
Abstract
To assess myocardial functional abnormalities in ischemia with non-obstructive coronary arteries (INOCA) using adenosine stress myocardial contrast echocardiography (AS-MCE) combined with Myocardial Work (MW). 208 patients who underwent coronary angiography (CAG) or coronary computed tomography angiography (CCTA) due to chest pain at Shaanxi Provincial People's Hospital from January 2022 to April 2025 were selected. Among them, 62 patients with negative results from CAG or CCTA and positive results from AS-MCE were classified as the INOCA group, and 48 normal patients were classified as the control group. Conventional parameters were measured by two-dimensional ultrasound. The left ventricular global longitudinal strain (GLS) and MW parameters were obtained through the EchoPAC (v203) workstation. QLab (v10.8) was used to analyze AS-MCE images at rest and under stress in all subjects to obtain myocardial perfusion parameters: peak signal intensity (A-value), Perfusion intensity (β-value), and A × β -value (reflecting myocardial blood volume). The differences in these parameters between the two groups were compared. Under both resting and stress conditions, the β values of patients in the INOCA group were significantly different from those in the control group, and the CFR in the INOCA group was significantly different from that in the control group (P < 0.05, Table 2). AS-MCE effectively identifies microcirculatory dysfunction in INOCA, demonstrating superior diagnostic utility over MW for non-obstructive ischemia.
Similar content being viewed by others


Introduction
Ischemia with non-obstructive coronary arteries (INOCA) is a clinical condition characterized by ischemic chest pain and myocardial ischemia, but without obstructive coronary artery stenosis as detected by coronary angiography (CAG) or coronary computed tomography angiography (CCTA)1. It mainly includes two subtypes: microvascular angina (MVA) and epicardial coronary artery vasospasm2. INOCA patients present with a wide range of symptoms and signs. Up to 70% of patients with angina pectoris have no obstructive coronary artery disease (epicardial vessel stenosis ≥ 50%) detected by CAG or CCTA. It is more common in women than in men. Patients with INOCA typically present with chest pain or angina-like symptoms, shortness of breath, fatigue and reduced physical capacity. They may also experience palpitations, dizziness or syncope, nausea, indigestion, etc. Long-term and recurrent symptoms may lead to psychological distress, such as anxiety and depression. These symptoms and signs are often misdiagnosed as non-cardiac diseases, leading to insufficient clinical diagnosis or treatment and missing the effective treatment window3, which imposes a substantial healthcare burden on patients4. Compared with stable coronary artery disease, INOCA is reported to cause physical limitations, frequent angina pectoris, and a decline in quality of life. There are various physiological indicators for evaluating myocardial ischemia, such as fractional flow reserve (FFR) and coronary flow reserve (CFR), as well as the further penetration of intravascular ultrasound (IVUS) and optical coherence tomography to supplement the diagnostic ability of CAG for epicardial lesions and microvascular function assessment5. Myocardial contrast echocardiography (MCE), also known as myocardial acoustic contrast echocardiography, is a new technique applied in clinical practice in recent years that can display myocardial microcirculation perfusion in real time6. adenosine stress myocardial contrast echocardiography (AS-MCE) is a non-invasive functional imaging method for diagnosing coronary heart disease, which uses adenosine as a stressor and combines it with myocardial contrast echocardiography7,8. Myocardial Work (MW) is a new technology based on two-dimensional echocardiography, which analyzes changes in cardiac function through the variations of left ventricular pressure-strain loops (PSL)9. Compared with myocardial strain analysis, MW takes into account the influence of afterload on left ventricular myocardial contractile function, thereby improving the accuracy of cardiac function assessment. For patients with coronary heart disease where at least one coronary artery has a stenosis degree of ≥ 50%, MW parameters can detect abnormal myocardial metabolic levels when the left ventricular ejection fraction (LVEF) is still normal and no segmental wall motion abnormalities have occurred10. MW as an emerging technique, theoretically can assess left ventricular function through PSL, but its application in microcirculation disorders remains unclear. In contrast, AS-MCE, by directly evaluating myocardial perfusion, may be more suitable for microcirculation assessment in INOCA. This study aims to apply both adenosine stress echocardiography and MW to compare and evaluate the abnormal changes in patients with ischemia with no obstructive coronary arteries (INOCA), providing a new diagnostic approach for identifying INOCA.
