
Abstract
Despite ferritin’s role in iron and metabolic health, its timing and pattern of change relative to other iron biomarkers during the menopausal transition remain unclear, as blood loss shifts alter iron metabolism. This retrospective study analyzed longitudinal changes in 1,885 women aged 31–56 undergoing natural menopause, with at least 3 years of follow-up, using linear mixed models relative to the final menstrual period (FMP), segmented into pre-FMP, around-FMP, and post-FMP periods. Serum iron, ferritin, and transferrin saturation increased over time, whereas total iron-binding capacity (TIBC) decreased. TIBC declined rapidly around FMP, while other iron measures increased sharply and plateaued post-FMP. Serum ferritin levels, however, continued to rise post-FMP, with its coefficient (Standard Error; SE) sharply increasing from 2.10 (0.34) to 20.27 (0.50) between pre-FMP and around-FMP segments and remaining high at 9.34 (0.40) post-FMP. High ferritin residuals (> 1 SD above the mean) from regression models predicting ferritin levels by transferrin saturation were associated with fatty liver and metabolic syndrome components. These findings suggest that serum ferritin levels increase steeply during the menopausal transition and continue to rise post-FMP, reflecting iron status and metabolic health.
Similar content being viewed by others


ORCiD: 0000-0002-3927-8646.
Introduction
Menopause indicates the permanent cessation of ovarian function, as well as significant changes in hormonal and menstrual patterns and physiological and psychosocial symptoms1,2,3. Additionally, during the menopausal transition, an increase in cardiometabolic risk factors, including heightened insulin resistance, increased fat mass, dyslipidemia, and endothelial dysfunction, occurs at the onset of menopause, contributing to a distinct deterioration in the cardiometabolic profile1,4,5.
One of the first physiological changes during menopause is the cessation of menstrual periods, leading to decreased iron loss and increased iron measures in the body, and it is also marked by estrogen deficiency. Although some studies have examined increased iron measure levels in postmenopausal women, these studies were limited owing to small sample sizes or a cross-sectional design6,7,8. Few studies have examined temporal changes in iron measures during menopause, primarily focusing on a binary classification of pre- and postmenopausal status9, leaving the precise timing and progression of these changes throughout the menopausal transition not yet fully understood. Serum ferritin is a commonly used indicator of the body’s iron store; however, as a positive acute-phase protein its hepatic synthesis is up-regulated by several pro-inflammatory cytokines, including TNF-α, IL-1α/β, and IL-610 and increased levels are associated with a heightened risk of type 2 diabetes mellitus11, elevated fasting insulin, central adiposity, and metabolic syndrome12–all of which are more frequently observed in postmenopausal women than in premenopausal women. Thus, the changing patterns of ferritin and other iron-related measures may differ, but the precise timing and distinct patterns of changes in ferritin and other iron-related measures during the menopausal transition, along with their health implications, remain unclear.
This study had two aims. First (primary objective), we characterized the temporal trajectories of multiple iron-status biomarkers—hemoglobin, iron, total iron-binding capacity(TIBC), transferrin saturation, and ferritin—across the menopausal transition, using the final menstrual period (FMP) as an anchor point. Second (secondary objective), we evaluated whether ferritin levels that exceed those expected from transferrin saturation (high ferritin residuals) are associated with adverse metabolic health indicators (hypertension, diabetes, hyperlipidemia, fatty liver, obesity) in the post-menopausal period.
Materials and methods
Study population
This study utilized a subset of the Kangbuk Samsung Health Study, which included Korean adults who were at least 18 years old and underwent regular health checkups at the Kangbuk Samsung Hospital Total Healthcare Centers in Seoul and Suwon, South Korea13,14.
This study specifically focused on women who experienced natural menopause between the ages of 40 and 55 years and had undergone repeated comprehensive health examinations with a minimum of three check-up visits before and after menopause from 2007 to 2022 (n = 2,607). We excluded women with a history of cancer (n = 205), women who underwent partial or total hysterectomy or oophorectomy (n = 390), and women who used female sex hormones, oral contraceptives, or intrauterine devices (n = 236) at baseline or during the follow-up period. The final sample size for analysis included 1,885 women.
This study was approved by the Institutional Review Board (IRB) of Kangbuk Samsung Hospital (IRB No. 2023-05-041) and conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived by the IRB owing to the use of de-identified data that were routinely collected during the health screening examinations.
