
Abstract
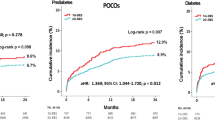
The effects of hyperglycemia on the prognosis of MI patients remain uncertain. This investigation evaluates the prognostic significance of hyperglycemia upon hospital admission in patients with ST-Elevation Myocardial Infarction and assesses how diabetes mellitus (DM) affects its prognostic relevance. This cross-sectional study examined data from 334 patients diagnosed with ST-segment elevation acute coronary syndrome, obtained from the Persian Cardiovascular Disease Registry. The study assessed hospital and one-year mortality as primary outcomes. Furthermore, cut-off points for blood glucose level on admission were determined and the predictive value of these cut-off values was analyzed using logistic regression analysis. In-hospital and one-year mortality rates were 22.1% and 26% for diabetic patients, and 20.2% and 24.1% for non-diabetic patients, with no substantial discrepancy between the groups (P = 0.607, P = 0.401). ROC curve analysis determined the admission blood glucose cut-off for predicting hospital mortality at 214 mg/dl in patients with diabetes (AUC = 0.66) and 148 mg/dl in patients without diabetes (AUC = 0.71). Blood glucose values was an independent factors related to in-hospital mortality, with odds ratios of 3.78 (95% CI 1.33–10.68, P = 0.012) for diabetics and 3.07 (95% CI 1.25–7.51, P = 0.014) for non-diabetics. Additionally, heightened admission glucose was correlated with greater mortality in one year in patients affected with MI irrespective of diabetes status. Blood glucose levels at admission independently predicted increased risk of mortality both during hospitalization and at one-year follow-up in patients with MI, with a notable effect on non-diabetic patients.
Similar content being viewed by others
Introduction
Coronary heart disease (CHD) is a significant contributor to both morbidity and mortality on a global scale. Acute myocardial infarction (MI) is the most prevalent form of CHD. Annually, it is documented that a minimum of 15% of deaths result from myocardial infarction, predominantly manifesting as ST-elevation myocardial infarction (STEMI)1,2. Despite the advancements in timely and effective revascularization and pharmacological interventions that have enhanced clinical outcomes for acute myocardial infarction (AMI), the mortality rate associated with AMI continues to be high3,4. Furthermore, the presence of concurrent medical conditions on patient outcomes is significant in this context, with diabetes mellitus being a prominent comorbidity observed in STEMI patients. Patients diagnosed with an acute heart attack and diabetes face a risk of mortality in the short and long term which is over twice that of those without diabetes5,6. Numerous studies have shown a positive relationship between adverse outcomes of acute myocardial infarction (AMI) and glucose-related variables, including serum glycosylated hemoglobin (HbA1c), fasting glucose levels, as well as admission hyperglycemia (AH) and post-admission hyperglycemia7,8,9,10. Hyperglycemia is regarded as a significant prognostic indicator in patients with and without diabetes admitted with an acute heart attack11,12. Although acute hyperglycemia is a common condition, there are no available standardized and commonly accepted threshold values in the literature13. The Scientific Statement from the American Heart Association on Hyperglycemia and Acute Coronary Syndrome suggested a limit for the “random glucose” level at admission, recommending a maximum of 140 mg/dl. This recommendation is supported by research showing that higher glucose values are linked to higher death rates in one month and 1 year after admission14,15. Since patients with diabetes and those without have different glucose metabolism mechanisms, the serum glucose threshold at admission for predicting mortality should be adjusted16. However, the majority of research employed the same prognostic threshold regardless of the presence of diabetes, which somewhat impacted the predictive significance of glucose levels on admission, particularly in individuals with both diabetes and AMI17. Concerning the heterogeneity of analyzed groups and conflicting report results on the predictive significance of blood glucose level, this study was carried out to determine the optimal numerical value of the glucose cut-off point, in patients with and without diabetic with ST-segment elevation acute myocardial infarction, as well as identifying the relationship of hyperglycemia during hospital admission with prognosis and hospital mortality.
