
Abstract
Limited research have been conducted on the interrelationship and role of oxidative stress and Metabolic Associated Fatty Liver Disease (MAFLD) within the population. The Oxidative Balance Score (OBS) serves as a metric for evaluating an individual’s overall oxidative stress status. This study seeks to investigate the impact of OBS on the population and elucidate its potential mechanisms. 9881 participants from the 2003–2018 NHANES were involved in our study. Covariate-adjusted regression models showed a statistically significant inverse association between elevated OBS and MAFLD risk. Specifically, participants in the upper threshold quartile (Q4) had 40% lower risk of MAFLD odds (OR = 0.60, 95% CI 0.50–0.72; P < 0.001) compared to those in the lowest reference quartile (Q1). The population attributable fraction analysis (PAF) suggested that MAFLD reduction could be attributed to approximately 12.67% Q4 OBS and 8.00% Q3 OBS. Restricted cubic spline (RCS) analysis revealed a non-linear association between oxidative balance score OBS and MAFLD. In the mediation analysis, inflammatory markers, insulin resistance markers, and body mass index (BMI) were found to partially mediate the association between OBS and MAFLD. The continuous OBS (HR: 0.97, 95% CI (0.94, 1.00); P = 0.049) demonstrated a reduced risk of total mortality among MAFLD patients. In the U.S. population, significant negative associations were observed between OBS and MAFLD. The results indicated that an antioxidant lifestyle may hold greater significance than an antioxidant diet in the prevention of MAFLD. Additionally, our findings implied that insulin resistance, inflammation, and BMI may contribute to the relationship between OBS and MAFLD.
Similar content being viewed by others


Introduction
Metabolic-associated fatty liver disease (MAFLD) is a prevalent chronic liver disease characterized by at least 5% hepatic steatosis infiltrating hepatocytes, occurring in association with type 2 diabetes, metabolic syndrome, or overweight and obesity1. Previously, non-alcoholic fatty liver disease (NAFLD), formerly known as MAFLD, affected around 25% of the global population1. The prevalence of MAFLD has increased significantly in recent years, coinciding with the rise in unhealthy lifestyles characterized by excessive calorie intake and a lack of physical activity2. This has significantly burdened the health system. The definition of alcohol consumption remains a topic of debate due to the ongoing observation of patients engaging in drinking behaviors, and the NAFLD definition’s inability to encompass the metabolic dysfunctions commonly associated with fatty liver4. Therefore, in early 2020, an international panel of experts proposed a change from NAFLD to MAFLD. This new definition is both comprehensive and accessible, and is independent of other liver diseases6. MAFLD is more comprehensive than NAFLD in identifying individuals at risk for progressive liver disease7. Some studies have shown that MAFLD has a greater advantage in predicting chronic kidney and cardiovascular diseases8. Despite recent advances in understanding MAFLD, there are currently no effective drugs to intervene or treat MAFLD. The development of MAFLD is influenced by several factors, including genetic predisposition, oxidative stress, insulin resistance (IR), and mitochondrial dysfunction10. Previous studies have indicated that dietary and lifestyle modifications may prove beneficial in the prevention and treatment of MAFLD. However, the isolated effects of diet and lifestyle on MAFLD have been the main focus of most of these studies. Concerning dietary modifications, evidence suggests that adherence to a low-inflammatory diet (DII), the Mediterranean diet, as well as diets low in saturated fats and low in inflammatory indexes, may potentially reduce the prevalence of MAFLD11. Higher levels of antioxidant nutrients, including vitamins and carotenoids, have been associated with a lower prevalence of MAFLD12. Additionally, consistent exercise and good sleep habits have been shown to reduce the prevalence of MAFLD15. It is important to understand that the human body is a complex system and the influence of any individual factor on disease cannot be fully understood without taking into account diet and lifestyle. While research has demonstrated a correlation between nutrients linked to oxidative stress and MAFLD, dietary interactions may influence the efficacy of combined nutrient supplementation17. The Oxidative balance scores (OBS), an integrated score of dietary and lifestyle effects on the overall oxidative/antioxidant system, was created to evaluate an individual’s overall antioxidant status18. This metric merges dietary/lifestyle elements related to oxidation, where a high OBS suggests dominant antioxidant influence19. In recent years, numerous studies have demonstrated a correlation between OBS and an array of chronic illnesses, including type 2 diabetes(T2DM)19, chronic kidney disease20, cardiovascular disease21, and metabolic syndrome22.
A number of cross-sectional studies have recently demonstrated an association between OBS and a reduced risk of developing non-alcoholic fatty liver disease (NAFLD)23 or metabolic dysfunction-associated steatotic liver disease (MASLD)25. However, there is lack evidence to support an association between OBS and MAFLD. To address this knowledge gap, we used cross-sectional NHANES 2003 to 2018 data to examine the association of OBS with MAFLD in US adults. We also investigated whether IR, inflammatory markers and BMI mediated the association between OBS and MAFLD.
Methods
Design and participants
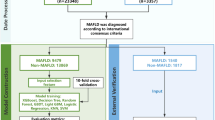
The National Health and Nutrition Examination Survey (NHANES) is a national survey of a periodic cross-sectional sample of adults and children in the United States. The NHANES aims to evaluate well-being and dietary habits across US demographics. The data from the survey include the presence or absence of disease, risk factors for disease, and nutritional status. These data were collected through household interviews and standardized physical exams that included blood and urine samples from mobile screening centers. This study was conducted on eight 2-year survey cycles from 2003–2018 (2003–2004, 2005–2006, 2007–2008, 2009–2010, 2011–2012, 2013–2014, 2015–2016, and 2017–2018) that recruited greater than 47,763 participants equal to 18 years of age. These individuals were excluded for various reasons. Firstly, 1964 participants with a weight of 0 and 26,295 subjects with missing defined MAFLD data were excluded. Secondly, 9527 subjects lacking defined OBS data were excluded. Lastly, 96 of the pregnant group were excluded. In conclusion, the final analysis included 9881 subjects. The detailed of inclusion criteria and exclusion criteria are shown in Fig. 1. The NHANES project received approval from the NCHS Ethics Review Board, and participants gave written informed consent. NHANES official site provides further details. (https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/default.aspx?Cycle=2017-2020).