Data collection
Information on reproductive factors (i.e., parity; dates of the two most recent menstruation periods; regularity and interval of menstrual cycles; age at menarche; and the use of oral contraceptives, intrauterine devices, and hormone replacement therapy), demographic characteristics, lifestyle factors, medical history, and medication use was collected using a standardized, structured, self-administered questionnaire. Alcohol consumption was assessed by recording the weekly frequency of alcohol intake and quantity consumed per drinking session. Average daily alcohol consumption was determined by considering the frequency and quantity of alcohol consumed per drinking day. Physical activity levels were evaluated using the Korean version of the International Physical Activity Questionnaire Short Form, as validated in prior studies15,16. Participant activity levels were categorized based on previously established criteria17. Health-enhancing physically active (HEPA) status was determined by meeting one of the following two criteria; (i) engaging in vigorous-intensity activity for a minimum of 3 days per week, totaling ≥ 1500 MET min/week or (ii) achieving at least 3000 MET min/week through any combination of walking or moderate- or vigorous-intensity activities performed over 7 days16.
Parity was defined as the total number of previous pregnancies, including live births and stillbirths. At baseline and throughout the follow-up period, menopausal status and dates of the last two menstrual periods were ascertained using a self-administered, structured questionnaire. Menopause was defined as absence of a menstrual period for ≥ 12 months18,19. The final menstrual period (FMP) was identified as the most recent menstruation date at the visit when the participant reported a period of amenorrhea lasting for 12 months or longer; the age at the FMP was calculated based on age at the first day of the FMP.
Trained nurses obtained anthropometric measurements and assessed blood pressure (BP) with patients in a seated position. Diabetes mellitus was identified by a fasting serum glucose level ≥ 126 mg/dL, glycated hemoglobin (HbA1c) level ≥ 6.5%, or self-reported use of insulin or other glucose-lowering medications20. Hypertension was defined as a BP ≥ 140/90 mmHg or self-reported use of BP-lowering medication21. Hyperlipidemia was defined as current lipid‑lowering medication, triglycerides > 200 mg/dL, or total cholesterol > 240 mg/dL22.
Blood samples were collected following an overnight fast. Serum fasting glucose was measured by the hexokinase method on a Cobas Integra 800 analyzer (Roche Diagnostics, Rotkreuz, Switzerland); samples were centrifuged within 30 min of collection. HbA1c was measured in hemolyzed whole blood using a turbidimetric inhibition immunoassay on the same analyzer. Serum total cholesterol and triglycerides were measured with enzymatic colorimetric assays, and HDL‑ and LDL‑cholesterol were measured directly with homogeneous enzymatic colorimetric assays on a Cobas 8000 c702 system (Roche Diagnostics, Tokyo, Japan). Serum iron and total iron‑binding capacity (TIBC) were measured by colorimetric assay and the FerroZine chromogen method, respectively, on the same analyzer. Serum ferritin was measured by electrochemiluminescence immunoassay on a Modular E170 analyzer (Roche Diagnostics, Tokyo, Japan); total coefficients of variation were ≤ 4.3% (normal control) and ≤ 4.9% (high‑level control). All assays were conducted in a single laboratory (Kangbuk Samsung Hospital) accredited biannually by the Korean Society of Laboratory Medicine(KSLM) and participating annually in external quality‑assurance programs run by the Korean Association of Quality Assurance for Clinical Laboratories(KAQACL) and the College of American Pathologists(CAP). Fasting blood sample measurements included glucose, HbA1c, complete blood cell counts, and iron-related biomarkers, including serum ferritin, iron, and total iron-binding capacity (TIBC). Transferrin saturation was determined by dividing serum iron levels by the TIBC and multiplying the result by 100. Complete blood counts, including hemoglobin levels, were obtained using an XE-2100 hematology analyzer (Sysmex Corporation, Kobe, Japan)23.
Statistical analysis
The index date was defined as the FMP. Time intervals in relation to the FMP were established by calculating the difference between the age at the FMP and time of each visit. These intervals were then divided into three distinct time periods relative to the FMP: >1 year before the FMP (pre-FMP), within 1 year of the FMP (around FMP), and > 1 year after the FMP (post-FMP).
Demographic and other characteristics, including iron measures for each of the three groups, are presented using summary statistics. All continuous variables are reported as mean ± standard deviation (SD); categorical variables are expressed as counts and percentages (n, %).
