
Abstract
Post Kala-azar Dermal Leishmaniasis (PKDL) is a complication of Visceral Leishmaniasis (VL) and acts as a reservoir for Leishmania parasites. With climatic changes and ozone depletion increasing ultraviolet radiation (UVR), we investigated the connection between UVR and PKDL development. We have measured sun-light UVR intensities by UV light meters and satellite-based methods. Our data showed a concerning increase in the UV index (> 12.0–14.5) during summer and pre-monsoon season. A cohort of 283 PKDL patients revealed a strong correlation between prolonged sun-light (UVR) exposure (4–8 h/day) and worsening skin lesions, with many patients, particularly labourers and farm workers, reporting sunburn and/or irritation, skin sensitivity. Additionally, in vitro studies with human THP-1 cells showed UVB-induced cytotoxicity and immuno-suppression, that likely to be associated with PKDL development. Serum analysis showed significant alterations in key cytokines concentrations (IL-10, IL-12), IFN-γR and Vitamin-D, iron level among PKDL and VL patients versus healthy controls. Specifically, PKDL patients exhibited upregulated expressions of TLRs-2/4 and TNFR-2, but down-regulation of TNFR-1 were observed in PKDL patients than the healthy controls. In essence, our findings implicate the risk posed by increasing sunlight UVR exposure for PKDL development in vulnerable populations from VL endemic regions of Bihar.
Similar content being viewed by others

Introduction
Visceral Leishmaniasis (VL) is caused by the digenetic protozoan parasite Leishmania donovani that mainly prevails as Kala-Azar or VL and Post Kala-azar Dermal Leishmaniasis (PKDL); where 50,000–90,000 new VL cases occur per year world wide as per WHO report 2023 (https://www.who.int/news-room/fact-sheets/detail/leishmaniasis). However in India, VL disease burden was very high in 2014–15 around 10, 000, which is going down every year, due to the strong efforts taken under the National Kala-Azar Elimination Programme (NKEP), but the number of PKDL cases was increased five-fold (from 421 to 1982 cases) from 2014 to 2017 as per NVBDCP (National Vector Borne Disease Control Programme, now known as National Center for Vector Borne Diseases Control, NCVBDC), Govt. of India data (https://ncvbdc.mohfw.gov.in/index.php). It is well known that Bihar and Jharkhand have contributed around 80–90% and 70–80% of total VL and PKDL burden, respectively in India1,2,3. In addition, the people’s poor quality of lives and/or low socio-economic conditions, public unawareness4, delay in seeking medical consultation5,6, undesirable gaps in the treatment stages and emergence of drug resistance7; are considered as some other reasons to alleviate the prevalence and/or incidence of VL/PKDL in Bihar. Although the fatal form of disease i.e. VL is decreasing due to the integrated efforts started a decade ago; but there are still more prevalence and/or incidences of PKDL cases in Bihar. The eastern Indian state Bihar has been the epicentre of L. donovani infections in the country, probably due to high sand fly vector P. argentipes density8,9 and their mysterious transmission dynamics in the community10. The NKEP has achieved the goal of VL elimination11,12 in Bihar only, but major challenges are to sustain it for at least next five years due to the factors like co-infection (VL-HIV, VL-TB), PKDL and asymptomatic cases including vector density.
The skin lesions (macules, papules or nodules of the PKDL patients) usually appear on the sun exposed body parts; and these lesions act apparently as L. donovani reservoirs in the skin12,13,14,15. However, the linkage of leishmaniasis prevalent countries receiving more amount of intense sun light per annum reveals more occurrences of PKDL cases in those regions. For example, African countries that are present near to the equator, like Ethiopia and Sudan usually receive higher amount of intense sunlight as compared to the Indian subcontinent; which is present near the tropical region that gets comparatively less intensity of sunlight. In Sudan, the incidence of PKDL is significantly higher (~ 50%) than in India (~ 10%; 4.4/10,000 population)10,16. This observation suggests a possible link between intense sunlight (UVR) exposure and PKDL prevalence, including other contributing factors, treatment regimens, host-susceptibility, effector memory T-cells17. The intense sunlight refers to the daytime light from the sun which possesses harmful UV radiations. However, UV index > 8 is harmful and it should be avoided for health protection as per WHO guidelines. Reports reveal that intense sun light possesses harmful ultraviolet radiations (UVR), which increases significantly with the gradual depletion of the protective ozone columns in the tropospheric atmosphere18,19. The solar UVR is known to be detrimental for skin health20 as more UVB radiations exert mutagenic or carcinogenic impacts leading to the alteration in dermal tissue structure21 and affects the components of skin immunology22. The UV rays of electromagnetic light (280–320 nm) from solar source is known as photo-carcinogenic in nature in Australia and New Zealand (equatorial countries)23,24; and also linked to damage the skin tissue. Although some melanoma and non-melanoma skin cancer cases are well-reported earlier in Australian regions23,25, the use of sunscreen formulations are promoted to prevent UV radiation-induced skin problems.
Now-a-days, climate-induced changes in local weather are one of the posing concerns for human health21 and the impact of climate changes also enhance the spread of certain disease causing pathogens. As climate change is known to have a variety of effects on human health26, in this context, enhanced ultraviolet (UV) radiations exposure due to changes in atmospheric conditions may be a contributing factor in the emergence of PKDL among populations previously treated for VL, in endemic regions17. As the increasing temperatures have been linked to enhance the incidence of heat related mortality27; the role of increased penetration of sunlight (UVR) in influencing the PKDL development among prolonged sunlight exposed VL-affected populations in Bihar needs further investigation. The occurrence of dermal lesions predominantly on sun light exposed body parts in PKDL patients raises the possibility that UV radiation may likely contribute to the disease pathogenesis14. However, the precise role of sunlight (UV) exposure in initiating PKDL lesions remains still unclear and requires further investigation.
Although, the impact on human health often cited as the consequences of climate changes remain less intuitive, predictable and indirect in nature; still the evidences of diseases of bacterial (Cholera28, Salmonellosis29), viral (Swine flu, infuenza etc.)30 and/or vectors origins like (Malaria31, Chikungunya, Dengue fevers32 etc.) take place as out-break usually after the episodes of climate changes33,34,35.
Moreover, the harmful UV light is reported to induce immuno-suppression either through its chromophore cis-urocanic acid36 or via the modulation of vitamin D337,38. Under the process of keratinisation, the transurocanic acid produced from histidine is known to undergo UV-induced photo-isomerisation to become cis-urocanic acid39,40. After sufficient UVR absorption in the skin, the conversion of the cis-urocanic acid to trans-urocanic acid is inhibited41,42 that results into the reduced expression of major histocompatibility complex (MHC) class II43, along with a loss of co-stimulatory molecules, CD80 and CD86, which translates into impaired antigen presentation44,45. The after maths of such photoreactions in skin also alters a vast array of cytokines. In the meantime, solar UV light is absorbed by the 7-Dehydrocholesterol, also known as pro-vitamin D46. In body, it enhances the synthesis of vitamin D3 that in turn, binds to vitamin D-binding protein (DBP) and subsequently enters into monocytes and macrophages. Inside cells, vitamin D3 is hydroxylated to 1α-25(OH)2D3 by the catalysis of mitochondrial enzyme CYP27B1, and forms a complex with vitamin D receptor (VDR), which leads to the induced synthesis of antibacterial peptides and immuno-modulatory factors, such as cathelicidin47,48. On the one hand, it inhibits Toll-like receptor (TLR)-induced activation of macrophages and forms the basis of immuno-suppression; and on the other hand, it also causes ultimate changes in the key cytokines trafficking in a cascade of mechanisms, which involve in appropriate immune regulations (Th1–Th2) balance for the host protection49,50,51. Past reports revealed that the Leishmania parasites either from the infected sand fly or after the apparent treatment of Kala-azar undergo strategic stress by-passing mechanism and show skin homing behaviour leading to lesions development. The persistence of live parasites in the skin, probably due to the Th2 immune modulated milieu, may cause further spread of the disease both in the hosts and in the community.
However, there is no ample information so far about the evidences of sunlight UVB radiations associated PKDL development conditions in the VL endemic population in the Bihar (Indian subcontinent regions).
We mentioned earlier that the ozone layer is continuously depleting from the stratospheric atmosphere and the UV rays penetration is increased in the ground surface. This may have a correlation with the increasing incidence of PKDL cases in Kala-azar endemic regions in Bihar, India. Thus, the present study provides important outcomes (insights) to understand the mechanism of PKDL pathogenesis, as we have evaluated the possible role of sunlight (UVR) from the solar source among the PKDL patients from the VL endemic regions in Bihar; and the association of prolonged exposure of intense sunlight with the disease prevalence has been explored in various occupational categories of these patients. Our study demonstrates the contributory role of sunlight (UVR) in the increased cases of PKDL, especially in intense sunlight exposed populations such as labourers, farmers. The mechanism of PKDL pathogenesis is mediated by immune mediators like pattern recognition receptors (TLRs) especially TLR2/4; and altered cytokines IL-10, IL-12, IFN-γR, TNF-R2, and vitamin-D level. This study will help to strategize the development of an early awareness or warning of PKDL progression and/or giving them advise or sunlight protective cream or therapeutics in VL endemic vulnerable populations in Bihar to control PKDL.
Materials and methods
Human ethics committee approval
This study was conducted in compliance with the guidelines of the Human Ethics Committee protocol of ICMR, INDIA52,53 and was approved (EC No. 19/RMRI/EC/2017) by the Institutional Ethics Committee of ICMR-Rajendra Memorial Research Institute of Medical Sciences, Patna, India as per code of ethics (Declaration of Helsinki)54. All the participants and /or their legal guardians were interviewed face-to-face, explained about the research objectives and overall methodology and then written informed consents were taken as per defined protocol of ICMR-National Ethical Guidelines for Biomedical and Health Research Involving Human Participants54 at the time of their enrolments under this study.
Selection of VL endemic study sites in Bihar
The populations that belong to the VL endemic regions of Bihar were selected for the present study. Although the active number of VL cases is decreasing, still there are high chances of getting PKDL patients, mostly due to the past history of Kala-azar. So two districts particularly, Vaishali (26.125° N, 85.125° E) and Saran (25.875° N, 85.875° E) including their entire blocks (N = 36) regions; were chosen as the sites for study. As a VL non-endemic area, Patna (25.625° N, 85.125° E) district was also taken for comparison (5 blocks selected), in compliance to the EC suggestions. Under the study districts, all the blocks areas such as gram panchayats and villages reported with any VL/PKDL cases or incidence were actively visited55 at least thrice per season in a year as field trips; after establishing the essential coordination with all the health stake-holders like ASHAs/AWWs56, Care/KTS staff, medical officers in-charge, block/community health managers, other volunteers57 for locating the patient’s houses.
Measurement of sunlight UV intensity
The ground level UV radiation was measured by using portable scientific UV meters (Lutron, Taiwan) as described previously58,59,60. Briefly, the probe of the UV meters was shown to the sun (in the sky) overhead in such a way that sun-probe-eyes remain in a straight line direction. For measurement of low and high intensity of sunlight UV radiations, two ranges (low and high) of recording modes were used to take solar (UVR) readings by the UV meters up to 2000 µW/cm2 and 20,000 µW/cm2 as outlined in the flow diagram along with other methodology (Fig. 2S). The UVA and UVB types of radiations were recorded each day round the year at selected/nodal places in the study sites at pre-selected central places. The sky and weather conditions (clear or cloudy or otherwise) were also taken into account61, while recording the sunlight UV radiations data.
