
Abstract
This retrospective study compared bone mineral density (BMD) measurements assessed by unenhanced computed tomography (CT)-based HU at L1 vertebrae to those by plain spine radiographs in ankylosing spondylitis (AS) patients with or without bamboo spine (BS). We also assessed whether BS affects dual-energy X-ray absorptiometry (DXA)-based osteoporosis diagnosis using unenhanced CT scans at the L1 vertebrae. All patients underwent DXA, unenhanced CT scans, and plain spine radiographs. The cohort of 524 AS patients was classified into BS (n = 189) and non-BS (n = 335) groups (Hu threshold for osteoporosis, 135). The BS group had significantly higher spine (P < 0.001) and hip (P < 0.001) T-scores and significantly lower L1 HU values (P < 0.001) than the non-BS group. Among non-BS patients, lowest T-scores correlated positively with L1 HU values (R-value, 0.437; P < 0.001); in BS patients a weak but significant correlation was observed between L1 HU values and hip T-scores (R-value, 0.341; P < 0.001). Using the Hu threshold, 77.8% of BS and 55.2% of non-BS patients were reclassified as osteoporotic despite DXA indicating no osteoporosis. Whether CT-based HU improves the accuracy of BMD evaluation in the AS population requires confirmation in larger cohort studies.
Similar content being viewed by others


Introduction
Ankylosing spondylitis (AS), alternatively known as radiographic axial spondyloarthritis, is a persistent inflammatory condition that predominantly affects the axial skeleton1. A key feature of AS is calcification of the entheses of the tendons and ligaments due to prolonged inflammation. The majority of patients with AS experience bone loss, the most common comorbidity in these patients2,3,4. Bamboo spine (BS) is a potential complication of AS. This inflammatory condition can lead to fusion of the bones of the spine, forming one long bone1. Research has shown that AS patients have a higher incidence of vertebral fractures, attendant neurological compromise, and spinal surgery-related complications than does the general population5,6,7. Therefore, accurately identifying AS patients at risk for fracture is crucial.
Osteoporosis is currently diagnosed using dual-energy X-ray absorptiometry (DXA), which evaluates bone mineral density (BMD). DXA of the total hip and the spine in anteroposterior (AP) projections is commonly used for BMD determination8. In patients with advanced AS involving ligamentous calcification, DXA of the spine in AP or lateral projections may be inaccurate9,10,11,12. In such cases, DXA may underestimate BMD due to masking by soft-tissue calcification and bony fusion of the facet joints in the spine. To address this issue, the European League Against Rheumatism recommends that AS patients with BS undergo DXA scan of the hip joint to assess osteoporosis13.
Several studies have reported promising results using computed tomography (CT)-based Hounsfield unit (HU) values to diagnose osteoporosis14,15,16,17,18. Using CT-based HU values at the L1 level together with corresponding DXA T-scores is an alternative method for diagnosing osteoporosis in the general population14,16,19. A threshold of 135 HU at the L1 vertebral body may clinically indicate osteoporosis, as reported by Ahern et al.20 and Anderson and colleagues21.
Clinical studies have yet to confirm whether CT-based HU values can be used to evaluate BMD in AS patients and whether this measurement correlates with DXA T-scores in this population. To address these questions, this retrospective study aims to compare the BMD measured by unenhanced CT-based HU at the L1 vertebral body to that using plain spine radiographs in AS patients with or without BS. The secondary outcome is to determine whether the presence of BS affects DXA-based osteoporosis diagnosis as re-evaluated at a threshold of 135 HU.