For Table 1, we compared baseline characteristics across the pre‑, around‑, and post‑FMP periods. Categorical outcomes (hypertension, diabetes, lipid‑lowering medication use) were analysed with generalized estimating equations (GEE; logit link, exchangeable correlation); continuous ferritin was analysed with a random‑intercept linear mixed‑effects model (LMM). Pairwise contrasts were Bonferroni‑adjusted.
This study examined the magnitude of change in ferritin and other iron measures by dividing the menopausal transition into three time periods relative to the FMP. A similar slope of the iron measure across all three time periods indicated chronological aging with no impact on the menopausal transition. To statistically test this hypothesis, we fitted two longitudinal models for each risk factor. The first was a linear mixed model that assumed a constant slope across the three time periods. The second model was a piecewise linear mixed model that allowed the slope to differ across the three time periods. We derived model-predicted annual mean values of iron measures from 11 years before to 11 years after the FMP using the piecewise linear mixed models. Because participants contributed different numbers of visits at each time-point, the sample size underlying each annual mean varied by year; these counts are provided in Supplementary Table S4.
We used separate longitudinal linear mixed models for each iron measure as a function of the years before and after the FMP24. This method considers within-subject correlations, differences in the number of observations per person, and variations in the time intervals between measurements. Linear and piecewise linear models were separately adjusted for age, education level, marital status, parity, and iron supplementation. To compare the fitness of a linear mixed with a piecewise linear mixed model, we examined their AIC values25,26.
To further investigate the distinct pattern of ferritin compared to other iron markers, we conducted an additional analysis, focusing on the residuals from simple linear regression models where ferritin levels were predicted by transferrin saturation. Because both variables were right‑skewed, ferritin and transferrin saturation were analysed on the natural‑log scale. We used the residuals quantify the portion of circulating ferritin that cannot be explained by iron availability (as represented by transferrin saturation). This “Transferrin saturation-independent ferritin” component is hypothesised to reflect inflammatory or metabolic stress, and therefore may show stronger associations with metabolic-health outcomes than total ferritin itself. By design, the residual is orthogonal to transferrin saturation (r = 0), allowing us to test whether elevations in ferritin beyond what iron status predicts are linked to hypertension, diabetes, hyperlipidemia, fatty liver or obesity without the collinearity that would arise from entering both ferritin and transferrin saturation in the same model. This analysis was carried out at two time points: baseline and five years post-final menstrual period (FMP 5YRS). Given the variable timing of visits pre-FMP, measures form the first visit were selected for analysis to ensure data availability for all subjects. Post-FMP time points were analysed at 5 years, approximating the end of the early stage of postmenopause (+ 1)27,28. Residual was defined as the difference between the actual value of ferritin and the predicted value of ferritin by transferrin saturation by linear regression models. To explore associations between these residuals and common chronic diseases (hypertension, diabetes, hyperlipidemia, obesity, and fatty liver) participants were categorized into three groups based on the standard deviation of the residuals: high (residuals > 1 SD above the mean), normal (within 1 SD of the mean), and low (residulas > 1 SD below the mean). Differences across ferritin residual categories were tested using chi-square tests or Fisher’s exact test for categorical variables, and ANOVA for continuous variables.
In a sensitivity analysis, LDL‑cholesterol values for lipid‑lowering medication users were multiplied by 1/0.7 (i.e., divided by 0.7) to account for the expected ≈ 30% lowering effect of lipid‑lowering medications, as recommended by recent ESC guidance29.
All analyses were conducted using R software (version 4.2.2); statistical significance was defined as a two-sided P-value < 0.05.
Results
Characteristics according to pre-FMP, within 1 year of the FMP, and post-FMP time periods
The characteristics of the 1,885 participants included in this study are detailed according to the FMP periods (Table 1). The average age at the time of the FMP was 49.82 years (standard deviation, 2.73), and 1.47% of the participants were current smokers. The majority of the participants (97.2%) were married, and 94.47% had given birth at least once (parous). Comorbidities included hypertension (9.1%), diabetes (4.29%), and lipid-lowering medication use (3.89%). Iron supplementation was observed 0.53% prior to their FMP and 0.8% around their FMP; 0.48% iron supplementation was reported during the post-FMP period.
The prevalence of hypertension (OR = 1.63 for around vs. pre; 2.84 for post vs. pre), diabetes (1.97; 3.38) and lipid‑lowering medication use (5.41; 21.5) increased significantly across periods (all P < 0.001, GEE). Mean ferritin increased by 42.2 µg/L around the FMP and by 99.0 µg/L after the FMP, equivalent to 2.04‑fold and 3.46‑fold rises relative to the pre‑FMP mean (calculated from LMM‑estimated stage‑specific means; P < 0.001). See Supplementary Table S3 for full estimates.
