
Abstract
Given the prevalence of Metabolic Syndrome (MetS) among employees and the role of lifestyle in its prevention, this study examined the effect of an educational intervention based on the Extended Parallel Process Model (EPPM) to promote a preventive lifestyle for MetS among Iranian employees. This parallel-group randomized clinical trial was conducted at Rafsanjan University of Medical Sciences in Iran from 2022 to 2023. A total of 144 employees without MetS were randomly assigned to either the intervention group (n = 72) or the control group (n = 72). Data were collected using two instruments to assess the EPPM variables and preventive lifestyle for MetS at baseline and six months after the intervention. The educational intervention for the intervention group was implemented over four weeks, and the data were analyzed using SPSS software. The primary outcome was the change in the overall preventive lifestyle score. Participants in the intervention group had an average age of 42.81 (± 8.37) years and an average employment duration of 14.85 (± 8.79) years, while the control group had an average age of 41.72 (± 7.55) years and an average employment duration of 12.66 (± 8.34) years. The results showed that prior to and following the intervention, all participants (100%) in both groups were in the danger control process. After the intervention, there was a significant increase in the mean scores of perceived efficacy (p < 0.001), perceived response efficacy (p < 0.001), self-efficacy (p < 0.001), perceived severity (p < 0.001), fear (p < 0.001), intention (p < 0.001), and adoption of a preventive lifestyle for MetS (p < 0.001) in the intervention group compared to the control group. Following the intervention, the scores for defense mechanisms (p < 0.001), and perceived susceptibility (p < 0.001) significantly decreased in the intervention group compared to the control group. Following the intervention, the control group experienced a significant decrease in their attitude score compared to the intervention group (p < 0.001). Public health professionals should prioritize shifting individuals from the fear control process to the danger control process when designing educational interventions to prevent MetS. This approach should ensure that educational content emphasizes perceived efficacy and perceived threat to promote adaptive behavioral changes.
Trial registration: Iranian Registry for Clinical Trial (the link to trial: https://www.irct.ir/trial/61288; IRCT registration number: IRCT20110727007132N21). Registered 02/02/2022. Prospectively registered.
Similar content being viewed by others

Introduction
Metabolic Syndrome (MetS) is not a disease but rather a cluster of metabolic factors, including abdominal obesity, hyperglycemia, hypertriglyceridemia, hypertension, and low levels of high-density lipoprotein (HDL) cholesterol. The combination of these factors constitutes the condition known as MetS, which serves as a predictor for both cardiovascular disease and type 2 diabetes1,2.
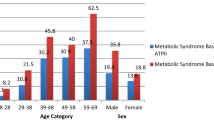
A meta-analysis indicated that the overall prevalence of MetS in Iran is 30.4%. Furthermore, it highlighted a significant upward trend in MetS prevalence across different age groups, increasing from 12.1% in individuals aged 20–29 to 51.7% among those over 603.
Literature indicates that the prevalence of MetS is particularly high among office workers and employees in Iran4,5,6. Contributing factors may include elevated Body Mass Index (BMI), insufficient physical activity, occupational stress, and low fruit consumption within this population5,6,7. Mordouei et al. found that 29.2% of employees at Rafsanjan University of Medical Sciences (RUMS) in 2016 had at least two risk factors for MetS. They suggested that increasing awareness and planning for lifestyle changes among employees is essential4. Establishing workplace health promotion programs aimed at identifying and preventing MetS is crucial for enhancing employee health5.
There is a significant association between an unhealthy lifestyle and the risk of MetS8. Lifestyle changes are the primary and most effective strategies for managing each component of MetS. These modifications not only improve all aspects of MetS but also lower the risk of developing diabetes and cardiovascular diseases9. Šoštarič et al. demonstrated that lifestyle factors significantly influence the development and management of MetS. Timely diagnosis can create early opportunities for lifestyle modification interventions in individuals who are still healthy, ultimately leading to cost savings and a reduction in disability-adjusted life years10.
Education is recognized as an important strategy for increasing awareness among the general population about MetS and the need for unhealthy lifestyle modifications11,12. The literature suggests that theory-based interventions positively influence self-care and behavior modification13,14. Behavior change theories and models serve as conceptual frameworks that assist practitioners in understanding their clients’ needs and the factors influencing specific behaviors within dietetic practice15. These theories provide insights into why individuals either engage in or refrain from certain behaviors16,17. In the present study, the Extended Parallel Process Model (EPPM) was employed as the theoretical framework for developing an educational intervention. The main elements of the EPPM include fear and threat (comprising perceived severity and perceived susceptibility), efficacy (encompassing self-efficacy and perceived response efficacy), and two response types: danger control and fear control18. Fear control is an emotional process that triggers defensive motivation when individuals encounter a significant threat but feel incapable of executing a recommended response or doubt its effectiveness. In contrast, danger control is a cognitive process that generates protective motivation, occurring when individuals believe they can effectively mitigate a significant threat through self-protective actions. During danger control, people consider strategies to address the threat, leading to changes in beliefs, attitudes, intentions, and behaviors aligned with the recommendations of the message18,19. Previous studies have demonstrated the successful application of EPPM in predicting self-care behaviors20,21 and developing intervention efforts for various health issues22,23,24.
Despite the recognition of lifestyle modifications as essential for preventing MetS, they have received insufficient attention25. Most interventions conducted globally and in Iran have primarily focused on the detection of MetS and lifestyle changes among individuals already diagnosed with it 10,26,27. More research is needed globally and in Iran on developing tailored interventions to prevent MetS through lifestyle modifications in healthy individuals who do not have this condition. There is a critical need to shift the focus of MetS diagnosis and treatment toward prioritizing primary prevention, early detection, and management of underlying atherogenic risk factors28. Additionally, due to the high prevalence of MetS among employees, who are considered a high-risk group, there are limited interventions aimed at changing habits and promoting a preventive lifestyle for MetS within this population4,5,6,7. Based on the above, the need for conducting the present study was recognized. The objective was to determine the effect of an educational intervention based on the EPPM on promoting a preventive lifestyle for MetS among a sample of Iranian employees.