Information and methods
Subjects
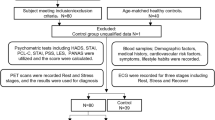
Patients who come to our hospital with clinical manifestations of chest tightness or pain will first undergo preliminary screening (electrocardiogram, myocardial enzyme detection, and echocardiography). If no obvious positive indicators are found, the patients are advised to undergo stress tests to detect reversible myocardial ischemia, including exercise electrocardiogram, stress echocardiography, myocardial perfusion imaging (MPI), and cardiac magnetic resonance (CMR). If necessary, CMR myocardial perfusion reserve index (MPRI) and PET myocardial blood flow quantification can be further conducted. If the patients have abnormalities, coronary angiography can be performed to rule out obstructive lesions (central coronary artery stenosis < 50%). If there is no stenosis, further assessment of microcirculation or spasm is required. Microvascular function assessment includes coronary flow reserve (CFR) and index of microcirculatory resistance (IMR), where CFR is measured by pressure wire, and CFR < 2.0 indicates microvascular dysfunction, while IMR ≥ 25 indicates increased microvascular resistance. Vascular spasm detection, such as acetylcholine or ergonovine provocation tests, can also induce spasm and observe chest pain, electrocardiogram changes, and angiographic confirmed vessel constriction (stenosis > 90% is positive). In this way, patients with INOCA disease manifestations can be selected. Sixty-two INOCA patients through coronary angiography (CAG) or coronary computed tomography angiography (CCTA) at Shaanxi Provincial People's Hospital from January 2022 to April 2025 were collected, including 26 males and 36 females, aged 38 to 82 years, with an average age of (60.5 ± 10.7) years. Forty-eight patients with no significant stenosis confirmed by CAG or CCTA and normal myocardial contrast echocardiography were selected as the control group, including 22males and 26 females, aged 27 to 82 years, with an average age of (56.4 ± 14.6) years. The LVEF of all subjects in both groups was ≥ 55%. Inclusion criteria: patients suspected of having INOCA. Exclusion criteria: poor cooperation or poor image quality, chronic kidney or liver damage, history of thyroid disease or tumors, coronary artery dilation, acute myocardial infarction, bronchial asthma, severe arrhythmia (second or third-degree atrioventricular block), clear allergy to adenosine or contrast agents, congenital heart disease or valvular disease, and hemodynamic instability.
This study was reviewed and approved by the Medical Ethics Committee of Shaanxi Provincial People's Hospital (Ethics Approval Number 2023-R032). All methods were carried out in accordance with the Declaration of Helsinki and in accordance with the Medical Research Involving Human Subjects Act (WMO).
Instruments and methods
Instruments
Philips EPIQ CVx cardiovascular ultrasound diagnostic instrument with M5Sc-D probe, equipped with MCE imaging mode, and QLab 10.4 and Echo PAC (version 203) analysis software were used. An IV pump, blood pressure monitor, and ultrasound ECG lead wires were prepared.