The analysis included data from 1,885 women who experienced natural menopause. Each participant underwent at least three health checkups, with at least one iron measurement obtained before the FMP and at least one after the FMP. Specifically, the average number of visits per person was 5.69 (median, 5; range, 1–11) before the FMP and 3.41 (median, 3; range, 1–11) after the FMP. The 1,885 women contributed 18,908 visits, each with complete measurements for hemoglobin, iron, TIBC, ferritin, and transferrin saturation (no missing values).
Changes in iron measures in relation to the FMP
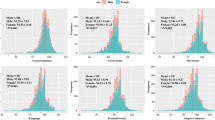
Figure 1 shows the annual mean values of iron measures from − 11 years before to 11 years after the FMP, as well as estimates from the piecewise linear mixed models. The temporal changes in hemoglobin, iron, TIBC, ferritin, and transferrin saturation were better fitted by the piecewise linear mixed versus linear mixed model (Table 2; Fig. 1). Likelihood ratio tests resulting in a p-value < 0.001 indicated a better fit for the piecewise linear mixed model compared with the linear mixed model. This suggests that the piecewise model, which had slopes in three different time periods based on the intervals surrounding the FMP, provided a better fit than the linear model and that the observed changes were attributed to the cessation of menstruation rather than solely to chronological aging.

Annual mean values of iron measures and estimated means for natural menopause group. Two longitudinal models were fitted for each iron measure: (1) a linear mixed model that assumed a constant slope across the time periods and (2) a piecewise linear mixed model that allowed the slope to differ across the three segments relative to the final menstrual period (FMP). The model-predicted annual mean values of the iron measures from 11 years before to 11 years after the FMP—derived from the piecewise linear mixed models—are shown. The number of observations contributing to each yearly mean for every biomarker is provided in Supplementary Table S4. The figure was created using R version 4.3.2 with the ggplot2 package version 3.5.1.
Hemoglobin, iron, ferritin, and transferrin saturation levels gradually increased before the FMP interval (Table 2). Iron levels rose significantly in the pre‑FMP segment (β = +0.83, P = 0.0005) and showed an even steeper increase around the FMP (β = +3.42, P < 0.0001); thereafter they declined modestly, but the post‑FMP slope did not reach statistical significance (β = − 0.56, P = 0.06). TIBC decreased up to the FMP and stabilized afterwards; the decrease in TIBC during the FMP was significantly greater than that during the pre-FMP interval. The slopes of the changes in hemoglobin and ferritin levels were significantly greater within 1 year of the FMP compared with those in the pre-FMP interval. Ferritin levels continued to rise gradually after the FMP, although the rate of increase was less steep compared with that during the around-the-FMP interval. Specifically, the coefficient between the pre-FMP and around-FMP intervals showed a sharp increase, from 2.10 (Standard error [SE], 0.34) to 20.27 (SE, 0.50). The coefficient remained steep at 9.34 (SE, 0.40) even during the post-FMP interval. This distinct pattern of ferritin differed from other the iron measures, in which the slope tended to stabilize or decrease in the post-FMP interval.
Ferritin residuals and metabolic health
At baseline, ferritin residuals from linear regression models predicting ferritin levels by transferrin saturation were significantly and positively associated with fatty liver, obesity and other metabolic syndrome components except hypertension (Table 3). The log‑linear relationship on which these residuals are based is presented in Supplementary Figure S5. Detailed cross‑tabulations, including stratification by obesity status, are provided in Supplementary Tables S1 (baseline) and S2 (5 years post‑FMP). The high ferritin residuals (> 1 SD above the mean; Group 3) were consistently associated with higher metabolic risk profiles. Specifically, the prevalence of fatty liver in Group 3(21.9%) was significantly higher compared to Groups 1(7.5%) and 2(9.0%), highlighting a strong correlation between higher ferritin residuals and fatty liver.
As we moved to the FMP 5YRS marker, the pattern of significant differences shifted slightly but still prominently featured obesity and fatty liver as conditions with statistically significant variations among the groups (Table 3).
Despite no overall statistical significance in hyperlipidemia across the groups at FMP 5YRS, Group 3 displayed significant differences within its subgroup, particularly noted in triglycerides and LDL cholesterol levels, indicating specific lipid metabolism issues (Table 3; Fig. 2). Findings were unchanged when statin‑adjusted LDL was used (Table 3, Adjusted LDL*).