Methods
Study population and demographic data
This study was approved by the Institutional Review Board of Taipei Veterans General Hospital (No. 2023-08-010BC), and informed consent was waived by the Institutional Review Board of Taipei Veterans General Hospital due to the retrospective nature of the analysis. This study was performed in accordance with the Declaration of Helsinki. Analysis included all AS patients treated at our institution between 2003 and 2022 who met the Modified New York Classification criteria for AS, were aged 20 years or above, and underwent both non-enhanced lung, abdominal or lumbar CT examination for any indication (which included the L1 vertebral body in all recruited) and DXA, with a maximum period of 6 months between the two examinations to ensure comparability. All participants were Asian. The medical records of the 811 patients were carefully reviewed, and 287 were excluded due to bone metastasis or tumor (n = 64), spine instrumentation (n = 67), infection (n = 79), trauma (n = 47), or incomplete medical records (n = 30). The final study cohort included 524 patients (Fig. 1). Demographic and clinical information including age, sex, body mass index, and medical history, including diabetes and underlying medications, were collected from medical records.

Flowchart of our enrolled population. AS, ankylosing spondylitis; DXA Dual-energy X-ray Absorptiometry; CT, computed tomography.
Whether BS was present in these patients was determined using plain spine lateral radiographs analyzed by one orthopedic spine surgeon (3 years of clinical practice) and confirmed by formal radiologic reports (Fig. 2). The 524 enrolled AS patients were categorized into BS (n = 189) and non-BS (n = 335) groups. The demographic and clinical characteristics of the two groups were similar (Table 1).

Radiographic appearance of bamboo spine (BS) and non-bamboo spine (non-BS) on lateral plain spine radiographs. (a, left) The white arrow indicates characteristic features of BS, with fusion of both the anterior and posterior longitudinal ligaments; (b, right) No radiographic evidence of BS is observed (non-BS).
Dual-energy X-ray absorptiometry (DXA)
Hologic Discovery W DXA (Hologic, Inc., Marlborough, MA, USA) was used to evaluate BMD in the hip or in AP projections of the lumbar spine (vertebrae L1 to L4) according to the European guideline for the diagnosis and management of osteoporosis22. For patients who underwent both AP spine and hip DXA scans within 6 months of the CT scan, we compared the lowest T-scores at either the hip or spine. According to World Health Organization (WHO) guidelines, osteoporosis is indicated by a DXA T-score ≤ − 2.5, while osteopenia corresponds to a DXA T-score ≤ − 1.0 and > − 2.5. A DXA T-score > − 1.0 is deemed normal8.
Computed tomography and Hounsfield unit (HU) measurements
All CT scans were performed using either a Canon Aquilion Prime SP (Canon Medical Systems, Japan) or a Siemens SOMATOM Definition Flash (Siemens Healthcare, Germany), depending on scanner availability. The scanned regions included the abdomen and lumbar spine. All examinations were performed without the use of intravenous contrast agents.
Standard acquisition parameters included a Tube voltage of 120 kVp with automatic tube current modulation (typically 100–300 mAs), detector collimation of 0.5–0.625 mm, and pitch ranging from 0.8 to 1.2 based on anatomical region and scanner type. For abdominal CT scans, axial images were reconstructed with a slice thickness of 5 mm and an increment of 5 mm, using a soft tissue reconstruction kernel. For lumbar spine CT scans, axial images were reconstructed with a slice thickness of 3 mm and an increment of 3 mm, using both soft tissue and bone kernels, as appropriate. Scans were acquired in the supine position, during breath-hold for abdominal imaging and during free breathing for lumbar spine imaging. On axial images of non-contrast CT scans, the region of interest (ROI) was defined as the trabecular bone within the vertebral body at L1 level, excluding posterior elements (Fig. 3). The largest possible elliptical ROI was drawn in the vertebral body at the L1 level, excluding the cortical margins, lateral walls, endplates, and obvious syndesmophytes to avoid measurement bias. The Hu was measured 3 times and averaged to give a mean Hu to reduce observer bias. All measurements for the 524 patients were conducted by the same orthopedic spine surgeon. We used a threshold of 135 HU at the L1 vertebrae to diagnose osteoporosis, based on Ahern et al.20 and Anderson et al.21

Illustration of region of interest (ROI) for Hounsfield Unit measurement at the L1 vertebrae level in the unenhanced abdominal computed tomography scan. ROI = circle.