Methods
Research design and participants
A parallel-group randomized clinical trial was conducted at RUMS, located in Rafsanjan, Kerman province, Iran, from 2022 to 2023. This randomized clinical trial was registered with the Iranian Registry of Clinical Crials (number 61288; Date 02/02/2022; https://www.irct.ir/trial/61288; IRCT registration number: IRCT20110727007132N21). The study is being reported following the 2010 CONSORT statement and checklist (www.consort-statement.org/).
The study participants were selected from the administrative employees of RUMS . The inclusion criteria for this study were as follows: 1) willingness to participate in the study; 2) employment in the administrative department of RUMS; 3) absence of MetS based on assessments by the research team; 4) no history of endocrine disorders or immunodeficiency; 5) no history of drug abuse; 6) no history of arteriosclerosis, coronary artery bypass surgery, or angioplasty; 7) not currently undergoing treatment for high blood sugar, high cholesterol, or high blood pressure; 8) not taking weight loss medications or specific dietary regimens; 9) not participating in sports at a professional level. The exclusion criteria included pregnancy, breastfeeding, and lack of participation in at least half of the educational classes. These criteria were evaluated using a self-reported checklist and were verified through a review of available medical records, along with baseline clinical measurements conducted by the research team.
In the current study, the components of MetS were defined as follows: the presence of obesity (waist circumference of 102 cm or more in men and 88 cm or more in women, or a BMI of 30 kg/m2 or more) along with two out of three criteria, which include high blood pressure (of 130/85 mmHg or higher, or taking antihypertensive medication), glucose metabolism disorder (fasting blood sugar of 100 mg/dL or higher, or fasting blood sugar 140 mg/dL or higher after 120 min in oral glucose tolerance test or mean HbA1C of 5.7 or higher, or use of glucose-lowering drug treatment), and an increase in non-HDL cholesterol (atherogenic dyslipidemia) (non-HDL cholesterol of 130 mg/dL or higher, or use of blood lipid-lowering medication)29.
In this diagnostic process, an expert in public health measured the weight, BMI, and blood pressure of the participants. Blood pressure was measured using an ALPK2 model V300 mercury sphygmomanometer (manufactured in Japan). Specific conditions were required for accurate blood pressure measurement, including abstaining from cigarettes, coffee, or tea, as well as refraining from vigorous physical activity or work for approximately 30 min prior to measurement. Blood pressure was measured twice from the right arm, with a 15-min interval between readings, and the average value was recorded as the blood pressure for each individual.
Weight was measured using a digital scale with a precision of 100 g, with minimal clothing and without shoes. Height was measured with a tape measure while the participant stood without shoes, ensuring that the shoulders were in a normal position. Waist circumference was assessed at its narrowest point during natural exhalation, using an inflexible tape measure with an accuracy of one millimeter, without applying any pressure to the body.
A skilled phlebotomy technician collected a fasting blood sample of 5 ml from each participant. The blood samples were then sent to the central laboratory of RUMS for laboratory tests, including fasting blood sugar, total cholesterol, triglycerides, low-density lipoprotein (LDL) cholesterol, and high-density lipoprotein (HDL) cholesterol. These tests were conducted using the Alpa Class autoanalyzer to ensure accurate results.
Since the diagnostic criteria for MetS were based on the definition introduced by Dobrowolski et al.29 participants self-reported their medical history concerning conditions such as reduced kidney function, fatty liver disease, obstructive sleep apnea, heart failure with preserved ejection fraction, polycystic ovary syndrome, chronic inflammation, sympathetic nervous system activation, and elevated uric acid levels. None of the participants reported a history of any of these conditions.
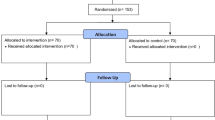
Initially, 171 employees were assessed based on the specified criteria, of which 22 were diagnosed with MetS and subsequently excluded. During the trial, 11 participants were lost to follow-up (4 from the intervention group and 7 from the control group) due to personal reasons (e.g., lack of interest and insufficient time), leaving 133 participants for the final analysis. The CONSORT flow diagram is presented in Fig. 1.

Consort flow diagram.
Randomization and blinding
Participants were initially recruited using a convenience sampling method, and once the baseline assessment was completed, they were randomly assigned to either the intervention or control groups. A research assistant utilized a web-based randomization program (Sealed Envelope.com) to assign the participants (n = 144) to either the intervention group (n = 72) or the control group (no intervention, n = 72) in a 1:1 ratio. Another research assistant, who had no involvement in the participant recruitment process, administered a follow-up questionnaire to each participant six months after the initial study. However, participants were aware of their group allocation due to the nature of the intervention. To ensure intervention fidelity and reduce cross-contamination, participants were instructed not to disclose any information about MetS to their colleagues. A researcher from the study was tasked with documenting all interactions between participants and the research team. In this study, randomization was stratified by age and gender to control for potential confounders. Additionally, although the two groups were matched, we examined the confounding effects of the baseline values of each variable using Analysis of Covariance (ANCOVA).
Sample size
Considering that the main outcome measurement tool (lifestyle) in the Persian version was translated and validated for the first time in this study, the mean and variance of the outcome in the study population were not available. Therefore, Cohen’s standardized effect size was used to calculate the sample size. Assuming a 5% probability of type 1 error, a 20% probability of type II error, and a Cohen’s standardized effect size of d = 0.5, which represents an average difference between the two groups, a sample size of 64 individuals per group was determined. Taking into account a 10% dropout rate, it was decided to include 72 participants in each group for the study. The output of G*Power software is shown below:

Measures
The primary outcome of the study was the change in the mean score of preventive lifestyle related to MetS from baseline to follow-up. The secondary outcome was the change in the mean scores of the EPPM variables over the same period.