Flow diagram of inclusion criteria and exclusion criteria. NHANES, National Health and Nutrition Examination Survey; MAFLD, metabolic-associated fatty liver disease; OBS, oxidative balance score.
Evaluation of OBS
Derived from past studies, the OBS consisted of 16 dietary and 4 lifestyle factors, categorized into 5 pre-oxidants (total fat, iron, alcohol intake and nicotine intake) and 15 antioxidants (dietary fiber, carotenoids, riboflavin, niacin, vitamin B6, total folate, vitamin B12, vitamin C, vitamin E, calcium, magnesium, zinc, copper, selenium, physical activity and BMI). Dietary data were obtained from the NHANES 24-h dietary recall, as listed in Supplemental Table 1. Lifestyle data were extracted from questionnaires and examinations (physical activity, alcohol intake, BMI) and laboratory measurements (nicotine intake). Serum cotinine is a metabolite of nicotine and was utilized as an indicator of tobacco smoke exposure. The scheme of assigning OBS scores was based on previous scholars, such as Zhang et al.26. Scores (0, 1, 2) were assigned based on gender stratification. In the case of antioxidants, a higher level of exposure results in a higher score. Conversely, greater exposure to pro-oxidants is associated with lower scores. The final score was calculated by summing the individual scores to obtain the total OBS, with higher scores indicating elevated antioxidant exposure. The specific scoring scheme was presented in the Online Appendix (Supplemental Table 1).
Definition of MAFLD
A positive diagnosis of MAFLD requires proof of liver fat accumulation by histology, imaging or blood biomarkers. It also requires one of the following three criteria: being overweight or obese (BMI ≥ 25 kg/m2), having Type 2 Diabetes or evidence of metabolic dysregulation. Evidence of metabolic dysregulation was defined by the presence of at least two risk abnormalities: (a) men waist ≥ 102 cm, women waist ≥ 88 cm; (b) blood pressure ≥ 130/85 mm Hg or pharmaceutical interventions; (c) and triglycerides ≥ 150 mg. (d) High cholesterol ≥ 150 mg/dL (≥ 1.70 mm/L) or specific medication; (e) Prediabetes (fasting glucose 100–125 mg/dL) Glucose 5.6- 6.9 mmol/L or 2-h meal 140–199 mg/dL (7.8–11 mmol/L); HbA1c 5.7–6.4% (39–47 mmol/mol); HOMA-IR ≥ 2.5(HOMA-IR = fasting glucose (mmol/L) ∗ fasting insulin (μU/mL)/22.5)27) and (g) plasma high-sensitivity C-reactive protein level > 2 mg/litre. C-reactive protein not available in NHANES 2011–201428.
Hepatic steatosis was defined by the US FLI, which was used as a proxy for the clinical diagnosis of NAFLD and was derived specifically for the NHANES database, Fig. 2. Its consensus included body mass index, waist circumference, triglycerides, and gamma glutamyl transferase (GGT) activity, defining fatty liver as a US FLI ≥ 3029.

The formula of US FLI.
The US FLI ranges from 0 to 100 and is derived using the following formula, where ‘non-Hispanic black’ and ‘Mexican American’ are assigned a value of 1 if the participant is of that ethnicity and 0 if they are not of that ethnicity:
Based on the comorbidity of MAFLD with Metabolic Syndrome and Type 2 Diabetes, MAFLD could be further categorized into four subtypes, namely metabolically unhealthy MAFLD, metabolically healthy MAFLD, pre-diabetic MAFLD and diabetic MAFLD. In this context, Metabolic health refers to the absence of metabolic syndrome and does not mean that the body is completely metabolically normal.
Covariates
The research considered covariates included age (continuous variable), gender (male, female), race (non-Hispanic black, non-Hispanic white, Hispanic, other races), Physical activity (activity (≥ 600 MET min/week); Inactive (< 600 MET min/week))30 and comorbidities. Comorbidities included hypertension, hyperlipidemia, and diabetes mellitus, which were diagnosed by index measurements, medication use, and self-report. Data of Neutrophil Percentage to Albumin Ratio (NPAR) and homeostasis model assessment of insulin resistance (METS-IR) also collected. The formula for calculating METS-IR and NPAR as follow: METS-IR = ln (2 × Fasting Plasma Glucose (FPG) [mg/dL] + fasting serum triglyceride [mg/dL]) × BMI (kg/m2) / ln (HDL cholesterol [mg/dL])31; NPAR = Neutrophil percentage (in total WBC count) (%) × 100/Albumin (g/dL)32.
Statistical analysis
We first downloaded the NHANES data associated with this study from 2003 through 2018. NHANES recommended sample weight records were used to determine individual sample weights. Data for continuous variables were presented using mean values and standard deviation (SD), while categorical variables were presented using numerical counts and percentages of frequencies (%). Weighted logistic analyses were used to examine the relationship between overall OBS, lifestyle OBS, dietary OBS, and MAFLD using three models. Model 1, a crude model with no additional adjustment for covariates; Model 2, adjusted for age, sex, and race/ethnicity; and Model 3, adjusted for age, sex, race, physical activity, diabetes, and hypertension. The population attributable fraction (PAF) has been commonly used to measure the burden of disease attributable to a given risk factor, and then the PAF was used to estimate the proportion of MAFLD that could be avoided if the exposure OBS were eliminated. In addition, based on logistic regression results, restricted cubic spline (RCS) analyses were used to test for nonlinear trends between variables. We also examined potential mediators of METS-IR, NPAR and BMI in the association between OBS and MAFLD. The association between OBS and all-cause mortality in MAFLD was examined using Cox proportional hazards models. R (version 4.2.1) was used for all data cleaning and processing. Additionally, all analyses were two-tailed and P < 0.05 was considered statistically significant.