Materials and methods
Study populations
In the cross-sectional design, all consecutive diabetic and non-diabetic patients hospitalized for ST‐elevation myocardial infarction (STEMI) were included. AMI was defined based on the recent guidelines, including ST‐elevation myocardial infarction (STEMI)18. The required data for this study were obtained from the Persian Cardiovascular Disease Registry (PROVE). PROVE is a registry that collects patient data from hospitals and outpatient clinics. Initiated in late 2014 and officially launched in March 2015. Data for the PROVE registry was gathered using two methods: the cold pursuit method, which involved extracting patient information from medical records, and the hot pursuit method, where data was obtained through face-to-face interviews with patients. Additionally, a dedicated website was developed to provide a brief introduction to the PROVE program. Long-term follow-up of patients was conducted over one year through phone calls and in-person visits.
For this cross-sectional investigation, data from about 334 individuals who attended 2022 Madani Heart Hospital, Tabriz University of Medical Science, Tabriz, Iran were selected.
The sample size for this study was calculated using Cochran’s formula. Given the target population (N = 2500) and an error rate of 0.05, the required sample size is 300 individuals. Considering a probable 10% missing data, the sample size was increased to 334. This sample size enables us to obtain precise results and allows for a valid assessment of the variables under investigation. With the calculated sample size, our study is designed to achieve a statistical power of 80%. This level of power allows for the detection of significant effects at an alpha level of 0.05, which is essential for the validity of the final results.
Inclusion criteria were diabetic and non-diabetic patients with chest pain lasting more than 30 min. Also, participants were required to exhibit ST-segment elevation exceeding 0.2 mV in anterior leads or greater than 0.1 mV in non-anterior leads, along with ST-segment elevation observed in two contiguous electrocardiogram leads within 24 h following the onset of symptoms. Exclusion criteria were as follows: patients with severe heart failure or cardiogenic shock (Killip class III or IV), patients with renal disorders undergoing hemodialysis, autoimmune diseases, malignancies, and age < 18 years old. Comprehensive clinical information was collected, including demographics, medical history, laboratory results, and echocardiogram parameters. Comorbidities, diabetes mellitus, hypertension, and one-year mortality were among the medical history characteristics that were evaluated. In addition, complete information on blood glucose levels recorded at the time of admission was also obtained.
Given the variations in glucose metabolism, distinct cut-off values for predicting hospital mortality in patients with acute myocardial infarction (AMI) are necessary for those with and without diabetes. Patients were classified into diabetic and non-diabetic groups based on data from the previous laboratory results of patients which acquired from HIS (Health Information System), recall from the patients and the caregivers of patients about his/her medication consumption and the admission glucose level and fasting blood sugar. Significant threshold measures for admission glucose levels were determined through receiver operating characteristic (ROC) curves. These threshold measures were subsequently utilized in multivariate analysis to assess their predictive value.
The research received approval from the Ethics Committee of TBZMED (IR.TBZMED.REC.1403.375). This study adhered to the guidelines outlined in the Declaration of Helsinki, ensuring that all participants were fully informed about their involvement in the registry and granted informed consent for the anonymous dissemination of scientific findings.
Study endpoints
In-hospital mortality and one-year mortality were chosen as the primary endpoints. A multivariate test was conducted to define independent predictors of hospital and one-year mortality.
Statistical analysis
Continuous variables were presented as median values with interquartile ranges (IQR) and were compared using the Wilcoxon rank-sum test. Categorical variables were reported as frequency (percentage) and were evaluated using either the chi-square test or Fisher’s exact test. ROC curve analyses were conducted to assess the optimal threshold point for admission glucose levels in predicting in-hospital mortality. Univariate logistic regression was initially utilized to determine influencing factors in both diabetic and non-diabetic groups. The Significant covariates and confounders were then included in the following multivariate regression models. The following potential covariates first were included in the univariate model: Hypertension, Dyslipidemia, LDL-c, HDL-c, TG, TC, consumed medications, Age, gender, Smoking status, Glucose level at admission, creatinine , BMI, history of congestive heart failure, HbA1c, hemoglobin levels, and left‐ventricular ejection fraction and the significant variables were chosen for multivariate regression models. Logistic regression was conducted to assess the effect of blood glucose levels at admission based on new cut-offs on hospital and one-year mortality. Analyses were conducted as two-sided, with a P value of less than 0.05 deemed statistically significant.