-
(1)
Instrument to assessing preventive lifestyle for MetS:
A measurement tool consisting of 36 items, developed by Kang, was used to assess preventive lifestyle factors associated with MetS. This scale included six subscales: physical activity and weight control, eating habits, alcohol consumption and smoking, sleep and rest, stress management, and drug and health management30. The psychometric characteristics of this instrument in Persian were determined by Didehban et al.31. The items of this instrument were measured on a Likert scale ranging from 4, indicating “always,” to 1, denoting “never”.
-
(2)
Instrument to assessing EPPM variables:
Researchers in the present study developed an instrument to collect information on EPPM variables related to preventive behaviors for MetS. First, item generation (n = 51 items) for the EPPM subscales was conducted based on a literature review and face-to-face interviews with five employees and health education experts. Next, the validity and reliability of this instrument were assessed, with the results of each test presented in the following section.
-
1.
Quantitative and qualitative content validity
First, a group of ten experts in health education, nutrition, and cardiovascular diseases evaluated the content validity of the instrument items. They assessed both the quantitative and qualitative aspects of the items by applying the Content Validity Index (CVI) and Content Validity Ratio (CVR) to each item32,33. The experts used a three-point rating scale to determine the necessity of the items, classifying them as essential, useful but not essential, or not necessary. The CVR formula was employed to measure the level of agreement among the experts regarding the essentiality of each item. To calculate the CVI, the number of experts who rated an item as relevant was divided by the total number of experts. Additionally, the relevance of the items was evaluated using a four-point rating scale that ranged from not relevant to very relevant. Items with CVI < 0.79 and CVR < 0.62 were deleted32,33. In this stage, six items from three subscales (perceived severity, perceived susceptibility, and perceived response efficacy) were deleted, and three items were edited.
-
2.
Quantitative and qualitative face validity
In the next stage, qualitative and quantitative face validity of the developed instrument items was evaluated by ten employees at RUMS. They evaluated the relevance, ambiguity, and difficulty of the items. Based on their feedback, minor wording errors were corrected. The impact score of each item was assessed, with a score of ≥ 1.5 considered acceptable34. Five items were revised, and all items achieved an impact score of 1.5 or higher.
-
3.
KMO and Bartlett’s test and factor analysis
At this stage, the proposed research model underwent Exploratory Factor Analysis (EFA) using the orthogonal varimax rotation method. A total of 239 employees who met the inclusion criteria completed the instrument (Table 1).
To assess the adequacy of the sample and the suitability of the factor analysis model, the instrument was subjected to the Kaiser–Meyer–Olkin (KMO) test and Bartlett’s test of sphericity using SPSS. The final selection of items for each subscale in the research model was based on commonality indexes surpassing the threshold of 0.434. The KMO in this study was 0.729, and Bartlett’s test of sphericity yielded a significant result (χ2 = 16368.525, df = 3003, p < 0.0001), indicating that the data were suitable for factor analysis34,35.
During this stage, two items from the perceived response efficacy and three items from the perceived self-efficacy were eliminated. The factor load of each item is presented in Additional File 1. The EFA revealed that the 40 items of the EPPM could be grouped into eight factors: perceived severity, perceived susceptibility, perceived response efficacy, perceived self-efficacy, fear, defense mechanisms, behavioral intention, and attitude (Additional File 1).
-
4.
Cronbach’s alpha
In this stage, Cronbach’s alpha was used to assess the internal consistency of the EPPM subscales based on data from 30 employees. A Cronbach’s alpha estimate of ≥ 0.70 was considered satisfactory34. In this study, the Cronbach’s alpha for the EPPM subscales ranged from 0.763 to 0.994 (Additional File 1). No items were removed during this stage.
-
5.
Intraclass correlation coefficient
In this stage, to assess the external reliability of the EPPM subscales, the Intraclass Correlation Coefficient (ICC) was measured (with a 2-week interval between the tests) in the thirty employees of RUMS with similar characteristics to the target population of the study. ICC ≥ 0.70 was considered satisfactory36. The ICC values of the EPPM subscales are shown in Additional file 1. The participants completed the instruments themselves, which took approximately 15 to 25 min to complete.
Intervention program
The instruments were completed by two study groups: the intervention group and the control group. An educational intervention was designed based on the analysis of pre-test results from both groups. The intervention group participated in a program focused on EPPM variables and preventive behaviors related to MetS. Since all participants were in the danger control process prior to the intervention, educational messages and content were developed and implemented for the intervention group to enhance the components of perceived threat and perceived efficacy. This program consisted of four in-person training sessions, each lasting 60 to 80 min, conducted over a four-week period with a seven-day interval between sessions.
During the sessions, employees were divided into small groups to discuss their experiences in adopting preventive behaviors for MetS, the feasibility of these behaviors, strategies to overcome obstacles, and the importance of planning and commitment for successful implementation.
The first training session introduced the symptoms of MetS and preventive behaviors, emphasizing their significance and effectiveness. Participants were encouraged to practice these behaviors at home and document their progress on a form for future sessions. Their performance was evaluated at the beginning of each subsequent session to address any challenges and provide encouragement. Additionally, participants received a brochure titled "The Preventive Behaviors of Metabolic Syndrome." A 6-min educational video (in MP4 format) on MetS, covering its diagnostic criteria, causes, and complications, was also presented during this session.
In the second session, participants received information about the negative health outcomes of MetS, the severity of its complications, and the susceptibility to MetS across all ages and genders. They discussed the implications of defense mechanisms used for fear control and the importance of a healthy lifestyle in preventing MetS. Participants were also provided with a brochure titled “Understanding Metabolic Syndrome: We Are All at Risk”.
The third session aimed to foster positive attitudes towards adopting preventive behaviors for MetS. Participants discussed their perceptions of the effectiveness of these behaviors and were encouraged to adopt a favorable attitude towards their consequences.
The primary objective of the fourth session was to enhance self-efficacy in adopting preventive behaviors for MetS. Participants who consistently practiced these behaviors shared their positive experiences, and practical step-by-step strategies were provided to encourage further adoption. Verbal persuasion was employed to reassure participants that they could successfully maintain a preventive lifestyle for MetS.