Ferritin residual analysis and health outcomes at baseline and FMP 5yrs. Residual was defined as the difference between the actual value of ferritin and the predicted value of ferritin by transferrin saturation by linear regression models. Group 1: Residuals > 1 SD above the mean, Group 2: Residuals within 1 SD of the mean, Group 3: Residuals > 1 SD below the mean. The figure was created using R version 4.3.2 with the forestplot package version 3.1.3.
Discussion
In women experiencing natural menopause, iron-related biomarker levels, including hemoglobin, iron, transferrin saturation, and ferritin, exhibited a rapid increase within 1-year of the FMP, whereas the TIBC displayed the opposite trend. After the FMP, ferritin levels continued to rise, whereas those of the other iron measures stabilized following the initial 1-year post-FMP period. The clinical implications of the different patterns of serum ferritin levels after the FMP compared with those of the other iron biomarkers should be elucidated in future research.
Previous studies have investigated elevated levels of iron measures in postmenopausal women and have observed higher levels compared with those in premenopausal women, although these studies were limited owing to small sample sizes or cross-sectional designs6,7,8. Only one longitudinal study demonstrated changes in iron measures during menopause after evaluating iron-related measures in 70 female participants at one premenopausal and one postmenopausal time point9. This study reported significant increases in iron stores based on ferritin and soluble transferrin receptor levels across the stages of menopause9; however, the average interval between the time of each woman’s premenopausal and postmenopausal assessment of iron measures was 5 years, thereby limiting their ability to precisely identify when and how these changes progressed throughout the menopausal transition. In our study of 1,885 women, we found that iron measures rapidly increased within 1 year of the FMP, followed by a distinctive pattern of continuous ferritin increase thereafter. A previous study that used National Health and Nutrition Examination Survey (NHANES) III data on the general US population, demonstrated different patterns of iron accumulation based on age and sex30 and observed that ferritin levels remain relatively low in women until after their fourth decade of life, at which point they sharply increase and continue to rise until the age of 60–6930. Notably, the distribution of values of serum ferritin differed from the percentage of transferrin saturation30.
The reasons for the distinctive patterns of ferritin levels compared with those of other iron measures are not fully understood, and several factors related to postmenopausal status and iron metabolism may be contributing factors. Menopause, which involves the cessation of iron blood loss due to menstruation and a decrease in estrogen levels, can affect iron absorption and storage. During premenopause, elevated estradiol levels suppress hepatic hepcidin—produced in the liver and acting on ferroportin in duodenal enterocytes to inhibit dietary iron uptake—thereby enhancing intestinal iron absorption31, while during postmenopause, decreased blood loss may contribute to higher iron stores. Although serum ferritin levels are commonly used to indicate iron stores, they can be influenced by proinflammatory markers, such as TNF-α and IL-1α, as well as certain chronic diseases, such as steatogenic liver disease, liver disease, diabetes, metabolic syndrome, certain malignancies, and inflammatory disorders11,12,32,33,34. Ferritin is also associated with various indexes of adiposity35 and a cross-sectional study demonstrated that serum ferritin has a positive association with waist circumference, total body fat, and trunk fat mass and an inverse association with leg fat mass36. Additionally, estrogen promotes the accumulation of gluteal-femoral adipose tissue in premenopausal women37, and gluteofemoral fat is associated with higher insulin sensitivity37,38 During menopause, estrogen deficiency redistributes fat from protective areas to visceral fat, which is associated with insulin resistance and increased ferritin levels37,38. Consequently, ferritin levels and those of other iron-related measures can vary considerably.
Our study’s ferritin residual analysis revealed compelling findings regarding health outcomes among postmenopausal women. We specifically noted that women in the high residual group, where ferritin levels were not explained by transferrin saturation, demonstrated marked health differences. At baseline, there was a significantly higher prevalence of fatty liver in this group (21.9%) compared to those with lower residuals (Groups 1 and 2 at 7.5% and 9.0%, respectively). This strong correlation underscores ferritin’s role beyond being a simple marker of iron status—it may also serve as an indicator of deeper metabolic issues.
Five years post-final menstrual period, this pattern persisted with significant health disparities still evident. Additionally, we observed significant variations in glucose levels and HbA1c, highlighting issues with glucose metabolism that are particularly pronounced in those with high ferritin residuals.