Statistical analysis
Demographic variables, medication histories, DXA-based T-scores, and CT-based HU values are presented as counts (percentage) or the mean ± standard deviation (SD). The independent t-test was used to compare continuous variables, and the chi-squared test was used to compare categorical variables. Simple linear regression analysis was used to determine the correlation between HU values and DXA T-scores. The significance of Pearson correlation coefficient (R-value) was determined using the t-test, with p < 0.05 considered statistically significant. The correlation strength was interpreted based on R-values, classified as follows: 0–0.19, very weak; 0.2–0.39, weak; 0.40–0.59, moderate; 0.6–0.79, strong; and 0.8–1, very strong23. Statistical computations were conducted using SPSS for Windows version 25.0 (IBM Corp., Armonk, NY, USA).
Results
The DXA-based T-scores and CT-based L1 HU values were compared between the two groups (Table 1). The mean lowest T-scores were significantly higher in the BS group than in the non-BS group (− 0.59 ± 2.65 vs. − 1.42 ± 1.38; p < 0.001). The mean spine T-score was significantly higher in the BS group than in the non-BS group (1.27 ± 3.03 vs. − 0.86 ± 1.44; p < 0.001). The mean CT-based L1 HU values were significantly lower in the BS group than in the non-BS group (41.4 ± 47.53 vs. 111.83 ± 56.34; p < 0.001).
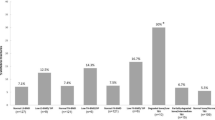
The distribution of CT-based L1 HU values across study groups is shown in Fig. 4. The CT-based HU values at the L1 level were significantly lower in the BS group than in the non-BS group (p < 0.001). Additionally, patients with osteoporosis in both groups had lower CT-based HU values, which aligns with clinical observations. Using the CT-based HU cut-off value of < 13520 identified an additional 147 (77.8%) patients in the BS group and 185 (55.2%) patients in the non-BS group as having osteoporosis, as compared to using the DXA-based classification (Table 2).

Decrease in Hounsfield Unit (HU) value at the L1 vertebrae in those with osteoporosis, as determined by Dual-energy X-ray Absorptiometry (DXA) T-score at the hip. Blue bars, non-osteoporosis subgroup (T score > − 2.5 on DXA; red bars, osteoporosis subgroup (T score ≤ − 2.5 on DXA) in patients with and without bamboo spine (BS).
The relationship between DXA T-scores and HU values was examined using linear regression analysis (Fig. 5). All scatterplots show a positive association. Subgroup analysis in non-BS patients revealed a significant moderate correlation between the lowest DXA T-scores and HU values at the L1 level (R, 0.437; p < 0.001). In the BS group, no significant correlation was found between the lowest DXA T-scores and HU values at the L1 level (R, 0.160; p = 0.129). A weak but significant correlation was observed between DXA T-scores at the hip and HU values at the L1 level in the BS group (R, 0.341; p < 0.001), but no significant correlation was seen between DXA T-scores at the spine and HU values at the L1 level.

Scatter plots illustrating positive correlations between Hounsfield Unit (HU) values and Dual-energy X-ray Absorptiometry (DXA) T-scores in different groups. (1) All ankylosing spondylitis (AS) patients; (2) AS patients without bamboo spine (BS); (3) AS patients with BS.(A) Lowest T-score; (B) spine T-Score; (C) hip T-score.
Discussion
This study is the first to report a poor correlation between the DXA-based T-score at the hip or lowest value at hip or spine and CT-based HU at the L1 level in AS patients, especially those with BS. Accordingly, DXA alone may not reflect the true BMD in those with advanced stage AS; CT-based HU at the L1 level may assist in the evaluation of BMD in the AS population. The underestimation of BMD by DXA might be caused by masking from calcification of the soft tissue and bony fusion of the facet joints in the AS spine. Our results may provide valuable information for spine surgeons treating AS patients with chance fracture or correcting ankylosing spine deformations.