Methods
Clinical doctors and patients were instructed to discontinue beta-blockers, theophylline drugs, vasodilators, and specific foods and beverages (coffee, tea, cola, chocolate, and bananas) that might affect the test results 12–24 h before the examination11. Before the examination, the subjects' blood pressure was measured, and basic information such as height and weight was recorded. The examinee lies on the left side, breathing calmly, and connected to an electrocardiogram (ECG). After a routine cardiac ultrasound examination, the MCE test was conducted. A contrast agent for ultrasound was selected as perfluoropropane human albumin microspheres for injection (trade name: Lida Xing). A bolus injection of 1.0–1.5 ml was administered through the median cubital vein of the left forearm. The LVO mode was selected, and the contrast imaging conditions were adjusted to a low MI (< 0.3) real-time contrast imaging mode. The focal point was placed at the level of the left atrioventricular valve annulus. After the contrast agent filled the entire left ventricular cavity and the endocardial boundary was displayed, the Flash button was pressed successively to store the dynamic images of the first 5 and the last 15 cardiac cycles12. Subsequently, the adenosine stress test (AS test) was conducted. Adenosine was infused at a rate of 140 μg/ (kg·min) through another cubital vein. At 4 min, myocardial contrast echocardiography (MCE) was performed using the same method. When the patient showed signs of termination of the stress test, MCE was performed again, and the images were collected and saved. Offline analysis was then conducted. Throughout the AS test, electrocardiogram (ECG) monitoring was performed, and the patient's clinical symptoms were inquired at each level of load. Blood pressure and ECG were recorded.
Termination criteria for the stress test13
Severe arrhythmia, angina pectoris reaching the upper limit of tolerance, abnormal changes in ventricular wall motion compared to before, significant changes in the ST segment on ECG (ST segment depression of at least 0.1 mV in two or more adjacent leads), the subject reaching the target heart rate (120–180 beats per minute, within 170 beats per minute for the elderly), and significant changes in blood pressure (systolic blood pressure drop of more than 10 mmHg or ≥ 220/120 mmHg compared to before).
Image analysis criteria
(1) The AS-MCE data saved were analyzed by software. According to the 16-segment analysis method of the left ventricle14, regions of interest (5 mm × 5 mm) were set at the center of each segment, generating time-intensity curves. The first frame after Flash reperfusion was set as the starting point. The peak signal intensity (A -value), Perfusion intensity (β -value), and A × β -value (reflecting myocardial blood volume) were obtained through analysis. The average value of three measurements for each region was included in the statistics. (2) The saved data were imported into the Echo PAC (version 203) workstation for MW parameter detection. The endocardial boundary was traced according to the prompts to create regions of interest. The software displayed the automatically tracked results, obtaining the GLS value of the left ventricle. Entering the MW mode, the brachial artery cuff pressure was input to obtain the left ventricular PSL and directly obtain the global work index (GWI), global work efficiency (GWE), global constructive work (GCW), and global waste work (GWW).
Statistical methods
Data were analyzed using SPSS 22.0 software. Some measurement data conformed to a normal distribution and were expressed as (x ± s), with independent sample t-tests used for comparisons between groups. Some measurement data did not conform to a normal distribution, and Mann–Whitney U tests were used for comparisons between groups. Count data were expressed in terms of cases, and χ2 tests or Fisher's exact probability method were used for comparisons between groups. A P value < 0.05 was considered statistically significant.
Results
Comparison of two groups of subjects in general
Among the 110 patients, compared with the control group, there were no significant differences in gender, age, heart rate, weight, height, body surface area, prevalence of hypertension and diabetes, hyperlipidemia, and conventional ultrasound parameters such as left atrial diameter, left ventricular end-systolic diameter and volume, end-diastolic diameter and volume, LVEF, diastolic mitral valve orifice velocity, E/A, e, EDT, and E/e' (P > 0.05, Table 1).
Comparison of myocardial blood flow perfusion parameters between the two groups
Under both resting and stress conditions, the β values of patients in the INOCA group were significantly different from those in the control group, and the CFR in the INOCA group was significantly different from that in the control group (P < 0.05, Table 2).
Comparison of GLS and MW parameters
Compared with the control group, there were no significant differences in GLS, GWI, GCW, GWE, and GWW parameters in the INOCA group (P > 0.05, Table 1).