At baseline, Group 3 showed the highest—and statistically significant—prevalence of hyperlipidaemia (p < 0.001) and the highest triglyceride levels (p < 0.001). Five years after the final menstrual period, the overall difference in hyperlipidaemia prevalence across groups was no longer significant (p = 0.33); nonetheless, the baseline pattern persisted. Because the follow-up cohort was smaller (n = 567 vs. 1 885 at baseline) and prevalence rose in all groups, between-group contrast narrowed, yet Group 3 still had the greatest prevalence (~ 42%), remaining > 11% points higher than Group 1 (~ 31%) and > 7 points higher than Group 2 (~ 35%). Group 3 also continued to display significantly higher triglyceride concentrations (117 ± 70 mg/dL) than Group 1 (93 ± 40 mg/dL) and Group 2 (104 ± 60 mg/dL; p = 0.028). Triglycerides are a sensitive marker of insulin-resistance–related metabolic dysfunction39, whereas clinical lipid management typically prioritises LDL-cholesterol and addresses triglycerides later40; this treatment focus may help explain the persistent group differences despite the reduced follow-up sample size. Collectively, these findings indicate that elevated transferrin saturation-independent ferritin is associated with a higher metabolic burden, reflected in persistently high triglyceride levels, glucose, HbA1c and adiposity measures—including fatty liver—in the highest residual group.The implications of these findings are significant for clinical practice. Monitoring ferritin levels in postmenopausal women can provide insights not only into iron status but also into potential metabolic dysfunctions. This is especially critical given the association of high ferritin residuals with conditions like fatty liver, which are substantial risk factors for more severe diseases, including cardiovascular diseases and diabetes. Such insights advocate for a more nuanced approach to health screening in postmenopausal women, taking into account the complexity of ferritin as a biomarker. This tailored approach could lead to earlier interventions and more personalized management strategies, potentially improving outcomes for this population.
Our study had some limitations. First, it should be noted that our determination of the final menstrual period (FMP) relied on self-reporting, which may introduce some potential for recall bias. To minimize inaccuracies from recall bias, we specifically selected the most recent menstrual period reported by participants when they transitioned to a postmenopausal state. Additionally, we did not assess female hormones such as FSH or estradiol to confirm menopausal status as a supplementary measure. Misclassification of the menopausal status might have resulted in reduced iron measure patterns since menstrual cessation-related iron loss would not have been evident. Second, we did not have access to dietary data or detailed information on lifetime drinking history, beverage type, and drinking patterns, which are relevant to iron intake and determinants of iron levels. Only mean alcohol intake(grams/day) at each visit was available; owing to this limited exposure information, alcohol was not included in the multivariable analyses. Consequently, residual confounding by alcohol consumption cannot be ruled out. Thus, residual confounding effects may exist due to unmeasured confounders. Third, we lacked detailed data on menstrual‑cycle irregularity and bleeding volume during the late perimenopausal years; fluctuations in cycle frequency and flow immediately before the FMP could have modified iron loss and may partly explain the progressive decline in TIBC observed in the pre‑FMP segment. Fourth, we did not adjust our models for post-menopausal changes in adiposity-related factors—body-mass index, obesity status, and LDL-cholesterol—which increased after the FMP and are mechanistically linked to ferritin, fatty liver, and other metabolic outcomes; residual confounding from these variables may have inflated some of the observed associations. Fifth, we did not measure any inflammatory biomarkers, which may also affect ferritin levels. Finally, the study sample predominantly comprised Korean women with a high socioeconomic status and education level and accessibility to health services as they attended regular comprehensive health examinations. Although the age at menopause was similar to that reported in the Korean NHANES data41, our findings may not be generalizable to other populations with a higher prevalence of comorbidities or different racial/ethnic backgrounds. Iron status varies substantially across ancestry groups due to genetic, environmental, and dietary factors. Pathogenic HFE variants (C282Y, H63D), common in northern Europeans (0.3–0.5% C282Y homozygosity)42, are rare in East Asian and African populations43. These ancestry-related differences may influence how iron status changes during the menopausal transition. Thus, validating our findings in ethnically diverse cohorts is crucial to assess the generalizability of menopause-related iron metabolism changes.