At the end of the intervention, participants received a booklet titled "Understanding Metabolic Syndrome: Is It Preventable?" This booklet began with a scenario about a 40-year-old man named Mr. Alavi, an employee who did not lead a healthy lifestyle. During the organization’s screening tests, he discovered several risk factors for MetS. The doctor informed him that these risk factors could be reduced through various methods. The booklet defined MetS and included information on its prevalence, causes, complications, and preventive measures. It also contained brief messages to enhance self-efficacy in adopting a healthy lifestyle, highlight the effectiveness of lifestyle changes, and emphasize the preventability of MetS. The content was verified by experts from health education, nutrition, and medicine.
Additionally, a virtual channel on Rubika, a proprietary cross-platform Iranian messaging app, was created to allow participants to ask questions. Thirty short messages covering all discussed topics were prepared and sent through this channel, along with educational materials for further reference. Both groups were followed up after six months, and a post-test survey was conducted.
Statistical analyses
The data were analyzed using the SPSS statistical software package (English version 13). The homogeneity of baseline demographic characteristics between the two groups was assessed using Chi-square tests and independent-samples t-tests. The normality of the data was evaluated with the Kolmogorov–Smirnov test. To assess whether an individual is in danger control or fear control, the EPPM proposes a simple calculation of a discriminating value. This involves subtracting the overall threat score from the overall efficacy score. A positive result indicates that the individual is in danger control, while a negative result signifies that the individual is in fear control18. Analysis of Covariance (ANCOVA) were used to compare differences in EPPM variables and the adoption of preventive lifestyles for MetS between the groups. Student’s paired-samples t-test was conducted to examine differences in EPPM variables and the adoption of preventive lifestyles for MetS before and after the intervention within each group. Results are presented as means and standard deviations, with a significance level of p < 0.05 considered statistically significant. The Cohen’s d effect size (ES) was calculated to measure the difference between the means of two groups and classified as follows: 0.20 for small effects, 0.50 for moderate effects, 0.80 for large effects, and 1.30 for very large effects37.
Ethics statement
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki, and all procedures involving human subjects received approval from the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.REC.1400.851). The participants were provided with information about the study’s objectives, and they provided written consent to participate.
Results
-
1)
Baseline characteristics
There was a 7.63% loss to follow-up. Eleven participants were excluded for personal reasons, including lack of interest and insufficient time. The average age of participants in the intervention and control groups was 42.81 (± 8.365) and 41.72 (± 7.549), respectively. Table 1 presents other demographic characteristics of the participants in both groups. The results of the independent samples t-test indicated no statistically significant differences between the two groups regarding age and years of employment. Additionally, the Chi-Square test results showed no significant differences in gender, educational level, and marital status between the two groups, as detailed in Table 1.
-
2)
Primary outcome: adopting a preventive lifestyle for MetS.
The results indicated that after the intervention, the score for adopting a preventive lifestyle for MetS (Intervention: 117.308 ± 7.393 vs. Control: 83.000 ± 13.444; Effect size = 0.720, p < 0.001) significantly increased in the intervention group compared to the control group. Considering the reported effect size, we can conclude that the intervention had a moderate to large impact on the adoption of a preventive lifestyle for MetS.
Furthermore, the results of paired-samples t-test indicated that there were no significant differences in the mean score for the adoption of a preventive lifestyle for MetS in the control group before and after the intervention (see Table 2).
-
3)
Secondary outcomes: EPPM variables
The intervention’s effect on the EPPM variables is detailed in Table 2. The results showed that after the intervention, the score for behavioral intention significantly increased in the intervention group (13.176 ± 2.424) compared to the control group (11.569 ± 2.417), with an effect size of 0.101 (p < 0.001). Additionally, the control group experienced a significant decrease in their attitude score compared to the intervention group (Intervention: 24.411 ± 2.781 vs. Control: 21.123 ± 5.829; effect size = 0.115, p < 0.001) after the intervention. Considering the reported effect sizes, we can conclude that the intervention had a small impact on both behavioral intention and attitude.
Perceived efficacy was assessed by the sum of the means of two variables: perceived response efficacy and self-efficacy. After the intervention, there was a significant increase in the mean score of perceived efficacy (Intervention: 88.000 ± 4.210 vs. Control: 76.230 ± 10.575; effect size = 0.360, p < 0.001), as well as in its two components: perceived response efficacy (Intervention: 51.808 ± 3.214 vs. Control: 44.076 ± 7.818; effect size = 0.301, p < 0.001) and self-efficacy (Intervention: 36.191 ± 2.131 vs. Control: 32.153 ± 4.744; effect size = 0.237, p < 0.001) in the intervention group compared to the control group. Based on the reported effect sizes, we can conclude that the intervention had a small to moderate impact on all three measures.
Perceived threat was calculated as the sum of the means of two variables: perceived severity and perceived susceptibility. The results indicated that after the intervention, the perceived threat score in the intervention group was not significantly different from that of the control group (Intervention: 28.235 ± 2.407 vs. Control: 28.400 ± 4.114; effect size = 0.001, p = 0.751). However, one component, perceived severity, showed a significant increase in the intervention group compared to the control group (Intervention: 22.558 ± 1.748 vs. Control: 19.923 ± 3.420; effect size = 0.201, p < 0.001) after the intervention. Conversely, the other component, perceived susceptibility, exhibited a significant decrease in the intervention group compared to the control group (Intervention: 5.576 ± 2.215 vs. Control: 8.476 ± 2.180; effect size = 0.298, p < 0.001) after the intervention. Based on the reported effect sizes, we can conclude that the intervention had a small impact on both perceived susceptibility and perceived severity.
After the intervention, the score for fear of MetS significantly increased in the intervention group (Intervention: 13.544 ± 1.587 vs. Control: 9.846 ± 2.948; effect size = 0.381, p < 0.001) compared to the control group. Considering the reported effect size, we can conclude that the intervention had a small to moderate impact on fear of MetS.