Results
Study population characteristics
The study population consisted of 9881 non-institutionalised US residents. 3111 of these had MAFLD, representing a prevalence of 31.48% in the national population. The baseline characteristics of the participants in the study are shown in Table 1. The mean age of the study population was 45.68 ± 16.75 years, 52.00% were male and 69.00% were non-Hispanic white. With regard to sociodemographic characteristics, individuals with MAFLD were more likely to be older, male, non-Hispanic white. With regard to blood markers, individuals with MAFLD exhibited elevated levels of LDL, HbA1c, METS-IR, HOMA-IR, while HDL levels were diminished. Furthermore, the NPAR which are indicative of systemic inflammation, were elevated in the MAFLD cohort. The prevalence of hypertension, diabetes, obesity and hyperlipidaemia was higher in people with MAFLD. Furthermore, individuals with MAFLD exhibited reduced levels of physical activity in their daily lives. In conclusion, the non-MAFLD subjects exhibited higher OBS scores. The Venn plots (Fig. 3) demonstrated that the population with metabolically unhealthy MAFLD constituted the largest proportion of the total MAFLD population and exhibited overlap with both pre-diabetic and diabetic MAFLD populations, with the largest number of individuals overlapping with diabetic MAFLD. The second most prevalent subtype was pre-diabetic MAFLD, followed by diabetic MAFLD. The smallest number of individuals with metabolically healthy MAFLD was observed. However, it is noteworthy that seven of the metabolically healthy MAFLD population exhibited comorbid diabetes. The pie chart (Fig. 4) illustrates that between 2003 and 2018, the prevalence of MAFLD was 31%, with metabolically unhealthy MAFLD representing the largest proportion of MAFLDs from a Metabolic Syndrome perspective, at 98%. In terms of Type 2 Diabetes, the highest prevalence was observed in pre-diabetic MAFLD cases (38%), followed by diabetic 2 MAFLD (33%) and MAFLD without comorbid glucose metabolism disorders (29%).

Venn of 4 subtypes MAFLD: Metabolic unhealthy MAFLD; Metabolic healthy MAFLD; Pre-diabetic MAFLD; Diabetic MAFLD.

Pie chart: the proportion of MAFLD, Type 2 diabetic MAFLD and Metabolic Syndrome MAFLD, respectively.
The association between OBS and MAFLD
As shown in Table 2, the results of the weighted logistic regression analyses showed a negative correlation between the different OBSs and MAFLD. Total OBS of continuous variables was associated with MAFLD in fully adjusted model 3 (OR = 0.97, 95% CI 0.96–0.98; P < 0.001). In quartiles of OBS, the highest quartile demonstrated a more pronounced negative correlation with the risk of MAFLD compared to Q1 of OBS (OR = 0.60, 95% CI 0.50–0.72; P < 0.001). The third quartile of OBS was associated with a 25% reduction in the risk of MAFLD per unit increase in OBS, compared to the lowest quartile of OBS (OR = 0.75, 95% CI 0.61–0.92; P = 0.007). Secondly, a higher lifestyle OBS was found to be significantly associated with a reduced risk of MAFLD. In Model 3, each 1-unit increase in the continuous variable lifestyle OBS was associated with a 39.00% reduction in the risk of MAFLD (OR = 0.61, 95% CI 0.58–0.65; P < 0.001). In quartiles, Q4 LOBS demonstrated a more pronounced inverse correlation with MAFLD (OR = 0.10, 95% CI 0.07–0.12; P < 0.001)), reducing the risk of MAFLD by 90.00%. Q3 LOBS exhibited the capacity to diminish the likelihood of MAFLD by 56% (OR = 0.44, 95% CI 0.36–0.54; P < 0.001), and Q2 LOBS was also demonstrated to reduce the risk of MAFLD by 37% (OR = 0.63, 95% CI 0.51–0.77; P < 0.001). In the fully adjusted model 3, a negative association between continuous DOBS and MAFLD was observed (OR = 0.99, 95% CI 0.98–1.00; P = 0.022). However, after fully adjusting for covariates, no statistically significant association was found between DOBS and MAFLD in quartile DOBS.
Additionally, we calculated PAF to estimate the fraction of participants at risk for MAFLD that could be reduced by OBS. As shown in Table 2, we find that 13.58% of the MAFLD reduction comes from high OBS. MAFLD decreased by 12.67% and 8.00% when OBS was in Q4 and Q3, respectively. In addition, higher lifestyle OBS was able to reduce MAFLD by 53.84 percent. Of these, 54% were attributed to Q4 lifestyle OBS and 34.36% to Q3 lifestyle OBS. Even lifestyle OBS in Q2 reduced MAFLD by 14.68 percent.
Mediation analyses
Additionally, mediation analyses were performed to explore the possible mediating roles of inflammatory markers, insulin resistance, and BMI in the link between OBS and MAFLD. The analysis of mediation effects showed that METS-IR, NPAR and BMI mediated 90.60%, 25.10%, and 82.07% of the association, respectively (P < 0.001). (Fig. 5), (Supplemental Table 3).

Path diagram of the mediation analysis of METS-IR/NPAR/BMI on the relationship between OBS and MAFLD.