The reported prevalence of osteoporosis in AS varies widely, ranging from 18.7–62%24. Explanations for the high prevalence of osteoporosis in the AS population include systemic inflammation and decreased mobility25. Because low BMD increases fracture risk, it is important for primary care physicians to accurately diagnose osteoporosis in AS patients to allow for patient counseling and education to reduce the risk of fracture. The use of a more accurate diagnostic tool will therefore improve patient care by allowing clinicians to better identify individuals within this population who are at increased risk. While we do not recommend using the CT-based HU value instead of the DXA-based T score for screening or assessing BMD in AS patients, we believe that HU values may provide valuable additional information for AS patients who undergo CT scans for other reasons.
Schreiber et al. observed a significant correlation between CT-based HU and BMD, suggesting clinical applications for CT-based HU to assess fracture risk, diagnose osteoporosis, and promote early initiation of needed treatment17. Several clinical investigations have used CT- based HU values to predict cage subsidence or screw loosening in lumbar fusion surgery26,27. CT-based HU is less affected by lumbar degeneration than DXA, as it avoids cortical bone and degenerative changes and also indicates the local surrounding bone quality at the index level28. However, the optimal cut-off value at the L1 level for diagnosing osteoporosis is still unclear. The current CT-based Hu threshold for diagnosing osteoporosis ranges from 78.517 to 13520 and is a major limitation in our clinical investigation. Study results may vary depending on the Hu threshold used to diagnose osteoporosis. Applying the 135 HU threshold20 to an Asian cohort may result in over-diagnosis of osteoporosis. Determination of the optimal HU cut-off for osteoporosis screening in this population requires further investigation through larger prospective cohort studies.
We found that CT-based HU at the L1 level (< 135) led to the re-classification of 157 AS patients with BS as having osteoporosis as compared to the original classification based on the DXA-based T-score (< − 2.5). This result suggests that DXA examination alone may underestimate the incidence of osteoporosis in the AS population. Artifacts related to the presence of syndesmophytes or other structural lesions such as an ankylosed posterior arch or a periosteal bone formation may increase the DXA-based BMD value25. In other words, the use of DXA alone to diagnose osteoporosis in advanced AS patients may not reflect the actual BMD. The use of CT-based HU in addition to DXA may improve BMD evaluation after prospective datasets are used to determine a cut-off value to re-define osteoporosis in the AS population.
For patients with severe AS who have received a CT examination for other indications, the use of CT HU may help evaluate their BMD without additional radiation exposure or the extra burden of time and cost for other DXA bone density examinations. Several studies also have reported a high incidence of osteopenic and normal DXA T-scores among AS patients with vertebral fractures18,29. This result echoes those we observed for CT-based HU, proving that CT-based HU more accurately reflects the true BMD than does DXA in AS patients. Our findings align with previous studies reporting that CT attenuation might serve as a more precise clinical indicator of fragility fractures30. These findings highlight the limitations of DXA, especially in patient with AS. In contrast, CT HU measurements are unaffected by spinal ligamentous calcification, a characteristic of AS, indicating that CT HU may provide a more accurate measure of bone quality in these patients. Although the most effective way to implement CT screening in AS patients remains to be determined, CT HU could potentially be incorporated into clinical practice as an opportunistic screening method, depending on the specific clinical objectives. These pivotal results highlight the usefulness of HU values in the advanced AS population and suggest that it may serve as a complementary tool for evaluating BMD.
Substantial evidence indicates that the false-negative rate for DXA of the spine in AP projections is higher among AS patients; therefore, follow-up studies are recommended to evaluate alternative assessment sites, such as lateral projections of the spine, femoral neck, or total hip12,31. However, these methods may still be affected by ligamentous calcification in those with advanced disease. Recent studies suggest that the trabecular bone score (TBS) is superior to DXA in detecting osteoporosis32,33. TBS is a textural parameter that measures variations in pixel gray-levels in DXA images of the lumbar spine34. However, TBS assessment is not widely available in clinical practice, and syndesmophytes may falsely increase the TBS35. Another tool for diagnosing BMD is quantitative computed tomography (QCT). However, QCT-derived T-scores do not align directly with DXA T-scores, thereby restricting the practical usefulness of this method16,36.