Results
Study population
As presented in Table 1, about 334 AMI patients attended the study including 131 patients with diabetes and 203 patients without diabetes. The median age of the patients with diabetes was 64(5571) years, of which 81.7% were men and 18.3% were women. Also. The median age of non-diabetes patients was 63(5570) years, with 78.3% men and 21.7% women. Compared with non-diabetes, individuals in the diabetes group are characterized by a higher prevalence of hypertension (32.1%) and hyperlipidemia (22.1%). The clinical outcome of patients is displayed in Table 2. In-hospital mortality, one-year mortality, and death type (cardiac, non-cardiac) did not vary between the two groups. The risk differences and 95% CI are shown in Table 2. The glucose values at admission in the non-diabetes group (130(106,166) mg/dl) were significantly less than those of the other group (191(133,324) mg/dl) (P < 0.001).
Patient treatment
Revascularization timing and strategy
All included patients underwent primary PCI as the revascularization strategy. The median of first medical contact to device (FTD) time was 240 min.
Coronary anatomy
The majority of patients had single-vessel disease (40.4%), with the most common culprit lesion located in the Left Anterior Descending artery (LAD: 14.2%) followed by the Right Coronary Artery (RCA: 9.7%) and Left Circumflex Artery (LCx: 4.8%). Multi-vessel disease was also frequent, including two-vessel (26.8%) and three-vessel disease (32.8%).
Post-PCI complications
Major post-PCI complications included bleeding, cardiogenic shock, pulmonary edema, cerebrovascular accidents, and secondary VF/VT, occurring in 0.1%, 2.2%, 0.2%, 0%, and 0.9% of cases, respectively.
Determination of cut-off point for glucose level at admission
The ROC analysis was utilized to define the threshold of glucose levels at admission, which may predict the mortality of patients with acute myocardial infarction (AMI) in the hospital, both in those with and without diabetes (see Fig. 1A, B and Table 3). For the diabetic group, the significant cut-off value was found to be 214 mg/dl, with an area under the curve (AUC) of 0.66, a sensitivity of 69%, and a specificity of 61% (P = 0.006). In the non-diabetic group, a significant threshold was 148 mg/dl, with an AUC of 0.71, a sensitivity of 67%, and a specificity of 75% (P < 0.001). The AUC is 0.66 (95% CI 0.56–0.76), indicating moderate predictive ability for the cut-off of 214 mg/dl in the diabetes group, while the AUC is 0.71 (95% CI 0.62–0.80) in the non-diabetes group, suggesting a better predictive ability compared to the diabetes group.

ROC curve of Glucose level at admission predicting hospital mortality of patients with AMI. (A) The ROC curve of Glucose level at admission to predict hospital mortality for patients with AMI with diabetes. (B) The ROC curve of Glucose level at admission to predict hospital mortality for patients with AMI without diabetes. AMI, acute myocardial infarction; AUC, area under curve; ROC, receiver operating characteristic.
Predictors of in-hospital mortality
A multivariate logistic regression test was conducted to assess whether admission glucose level based on the new cut-off point (Glucose at admission ≥ 214 mg/dl in diabetes patients and ≥ 148 mg/dl in patients without diabetes) was an independent predictor of hospital mortality (Table 4). It is proved that in patients with diabetes, admission glucose level ≥ 214 mg/dl is an independent risk factor of higher hospital mortality (OR = 3.78; 95% CI 1.33–10.68; P = 0.012). Also, hypertension (OR = 3.41; 95% CI 1.19–9.77; P = 0.022) and dyslipidemia (OR = 4.09; 95% CI 1.30–12.86; P = 0.016) appeared to be the determinant factor hospital mortality in patients with diabetes. Female gender was negatively related to hospital mortality (OR = 0.16; 95% CI 0.02–0.91; P = 0.039) (Table 4). In the non-diabetes group, glucose level at admission was also the factor affecting in-hospital mortality (OR = 3.07; 95% CI 1.25–7.51; P = 0.014). Hypertension (OR = 3.40; 95% CI 1.36–8.51; P = 0.009) and dyslipidemia (OR = 4.92; 95% CI 1.75–13.80; P = 0.002) were also positively correlated with in-hospital mortality and the female gender was related with decreased hazard of in-hospital mortality in non-diabetes patients (OR = 0.29; 95% CI 0.09–0.93; P = 0.038) (Table 4).