Restricted cubic spline analysis
We found a significant non-linear relationship between OBS and MAFLD using restricted cubic spline regression (P non-liner < 0.001, Fig. 6A). As OBS increased, the OR of MAFLD tended to decrease. The nonlinear relationship between MAFLD and OBS was also present in lifestyle OBS (P non-liner < 0.001, Fig. 6B). However, a linear relationship was not present in dietary OBS (P non-liner < 0.3820, Fig. 6C). Figure 6.B.C shows that lifestyle and dietary OBS, like overall OBS, showed an overall decreasing trend in the OR of MAFLD as LOBS and DOBS increased.

Restricted cubic spline regression analysis. Model adjusted for age, sex, race, exercise, diabetes, hypertension.
Cox risk proportional regression for OBS in patients with MAFLD
Correlations are presented in Table 3. For continuous OBS, there was a 3% reduction in all-cause mortality with OBS (OR = 0.97, 95% CI 0.94–1.00; P = 0.049). When OBS was the categorical variable, OBS appeared to have an ameliorating effect on all-cause mortality in Q3 (OR = 0.59, 95%CI 0.37–0.96; P = 0.032) and Q4 (OR = 0.51, 95%CI 0.27–0.98; P = 0.042) in Model 1. OBS had a statistically significant effect on the Q4 group in model 2. (OR = 0.49, 95% CI 0.26–0.95; P = 0.034). In the Q4 group in model3, however, the association between OBS and MAFLD disappeared (OR = 0.53, 95%CI 0.28–1.02; P = 0.056).
Discussion
Using the nationally representative NHANES 2003–2018 dataset, this research explored the OBS/MAFLD relationship. Our findings indicated that OBS exhibited a significant negative correlation with MAFLD in multivariate models, with a 40% reduction in MAFLD prevalence observed when OBS > 26. Furthermore, a 13.58% reduction in MAFLD could be attributed to higher levels of OBS (OBS > 21). In addition, the mediation analysis further suggested that METS-IR, NPAR, and BMI may mediate the association between OBS and MAFLD. The restricted cubic spline curves revealed a nonlinear relationship between OBS and MAFLD. Moreover, continuous OBS reduced all-cause mortality associated with MAFLD by approximately 3%.
We found that the higher OBS levels were significantly associated with a lower prevalence of MAFLD. Although the precise mechanism underlying the effect of OBS on MAFLD risk remains unclear, oxidative stress likely plays a pivotal role in this association. OBS is a composite measure of lifestyle and dietary factors that assesses an individual’s antioxidant status. ROS overload arises from an imbalance between ROS generation and antioxidant neutralization33. The widely accepted ‘multiple hits’ hypothesis explains the pathogenesis of MAFLD34, incorporating envirnmental factors (e.g. diet and sedentary behaviors). metabolic factors and genetic factors. These factors contribute to insulin resistance, visceral fat accumulation, and alterations in gut microbiota, ultimately leading to hepatic steatosis35. Hepatic fat accumulation induces mitochondrial and endoplasmic reticulum stress, resulting in high levels of ROS production, which may trigger inflammation, apoptosis, fibrosis and eventually hepatitis and liver fibrosis within the intrahepatic cells35. Recent studies have shown that MBOAT7 rs8736 (T) risk allele leads to excessive activation of the TLR signaling pathway in macrophages, increasing pro-inflammatory eicosanoid acid production and mitochondrial dysfunction through reduced gene expression, thereby exacerbating liver inflammation and metabolic imbalance36. This highlights the central role in of genetic variants in regulating the metabolic-epigenetic axis of immune cells in MAFLD pathogenesis. The RCS results confirmed that the risk of MAFLD decreases nonlinearly with increasing OBS levels. Furthermore, the protective effect of OBS on MAFLD is only observed when OBS exceeds 24. This is because OBS evaluates the combined effects of pro-oxidants and antioxidants, aligning with the oxidative stress mechanism where protection against MAFLD occurs only when the antioxidant response outweighs the pro-oxidant response. Consequently, modulating oxidative stress pathways represents a potential strategy to mitigate MAFLD.
The antioxidant lifestyle showed a robust association with MAFLD. Our study indicated that a continuous type of LOBS alone could reduce the likelihood of developing MAFLD by approximately 35%. Quartile LOBS analysis revealed that Q4, Q3, and Q2 LOBS reduced MAFLD prevalence by 90%, 56%, and 37%, respectively. By calculating the PAF of LOBS, we determined that approximately 53.84% of the reduction in MAFLD prevalence could be attributable to LOBS. As LOBS increased from Q2 to Q4, the percentage of MAFLD prevalence reduction attributable to lifestyle OBS rose incrementally by 14.68%, 34.36%, and 54.00%, respectively. Physical activity, well-known for its benefits, has been shown to significantly improve MAFLD. Multiple cross-sectional studies have demonstrated that physical activity is associated with MAFLD and mediates the relationship between HOMA-IR and MAFLD. One cross-sectional study reported that approximately 25% of the reduction in MAFLD prevalence could be attributed to physical activity37. This is because appropriate physical activity reduces obesity, promotes triglyceride metabolism, and improves insulin resistance38. Such physical activities include high-intensity interval training, moderate-to-high intensity training, and aerobic exercise39. We conducted a mediation analysis to explore the mechanisms by which OBS reduces MAFLD. The findings suggested that OBS may reduce MAFLD by improving METS-IR, inflammatory markers (NPAR), and BMI, consistent with evidence from prior studies.