Satellite-based sunlight UVR monitoring
The incoming UV radiation (UVR) from the sun light is worth monitoring by using weather satellites62 with advanced software packages from Tropospheric Emission Monitoring Internet Service (TEMIS), KNMI, Netherlands using SCIAMACHY and GOME 2.0. The UVR data products like UV index, UV dose (kJ/m2), Vitamin-D UV doses (kJ/m2), doses for DNA damage etc. are accessible each day of a year, across different season’s viz. summer, pre-monsoon, monsoon and winter months (Fig. 2S). The satellite-based study of the study regions is based on the latitude and longitude (geographical coordinates, as shown in the Table 1). The coordinates of TEMIS were used after comparing the same from different sources such as NASA and Govt. of India website. The European Space Agency (ESA)/TEMIS team has extended this facility of satellite-based ultraviolet radiation monitoring of our study region in three formats: daily UV data, mapping and overpass file. The daily UV data (intensity) was recorded every day round the year during the study duration (3 years) from June 2017 to December 2020; while the overpass file and map data was obtained from TEMIS/ESA continuously. Briefly, the validation of sunlight UVR data was carried out from the patient’s study site; and the daily weather reports of the study sites were regularly recorded (apart from the information of Indian Meteorological Department/IMD). The comparison of manual measurement and satellite-based data of sunlight UVR helped63 to ascertain a trend of increasing UV rays from the sun. The comparative UVR data of TEMIS/KNMI and ground level UV radiations is measured every day, but represented as monthly mean values of sunlight UV rays intensity and doses (kJ/m2) at the solar noon time.
Study participants and sample size
The sample size of PKDL patients was determined in this study using the Raosoft Inc. sample size calculator http://www.raosoft.com/samplesize.html (USA). The power of calculation was taken as 80%; along with a desired margin of error 5% and a confidence level of 95%. Accounting a response distribution of 50% and a selected population size of 5000 from the listed block areas of study sites, the recommended sample size was calculated to be 357 individuals, but the sample size of PKDL patients was finally taken as 358, distributed across different categories (shown in Fig. 3S). In this study, 358 PKDL patients were screened initially, but 307 of them could be recruited, because 32 patients did not provide the required information in the structured questionnaire and 19 PKDL patients were found under the exclusion criteria of co-morbidity or unwillingness to participate in this study as per EC guidelines. Thereafter, 24 recruited patients either left or lost essential contact with our study team during the course of study. Thus, the number of PKDL patients were participated in the present work was 283 at final stage. Besides, we have taken 30 VL patients as control group, along with 45 healthy persons in this study, comprising from both endemic (n = 25) and non-endemic (n = 20) regions. All the participants were screened as per the inclusion/exclusion criteria, and they got enrolled in the study after being convinced to a good extent. Informed consent was taken from all the patients (> 18 years) and in case the patient was minor (< 18 years) his/her legal guardian was asked to give consent at the time of recruitment under this study. The PKDL patients, suitable as per EC guidelines, were contacted in their locality and oriented with counselling during our field trip programs57; and then brought to ICMR-RMRIMS hospital and shifted to the wards for providing proper consultations, diagnosis and treatment by the Co-PIs who are clinicians and medical experts.
Questionnaire study
The participants of the study were assessed in two major categories of PKDL patients viz. (A) Group of high-intensity sunlight exposure (> 2 h/day) and (B) Group of minimal/low sun light exposure (< 2 h/day). In category A, PKDL patients with personal exposure to sunlight containing UV rays were again divided in four sub-groups based on their occupations and average exposure time durations: 2–4 h/day, 4–6 h/day, 6–8 h/day and 8–10 h/day. Similarly in category B, PKDL patients with minimal or low exposure of non-intense sunlight (< 2 h/day) were studied. Other components of the self-structured questionnaire (Fig. 5S) were used and few of them are as follows (1) the level of personal UVR exposure for their conditions; (2) past history of kala-azar; (3) clinical symptoms and types of skin; (4) their level of hygiene and sanitation; (5) dietary source of Vitamin-D (6) living conditions and peripheral surrounding; and (7) their style of clothing and quality of lives etc. The structured questionnaire was practically useful for collecting all the relevant information from the participants64, based on the aim of the study. Each of the patients was interviewed face-to-face and written informed consent was taken. The study participants were provided special attention for the issues of skin/sun sensitivity and essential medical consultations by the medical team at regular intervals or during their follow-up visits.
Haematological profiling
Briefly, EDTA anti-coagulated blood (1.5 ml) was taken and mixed thoroughly in rolling shaker. The blood samples of the patients were tested for haemoglobin (% Hb) profiling as well as complete blood count (CBC) analysis by using a fully automated blood analyser (Pentra-ES60, Horiba, Japan), as per the manufacturer’s instructions65. Then the blood volume was taken up by the sipper of the machine and counts for the total RBC, total WBC, neutrophils, lymphocytes, monocytes, eosinophils were performed. The correlation of % Hb was done by microscopically reviewing the haemogram. Apart from this, blood samples of some PKDL patients and VL patients were utilised for the measurement of the biochemical parameters such as; total protein, albumin, globulin, billirubin, creatinine, SGPT, SGOT, alkaline phosphatise and electrolytes (Na+, K+) by using a fully automated Biochemistry analyser (Mindray India, BS-240) as per the standard protocol described earlier65. Briefly, 20–30 µl of serum samples were aspirated by the aspirator needle and then processed in the reaction carousel automatically after setting the respective reagent bottles in this Biochemistry analyser.
Estimation of iron contents from patient’s sera
The estimation of iron contents from the patient’s blood was performed by the Serum Iron Assay Kit (ImmunoTag, G-Biosciences, USA) according to the manufacturer’s instructions66,67. Briefly, serum samples (125 µl) were taken, added with the Reagent-I and Reagent-II (125 µl each) in the test reaction vial; while 125 µl each of iron standard solution (125 µmol/L) and sterile autoclave water were taken respectively in standard and blank tubes. After 30 min of incubation at rotary shaker (120 rpm), the absorbance of the reaction mixture as well as standard and blank tubes was observed at 520 nm. The concentration of iron contents of the patient’s sera was then calculated using the standard formula given below.
Serum iron (µmol/L) = [Conc. of standard × (Abs. of test tubes – Abs. of blank tube] ÷ [Abs. of standard – Abs. of the bank tube]
The estimation of iron contents from some sera samples was also carried out using a fully automated Biochemistry Analyzer66,67 for the confirmation of the obtained values.
Estimation of vitamin-D among the patients
For the Vitamin-D measurement from the PKDL patient’s sera samples, along with VL/healthy controls; the cartridge-based iChroma kit method (BodyTech kit, Korea) was used as per the manufacturer’s instructions68,69. Briefly, releasing buffer (50 μl) was taken in reaction tubes; in which 50 μl of the serum sample were then added and mixed gently. After incubation for 10 min at RT, detection buffer (100 μl) was added to these tubes; followed by mixing gently by pipetting and incubated at rotary shaker for 15 min at RT. Then 75 μl of reaction product were loaded into the test cartridge and finally absorbance was taken by iChroma II Reader (BodyTech kit, Korea).
Profiling of cytokines from the patient’s sera samples
The quantifications of the key cytokines such as IL-10, IL-12 and IFNγR were performed by using specific antibody-coated ELISA (G-Biosciences, USA) as per standard manufacturer’s instructions. Briefly, 40 µl sera samples were taken in pre-coated ELISA wells, in which 10 µl of antibodies (anti-IL-10/anti-IL12/anti-IFNγR as applicable) were added. Then 50 µl of streptavidin-HRP solution was added to the test reaction wells and standard wells; followed by incubation at 37 °C for 60 min. After thorough washing for five times, equal volumes (50 µl) each of substrate solutions A and B were mixed, followed by 10 min further incubation at 37 °C in dark. Finally, 50 µl of stop solution was added to the reaction as well as standard and blank well followed by 10 min incubation; and absorbance was recorded at 450 nm. The standard curve was generated from the absorbance of the standards and the concentration of the test sample was quantified by extrapolation.
Culture of THP-1 cell lines
THP-1 cells (human monocytic cell line; source from NCCS Pune) were cultured in RPMI 1640 medium supplemented with 10% fetal bovine serum (FBS) and 1% penicillin–streptomycin as per our lab protocol. The cells were maintained in a CO2 incubator at 37 °C with 5% CO270. Frozen THP-1 cells were rapidly thawed in a 37 °C water bath for 1–2 min. The contents of the vial were transferred to a sterile 15 ml centrifuge tube containing 9 ml of pre-warmed RPMI 1640 medium. The cells were centrifuged at 500 x g for 5–7 min to remove DMSO, and the resulting pellet was resuspended in 10 ml of complete medium and transferred to a culture flask (25 cm2, Tarsons, INDIA). For passaging, the cells were passaged every 2–3 days upon reaching 80–90% confluence. The old medium was removed, and the cells were rinsed with phosphate-buffered saline (PBS). Trypsin–EDTA solution (2 ml) was added, and the cells were incubated at 37 °C for 5–10 min until detachment took place. The cell suspension was centrifuged at 500 × g for 5–7 min, and the pellet was resuspended in fresh medium. Cells were seeded at a density of 1 × 105 to 1 × 106 cells/ml. For the assessment of viable cells, the viability was assessed using a haemo-cytometer as per our lab protocol. An aliquot of the cell suspension was mixed with 0.4% (w/v) trypan blue dye (1:1 ratio) and counted under an inverted microscope (Nikon, Japan), with viable cells identified as unstained.
Experimental UVB irradiation to THP-1 cells:
The growth pattern and morphology of THP-1 cells exposed to UVB irradiation were analyzed to assess the effects of varying exposure intervals (0, 1, 2.5, 5, 10, and 15 min) using a narrow band UVB lamp (peak 310 nm, Phillips). The THP-1 cells were irradiated with UVB light (wavelength 280–320 nm) using a UV lamp (Phillips)71. The irradiation dose was calibrated to deliver a total energy dose of (3.3 kJ/m2 per minute) to the cells. The distance between the UV source and the cells was maintained (at specify distance of ~ 20 cm) to ensure uniform exposure. Each day the morphology of the cells was studied under inverted microscope as per standard practice till the 3th day of UVB treatment. For post-irradiation care, the cells were immediately returned to the incubator for recovery, after irradiation. Cell viability was evaluated daily from day 0 to day 6 using the Trypan blue exclusion method. Growth curve showed that 5–10 min UV radiation exposure for three days looks optimum. However, the shape, size and viability of the cells after 10 min comparatively looks unhealthy; so we have decided 5 and 7 min exposure time in the future course of our experiments.
2.5 × 106 viable THP-1 cells were taken in each of the 8 flasks containing 5 ml complete RPMI medium. Two flasks were for UVB-ve group, in which no UVB radiation was given. In a set of 3 flasks (UVB + 5 m group), 5 min UVB radiation was done per day in UVR box (dimension: 21 × 21x 20 cm3) and another set of 3 flasks (UVB + 7 m group), 7 min UVB radiation was treated per day to THP-1 monocytic cells up to 3 days.