Predictors of one-year mortality
As tabulated in Table 5, glucose level at admission ≥ 214 mg/dl (OR = 3.40; 95% CI 1.32–8.75; P = 0.011) in diabetes patients and ≥ 148 mg/dl (OR = 4.21; 95% CI 1.79–9.87; P = 0.001) in patients without diabetes was independent predictors of 1-year mortality. Furthermore, hypertension was related to 3.03 times (95% CI 1.15–7.96; P = 0.024) and 3.67 times (95% CI 1.54–8.72; P = 0.003) extended hazard of 1-year mortality in patients with and without diabetes and AMI respectively.
Discussion
This study investigated the association of glucose levels at admission and mortality outcomes in patients with acute myocardial infarction (AMI) with and without diabetes. Our results suggest that increased glucose levels at admission are a significant predictor of both in-hospital and one-year mortality in AMI patients, regardless of diabetes status.
Our findings and previous studies highlighted the importance of admission glucose levels as a predictor of mortality in AMI patients19. A systematic review by Capes SE et al. concluded that elevated glucose levels on admission serve as an important predictor for poor outcomes, particularly in patients with existing diabetes20. Furthermore, the results of recent metanalysis revealed that admission blood glucose was remarkably related to mortality in the short term and long term after STEMI, with a pooled risk ratio (RR) of 3.02 (95%CI 2.65–3.45) and 4.47 (95% CI 2.54–7.87), respectively, emphasizing the relation between blood glucose levels at admission and the hospital and long-term mortality risk13.
It is suggested that Hyperglycemia frequently happens in patients with STEMI, even among those without diabetes21. The mechanisms that bring about hyperglycemia event in myocardial infarction are: the stimulation of the sympathetic nervous system and enhanced functioning of the hypothalamic-pituitary axis, leading to the secretion of catecholamines and glucocorticoids, especially cortisol22. Furthermore, elevated sympathetic nerve activity prompts the secretion of glucagon, which encourages glycogen lysis in both muscle and liver tissues, leading to the conversion of glycogen into glucose that is released into the bloodstream23. Acute stress also leads to pancreatic beta cell dysfunction and insulin resistance, although the exact mechanisms are unclear. Research indicates that stress during a myocardial infarction may impair insulin production and increase resistance. Hyperglycemia may be a stress response linked to neurohormonal changes during the infarction, causing elevated sympathetic activation and the release of hormones like cortisol and glucagon, which disrupt insulin secretion and glucose regulation.
The definition of hyperglycemia in STEMI patients has changed across studies. In 2008, the American Heart Association (AHA) recommended a cutoff of > 140 mg/dl for blood glucose levels at admission to classify hyperglycemia15. A study by Capes et al. found that in patients without diabetes, an admission glucose level > 110 mg/dl faced a 3.9 times greater risk of in-hospital mortality relative to those with normal levels. In patients with diabetes, an augmented risk of in-hospital mortality was noted only when glucose levels at admission were ≥ 180 mg/dl20. Despite numerous studies on hyperglycemia’s impact on cardiovascular outcomes, there is still no consensus on a standard definition or cutoff for acute hyperglycemia in myocardial infarction patients.
Our analysis of glucose levels at admission demonstrated that the cut-off points of 214 mg/dl for diabetic patients and 148 mg/dl for non-diabetic patients effectively predicted in-hospital and one-year mortality, as evidenced by the ROC curve analysis. The cutoff value of 148 mg/dl for the non-diabetic group, has a higher AUC of 0.71 compared to 0.66 in the diabetic group, indicating better overall predictive accuracy. The specificity for the nondiabetic group is 75%, which is remarkably greater than the 61% specificity for patients with diabetes. It seems that the 148 mg/dl cutoff for the nondiabetic group is the better option overall, demonstrating superior specificity and predictive power, despite the higher accuracy in the diabetic group.
It seems that the acquired cut-offs for glucose levels specially in non-diabetes group are in accordance with the current ESC/AHA guidelines for management of hyperglycemia in STEMI. Based on the ESC/AHA statement elevated blood glucose levels during STEMI are associated with worse outcomes, including increased mortality. ESC/AHA recommend that blood glucose levels should be routinely monitored in all patients presenting with STEMI and the target glucose level should be aimed at 140–180 mg/dL during STEMI management24.