Discussion
Over the past two decades, research has shown that coronary microvascular dysfunction (CMD) and coronary artery spasm (CAS) are important mechanisms leading to myocardial ischemia. Currently, non-invasive functional imaging methods such as transthoracic echocardiography coronary flow imaging, positron emission tomography, single photon emission computed tomography, cardiac magnetic resonance imaging, and myocardial contrast echocardiography (MCE) can be used to evaluate the coronary microcirculation in patients with ischemia not due to obstructive coronary artery disease (INOCA)1. When non-invasively assessing the coronary microcirculation, drugs are also used to induce maximum dilation of the coronary circulation, and the inducing drugs and intravenous infusion methods are the same as those used in invasive examinations. Coronary flow reserve (CFR) is the ratio of blood flow when the coronary artery is maximally dilated to that at rest, and it is an important indicator of coronary microcirculation dysfunction (CMD)15. In recent years, non-invasive methods for evaluating CFR have received increasing attention. Studies have confirmed that to obtain accurate CFR, non-invasive imaging techniques must accurately capture the basal myocardial blood flow and the maximum myocardial blood flow during maximum coronary artery hyperemia, that is, the imaging technique must simultaneously accurately capture the peak time and peak efficiency of myocardial perfusion. The results of CFR measured by AS-MCE are consistent with those obtained by PET imaging and CAG16. AS-MCE can also be combined with strain rate or three-dimensional speckle tracking to assess myocardial viability, etc.17. Currently, Doppler technology is also used to measure coronary flow velocity reserve, and its feasibility range is 66–100% depending on the machine and the use of contrast agents, with 89% of the examinations considered high quality. Coronary flow velocity reserve is usually measured in the left anterior descending artery (LAD), and the success rate is higher compared to other arteries18. MCE technology can display myocardial perfusion at the microcirculation level in real-time, not only analyzing related data19 but also carrying prognostic information20.
Unlike coronary heart disease, the proportion of female patients is higher (up to 50–70%)1. It has also been pointed out that abnormal regulation of vascular endothelial function by estrogen may increase the risk of microvascular dysfunction21. In this study, it was also reflected that there were more female patients. Among the 110 patients in this study, there were no significant differences between the two groups in terms of gender, age, heart rate, weight, height, body surface area, hypertension, and diabetes. There might be an imbalance in baseline characteristics (such as age, gender, and disease stage) between the INOCA group and the control group, or uncontrolled confounding factors, such as concomitant medications and dietary habits. In subsequent studies, the sample size will be increased and multicenter research will be conducted.
The most common microvascular causes of myocardial infarction in INOCA are thromboembolism (left heart-related coronary microcirculation occlusion, paradoxical embolism caused by dx-sn shunt or hereditary prothrombotic disorders) or microvascular spasm. It has also been reported22 that the microvascular effects of insulin are impaired in INOCA patients with insulin resistance, diabetes, obesity, and hypertension. Although impaired vasodilation is the most common identifiable symptom mechanism in effort angina patients, microvascular spasm is usually associated with rest angina and sometimes with acute manifestations23.
In this study, the parameters of LAD, LVIDd, LVEDV, LVIDs, LVESV, etc. in the two groups were compared, and there was no significant difference. The parameters of e, E/A, E/e, and EDT in the INOCA group were not significantly different from those in the control group, which is contrary to the results of Zhang Hebin et al.24. The authors hypothesize that coronary microcirculatory dysfunction exists in the INOCA group, but it is not severe enough to cause changes in the morphology and structure of the left atrium left ventricle and the left ventricular systolic and diastolic functions.
Under both resting and stress conditions, the β values of patients in the INOCA group were significantly different from those in the control group, and the CFR in the INOCA group was significantly different from that in the control group (P < 0.05, Table 2). This indicates that AS-MCE can effectively identify microcirculatory dysfunction in INOCA, demonstrating its superiority in the diagnosis of non-obstructive ischemia (Fig. 1).

Quantitative analysis of contrast echocardiography of the left ventricular lateral wall in the INOCA group: After the drug load test (b), the contrast agent filling rate was significantly slower (Wash-in Slope 0.09 dB/s) compared to before the test (a), the time to peak was delayed (TTP 13.40 s), the peak intensity was reduced (Peak Intensity 1.27 dB), and the total contrast agent flow was significantly decreased (AUC 8.3 dB·s). This perfusion pattern (One Minus Exp curve) highly suggests that there is myocardial blood flow perfusion impairment in this area, and the possible cause may be microcirculation dysfunction. (a) Myocardial perfusion time-intensity curve of the left ventricular lateral wall in INOCA patients before drug stress test. (b) Myocardial perfusion time-intensity curve of the left ventricular lateral wall in INOCA patients after drug stress test.
