional area was predominantly increased in the VED model (p < 0.05). 4D-flow MRI with 7T-MRI enabled analysis of changes in flow velocity, flow rate, WSS, and cross-sectional area due to vascular endothelial injury.
Similar content being viewed by others


Introduction
Atherosclerosis is the leading cause of disease and mortality in most developed countries1. Although age-related deaths attributable to atherosclerosis are declining, in 2019, approximately 18 million people worldwide died from cardiovascular diseases, primarily coronary and cerebrovascular atherosclerosis. Atherosclerosis has several types: an intracranial lesion called intracranial atherosclerotic disease (ICAD), and an extracranial lesion called internal carotid artery stenosis (ICS). When the vascular intima-media is damaged, atherosclerosis develops due to plaque formation, resulting in changes in blood flow and cross-sectional area2. The evaluation of vascular characteristics is important for understanding the pathogenesis of atherosclerosis. Despite advances in our understanding of the pathophysiology, pathogenesis, and new treatment modalities, the absence of an adequate non-invasive imaging tool for early detection limits the prevention and treatment of patients with various degrees and anatomical localizations of atherothrombotic disease. An ideal clinical imaging modality for atherosclerotic vascular disease should be safe, inexpensive, non-invasive, minimally invasive, accurate, and reproducible. Moreover, the imaging results should correlate with the extent of atherosclerotic disease and have a high predictive value for future clinical events.
Ultrasonography (US) is a versatile diagnostic tool for arteriosclerosis3,4. Although US is simple and enables real-time observation, it is limited to the evaluation of temporal changes in a single cross-section. Magnetic resonance imaging (MRI) is the most promising technique for studying atherothrombotic diseases in humans5,6. MRI has various tissue-contrast imaging techniques and allows for the characterization of plaque composition, including the discrimination of the lipid core, fibrosis, calcification, and intraplaque hemorrhage deposits7. Therefore, MRI is considered the gold standard for non-invasive evaluation of carotid artery plaque morphology and composition. In addition to measuring plaque formation, MRI can be used to assess changes in vascular blood flow and wall shear stress (WSS), providing useful diagnostic information on the pathogenesis of atherosclerosis. 4D-flow MRI can quantitatively evaluate temporal changes in blood vessels in three dimensions and multiple cross-sections and can also evaluate basic factors related to arterial stiffness, such as WSS8,9. Several animal studies have demonstrated the usefulness of 4D-flow MRI in evaluating rodent models10,11,12.
The purpose of this study is to perform 4D-flow MRI on rat carotid arteries to evaluate changes in flow velocity, WSS, and vessel cross-sectional area due to endothelial injury in rats used as a model of atherosclerosis.
Materials and methods
Animal preparation
All experimental protocols were approved by the Research Ethics Committee of our University. All experimental procedures involving animals and their care were performed in accordance with the Osaka University Guidelines for Animal Experimentation and the National Institutes of Health Guide for the Care and Use of Laboratory Animals. Sprague-Dawley rats (10–12 weeks old) were purchased from Japan SLC (Hamamatsu, Japan). Seven control rats and 16 rats with right endothelial injury (VED) were used in this study. All rats were housed in a controlled vivarium environment (24 °C; 12:12 h light/dark cycle) and were fed a standard pellet diet and water ad libitum. Rat carotid artery balloon injury models (right carotid artery endothelial injury) were generated as follows: (1) The rat was given isoflurane 1.5 to 2.0% inhalation anesthesia using an inhalation anesthetic device. (2) The rat was placed in a supine position with the treated side up. (3) The skin near the right margin of the laryngeal cartilage was incised, and the external carotid artery (ECA) and common carotid artery (CCA) were dissected. (4) A balloon catheter was inserted into the CCA through an incision in the dissected ECA. (5) The balloon catheter was inserted into the CCA, the incision was incised, and a balloon catheter was inserted into the CCA. 10 µL of the balloon was inflated and passed through the artery one time to disrupt the endothelium, the balloon catheter was removed, the ECA was ligated and the incision was sutured. (6) An antibiotic (enrofloxacin) was administered subcutaneously at a dose of 5 mg/kg. (7) An analgesic (buprenorphine) of 0.05 mg/kg was administered subcutaneously once postoperatively.The time interval between the balloon injury and MR examination was 1 week.
MRI
MR images of the animal necks were acquired using a horizontal 7-T scanner (PharmaScan 70/16 US; Bruker Biospin, Ettlingen, Germany) equipped with a 60 mm inner diameter volume coil. The rats were positioned in stereotaxic frames with their mouths secured to prevent movements during acquisition13,14. The body temperature was maintained at 36.5 °C with regulated water flow and was continuously monitored using a physiological monitoring system (SA Instruments Inc., Stony Brook, NY, USA). All MR experiments were performed under general anesthesia using isoflurane (3.0% for induction and 2.0% for maintenance).