The total score of defense mechanisms (Intervention: 12.985 ± 4.286 vs. Control: 20.538 ± 6.912; effect size = 0.307, p < 0.001) and its three subscales—perceived manipulation (Intervention: 6.426 ± 2.111 vs. Control: 10.446 ± 3.495; effect size = 0.334, p < 0.001), defensive avoidance (Intervention: 3.220 ± 1.048 vs. Control: 4.907 ± 1.893; effect size = 0.238, p < 0.001), and message minimization (Intervention: 3.338 ± 1.531 vs. Control: 5.184 ± 2.022; effect size = 0.213, p < 0.001)—as fear control responses, significantly decreased in the intervention group compared to the control group after the intervention (see Table 3). Based on the reported effect sizes, we can conclude that the intervention had a small to moderate impact on the overall score of defense mechanisms.
Furthermore, the results of the paired-samples t-test showed no significant differences in the mean scores of EPPM variables (except for attitude) in the control group before and after the intervention (see Tables 2,3). The findings indicated that prior to and following the intervention, all participants (100%) in both groups were in the danger control process.
Discussion
This study aimed to examine the effect of an educational intervention based on the EPPM on the preventive lifestyle of MetS among a sample of Iranian employees. Among the danger control responses, which encompass attitude, intention, and behavior changes, the results indicated that after the intervention, the scores for behavioral intention and the adoption of a preventive lifestyle for MetS significantly increased in the intervention group compared to the control group. Considering the reported effect size, we can conclude that the intervention had a moderate to large impact on the adoption of a preventive lifestyle for MetS.
In line with our findings, Tejera et al. reported a notable reduction in four out of five features of MetS among obese adults who participated in a program promoting healthy lifestyle habits over six weekly sessions38. Orchard et al. demonstrated that the incidence of MetS was reduced by 41% in the group receiving lifestyle intervention and by 17% in the group receiving metformin therapy, compared to the group receiving placebo39. Pozar et al. reported that a nutrition education intervention can alter the prevalence of certain risk factors for MetS, such as BMI and total cholesterol levels in adults40. Since most interventions have focused on individuals with MetS, it is essential for health professionals in each country to design and implement more educational programs aimed at improving community lifestyles to prevent MetS.
Findings showed that the control group experienced a significant decrease in their attitude score compared to the intervention group after the intervention. The findings of the present study are inconsistent with the conclusions of a study conducted by Didehban et al., which highlighted that educational interventions could alter attitudes and enhance the adoption of preventive behaviors related to MetS among a group of Iranian employees31. Similarly, Askari et al. found that educational interventions could increase attitude score and improve metabolic indices in elderly patients with type II diabetes41. This discrepancy may be attributed to variations in follow-up periods, intervention methodologies, or the specific population studied. This suggests that factors beyond perceived threat and perceived efficacy may have influenced participants’ attitude. Variables such as perceived barriers, enabling factors, and social support could play a significant role, but these elements are not included in the developed EPPM. The researchers should consider refining the EPPM by incorporating these additional variables to enhance understanding of the mechanisms underlying behavior and attitude changes. Conducting qualitative research could provide deeper insights into participants’ experiences, along with the barriers and facilitators influencing attitude changes related to preventive behaviors for MetS.
When individuals possess high levels of perceived efficacy (a combination of perceived response efficacy and perceived self-efficacy) and perceived threat (a combination of perceived severity and perceived susceptibility), it triggers protective motivation, prompting individuals to make adaptive changes42. In the present study, the educational intervention increased the mean scores of perceived severity, perceived response efficacy, and self-efficacy in the intervention group compared to the control group. Considering the reported effect sizes, we can conclude that the intervention had a small to moderate impact on the components of response efficacy and a small impact on the components of perceived threat. Since all participants were in the danger control process prior to the intervention, educational messages and content were developed and implemented for the intervention group to enhance the components of perceived threat and perceived efficacy. Therefore, the increase in these variables in the intervention group is justified. In line with this, Karimzadeh Shiraz et al. demonstrated that implementing an educational intervention based on health belief model could modify women’s perceptions of severity and self-efficacy concerning the adoption of preventive behaviors for MetS43. Okube et al. demonstrated that developing and implementing an educational intervention based on the Transtheoretical model could enhance self-efficacy score and promote the adoption of a healthy lifestyle among patients with MetS44. Roberto et al. demonstrated that physicians who perceived a higher threat to their patients and had greater efficacy exhibited increased intentions and behaviors to assess their patients’ kidney function45. Similarly, Babafunke et al. concluded that creating messages with an appropriate balance of threat and efficacy tailored to diverse audiences would likely promote the adoption and implementation of recommended COVID-19 preventive measures46.
The results indicated a significant decrease in the defense mechanisms score and its three subscales—perceived manipulation, defensive avoidance, and message minimization—among participants in the intervention group compared to the control group after the intervention. Considering the reported effect size, we can conclude that the intervention had a small to moderate impact on the overall score of defense mechanisms. The decrease in the score for defense mechanisms and its subscales may be attributed to the significant impact of the intervention on increasing the perceived efficacy score in the intervention group compared to the control group. However, the overall perceived threat score did not show a significant difference between the two groups after the intervention. Previous studies have highlighted associations between the use of defense mechanisms and various outcomes47,48. Health professionals should identify the types of defense mechanisms individuals use when confronted with the threat of MetS and work to enhance their perceived efficacy in engaging in preventive behaviors through education.