Echocardiographic MW is a way to quantitatively evaluate the overall and segmental left ventricular function, it non-invasively estimates the left ventricular pressure and myocardial strain through the pressure-strain curve. Wang Yan et al. proposed that in the mild coronary heart disease group, GLS, GWI, GCW, GWE, and GWW were not significantly different from the control group (P > 0.05)10, and the data analysis results were consistent with this (Fig. 2). Some studies have also pointed out that the ischemia in INOCA may be more diffuse or limited to the microcirculation, and it is not clear whether resting GLS can reflect such abnormalities25, indicating that when there is no obvious coronary stenosis, the MW performance shows no significant difference. This does not mean that it is completely unable to reflect microvascular lesions, but rather that its core principle and parameter calculation method determine that it mainly reflects the overall contractile function and energy efficiency of the myocardium, and is indirect and relatively insensitive to perfusion and metabolic changes at the microvascular level. It mainly relies on changes in the macroscopic contractile function (strain) of the myocardium. Early or mild microvascular lesions may not affect myocardial contractile function, so MW parameters may remain normal. MW detects microvascular lesions usually indirectly and with a lag (when the lesion leads to myocardial dysfunction). In contrast, techniques such as myocardial contrast echocardiography (MCE) and coronary flow reserve (CFR) are the gold standards or main methods for directly and sensitively assessing coronary microvascular function.

LV pressure-strain rings and each MW parameter in patients in the INOCA group. The GWI and GWW were slightly lower than in the control group, the rest of the MW parameters were in the normal range, the area of the LV pressure-strain ring was slightly reduced, with the values remaining high overall.
Limitations of this study: (1) Due to the multiple inclusion criteria of patients and the complexity of the detection methods, the sample size was small and it was a single-center study. The lack of longitudinal follow-up in the INOCA group limits the interpretation of the prognostic value of AS-MCE and MW in INOCA; (2) The evaluation of MW showed no significant difference in parameters between the INOCA group and the control group, which may be due to the mild condition of INOCA patients and further verification is needed; (3) The accuracy of MCE is easily affected by image quality, so samples with unclear images were excluded; (4) This study discusses INOCA as a unified entity. As INOCA encompasses various pathophysiological conditions (such as microvascular angina and vasospastic angina), the lack of differentiation may dilute specific outcomes. Further in-depth research will be conducted subsequently. (5) The impact of perfusion or MW outcomes was not analyzed in combination with important confounding factors, such as concurrent medication use, dietary patterns, and baseline cardiovascular risk characteristics.
This study demonstrates that AS-MCE can effectively identify microcirculation dysfunction in INOCA by directly evaluating myocardial perfusion parameters (such as β values), while the application of MW technology in such patients may be limited by its reliance on global function analysis. Future studies need to expand the sample size and include more clinical endpoints (such as cardiovascular events) to verify the prognostic value of AS-MCE.
Data availability
All data generated or analysed during this study are included in this published article [and its supplementary information files].
References
Chinese Society of Cardiovascular Disease, & Chinese Journal of Cardiovascular Disease Editorial Committee. Chinese expert consensus on the diagnosis and management of ischemia with non-obstructive coronary artery disease. Chin. J. Cardiovasc. Dis. 50(12), 1148–1160. https://doi.org/10.3760/cma.j.cn112148-20220908-00682 (2022) (In Chinese).
Zhao, L. et al. Evaluation of left ventricular function in ischemia with non-obstructive coronary arteries: A research based on adenosine stress myocardial contrast echocardiography. Int. J. Cardiovasc. Imaging 39(2), 349–357. https://doi.org/10.1007/s10554-022-02740-7 (2023).