Morphological information was acquired using 3D time-of-flight magnetic resonance angiography (MRA) with the following parameters: pulse sequence, flow-compensated 3D gradient-echo sequence; TR, 12 ms; TE, 2.6 ms; flip angle (FA), 20°; field-of-view, 32 × 32 × 32 mm3; matrix size, 200 × 200 × 200; number of averages, 1; slice thickness, 32 mm; slab orientation, trans-axial; spatial resolution, 160 μm × 160 μm × 160 μm; scan time, 6 m 37 s. 4D-flow images were acquired using time-resolved 3D phase contrast angiography under ECG gating with the following parameters: pulse sequence, flow-compensated gradient-echo sequence with bipolar gradients; TR,12 ms; TE, 2.9 ms; flip angle (FA), 30°; field-of-view, 32 × 32 × 32 mm3; matrix size, 150 × 150 × 25 mm3; number of averages, 2; slice thickness, 5 mm; number of frames, 10; slab orientation, trans-axial; spatial resolution, 200 μm × 200 μm × 200 μm; scan time, around 2 h; VENC, 125 cm/s. Flow velocities along the three orthogonal spatial directions were calculated using four velocity-encoding gradient steps based on a Hadamard encoding scheme.
MRI data analysis
From the MRI image, the CCA was defined from the aortic arch bifurcation to the internal and external carotid bifurcations. The CCA was divided into three parts: proximal, middle, and distal, starting from the portion closest to the heart (Fig. 1). The dotted line indicates the area of each part and the area’s vertical width is about 1 cm. The values of the flow rate and cross-sectional area, we draw a line through the center of the area and measured the average value at the centerline of each part. The WSS was measured the average value from the entire area of each part. All values were calculated using a fluid analysis software iTFlow@ (Cardio Flow Design Inc. Tokyo, Japan).

Definition of parts in MRA MIP image of control rat. The common carotid artery is divided into three parts: proximal, middle, and distal, starting from the section closest to the heart. The dotted lines indicate the areas of each part. The average values of the flow rate and cross-sectional area were measured at the centerline of each part, and the wall shear stress was measured from the entire area of each part.
Statistical analysis
All data are presented as mean ± standard deviation. Differences were compared using one-way ANOVA followed by Tukey’s post-hoc test to evaluate all parameters (velocity, WSS, and vessel area). All analyses were performed using Prism 8 software (GraphPad Software, San Diego, CA, USA). P < 0.05 was considered statistically significant.
Results
The average body weight of the control rats was 353.1 ± 23.4 g, while the average body weight of the VED model rats was 339.2 ± 5.0 g. There was no significant difference between the average body weights of the control and VED model rats.
Figure 2 shows the maximau intensity projection (MIP) images of the control (Fig. 2a) and VED model (Fig. 2b) rats. As indicated by the white arrow, the right CCA of the VED model was clearly thinner and narrower than that of the control. Figure 3 shows the average cross-sectional areas. In the control group, the cross-sectional area significantly decreased from proximal to distal on both sides ([left] proximal:1.3 ± 0.3 mm2, distal: 0.0 ± 0.2 mm2, p < 0.05 [right] proximal: 1.4 ± 0.3 mm2, distal: 0.9 ± 0.3 mm2, p < 0.01, Fig. 3a). A similar trend was observed in the VED model ([left] proximal: 2.1 ± 0.6 mm2, distal: 1.1 ± 0.4 mm2, p < 0.01 [right] proximal: 1.5 ± 0.5 mm2, distal: 0.6 ± 0.2 mm2, p < 0.05, Fig. 3b). The value of left proximal CCA in VED model significantly improved 60% (control: 1.3 ± 0.3 mm2, VED model :2.1 ± 0.6 mm2, p < 0.05).

MRA MIP images of (a) control and (b) VED model rats. The white arrow indicates that the right common carotid artery of the VED model was thinner and narrow compared to that of the control group.

Cross-sectional area. The cross-sectional area of the control group was significantly reduced from proximal to distal ([left] proximal:1.3 ± 0.3 mm2, distal: 0.0 ± 0.2 mm2, p < 0.05, [right] proximal: 1.4 ± 0.3 mm2, distal: 0.9 ± 0.3 mm2, p < 0.01). A similar trend was observed in the VED model ([left] proximal:2.1 ± 0.6 mm2, distal: 1.1 ± 0.4 mm2, p < 0.01, [right] proximal: 1.5 ± 0.5 mm2, distal: 0.6 ± 0.2 mm2, p < 0.05). The value of proximal of light common carotid artery was significantly different between control and VED model (control: 1.3 ± 0.3 mm2, VED model: 2.1 ± 0.6 mm2, p < 0.05). *p < 0.05, **p < 0.01.