Evaluation of cytokines release from THP1 cells in next passages under UVB radiation exposure
In order to monitor the pattern of release of key cytokines (like IL-10, IL-12), the viable THP-1 cells were taken for further study at 3rd day post incubation. Total 2.5 × 106 cells in 5 ml complete medium were taken in each of 8 flasks. From the control (UVB-ve) group, two flasks containing THP1 cells were kept without any UVB radiation treatment, while other two flasks were treated with UVB for 5 min up to 3 days (UVB + 5 mG1). On the other hand, out of four flasks, two flasks from (previous UVB + 5 m group) were continued with UVB radiation for 5 min/day up to 5 days (UBV + 5 mG2), while two flasks of cells were kept without any UVB radiation, but cultured in the same 5% CO2 incubator for a period of 5 days (UVB-ve G2). On 3rd day and 5th day, the culture supernatant fractions from each of the THP cells grown in flasks were taken for the estimation of IL-10, IL-12 and IFN-γR using the specific kits (G-Biosciences, USA) as per the manufacturer’s instructions mentioned previously.
Immuno-phenotyping of TLRs and TNFRs from patient’s blood samples
In order to know the level of expression of TLRs (Toll like receptors) or cytokines in PKDL patients vs. healthy controls, immuno-phenotyping assays of Fluorescence-activated cell sorting (FACS; BD Calibur) were performed as per the standard protocol72,73. In the initial phase, or few important immuno-modulatory molecules associated with pattern recognition receptors i.e. TLR2 (CD282-Alexa Flour), TLR4 (CD284-P.E.), TNFR1 (CD120a-FITC) and TNFR2 (CD120b-PE) relative expression studies were done using monoclonal human antibodies, purchased from BD Biosciences, USA. All the experiments were conducted independently with suitable controls and compensation groups. From the heparinised whole blood samples (100 μl) with ~ 1 × 106 cells flurochrome-conjugated antibodies were added (1–3 μl) and then mixed for 5 min in dark at RT. Then RBC lysis buffer were added and then tubes were kept at RT in dark for 20 min (with occasional mixing, 2 times). Then the tubes were centrifuged at 500×g for 15 min (in swing-out rotors) and the supernatants were discarded. Then cell pellets in the FACS tubes were washed with freshly prepared stain buffer twice and the cells were finally acquired by Flow cytometer (BD FACS Calibur, USA74) and then data was be analysed by both CellPro Quest as well as WinMDI 2.5 software.
Statistics
The analyses of statistics of experimental datasets were mainly done using Graph pad prism 5.0 (La Jolla, CA USA); and some other works like plotting data representation of study participants were performed using MS Excel 2010. The results of certain parameters were expressed as mean ± SEM, based on the individual values of total number of participants. In order to calculate the p-value, one way ANOVA or student t-test was applied for analysing the group datasets of the patients and healthy controls, wherever applicable. The p-values less than 0.05 were considered significant.
Results
Study area and measurement of sunlight UV radiation intensity
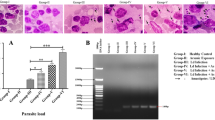
In order to evaluate the magnitude of UV radiations (UVR) coming from the sun light, we have measured UVR intensity in the study regions (Saran and Vaishali districts) as shown in Fig. 1A during June 2017 to December 2020 by manual method as well as by using the satellite based method empowered by TEMIS from ESA/KNMI, the Netherlands; as discussed in the methodology section. We have taken Saran district as endemic region for PKDL cases and Vaishali district as the region with low PKDL cases, due to the ‘Vaishali model’ in which number of cases reduced dramatically. We have also taken Patna district that covers both urban and rural areas, containing very low PKDL cases (Fig. 1B). The number of blocks in each of the study sites in these 3 districts were visited 3–4 times (per year) to identify new cases and UV light intensity was also analysed in each block of these districts as shown in Fig. 1C, D. Considering the local weather conditions such as temperature, relative humidity, fog, rainfall etc., we recorded the sunlight UVR intensity (in µW/cm2) on daily basis, which then was converted into UV doses (kJ/m2; time period = 5 min at the solar noon) Fig. 2. We observed that highest sunlight UVR intensity (UV index > 12–14) Fig. 2A or erythemal UV dose (> 8–9 kJ/m2) Fig. 2B was found in the monsoon (June–August) and summer (March–May) months; while lowest values of sunlight UVR (UV index < 6–5) or UV dose (< 4–5 kJ/m2) was recorded in the winter (December-February) as shown in Fig. 2A, B. We have found that both UV index and UV dose are changing significantly from summer to winter seasons each year during the study from 2017 to 2020. In summer seasons, much heat-related mortality was reported due to the heat waves in India75. The pattern of the UV dose and intensities in three years from June 2017 to December 2020 were also found similar. The satellite-based sunlight UVR measurement data was also obtained from TEMIS maps in terms of erytheml UV index and erythemal UV dose (kJ/m2). The representative images of the map-based data panels are displayed in four different seasons (Fig. 4S). It can be found that during summer and monsoon months, there is high recorded values of both UV index and UV dose in Bihar region (coordinates ~ 85.37° E, 25.12° N) shown in the map panels. For example, the erythemal UV index in December month becomes low (< 6, greenish colour), while its values in March rises to > 12 (reddish colour, as per scale bar colour) in the area. Similarly, the value of erythemal UV index crosses 14 in June month; but it gets further decreased in September (~ 12) onwards Fig. 4S(A). It is noted that during winter season not only Bihar region, but also south Indian region is showed with erythemal UV index < 6 (greenish colour). However, in the month of June, whole Indian region has very high erythemic UV index over 12 as indicated in scale bar. Similarly, we have also observed erythemal UV dose to quantify the magnitude of UV radiation penetration at ground level, which is also showed same pattern as above for the UV index. The erythemal UV dose (kJ/m2) in December is found < 4 kJ/m2; while its value reaches 6–7 kJ/m2 in March. However, highest values of erythemal UV dose (> 8 kJ/m2) is recorded in June in Bihar followed by gradual decrease is taking place September (7 kJ/m2) onwards as per colour scale bar Fig. 4S(B). The UV intensity is always found higher due to very hot weather and open sky conditions in Bihar, India. The satellite based UVR data received from the ESA/KNMI sources was also validated by the measurement of surface/ground UV (GUV) radiations in the study sites. The comparative UVR data of TEMIS/KNMI and GUV radiations is summarised (Table 2), highlighting the monthly mean values of sun light UV rays intensity and doses (kJ/m2) measured at the solar noon time. The average sun light UVR doses at the ground/surface showed the similar trend in concordance with satellite-based (TEMIS) data.

Map of Indian subcontinent showing the VL affected regions for assessment of sunlight UV rays intensity of State of Bihar: Figure was prepared originally using Microsoft PowerPoint and Google Earth (version 9.4.50.2, https://earth.google.com). The location of Bihar in Indian sub-continent was identified by using Google earth map. The selected area of map was cut and enlarged for visibility so that study sites information’s can be included in the map area as shown A. Similarly in C, Zoon-in picture of map showing study sites at district level and locations were added in the map. The three study sites districts and their location at block level were further zoomed in and number of blocks visited in each district has been shown in D. However, Bihar political map was taken from the Government of India website. All three districts and their blocks visited during the course of study including their latitude and longitude were mentioned in B as per TEMIS co-ordinates.

Graphical presentation of UV index and UV dose across seasons: The trends of sunlight UV radiations index were displayed in four seasons: March–May, June–Aug, Sept–Nov and Dec–Feb from 2017 to 2020 (A). Similarly, the patterns of sunlight UV radiations dose (kJ/m2) were demonstrated in four seasons: March–May, June–Aug, Sept–Nov and Dec–Feb from 2017 to 2020 (B). The daily datasets were made average each month and similarly the mean of the given three months were plotted with standard deviations for year-wise comparison. The statistical analysis shows as p-values p < 0.001 (**) significant and < 0.0001 (***) are highly significant.
Study participants and analysis of questionnaire-based information
As per the EC approved guidelines, total number of patients with PKDL (n = 358) were screened for this study, and finally 283 patients completed their participation in this project work (Fig. 3S). In addition, 30 VL patients and 45 healthy persons (25 persons from non-endemic and 20 from endemic regions) were also included in the control groups. In the present study, the “occupational categories” of the patients were grouped such as labourers, workers at field, hawkers, vegetable salesmen, indoor workers etc. (Fig. 3). Among the 283 PKDL patients, 93 cases (33%) were found to be in the category of labourers; followed by 57 patients (20%) were seen as field-workers as compared to other groups as house-wife (n = 41, 15%), students (n = 34, 12%), outdoor workers (n = 23, 8%), shopkeepers (n = 20, 7%) and indoor workers (n = 15, 5%) (Fig. 3A). This showed that labourers and farm workers are comparatively more exposed to sunlight containing UV rays. The complaints of sun sensitivity, skin sensitivity and irritation on exposure to sun light were also screened among the PKDL patients, where skin pinching 21% (n = 60) and sun burning 15% (n = 41) or both (19%, n = 53), with irritation (10%, n = 29) and combinations of all three complains were noted to be sensitive to sun and/or skin, respectively (Fig. 3B). The photographs of such PKDL patients with the complaints of sun and/or skin sensitivity were presented (Fig. 1S), those who have already received appropriate treatment from the doctors of this study. As per the clinician’s assessment, it is evident that 73% (n = 207/283) of the PKDL patients were found to be complaining under the exposure to intense sunlight. Some PKDL patients (n = 76) did not report any complaints regarding the symptoms of sun burning, skin irritation (pinching) or combinations of any two/all symptoms.

PKDL patients (n = 283): Occupation distribution and complaints of skin and/or sun sensitivity. The distribution of the occupation types of the PKDL patients reported in the study are described as labourers, farm field workers, house wife, students, shopkeeper, outdoor workers and indoor workers in percentage (shown in pie chart, A). Similarly, the major complaints of the PKDL patients were noted as either of skin sensitivity, sun sensitivity, or both, skin irritation (pinching), or all of these, or no sensitivity (shown as pie chart, B).

Distribution of occupation sub-categories and UVR exposure periods in PKDL patients. The percentage of the sub-categories of the labourers (n = 93) were divided as daily wagers, mason, plumbers, carpenters, fitter, electrician, mechanics, rickshaw pullers or any others (A). However, the average sunlight exposure usually received by the patients (n = 283) was mentioned in the time slots like 0–2 h, 2–4 h, 4–6 h, 6–8 h or 8–10 h per day (B); in form of percentage (pie-chart). The past history of the patients (n = 283) either with or without VL, with past PKDL episode or combinations of both VL and PKDL were shown (in percentage) shown as pie chart C. Similarly the clinical manifestations were demonstrated with the appearance of lesions like macular, nodular, popular, or mixed types found among the patients (n = 283) shown as pie-chart, D. The body mass index of these patients was mentioned as percentage population of below average, average or more than average (E); while their habitual intake of Vitamin-D from dietary sources were noted as poor, deficient, average or good (F).