Kunadian, V. et al. An EAPCI expert consensus document on ischemia with non-obstructive coronary arteries in collaboration with the European society of cardiology working group on coronary pathophysiology & microcirculation endorsed by coronary vasomotor disorders international study group. Eur. Heart J. 41(37), 3504–3520. https://doi.org/10.1093/eurheartj/ehaa503 (2020).
Zhang, J. et al. Early diagnosis of coronary microvascular dysfunction by myocardial contrast stress echocardiography. Math. Biosci. Eng. 20(5), 7845–7858. https://doi.org/10.3934/mbe.2023339 (2023).
Ahn, S. et al. Discordance between fractional flow reserve and coronary flow reserve: Insights from intracoronary imaging and physiological assessment. J. Am. Coll. Cardiol. Intv. 10(10), 999–1007. https://doi.org/10.1016/j.jcin.2017.03.006 (2017).
Fang, J. et al. Clinical study on quantitative evaluation of myocardial perfusion in patients with coronary artery disease by myocardial contrast dobutamine loading echocardiography. Adv. Cardiovasc. Dis. 42(8), 742–747. https://doi.org/10.16806/j.cnki.issn.1004-3934.2021.08.017 (2021) (In Chinese).
Wu, J.-F. et al. Clinical application of adenosine-loaded myocardial acoustic imaging. Chin. J. Med. Ultrasound (Electron. Ed.) 16(10), 723–726. https://doi.org/10.3877/cma.j.issn.1672-6448.2019.10.002 (2019) (In Chinese).
Wu, H. & Xiao, Z. A knowledge graph-based analytical model for mining clinical value of drug stress echocardiography for diagnosis, risk stratification and prognostic evaluation of coronary artery disease. Int. J. Cardiol. 387, 131107. https://doi.org/10.1016/j.ijcard.2023.05.057 (2023).
Minghu, X. I. A. O. et al. Myocardial work in non-obstructive hypertrophic cardiomyopathy. Chin. J. Ultrasound Med. 37(6), 649–651. https://doi.org/10.3969/j.issn.1002-0101.2021.06.015 (2021).
Yan, W. A. N. G. et al. Diagnostic value of left ventricular systolic function in patients with left anterior descending stenosis by ultrasound myocardial work technique. Chin. J. Med. Imaging 31(4), 349–355. https://doi.org/10.3969/j.issn.1005-5185.2023.04.010 (2023).
Pellikka, P. A. et al. Guidelines for performance, interpretation, and application of stress echocardiography in ischemic heart disease: From the American Society of Echocardiography. J. Am. Soc. Echocardiography 33(1), 1–41. https://doi.org/10.1016/j.echo.2019.07.001 (2020).
Ling, C. et al. Comparison of the detection of apical ventricular wall tumor and its attached thrombus in patients with coronary artery disease by left heart cavity acoustic imaging and transthoracic echocardiography. J. Pract. Heart Brain Lung Blood Vessel Dis. 28(12), 109–112. https://doi.org/10.31083/j.rcm2501022 (2020).
Zhe, C. H. E. N. et al. Adenosine-loaded myocardial ultrasonography to evaluate myocardial perfusion abnormalities in patients with hypertrophic cardiomyopathy. Chin. J. Ultrasonography 32(1), 3–9. https://doi.org/10.3760/cma.j.cn131148-20220731-00528 (2023).
Schroder, J. & Prescott, E. Doppler echocardiography assessment of coronary microvascular function in patients with angina and no obstructive coronary artery disease. Front. Cardiovasc. Med. 8, 723542. https://doi.org/10.3389/fcvm.2021.723542 (2021).
Gulati, M. et al. AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: A report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J. Am. College Cardiol. 78(22), e187–e285. https://doi.org/10.1016/j.jacc.2021.07.053 (2021).
Liu, J. et al. Clinical application of loaded myocardial ultrasonography for determination of coronary flow reserve. Chin. J. Clin. Med. Imaging 31(3), 180–183. https://doi.org/10.12117/jccmi.2020.03.008 (2020).