The observed differences in cut-off points for diabetic and non-diabetic patients can be attributed to several physiological and pathophysiological mechanisms: (1) Diabetic patients often have impaired glucose metabolism and insulin resistance, which can lead to chronic hyperglycemia25. In this context, a higher admission glucose threshold elicits a significant increase in mortality risk since their baseline glucose levels are usually elevated. Non-diabetic patients, on the other hand, maybe more sensitive to acute elevations in glucose due to stress or the physiological response to AMI, necessitating a lower cut-off to predict mortality26. (2) AMI induces stress responses that can transiently elevate glucose levels, particularly in nondiabetic patients. This stress-induced hyperglycemia can reflect an underlying severity of the acute event, where even moderate elevations might signify a significant risk of adverse outcomes27. Consequently, the lower threshold for non-diabetic patients might represent a critical point beyond which mortality risk increases noticeably. Furthermore, the pathways leading to mortality in diabetic versus non-diabetic patients may also vary. Patients with diabetes might experience mortality due to chronic complications such as cardiovascular disease or kidney failure, while non-diabetic patients might be subjected to more acute events that lead to rapid mortality28. Thus, the influence of glucose on mortality is related to the patient’s baseline health status and the mechanisms through which AMI progresses.
Increased glucose levels at admission are a significant independent predictor of in-hospital mortality for both patients with and without diabetes experiencing acute myocardial infarction (AMI). Additionally, the analysis identified that hypertension and dyslipidemia emerged as strong predictors of in-hospital mortality, reinforcing the need for comprehensive management of these conditions in AMI patients. Interestingly, female gender was correlated with a reduced hazard for in-hospital mortality in both groups.
Studies have consistently demonstrated that hyperglycemia at the time of admission is linked to worse prognoses in patients with and without diabetes. Moreover, the significance of co-morbidities like hypertension and dyslipidemia is well-supported by prior research, which highlights their roles in exacerbating cardiovascular risks and mortality rates in AMI29,30,31,32.
In terms of one-year mortality, our results indicate that glucose levels ≥ 214 mg/dl in diabetic patients and ≥ 148 mg/dl in non-diabetic patients are significant predictors, with odds ratios of 3.40 and 4.21, respectively which emphasize the importance of early glucose management in the acute setting, as it may influence long-term outcomes. The association of hypertension with an increased risk of one-year mortality further emphasizes the necessity for ongoing monitoring and treatment of comorbidities in AMI patients25,26.
Notably, patients in the diabetes group exhibited a higher prevalence of hypertension and hyperlipidemia, which aligns with existing literature that suggests these conditions are more prevalent in diabetic patients and contribute to worse cardiovascular outcomes33,34,35.
Despite these important findings, our study has limitations. The observational nature of the present investigation limits the ability to establish causality. Additionally. Future research should consider larger, multicenter studies to validate these findings and explore the mechanisms underlying the association of hyperglycemia and mortality in AMI patients.
Conclusion
In conclusion, our study highlights the critical role of admission glucose levels as independent predictors of in-hospital and one-year mortality in patients with AMI, both with and without diabetes. These findings support the need for routine assessment and management of glucose levels in the acute setting, as well as the importance of addressing comorbid conditions such as hypertension and dyslipidemia to improve patient outcomes. The cutoff value of 148 mg/dl for the non-diabetic group, has a higher AUC of 0.71 compared to 0.66 in the diabetic group, indicating better overall predictive accuracy. It seems that the 148 mg/dl cutoff for the nondiabetic group is the better option overall, demonstrating superior specificity and predictive power, despite the higher accuracy in the diabetic group which might be considered as limitation when considering clinical application of glucose at admission levels. The distinct cut-off values for admission glucose levels emphasize the need for the management of AMI patients based on their diabetes status.
Hyperglycemia at the time of admission was found to be better predictor for patients with acute myocardial infarction (AMI) who do not have diabetes rather than those with diabetes. As a result, it is crucial to implement timely and effective hypoglycemic treatment strategies and nursing interventions for AMI patients without diabetes. Future research should investigate the underlying biological mechanisms that differentiate responses between groups.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Jayaraj, J. C. et al. Epidemiology of myocardial infarction. Myocard. Infarct. 10, 9–17 (2019).