Since the labourers and farm workers cover large number of populations/patients, so the labourers again sub-divided into different categories. In the sub-category analysis of labourers (n = 93), it was noted that 37% (n = 34) were daily wagers and 20% (n = 19) were masons workers; followed by rickshaw pullers (12%, n = 11), electricians (9%, n = 8), mechanic (8%, n = 7) who used to routinely get exposed to sun light everyday (Fig. 4A). However, other categories (Carpenter, n = 5; plumber, n = 3; fitter, n = 1; or any other semi-skilled field workers, n = 5) come total 14% but individually ranged 1–5% (Fig. 4A). The mean values of daily exposure to sunlight on the skin of these (n = 283) patients were recorded in five groups based on duration of exposure time period: 0–2, 2–4, 4–6, 6–8, 8–10 (hours); in which 38% (n = 108) and 22% (n = 63) of the patients were habituated of having solar UVR exposure/day for 6–8 h and 4–6 h, respectively (Fig. 4B). We found that 57 patients with exposure of 8–10 h, followed by 35 patients with exposure of 2–4 h; and 20 patients with exposure of < 2 h (Fig. 4B). We also correlated the new PKDL cases with past history of VL or treated cases, as it is generally thought that PKDL developed after VL treatment with SAG and/or liposomal Amphotericin-B. Among the PKDL patients (n = 283), 61% (n = 173) patients were found with past history of VL, while 11% (n = 31) patients had earlier episodes of PKDL/history. However, 10% (n = 28) patients had no previous history of VL or PKDL; whereas 18% (n = 51) patients were noticed with the past history of both VL and PKDL (Fig. 4C). When we looked for the category of PKDL cases based on their signs, symptoms and types of PKDL lesions, we found that among the patients, 51% (n = 144) were found as macular PKDL lesions, followed by nodular (24%, n = 68), popular (14%, n = 40), and cases with the mixed types (11%, n = 31) including the nodulo-macular (8%, n = 23) and maculo-papular (3%, n = 8) (Fig. 4D). However, 50% have shown average BMI and 38% under below average category of BMI, but only 13% have above normal range of BMI (Fig. 4E).In the analysis of the Questionnaire-filled information among the patients, > 44% of the cases was found to be deficient in consuming Vitamin-D from dietary sources. However, PKDL patients were showed taking poor (20%), average (24%) and good (12%) dietary sources of Vitamin-D on the basis of their dietary intake of vitamin D enriched food (Fig. 4F). This suggested that food quality or nutritional value is poor in their food consumed every day in rural area or labourers and farm-working persons. We could not correlate directly with BMI value, but food quality is really important nutritional factor to control diseases like VL, TB, and HIV.
Level of vitamin-D in PKDL & VL patients
In order to evaluate the role of vitamin-D in PKDL pathogenesis, we estimated vitamin-D concentration (ng/ml) from the sera samples of the PKDL patients (n = 60) and compared it with VL patients (n = 20) as positive controls and healthy persons (n = 25) as control (Fig. 5). It is found that PKDL patients contain more vitamin-D (1.25 fold; p < 0.05) in comparison to healthy controls. However, when we compared the level of vitamin D concentration in PKDL vs. VL patients it showed ~ two-fold higher value (p < 0.005) (Fig. 5). The differences in the mean values of vitamin D concentrations were found statistically significant. Thus, vitamin D level in PKDL patients showed more vitamin D concentration as compared to healthy control and VL patients.

Vitamin-D concentration profiling among PKDL patients vs. healthy and VL patients. The concentration (ng/ml) of vitamin-D was measured from the sera samples of the patients and compared among the healthy controls (n = 20) versus PKDL (n = 60) and VL (n = 25) patients. The statistical p-values were p < 0.05 (*) or p < 0.005 (**).
Iron and haemoglobulin concentrations in the PKDL and VL patients
It is reported in past publications20,22,76,77 that UV rays have pleotropic role in human skin immunology and furthermore, vitamin-D along with iron contents are reported as, mediatory bio-chemicals37,78,79 which likely to play immuno-modulatory roles in Leishmania infections. Hence, we also evaluated the concentration of iron from the sera samples of PKDL (n = 25) and VL patients (n = 25) vis-à-vis healthy controls (n = 15). It was found that iron concentration in PKDL patients was twofold higher than the VL patients and found similar concentration with the healthy persons (Fig. 6A). The differences in mean values of PKDL vs healthy controls statistically non-significant (p > 0.05) and PKDL vs VL cases were showed statistically significant (**p < 0.005). We have also measured the concentration of haemoglobin (% Hb) in PKDL (n = 39), VL patients (n = 15) and healthy control (n = 20). The Hb concentration in PKDL patients is similar to healthy persons, but two-fold lower in VL patients (Fig. 6B). It showed that the Hb concentration in PKDL patients is similar to healthy control, but it is different in the VL patients. The VL patients are generally anaemic and weaker than the PKDL patients4,17,67,80. However, the analysis of other parameters from Biochemistry (Table 3) and Complete blood count (Table 4) was not found significant among PKDL patients and VL patients vs. healthy controls, except %Hb, total RBC and iron concentrations.

Iron and Hb concentration profiling among PKDL patients vs. healthy and VL patients. The concentration of iron (µMol/L) was measured from the sera samples of the patients and compared among the healthy (n = 15) control versus PKDL (n = 25) and VL (n = 25) patients. Similarly the concentration of haemoglobin (% g/dL) was mentioned in the form of comparison of healthy controls (n = 15) versus PKDL (n = 39) and VL (n = 20) patients. The statistical p-value was p < 0.005 (**).
Cytokines profiling in the PKDL and VL patients patients from serum samples
The aspects of immunological changes induced in PKDL patients due to the prolonged exposure of intense sunlight UVR was important step. The cytokine expression pattern is known in VL and PKDL patients, but the role of cytokines alteration in sun-light UV exposed patients with PKDL having < 2 h/day vs. > 4 h/day times has been evaluated first time. In order to evaluate the release of cytokines (IL-10, IL-12) and IFN-γR in the PKDL patients, we performed ELISA with sera samples from PKDL patients versus healthy and VL patients. It was found that IL-10 concentration was higher (327.024 ± 283.328 pg/dL; n = 11) in VL patients than PKDL cases (284.227 ± 236.144 pg/dL; n = 24) as compared to the healthy controls (Table 5). Similarly, IL-12 concentration was two-fold higher in the PKDL patients (14.503 ± 14 ng/L) as compared to healthy control and slightly higher as compared to the VL cases (12.757 ± 9 ng/L) (Table 5). Similarly, the IFN-γR profiling also revealed an increased concentration in PKDL as compared to VL patients and healthy control. We have observed that nodular PKDL cases have higher concentration of above measured cytokines than the macular PKDL cases; which are higher as compared to both VL patients and healthy controls. Thus, we have found very low concentration of Th1 type cytokines before treatment (BT) in VL cases than after treatment (AT). So the less expression of Th-1 type cytokine (IL-12) and/or higher expression of Th-2 type cytokine (IL-10) in VL cases implicated a potential role of photosensitisation from the sunlight UV rays that favour VL to PKDL conversion81,82.
Morphology and growth curve of THP-1 cells
Cell viability and morphological changes
As per protocol, it was observed that THP-1 cells exposed to 5 and 10 min of UVB irradiation approached the lethal dose 50 (LD50) 5th and 4th days, indicating a threshold beyond which cell viability significantly declined. It is noted that 15 min exposure is more lethal and cells were non-viable or LD50 on the second day. Growth curve showed that 5–10 min UV radiation exposure for three days looks optimum (Fig. 7A). However, the shape, size and viability of the cells are on 10 min comparatively looks unhealthy so we have decided 5 and 7 min exposure time in future course of experiments. The prolonged irradiation beyond 10 min resulted in notable morphological distortions and signs of cytotoxicity, suggesting that extended UVB exposure adversely affects cell integrity (Fig. 7B). The morphological analysis demonstrated that THP-1 cells cultured under UVB stress for 5 min showed optimal growth on day 3, with intact and viable morphology. This observation implies that further experiments can be conducted using the UVB + 5 m group on both day 3 and/or day 5 for more in-depth analysis (Fig. 7B). Overall, these results indicate that while short-term UVB exposure (up to 5 min) does not severely compromise cell viability, extended exposure leads to significant cytotoxic effects, warranting caution in the experimental design. The favourable growth and morphology of THP-1 cells at day 3 post-irradiation establish a suitable basis for subsequent investigations.

The impact of UVB radiation treatment on THP-1 cells. The percentage viability of cells with UVB irradiation (0, 5, 10, and 15 min) was observed from day 0 to day 6 (A). The morphology of THP-1 cells were analysed at different doses of UVB radiation at (0, 1.0, 2.5, 5.0, 10.0, and 15 min) durations (B).
The expression analysis of IL-10, IL-12, and IFN-γ Receptor-1 in THP-1 cells subjected to UVB irradiation revealed significant alterations in cytokine profiles and receptor expression. Under UVB irradiation, the expression of IL-10 tended to decrease compared to the UVB-negative control group. However, in subsequent increase in time exposure where THP-1 cells were maintained under UVB stress (7 min), IL-10 expression was found recovered after 3 days compared to the control group (Fig. 8A). However, the expression of IL-12 exhibited a gradual decrease in THP-1 cells exposed to UVB irradiation (5 and 7 min) relative to the control group after 3 days. This trend highlights a sustained suppression of IL-12 under UVB stress conditions (Fig. 8B). Similarly, IFN-γ Receptor expression showed to be decreased gradually as the case for IL-12. The expression of IFN-γ Receptor 1 was reduced in THP-1 cells subjected to UVB irradiation combined with a 5- and 7-min exposure compared to the control group after 3 days (Fig. 8C). The cytokines pattern is altered in UVB radiation exposure and favourable to Th2 type immune response, which can help in the development of PKDL/VL infection in host cells.

Concentration of cytokines in THP-1 cells under UVB irradiation. A IL-10 concentration was remarkably decreased in THP-1 cells exposed to UVB for 5 min (UVB + 5 m) compared to UVB-negative controls. B IL-12 concentration also showed a notable decrease under UVB + 5 m conditions. C Similarly, IFN-γ Receptor (IFN-GR) concentration was reduced in THP-1 cells exposed to UVB + 5 m relative to controls. However, with extended UVB exposure (7 min), a slight increase in IL-10 concentration was observed, while both IL-12 and IFN-GR concentrations remained downregulated in THP-1 cells subjected to UVB + 5 m irradiation. Data are representative of three independent experiments.
Furthermore, we have analysed whether alteration in cytokines pattern in UVB irradiated THP-1 cells which favours Th2 type immune response is sustained for longer duration of the treatment. So a comparative analysis of these key cytokines secretion between 3 days (left panel) versus 5 days (right panel) of UVB irradiation was performed that revealed IL-10 expression recovered/increased over time (Fig. 9A2), while both IL-12 and IFN-γ Receptor expression further decreased under continuous UVB stress conditions in the second/subsequent passages (Fig. 9B2, C2). Specifically, the expressions of IL-12 and IFN-γ Receptor were found lower compared to UVB-negative THP-1 cells after the extended exposure either 3rd days or 5th days on subsequent passages (Fig. 9). However, alteration in cytokines at 5th days in subsequent passages was not very significant, because we have used cells culture without any parasites infection. These findings suggest that THP-1 cells exhibit an increased secretion of IL-10 in response to continuous UVB irradiation in subsequent passages. However, secretion of IL-12 and IFN-γ Receptor are slightly reduced for 3 days and upto 5 days exposure, indicating a shift towards a more immunosuppressive phenotype under UVB stress conditions. This observation may have broader implications for understanding how chronic or repeated UV exposure may influence immune responses in monocytic lineages, and potentially contribute to immune evasion in PKDL pathogenesis.