There is also evidence that physical activity enhances mitochondrial function, including mitochondrial biogenesis and autophagy, reducing MAFLD activity and affecting oncogenic signaling pathways40. Experiments in mice revealed that regularly exercised mice exhibited lower plasma levels of biochemical markers indicative of liver disease, such as ALT and AST, compared to sedentary mice40. Previous studies indicated that even low levels of alcohol intake were harmful to the liver in individuals with MAFLD43. Smoking may also contribute to the development of MAFLD44. Meta-analyses of multiple cohort studies provided evidence that obesity was an independent risk factor for MAFLD and that increasing BMI was associated with a significant dose–response effect on MAFLD risk45. In summary, reducing the incidence of MAFLD in populations through lifestyle improvements is crucial.
We found that continuous DOBS reduced the prevalence of MAFLD by approximately 1%. Antioxidant dietary practices and dietary antioxidants have been shown to improve MAFLD in various studies. Vitamin C, as an antioxidant46 has been demonstrated to lower MAFLD incidence in males and individuals with excess weight47. This aligns with our study results (Supplemental Table 2), which revealed a significant difference in vitamin C intake between MAFLD and non-MAFLD patients at baseline50. In mouse models, vitamin C has been linked to improv MAFLD and hepatitis prevention51. Similarly, vitamins D and E have shown varying degrees of efficacy in improving MAFLD53. Furthermore, we should emphasize the comprehensive role of diet in managing MAFLD. A large cross-sectional study demonstrated that higher levels of CDAI were associated with a reduced risk of MAFLD, with 4.8% of this reduction attributed to elevated dietary antioxidant levels37. Both cross-sectional and cohort studies have identified the Mediterranean diet and low-inflammatory diets as potential interventions for MAFLD55. The Mediterranean diet is characterized by lower consumption of red meat (saturated fat) and an emphasis on dietary fiber, fresh fruits and vegetables57. This diet typically contains antioxidants, including vitamins, and rich in monounsaturated fats, which protect against MAFLD58. Additionally, the Mediterranean diet enhances insulin sensitivity and reduces adipose tissue. One study found that adherence to Mediterranean diet improved insulin resistance in individuals with MAFLD, even in the absence of weight loss59. Our study revealed significant differences in saturated fat consumption between patients without and with MAFLD, with those with MAFLD tending to consume more fat (Supplemental Table 2). Therefore, the role of dietary factors in improving MAFLD cannot be overlooked.
Cultural and socioeconomic influences on dietary choices significantly impact OBS. For example, diets rich in plant-based foods, such as the Mediterranean diet58 and the East Asian diet60, are associated with higher antioxidant intake62. In contrast, Westernized diets, predominantly composed of processed foods, may increase exposure to pro-oxidants63. Furthermore, socioeconomic disparities exacerbate these effects; individuals with lower income or education levels often choose more affordable, energy-dense, pro-oxidant processed foods64.
We conducted a Cox proportional hazards regression analysis in patients with MAFLD, revealing that continuous OBS was associated with a 3% reduction in all-cause mortality. This finding aligns with previous research indicating that higher OBS in MAFLD populations reduces all-cause mortality25. However, further exploration is warranted. This study also categorizes MAFLD into different subtypes. No significant differences were observed in their OBS scores at baseline (Supplemental Tables 4 and 5). In a prior study of MAFLD with T2DM, MAFLD with T2DM was associated with a higher risk of all-cause and cardiac-specific mortality compared to than metabolically healthy MAFLD, followed by MAFLD with Pre-D and metabolically unhealthy MAFLD65. Some studies have shown that metabolic healthy MAFLD has a significantly lower risk of atherosclerotic cardiovascular disease compared to metabolic unhealthy MAFLD66. Moreover, in a cross-sectional study, diabetic MAFLD patients exhibited higher all-cause mortality than overweight or obese MAFLD patients67. We found no significant difference in OBS scores among subtypes, suggesting that OBS exerts a consistent ameliorative effect across different MAFLD subtypes. Beyond these subtypes, lean MAFLD is a prevalent variant68. Its prognosis may be relatively more favorable compared to obese MAFLD69. It has been proposed that the onset of lean MAFLD may result from a decline in metabolic fitness driven by endotoxemia70. Compared to non-lean patients, those with a healthy weight (lean) displayed more advantageous metabolic and histological profiles71. Paradoxically, they experienced a higher overall mortality rate71. The underlying pathophysiology of this paradox remains unclear and requires further investigation.
This study possesses several strengths. Firstly, we utilized a complex multi-stage probability sampling technique to ensure that the sample size derived from the NHANES database was sufficiently large to accurately represent the non-institutionalized population, thereby enhancing the study’s generalizability. Secondly, the OBS, a composite score integrating dietary and lifestyle components, was employed to assess individual antioxidant status. Thirdly, mediation analysis was conducted to explore the mechanisms linking OBS and MAFLD. Nevertheless, this study has certain limitations. Initially, the assessment of dietary composition and physical activity relied on self-reported questionnaires, which may introduce recall bias and social desirability bias. Participants might underreport unhealthy behaviors (e.g., high-fat diet) or overestimate their exercise frequency, potentially leading to an underestimation of the true association between lifestyle factors and MAFLD. Secondly, residual and unmeasured confounders might have biased the analysis. Although this study adopted the MAFLD framework, we recognize that the consensus on MASLD continues to evolve. MASLD simplifies the diagnostic criteria, a shift that may enhance clinical utility. Future studies could utilize longitudinal data to verify whether our findings can be generalized to the MASLD population. Finally, our mediation in the cross-sectional study design posed challenges for inferring causality. Considering the constraints of this study, the results should be approached carefully, and further research is required to validate our conclusions.
Future studies should incorporate biomarker-based measurements, such as lipid peroxidation markers and antioxidant enzyme activity, to complement self-reported OBS data, thereby enhancing the accuracy of oxidative stress evaluations. Our findings suggest that lifestyle modifications, particularly physical activity, may be more effective than dietary adjustments in managing MAFLD. Further research is needed to identify optimal intervention types, such as aerobic exercise protocols. Prospective cohort studies with repeated OBS assessments are necessary to confirm the temporal relationship between oxidative balance and MAFLD progression, while also exploring causal mechanisms through mediation analysis. Although this study establishes an association between OBS and MAFLD, additional research is required to address residual confounding factors to refine clinical translation strategies.