Although previous clinical investigations vary in the CT HU values used to diagnose osteoporosis, the L1 vertebral body serves as an excellent site for CT-based assessment of osteoporosis for several reasons. First, as the first non–rib-bearing vertebra, the L1 vertebral body is easily identifiable, increasing the efficiency of its clinical use. Second, all chest, abdominal, pelvic, and lumbar CT scans include the L1 level, allowing for its wide application in opportunistic screening without additional radiation exposure. Moreover, L1 has been comprehensively studied, and evidence suggests that lumbar spine HU values obtained from CT scans correlate with BMD and can predict osteoporosis14.
Limitations
While our study results indicate the use of CT-based HU as an alternative tool to assist BMD assessment in AS patients, it is important to note the potential limitations associated with this approach. First, the availability of CT equipment and the cost of CT scans may be prohibitive in some settings. Furthermore, the radiation exposure associated with CT scans is a critical consideration, particularly when these scans are used for routine or repeated assessment of bone density. However, if patients with severe AS have undergone CT screening for other indications, CT-based HU measurements can be used without additional radiation exposure, time, or cost. Second, this retrospective study with a small sample size may have some selection bias, and a larger prospective study is warranted to validate our results. Third, we were unable to determine a cut-off point for predicting fracture risk in the AS group based on our results using CT-based HU values at the L1 level. Fourth, due to the retrospective nature of our analysis, we did not evaluate the effect of osteoporosis drugs on changes in CT-based HU values37. Treatment with romosozumab (mean treatment time, 10.5 months) significantly increased the mean Hu by 26%, from a baseline of 85 to 107. Patients treated with teriparatide for > 12 months (mean treatment time, 23 months) had a significant improvement in the mean Hu of 25%, from 106 to 13237. Fifth, not all patients completed both the DXA and CT scan examinations simultaneously within 6 months due to retrospective analysis, and DXA examinations were not routinely performed at both the hip and the spine. By acknowledging these limitations and providing direction for future research, we hope to encourage continued exploration in this field to ultimately improve diagnostic accuracy and patient outcomes in the AS population.
Conclusions
Using the CT-based HU cut-off value of < 135, an approximate additional 78% of BS and 55% of non-BS patients were classified as having osteoporosis, as compared with using the DXA-based classification. The appearance of BS in plain spine radiographs plays an important role in affecting DXA-based BMD assessment. The use of CT-based HU as a more accurate diagnostic tool for BMD evaluation in the AS population may be recommended after further validation by studies with prospective datasets and larger patient cohorts.
Data availability
The datasets generated during and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
Abbreviations
- AP:
-
Anteroposterior
- AS:
-
Ankylosing spondylitis
- BMD:
-
Bone mineral density
- BS:
-
Bamboo spine
- CT:
-
Computed tomography
- DXA:
-
Dual-energy X-ray absorptiometry
- HU:
-
Hounsfield units
- ROI:
-
Region of interest
- SD:
-
Standard deviation
- WHO:
-
World Health Organization
References
Sieper, J. & Poddubnyy, D. Axial spondyloarthritis. Lancet 390, 73–84 (2017).
McGonagle, D., Gibbon, W. & Emery, P. Classification of inflammatory arthritis by enthesitis. Lancet 352, 1137–1140 (1998).
Hu, L. Y. et al. Should clinicians pay more attention to the potential underdiagnosis of osteoporosis in patients with ankylosing spondylitis? A National population-based study in Taiwan. PLoS One. 14, e0211835 (2019).
Karberg, K., Zochling, J., Sieper, J., Felsenberg, D. & Braun, J. Bone loss is detected more frequently in patients with ankylosing spondylitis with syndesmophytes. J. Rheumatol. 32, 1290–1298 (2005).