Secretion of cytokines in THP-1 cells under UVB + 5 m irradiation for varying durations for day 3 versus day 5 from first passages (G1) to second/subsequent passages (G2). A IL-10 concentration increased significantly from 3 to 5 days of UVB + 5 m irradiation in G2 compared to the UVB-negative control group (A1, A2). B Conversely, IL-12 concentration decreased under the same conditions, with reduced levels observed at both time points and even in G2 (B1, B2). C Similarly, IFN-γ Receptor concentration was also down-regulated in THP-1 cells exposed to UVB + 5 m irradiation, with comparable reductions seen after 3 and 5 days in both G1& G2 passages (C1, C2). Data are representative of three independent experiments. The statistical analysis shows as p-values p < 0.05 (*) or p < 0.005 (**) are significant, while p > 0.05 (ns) as non-significant.
Expression analysis of pattern recognition (Toll-like) receptors
In order to find the relative expression levels of pattern recognition receptors such as TLRs-2/4 (Toll-like receptors) in PKDL patients vs. healthy controls, immuno-phenotyping assays were carried out from blood samples using CD282-AF (TLR2), CD284-PE (TLR4) monoclonal human antibodies by FACS analysis (BD Calibur). We have performed this expression analysis in 16 PKDL patients and 14 healthy persons; which are divided in two main categories of average sunlight UVR exposure, such as low (< 2 h/day; Fig. 10A1, B1) and high (> 4 h/day; Fig. 10A2, B2) daily limits, depending on their occupational habits. It was observed that TLR2 expression is ~ two-fold higher in PKDL patients as compared to healthy controls at < 2 h and > 4 h daily exposure time period (Fig. 10). Similarly, TLR4 expression is ~ 1.4 fold higher in PKDL patients as compared to healthy control. However, if we looked joint expression pattern of both TLR2/4 in PKDL patients vs. healthy control then slightly increased (1.2 fold) was observed. We have analysed quantative data and represent as bar diagram to understand easily in terms of fold changes in the expression of TLR-2, TLR-4. It was found upregulated two-fold in the PKDL patients (MFI: 58.59, 14.33 & n = 7) as compared to the healthy control (MFI: 27.32, 9.463 & n = 5) under < 2 h/day exposure category (Fig. 10C1). Similarly, under the category of > 4 h/day exposure, the expression of TLR-2 was observed increasing two-fold in PKDL patients (MFI: 76.77, 25.03 & n = 9) in comparison with healthy control (MFI: 44.86, 18.19 & n = 9) (Fig. 10C2). Similar to TLR2, expression of TLR4 alone and combined expression of TLR2 &TLR4 were also upregulated in PKDL patients. Thus, TLR2 and TLR4 expression were up-regulated twofold and 1.4 fold, respectively in the PKDL patients.

Expression profiling of TLRs (TLR2/4) in PKDL cases (n = 16) vs. healthy controls (n = 14). The analyses of expressions of TLR-2 (CD282-AF) and TLR-4 (CD284-PE) were carried out from the blood samples of the healthy controls (A) and PKDL patients (B). Based on the average daily sunlight exposure of the study participants, the profiling of TLRs was performed in two main categories i.e. sunlight UVR < 2 h/day (A1 & B1) and sunlight UVR > 4 h/day (A2 & B2). By using the CellPro Quest and WinMDI tools, the representative panels of FACS analysis were mentioned involving the gating strategy, unstained controls and TLR-2/4 individual sets and compensation etc. The analyses of quantitative data of TLR2, TLR4, & TLR2&4 were displayed (C1, C2). The statistical analysis shows as p-values p < 0.05 (*) or p < 0.005 (**) are significant, while p > 0.05 (ns) as non-significant.
The expressions of Tumour Necrosis Factor Receptors (TNFRs-1 & 2) were also evaluated in the PKDL patients vs. healthy controls. The gating strategy and unstained controls were given (Fig. 11A, B). The expression analysis of TNFR-1 and TNFR-2 was carried out in two main categories, based on the average sunlight UVR exposure: < 2 h/day (Fig. 11A1, B1) and > 4 h/day (Fig. 11A2, B2) among the PKDL patients (n = 16) and healthy controls (n = 14). We have observed that TNFR2 was up-regulated (~ 1.8 fold) in PKDL patients than healthy persons, but TNFR1 expression was marginally down regulated. However, TNFR2 & TNFR1 expression is marginally increased 1.2 fold in PKDL patients as compared to healthy control. Similarly, as above mentioned for TLR2 & TLR4, we have also presented the post quantitative analysed data here for TNFR2 & TNFR1 expression pattern. The expression profiling of TNFR2 was found upregulated (two-fold) in the PKDL patients (MFI: 6.52, & n = 7) as compared to the healthy control (MFI: 3.14 & n = 5) under < 2 h/day exposure category; while the TNFR1 expression was observed marginally decreasing in the PKDL patients (MFI: 18.22) as compared to healthy persons (MFI: 19.28) as shown in (Fig. 11C1). Under the category of > 4 h/day exposure, the expression (TNFR-2) was observed increasing two-fold in PKDL patients (MFI: 7.39 & n = 9) in comparison with healthy control (MFI: 3.9 & n = 9); while the TNFR1 expression was also found marginally lower in the PKDL patients (MFI: 22.396) as compared to healthy persons (MFI: 23.65) as shown in (Fig. 11C2). Therefore, it is observed that the intense sunlight UV rays exposure (> 4 h/day) showed higher expression of the TNFR-1/2 than the low UVR exposure groups.

Expression profiling of TNFRs-1/2 in PKDL cases (n = 16) vs. healthy (n = 14). The analyses of expressions of TNF-R1 (CD120a-FITC) and TNF-R2 (CD120B-PE) were carried out from the blood samples of the healthy controls (A) and PKDL patients (B). Based on the average daily sunlight exposure of the study participants, the profiling of TNFRs was performed in two main categories i.e. sunlight UVR < 2 h/day (A1, B1) and sunlight UVR > 4 h/day (A2, B2). By using the CellPro Quest and WinMDI tools, the representative panels of FACS analysis were mentioned involving the gating strategy, unstained controls and TNFR-1/2 individual sets and compensation etc. The analyses of quantitative data of TNFR1, TNFR2, and TNFR1&2 were displayed (C1, C2). The statistical analysis shows as p-values: p < 0.05 (*) or p < 0.005 (**) are significant, while p > 0.05 (ns) as non-significant.
Discussion
Tissue homeostasis is an important phenomenon of the human body, which is largely executable by host macrophages83. In the presence of pathogenic ligands, monocytes or macrophages are very active to provide the first line of host defence, or else by self-limiting feedback mechanisms, they mediate only for the signalling network essential for normal tissue functioning84,85. As the poor population or poor socioeconomic community, with low personal income, they are usually more susceptible to the high density of the sand-fly vector Leishmania infections catch them easily, and also due to the known fact of malnourishment in these less privileged communities3,4,86. Among them, VL patients with fatal symptoms get early medical consultations, diagnosis and treatment because of the integrated efforts under KEP/NVBDCP/MoHFW, Govt. of India. But the poor people with mild to moderate PKDL symptoms are often found neglecting the clinical manifestations, for the sake of their daily livelihoods5,6,55,87; that later leads to profuse occurrence of lesions on the skin. Additionally, constant irregularities in their follow-up visits and treatment delays worsen the healing period, with increasing prevalence of PKDL5,87. The Leishmania parasites, during active PKDL conditions, stay happily in the skin either as macules, papules, nodules or polymorphic lesions15. More cases of papulo-nodular appearance on the sun exposed body parts of these patients provide support to postulate that Leishmania infections get favour for development of PKDL in the skin17; as the immune homeostasis, i.e. Th1-Th2 balance in the patients becomes badly affected for the proxy war of modulatory cytokines, whose antagonistic actions are responsible for the disease chronicity88. Exposure of human skin to UV radiations from intense sun light induces oxidative stress20,89, allergic inflammation37,90 and immunosuppression responses81,82; which collectively have been implicated in different dermal disorders such as photo-ageing of skin, photo-carcinogenesis etc.22,38. The increased blood flow and vascular permeability are reported under UV-induced conditions leading to development of erythema, edema, hyperplasia; with marked enhancement of COX-2 and PGs22,81,82. Our results showed that majority of poor population includes labourer, field workers and followed by house wife, who were prone to develop PKDL and covers > 65% disease burden. The house wife means here who generally worked in the field with their husband in rural area (assist their husband work in farming, construct, and other types of work) but exposure time is comparatively lower than labourers and farm field workers. Similar trend were also observed in students category in rural area as they are supporting their parents in farming and field work. Thus, highly exposed poor population of rural area is found more suffering from PKDL incidence as compared to other population, who get exposed less time or living in urban area. We have further analysed labourers (93 patients), which showed that daily wagers and mason/construction covers > 50% PKDL cases because they were exposed over 6 h every day. The PKDL cases who were exposed 6–8 h (n = 108) covered 38% patients of overall PKDL cases. Therefore, highly exposed from UVB radiation poor population is more prone for PKDL development including other factors (VL history, vitamin D intake, host susceptibility etc.)14,17.
In human skin, induction of immunity is reported to be suppressed by urocanic acid91. Similarly, in sojourners to high altitude; malnutrition, sun exposure and urocanic acid are correlated to be interacting for immunity suppression92. Moreover, UV-induced vitamin-D3 acts as a mediator for contributing in immunity suppression, under human skin exposure to UV wavelengths in sun light37,46,79,93. In response to UVB radiations, tumor necrotic factor alpha (TNF-α) is released from the keratinocytes, which stimulate TNFα gene transcription; resulting in the initiation of NF-κβ translocation to the nucleus, that in turn carries the downstream functions. Besides, IL-10 expression is up-regulated and IL-10 level is increased abundantly after secretion from sweat glands, melanocytes; while IL-12 expression is found at comparatively low levels88,94. Induction of IL-10 is initiated early than IL-12 expression by UVR, preferentially in the expanding populations of monocytes or macrophages95. High expression of IL-10 implicates the Th2 response, with limiting IL-12 immuno-protection; leading ultimately to immunosuppression. Meantime, the Th2 cells, already differentiated in the dermal microenvironment, access the skin-homing potential from IL-12 before inducing their cytokine secretion; that produces chronicity of the disease. We have observed that IL-10 expression was higher in VL patients than PKDL cases as compared to the healthy patients. Similarly, IL-12 concentration was higher in the PKDL patients than the VL cases. So less expression of IL-12 and higher expression of IL-1095 played a potential role of photosensitisation from the sunlight UV rays among the PKDL patients. Thus, PKDL cases are more in village’s area and propositionally associated with sun light exposure time. However, vitamin D concentration could be associated in contributory role in PKDL development46,79,93, but serum iron, and Hb concentrations were similar to healthy control and could not play a major role in PKDL incidence or development. In contrast to PKDL, VL cases have generally two fold lower vitamin D, serum iron and Hb concentration and thus, could be considered as the risk factors for VL pathogenesis or development.