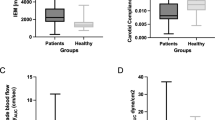
Figure 4 shows the 4D-flow streamline images of the control (Fig. 4a) and VED model (Fig. 4b) rats. As seen in the velocity maps derived from 4D-flow imaging, the velocity of the right CCA in the VED model was lower than in the control group (Fig. 4b). Figure 5 shows the average values of the mean flow rate. In the control group, there was no significant left-right difference in flow velocity (Fig. 5a). While the flow rate of the right proximal CCA was significantly decreased compared to the flow rate of the left proximal CCA (L: 46.0 ± 17.8 µL/beat, R: 20.0 ± 7.8 µL/beat, p < 0.05, Fig. 5b), the value of the right CCA was reduced by 38% compared to that of control rats in the VED model (control: 32.1 ± 7.9 µL/beat, VED model: 20.0 ± 7.8 µL/beat, p < 0.05).

4D-flow streamline images of (a) control and (b) VED model. The endothelial injury was made over the entire right common carotid artery in VED model. The velocity of the right common carotid artery in the VED model (b) was lower than that in the control (a).

Flow rate. There was a significant difference between the flow rates of the right and left proximal common carotid artery in the VED model (L:46.0 ± 17.8 µL/beat, R:20.0 ± 7.8 µL/beat, p < 0.05). The flow rate of the proximal right CCA was significantly different between the control and the VED model (control: 32.1 ± 7.9 µL/beat, VED model: 20.0 ± 7.8 µL/beat, p < 0.05). * p < 0.05, unpaired t-test.
Figure 6 shows the 4D-flow WSS images of the control group (Fig. 6a) and VED rats (Fig. 6b). The WSS of the right CCA in the VED model was lower than that in the control group. Figure 7 presents the average values of mean WSS. There was no significant left-right difference in velocity in either group of rats (Fig. 7a, b). However, the WSS in right proximal CCA was significantly decreased 35% compared to that of the control group (control: 7.2 ± 1.2 Pa, VED model :4.7 ± 1.4 Pa, p < 0.05).

4D-flow WSS images of (a) control and (b) VED model. The endothelial injury was made over the entire right common carotid artery in VED model. The WSS of the right common carotid artery in the VED model (b) was lower than that in the control (a).

WSS (a) Control (b) VED model. Comparisons of the same model showed no significant differences between the parts. WSS of proximal of right common carotid artery was significantly different between the control and the VED model (control: 7.2 ± 1.2 Pa, VED model: 4.7 ± 1.4 Pa, p < 0.05).
Discussion
Our study is the first to demonstrate changes in flow velocity, flow rate, WSS, and cross-sectional area due to endothelial injury using 4D-flow MRI of the bilateral carotid arteries in a rat model of unilateral carotid artery injury. In the VED models, the blood flow rate and WSS were predominantly decreased on the proximal injured side compared to the ipsilateral control side. Furthermore, the cross-sectional area of the vessel distal to the injured side in the VED model was reduced compared to that of the non-injured side. A comparison of the proximal area of the uninjured side between the control group and the VED model showed that the vascular cross-sectional area was predominantly increased in the VED models. The area in which these results were seen was uniform throughout the VED models.
In this study, significant reductions in velocity and flow were observed in the proximal part of the CCA in the VED model using 4D-flow MRI. This may be attributed to the fact that the distal part of the CCA is smaller in diameter than the proximal part (Fig. 3) and that a strong stenosis occurs at the catheter insertion stage of modeling. In carotid vascular echocardiography, in humans, the maximum systolic blood flow velocity increases when carotid artery stenosis exceeds 50%, and the blood flow velocity increases as stenosis progresses15. In patients with stenosis, 4D-flow MRI was used to measure end-diastolic and systolic flow velocities in the common and internal carotid arteries; flow velocity was decreased in the CCA and increased in the internal carotid artery (ICA)16. In other words, the flow velocity increases at the site of stenosis and decreases proximal to the stenosis, a pattern observed during both end-diastole and systole. The trend of increased flow velocity at the stenosis and decreased flow velocity proximal to the stenosis is consistent with findings from previous studies. Even within the newly stenosed vessel in this study, there was a difference in flow velocity between the stenotic area and the proximal part of the stenosis, with the flow velocity being lower at the proximal part of the stenosis.