Seifimansour, S. et al. Investigation of the impact of iron deficiency anemia on the clinical outcome of hospitalized patients and the 6-month outcome of acute STEMI patients undergoing primary angioplasty. Biomed. Adv. 1(1), 20–26 (2024).
Bahloul, M. et al. Incidence, mechanisms and impact outcome of hyperglycaemia in severe scorpion-envenomed patients. Ther. Adv. Endocrinol. Metab. 9(7), 199–208 (2018).
Matin, E. et al. Oxidative stress and its association with ST resolution and clinical outcome measures in patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention. BMC Res. Notes 13, 1–6 (2020).
Arnold, S. V. et al. Predicting adverse outcomes after myocardial infarction among patients with diabetes mellitus. Circ. Cardiovasc. Qual. Outcomes 9(4), 372–379 (2016).
Irandoost, P. et al. The effect of Capsaicinoids or Capsinoids in red pepper on thermogenesis in healthy adults: A systematic review and meta-analysis. Phytother. Res. 35(3), 1358–1377 (2021).
Sato, Y. et al. Association of glycated albumin with the presence of carotid plaque in patients with type 2 diabetes. J. Diabetes Investig. 4(6), 634–639 (2013).
Avogaro, A. et al. Glucose-lowering therapy and cardiovascular outcomes in patients with type 2 diabetes mellitus and acute coronary syndrome. Diab. Vasc. Dis. Res. 16(5), 399–414 (2019).
Goyal, A. et al. Differential clinical outcomes associated with hypoglycemia and hyperglycemia in acute myocardial infarction. Circulation 120(24), 2429–2437 (2009).
Liang, H. et al. Relationship between fasting glucose levels and in-hospital mortality in Chinese patients with acute myocardial infarction and diabetes mellitus: A retrospective cohort study. BMC Cardiovasc. Disord. 16(1), 156 (2016).
Kosiborod, M. & Deedwania, P. An overview of glycemic control in the coronary care unit with recommendations for clinical management. J. Diabetes Sci. Technol. 3(6), 1342–1351 (2009).
Roshanravan, N. et al. The effects of zinc supplementation on inflammatory parameters in pregnant women with impaired glucose tolerance: A randomized placebo controlled clinical trial. Prog. Nutr. 20(1-S), 330e6 (2018).
Alkatiri, A. H. et al. Stress hyperglycemia and poor outcomes in patients with ST-elevation myocardial infarction: A systematic review and meta-analysis. Front. Cardiovasc. Med. 11, 1303685 (2024).
Kosiborod, M. et al. Admission glucose and mortality in elderly patients hospitalized with acute myocardial infarction: Implications for patients with and without recognized diabetes. Circulation 111(23), 3078–3086 (2005).
Deedwania, P. et al. Hyperglycemia and acute coronary syndrome: a scientific statement from the American heart association diabetes committee of the council on nutrition, physical activity, and metabolism. Circulation 117(12), 1610–1619 (2008).
Koracevic, G. P. Using a single cut-off for stress hyperglycemia in myocardial infarction decreases its prognostic value particularly in diabetes. Am. J. Emerg. Med. 32(1), 103–104 (2014).
Koraćević, G. et al. Single prognostic cut-off value for admission glycemia in acute myocardial infarction has been used although high-risk stems from hyperglycemia as well as from hypoglycemia (a narrative review). Prim. Care Diabetes 14(6), 594–604 (2020).
Thygesen, K. et al. Third universal definition of myocardial infarction. Eur. Heart J. 33(20), 2551–2567 (2012).
Haffner, S. M. et al. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N. Engl. J. Med. 339(4), 229–234 (1998).
Capes, S. E. et al. Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: A systematic overview. Lancet 355(9206), 773–778 (2000).
Ishihara, M. Acute hyperglycemia in patients with acute myocardial infarction. Circ. J. 76(3), 563–571 (2012).
Angeli, F. et al. Hyperglycemia in acute coronary syndromes: From mechanisms to prognostic implications. Ther. Adv. Cardiovasc. Dis. 9(6), 412–424 (2015).