Bengtsson, K. et al. Occurrence and relative risks for non-vertebral fractures in patients with ankylosing spondylitis compared with the general population: a register-based study from Sweden. RMD Open. 9, e002753 (2023).
Kandregula, S. et al. Spinal fractures in ankylosing spondylitis: patterns, management, and complications in the united states - analysis of latest nationwide inpatient sample data. Neurospine 18, 786–797 (2021).
Tu, P. H. et al. Spinal cord injury and spinal fracture in patients with ankylosing spondylitis. BMC Emerg. Med. 22, 73 (2022).
World Health Organization. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO study group. World Health Organ. Tech. Rep. Ser. 843, 1–129 (1994).
Lange, U., Kluge, A., Strunk, J., Teichmann, J. & Bachmann, G. Ankylosing spondylitis and bone mineral density–what is the ideal tool for measurement? Rheumatol. Int. 26, 115–120 (2005).
Lee, Y. S. et al. Skeletal status of men with early and late ankylosing spondylitis. Am. J. Med. 103, 233–241 (1997).
Donnelly, S. et al. Bone mineral density and vertebral compression fracture rates in ankylosing spondylitis. Ann. Rheum. Dis. 53, 117–121 (1994).
Deminger, A. et al. Which measuring site in ankylosing spondylitis is best to detect bone loss and what predicts the decline: results from a 5-year prospective study. Arthritis Res. Ther. 19, 273 (2017).
Mandl, P. et al. EULAR recommendations for the use of imaging in the diagnosis and management of spondyloarthritis in clinical practice. Ann. Rheum. Dis. 74, 1327–1339 (2015).
Yang, G., Wang, H., Wu, Z., Shi, Y. & Zhao, Y. Prediction of osteoporosis and osteopenia by routine computed tomography of the lumbar spine in different regions of interest. J. Orthop. Surg. Res. 17, 454 (2022).
Emohare, O., Cagan, A., Polly, D. W. Jr. & Gertner, E. Opportunistic computed tomography screening shows a high incidence of osteoporosis in ankylosing spondylitis patients with acute vertebral fractures. J. Clin. Densitom. 18, 17–21 (2015).
Pickhardt, P. J. et al. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann. Intern. Med. 158, 588–595 (2013).
Schreiber, J. J., Anderson, P. A., Rosas, H. G., Buchholz, A. L. & Au, A. G. Hounsfield units for assessing bone mineral density and strength: a tool for osteoporosis management. J. Bone Joint Surg. Am. 93, 1057–1063 (2011).
Lee, S., Chung, C. K., Oh, S. H. & Park, S. B. Correlation between bone mineral density measured by dual-energy X-ray absorptiometry and Hounsfield units measured by diagnostic CT in lumbar spine. J. Korean Neurosurg. Soc. 54, 384–389 (2013).
Vadera, S., Osborne, T., Shah, V. & Stephenson, J. A. Opportunistic screening for osteoporosis by abdominal CT in a British population. Insights Imaging. 14, 57 (2023).
Ahern, D. P. et al. A meta-analysis of the diagnostic accuracy of Hounsfield units on computed topography relative to dual-energy X-ray absorptiometry for the diagnosis of osteoporosis in the spine surgery population. Spine J. 21, 1738–1749 (2021).
Anderson, P. A., Polly, D. W., Binkley, N. C. & Pickhardt, P. J. Clinical use of opportunistic computed tomography screening for osteoporosis. J. Bone Joint Surg. Am. 100, 2073–2081 (2018).
Kanis, J. A. et al. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 30, 3–44 (2019).
Campbell, M. J. Statistics at Square One (Wiley-Blackwell, 2021).
Kim, J. W. et al. Prevalence and factors of osteoporosis and high risk of osteoporotic fracture in patients with ankylosing spondylitis: a multicenter comparative study of bone mineral density and the fracture risk assessment tool. J. Clin. Med. 11, 2830 (2022).