In this group of apparently healthy women experiencing natural menopause, iron-related biomarkers such as hemoglobin, iron, and transferrin saturation exhibited a rapid increase within 1 year of the FMP and then stabilized. In contrast, ferritin levels rapidly increased within 1 year of the FMP and continued to increase throughout the postmenopausal period. This discrepancy between serum ferritin levels and the other iron-related biomarkers cannot be solely attributed to changes in iron stores; however, it may be due to estrogen deficiency or other postmenopausal alterations in the body. This suggests that ferritin levels may have different implications other than iron stores. Therefore physicians should use caution when determining a patient’s iron status based solely on ferritin levels. Further studies are required to identify the different ferritin patterns that may aid our understanding of iron metabolism and its determinants.
Data availability
The data are not available to be shared publicly as per the policy of institutional review board (IRB) regarding data distribution. However, data is available from the corresponding author on reasonable request. The R scripts used for data management and all statistical analyses are archived at https://github.com/MJ-S-Kim/menopause-ferritin-analysis and will be made publicly accessible upon publication.
References
Hickey, M., Davis, S. R. & Sturdee, D. W. Treatment of menopausal symptoms: what shall we do now? Lancet 366(9483), 409–421 (2005).
El Khoudary, S. R. et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: A scientific statement from the American heart association. Circulation 142(25), e506–e532 (2020).
Nelson, H. D. Menopause Lancet, 371(9614): 760–770. (2008).
Samargandy, S. et al. Trajectories of blood pressure in midlife women: does menopause matter? Circul. Res. 130(3), 312–322 (2022).
The Lancet & Diabetes, E. Menopause: a turning point for women’s health. Lancet Diabetes Endocrinol. 10(6), 373 (2022).
Cho, G. J. et al. Serum ferritin levels are associated with metabolic syndrome in postmenopausal women but not in premenopausal women. Menopause 18(10), 1120–1124 (2011).
Milman, N. et al. Iron status in Danish women, 1984–1994: a cohort comparison of changes in iron stores and the prevalence of iron deficiency and iron overload. Eur. J. Haematol. 71(1), 51–61 (2003).
Looker, A. C. et al. Prevalence of iron deficiency in the united States. Jama 277(12), 973–976 (1997).
Kim, C. et al. Changes in iron measures over menopause and associations with insulin resistance. J. Women’s Health. 21(8), 872–877 (2012).
Wessling-Resnick, M. Iron homeostasis and the inflammatory response. Annu. Rev. Nutr. 30, 105–122 (2010).
Liu, J. et al. Iron metabolism and type 2 diabetes mellitus: A meta-analysis and systematic review. J. Diabetes Investig. 11(4), 946–955 (2020).
Abril-Ulloa, V. et al. Ferritin levels and risk of metabolic syndrome: meta-analysis of observational studies. BMC Public. Health. 14, 483 (2014).
Chang, Y. et al. Metabolically-healthy obesity and coronary artery calcification. J. Am. Coll. Cardiol. 63(24), 2679–2686 (2014).
Chang, Y. et al. Metabolically healthy obesity and development of chronic kidney disease: A cohort study. Ann. Intern. Med. 164(5), 305–312 (2016).
Chun, M. Y. Validity and reliability of Korean version of international physical activity questionnaire short form in the elderly. Korean J. Fam Med. 33(3), 144–151 (2012).
Craig, C. L. et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 35(8), 1381–1395 (2003).
Ryu, S. et al. Relationship of sitting time and physical activity with non-alcoholic fatty liver disease. J. Hepatol. 63(5), 1229–1237 (2015).
Choi, Y. et al. Menopausal stages and serum lipid and lipoprotein abnormalities in middle-aged women. Maturitas 80(4), 399–405 (2015).
Harlow, S. D. et al. Executive summary of the stages of reproductive aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. J. Clin. Endocrinol. Metab. 97(4), 1159–1168 (2012).
American Diabetes Association Professional Practice. Introduction and methodology: standards of care in Diabetes-2024. Diabetes Care. 47(Supplement_1), S1–S4 (2024).
Lee, H. Y. et al. 2018 Korean society of hypertension guidelines for the management of hypertension: part II-diagnosis and treatment of hypertension. Clin. Hypertens. 25, 20 (2019).
Cleeman, J. I. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). (2001).
Ruzicka, K. et al. The new hematology analyzer sysmex XE-2100: performance evaluation of a novel white blood cell differential technology. Arch. Pathol. Lab. Med. 125(3), 391–396 (2001).
Fitzmaurice, G. M. Applied longitudinal analysis. Wiley Series in Probability and Statistics (eds Laird, N. M. & Ware, J. H.) (Wiley-Interscience, 2004).