In the VED model used in this study, the WSS was also significantly lower in the proximal part of the stenotic vessel, likely due to the decreased flow velocity at the proximal end of the CCA, as mentioned above. This is because WSS is calculated by dividing the flow velocity by the vessel radius17. Furthermore, we believe that the lack of a significant change in vessel diameter, despite the significant decrease in flow rate, is another factor contributing to the lower WSS. In a previous study, after 6–12 weeks of clipping the unilateral CCA in rats, flow and vessel diameter were measured, and the clipped vessels showed an average 35% decrease in flow and a 10.2% decrease in diameter18. Alterations in WSS affect the function and shape of endothelial cells, potentially leading to the development of atherosclerosis and other vascular diseases. It is known that an increase in flow velocity results in an increase in vessel diameter, while a decrease in flow velocity reduces vessel diameter to maintain a constant WSS19. In this study, a significant increase in the cross-sectional area was observed in the proximal part of the non-stenotic vessel in the VED model. The WSS in this area was not significantly different from that of the controls. Although there was no statistically significant difference in the flow rate due to the size of the SD, there was a trend toward increased flow in the proximal part of the non-stenotic vessel in the VED model compared with the control group (Fig. 5). Because there was no significant change in WSS with increased flow, we considered that the cross-sectional area of the vessel increased with changes in flow to maintain constant WSS, consistent with previous studies.
Limitation
This study had some limitations. First, we used a VED model in which endothelial damage was induced by inserting a balloon catheter to promote endothelial thickening. However, it was difficult to control the degree of damage (severe or mild) due to the nature of the model, and there were individuals in whom blood flow could not be measured using MRI because of severe damage. Even in individuals in whom blood flow in the CCA could be confirmed, evaluating the distal portion of the carotid artery was challenging data variability increased as the evaluation moved farther distally. Although the VED model used in this study is widely accepted as a model of carotid artery stenosis, it has been noted that creating a stable model remains difficult. Various alternative models of carotid artery stenosis and endothelial thickening have been proposed, such as those involving hypertension or high-fat diet feeding. However, it is necessary to validate findings using these other models in future studies.
Second, the flow velocity was calculated based on the mean flow velocity per cardiac cycle. Many previous studies on human subjects measured flow velocities during the end-diastole and systole phases of the cardiac cycle. While the same evaluation was performed in this study, maintaining a constant heart rate was challenging due to the extended imaging time and the effects of anethesia. Consequently, evaluation was conducted in units of one cardiac cycle.
Finally, carotid screening in clinical practice typically involves US to measure the rate of stenosis caused by endothelial thickening of the carotid artery for diagnostic purposes. In this study, we attempted to confirm the degree of endothelial thickening by excising the CCA and staining it with HE. However, identifying the stenotic area and calculating the stenosis rate proved difficult.
In the future, we plan to review imaging time, anesthesia management, and other influencing factors to calculate and evaluate values for each parameter during end-diastole and systole. Additionally, we intend to conduct further research using alternative models to enhance clinical applicability.
Conclusion
4D-flow MRI with 7T-MRI enabled the analysis of changes in flow velocity, flow rate, WSS, and cross-sectional area caused by vascular endothelial injury in a rat model of unilateral carotid artery injury.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Chen, W., Li, Z., Zhao, Y., Chen, Y. & Huang, R. Global and National burden of atherosclerosis from 1990 to 2019: trend analysis based on the global burden of disease study 2019. Chin. Med. J. (Engl). 136, 2442–2450. https://doi.org/10.1097/CM9.0000000000002839 (2023).
Virani, S. S. et al. Heart disease and stroke Statistics-2021 update: A report from the American heart association. Circulation 143, e254–e743. https://doi.org/10.1161/CIR.0000000000000950 (2021).
Carroll, B. A. Carotid ultrasound. Neuroimaging Clin. N Am. 6, 875–897 (1996).
Wilson, E. P. & White, R. A. Intravascular ultrasound. Surg. Clin. North. Am. 78, 561–574. https://doi.org/10.1016/s0039-6109(05)70334-0 (1998).
Yuan, C. & Kerwin, W. S. MRI of atherosclerosis. J. Magn. Reson. Imaging. 19, 710–719. https://doi.org/10.1002/jmri.20070 (2004).