Briot, K. & Roux, C. Inflammation, bone loss and fracture risk in spondyloarthritis. RMD Open. 1, e000052 (2015).
Yao, Y. C. et al. CT Hounsfield unit is a reliable parameter for screws loosening or cages subsidence in minimally invasive transforaminal lumbar interbody fusion. Sci. Rep. 13, 1620 (2023).
Zou, D., Sun, Z., Zhou, S., Zhong, W. & Li, W. Hounsfield units value is a better predictor of pedicle screw loosening than the T-score of DXA in patients with lumbar degenerative diseases. Eur. Spine J. 29, 1105–1111 (2020).
Zou, D., Li, W., Deng, C., Du, G. & Xu, N. The use of CT Hounsfield unit values to identify the undiagnosed spinal osteoporosis in patients with lumbar degenerative diseases. Eur. Spine J. 28, 1758–1766 (2019).
Alacreu, E., Moratal, D. & Arana, E. Opportunistic screening for osteoporosis by routine CT in Southern Europe. Osteoporos. Int. 28, 983–990 (2017).
Lee, S. J., Graffy, P. M., Zea, R. D., Ziemlewicz, T. J. & Pickhardt, P. J. Future osteoporotic fracture risk related to lumbar vertebral trabecular Attenuation measured at routine body CT. J. Bone Min. Res. 33, 860–867 (2018).
Klingberg, E. et al. Osteoporosis in ankylosing spondylitis - prevalence, risk factors and methods of assessment. Arthritis Res. Ther. 14, R108 (2012).
Żuchowski, P., Dura, M., Jeka, D. & Waszczak-Jeka, M. The applicability of trabecular bone score for osteoporosis diagnosis in ankylosing spondylitis. Rheumatol. Int. 42, 839–846 (2022).
Nam, S. W. et al. The usefulness of trabecular bone score in patients with ankylosing spondylitis. Korean J. Intern. Med. 36, 1211–1220 (2021).
Bousson, V., Bergot, C., Sutter, B., Levitz, P. & Cortet, B. Trabecular bone score (TBS): available knowledge, clinical relevance, and future prospects. Osteoporos. Int. 23, 1489–1501 (2012).
Rajan, R., Cherian, K. E., Kapoor, N. & Paul, T. V. Trabecular bone Score-An emerging tool in the management of osteoporosis. Indian J. Endocrinol. Metab. 24, 237–243 (2020).
Engelke, K. et al. Clinical use of quantitative computed tomography and peripheral quantitative computed tomography in the management of osteoporosis in adults: the 2007 ISCD official positions. J. Clin. Densitom. 11, 123–162 (2008).
Mikula, A. L. et al. Change in spinal bone mineral density as estimated by Hounsfield units following osteoporosis treatment with romosozumab, teriparatide, denosumab, and alendronate: an analysis of 318 patients. J. Neurosurg. Spine. 41, 309–315 (2024).
Funding
The authors received no financial or material support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
Wei Hsiung: Investigation, Formal analysis, Writing - Original DraftHsi-Hsien Lin: Formal analysis, Investigation, Data CurationYu-Cheng Yao: Conceptualization, SupervisionChun Hsiung: Investigation, Formal analysisElisa Chen: Investigation, Formal analysisShih-Tien Wang: SupervisionChien-Lin Liu: Investigation, Formal analysisPo-Hsin Chou: Conceptualization, Writing - Original Draft, Supervision.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Taipei Veterans General Hospital (No. 2023-08-010BC), and informed consent was waived by the Institutional Review Board of Taipei Veterans General Hospital due to the retrospective nature of the analysis.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hsiung, W., Lin, HH., Yao, YC. et al. CT-based hounsfield unit as an alternative osteoporosis assessment in ankylosing spondylitis patients with bamboo spine. Sci Rep 15, 35540 (2025). https://doi.org/10.1038/s41598-025-19528-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-19528-z