Chieh-Chieh, Lv. et al. Diagnostic value of adenosine-loaded myocardial acoustic imaging in chronic coronary syndrome. Chin. J. Ultrasound Med. 36(9), 805–809. https://doi.org/10.3969/j.issn.1002-0101.2020.09.011 (2020).
Al-Mohaissen, M. A. Echocardiographic assessment of primary microvascular angina and primary coronary microvascular dysfunction. Trends Cardiovasc. Med. https://doi.org/10.1016/j.tcm.2022.02.007 (2022).
Billig, S. et al. Comparative assessment of coronary physiology using transthoracic pulsed-wave Doppler and myocardial contrast echocardiography in rats. Eur. Radiol. Exp. 7(1), 6. https://doi.org/10.1186/s41747-022-00319-4 (2023).
Mygind, N. D. et al. Myocardial first-pass perfusion assessed by cardiac magnetic resonance and coronary microvascular dysfunction in women with angina and no obstructive coronary artery disease. Scand. J. Clin. Lab. Invest. 79(4), 238–246. https://doi.org/10.1080/00365513.2019.1587670 (2019).
Reynolds, H. R. et al. Natural history of patients with ischemia and no obstructive coronary artery disease: The CIAO-ISCHEMIA study. Circulation 144(13), 1008–1023. https://doi.org/10.1161/CIRCULATIONAHA.120.046791 (2021).
Vink, C. E. M. et al. Reduced microvascular blood volume as a driver of coronary microvascular disease in patients with nonobstructive coronary artery disease: Rationale and design of the MICORDIS study. Front. Cardiovasc. Med. 8, 730810. https://doi.org/10.3389/fcvm.2021.730810 (2021).
Del Buono, M. G. et al. Coronary microvascular dysfunction across the spectrum of cardiovascular diseases: A JACC state-of-the-art review. J. Am. College Cardiol. 78(13), 1352–1371. https://doi.org/10.1016/j.jacc.2021.07.042 (2021).
Zhang, H.-B. et al. Correlation analysis of left ventricular rotational and torsional motion characteristics with myocardial perfusion in patients with coronary slow flow. Chin. J. Med. Ultrasound (Electron. Ed.) 17(4), 320–326. https://doi.org/10.3877/cma.j.issn.1672-6448.2020.04.006 (2020).
Davis, E. F. et al. Global longitudinal strain as predictor of inducible ischemia in no obstructive coronary artery disease in the CIAO-ISCHEMIA study. J. Am. Soc. Echocardiogr. 37(1), 89–99. https://doi.org/10.1016/S0735-1097(21)02749-2 (2024).
Funding
Supported by the Shaanxi Provincial People’s Hospital Top-notch Talent Project (2023BJ-01) and the Xi’an Science and Technology Plan Project (23YXYJ0110).
Author information
Authors and Affiliations
Contributions
Zhang Xuemei proposed the main research objectives, was responsible for the conception and design of the study, wrote the paper, implemented the research, developed the research ideas, controlled the quality, and reviewed and revised the final version, taking overall responsibility for the paper and supervising the management. Li Yuhuan designed the research plan, wrote and revised the paper, conducted statistical processing, and drew the tables. Li Fengsheng revised the paper. Dou Shuixiu, Zhang Feifei, Lou Ping, Jin Jing, Zhao Ying, and Zhao Xin collected and organized the data.
Corresponding author
Ethics declarations
Competing interest
The authors declare no competing interests.
Ethical approval
Ethical approval for this study was given by the Medical Ethics Committee of Shaanxi Provincial People's Hospital (Ethics Approval Number 2023-R032). This study was performed in line with the principles of the Declaration of Helsinki for the involvement of humans.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, X., Dou, S., Zhang, F. et al. Adenosine stress myocardial perfusion imaging and myocardial work in evaluating INOCA. Sci Rep 15, 26129 (2025). https://doi.org/10.1038/s41598-025-10614-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-10614-w