Conclusion
Our study demonstrates a significant inverse association between oxidative balance score and metabolic-associated fatty liver disease. An antioxidant lifestyle may be more important than an antioxidant diet in preventing MAFLD. Furthermore, our findings suggest that insulin resistance, inflammatory factors, and BMI may play a mediating role in the relationship between OBS and MAFLD. Elevating bodily antioxidant concentrations could thus prove an effective strategy for healthcare providers to mitigate MAFLD’s prevalence and impact. However, future experimental studies are needed to confirm this association and to elucidate the mechanisms behind it.
Data availability
The data that support the findings of this study are openly available in Https://www.cdc.gov/nchs/nhanes/. Information from NHANES is made available through an extensive series of publications and articles in scientific and technical journals.
References
Araújo, A. R., Rosso, N., Bedogni, G., Tiribelli, C. & Bellentani, S. Global epidemiology of non-alcoholic fatty liver disease/non-alcoholic steatohepatitis: What we need in the future. Liver Int. 38(S1), 47–51 (2018).
Chen, K. et al. Advancing the understanding of NAFLD to hepatocellular carcinoma development: From experimental models to humans. Biochim. Biophys. Acta Rev. Cancer 1871(1), 117–125 (2019).
Younossi, Z. M. et al. The economic and clinical burden of nonalcoholic fatty liver disease in the United States and Europe. Hepatology 64(5), 1577–1586 (2016).
Grant, B. F. Barriers to alcoholism treatment: Reasons for not seeking treatment in a general population sample. J. Stud. Alcohol. 58(4), 365–371 (1997).
Nah, B. K. Y. et al. Historical changes in weight classes and the influence of nafld prevalence: A population analysis of 34,486 individuals. Int. J. Environ. Res. Public Health 19(16), 9935 (2022).
Eslam, M. et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 73(1), 202–209 (2020).
Tilg, H. & Effenberger, M. From NAFLD to MAFLD: When pathophysiology succeeds. Nat. Rev. Gastroenterol. Hepatol. 17(7), 387–388 (2020).
Pan, Z. et al. MAFLD criteria are better than MASLD criteria at predicting the risk of chronic kidney disease. Ann. Hepatol. 29(5), 101512 (2024).
Pan, Z., Shiha, G., Esmat, G., Méndez-Sánchez, N. & Eslam, M. MAFLD predicts cardiovascular disease risk better than MASLD. Liver Int. 44(7), 1567–1574 (2024).
Loomba, R., Friedman, S. L. & Shulman, G. I. Mechanisms and disease consequences of nonalcoholic fatty liver disease. Cell 184(10), 2537–2564 (2021).
Tian, T. et al. Dietary quality and relationships with metabolic dysfunction-associated fatty liver disease (MAFLD) among United States Adults, results from NHANES 2017–2018. Nutrients 14(21), 4505 (2022).
Wang, X., Zhang, W., Huang, J., Li, H. & Gao, J. The relationship between vitamin K and metabolic dysfunction-associated fatty liver disease among the United States population: National Health and Nutrition Examination Survey 2017–2018. Front. Nutr. 14(10), 1086477 (2023).
Yu, J. & Guo, P. Association between dietary intake of carotenoids and metabolic dysfunction-associated fatty liver disease in US adults: National Health and Nutrition Examination Survey 2017–March 2020. Public Health Nutr. 27(1), e168 (2024).
Tong, J. et al. Association between flavonoid and subclasses intake and metabolic associated fatty liver disease in U.S. adults: Results from National Health and Nutrition Examination Survey 2017–2018. Front. Nutr. 9, 1074494 (2022).
Yang, J. et al. Short sleep duration and the risk of nonalcoholic fatty liver disease/metabolic associated fatty liver disease: A systematic review and meta-analysis. Sleep Breath 27(5), 1985–1996 (2023).
Peng, H. et al. METS-IR/HOMA-IR and MAFLD in US adults: Dose–response correlation and the effect mediated by physical activity. BMC Endocr. Disord. 24(1), 132 (2024).
Meydani, M. Dietary antioxidants modulation of aging and immune-endothelial cell interaction. Mech. Ageing Dev. 111(2–3), 123–132 (1999).
Goodman, M., Bostick, R. M., Dash, C., Flanders, W. D. & Mandel, J. S. Hypothesis: Oxidative stress score as a combined measure of pro-oxidant and antioxidant exposures. Ann. Epidemiol. 17(5), 394–399 (2007).
Zhang, W. et al. Association between the oxidative balance score and telomere length from the National Health and Nutrition Examination Survey 1999–2002. Oxidat. Med. Cell. Longev. 2022, 1–11 (2022).
Son, D. H., Lee, H. S., Seol, S. Y., Lee, Y. J. & Lee, J. H. Association between the oxidative balance score and incident chronic kidney disease in adults. Antioxidants 12(2), 335 (2023).
Chen, K. et al. Association between oxidative balance score, systemic inflammatory response index, and cardiovascular disease risk: A cross-sectional analysis based on NHANES 2007–2018 data. Front. Nutr. 5(11), 1374992 (2024).
Lu, Y., Wang, M., Bao, J., Chen, D. & Jiang, H. Association between oxidative balance score and metabolic syndrome and its components in US adults: A cross-sectional study from NHANES 2011–2018. Front. Nutr. 13(11), 1375060 (2024).