The results indicated a significant increase in the fear score among participants in the intervention group compared to the control group after the intervention. Considering the reported effect size, we can conclude that the intervention had a small to moderate impact on the score of fear related to MetS. In this study, it was anticipated that fear would increase in the intervention group alongside the rise in perceived severity of MetS during the post-intervention phase. The role of fear in triggering behavior change has been highlighted in various studies. For instance, Harper et al. found that the primary predictor of favorable behavior modifications—such as practicing social distancing and improving hand hygiene—among their study participants was the fear of COVID-1949. Fear appeals have great potential to drive behavior changes, but they can also backfire. Cognitive elements play a crucial role in the effectiveness of fear appeals by engaging danger control processes. In contrast, the emotion of fear can lead to the ineffectiveness of these appeals, manifesting as defensive avoidance or reactance through fear control processes50. A meta-analysis indicated that strong fear appeals combined with high-efficacy messages result in the most significant behavior changes, while strong fear appeals paired with low-efficacy messages lead to the highest levels of defensive responses51. Mishi et al. concluded that fear appeals are effective in encouraging participants to adopt pandemic preventive measures, thus promoting positive behavioral change. The effectiveness of this approach varies based on factors such as gender and population group, particularly when it is combined with self-efficacy and socio-cultural considerations52. Health professionals should consciously use fear appeals to enhance the effectiveness of messages about the complications of MetS. They should take into account individuals’ cognitive and demographic characteristics to assess the threat level posed by messages about MetS. Additionally, when delivering threatening messages, it is important to provide a series of messages designed to enhance individuals’ self-efficacy in reducing the risk of developing MetS.
Strengths and limitations of the study
Although the present study was one of the few theory-based intervention efforts conducted in Iran focusing on primary prevention among employees without MetS at the time of the study, it had several limitations. Due to time constraints in postgraduate courses, the follow-up duration was limited to 6 months. Future studies should include longer follow-up periods to assess the sustainability of lifestyle change and the long-term impact on MetS prevention.
In this study, biomarkers, such as blood pressure and cholesterol levels, were measured only before the intervention to identify participants without MetS. Data on preventive lifestyles for MetS were collected using a self-report instrument, which could introduce potential response bias in the findings. It is recommended that these biomarkers be measured both before and during the follow-up periods after the intervention.
Given the employees’ workloads, this study utilized both virtual and in-person channels to communicate with participants in the intervention group and present content. Future studies should evaluate the impact of the educational intervention through each of the two communication channels on individuals’ preventive lifestyles for MetS separately.
Another limitation of this study is its focus on participant engagement within the study, without accounting for variations in engagement outside the study environment.
Since the educational intervention was designed and implemented for a specific group of employees at a university and within a city, the findings cannot be generalized to other population groups in Iran. It is recommended to conduct similar studies in diverse populations (e.g., different occupational groups and geographic regions) to enhance the generalizability of the results.
Suggestions for future research
The instrument developed in this study is proposed for assessing the factors influencing the adoption of preventive behaviors related to MetS within the framework of the EPPM. Healthcare providers require instruments that are validated across cultures to evaluate the implementation of interventions and their outcomes. Therefore, it is recommended to assess the psychometric properties of the instrument across diverse cultures and countries. It is recommended that similar interventions aimed at preventing MetS in healthy individuals without the condition be developed and implemented in other countries, taking into account lifestyle habits and demographic information.
Additionally, it is recommended to design theory-based educational interventions to eliminate risk factors for MetS in affected individuals. Greater efforts are also needed to apply and test the EPPM as a theoretical framework for developing public health campaigns aimed at preventing other chronic diseases. It is recommended that future studies conduct qualitative research to uncover deeper insights into participants’ experiences, as well as the barriers and facilitators that influence their attitudes toward adopting preventive behaviors for MetS.
Conclusion
Our findings suggest that developing educational interventions based on the EPPM variables can enhance a healthy lifestyle among employees without MetS. By balancing fear appeals with efficacy-building strategies, health educators can promote adaptive danger control responses and encourage long-term preventive behaviors. It is recommended to test this theoretical framework in the development of educational initiatives for individuals with MetS and other prevalent health conditions. To promote behavior changes aimed at the primary prevention of MetS, a comprehensive program should be implemented, led by trained health professionals for employees in Iran.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request. Please contact the corresponding author for the data requests.
References
Wang, H. H., Lee, D. K., Liu, M., Portincasa, P. & Wang, D. Q. Novel insights into the pathogenesis and management of the metabolic syndrome. Pediatr. Gastroenterol. Hepatol. Nutr. 23(3), 189–230. https://doi.org/10.5223/pghn.2020.23.3.189 (2020).
Nilsson, P. M., Tuomilehto, J. & Rydén, L. The metabolic syndrome—What is it and how should it be managed?. Eur. J. Prev. Cardiol. 26(2_suppl), 33–46. https://doi.org/10.1177/2047487319886404 (2019).
Kalan Farmanfarma, K. et al. Prevalence of metabolic syndrome in Iran: A meta-analysis of 69 studies. Diabetes Metab. Syndr. 13(1), 792–799. https://doi.org/10.1016/j.dsx.2018.11.055 (2019).
Mordouei, Z. et al. The survey of metabolic syndrome frequency and its factors in employees of Rafsanjan University of Medical Sciences faculties in 2016: A short report. JRUMS. 16(8), 789–796 (2017).
Alavi, S. S., Makarem, J., Mehrdad, R. & Abbasi, M. Metabolic syndrome: A common problem among office workers. Int. J. Occup. Environ. Med. 6(1), 34–40. https://doi.org/10.15171/ijoem.2015.492 (2015).
Niazi, E., Saraei, M., Aminian, O. & Izadi, N. Frequency of metabolic syndrome and its associated factors in health care workers. Diabetes Metab. Syndr.: Clin. Res. Rev. 13(1), 338–342. https://doi.org/10.1016/j.dsx.2018.10.013 (2019).
Listyandini, R., Dewi Pertiwi, F., Puspa-Riana, D. & Asih Lestari, W. The dominant factor of metabolic syndrome among office workers. J. Health Sci. Prev. 5(1), 40–47. https://doi.org/10.29080/jhsp.v5i1.421 (2021).
Park, Y. S., Kang, S. H., Jang, S. I. & Park, E. C. Association between lifestyle factors and the risk of metabolic syndrome in the South Korea. Sci. Rep. 12(1), 13356. https://doi.org/10.1038/s41598-022-17361-2 (2022).
Kim, H. L. et al. Lifestyle modification in the management of metabolic syndrome: Statement from Korean Society of CardioMetabolic Syndrome (KSCMS). Korean Circ. J. 52(2), 93–109. https://doi.org/10.4070/kcj.2021.0328 (2022).