Lønborg, J. et al. Impact of acute hyperglycemia on myocardial infarct size, area at risk, and salvage in patients with STEMI and the association with exenatide treatment: Results from a randomized study. Diabetes 63(7), 2474–2485 (2014).
Rao, S. V. et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI guideline for the management of patients with acute coronary syndromes: A report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J. Am. Coll. Cardiol. 85(22), 2135–2237 (2025).
Ferreira, J. A., et al. Admission hyperglycemia and all-cause mortality in diabetic and non-diabetic patients with acute myocardial infarction: A tertiary center analysis. Intern. Emerg. Med. 1–11 (2021).
Demarchi, A. et al. Has hyperglycemia a different prognostic role in STEMI patients with or without diabetes?. Nutr. Metab. Cardiovasc. Dis. 31(2), 528–531 (2021).
Dong-bao, L. et al. Admission glucose level and in-hospital outcomes in diabetic and non-diabetic patients with ST-elevation acute myocardial infarction. Intern. Med. 50(21), 2471–2475 (2011).
Eitel, I. et al. Prognostic impact of hyperglycemia in nondiabetic and diabetic patients with ST-elevation myocardial infarction: Insights from contrast-enhanced magnetic resonance imaging. Circ. Cardiovasc. Imaging 5(6), 708–718 (2012).
Straumann, E. et al. Admission glucose concentrations independently predict early and late mortality in patients with acute myocardial infarction treated by primary or rescue percutaneous coronary intervention. Am. Heart J. 150(5), 1000–1006 (2005).
Rousan, T. A. et al. Impact of diabetes mellitus on clinical characteristics, management, and in-hospital outcomes in patients with acute myocardial infarction (from the NCDR). Am. J. Cardiol. 114(8), 1136–1144 (2014).
Pres, D. et al. Blood glucose level on admission determines in-hospital and long-term mortality in patients with ST-segment elevation myocardial infarction complicated by cardiogenic shock treated with percutaneous coronary intervention. Kardiologia Polska (Pol. Heart J.) 68(7), 743–751 (2010).
Zarezadeh, M. et al. Probiotics act as a potent intervention in improving lipid profile: An umbrella systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 63(2), 145–158 (2022).
Iglay, K. et al. Prevalence and co-prevalence of comorbidities among patients with type 2 diabetes mellitus. Curr. Med. Res. Opin. 32(7), 1243–1252 (2016).
Shahwan, M. J. et al. Prevalence of dyslipidemia and factors affecting lipid profile in patients with type 2 diabetes. Diabetes Metab. Syndr. Clin. Res. Rev. 13(4), 2387–2392 (2019).
Roshanravan, N. et al. A comprehensive systematic review of the effectiveness of Akkermansia muciniphila, a member of the gut microbiome, for the management of obesity and associated metabolic disorders. Arch. Physiol. Biochem. 129(3), 741–751 (2023).
Acknowledgements
The Research Vice Chancellor of Tabriz University of Medical Sciences, IRAN sponsored the study Grant number:74350. This study is based on the data of the Persian Cardiovascular Disease Registry.
Funding
The Research Vice Chancellor of Tabriz University of Medical Sciences, IRAN sponsored the study Grant number: 74350. This study is based on the data of the Persian Cardiovascular Disease Registry.
Author information
Authors and Affiliations
Contributions
The authors declare that all data were generated in-house and that no paper mill was used. N.MA: Conception; Data collection; Analysis; Research; Method; Writing the draft. N.LY: Data Collection; analysis; research; Method; manuscript draft. S.Gh: Writing-review & editing. N.R: Method; Data collection; Analysis. M.M and A.Z: Analysis; Funding Project management; Supervision; manuscript draft.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The research received approval from the Ethics committee of TBZMED (IR.TBZMED.REC.1403.375). This study adhered to the guidelines outlined in the Declaration of Helsinki, ensuring that all participants were fully informed about their involvement in the registry and granted informed consent for the anonymous dissemination of scientific findings.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mesri Alamdari, N., Lotfi Yagin, N., Ghaffari, S. et al. The different effects of admission blood glucose levels on the outcomes of ST elevation myocardial infarction patients with and without diabetes. Sci Rep 15, 27682 (2025). https://doi.org/10.1038/s41598-025-13032-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-13032-0