Liu, X. et al. Higher oxidative balance scores are associated with lower nonalcoholic fatty liver disease and not with fibrosis in US adults. Nutr. Metab. Cardiovasc. Dis. 33(12), 2488–2496 (2023).
Liu, Y. & Chen, M. Dietary and lifestyle oxidative balance scores are independently and jointly associated with nonalcoholic fatty liver disease: A 20 years nationally representative cross-sectional study. Front. Nutr. 18(10), 1276940 (2023).
Peng, L., Li, L., Liu, J. & Li, Y. New insights into metabolic dysfunction-associated steatotic liver disease and oxidative balance score. Front. Nutr. 5(10), 1320238 (2024).
Lei, X., Xu, Z. & Chen, W. Association of oxidative balance score with sleep quality: NHANES 2007–2014. J. Affect. Disord. 339, 435–442 (2023).
Son, D. H., Lee, H. S., Lee, Y. J., Lee, J. H. & Han, J. H. Comparison of triglyceride-glucose index and HOMA-IR for predicting prevalence and incidence of metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 32(3), 596–604 (2022).
Tian, T. et al. Dietary quality and relationships with metabolic dysfunction-associated fatty liver disease (MAFLD) among United States Adults, results from NHANES 2017–2018. Nutrients 14(21), 4505 (2022).
Ruhl, C. E. & Everhart, J. E. Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey. Aliment Pharmacol. Ther. 41(1), 65–76 (2015).
Xu, F., Earp, J. E., Adami, A., Weidauer, L. & Greene, G. W. The relationship of physical activity and dietary quality and diabetes prevalence in US adults: Findings from NHANES 2011–2018. Nutrients 14(16), 3324 (2022).
Cheng, H. et al. Association between METS-IR and prediabetes or Type 2 diabetes mellitus among elderly subjects in China: A large-scale population-based study. IJERPH. 20(2), 1053 (2023).
Wang, L., Liu, L., Liu, X. & Yang, L. The association between neutrophil percentage-to-albumin ratio (NPAR) and depression among US adults: A cross-sectional study. Sci. Rep. 14(1), 21880 (2024).
Chen, Z., Tian, R., She, Z., Cai, J. & Li, H. Role of oxidative stress in the pathogenesis of nonalcoholic fatty liver disease. Free Radical Biol. Med. 152, 116–141 (2020).
Fang, Y. L., Chen, H., Wang, C. L. & Liang, L. Pathogenesis of non-alcoholic fatty liver disease in children and adolescence: From “two hit theory” to “multiple hit model”. WJG. 24(27), 2974–2983 (2018).
Buzzetti, E., Pinzani, M. & Tsochatzis, E. A. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism 65(8), 1038–1048 (2016).
Alharthi, J. et al. A metabolic associated fatty liver disease risk variant in MBOAT7 regulates toll like receptor induced outcomes. Nat. Commun. 6(13), 7430 (2022).
Gao, L. et al. Synergistic impact of composite dietary antioxidant index and physical activity on fatty liver disease. Front. Nutr. 5(11), 1486700 (2024).
Lin, X. et al. Effects of exercise training on cardiorespiratory fitness and biomarkers of cardiometabolic health: A systematic review and meta-analysis of randomized controlled trials. JAHA. 4(7), e002014 (2015).
Rinella, M. E. Nonalcoholic fatty liver disease: A systematic review. JAMA 313(22), 2263 (2015).
Guarino, M. et al. Exercise attenuates the transition from fatty liver to steatohepatitis and reduces tumor formation in mice. Cancers 12(6), 1407 (2020).
Longo, M., Meroni, M., Paolini, E., Macchi, C. & Dongiovanni, P. Mitochondrial dynamics and nonalcoholic fatty liver disease (NAFLD): New perspectives for a fairy-tale ending?. Metabolism 117, 154708 (2021).
Saran, U. et al. Anti-tumoral effects of exercise on hepatocellular carcinoma growth. Hepatol. Commun. 2(5), 607–620 (2018).
Jarvis, H. et al. Does moderate alcohol consumption accelerate the progression of liver disease in NAFLD? A systematic review and narrative synthesis. BMJ Open 12(1), e049767 (2022).
Jung, H. S. et al. Smoking and the risk of non-alcoholic fatty liver disease: A cohort study. Am. J. Gastroenterol. 114(3), 453–463 (2019).
Li, L. et al. Obesity is an independent risk factor for non-alcoholic fatty liver disease: Evidence from a meta-analysis of 21 cohort studies. Obes. Rev. 17(6), 510–519 (2016).
Abe RAM, Masroor A, Khorochkov A, Prieto J, Singh KB, Nnadozie MC, et al. The role of vitamins in non-alcoholic fatty liver disease: A systematic review. Cureus (2021). Available from: https://www.cureus.com/articles/63283-the-role-of-vitamins-in-non-alcoholic-fatty-liver-disease-a-systematic-review
Liu, X. H. et al. Potassium affects the association between dietary intake of vitamin C and NAFLD among adults in the United States. PLoS ONE 19(4), e0295986 (2024).
Xie, Z. Q. et al. Association of serum vitamin C With NAFLD and MAFLD among adults in the United States. Front Nutr. 4(8), 795391 (2022).
Wei, J. et al. Association between dietary vitamin C intake and non-alcoholic fatty liver disease: A cross-sectional study among middle-aged and older adults. PLoS ONE 11(1), e0147985 (2016).
Zhao, Y. et al. Mitochondrial dysfunction in metabolic dysfunction fatty liver disease (MAFLD). IJMS. 24(24), 17514 (2023).
Lee, S. W. et al. Mega-dose vitamin C ameliorates nonalcoholic fatty liver disease in a mouse fast-food diet model. Nutrients 14(11), 2195 (2022).