Šoštarič, A. et al. Detection of metabolic syndrome burden in healthy young adults may enable timely introduction of disease prevention. Arch. Med. Sci. 15(5), 1184–1194. https://doi.org/10.5114/aoms.2019.87462 (2019).
Soósová, M. S. & Hrehová, J. The effect of education on lifestyle changes and metabolic syndrome components. Cent. Eur. J. Nurs. Midw. 5(4), 161–168. https://doi.org/10.15452/CEJNM.2014.05.0012 (2014).
Nádas, J., Putz, Z., Jermendy, G. & Hidvégi, T. Public awareness of the metabolic syndrome. Diabetes Res. Clin. Pract. 76(1), 155–156. https://doi.org/10.1016/j.diabres.2006.07.017 (2007).
Ghoreishi, M. S., Vahedian-Shahroodi, M., Jafari, A. & Tehranid, H. Self-care behaviors in patients with type 2 diabetes: Education intervention base on social cognitive theory. Diabetes Metab Syndr. 13(3), 2049–2056. https://doi.org/10.1016/j.dsx.2019.04.045 (2019).
Tavakoly Sany, S.B., Ferns, G.A., Jafari, A. The effectiveness of an educational intervention based on theories and models on diabetes outcomes: a systematic review. Curr Diabetes Rev. 16(8), 859-868. https://doi.org/10.2174/1573399816666191223110314 (2020).
Spahn, J. M. et al. State of the evidence regarding behavior change theories and strategies in nutrition counseling to facilitate health and food behavior change. J. Am. Diet Assoc. 110(6), 879–891. https://doi.org/10.1016/j.jada.2010.03.021 (2010).
Croyle, R. T. Theory at a Glance: Application to Health Promotion and Health Behavior 2nd edn. (United States Department of Health and Human Services, National Cancer Institute, 2005).
Jackson, C. Behavioral science theory and principles for practice in health education. Health Educ. Res. 12, 143–150. https://doi.org/10.1093/her/12.1.143 (1997).
Popova, L. The extended parallel process model: Illuminating the gaps in research. Health Educ. Behav. 39(4), 455–473. https://doi.org/10.1177/1090198111418108 (2012).
Witte, K., Cameron, K. A., McKeon, J. K. & Berkowitz, J. M. Predicting risk behaviors: Development and validation of a diagnostic scale. J. Health Commun. 1, 317–341. https://doi.org/10.1080/108107396127988 (1996).
Lael-Monfared, E. et al. Health literacy, knowledge and self-care behaviors to take care of diabetic foot in low-income individuals: Application of extended parallel process model. Diabetes Metab. Syndr. 13(2), 1535–1541. https://doi.org/10.1016/j.dsx.2019.03.008 (2019).
Abawari, M. J., Amdisa, D., Birhanu, Z. & Kebede, Y. Response to self-care practice messages among patients with diabetes mellitus visiting Jimma University medical center facility based cross sectional design application of extended parallel process model. PLoS ONE 16(12), e0261836. https://doi.org/10.1371/journal.pone.0261836 (2021).
Termeh Zonouzy, V., Niknami, S., Ghofranipour, F. & Montazeri, A. An educational intervention based on the extended parallel process model to improve attitude, behavioral intention, and early breast cancer diagnosis: A randomized trial. Int. J. Womens Health. 11, 1–10. https://doi.org/10.2147/IJWH.S182146 (2018).
Hosseini-Amiri, M., Aliyari, S., Zareiyan, A. & Dabbagh-Moghadam, A. The effects of extended parallel process model on obese soldiers’ knowledge, attitudes, and practices about obesity management: a randomized controlled clinical trial. Iran J. Nurs. Midwifery Res. 23(6), 458–464. https://doi.org/10.4103/ijnmr.IJNMR_141_17 (2018).
Gerayllo, S., Ali Morowatisharifabad, M., Jouybari, L., Karimiankakolaki, Z. & Sadeghi, R. Design and evaluation of a theory-based intervention of knowledge and perceptions to improve self-care amongst relatives of esophageal cancer patients: A randomised controlled trial study protocol. Int. J. Surg. Protoc. 24, 12–16. https://doi.org/10.1016/j.isjp.2020.09.001 (2020).
Rabbani, B., Chiti, H., Sharifi, F. & Mazloomzadeh, S. Effect of lifestyle modification for two years on obesity and metabolic syndrome components in elementary students: A community- based trial. Caspian J. Intern, Med. 13(3), 555–566. https://doi.org/10.22088/cjim.13.3.555 (2022).
Rahimi, G. R. M., Yousefabadi, H. A., Niyazi, A., Rahimi, N. M. & Alikhajeh, Y. Effects of lifestyle intervention on inflammatory markers and waist circumference in overweight/obese adults with metabolic syndrome: A systematic review and meta-analysis of randomized controlled trials. Biol. Res. Nurs. 24(1), 94–105. https://doi.org/10.1177/10998004211044754 (2022).
Jeitler, M. et al. A randomized controlled trial of fasting and lifestyle modification in patients with metabolic syndrome: effects on patient-reported outcomes. Nutrients 14(17), 3559. https://doi.org/10.3390/nu14173559 (2022).
Scott, C. L. Diagnosis, prevention, and intervention for the metabolic syndrome. Am. J. Card. 92(1), 35–42. https://doi.org/10.1016/S0002-9149(03)00507-1 (2003).
Dobrowolski, P. et al. Metabolic syndrome—a new definition and management guidelines. Arch. Med. Sci. 18(5), 1133–1156 (2022).
Kang, S. W. The validity and reliability of a lifestyle evaluation tool for patients with metabolic syndrome. J. Korean Acad. Fundam. Nurs. 17, 487–497 (2010).
Didehban, S., Dehdari, T., Janani, L. & Masoudkabir, F. Employees’ behaviors concerning metabolic syndrome prevention: A cellphone-based text message education intervention. J. Teh Univ. Heart. Ctr. 16(4), 162–168 (2021).