Agresti, A. & Caffo, B. Measures of relative model fit. Comput. Stat. Data Anal. 39(2), 127–136 (2002).
Conner, J. S., Seborg, D. E. & Larimore, W. E. Analysis of the /spl Delta/AIC statistic for optimal detection of small changes in dynamic systems. in Proceedings of the 2004 American Control Conference (2004).
Ambikairajah, A., Walsh, E. & Cherbuin, N. A review of menopause nomenclature. Reprod. Health. 19(1), 29 (2022).
Harlow, S. D. et al. Executive summary of the stages of reproductive aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. J. Clin. Endocrinol. Metabolism. 97(4), 1159–1168 (2012).
Abrignani, M. G. Evaluating Statin effect on LDL-cholesterol: when predicted is not measured. Eur. J. Prev. Cardiol. 27(15), 1627–1629 (2020).
Zacharski, L. R. et al. Association of age, sex, and race with body iron stores in adults: analysis of NHANES III data. Am. Heart J. 140(1), 98–104 (2000).
Yang, Q. et al. 17beta-Estradiol inhibits iron hormone Hepcidin through an Estrogen responsive element half-site. Endocrinology 153(7), 3170–3178 (2012).
Kernan, K. F. & Carcillo, J. A. Hyperferritinemia and inflammation. Int. Immunol. 29(9), 401–409 (2017).
Senjo, H. et al. Hyperferritinemia: causes and significance in a general hospital. Hematology 23(10), 817–822 (2018).
Jian, J., Pelle, E. & Huang, X. Iron and menopause: does increased iron affect the health of postmenopausal women? Antioxid. Redox Signal. 11(12), 2939–2943 (2009).
Iwasaki, T. et al. Serum ferritin is associated with visceral fat area and subcutaneous fat area. Diabetes Care. 28(10), 2486–2491 (2005).
Wu, H. et al. Opposite associations of trunk and leg fat depots with plasma ferritin levels in middle-aged and older Chinese men and women. PLoS One. 5(10), e13316 (2010).
Goossens, G. H., Jocken, J. W. E. & Blaak, E. E. Sexual dimorphism in cardiometabolic health: the role of adipose tissue, muscle and liver. Nat. Rev. Endocrinol. 17(1), 47–66 (2021).
Manolopoulos, K. N., Karpe, F. & Frayn, K. N. Gluteofemoral body fat as a determinant of metabolic health. Int. J. Obes. (Lond). 34(6), 949–959 (2010).
Ma, M. et al. Triglyceride is independently correlated with insulin resistance and islet beta cell function: a study in population with different glucose and lipid metabolism States. Lipids Health Dis. 19, 1–12 (2020).
Committee, W. et al. 2022 ACC expert consensus decision pathway on the role of nonstatin therapies for LDL-cholesterol Lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American college of cardiology solution set oversight committee. J. Am. Coll. Cardiol. 80(14), 1366–1418 (2022).
Park, C. Y., Lim, J. Y. & Park, H. Y. Age at natural menopause in koreans: secular trends and influences thereon. Menopause 25(4), 423–429 (2018).
Kang, W. et al. Ethnic differences in iron status. Adv. Nutr. 12(5), 1838–1853 (2021).
Adams, P. C. et al. Hemochromatosis and iron-overload screening in a Racially diverse population. N. Engl. J. Med. 352(17), 1769–1778 (2005).
Acknowledgements
We thank our staff members at the Kangbuk Samsung Health Study for their hard work, dedication, and support. This study was supported by the SKKU Excellence in Research Award Research Fund, Sungkyunkwan University (2022). For Minjeong Kim and Jae Keun Yoo, this work was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Korean Ministry of Education (RS-2023-00217022).
Author information
Authors and Affiliations
Contributions
M. K conceived the study, analyzed the data, designed the analytical strategy, and drafted the manuscript. Y. C. and S. R. planned, designed, and directed the study and were responsible for quality assurance and control. G.Y.L, R.K., J.A. and J.P. collected the data and reviewed the literature.J.K.Y. designed the statistical analysis, interpreted the data and critically revised the manuscript. Y.C, M.J. K, H.K.J, and K.H.K interpreted the data and critically revised the manuscript. All authors saw and approved the final version and no other person made a substantial contribution to the paper.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kim, M., Chang, Y., Cho, Y. et al. Accelerated increase in ferritin levels during menopausal transition as a marker of metabolic health. Sci Rep 15, 29311 (2025). https://doi.org/10.1038/s41598-025-14295-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-14295-3