Similarly, high expression of Toll-like receptors (TLRs-2 & 4) in the intense sun exposed patients with PKDL, as compared to the healthy controls; adds important information on the mechanism of disease pathogenesis, implying a role of these pattern recognition receptors in patient’s population. The TLR-2 is up-regulated (~ two-fold) than TLR-4 in the PKDL patients vis-à-vis the healthy people; that reveals TLRs ligands from Leishmania pathogens are more51. Further, the lower expression of TNF-R1 than TNF-R2, among the PKDL patients with exposure to intense sun light, than the healthy persons; implicates the fact of less immuno-protection, and more immuno-suppression; because the activation of TNFR1, known as death receptors for triggering apoptosis and NF-κβ signalling, results in allergic inflammatory responses and TNFR2 in turn, contributes in immune tolerance to the pathogens51. Thus, our results suggest a key role of TLRs-2/4 and TNFR2 interactions in the modulation of PKDL pathophysiology under harmful UV-induced conditions.
There are reports that UVB radiations cause alterations in human cells, but little is known about the UVB-mediated PKDL pathogenesis so far. We have taken the human monocytic cells (THP-1) irradiated with UVB at different doses (as mentioned in the methodology) and evaluated the impact along with the release of key cytokines (IL-10, IL-12 and IFNγR). Therefore, in-vitro datasets cumulatively indicate in favour of our hypothesis on human population-based data (PKDL patients) occupationally exposed with sunlight UVR. As it is not feasible to artificially give UVB exposure to the VL-treated patients (before PKDL development), we adapted a workable approach to evaluate the intensity/dose of UV radiation from sun-light in PKDL patients, based on their occupations and average sunlight exposure hours/day. The immunology of skin is largely influenced by the UV radiations: sun burning or tanning is the simple example; and melanoma, skin cancers or carcinogenesis are another group of complications/outcomes of intense light (radiations) from the sun20,42,82. However in PKDL, clear complaints of photosensitivity i.e. skin reddening, pinching or irritations seem to be associated with the pathogenesis of the disease17. In Bihar, the VL epicentre of Indian subcontinent4,8,11, a large population of the labourers and field workers regularly work very hard96 for 5–7 h daily or even more depending on the nature of work; and exposed sufficiently to intense sun light for prolonged day time. The ultraviolet radiations from direct solar source and surface albedo indirectly get ample skin penetration in these people, who typically belong to the poor socioeconomic community, with low personal and environmental hygiene in their surroundings. Based on above results and previously reported information on PKDL pathogenesis, we have drawn a feasible explanation (Fig. 12). Upon ample exposure to sun light UVR, the E-LCs morphologically undergo changes, become round shaped losing its place from the dermal milieu, and its antigen presenting ability is also compromised with inhibition to contact hypersensitivity and alloantigenic responses. The photo-isomerisation of urocanic acid, endogenous sunscreen available from the stratum conium and sweat glands is inhibited by excess UVR absorption42. As the conversion of trans- to cis- forms of this immuno-modulatory urocanic acid in epidermis is blocked36, then the cascade of mechanism leading to activation of regulatory T-cells and immune tolerance in skin is hampered under UV-induced conditions42,81. Moreover, UV-induced vitamin-D3 acts as a mediator for contributing in immunity suppression37,46,79. Thus, exposure of UVB radiations causes TNF-α release in the skin that can affect the downstream signalling pathways. Moreover, increased IL-10 expression and limiting IL-12 expression is resulted under prolonged exposure to sun light in labourers and farmers persons. In such condition, the expression of TLR2/4 increased which is leading to further up-regulation of TNFR2 causing altered NF-kβ signalling pathway51. High expression of IL-10 implicates the Th2 response, with limiting IL-12 immuno-protection; leading ultimately to immuno-suppression36,81. Meantime, the Th2 cells, already differentiated in the dermal microenvironment, access the skin-homing potential from IL-12 before inducing their cytokine secretion; that produces chronicity of the PKDL development. Although presence of pro-inflammatory cytokines like TNF-α is in abundance, still in the skin milieu, significant co-occurrence of antagonising cytokines like IL-10 creates a favourable buffer effect to the Leishmania parasites; for which macrophage’s pathogen killing capability is largely curtailed. Meanwhile, the homeostasis of Th1-Th2 types immune responses become unbalanced; and the tropism of intracellular L. donovani parasites tend to change and migrate for skin homing (Fig. 12). Henceforth, the perilous ultraviolet radiation from the intense sun light is likely to be responsible for the recrudescence of Leishmania infections as PKDL lesions in skin. Our findings implicate that sunlight UVR induced conditions modulate the immunological responses leading to PKDL pathogenesis, which is likely mediated by vitamin-D. Thus, the role of sunlight UVR is apparently to be associated for the development of PKDL as an important environmental factor in the VL endemic populations of Bihar. One major limitation of the study is that we don’t have animal model for PKDL, so we have tried to develop mice or hamsters model, but failed so far. High sun-light exposure to human population depending on their occupations is a natural condition, but we could not expose healthy human persons or VL treated persons with UVB radiation due to the ethical issues. However, as in other research, our study also has some limitations, that we have included the data only from two districts of Bihar. So our results may not be applicable to different ethnic regions.

Mechanism of sunlight UV rays-induced PKDL pathogenesis. This schematic model was prepared using MS PowerPoint based on our findings, past literature and hypothesis as mentioned in text. With the ample exposure of the sunlight UV rays on the human skin, the photo-isomerisation of trans-UCA to cis-UCA is stopped due to inactivation of enzymes (A). Simultaneously, absorption of sunlight by the epidermal Langerhan’s cells (DC or ELCs) causes loosening of skin homing and leading to migration to lymph nodes (LN). On the other hand, the damage of keratinocytes present in the epidermis causes activation of the regulatory T-lymphocytes (T-cells). Besides, vitamin D synthesis during sun-light exposure also modulates the host immunity through altered expression of vitamin D binding proteins which leads down-stream signalling (B). The increased expression of IL-10, TLRs-2,4, TNFR2 coupled with decreased expression of IL-12 and TNFR1 in the skin milieu lead an immuno-modulatory cascade, undergoing NF-kβ signalling (C). In turn, the immune functions of down-stream signalling become altered; and Th1–Th2 imbalance is resulted in defective immune homeostasis. The ability of the macrophages to kill pathogen is reduced ultimately in the host system; and usually the Leishmania parasites show skin homing behaviour, sustaining under the favourable conditions. However, the series of the immune changes followed by the prolonged photo-exposure of UV light promote cell mediated and humoral immuno-suppression in the dermal skin of the host which likely induces PKDL pathogenesis.
Conclusion
In the climate change scenario, significant seasonal variability of sunlight UVR is prominent; whereby the highest UVR data was recorded in seasons during May–July and lowest UVR found during December-February each year. In the VL endemic regions, the poor socioeconomic populations work as labourers and farm/field workers and in turn get maximum exposure to intense sunlight for prolong time. Thus, there is more incidences and prevalence of PKDL cases in this population of Bihar. Photosensitivity of sunlight UV rays is the responsible factors to induce immunological changes leading to PKDL pathogenesis. Under the sunlight UVR induced conditions, the up-regulated expressions of TLR-2/4, TNFR2, IL-10, IL-12 indicate the underlying changes in the host immune system, that further cause Th1-Th2 imbalance, after downstream trafficking of mutually antagonising other cytokines. So, the lesions of PKDL on the sunlight exposed body parts show the evidence of pathogenesis under UVR induced stimuli, as a result the dermal homing behaviour of Leishmania parasites is found.
Data availability
The authors declare that Data will be available on request basis of this work reported in this paper to the Corresponding Author.
Abbreviations
- PKDL :
-
Post Kala-azar Dermal Leishmaniasis
- UVR :
-
Ultraviolet radiations
- T-cells:
-
T-lymphocytes
- B-cells:
-
B-lymphocytes
- IL:
-
Interleukins
- IFN-γ:
-
Interferons Gamma
- TNF-α:
-
Tumor Necrotic Factors Alpha
- LC:
-
Langerhans cells
- TLR:
-
Toll-like receptors
- TNFRs:
-
Tumor Necrosis Factor Receptors
- NF-κβ:
-
Nuclear factor kappa-light chain-enhancer of activated B-cells
- ESA:
-
European Space Agency
- TEMIS:
-
Tropospheric Emission Monitoring Internet Service
- NASA:
-
The National Aeronautics and Space Administration
- CD cells:
-
Cluster of differentiation cell
- FACS:
-
Fluorescence activated cell sorting
References
Kumar, V. et al. Kala-azar elimination in a highly-endemic district of Bihar, India: A success story. PLoS Negl. Trop. Dis. 14, e0008254. https://doi.org/10.1371/journal.pntd.0008254 (2020).
Burza, S., Croft, S. L. & Boelaert, M. Leishmaniasis. Lancet 392, 951–970. https://doi.org/10.1016/S0140-6736(18)31204-2 (2018).
Priyamvada, K. et al. Visceral leishmaniasis outbreaks in Bihar: Community-level investigations in the context of elimination of kala-azar as a public health problem. Parasit. Vectors 14, 52. https://doi.org/10.1186/s13071-020-04551-y (2021).
Sinha, P. K. et al. Visceral leishmaniasis (kala-azar)—The Bihar (India) perspective. J. Infect. 53, 60–64 (2006).
Garapati, P. et al. Knowledge, stigma, health seeking behaviour and its determinants among patients with post kalaazar dermal leishmaniasis, Bihar, India. PLoS ONE 13, e0203407. https://doi.org/10.1371/journal.pone.0203407 (2018).
Basher, A. et al. A study on health seeking behaviors of patients of Post-Kala-Azar Dermal Leishmaniasis. Biomed. Res. Int. 2015, 314543. https://doi.org/10.1155/2015/314543 (2015).
Croft, S. L., Sundar, S. & Fairlamb, A. H. Drug resistance in leishmaniasis. Clin. Microbiol. Rev. 19, 111–126 (2006).
Thakur, C. P. Is elimination of kala-azar feasible by 2017?. Indian J. Med. Res. 144, 799–802 (2016). https://doi.org/10.4103/ijmr.IJMR_335_16
Thakur, C. P. & Thakur, M. Accelerating kala-azar elimination in India. Indian J. Med. Res. 152, 538–540. https://doi.org/10.4103/ijmr.IJMR_841_19 (2020).
Hirve, S. et al. Transmission dynamics of visceral leishmaniasis in the Indian subcontinent: A systematic literature review. PLoS Negl. Trop. Dis. 10, e0004896. https://doi.org/10.1371/journal.pntd.0004896 (2016).
Bhattacharya, S. K. & Dash, A. P. Elimination of Kala-Azar from the Southeast Asia Region. Am. J. Trop. Med. Hyg. 96, 802–804. https://doi.org/10.4269/ajtmh.16-0279 (2017).
Zijlstra, E. E., Alves, F., Rijal, S., Arana, B. & Alvar, J. Post-kala-azar dermal leishmaniasis in the Indian subcontinent: A threat to the South-East Asia Region Kala-azar Elimination Programme. PLoS Negl. Trop. Dis. 11, e0005877. https://doi.org/10.1371/journal.pntd.0005877 (2017).
Zijlstra, E. E., Musa, A. M., Khalil, E. A. G., El Hassan, I. M. & El-Hassan, A. M. Post-kala-azar dermal leishmaniasis. Lancet Infect. Dis. 3, 87–98 (2003).
Ismail, A. et al. The pathogenesis of post kala-azar dermal leishmaniasis from the field to the molecule: Does ultraviolet light (UVB) radiation play a role?. Med. Hypotheses 66, 993–999. https://doi.org/10.1016/j.mehy.2005.03.035 (2006).