Lawshe, C. H. A quantitative approach to content validity. Pers Psychol. 28, 563–575. https://doi.org/10.1111/j.1744-6570.1975.tb01393.x (1975).
Polit, D.F. & Beck, C.T. Nursing research: principles and methods. LWW. (2004).
Hajizadeh, E. & Asghari, M. Statistical methods and analysies in health and biosciences a research methodological approach. 401-421 (Jahade Daneshgahi Publications, 2011).
Wang, J. & Wang, X. Structural equation modeling: Application using Mplus. 17–23 (Chichester: John Wiley & Sons, 2012).
Clark, R. A. et al. Reliability and concurrent validity of the Microsoft Xbox One Kinect for assessment of standing balance and postural control. Gait Posture. 42(2), 210–213. https://doi.org/10.1016/j.gaitpost.2015.03.005 (2015).
Sullivan, G. M. & Feinn, R. Using effect size-or why the p value is not enough. J. Grad. Med. Educ. 4(3), 279–282. https://doi.org/10.4300/JGME-D-12-00156.1 (2012).
Tejera, C. et al. Reducing metabolic syndrome through a group educational intervention program in adults with obesity: IGOBE Program. Nutrients 14(5), 1066. https://doi.org/10.3390/nu14051066 (2022).
Orchard, T. J. et al. Diabetes prevention program research group the effect of metformin and intensive lifestyle intervention on the metabolic syndrome: The diabetes prevention program randomized trial. Ann. Intern Med. 142(8), 611–619. https://doi.org/10.7326/0003-4819-142-8-200504190-00009 (2005).
Požar, H. et al. Effects of nutritional education on metabolic syndrome parameters in a sample of adults in Subotica, Northern Serbia. Discov Public Health. 21, 70. https://doi.org/10.1186/s12982-024-00189-8 (2024).
Askari, A., Jeihooni, A. K., Kashfi, S. M., Marzban, A. & Khiyali, Z. The effect of educational program based on belief, attitude, subjective norm, and enabling factors model on changing the metabolic indices in elderly patients with type II diabetes. Int. J. Prev. Med. 9, 74. https://doi.org/10.4103/ijpvm.IJPVM_308_16 (2018).
Witte, K. Putting the fear back into fear appeals: The extended parallel process model. Commun. Monogr. 59(4), 329–349. https://doi.org/10.1080/03637759209376276 (1999).
Karimzadeh Shirazi, K., Davoodi, S. & Akbartabar Toori, M. Effect of educational intervention based on the health belief model to promote metabolic syndrome preventive behaviors in premenopausal women over 40. J. Clinic Care Skill. 1(4), 181–187 (2020).
Okube, O. T. & Kimani, S. T. Effectiveness of trans-theoretical model-based health education intervention in the promotion of lifestyle changes among adults with metabolic syndrome: A randomized controlled trial. SAGE Open Nurs. 10, 23779608241251656. https://doi.org/10.1177/23779608241251658 (2024).
Roberto, A. J. & Goodall, C. E. Using the extended parallel process model to explain physicians’ decisions to test their patients for kidney disease. J. Health Commun. 14(4), 400–412. https://doi.org/10.1080/10810730902873935 (2009).
Babafunke, F. et al. Perceived risk and protective behaviors related to COVID-19 among the Nigerian general population: An application of the extended parallel process model. Sci. Afr. 16, e01259. https://doi.org/10.1016/j.sciaf.2022.e01259 (2022).
Di Giuseppe, M. et al. Defense mechanisms in cancer patients: A systematic review. J. Psychosom. Res. 115, 76–86. https://doi.org/10.1016/j.jpsychores.2018.10.016 (2018).
Hyphantis, T., Goulia, P. & Carvalho, A. F. Personality traits, defense mechanisms and hostility features associated with somatic symptom severity in both health and disease. J. Psychosom. Res. 75(4), 362–369. https://doi.org/10.1016/j.jpsychores.2013.08.014 (2013).
Harper, C. A., Satchell, L. P., Fido, D. & Latzman, R. D. Functional fear predicts public health compliance in the COVID-19 pandemic. Int. J. Ment. Health Addict. 19, 1875–1888. https://doi.org/10.1007/s11469-020-00281-5 (2021).
Witte, K. Fear control and danger control: A test of the extended parallel process model (EPPM). Commun. Monogr. 61(2), 113–134. https://doi.org/10.1080/03637759409376328 (1994).
Witte, K. & Allen, M. A meta-analysis of fear appeals: Implications for effective public health campaigns. Health Educ. Behav. 27(5), 591–615. https://doi.org/10.1177/109019810002700506 (2000).
Mishi, S., Mushonga, F. B. & Anakpo, G. The use of fear appeals for pandemic compliance: A systematic review of empirical measurement, fear appeal strategies and effectiveness. Heliyon. 10(9), e30383. https://doi.org/10.1016/j.heliyon.2024.e30383 (2024).
Acknowledgements
This research was supported by Iran University of Medical Sciences (Code number: 22497). The funding body had no role in the design, analysis, interpretation, or reporting of the study results. We would like to thank the employees of RUMS for their participation in the study.
Author information
Authors and Affiliations
Contributions
FEFA and TD were the supervisors of the study, developed the study, interpreted the results, wrote and edited the manuscript. SSHZ collected the data, conducted the intervention, drafted and wrote the manuscript. MA and STR were the consultant of the study, contributed towards the intervention design and implement. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent to participate
All the participants read a statement that explained the purpose of the study and provided written informed consent before participation in the study. The participants were reminded that the study was voluntary, confidential and the results would remain anonymous. Ethics approval was obtained from the Ethics Committee of Iran University of Medical Sciences (no. IR.IUMS.REC.1400.851).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hosseini Zijoud, SS., Dehdari, T., Ebadi Fard Azar, F. et al. Effect of an educational intervention using the extended parallel process model on preventive lifestyle for metabolic syndrome among Iranian employees. Sci Rep 15, 41806 (2025). https://doi.org/10.1038/s41598-025-25720-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-25720-y