Zeng, Q. et al. Prophylactic and therapeutic effects of different doses of vitamin C on high-fat-diet-induced non-alcoholic fatty liver disease in mice. Biomed. Pharmacother. 131, 110792 (2020).
Qi, X. et al. Vitamin E intake is inversely associated with NAFLD measured by liver ultrasound transient elastography. Sci. Rep. 14(1), 2592 (2024).
Liu, S. et al. Association between vitamin D status and non-alcoholic fatty liver disease: A population-based study. J. Nutr. Sci. Vitaminol. 65(4), 303–308 (2019).
Doustmohammadian, A. et al. Favorable association between Mediterranean diet (MeD) and DASH with NAFLD among Iranian adults of the Amol cohort study (AmolCS). Sci. Rep. 12(1), 2131 (2022).
Tian, T. et al. Dietary quality and relationships with metabolic dysfunction-associated fatty liver disease (MAFLD) among United States adults, results from NHANES 2017–2018. Nutrients 14(21), 4505 (2022).
Guasch-Ferré, M. & Willett, W. C. The Mediterranean diet and health: a comprehensive overview. J. Intern. Med. 290(3), 549–566 (2021).
Gosal, H., Kaur, H., Chakwop Ngassa, H., Elmenawi, K. A., Anil, V. & Mohammed, L. The significance of the mediterranean diet in the management of non-alcoholic fatty liver disease: A systematic review. Cureus (2021). Available from: Https://www.cureus.com/articles/59985-the-significance-of-the-mediterranean-diet-in-the-management-of-non-alcoholic-fatty-liver-disease-a-systematic-review
Ryan, M. C. et al. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 59(1), 138–143 (2013).
Kim, J., Kim, H. & Giovannucci, E. L. Plant-based diet quality and the risk of total and disease-specific mortality: A population-based prospective study. Clin. Nutr. 40(12), 5718–5725 (2021).
Yuan, Y. Q. et al. The development of a Chinese healthy eating index and its application in the general population. Nutrients 9(9), 977 (2017).
Aleksandrova, K., Koelman, L. & Rodrigues, C. E. Dietary patterns and biomarkers of oxidative stress and inflammation: A systematic review of observational and intervention studies. Redox Biol. 1(42), 101869 (2021).
Kopp, W. How western diet and lifestyle drive the pandemic of obesity and civilization diseases. DMSO 24(12), 2221–2236 (2019).
Hosseinpour-Niazi, S. et al. The association between ultra-processed food consumption and health-related quality of life differs across lifestyle and socioeconomic strata. BMC Public Health 24(1), 1955 (2024).
Golabi, P. et al. Nonalcoholic fatty liver disease (NAFLD) and associated mortality in individuals with type 2 diabetes, pre-diabetes, metabolically unhealthy, and metabolically healthy individuals in the United States. Metabolism 146, 155642 (2023).
Park, H. et al. Nomenclature dilemma of metabolic associated fatty liver disease (MAFLD): Considerable proportions of MAFLD are metabolic healthy. Clin. Gastroenterol. Hepatol. 21(4), 1041–1049 (2023).
Chung, G. E. et al. Lean or diabetic subtypes predict increased all-cause and disease-specific mortality in metabolic-associated fatty liver disease. BMC Med. 21(1), 4 (2023).
Pan, Z. et al. MAFLD: An ideal framework for understanding disease phenotype in individuals of normal weight. Ther. Adv. Endocrinol. Metab. 27(15), 20420188241252544 (2024).
Eslam, M. et al. Metabolic (dysfunction)-associated fatty liver disease in individuals of normal weight. Nat. Rev. Gastroenterol. Hepatol. 19(10), 638–651 (2022).
Alharthi, J. et al. Loss of metabolic adaptation in lean MAFLD is driven by endotoxemia leading to epigenetic reprogramming. Metabolism 1(144), 155583 (2023).
Alarabi, M., Pan, Z., Romero-Gómez, M., George, J. & Eslam, M. Telomere length and mortality in lean MAFLD: The other face of metabolic adaptation. Hepatol. Int. 18(5), 1448–1458 (2024).
Acknowledgements
Expressions of gratitude are extended to the National Center for Health Statistics (NCHS), a division of the Centers for Disease Control (CDC) and Prevention. Furthermore, sincere appreciation is conveyed to all participants who have enrolled in the National Health and Nutrition Examination Survey. At the same time, I would like to thank Professor Jin Lina of the School of Public Health, Jilin University, for helping to guide the methodology used, and the funding from Jilin Province’s Science and Technology Department (Grant No. 20240601018RC).
Funding
This study received funding from Jilin Provincial Scientific and Technological Development Program (Grant No. 20240601018RC) .
Author information
Authors and Affiliations
Contributions
Conceptualization: Linyin Huang, Data curation: Linyin Huang, Formal analysis: Linyin Huang, Shifang Qu, Xinyu Cui, Yujin Jin, Yan Yao Funding acquisition: Yan Yao Methodology: Linyin Huang, Xinyu Cui, Yujin Jin, Shifang Qu Project administration: Linyin Huang, Yan Yao . Visualization: Linyin Huang Writing–original draft: Linyin Huang Writing–review & editing: Linyin Huang, Shifang Qu, Xinyu Cui, Yujin Jin, Yan Yao.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
All NHANES protocols were approved by the National Center for Health Statistics’ Research Ethics Review Board, all participants signed a consent form before their participations and all research was performed in accordance with relevant guidelines/regulations. The statement of informed consent is openly available in Https://www.cdc.gov/nchs/nhanes/biospecimens/participants.htm.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, L., Qu, S., Cui, X. et al. Association between oxidative stress and metabolic-associated fatty liver disease in the US population. Sci Rep 15, 21352 (2025). https://doi.org/10.1038/s41598-025-05044-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-05044-7