Ramesh, V., Kaushal, H., Mishra, A. K., Singh, R. & Salotra, P. Clinico-epidemiological analysis of Post kala-azar dermal leishmaniasis (PKDL) cases in India over last two decades: A hospital based retrospective study. BMC Public Health 15, 1092. https://doi.org/10.1186/s12889-015-2424-8 (2015).
Zijlstra, E. E. et al. Report of the fifth Post-Kala-Azar Dermal Leishmaniasis Consortium Meeting, Colombo, Sri Lanka, 14–16 May 2018. Parasit. Vectors 13, 159. https://doi.org/10.1186/s13071-020-04011-7 (2020).
Mukhopadhyay, D., Dalton, J. E., Kaye, P. M. & Chatterjee, M. Post kala-azar dermal leishmaniasis: An unresolved mystery. Trends Parasitol. 30, 65–74. https://doi.org/10.1016/j.pt.2013.12.004 (2014).
Bernhard, G. H. et al. Environmental effects of stratospheric ozone depletion, UV radiation and interactions with climate change: UNEP Environmental Effects Assessment Panel, update 2019. Photochem. Photobiol. Sci. 19, 542–584. https://doi.org/10.1039/d0pp90011g (2020).
Barnes, P. W. et al. Environmental effects of stratospheric ozone depletion, UV radiation, and interactions with climate change: UNEP Environmental Effects Assessment Panel, Update 2021. Photochem. Photobiol. Sci. 21, 275–301. https://doi.org/10.1007/s43630-022-00176-5 (2022).
D’Orazio, J., Jarrett, S., Amaro-Ortiz, A. & Scott, T. UV radiation and the skin. Int. J. Mol. Sci. 14, 12222–12248. https://doi.org/10.3390/ijms140612222 (2013).
Lucas, R. M. et al. Human health in relation to exposure to solar ultraviolet radiation under changing stratospheric ozone and climate. Photochem. Photobiol. Sci. 18, 641–680. https://doi.org/10.1039/c8pp90060d (2019).
Bernard, J. J., Gallo, R. L. & Krutmann, J. Photoimmunology: how ultraviolet radiation affects the immune system. Nat. Rev. Immunol. 19, 688–701. https://doi.org/10.1038/s41577-019-0185-9 (2019).
Morabito, K., Shapley, N. C., Steeley, K. G. & Tripathi, A. Review of sunscreen and the emergence of non-conventional absorbers and their applications in ultraviolet protection. Int. J. Cosmet. Sci. 33, 385–390. https://doi.org/10.1111/j.1468-2494.2011.00654.x (2011).
Hammond, V., Reeder, A. I. & Gray, A. Patterns of real-time occupational ultraviolet radiation exposure among a sample of outdoor workers in New Zealand. Public Health 123, 182–187. https://doi.org/10.1016/j.puhe.2008.12.007 (2009).
Whiteman, D. C. et al. When to apply sunscreen: A consensus statement for Australia and New Zealand. Aust. N. Z. J. Public Health 43, 171–175. https://doi.org/10.1111/1753-6405.12873 (2019).
Patz, J. A., Campbell-Lendrum, D., Holloway, T. & Foley, J. A. Impact of regional climate change on human health. Nature 438, 310–317. https://doi.org/10.1038/nature04188 (2005).
Harlan, S. L. et al. Heat-related deaths in hot cities: Estimates of human tolerance to high temperature thresholds. Int. J. Environ. Res. Public Health 11, 3304–3326. https://doi.org/10.3390/ijerph110303304 (2014).
Asadgol, Z. et al. How climate change can affect cholera incidence and prevalence? A systematic review. Environ. Sci. Pollut. Res. Int. 27, 34906–34926. https://doi.org/10.1007/s11356-020-09992-7 (2020).
Akil, L., Ahmad, H. A. & Reddy, R. S. Effects of climate change on Salmonella infections. Foodborne Pathog. Dis. 11, 974–980. https://doi.org/10.1089/fpd.2014.1802 (2014).
Baker, R. E. et al. Infectious disease in an era of global change. Nat. Rev. Microbiol. 20, 193–205. https://doi.org/10.1038/s41579-021-00639-z (2022).
Lindsay, S. W. & Birley, M. H. Climate change and malaria transmission. Ann. Trop. Med. Parasitol. 90, 573–588. https://doi.org/10.1080/00034983.1996.11813087 (1996).
Paixao, E. S., Teixeira, M. G. & Rodrigues, L. C. Zika, chikungunya and dengue: The causes and threats of new and re-emerging arboviral diseases. BMJ Glob. Health 3, e000530. https://doi.org/10.1136/bmjgh-2017-000530 (2018).
Kurane, I. The effect of global warming on infectious diseases. Osong Public Health Res. Perspect. 1, 4–9. https://doi.org/10.1016/j.phrp.2010.12.004 (2010).
Dhara, V. R., Schramm, P. J. & Luber, G. Climate change & infectious diseases in India: Implications for health care providers. Indian J. Med. Res. 138, 847–852 (2013).
Nichols, G., Lake, I. & Heaviside, C. Climate change and water-related infectious diseases. J. Atmos. 9, 385. https://doi.org/10.3390/atmos9100385 (2018).
Noonan, F. P. & De Fabo, E. C. Immunosuppression by ultraviolet B radiation: Initiation by urocanic acid. Immunol. Today 13, 250–254. https://doi.org/10.1016/0167-5699(92)90005-R (1992).
Hart, P. H., Gorman, S. & Finlay-Jones, J. J. Modulation of the immune system by UV radiation: More than just the effects of vitamin D?. Nat. Rev. Immunol. 11, 584–596. https://doi.org/10.1038/nri3045 (2011).
Hart, P. H. & Norval, M. Ultraviolet radiation-induced immunosuppression and its relevance for skin carcinogenesis. Photochem. Photobiol. Sci. 17, 1872–1884. https://doi.org/10.1039/c7pp00312a (2018).
Rattis, F. M., Peguet-Navarro, J., Courtellemont, P., Redziniak, G. & Schmitt, D. Cis-urocanic acid failed to affect in vitro human Langerhans cell allostimulatory function. Photochem. Photobiol. 62, 914–916. https://doi.org/10.1111/j.1751-1097.1995.tb09155.x (1995).
de Fine Olivarius, F., Wulf, H. C., Crosby, J. & Norval, M. Isomerization of urocanic acid after ultraviolet radiation is influenced by skin pigmentation. J. Photochem. Photobiol. B 48, 42–47. https://doi.org/10.1016/S1011-1344(99)00007-X (1999).
Mohammad, T., Morrison, H. & HogenEsch, H. Urocanic acid photochemistry and photobiology. Photochem. Photobiol. 69, 115–135 (1999).
Norval, M. & Halliday, G. M. The consequences of UV-induced immunosuppression for human health. Photochem. Photobiol. 87, 965–977. https://doi.org/10.1111/j.1751-1097.2011.00969.x (2011).
Duthie, M. S., Kimber, I. & Norval, M. The effects of ultraviolet radiation on the human immune system. Br. J. Dermatol. 140, 995–1009. https://doi.org/10.1046/j.1365-2133.1999.02898.x (1999).
Matsumura, Y. & Ananthaswamy, H. N. Toxic effects of ultraviolet radiation on the skin. Toxicol. Appl. Pharmacol. 195, 298–308. https://doi.org/10.1016/j.taap.2003.08.019 (2004).
Simon, J. C., Tigelaar, R. E., Bergstresser, P. R., Edelbaum, D. & Cruz, P. D. Jr. Ultraviolet B radiation converts Langerhans cells from immunogenic to tolerogenic antigen-presenting cells Induction of specific clonal anergy in CD4+ T helper 1 cells. J. Immunol. 146, 485–491 (1991).
Lucas, R. M., Gorman, S., Geldenhuys, S. & Hart, P. H. Vitamin D and immunity. F1000Prime Rep. 6, 118. https://doi.org/10.12703/P6-118 (2014).
Das, S. et al. Cathelicidin augments VDR-dependent anti-leishmanial immune response in Indian Post-Kala-Azar Dermal Leishmaniasis. Int. Immunopharmacol. 50, 130–138. https://doi.org/10.1016/j.intimp.2017.06.010 (2017).
Glaser, R. et al. UV-B radiation induces the expression of antimicrobial peptides in human keratinocytes in vitro and in vivo. J. Allergy Clin. Immunol. 123, 1117–1123. https://doi.org/10.1016/j.jaci.2009.01.043 (2009).
Mandal, A. et al. TLR4 and TLR9 polymorphism: Probable role in susceptibility among the population of Bihar for Indian visceral leishmaniasis. Innate Immun. 27, 493–500. https://doi.org/10.1177/1753425920965658 (2021).
Song, H. J., Lee, S. H., Choi, G. S. & Shin, J. Repeated ultraviolet irradiation induces the expression of Toll-like receptor 4, IL-6, and IL-10 in neonatal human melanocytes. Photodermatol. Photoimmunol. Photomed. 34, 145–151. https://doi.org/10.1111/phpp.12359 (2018).
Chauhan, P., Shukla, D., Chattopadhyay, D. & Saha, B. Redundant and regulatory roles for Toll-like receptors in Leishmania infection. Clin. Exp. Immunol. 190, 167–186. https://doi.org/10.1111/cei.13014 (2017).
Behera, S. K., Das, S., Xavier, A. S., Selvarajan, S. & Anandabaskar, N. Indian Council of Medical Research’s National Ethical Guidelines for biomedical and health research involving human participants: The way forward from 2006 to 2017. Perspect. Clin. Res. 10, 108–114. https://doi.org/10.4103/picr.PICR_10_18 (2019).
Mathur, R., Thakur, K. & Hazam, R. K. Highlights of Indian council of medical research national ethical guidelines for biomedical and health research involving human participants. Indian J. Pharmacol. 51, 214–221. https://doi.org/10.4103/0253-7613.262456 (2019).
Mathur, R. & Swaminathan, S. National ethical guidelines for biomedical & health research involving human participants, 2017: A commentary. Indian J. Med. Res. 148, 279–283. https://doi.org/10.4103/0971-5916.245303 (2018).
Das, V. N. et al. Longitudinal study of transmission in households with visceral leishmaniasis, asymptomatic infections and PKDL in highly endemic villages in Bihar, India. India. PLoS Negl Trop Dis 10, e0005196. https://doi.org/10.1371/journal.pntd.0005196 (2016).
Das, V. N. et al. Repeated training of accredited social health activists (ASHAs) for improved detection of visceral leishmaniasis cases in Bihar. India. Pathog Glob Health 110, 33–35. https://doi.org/10.1080/20477724.2016.1156902 (2016).
Das, V. N. R. et al. The usefulness of trained field workers in diagnosis of post-kala-azar dermal leishmaniasis (PKDL) and clinico-epidemiological profile in highly endemic areas of Bihar. Trans R Soc Trop Med Hyg 113, 332–340. https://doi.org/10.1093/trstmh/trz007 (2019).
Lee, S. J. et al. Transglutaminase 2 mediates UV-induced skin inflammation by enhancing inflammatory cytokine production. Cell Death Dis 8, e3148. https://doi.org/10.1038/cddis.2017.550 (2017).