Coolen, B. F. et al. Vessel wall characterization using quantitative MRI: what’s in a number? MAGMA 31, 201–222, (2018). https://doi.org/10.1007/s10334-017-0644-x
Benson, J. C. et al. Cervical carotid plaque MRI: review of atherosclerosis imaging features and their histologic underpinnings. Clin. Neuroradiol. 31, 295–306. https://doi.org/10.1007/s00062-020-00987-y (2021).
Soulat, G., McCarthy, P. & Markl, M. 4D flow with MRI. Annu. Rev. Biomed. Eng. 22, 103–126. https://doi.org/10.1146/annurev-bioeng-100219-110055 (2020).
Markl, M., Schnell, S. & Barker, A. J. 4D flow imaging: current status to future clinical applications. Curr. Cardiol. Rep. 16, 481. https://doi.org/10.1007/s11886-014-0481-8 (2014).
Nahardani, A. et al. Pulmonary arteriovenous pressure gradient and Time-Averaged mean velocity of small pulmonary arteries can serve as sensitive biomarkers in the diagnosis of pulmonary arterial hypertension: A preclinical study by 4D-Flow MRI. Diagnostics (Basel). 12. https://doi.org/10.3390/diagnostics12010058 (2021).
Braig, M. et al. Preclinical 4D-flow magnetic resonance phase contrast imaging of the murine aortic arch. PLoS One. 12, e0187596. https://doi.org/10.1371/journal.pone.0187596 (2017).
Andelovic, K. et al. 2D projection maps of WSS and OSI reveal distinct Spatiotemporal changes in hemodynamics in the murine aorta during ageing and atherosclerosis. Biomedicines 9 https://doi.org/10.3390/biomedicines9121856 (2021).
Saito, S., Takahashi, Y., Ohki, A., Shintani, Y. & Higuchi, T. Early detection of elevated lactate levels in a mitochondrial disease model using chemical exchange saturation transfer (CEST) and magnetic resonance spectroscopy (MRS) at 7T-MRI. Radiol. Phys. Technol. 12, 46–54. https://doi.org/10.1007/s12194-018-0490-1 (2019).
Saito, S. & Ueda, J. Preclinical magnetic resonance imaging and spectroscopy in the fields of radiological technology, medical physics, and radiology. Radiol. Phys. Technol. 17, 47–59. https://doi.org/10.1007/s12194-024-00785-y (2024).
Arous, E. J. et al. Institutional differences in carotid artery duplex diagnostic criteria result in significant variability in classification of carotid artery stenoses and likely lead to disparities in care. Circ. Cardiovasc. Qual. Outcomes. 7, 423–429. https://doi.org/10.1161/CIRCOUTCOMES.113.000855 (2014).
Harloff, A. et al. Comparison of blood flow velocity quantification by 4D flow MR imaging with ultrasound at the carotid bifurcation. AJNR Am. J. Neuroradiol. 34, 1407–1413. https://doi.org/10.3174/ajnr.A3419 (2013).
Efstathopoulos, E. P. et al. Wall shear stress calculation in ascending aorta using phase contrast magnetic resonance imaging. Investigating effective ways to calculate it in clinical practice. Phys. Med. 24, 175–181. https://doi.org/10.1016/j.ejmp.2008.01.004 (2008).
Guyton, J. R. & Hartley, C. J. Flow restriction of one carotid artery in juvenile rats inhibits growth of arterial diameter. Am. J. Physiol. 248, H540–546. https://doi.org/10.1152/ajpheart.1985.248.4.H540 (1985).
Fujiwara, Y., Furukawa, K., Tanaka, M., Tanaka, S. & Nakade, Y. [Evaluation of platelet transfusion]. Rinsho Ketsueki. 19, 1417–1421 (1978).
Acknowledgements
This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (grant number 19K08172, 23H03763) and JPMXS0450400023, 24/Ministry of Education, Culture, Sports, Science and Technology.
Author information
Authors and Affiliations
Contributions
S.Y., N.B., M.I., K.B., R.S., J. U. and S.S. conceived the study, collected the data, performed data analysis, wrote the manuscript, and prepared all figures; S.Y. also assisted in data collection and data analysis; N.B., M.I., J.U., K.B., R.S. and S.S. reviewed the manuscript; S.S. conceived the study, obtained funding, and reviewed the manuscript All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics declarations
This animal study was conducted in accordance with the ARRIVE guidelines. All experimental protocols were approved by the Research Ethics Committee of Osaka University, Osaka, Japan (Number: R02-05-0).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yasuda, S., Banura, N., Ito, M. et al. In-vivo assessment of vascular endothelial injury in a rat model of unilateral carotid artery injury using 4D-flow MRI. Sci Rep 15, 18571 (2025). https://doi.org/10.1038/s41598-025-03721-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-03721-1