Chen, Y. et al. Effects of UV-B Radiation on the Content of Bioactive Components and the Antioxidant Activity of Prunella vulgaris L. Spica during Development. Molecules 23 (2018). https://doi.org/10.3390/molecules23050989
Park, J., Seok, J. K., Suh, H. J. & Boo, Y. C. Gardenia jasminoides Extract Attenuates the UVB-Induced Expressions of Cytokines in Keratinocytes and Indirectly Inhibits Matrix Metalloproteinase-1 Expression in Human Dermal Fibroblasts. Evid Based Complement Alternat Med 2014, 429246. https://doi.org/10.1155/2014/429246 (2014).
Jaswal, A. K., Narkhede, N. M. & Rachel, S. Atmospheric data collection, processing and database management in India Meteorological Department. Proc. Indian Natl. Sci. Acad. 80, 697–704 (2014).
Singh, S. et al. Assessment of satellite-retrieved surface UVA and UVB radiation by comparison with ground-measurements and trends over Mega-city Delhi. Atmos. Environ. 188, 60–70. https://doi.org/10.1016/j.atmosenv.2018.06.027 (2018).
Zempila, M. M. et al. TEMIS UV product validation using NILU-UV ground-based measurements in Thessaloniki, Greece. Atmos. Chem. Phys. 17, 7157–7174. https://doi.org/10.5194/acp-17-7157-2017 (2017).
Kishore, K., Jaswal, V., Kulkarni, V. & De, D. Practical guidelines to develop and evaluate a questionnaire. Indian Dermatol. Online J. 12, 266–275. https://doi.org/10.4103/idoj.IDOJ_674_20 (2021).
Wang, D. et al. Influence of sleep disruption on inflammatory bowel disease and changes in circadian rhythm genes. Heliyon 8, e11229. https://doi.org/10.1016/j.heliyon.2022.e11229 (2022).
Kumari, R. et al. Prevalence of iron deficiency and iron deficiency anaemia in adolescent girls in a tertiary care hospital. J. Clin. Diagn. Res. 11, BC04–BC06. https://doi.org/10.7860/JCDR/2017/26163.10325 (2017).
Lal, C. S. et al. Comparative analysis of serum zinc, copper, magnesium, calcium and iron level in acute and chronic patients of visceral leishmaniasis. J. Trace Elem. Med. Biol. 27, 98–102. https://doi.org/10.1016/j.jtemb.2012.09.007 (2013).
Sattar, N., Welsh, P., Panarelli, M. & Forouhi, N. G. Increasing requests for vitamin D measurement: Costly, confusing, and without credibility. Lancet 379, 95–96. https://doi.org/10.1016/S0140-6736(11)61816-3 (2012).
Bilinski, K. L. & Boyages, S. C. The rising cost of vitamin D testing in Australia: Time to establish guidelines for testing. Med. J. Aust. 197, 90. https://doi.org/10.5694/mja12.10561 (2012).
Chanput, W., Mes, J. J. & Wichers, H. J. THP-1 cell line: An in vitro cell model for immune modulation approach. Int. Immunopharmacol. 23, 37–45. https://doi.org/10.1016/j.intimp.2014.08.002 (2014).
Bosshart, H. & Heinzelmann, M. THP-1 cells as a model for human monocytes. Ann. Transl. Med. 4, 438. https://doi.org/10.21037/atm.2016.08.53 (2016).
Muirhead, K. A. et al. Methodological considerations for implementation of lymphocyte subset analysis in a clinical reference laboratory. Ann. N. Y. Acad. Sci. 468, 113–127. https://doi.org/10.1111/j.1749-6632.1986.tb42034.x (1986).
Landay, A. L. & Muirhead, K. A. Procedural guidelines for performing immunophenotyping by flow cytometry. Clin. Immunol. Immunopathol. 52, 48–60. https://doi.org/10.1016/0090-1229(89)90192-x (1989).
Holmes, K. L., Otten, G. & Yokoyama, W. M. Flow cytometry analysis using the Becton Dickinson FACS Calibur. Curr. Protoc. Immunol. https://doi.org/10.1002/0471142735.im0504s49 (2002).
Mazdiyasni, O. et al. Increasing probability of mortality during Indian heat waves. Sci. Adv. 3, e1700066. https://doi.org/10.1126/sciadv.1700066 (2017).
Kripke, M. L. & Morison, W. L. Modulation of immune function by UV radiation. J. Investig. Dermatol. 85, 62s–66s. https://doi.org/10.1111/1523-1747.ep12275479 (1985).
Hart, P. H. & Norval, M. More than effects in skin: Ultraviolet radiation-induced changes in immune cells in human blood. Front. Immunol. 12, 694086. https://doi.org/10.3389/fimmu.2021.694086 (2021).
Zughaier, S. M., Lubberts, E. & Bener, A. Editorial: Immune-modulatory effects of vitamin D. Front. Immunol. 11, 596611. https://doi.org/10.3389/fimmu.2020.596611 (2020).
Sassi, F., Tamone, C. & D’Amelio, P. Vitamin D: Nutrient, hormone, and immunomodulator. Nutrients https://doi.org/10.3390/nu10111656 (2018).
Varma, N. & Naseem, S. Hematologic changes in visceral leishmaniasis/kala azar. Indian J. Hematol. Blood Transfus. 26, 78–82. https://doi.org/10.1007/s12288-010-0027-1 (2010).
Salminen, A., Kaarniranta, K. & Kauppinen, A. Photoaging: UV radiation-induced inflammation and immunosuppression accelerate the aging process in the skin. Inflamm. Res. 71, 817–831. https://doi.org/10.1007/s00011-022-01598-8 (2022).
Clydesdale, G. J., Dandie, G. W. & Muller, H. K. Ultraviolet light induced injury: Immunological and inflammatory effects. Immunol. Cell Biol. 79, 547–568. https://doi.org/10.1046/j.1440-1711.2001.01047.x (2001).
Mosser, D. M., Hamidzadeh, K. & Goncalves, R. Macrophages and the maintenance of homeostasis. Cell Mol. Immunol. 18, 579–587. https://doi.org/10.1038/s41423-020-00541-3 (2021).
Murray, P. J. & Wynn, T. A. Protective and pathogenic functions of macrophage subsets. Nat. Rev. Immunol. 11, 723–737. https://doi.org/10.1038/nri3073 (2011).
Italiani, P. & Boraschi, D. From monocytes to M1/M2 macrophages: Phenotypical vs. functional differentiation. Front. Immunol. 5, 514. https://doi.org/10.3389/fimmu.2014.00514 (2014).
Kumar, V. et al. Leishmania donovani: Dynamics of L. donovani evasion of innate immune cell attack due to malnutrition in visceral leishmaniasis. Nutrition 30, 449–458. https://doi.org/10.1016/j.nut.2013.10.003 (2014).
Sengupta, R. et al. Active surveillance identified a neglected burden of macular cases of Post Kala-azar Dermal Leishmaniasis in West Bengal. PLoS Negl. Trop. Dis. 13, e0007249. https://doi.org/10.1371/journal.pntd.0007249 (2019).
Singh, A. K. et al. Cytokines and chemokines differentially regulate innate immune cell trafficking during post kala-azar dermal leishmaniasis. J. Cell Biochem. 119, 7406–7418. https://doi.org/10.1002/jcb.27048 (2018).
Panich, U., Sittithumcharee, G., Rathviboon, N. & Jirawatnotai, S. Ultraviolet radiation-induced skin aging: The role of DNA damage and oxidative stress in epidermal stem cell damage mediated skin aging. Stem Cells Int. 2016, 7370642. https://doi.org/10.1155/2016/7370642 (2016).
Ansary, T. M., Hossain, M. R., Kamiya, K., Komine, M. & Ohtsuki, M. Inflammatory molecules associated with ultraviolet radiation-mediated skin aging. Int. J. Mol. Sci. https://doi.org/10.3390/ijms22083974 (2021).
Dahl, M. V., McEwen, G. N. Jr. & Katz, H. I. Urocanic acid suppresses induction of immunity in human skin. Photodermatol. Photoimmunol. Photomed. 26, 303–310. https://doi.org/10.1111/j.1600-0781.2010.00550.x (2010).
Hug, D. H., Hunter, J. K. & Dunkerson, D. D. Malnutrition, urocanic acid, and sun may interact to suppress immunity in sojourners to high altitude. Aviat. Space Environ. Med. 72, 136–145 (2001).
Holick, M. F. Sunlight, UV radiation, vitamin D, and skin cancer: How much sunlight do we need?. Adv. Exp. Med. Biol. 1268, 19–36. https://doi.org/10.1007/978-3-030-46227-7_2 (2020).
Yoshida, Y. et al. Monocyte induction of IL-10 and down-regulation of IL-12 by iC3b deposited in ultraviolet-exposed human skin. J. Immunol. 161, 5873–5879 (1998).
Kang, K., Gilliam, A. C., Chen, G., Tootell, E. & Cooper, K. D. In human skin, UVB initiates early induction of IL-10 over IL-12 preferentially in the expanding dermal monocytic/macrophagic population. J. Investig. Dermatol. 111, 31–38. https://doi.org/10.1046/j.1523-1747.1998.00121.x (1998).
Rodgers, J. Labour force participation in rural Bihar: A thirty-year perspective based on village surveys. 1–30 (2012). https://www.ihdindia.org/PDFs/Labour_Force_Participation_in_Rural_Bihar_A_Thirty-Year_Perspective_based_on_Village_Surveys.pdf.
Acknowledgements
The authors sincerely acknowledge Department of Science and Technology, New Delhi for the financial Grant [DST/CCP/NHH/113/2017(G)]; and ICMR-RMRIMS, Patna for providing essential facilities for research as well as field study programs. The authors are grateful to Dr. Jos van Geffen and Dr. Ronald van der A of TEMIS team, ESA/KNMI, the Netherlands for their consistent help and technical support in satellite-based UV data monitoring and records. Also, we express sincere thanks to Dr. Sachidanand Singh, Principal Scientist, Division of Environmental Science and Biomedical Metrology at CSIR-National Physical Laboratory, New Delhi for his suggestion and discussion in this work. University of Calcutta, Kolkata is duly acknowledged for the Ph.D. program support to SB. The authors extend special thanks to Mrs. Parool Gupta for her constant help in experimental works and technical discussions. Finally, the technical supporting staff viz. Mr. Sudarshan Prasad, Mrs. Rakhi Kumari, Mr. Subhash Kumar; integrated field teammates; and all the PKDL patients along with the healthy individuals as study participants are heartily appreciated and deeply acknowledged.
Author information
Authors and Affiliations
Contributions
V.A. and S.K.S. conceived and designed the experiments. S.B., N.K., VA performed the experiments and other research works mentioned. S.B., V.A. analyzed the data and wrote the main draft of the manuscript. S.B., M.D.K., V.A., S.K.S., V.N.R., N.A. S., K.P. helped in field-based data acquisition analysis, as well as in immunological profiling of the PKDL patients and participated in the technical discussion, and V.A. reviewed, edited the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Behera, S., Kalim, M.D., Kumar, N. et al. Association of Post Kala-Azar Dermal Leishmaniasis pathogenesis with prolonged sunlight (ultraviolet radiations) exposure in VL endemic population of Bihar. Sci Rep 15, 25916 (2025). https://doi.org/10.1038/s41598-025-08738-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-08738-0
Keywords
This article is cited by
-
Post-Kala-Azar dermal leishmaniasis: a systematic review of immunopathogenesis, molecular diagnostics, and public health impact
Journal of Parasitic Diseases (2026)
